

Abstract
Objective
E-diaries and accelerometers promise more objective, real-time measurements of health behavior. However, social-psychological theory suggests that using electronic behavioral monitoring may influence rather than just record physical activity (PA), especially when a device is novel.
Design
Participants (n=146) were randomly assigned to either an accelerometer-only, e-diary-only, accelerometer+e-diary, or a no-technology control group for one week to assess how these technologies influenced PA, both perceived and actual, in young adults.
Method
Participants reported their PA, overall and number of discrete exercise sessions (DES) at baseline and follow-up; accelerometers provided daily step counts and e-diaries captured daily reports of PA for the active week of the study.
Results
Average daily steps in the accelerometer-only and accelerometer+e-diary groups did not differ nor did daily reports of PA via e-diary compared to accelerometer+e-diary group, showing that neither technology affected actual PA. ANCOVAS tested group differences in perceived PA; The accelerometer-only group had increased perceived overall PA but not DES compared to no-technology control.
Conclusions
Accelerometers may increase perceived overall PA, but the tested technologies did not increase DES or actual PA, suggesting that they may be viable unbiased measures of PA.
E-diaries (electronic daily diaries) and accelerometers offer considerable advantages over traditional, retrospective paper and pencil data collection by enabling increased objectivity and real-time data collection in naturalistic settings. This reduces the potential for participant recall error and social-desirability bias, both of which are problems associated with retrospective self-reports of behavior (Adams et al., 2005; Baranowski, 1988; Shephard, 2003). These technologies can also be used to tailor interventions to individuals’ or populations’ specific needs, such as providing age-appropriate and goal-appropriate cues for behavior or to measure the effects of interventions on physical activity (PA). Further, many of these technologies are already accessible to the public, which can be useful to researchers with limited funding. As a result, electronic and mobile methods, like e-diaries or accelerometers, are considered by many to be the “gold standard” in measurement (e.g., electronic monitoring bottles for medication adherence; Cramer, 1995; Riekert & Rand, 2002) and are increasingly being used in behavior change interventions (Conroy, Yang, & Maher, 2014; King et al., 2013). However, a fundamental question regarding validity of these technologies for behavioral measurement is whether and to what extent they influence behavior, rather than just record it.
Understanding the extent to which these technologies may influence behavior could improve the accuracy of behavioral measurement. Behavior theories may be insufficient for determining whether, to what extent, and in what direction electronic monitoring could influence behavior. For example, the mere measurement effect suggests that simple awareness of being measured could change behaviour (Clemes & Deans, 2012; Vandoni, Correale, Del Bianco, Marin, & Codrons, 2016). The increased feedback provided by electronic monitoring devices could further increase behavior (Clemes & Deans, 2012; Clemes, Matchett, & Wane, 2008), especially when participants are specifically required to report that feedback (Clemes & Deans, 2012), but participants could also experience reactivity and decrease their behavior (Motl, McAuley, & Dlugonski, 2012). Researchers already have begun testing the effects of behavioral monitoring across a wide range of behaviors such as physical activity, eating, and medication adherence (French & Sutton, 2010; Sutton et al., 2014; Thomas, Dourish, & Higgs, 2015), but data are still scarce and results may be condition and behavior dependent. Using a technology that not only measures behavior but changes it as well could compromise the validity of the research. Thus, more empirical data testing the effects of wearing accelerometers and/or completing e-diaries is needed.
It is of research interest to determine the unique effects of e-diaries and accelerometers not only on actual PA but also on perceived PA(i.e., self-reports of PA), since it is often used as a proxy for actual PA when objective measurement is not available. Further, perceived PA may influence actual PA indirectly, such as through self-efficacy beliefs (McAuley & Blissmer, 2000).
In addition to examining the effects of e-diaries and accelerometers on both perceived and actual PA, it is also of interest to examine the effect of each technology on multiple components of perceived PA such as duration (for how long one is active), intensity (mild, moderate, or vigorous), and frequency (how often one engages in PA), as these are each associated with optimal health (Hordern et al., 2012; Swain & Franklin, 2006; Tanasescu et al., 2002). Another component of PA important to health or other activity-related goals is the frequency of discrete exercise sessions. Discrete exercise sessions refers to engagement in intentional PA (i.e., exercise) for an extended duration (Caspersen, Powell, & Christenson, 1985; Gettman et al., 1976). Assessing multiple components of perceived PA could also be informative to researchers using e-diaries and/or accelerometers since each devise could differentially influence each component of PA. For example, the feedback provided by many accelerometers could potentially increase steps per day (Burke et al., 2012) but not vigorous PA or frequency of discrete exercise sessions, which presumably require more forethought and planning (Rhodes & de Bruijn, 2010).
