

Supplemental Digital Content is available in the text
Keywords: collaborative practice, health care, interprofessional education, interprofessional learning, medical education
Abstract
Background:
The World Health Organization (WHO) and its partners identify interprofessional (IP) collaboration in education and practice as an innovative strategy that plays an important role in mitigating the global health workforce crisis. Evidence on the practice of global health level in interprofessional education (IPE) is scarce and hampered due to the absence of aggregate information. Therefore, this systematic review was conducted to examine the incidences of IPE and summarize the main features about the IPE programs in undergraduate and postgraduate education in developed and developing countries.
Methods:
The PubMed, Embase, Web of Science, and Google Scholar were searched from their inception to January 31, 2016 for relevant studies regarding the development of IPE worldwide, IPE undergraduate and postgraduate programs, IP interaction in health education, IPE content, clinical placements, and teaching methods. Countries in which a study was conducted were classified as developed and developing countries according to the definition by the United Nations (UN) in 2014.
Results:
A total of 65 studies from 41 countries met our inclusion criteria, including 45 studies from 25 developed countries and 20 studies from 16 developing countries. Compared with developing countries, developed countries had more IPE initiatives. IPE programs were mostly at the undergraduate level. Overall, the university was the most common academic institution that provided IPE programs. The contents of the curricula were mainly designed to provide IP knowledge, skills, and values that aimed at developing IP competencies. IPE clinical placements were typically based in hospitals, community settings, or both. The didactic and interactive teaching methods varied significantly within and across universities where they conducted IPE programs. Among all health care disciplines, nursing was the discipline that conducted most of the IPE programs.
Conclusion:
This systematic review illustrated that the IPE programs vary substantially across countries. Many countries, especially the academic institutions are benefiting from the implementation of IPE programs. There is a need to strengthen health education policies at global level aiming at initiating IPE programs in relevant institutions.
1. Introduction
Internationally, the health care system is under increasing pressure due to rising global health issues and needs,[1,2] increased health care costs,[3] shortages in the health care-related workforce,[4] and inadequate understanding and respect for the contributions of health professionals.[5] Interprofessional education (IPE) and interprofessional collaborative practice (IPCP) can play a significant role in mitigating the challenges faced by global health systems. According to the WHO, “interprofessional education (IPE) mainly occurs when two or more professions learn from each other to improve health outcomes,” and “IPCP occurs when a number of health workers from different professional backgrounds work with patients, their families, caregivers and communities to provide comprehensive service and deliver the highest practicable quality of care.”[1] Barr et al and Kitto et al exemplified that IPE was an educational activity designed and implemented around the world to enhance attitudes, knowledge, skills and behaviors for collaborative practice.[6,7]
As challenges of improving health care quality in the 21st century continue to be identified, a collaborative team in health care is essential for the improvement of health outcomes. Studies of IPE have indicated that health professionals have worked together in teams to manage complex practice situations that require systematic and informed collaboration between different professions and professional specialties in recent years.[1,2,8] Furthermore, research has also shown that collaborative practice can improve the access and the coordination of health services, resources, and outcomes for people with chronic diseases while also decreasing patients’ complications, tension, conflicts with caregivers, hospital readmission, clinical error rates, and staff turnover.[1,4,5] The current health workforce is a critical element in strengthening health care systems and expanding universal health coverage: IPE has been initiated by the WHO[1] to improve the health care workers’ ability to provide high-quality care.
In the last 15 years many studies have focused exclusively on IPE and IPCP by country. In most of these, the nature and scope of exposure has been on IPE and the implementation is targeting the interaction between medicine, nursing, or multiple health science disciplines and social work. Many advantages of IPE have been identified in previous studies. For example Best Evidence in Medical Education (BEME) reported that IPE has been well implemented and practiced in quality improvement initiatives. It promotes knowledge and skills that are essential in service delivery and facilitates collaboration.[8] However, there are several unique barriers encountered by educators and practitioners during the implementation of IPE programs.[9–11] Therefore, evidence of common structured curricula, disciplines, and practice models effects on standardization of global IPE programs will be a key to the development of effective health education policies. This review of published evidence aimed to assess the practice of IPE and summarized data about the IPE programs in undergraduate and postgraduate level of education in developed and developing countries.
2. Methods
2.1. Search strategy and selection criteria
A systematic review was conducted using the 2009 PRISMA guidelines.[12] A search strategy was designed to identify publications which described IPE initiatives. Relevant publications in English were electronically searched in 4 databases: PubMed, Embase, Web of Science, and Google Scholar from their inception through January 31, 2016. The following keywords were used to collect relevant citations: (“global interprofessional education” OR “interprofessional education initiatives”) AND (“undergraduate programs” OR “postgraduate programs”). We also scrutinized the published studies from the (UK) Centre for the Advancement of Interprofessional Education (CAIPE), the Japan Association for Interprofessional Education (JAIPE), the European Interprofessional Practice and Education Network (EIPEN), the Canadian Interprofessional Health Collaborative (CIHC), and the Australasian Interprofessional Education and Practice Network (AIPPEN).
