

Abstract
This study considers potential policy responses to the still very high levels of exposure to arsenic (As) caused by drinking water from shallow tubewells in rural Bangladesh. It examines a survey of 4,109 households in 76 villages of Araihazar upazila conducted two years after a national testing campaign swept through the area. The area is adjacent to the region where a long-term study was initiated in 2000 and where households are periodically reminded of health risks associated with well-water elevated in As. Results confirm that testing spurs switching away from unsafe wells, although the 27% fraction who switched was only about half of that in the long-term study area. By village, the fraction of households that switched varied with the availability of safe wells and the distance from the long-term study area. Lacking follow-up testing, two years only after the campaign 21% of households did not know the status of their well and 21% of households with an unsafe well that switched did so to an untested well. Well testing is again urgently needed in Bangladesh and should be paired with better ways to raise awareness and the installation of additional deep community wells.
Keywords: Groundwater, arsenic, mitigation, Bangladesh
INTRODUCTION
The scale of the groundwater arsenic (As) problem in Bangladesh was recognized in the mid-1990s but mitigation of this public health crisis has stagnated. The first representative national survey showed that a population of 57 million was exposed in 2000 to levels up to a hundred times the World Health Organization guideline of 10 μg/L for As in drinking water (BGS/DPHE, 2001; WHO, 2011). Two national drinking-water surveys conducted since indicate a decline in the population exposed relative to the same guideline from 52 million in 2009 to 40 million in 2013, which is still an enormous number (BBS/UNICEF, 2011, 2015). Relative to the outdated Bangladesh drinking water standard of 50 μg/L, the corresponding decline in the exposed population over the same period has been from an initial 35 to 22 and 20 million, respectively.
Epidemiological studies conducted in Bangladesh over the past two decades have linked a range of illnesses to As exposure from drinking well-water, including cardio-vascular disease and cancers of the lung, liver, and bladder in adults, and reduced intellectual and motor function in children (Smith et al., 2000; Wasserman et al., 2004; Argos et al., 2010; Chen et al., 2011; Sohel et al., 2012). On the basis of these studies, Flanagan et al. (2012) calculated an As-related mortality rate of 1 in every 18 adults over the next 20 years in Bangladesh associated with US$13 billion in economic losses, to which Pitt et al. (2015) add an estimated 9% reduction in household income associated with each As-exposed income earner across his or her lifetime.
The task of further reducing the exposure to As in rural Bangladesh through new safe sources is enormous yet progress clearly is possible. Flanagan et al. (2012) report that investing US$11 per capita in mostly deep community wells lowered the exposure of a large population in the highly affected district of Comilla. In the less severely affected area of Araihazar upazila, a sub-district 20 km east of Dhaka, community wells reaching low-As aquifers at intermediate depths have provided low-As water to the surrounding populations for over a decade for an initial investment closer to US$1 per capita (van Geen et al., 2003; 2007). Community wells for the 40 million villagers still exposed to As >10 μg/L nationally would therefore require investment in the range of US$40–440 million, less than one tenth the cost of no action of over US$10 billion. Such an investment could double the already large number of deep community wells installed across the country over the past decade (DPHE/JICA, 2009; Ravenscroft et al., 2014).
Installing more community wells alone will not be sufficient to further reducing As exposure, however. Surveys conducted after blanket well-testing under the government’s Bangladesh Arsenic Mitigation and Water Supply Program (BAMWSP) that ended in 2005 indicate a surprisingly large number of new installations of private wells that have remained largely untested (Ahmed et al., 2006; Opar et al., 2007; WASH, 2008; George et al., 2012, van Geen et al., 2014). For deep community wells to have the desired impact on household decisions, villagers must know if the wells that they own are safe or unsafe, given that fetching water from their well typically requires less effort than walking to a community well (Madajewicz et al., 2007). An additional benefit of testing wells is that, lacking a deep community well, households in many villages currently using an unsafe well have the option of walking to tested, safe neighboring wells to collect water (van Geen et al., 2002; George et al., 2012). These nearby switching options have little or no financial cost but can be hampered by social barriers (Johnston et al., 2014). The cost of blanket testing approximately 10 million wells in the affected portions of the country would be on the order of U$20 million if a durable placard with the test result is provided (van Geen et al. 2014). The additional cost of maintenance testing to keep up with the replacement of 10% of wells annually would be about US$2 million/year.