Study Overview
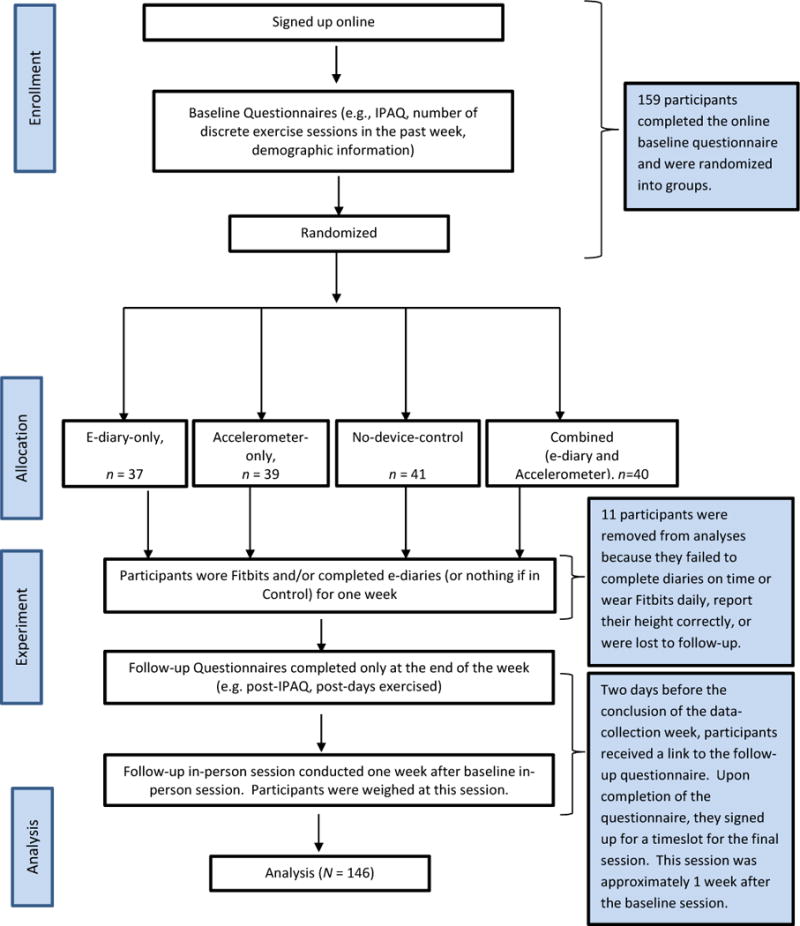
The current paper presents an experiment that evaluates the effect of two different, commercially available technologies, e-diaries and accelerometers, on participants’ perceived and actual PA. The e-diary was completed through Google Docs every night and the commercially available accelerometer was a Fitbit Zip (Fitbit Inc.) that participants wore daily. Participants were randomized into one of four groups: Accelerometer-only, e-diary-only, combined accelerometer+e-diary, or control. Participants completed a baseline questionnaire then completed/wore the accelerometer, e-diary, both, or neither for one week before completing the final questionnaire (see Figure 1), since evidence suggests that the most reactivity to devices occurs within the first week (Clemes & Denes, 2012). Given the literature on the effects of behavioral monitoring and feedback on behavior, the purpose of this study was to examine the extent to which the e-diary and accelerometer influenced participants’ actual and perceived total PA.
Figure 1.
Study Flow Chart
Hypotheses
We hypothesized that (1) the accelerometer will increase actual and perceived PA (2) the e-diary will increase actual and perceived PA, but to a lesser extent than the accelerometer since the accelerometer monitors behavior and provides feedback to the wearer; (3) Because it requires forethought and planning, the e-diary and accelerometer will not influence perceived discrete exercise sessions.
Method
Design
A randomized controlled experiment evaluated the unique effects of using the accelerometer and e-diaries for one week on actual and self-reported PA. A 2 (accelerometer, No accelerometer) × 2 (e-diary, no e-diary), randomized, between-subjects design was used and participants were either in the accelerometer-only, e-diary-only, combined (both devices) or control (no devices) group (see Figure 1 for study flowchart). A one-week use-period for the devices was chosen for feasibility reasons and because the greatest influence of a device should be when it is novel – when the individual is likely to be most reactive to the device (Piazza et al., 1990).
To evaluate the influence of a technology on actual PA, actual PA among those in the e-diary or accelerometer group should be compared to actual PA among those in the control group. However, accurate measure of actual PA requires a device (e.g., accelerometer or e-diary), eliminating the opportunity for a true no-device control group. Thus, to evaluate the influence of each device on participants’ actual PA, the accelerometer-only group was compared to the combined group to gauge the unique influence of the e-diary. The e-diary group was compared to the combined group to gauge the influence of the accelerometer. To evaluate the influence of each device on participants’ perceptions of their PA, we used parallel comparisons as with actual PA, but also compared each device to no-device-controls.