Studies were included if they investigated IPE implementation. The following were inclusion criteria for this review: studies aimed to explore the IPE programs globally, including universities or institutions; studies focused on IPE programs at undergraduate and/or postgraduate levels; studies that reported the disciplines of IPE and core contents included in IPE modules in health education curricula; and studies that reported the teaching and learning methods on IPE.
Studies were excluded if they did not meet the aim and objective of this systematic review. Letters and commentaries were also excluded. This systematic review was based on published literature, and no data were collected on animals. Therefore, there was no need to submit to the ethics committee.
2.2. Data extraction and analysis
The included articles were assessed for relevance and content. This was conducted by 2 investigators (CH and YZ) who reviewed all identified articles independently. Disagreements between investigators were resolved by consensus with a third investigator (ZL). Extracted data included the reported evidence on the academic institution in which IPE was initiated or evaluated, undergraduate and postgraduate program, interdisciplinary interaction for IPE, core content included in IPE module in curricula, teaching methods, and clinical placements. To accumulate the country-specific evidence of IPE program, countries were divided into 2 categories of developed and developing countries according to the classification of the United Nation (UN) in 2014.[11] The assessment of IPE programs concerns students who received IPE at undergraduate and postgraduate levels. For comparison, the background of IPE in developed and developing countries incorporated all the aforementioned factors together.
The data analysis consisted of 3 main steps: selecting the countries that conducted undergraduate and/or postgraduate level IPE programs; examining the academic institution and departments which conducted IPE programs; exploring the IPE contents including curricula, teaching and learning methods, and conditions of clinical placements for particular IPE programs.
If academic institutions had more than 1 study available on IPE programs, we used a quality assessment tool to select studies that were of the best quality. The quality assessment decision to identify which studies to include in the final analysis was according to the following hierarchical order: studies that reported information about IPE initiatives at undergraduate and or postgraduate level; studies with complete information about overall IPE programs, curricula, content, clinical placements, and teaching methods; and studies focused on IPE initiatives only, not considering IPCP programs. To allow comparisons across studies, we used all data that was available since 1999 to identify the nature of IPE programs. Data extracted from the included studies were qualitatively summarized, and no statistical analysis conducted.
3. Results
Initially, 870 articles were identified from the databases of which 108 articles were identified as having potentially relevant abstracts. After retrieving the full-text review for detailed evaluation, 65 studies from 41 countries met our inclusion criteria and were included in the review (Fig. 1).[13–79] Forty-five studies (Supplementary Table S1) came from 25 developed countries which reported IPE programs.[13–58] Supplementary Table S2, summarized the 20[59–79] studies that conducted the IPE program in 16 developing countries, and mostly from West and East Asia. Few studies were available from Africa, and the Latin America and Caribbean region. Compared with developing countries, developed countries had a rapid development of IPE programs and initiatives. Findings illustrated that developed countries had capacities to expand IPE further than developing countries, which needed more direction to improve IPE programs. This indicates that IPE initiatives vary across the world with different pattern in nature of the program.
Figure 1.
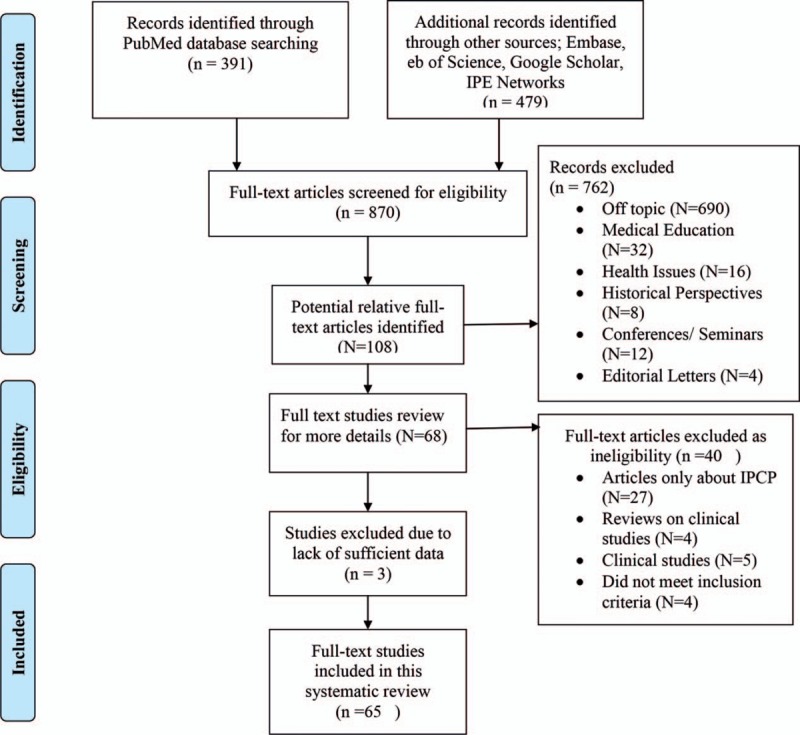
Study selection process.