To inform policy responses, the present study focuses on learning from the initial impacts the BAMWSP testing campaign had on household reactions to As more than a decade ago. The findings are based on a household survey conducted in 76 villages in 2005, two years after testers hired under BAMWSP covered the study area using field kits. The aggregate switching in this area has previously been reported (Ahmed et al., 2006; Balasubramanya et al., 2013) but the impact of testing on household reactions was not interpreted geographically to the extent it is here. New features of the study include recording the location and As status of wells that households switched to and switching from untested wells. The study highlights the importance of raising awareness by relating household responses in the surveyed area to that of an adjacent region where, since 2000, households have been periodically reminded of the health risks associated with well-water elevated in under the Health Effects of Arsenic Longitudinal Study (HEALS) described by Ahsan et al. (2006).
METHODS
Data collection
The household survey was conducted in Araihazar upazila between March and June 2005 (Fig. 1) following approval from the Columbia University IRB. Growing rice and other crops is the traditional activity in this area about 20 km east of Dhaka (Fig. 2), but textile and other industries have been developing rapidly. By 2003, essentially all the wells in the upazila had been tested for As by BAMWSP using a reasonably accurate field kit as part of a blanket national survey (van Geen et al., 2005). Each well was painted red (or painted green) if the field kit’s test result was over (at or below) the national standard for drinking water in Bangladesh of 50 μg/L As.
Figure 1.
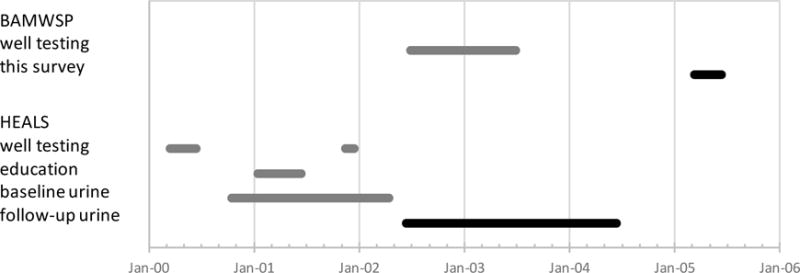
Timeline of interventions and surveys conducted in Araihazar. Within the area considered in this study, this includes testing of wells conducted under BAMWSP (grey line) and the present response survey (black line). Also shown is the timing of testing and sampling activities conducted within the HEALS area. The text refers to response survey data of Chen et al. (2007) collected as part of the follow-up urine collection (black).
Figure 2.
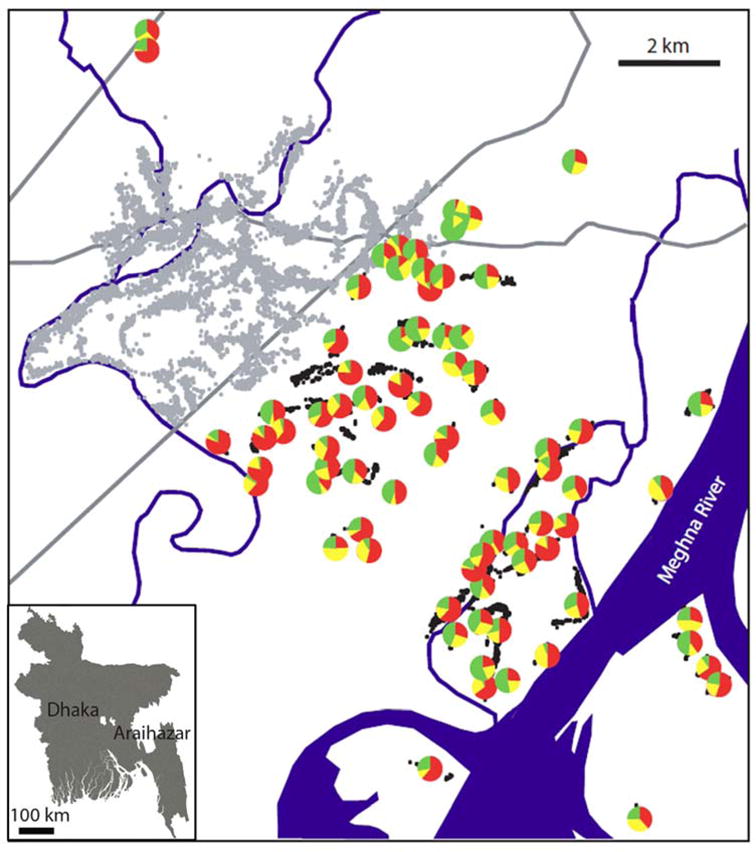
Map of Araihazar upazila showing as pie diagrams the location of the 76 villages surveyed in 2005. Each pie diagram indicates the well status reported by the household: safe (green), unsafe (red), or unknown (yellow). The position of individual wells in the HEALS study area is show as grey dots; the position of wells surveyed under this study as black dots. The HEALS clinic is located at the intersection between the two major roads through the area, which are shown as grey lines. The inset shows the location of Araihazar and the Dhaka metropolitan area in Bangladesh.