Participants and Procedure
Participants were 146 undergraduates from a medium-sized, private, urban university. Power analyses conducted using G*Power 3.1 (Faul, Erdfelder, Buchner, & Lang, 2009), indicated that 32 participants per group (128 total) would be required to detect a medium effect (f = 0.25) in the difference between four group means (as will be used for the self-reported PA outcome). Our effect size estimation was based on the very limited existing literature examining reactivity to pedometers (Clemes & Deans, 2012) as well as logistical reasons such as time, money, and availability of accelerometers.
Participants signed up for the study online using a departmental research website. After signing up for the study, participants completed an online survey using Qualtrics software (Qualtrics, Provo, UT), where they completed the baseline measures of self-reported PA and discrete exercise sessions as well as demographic information. Upon completion of the survey, participants signed up to meet with the researchers in person. In the in-person session, participants were randomized into one of the four groups—wear the accelerometer only (accelerometer-only), report exercise daily via an e-diary only (e-diary-only), both wear the accelerometer and complete the e-diary daily (combined), or to use neither technology (control) and reviewed all steps of the study with the researchers. Depending on their group, participants were also instructed on how to complete the e-diary and/or wear the accelerometer correctly at this in-person session. Research assistants never discussed how long, often, or intense to exercise in order to avoid influencing any group and preserve consistency between groups. Length of meetings ranged from five minutes for those in the control group to ten minutes for those in the combined and accelerometer-only groups.
During the subsequent week, participants wore their accelerometers daily and/or completed their e-diaries every night. In the e-diary-only and combined groups, participants completed four questions via the e-diary regarding their minutes of mild, moderate, and vigorous PA and their discrete exercise sessions for each day using Google Docs. The link to the Google Doc was emailed to participants each evening at 6pm. This time was carefully chosen because it was near the end of the day while still giving participants options for when to fill it out in order to increase compliance. Those in the control group were not expected to do anything.
One week after their initial in-person meeting, participants completed a follow-up questionnaire, where they completed the IPAQ and exercise-session frequency questions again and evaluated the accuracy and ease of the methods they used. In the follow-up session, researchers weighed and measured the height of all participants and collected the accelerometers from those who had them. Participants in all groups were expected to attend both in-person meetings in order to minimize differences between groups. Only two participants failed to attend the follow-up in-person session; one was in the combined group and the other in the e-diary group. Participants received partial course credit for full participation in the study. All procedures were approved by the Institution’s Review Board.
Measures/Instruments
Self-reported physical activity
Total PA
(International Physical Activity Questionnaire (IPAQ); Ainsworth et al., 2006; Booth, 2000). The short form of the IPAQ was used to estimate self-reported total minutes and intensity of PA. Instructions were modified so that participants only reported their typical minutes per day of intentional mild, moderate, and vigorous PA. Instructions explained that intentional PA was any activity in which they engaged, at least to some degree, because they wanted to be active. The example given to participants was taking the stairs versus taking an elevator; if they chose to take the stairs instead of an elevator because they would be getting activity, then that counted as intentional, even if they also took the stairs for other reasons, such as potentially being a faster way to class. Participants were provided standard examples of an activity (example for vigorous: running) as well as physiological cues (difficult to maintain a conversation, increased heart rate). With mild, moderate, and vigorous levels of PA estimated to utilize, respectively, 3.3, 4, and 8 calories per minute (Guidelines for Data Processing and Analysis of the International Physical Activity Questionnaire (IPAQ). Short and Long Forms, 2005), each participant’s Metabolic Equivalent of a Task (MET)—reflecting their overall PA— was calculated using the following formula:
with Amld representing minutes per week of mild activity, Amod representing minutes per week of moderate activity, and Avig representing minutes per week of vigorous activity. Among college students, the IPAQ is not highly correlated to accelerometers and pedometers (scores range from 0.15–0.26 in previous studies). The IPAQ does have reasonable test-retest reliability (scores range from 0.71–0.89; Dinger, Behrens, & Han, 2006).
Number of discrete exercise sessions
At baseline and one week after baseline, participants reported how many days in the past week they engaged in at least 20 minutes of consecutive exercise at a moderate or higher intensity level. National guidelines on PA amounts for cardiovascular health suggest at least 20 minutes of vigorous activity per day, at least three times per week, and/or 30 minutes of moderate activity every day of the week (Physical Activity Guidelines for Americans, 2008). We chose a lenient threshold when combining these recommendations into a single item for defining an exercise session, and hence the thresholds of at least 20 minutes of at least moderate activity. Research has demonstrated that moderate and vigorous exercise paired together leads to greater health outcomes than moderate exercise alone.