The Supplementary Table S1, and Table S2, summarized the academic institutions that conduct IPE, interdisciplinary interaction in IPE, core contents included in IPE modules in health education curricula, teaching and learning methods, and clinical placements of IPE programs. Based on all of the studies that we reviewed, we found that the university is the most common academic institution in IPE programs, except 1 IPE program which is conducted by the National Center for Global Health and Medicine in Japan.[58] However, the global movement of IPE initiatives and programs are unique for each university in developed and developing countries. As early as 1960, universities in Canada, the United States, the United Kingdom (UK), and Australia initiated IPE programs, whereas most universities in developing countries introduced IPE programs more recently.
Most of the IPE programs were at the undergraduate level in both developed and developing countries. Methodological differences existed in teaching, curricula, and placements between undergraduate- and postgraduate-level IPE programs. Seventeen studies reported postgraduate level IPE programs on children palliative care,[38] dental care,[32,45,47] social work,[26,54] and gerontology.[36,64] Undergraduate-level IPE programs emphasized the interdisciplinary collaboration, professionals in health care and team work,[18] dental care,[33,36] crisis management,[70] palliative oncology care,[19] ethics and professionalism training,[60] and psychosocial oncology practice and research.[19] Undergraduate-level IPE programs were the basic academic programs which were designed to provide IPE and IPCP training. Most of the IPE programs were conducted as workshops and training within the health care education curricula. However, at Hong Kong Polytechnic University they were designed to conduct IPE programs as seminar basis for undergraduate nursing and social work students.[72] Both undergraduate- and postgraduate-level IPE educational programs were designed to provide interprofessional (IP) knowledge, skills, and values which aimed at developing IP competencies.
Several articles described the multiple disciplines and departments that conducted IPE programs. The findings showed that among all health science disciplines, nursing was the discipline that conducted the most IPE programs.[23,29,71,76] Apart from that, medicine, pharmacy, and dentistry were the top 3 departments which frequently established IPE programs.[15,33,36,51,56,59] Midwifery, physiotherapy, occupational therapy, and other health sciences incorporated IPE programs, but IPE-specific initiatives implemented by these departments were not found. In addition to the health disciplines, social science departments also established and implemented IPE programs. For example, IPE initiatives were reported in departments of social work in a few universities in Canada, the United States, the UK and Australia.[17,27,34,54] The findings showed that interdisciplinary interaction has been increased gradually in the development and implementation of IPE projects.
The core content of IPE modules in health education curricula is included in Supplementary Table S3. The central components of curricula and the contents of IPE modules were mainly based on the structure of knowledge, skills, and values. In addition, IPE occurred largely in 3 formats: theory-based curricula, clinical curricula, and a combination of theory- and clinical-based curricula.[21,52,57,61] For example curricula for team-based oncology palliative care education was identified in 1 study as the framework for teaching students IP practice skills.[19] In most universities, the content of IPE modules in health education curricula was more focused on skill based than value based. Curricula content on dealing with IP conflicts were identified in a few studies.[20,21,41] Gaps in the content of IPE curricula, lack of common competency framework for curriculum development, and benchmarks for academic standards were also identified.
IP clinical placements were typically based in hospitals, communities, or a combination of the 2 places. The profession-specific clinical practice was reported in 1 study[32] and an unstructured IP clinical practice in the curricula was identified across the IPE programs. A few studies showed that evidence-based clinical practice took place in the department of social work IPE initiatives.[27,53,54] Additionally, findings of this review showed that an integral part of professional education and training is that field practice should be concerned in upgrading the curricula component of IPE placements based on micro and macro levels of practice.
The didactic and interactive teaching methods employed in the IPE programs varied greatly across universities. Traditional teaching methods including problem based, case based, and team based were common among IPE programs. According to the evidence, 2 universities in the United States[19,26,27] used the aforementioned 3 methods together, and 3 universities in Canada, the United States, and Philippines[16,27,68] used case-based and problem-based approaches together. Other studies used 1 single method, or used it in combination with other nontraditional teaching methods. For example, simulation-based education was used in some universities[24,40,76] as a powerful and evidence-based teaching method. Conversely, work-based learning and competency-based teaching methods got more attention to develop the IPCP competencies.[33,59] A shared-learning approach had been employed in IPE, particularly in some European countries and China.[32,38,75] The effectiveness of teaching and outcomes depended on the educational formats, standards of teaching methods, and selection of appropriate methods.