Within an adjacent portion of Araihazar upazila (Fig. 2), Columbia University launched HEALS in 2000 by sampling 6,000 wells that were tested in the laboratory (van Geen et al., 2003). This was followed by an education campaign at the village level that relied on skits, songs, and focus-group discussions to encourage households to switch to a low-As well (Madajewicz et al., 2007). Roughly one out of ten households within the HEALS area were also reminded of the risks of exposure to As when baseline urine samples were collected (Fig. 1). Both the education campaign and the baseline urine collection preceded a response survey conducted in 2002–04 within the HEALS area as part of a follow-up of urine collection. BAMWSP testing was paired with a national media campaign and the vast majority of households in the study area were therefore aware of the As issue. This does not mean all households were necessarily correct in their perception of the risks and potential solutions.
Using BAMWSP data, 76 out of a total 300 villages in Araihazar were selected for this study. Selection criteria included a target minimum of 10 wells, in order to exclude very small villages, a minimum of 50% unsafe wells, and a location outside the HEALS area (Fig. 2). A subset of 63 villages meetings these criteria was selected using a random number generator. An additional 13 villages were selected based on their proximity to the HEALS clinic to set the stage for an expansion of the cohort study (Fig. 2). In each village, the field team approached the owners of all wells that they could find and conducted a ~20 min survey by asking the wife of the well-owner, or instead a close female relative, a total of 15 questions. The teams recorded the position of each well (within 5–10 m) using a handheld Global Positioning System (GPS) receiver and recorded whether the red or green paint that had been applied to the pumphead of the well by BAMWSP was still visible. GPS coordinates and survey responses were recorded in the field using ESRI ArcPad 6.02 software. Each respondent was asked to recall her well’s As result as well as whether her household had switched its main source of drinking water between 2003 and 2005. Respondents also were asked about their years of formal education. For all of those households who had switched their drinking water source, the tubewell to which they had switched as their new primary drinking source was linked in the database. Water samples were collected in 2005 from wells whose status was unknown then. Laboratory results were communicated to households as part of a subsequent household survey in a subset of the villages discussed in the present study (Cheng et al., 2007; Balasubramanya et al., 2013).
To the extent this could be ascertained, the position and status of all 4,372 wells across 76 villages was recorded during the survey. The number of wells per village averaged 54 and ranged from 8 to 206. This suggests a population per village ranging from ~100 to ~2000 when applying the average of 11 users per well documented in the adjacent HEALS area (van Geen et al. 2002). To help explain well-switching decisions by households, the linear distance from each unsafe well to the nearest safe well was calculated using ArcView 3.2. In addition, for all households who had switched their drinking source, the linear distances to the wells to which they had switched were calculated. These distances do not reflect the often tortuous paths that villagers have to follow from a home to a well because of the various obstacles present, such as ponds or property boundaries. For analyzing village-level average switching rates, a central village location was calculated by averaging well coordinates for each village, then the distance from each central location to the nearest well sampled within the HEALS area was calculated.
Statistics
Well-switching responses two years after the end of BAMWSP testing are first analyzed at the household level. We use village effects, within linear least-squares regressions, to avoid bias due to differences across villages in factors we do not observe that influence average switching levels for villages. Their inclusion yields a more robust measure, relying on variation within each village, of the impacts of well-As status and, thus, the impacts of well-As testing. The three dependent variables considered in different regressions are: whether a household switched wells at all; whether a household that did switch wells went to a safe well, an untested well or an unsafe well; and how far a household member travels beyond the nearest safe well, if the household switched to a different well. The explanatory variables that were measured at the household level include whether the status of a well was safe, unsafe or unknown, the number of years of formal education of the respondent, and the linear distance to the nearest safe well if the household’s well was unsafe. Aggregations of household responses are subsequently analyzed at the village-level in an attempt to explain variations in the fraction who switched from unsafe wells within each village. For this purpose, the distance of the village to the nearest HEALS well is an additional explanatory variable as a proxy for awareness.
RESULTS
In total 4,356 respondents were interviewed at the 4,372 wells, as the owners of 16 of those wells could not be identified. Of these 4,356 wells, only the 95% that did not have a mechanical problem and therefore functioned at the time of the survey were considered for our analyses. The sample for analyses is further slightly reduced by considering only those 4,109 functioning wells for which household information concerning well status and well usage was recorded.
As previously reported (Ahmed et al., 2006), interviewed households believed that 30% (i.e. 1,252) of their wells were safe while 49% (2,003) were considered unsafe. For the remaining 21% (854) of the wells, owners did not know the status of their well with respect to As (Fig. 3). Paint was no longer visible on 24% of the wells because it had flaked off the rusty pumpheads between 2003 and 2005. However, the perception of well status matched the color of any paint recorded by the enumerator in 98% of cases. As also previously reported, 27% of households who indicated in 2005 that their well had been tested and found to be unsafe in 2003 reported having switched to a different drinking-water source (Ahmed et al., 2006; Balasubramanya et al., 2013). Further analysis of the data reported hereon has not been presented previously.
Figure 3.
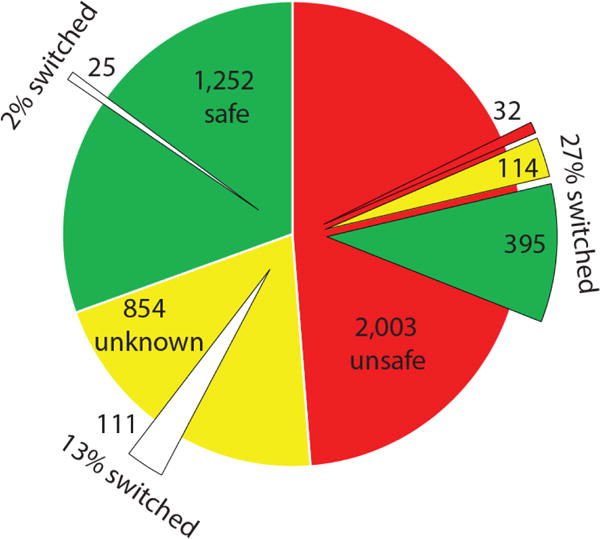
Pie diagrams showing the proportion of wells in the study area whose status reported by the households that own them was unsafe (red), unknown (yellow), and safe (green). The number of wells within each pie is listed. The overlying portions of each pie shows the proportion of households that switched to a well other than their own and whose status they reported. Only in the case of unsafe wells is the perceived status of the wells households switched to known and indicated using the same color coding as above.
Comparison between switching from safe, untested and unsafe wells
The proportion of wells perceived by their owners to be unsafe varied from 0 to 83% across villages. There is no clear geographic pattern to this distribution, with some villages that contained > 75% unsafe wells located within a few kilometers of villages that contained < 25% unsafe wells (Fig. 2). Eighty-five percent of wells of unknown status were installed after the BAMWSP well-testing campaign in Araihazar ended in 2003. The proportion of wells of unknown status within a village also varied widely from 4 to 46% across the study area, again without any clear geographic pattern.
For those households believing their well to be safe, only 2% reported having switched their water source. Compared also to the 27% of households that switched from unsafe wells, an intermediate share of 13% of households reported switching from wells of unknown status (Fig. 3). Regression analysis (not shown) indicates that the differences between these switching rates are significant whether village fixed effects are included or not.
Perceived well status with respect to As was not the only determinant of well switching. The average distance to the nearest safe well in a village decreases with the proportion of safe wells within that village (Fig. 4A). Geography has an impact on switching, as indicated by the relationship between the proportion of switching and the average distance to the nearest safe well (Fig. 4B). Education of the interviewed household member also had an impact on switching. Across all unsafe wells, there was predictable variation in rates of switching as a function of both education and distance to the nearest safe well (Table 1). Years of formal education of the respondents ranged from 0 to 16 years, averaging 4 years, and distance to the nearest safe well varied widely (10–600 m) across the study area, averaging 69 m. A one-standard-deviation increase in years of formal education (4 1/4 years) raised the well-switching rates by 3.5% (in absolute terms, i.e., percent of the group, the convention we use for all percentage results), while a one-standard-deviation increase in the distance to the nearest safe well (82 m) decreased the well-switching rates by 8%.
Figure 4.
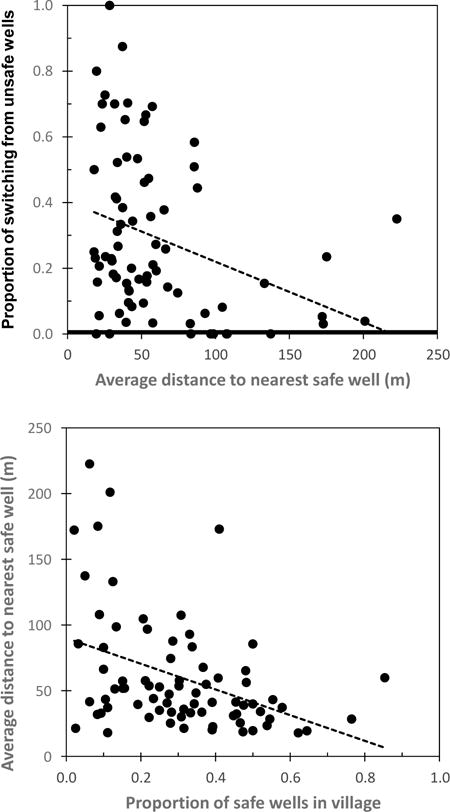
(A) Relationship between the proportion of switching from unsafe wells in a village and the average distance from an unsafe well to a safe well in that village (p<0.05). (B) Relationship between the average distance from an unsafe well to the nearest safe well and the proportion of safe wells in that village (p<0.05).