4. Discussion
The findings from this systematic review showed that IPE initiatives were prevalent in Canada, the United States, the United Kingdom, Australia, and European countries. In contrast, slight improvements in IPE programs were seen in the developing regions. Additionally, IPE courses were typically short and varied in nature. IP placements were not systematically delivered: students’ engagement mainly occurred at the undergraduate level. The scheduled evaluation of IPE impact on health outcomes and service delivery were rare, and internationally preparing teaching staff to deliver IPE was uncommon. In total, findings showed that many countries and academic institutions benefited by introducing collaborative teaching, learning, and practice methods from the implementation of IPE programs.
Previous studies reported that collaborative practices were needed to face the world's most urgent health challenges, overcome the health actions in crisis, enhance the region's capacity to respond to the health security issues, provide a comprehensive approach to prevent and manage the chronic conditions, and improve the strengths and skills of health workers.[13,29,63,79] One advantage of establishing IPE and IPCP is that it could positively contribute to urgent health challenges. For example, a paradigm shift in the epidemiological transition in low and middle-income countries necessitates a number of health workers from various disciplines to work together to address the pertinent global health challenges, especially in Africa, where the shortage and inequality of health care resources is common.[1]
As the WHO stated, patient and population’ outcomes could be improved through multidisciplinary and collaborative care.[1] Joining value-based contents into the curricula might also play an important role. Our study indicated that the health educators typically considered values and ethics as contents that is an element of professionalism, which had significant overlap with constructs of humanism and morality. This has been shown across all countries and institutions where the studies have been conducted, these values and ethics components were patient-centered with a community/population orientation, grounded in a sense of sharing purpose to support the quality in health care, and reflected a shared commitment to establish safer, more efficient, and effective systems of care.
IPE programs might be difficult to implement for a number of reasons, such as the length of professional education, limited hospital resources, the faculty availability and teaching loads, and the power and leadership of institution and/or government. Based on the findings from current studies, some important aspects about successful implementation of IPE programs were identified.[18,34,46,51,52,70]
First, governments, institutions, or hospitals needed to perform an assessment before implementation. It is worth mentioning that all institutions had to make a precise assessment plan to provide necessary evidence about how IPE was to be initiated, how curricula were revised, and how health education programs were redesigned. In addition to recognizing, leveraging, and acting on IPE opportunities, collaborating with existing organizations that have similar goals will greatly enhance the efficiency, minimize the redundancy in work, and allow all entities to share in the impact of IPE programs. Second, education efforts were required to align with practice requirements as health delivery rapidly moves toward more integrated models. Therefore educational leaders must be more responsive to practice needs in the pace of preparation, means of assessing effectiveness, and methods of educational research. Third, the expansion of infrastructure, training initiatives, faculty leadership, and capacity development are essential. The successful implementation of IPE requires leadership at all levels, both in academic and practice settings. Fourth, the curriculum for health care professionals was primarily dictated by the demands of the specific disciplines and detailed curricula. However promoting curriculum innovation, developing IP competency, and increasing interdisciplinary practice need to be in harmony with educational modules and ensure the alignment of team collaboration and practice models. Fifth, accreditation requirements and academic institutions were required to include IPE as a standard part of their curricula. Lack of accreditation was an obstacle to conduct IPE programs, which made courses and teaching less standardized in academic programs and practice in IPE. Finally, for coordinating IPE programs to gain widespread support, establishing an IP team to co-create cases and evaluate plans to ensure the relevancy and authenticity was essential.
Inevitably, there were several obstacles in achieving a successful implementation of IPE programs. In earlier studies, the barriers were encountered in planning, initiating, and implementing IPE in various locations.[16,40,44] The 4 types of barriers that influenced the implementation of IPE in Germany were classified as systemic, behavioral, attitudinal, and methodological barriers.[10] Additionally, a review summarized 10 challenges or barriers including curriculum, leadership, resources, stereotypes, and attitudes, a diversity of students, IPE concept, teaching, enthusiasm, professional jargons, and accreditation.[9] Barriers reported in other studies were lack of institutional leadership and geographical proximity of the different disciplinary institutions, variability in the academic calendar, faculty attitudes, lockstep curricular patterns, inconsistency of professional program entry, limited financial funding, problems of scheduling, and lack of administrative support.[52,61] For example, the Makerere University College of Health Sciences in Uganda exemplified that the training curriculum, the issue of role models and leaders, good planning, and training of implementers, as well as commitment from all stakeholders were main barriers.[60] Furthermore, other studies also indicated that gender segregation due to cultural issues, lacking partners students, lack of faculty designation, dedicated personnel, and lack of professional accreditation and professional development of IPE educators were barriers.[66,68] Being aware of these challenges and barriers in advance, those institutions who seek to plan and implement IPE programs elsewhere will be much more prepared and their efforts may proceed more smoothly and successfully.
In this review, we noted that IPE had concentrated on 4 professionals: nursing, medicine, pharmacy, and dentistry. IPE programs reported in the studies tended to focus on the activities at an undergraduate level, postgraduate level, or both. Clinical placements were typically based in hospital, community, or both. Very little literature reported on how to coordinate the various departments, disciplines, distributions, and clinical placements to achieve sustainable outcomes, or how to transform the teaching methods and core contents to strengthen the connection between education systems and health systems in the process of IPE implementation. The strong internationally designed IPE framework and need for planning a practice platform to achieve sustainable outcomes should become the priority in further research. An international research agenda should be set by experts to investigate the reasonable use of resources, new health care financial strategies, and the attitudes toward IPE. Ideally, follow-up research should be essential to explore the attitudes, cultural spaces, and practice of health care. Simultaneously, the international health academia, policy experts, and health care delivery organizations in conjunctions with national governments should create policy solutions for IPE and IPCP aiming to achieve standardized IPE programs globally.
The strength of our study is that it is the first review to systematically summarize the evidence on worldwide IPE in undergraduate and postgraduate education. The results of our study provide valuable insight for related researchers regarding the necessity of IPE in medical education. Notably, the assessment of the effectiveness of IPE's was also an important aspect. This study also had limitations. First, the limited information provided in the included original studies precluded the possibility of the effective assessment of IPE programs across different countries, institutions, programs, teaching methods, and clinical placements. Second, some studies did not provide information about the IPE implementation mechanisms and enabling factors. As such the analysis did not provide the most conservative implications for IPE initiatives. Despite these limitations, our results focused on conservative implications on IPE initiatives: our findings underscore the direction to design IPE programs, especially in developing countries.
5. Conclusion
In conclusion, our systematic review illustrated that the IPE programs varied substantially across different countries. Worldwide IPE initiatives have progressively developed mainly in developed countries, but not sufficient enough to meet global health targets for establishing IPCP. IPE initiatives are popularly conducted at the undergraduate level, while a smaller number of initiatives were seen at the postgraduate level. Universities should further expand the scope of IPE programs and coordinate the IPE programs at each stage. The results of this review emphasize the need to better elucidate health education policy, implement policies to reduce the inequities in IPE initiatives, and improve the quality and quantity of IPE programs to seek the global health equality. More studies aimed to assess the effects of IPE programs on different institutions, different types of program, different clinical placements, and different teaching methods are warranted.
Supplementary Material
Footnotes
Abbreviations: IP = interprofessional, IPCP = interprofessional collaborative practice, IPE = interprofessional education, IPL = interprofessional learning, UN = United Nations, WHO = World Health Organization.
CH, YZ, and YG contributed equally to this work. CH and ZL initiated the report. CH and ZL wrote the review protocol. CH, YZ, and YG did the initial search and collection of articles. CH and YZ independently reviewed articles and determined included articles. CH, YZ, YG, NN, and YG wrote the first and final versions. All authors independently reviewed and approved the final manuscript. ZL is the guarantor of this work and had full access to all the data in the study, and takes responsibility for its integrity and the accuracy of the data analysis.
The Fundamental Research Funds for the Central Universities (2016YXMS215), Huazhong University of Science and Technology, China supported this study.
The authors declare that they have no conflicts of interest.
Supplemental Digital Content is available for this article.
References
- [1].Framework for Action on Interprofessional Education & Collaborative Practice. Health Professions Networks Nursing & Midwifery Human Resources for Health, World Health Organization; 2010. [Google Scholar]
- [2].Thistlewaite J. Interprofessional education: a review of context, learning and the research agenda. Med Educ 2012;46:58–70. [DOI] [PubMed] [Google Scholar]
- [3].Lee B, Celetti F, Makino T, et al. Attitudes of medical schools deans toward interprofessional education in western pacific region countries. J Interprof Care 2012;26:479–83. [DOI] [PubMed] [Google Scholar]
- [4].Patricia A, Interprofessional Education for Collaboration, Institute of Medicine, 2013. [Google Scholar]
- [5].Greiner A, Knebel E, eds. Health Professions Education: A Bridge to Quality. National Research Council; 2003;2–3. [PubMed] [Google Scholar]