Table 1.
Results from two household-level regressions and one village-level regression to determine relation between probability of switching, education, distance to the nearest safe well, and distance to the HEALS area.
| Independent variables of household-level regression | Probability of switching from unsafe wells | Independent variables of household-level regression | Probability of switching beyond nearest safe well | Independent variables of village-level regression | Probability of switching from unsafe wells |
|---|---|---|---|---|---|
| Education (year) | 0.008 (p<0.001) | Education (yr) | 0.008 (0.11) | Education (yr) | 0.039 (0.00) |
| Distance to nearest safe well (m) | −0.001 (p<0.001) | Distance to nearest safe well (m) | −0.024 (p<0.001) | Distance to nearest safe well (m) | −0.001 (0.01) |
| Log (distance to HEALS) | −0.058 (0.01) | ||||
| Constant | 0.68 (0.00) | ||||
| n | 2003 | n | 467 | n | 76 |
| Adjusted r2 | 0.22 | Adjusted r2 | 0.11 | Adjusted r2 | 0.28 |
| Village effects included as controls for village differences in factors not observed | Village effects included as controls for village differences in factors not observed | F Statistic Prob > F |
F(3, 72) = 10.7 0.0000 |
Comparison of switching to safe, untested and unsafe wells
The survey data include information about the type of well households switched to when moving away from unsafe wells and, therefore, provide additional information on the impact of testing. Of those 559 households who had switched away from As-unsafe wells, the type and location of the well to which they had switched was recorded for 467 (Fig. 3). The majority of these (73%) switched to safe wells but significant proportions also went to untested (21%) and to unsafe wells (6%).
The location of the wells households switched to suggest that additional factors, including possibly social barriers, may have significantly affected well switching. More than half (63%) of the households who switched from unsafe wells switched to a well that was farther away than the nearest safe well. The additional distance ranged from 4 m to 162 m and averaged 36 m. A regression suggests that the distance to safe water influenced whether any such effective barriers were sufficient to dissuade households from switching to the nearest safe well (Table 1). The probability of switching to a well further than the nearest safe well fell by 24% for an additional 10 m of distance to the nearest safe well. During a subsequent survey conducted in the region, our field staff noted that a considerable number of households reported knowing of nearby safe wells but also that the well owners did not allow them to draw water there. Distance to source, considered here a proxy for access and effort required to switch to a different well, clearly plays a key role in household choices about their water used for drinking and cooking but is not the only consideration. This is consistent with the modest proportion of the variance in household behavior that is explained by the factors that were explicitly considered (Table 1).
The impact of reinforcement
In the household-level analyses, unattributed differences in rates of switching averaged at the village level were removed using village effects in the regressions in order to focus on the differences in behavior between households. In this section, factors measured at the village level are instead considered to examine why the proportions of switching away from unsafe wells range so widely between villages (Fig. 4). Not switching could represent household preferences but also could indicate other constraints including awareness.
One constraint on switching from unsafe wells already inferred from the analysis at the household level is the availability of safe wells. This is proxied here at the village level by the averaged distance between an unsafe well and the nearest safe well. Another potential factor affecting well-switching is information from the HEALS area where awareness has been raised as a result of the cohort study (Chen et al., 2007). Proximity to the HEALS area could plausibly affect a household’s awareness of the health risks from exposure to As outside the immediate area. That proximity is proxied here by using the village’s distance to the nearest well within the HEALS area. In this village-level regression, we use the logarithm of the distance to give more weight to shorter distances given that additional distance is unlikely to matter at large distances. The results show that education, average distance to the nearest safe well, and log distance to the HEALS area all are statistically significant determinants of switching from an unsafe well (Table 1). Similar results are obtained using distance to the nearest HEALS well itself or whether that distance is above or below the median for distances of the study villages.
Our field staff reported that an ‘activist’ individual had put extraordinary effort into raising awareness of the As threat and mobilizing responses. For any regression specification, the activist village clearly stands out as a significant positive outlier in terms of the rate of well switching controlling for other factors. This may indicate that such reinforcement lowered social barriers to switching.
DISCUSSION
The growing number of untested wells
No national or regional blanket testing has been attempted in Bangladesh since 2003 whereas households have continued to install additional wells and replace old wells (Opar et al. 2007). In Araihazar in 2012–2013, the As status of half of the wells was unknown, both because the total number of wells doubled since 2001 and because wells are abandoned at an average rate of 7% per year (van Geen et al., 2014). The proportion of untested wells has grown rapidly not only in Arahaizar. A country-wide survey of over 19,000 households showed that the proportion of untested wells in 35 As-affected upazilas distributed throughout Bangladesh grew by 2009 to an average of 39% (DPHE/JICA, 2009). A more recent blanket survey of over 6,700 households within 26 villages in Singar upazila found that 56% of the wells were untested in 2009–2010 (George et al., 2012).