- [6].Barr H, Koppel I, Reeves S, et al. Effective Interprofessional Education: Assumption, Argument and Evidence. London: Blackwell; 2005. [Google Scholar]
- [7].Kitto S, Chesters J, Thistlethwaite J, Reeves S. Nova Science Publishers, A Sociology of Interprofessional Healthcare Practice: Critical Reflections and Concrete Solutions. Hauppauge, NY:2011. [Google Scholar]
- [8].Hammick M, Freeth D, Koppel I, et al. A best evidence systematic review of interprofessional education: BEME Guide no. 9. Med Teach 2007;29:735–51. [DOI] [PubMed] [Google Scholar]
- [9].Sunguya BF, Hinthong W, Jimba M, et al. Interprofessional education for whom? Challenges and lessons learned from its implementation in developed countries and their application to developing countries: a systematic review. PloS One 2014;9:e96724. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [10].Altin SV, Tebest R, Kautz-Freimuth S, et al. Barriers in the implementation of interprofessional continuing education programs—a qualitative study from Germany. BMC Med Educ 2014;14:227. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [11].Country Classification, United Nations 2015. World Economic Situation and Prospects; 2014. [Google Scholar]
- [12].Moher D, Liberati A, Tetzlaff J, et al. The PRISMA Group preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. PLoS Med 2009;6:e1000097. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [13].Gilbert JH. Interprofessional education for collaborative, patient-centred practice. Nurs Leadersh 2005;18:32–8. [DOI] [PubMed] [Google Scholar]
- [14].Hunter JP, Stinson J, Campbell F, et al. A novel pain interprofessional education strategy for trainees: assessing impact on interprofessional competencies and pediatric pain knowledge. Pain Res Manag 2015;20:e12–20. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [15].Cameron A, Ignjatovic M, Langlois S, et al. An interprofessional education session for first-year health science students. Am J Pharm Educ 2009;73:62. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [16].Fernandes AR, Palombella A, Salfi J, et al. Dissecting through barriers: a mixed-methods study on the effect of interprofessional education in a dissection course with healthcare professional students. Anat Sci Educ 2015;8:305–16. [DOI] [PubMed] [Google Scholar]
- [17].Rotz EM, Dueñas GG, Grove AB, et al. Exploring first-year pharmacy and medical students’ experiences during a longitudinal interprofessional education program. Pharm Teach Learn 2015;7:302–11. [Google Scholar]
- [18].Bridges DR, Davidson RA, Odegard PS, et al. Interprofessional collaboration: three best practice models of interprofessional education. Med Educ Online 2011;16:6035. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [19].Hermann CP, Head BA, Black K, et al. Preparing nursing students for interprofessional practice: the interdisciplinary curriculum for oncology palliative care education. J Prof Nurs 2016;32:62–71. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [20].Russell KM, Hymans D. Interprofessional education for undergraduate students. Public Health Nurs 1999;16:254–62. [DOI] [PubMed] [Google Scholar]
- [21].Vanderwielen LM, Vanderbilt AA, Dumke EK, et al. Improving public health through student-led interprofessional extracurricular education and collaboration: a conceptual framework. J Multidiscip Healthc 2014;7:105–10. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [22].Poirier T, Wilhelm M. An interprofessional faculty seminar focused on interprofessional education. Am J Pharma Educ 2014;78:80. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [23].Aston SJ, Rheault W, Arenson C, et al. Interprofessional education: a review and analysis of programs from three academic health centers. Acad Med 2012;87:949–55. [DOI] [PubMed] [Google Scholar]
- [24].Miller JL, Rambeck JH, Snyder A. Improving emergency preparedness system readiness through simulation and interprofessional education. Public Health Rep 2014;129:129–35. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [25].Lehrer MD, Murray S, Benzar R, et al. Peer-led problem-based learning in interprofessional education of health professions students. Med Educ Online 2015;20:28851. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [26].Iachini AL, Warren ME, Splett JW, et al. Exploring the impact of a pre-service interprofessional educational intervention for school mental health trainees. J Interprof Care 2015;29:162–4. [DOI] [PubMed] [Google Scholar]
- [27].Phillips JB. Social work and interprofessional education in health care: a call for continued leadership. J Soc Work Educ 2016;52:18–29. [Google Scholar]
- [28].Davis BP, Clevenger CK, Posnock S, et al. Teaching the teachers: faculty development in inter-professional education. Appl Nurs Res 2015;28:31–5. [DOI] [PubMed] [Google Scholar]
- [29].Pilon BA, Ketel C, Davidson HA, et al. Evidence-guided integration of interprofessional collaborative practice into nurse managed health centers. J Prof Nurs 2015;31:340–50. [DOI] [PubMed] [Google Scholar]
- [30].Barr H. Review of interprofessional education in the United Kingdom. Centre for the Advancement of Interprofessional Education; 2014. [Google Scholar]