Opportunities for further reductions in exposure
A new national well-testing campaign has been under discussion in Bangladesh, a decade after the only previous blanket testing campaign ended. Our response data from Araihazar allows us to estimate the potential exposure reductions from renewed testing. We start from average concentrations of 16 and 167 μg/L As, respectively, measured in wells of the adjacent HEALS area classified as safe and unsafe relative to the national standard (van Geen et al., 2003). On this basis, the exposure by drinking from 1,252 safe wells and 2,003 unsafe wells in the present study area before BAMWSP testing averaged 109 μg/L. Sadly, the proportion of safe wells in newly installed wells has been shown to be no higher than in older wells and the average exposure from the remaining 854 wells of unknown status is therefore also 109 μg/L. After switching from unsafe wells according to the proportions recorded in 2005, the average exposure in the area was only lowered to 93 μg/L (for simplicity, this calculation ignores the smaller effects of switching from wells of unknown status and safe wells).
If well testing had continued and the status of all wells had remained known, a similar calculation shows that the average exposure would have declined further to 84 μg/L by eliminating wells of unknown status. Continued testing probably would also have raised awareness and reduced social barriers and could therefore plausibly have doubled the switching rate to that observed in the HEALS, resulting in a further decline to an average of 59 μg/L, a little over half the initial exposure. Given the evidence that social barriers inhibit well switching and sharing, future interventions should place more emphasis on behavior-change techniques that can alter intentions and commitment strength and have proved effective at enhancing well-switching (Munshi and Myaux, 2006; Inauen et al., 2013; Johnston et al., 2014).
Further reductions in exposure that do not require water treatment could be achieved by installing additional deep community wells in affected areas of the country. A spatial calculation based on the distribution of wells in Araihazar has shown that the installation of about 2000 deep community wells could have brought 90% of the population with an unsafe well to live within a 100 m of safe well. However, the siting of these deep community wells would have to be optimized to benefit the overall population (van Geen et al., 2015; Human Rights Watch, 2016). The benefits of such an investment would be substantial in terms of exposure given that deep aquifers in Araihazar average 3 μg/L As (van Geen et al., 2003).
CONCLUSIONS
This survey conducted a few years after the only comprehensive campaign to test wells for As across Bangladesh provides evidence of the impact of this massive intervention. However, only about half as many as households switched away from unsafe wells when compared with a neighboring area where risks of exposure to As were periodically reinforced. The reduction in exposure was also limited by the installation of new wells that have remained largely untested. Lack of testing and reinforcement therefore seriously limit the reduction of exposure that is possible even without installing additional deep community wells.
Acknowledgments
This study was supported in part by NIEHS grant P42 ES010349. We thank the team of Dhaka University students who tirelessly collected the household and well data. We thank Joseph Graziano for his support of the project and comments on the manuscript. This is LDEO contribution number 8086.
References
- Ahmed MF, Ahuja S, Alauddin M, Hug SJ, Lloyd JR, Pfaff A, et al. Ensuring safe drinking water in Bangladesh. Science. 2006;314:1687–8. doi: 10.1126/science.1133146. [DOI] [PubMed] [Google Scholar]
- Ahsan H, Chen Y, Parvez F, Argos M, Hussain I, Momotaj H, et al. Health Effects of Arsenic Longitudinal Study (HEALS): Description of a multidisciplinary epidemiologic investigation. J Exposure Science and Environmental Epidemiology. 2006;16:191–205. doi: 10.1038/sj.jea.7500449. [DOI] [PubMed] [Google Scholar]
- Argos M, Kalra T, Rathouz PJ, Chen Y, Pierce B, Parvez F, et al. A prospective cohort study of arsenic exposure from drinking water and all-cause and chronic disease mortality in Bangladesh. The Lancet. 2010 doi: 10.1016/S0140-6736(10)60481-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Balasubramanya S, Pfaff A, Bennear L, Tarozzi A, Ahmed KM, Schoenfeld A, et al. Evolution of households’ responses to the groundwater arsenic crisis in Bangladesh: information on environmental health risks can have increasing behavioral impact over time. Environment & Development Economics. 2013 doi: 10.1017/S1355770X13000612. [DOI] [PMC free article] [PubMed] [Google Scholar]
- BBS/UNICEF. Bangladesh National Drinking Water Quality Survey of 2009. Dhaka: Bangladesh Bureau of Statistics and UNICEF; 2011. [Google Scholar]
- BGS/DPHE (British Geological Survey, Dept. of Public Health Engineering) Final Report. British Geological Survey; 2001. Arsenic Contamination of Groundwater in Bangladesh. [Google Scholar]
- Bennear L, Tarozzi A, Pfaff A, Balasubramanya S, Ahmed KM, van Geen A. Impacts of a randomized controlled trial in arsenic risk communication on household water supply choices in Bangladesh. Journal of Environmental Economics and Management. 2012;65:225–40. doi: 10.1016/j.jeem.2012.07.006. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cheng Z, Zheng Y, Mortlock R, van Geen A. Rapid multi-element analysis of groundwater by high-resolution inductively coupled plasma mass spectrometry. Analytical and Bioanalytical Chemistry. 2007;379:513–8. doi: 10.1007/s00216-004-2618-x. [DOI] [PubMed] [Google Scholar]
- Chen Y, van Geen A, Graziano J, Pfaff A, Madajewicz M, Parvez F, et al. Reduction in urinary arsenic levels in response to arsenic mitigation in Araihazar, Bangladesh. Environmental Health Perspectives. 2007;115:917–23. doi: 10.1289/ehp.9833. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Chen Y, Graziano JH, Parvez F, Liu M, Slavkovich V, Kalra T, et al. Arsenic exposure from drinking water and cardiovascular disease mortality: A prospective cohort study in Bangladesh. British Medical Journal. 2011;342:d243. doi: 10.1136/bmj.d2431. [DOI] [PMC free article] [PubMed] [Google Scholar]
- DPHE/JICA. Situation analysis of arsenic mitigation. Dhaka, Bangladesh: Department of Public Health Engineering, Government of Bangladesh, and Japan International Cooperation Agency; 2009. [Google Scholar]
- Flanagan SV, Johnston RB, Zheng Y. Arsenic in tube well water in Bangladesh: health and economic impacts and implications for arsenic mitigation. Bulletin of the World Health Organization. 2012;90:839–46. doi: 10.2471/BLT.11.101253. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gelman A, Trevisani M, Lu H, van Geen A. Direct data manipulation for local decision analysis, as applied to the problem of arsenic in drinking water from tube wells in Bangladesh. Risk Analysis. 2004;24:1597–612. doi: 10.1111/j.0272-4332.2004.00553.x. [DOI] [PubMed] [Google Scholar]
- George CM, van Geen A, Slavkovich V, Singha A, Levy D, Islam T, et al. A cluster-based randomized controlled trial promoting community participation in arsenic mitigation efforts in Bangladesh. Environmental Health. 2012;11:41. doi: 10.1186/1476-069X-11-41. [DOI] [PMC free article] [PubMed] [Google Scholar]
- George CM, Graziano JH, Mey JL, van Geen A. Impact on arsenic exposure of a growing proportion of untested wells in Bangladesh. Environmental Health. 2012;11:7. doi: 10.1186/1476-069X-11-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- George CM, Inauen J, Rahman SM, Zheng Y. The effectiveness of educational interventions to enhance the adoption of fee-based arsenic testing in Bangladesh: A cluster randomized controlled trial. Am J Trop Med Hyg. 2013;89:138–44. doi: 10.4269/ajtmh.12-0664. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Human Rights Watch. Nepotism and Neglect: The Failing Response to Arsenic in the Drinking Water of Bangladesh’s Rural Poor. 2016 ( https://www.hrw.org/sites/default/files/report_pdf/bangladesh0416web.pdf)
- Inauen J, Tobias R, Mosler HJ. The role of commitment strength in enhancing safe water consumption: Mediation analysis of a cluster-randomized trial. British Journal of Health Psychology. 2013 doi: 10.1111/bjhp.12068. [DOI] [PubMed] [Google Scholar]
- Johnston R, Hug SJ, Inauen J, Khan NI, Mosler JH, Yang H. Enhancing arsenic mitigation in Bangladesh. Findings from institutional, psychological, and technical investigations. Sci Total Environ. 2014:488–489. doi: 10.1016/j.scitotenv.2013.11.143. [DOI] [PubMed] [Google Scholar]