- [31].Barr H, Ross F. Mainstreaming interprofessional education in the United Kingdom: a position paper. J Interprof Care 2006;20:96–104. [DOI] [PubMed] [Google Scholar]
- [32].Colonio Salazar FB, Andiappan M, Radford DR, et al. Attitudes of the first cohort of student groups trained together at the University of Portsmouth Dental Academy towards dental interprofessional education. Eur J Dent Educ 2016;21:91–100. [DOI] [PubMed] [Google Scholar]
- [33].Evans J, Henderson AJ, Sun J, et al. The value of inter-professional education: a comparative study of dental technology students’ perceptions across four countries. Br Dent J 2015;218:481–7. [DOI] [PubMed] [Google Scholar]
- [34].Dunworth M. Joint assessment in inter-professional education: a consideration of some of the difficulties. Soc Work Educ 2007;26:414–22. [Google Scholar]
- [35].Walkenhorst U, Mahler C, Aistleithner R, et al. Position statement GMA Committee: “Interprofessional Education for the Health Care Professions”. GMS Zeitschrift fur Medizinische Ausbildung 2015;32:1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [36].Barr H. The Genesis of a Global Movement. Centre for the Advancement of Interprofessional Education; 2015. [Google Scholar]
- [37].Graham I. Issues, and the questions they inspire, when one considers the development of European higher education for health care professionals. J Allied Health 2008;37:e124–39. [PubMed] [Google Scholar]
- [38].Nicholl H, Price J, Tracey C. An evaluation of an interprofessional master's level programme in children's palliative care: the students’ evaluation. Nurse Educ Pract 2016;17:60–6. [DOI] [PubMed] [Google Scholar]
- [39].Hernandez-Marrero P, Pereira SM, Carvalho AS. Ethical decisions in palliative care: interprofessional relations as a burnout protective factor? Results from a Mixed-Methods Multicenter Study in Portugal. Am J Hosp Palliat Care 2015;33:723–32. [DOI] [PubMed] [Google Scholar]
- [40].Vermeulen J, Beeckman K, De Clercq G, et al. Inter-professional Perinatal Simulation training: a valuable educational model to improve competencies amongst student midwives in Brussels, Belgium. Midwifery 2016;33:49–51. [DOI] [PubMed] [Google Scholar]
- [41].Tsakitzidis G, Timmermans O, Callewaert N, et al. Participant evaluation of an education module on interprofessional collaboration for students in healthcare studies. BMC Med Educ 2015;15:188. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [42].Ko J, Bailey-Kloch M, Kim K. Interprofessional experiences and attitudes toward interprofessional health care teams among health sciences students. Soc Work Health Care 2014;53:552–67. [DOI] [PubMed] [Google Scholar]
- [43].Jakobsen F, Larsen K, Hansen TB. This is the closest I have come to being compared to a doctor: views of medical students on clinical clerkship in an Interprofessional Training Unit. Med Teach 2010;32:e399–406. [DOI] [PubMed] [Google Scholar]
- [44].Johnsen H. Learning to create new solutions together: a focus group study exploring interprofessional innovation in midwifery education. Nurse Educ Pract 2016;16:298–304. [DOI] [PubMed] [Google Scholar]
- [45].Larivaara P, Taanila A. Towards interprofessional family-oriented teamwork in primary services: the evaluation of an education programme. J Interprof Care 2004;18:153–63. [DOI] [PubMed] [Google Scholar]
- [46].Dahlberg J, Falk AL, Kjellgren K, et al. Creating a common curriculum for interprofessional learning: Strategic Development of Undergraduate program in Medicine and Health, CAIPE 2014. [Google Scholar]
- [47].Liaskos J, Frigas A, Antypas K, et al. Promoting interprofessional education in health sector within the European Interprofessional Education Network. Int J Med Inform 2009;78:S43–7. [DOI] [PubMed] [Google Scholar]
- [48].Stalmeijer RE, Dolmans DH, Wolfhagen IH, et al. The development of an instrument for evaluating clinical teachers: involving stakeholders to determine content validity. Med Teach 2008;30:e272–7. [DOI] [PubMed] [Google Scholar]
- [49].Oeseburg B, Hilberts R, Luten TA, et al. Interprofessional education in primary care for the elderly: a pilot study. BMC Med Educ 2013;13:161. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [50].Pahor M, Rasmussen BH. How does culture show? A case study of an international and interprofessional course in palliative care. J Interprof Care 2009;23:474–85. [DOI] [PubMed] [Google Scholar]
- [51].Zanotti R, Sartor G, Canova C. Effectiveness of interprofessional education by on-field training for medical students, with a pre-post design. BMC Med Educ 2015;15:121. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [52].Pumar Mendez MJ, Armayor NC, Diaz Navarlaz MT, et al. The potential advantages and disadvantages of introducing interprofessional education into the healthcare curricula in Spain. Nurse Educ Today 2008;28:327–36. [DOI] [PubMed] [Google Scholar]
- [53].Nicol P. Interprofessional Education for Health Professionals in Western Australia: Perspectives and Activity. University of Technology, Sydney; 2015. [Google Scholar]
- [54].Pockett R. Interprofessional education for practice: some implications for Australian social work. Aust Soc Work 2010;63:207–22. [Google Scholar]
- [55].Darlow B, Coleman K, McKinlay E, et al. The positive impact of interprofessional education: a controlled trial to evaluate a programme for health professional students. BMC Med Educ 2015;15:98. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [56].McKimm J, Sheehan D, Poole P, et al. Interprofessional learning in medical education in New Zealand. NZ Med J 2010;123:96–106. [PubMed] [Google Scholar]
- [57].Ogawara H, Hayashi T, Asakawa Y, et al. Systematic inclusion of mandatory interprofessional education in health professions curricula at Gunma University: a report of student self-assessment in a nine-year implementation. Hum Res Health 2009;7:60. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [58].Kishimoto M, Noda M. The difficulties of interprofessional teamwork in diabetes care: a questionnaire survey. J Multidiscip Healthc 2014;7:333–9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [59].Rowthorn V. A place for all at the global health table: a case study about creating an interprofessional global health project. J Law Med Ethics 2013;41:907. [DOI] [PubMed] [Google Scholar]
- [60].Byakika-Kibwika P, Kutesa A, Baingana R, et al. A situation analysis of inter-professional education and practice for ethics and professionalism training at Makerere University College of Health Sciences. BMC Res Notes 2015;8:598. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [61].Ngassapa OD, Kaaya EE, Fyfe MV, et al. Curricular transformation of health professions education in Tanzania: the process at Muhimbili University of Health and Allied Sciences (2008–2011). J Public Health Policy 2012;33:S64–91. [DOI] [PubMed] [Google Scholar]
- [62].Hosny S, Kamel MH, El-Wazir Y, et al. Integrating interprofessional education in community-based learning activities: case study. Med Teach 2013;35:S68–73. [DOI] [PubMed] [Google Scholar]
- [63].Minning S. Jones M, Forman D, Thistlethwaite J. Community development of interprofessional practice in Kenya. Leadership Development for Interprofessional Education and Collaborative Practice. London: Palgrave Macmillan; 2014. 196–205. [Google Scholar]
- [64].de Miranda Neto MV, Leonello VM, Oliveira MA. Multiprofessional residency in health: a document analysis of political pedagogical projects. Rev Bras Enferm 2015;68: 502–9, 586–93. [DOI] [PubMed] [Google Scholar]
- [65].Wilbur K, Hasnani-Samnani Z, Kelly I. Interprofessional education activity among undergraduate nursing and pharmacy students in the Middle East. Nurse Educ 2015;40:163–4. [DOI] [PubMed] [Google Scholar]
- [66].Wilbur K, Kelly I. Interprofessional impressions among nursing and pharmacy students: a qualitative study to inform interprofessional education initiatives. BMC Med Educ 2015;15:53. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [67].Wilby KJ, Al-Abdi T, Hassan A, et al. Attitudes of pharmacy and nutrition students towards team-based care after first exposure to interprofessional education in Qatar. J Interprof Care 2015;29:82–4. [DOI] [PubMed] [Google Scholar]
- [68].Opina-Tan LA. A pilot implementation of interprofessional education in a community-academe partnership in the Philippines. Educ Health 2013;26:164–71. [DOI] [PubMed] [Google Scholar]
- [69].Samarasekera DD, Ooi S, Yeo SP, et al. Medical education in Singapore. Med Teach 2015;37:707–13. [DOI] [PubMed] [Google Scholar]
- [70].Jacobs JL, Samarasekera DD, Chui WK, et al. Building a successful platform for interprofessional education for health professions in an Asian university. Med Teach 2013;35:343–7. [DOI] [PubMed] [Google Scholar]
- [71].Lam W, Chan EA, Yeung KS. Implications for school nursing through interprofessional education and practice. J Clin Nurs 2013;22:1988–2001. [DOI] [PubMed] [Google Scholar]
- [72].Chan EA, Chi SP, Ching S, et al. Interprofessional education: the interface of nursing and social work. J Clin Nurs 2010;19:168–76. [DOI] [PubMed] [Google Scholar]
- [73].Lo EC. Enhancing health care services through close collaboration between medical and dental professionals. Hong Kong Med J 2014;20:92–3. [DOI] [PubMed] [Google Scholar]
- [74].Hui EC. Perceptions of ethical practices in Hong Kong public hospitals: inter- and intra-professional similarities and differences. J Nurs Manag 2010;18:746–56. [DOI] [PubMed] [Google Scholar]
- [75].Wang Y, Liu YF, Li H, et al. Attitudes toward physician-nurse collaboration in pediatric workers and undergraduate medical/nursing students. Behav Neurol 2015;2015:846498. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [76].Wang R, Shi N, Bai J, et al. Implementation and evaluation of an interprofessional simulation-based education program for undergraduate nursing students in operating room nursing education: a randomized controlled trial. BMC Med Educ 2015;15:115–23. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [77].Wiwik K OS. Natural disaster and inter professional education. Pharmaçiana 2015;5: 93–100, 08. [Google Scholar]
- [78].Bansal P, Jamker A. Faculty development in health professional education—The Health Sciences University models—Interprofessional leadership in action. Palgrave Macmillan 2014;7:151–61. [Google Scholar]
- [79].Olupeliyawa AM, Balasooriya CD, Hughes C, et al. Transition to clinical practice as a medical graduate: what collaborative competencies and behaviours are critical? Focus Health Prof Educ 2013;14:57–70. [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.