- Madajewicz M, Pfaff A, van Geen A, Graziano J, Hussein I, Momotaj H, et al. Can information alone both improve awareness and change behavior? Response to arsenic contamination of groundwater in Bangladesh. Journal of Development Economics. 2007;84:731–54. [Google Scholar]
- Miguel E, Kremer M. Worms: identifying impacts on education and health in the presence of treatment externalities. Econometrica. 2004;72:159–217. [Google Scholar]
- Mosler HJ, Blöchliger OR, Inauen J. Personal, social, and situational factors influencing the consumption of drinking water from arsenic-safe deep tubewells in Bangladesh. Journal of Environmental Management. 2010;91:1316–23. doi: 10.1016/j.jenvman.2010.02.012. [DOI] [PubMed] [Google Scholar]
- Munshi K, Myaux J. Social norms and fertility transition. Journal of Development Economics. 2006;80:1–38. [Google Scholar]
- Opar A, Pfaff A, Seddique AA, Ahmed KM, Graziano JH, van Geen A. Responses of 6500 households to arsenic mitigation in Araihazar, Bangladesh. Health & Place. 2007;13:164–72. doi: 10.1016/j.healthplace.2005.11.004. [DOI] [PubMed] [Google Scholar]
- Pitt MM, Rosenzweig MR, Hassan N. (NBER Working Paper No. 21741).Identifying the cost of a public health success: Arsenic well water contamination and productivity in Bangladesh. 2015 [Google Scholar]
- Ravenscroft P, Kabir A, Hakim SAI, Ibrahim AKM, Ghosh SK, Rahman MS, Akter F, Sattar MA. Effectiveness of public rural waterpoints in Bangladesh with special reference to arsenic mitigation. Journal of Water, Sanitation and Hygiene for Development. 2014 doi: 10.2166/washdev.2014.038. [DOI] [Google Scholar]
- Smith A, Lingas E, Rahman M. Contamination of drinking-water by arsenic in Bangladesh: a public health emergency. Bulletin of the World Health Organization. 2000;78:1093–103. [PMC free article] [PubMed] [Google Scholar]
- Sohel N, Persson LA, Rahman M, Streatfield PK, Yunus M, Ekström EC, Vahter M. Arsenic in drinking water and adult mortality: a population-based cohort study in rural Bangladesh. Epidemiology. 2009;20:824–30. doi: 10.1097/EDE.0b013e3181bb56ec. [DOI] [PubMed] [Google Scholar]
- van Geen A, Ahmed KM, Seddique AA, Shamsudduha M. Community wells to mitigate the current arsenic crisis in Bangladesh. Bull World Health Organ. 2003;82:632–8. [PMC free article] [PubMed] [Google Scholar]
- van Geen A, Cheng Z, Jia Q, Seddique AA, Rahman MW, Rahman MM, et al. Monitoring 51 deep community wells in Araihazar, Bangladesh, for up to 5 years: Implications for arsenic mitigation. Journal of Environmental Science and Health Part A. 2007;42:1729–40. doi: 10.1080/10934520701564236. [DOI] [PubMed] [Google Scholar]
- van Geen A, Ahsan H, Horneman AH, Dhar RK, Zheng Y, Hussain I, et al. Promotion of well-switching to mitigate the current arsenic crisis in Bangladesh. Bull World Health Organ. 2002;81:732–7. [PMC free article] [PubMed] [Google Scholar]
- van Geen A, Ahmed EB, Pitcher L, Mey JL, Ahsan H, Graziano JH, et al. Comparison of two blanket surveys of arsenic in tubewells conducted 12 years apart in a 25 km2 area of Bangladesh. Science of the Total Environment. 2014:488–9. 484–92. doi: 10.1016/j.scitotenv.2013.12.049. [DOI] [PMC free article] [PubMed] [Google Scholar]
- van Geen A, Cheng Z, Seddique AA, Hoque MA, Gelman A, Graziano JH, Ahsan H, Parvez F, Ahmed KM. Reliability of a commercial kit to test groundwater for arsenic in Bangladesh. Environmental Science and Technology. 2005;39:299–303. [PubMed] [Google Scholar]
- van Geen A, Zheng Y, Versteeg R, Stute M, Horneman A, Dhar R, et al. Spatial variability of arsenic in 6000 tube wells in a 25 km2 area of Bangladesh. Water Resources Research. 2003;39:1140. doi: 10.1029/2002WR001617. [DOI] [Google Scholar]
- van Geen A, Singh CK. Piloting a novel delivery mechanism of a critical public health service in India: arsenic testing of tubewell water in the field for a fee. 2013. (IGC Policy Note 13/0238). [Google Scholar]
- WASH. WASH programme of BRAC: Towards attaining the MDG targets: Baseline findings. BRAC; Dhaka, Bangladesh: 2008. [Google Scholar]
- World Health Organization. Guidelines for drinking-water quality. fourth. 2011. [Google Scholar]
- Wasserman GA, Liu X, Parvez F, Ahsan H, Factor-Litvak P, van Geen A, et al. Water arsenic exposure and children’s intellectual function in Araihazar, Bangladesh. Environmental Health Perspectives. 2004;112:1329–33. doi: 10.1289/ehp.6964. [DOI] [PMC free article] [PubMed] [Google Scholar]