We chose to query bouts of exercise lasting at least 20 minutes rather than 10 minutes because the former is a better barometer of meeting exercise guidelines. Participants’ choices ranged from zero to seven days.
E-diaries
Participants completed an electronic daily diary (e-diary) each night using a form created and managed in Google Docs- word-processing documents maintained online that are shareable with specified individuals via email address “invitations.” Google Docs can be pre-formatted with questions and participants’ responses to questions are automatically recorded and time-stamped in the maintaining server, which is accessible only by the researcher. Each time a Google Doc link is accessed by a participant, the previous responses are gone, leaving blank questions to answer anew. Google Docs are a widely used medium by college students in the US, and were, therefore, familiar to participants in the current study, reducing training demands. The form included the IPAQ for intentional PA and MET scores were calculated to estimate electronically-assessed PA (see description in the IPAQ section of Measures for more details). Participants also indicated whether they had engaged in at least 20 consecutive minutes of intentional moderate to vigorous activity that day (with a “Yes” or “No” response option). Participants were e-mailed daily by 6pm with the link to the e-diary reminding them to complete the form.
Only e-diary entries completed by midnight the following day were used in analyses. After 24 hours, the accuracy of participants’ daily report may decrease due to interference of the subsequent day’s activity. Only participants who had actually completed the diary on at least 70% of the days (at least five out of seven) were included in analyses (92% of those in the e-diary or combined group).
Accelerometer
Participants wore a Fitbit Zip (Fitbit Inc., San Francisco, CA) on their shirt collars, bras, pockets, or belt loops every day for one week. The Zip is the basic Fitbit model, which provides information to the researcher on number of steps per minute (providing intensity information as well as overall number of steps). Participants could see only the number of steps taken within the current day (the running total display on the Fitbit Zip resets to zero steps at midnight each day). Since the purpose of the study was to determine whether researchers could measure activity objectively without changing activity, participant data was intentionally not linked to the smartphone application in order to limit the amount of feedback that participants received. We also collected only steps-per-day since this was the most likely to change as a result of using the device since it encompassed all intensity levels and mirrored the feedback provided on the screen. If participants were wearing their Fitbits at all, there should have been at least some movement recorded each day. Therefore, any days with zero minutes of mild activity were considered “incomplete” (all days with zero minutes of mild activity also had zero minutes of moderate and vigorous activity). Like the diaries, participants were included in analyses if they wore the Fitbit on at least five out of seven days (92% of those in the accelerometer or combined group). Since Fitbits are water resistant but not water proof, participants were instructed to remove devices when they were swimming, in the shower, or any other times when they felt they were at risk of breaking or losing their Fitbits. As such, for some participants, Fitbits may have underestimated actual PA. Previous research has shown high test-retest reliability for the Fitbit Zip (r = .90) as well as similar step estimates to a gold standard tracker (Mean absolute percentage error = 0.3) (Kooiman et al., 2015).
Sample Characteristics
Participants self-reported their gender, age, year in school, ethnicity, and race. Researchers also weighed participants and measured their height when they came in for their follow-up but not at baseline to avoid influencing reports of exercise. Height was collected using a tape measurer to the 10th inch and weight was collected using a Full Body Sensor Body Composition Monitor and Scale (Model HBF-514 by Omron Health Care Co, Ltd. (Lake Forest, IL). Data was reported to the 100th of a pound. Participants removed their shoes for both measurements. Measured height and weight were used to calculate the body mass index (BMI) using the equation BMI = kilograms/meters2.
Statistical Analysis
First, a one-way Analysis of Variance (ANOVA) was conducted to check if randomization was successful on baseline levels of perceived PA (IPAQ), number of discrete exercise sessions, and sample characteristics. Next, independent samples t-tests were used to test whether the accelerometer or the e-diary influenced actual PA. The unique influence of the accelerometer was tested by comparing e-diary scores for the e-diary-only and the combined groups. The unique influence of the e-diary was ascertained by comparing accelerometer scores for the accelerometer-only and the combined groups. Analyses of co-variance were used to test the influence of the accelerometer and/or the e-diary on perceived PA (both total PA and separated by intensity) and number of discrete exercise sessions during the week of the study controlling for the appropriate baseline perceived PA (total PA, by intensity, or discrete exercise sessions respectively). Tukey A-priori planned comparisons were used for each comparison. Reports of PA for each device were compared to reports from the no-device control group. Further, to examine the unique effects of each device, pair-wise comparisons paralleled those for actual PA (See table 1 for a description of each objective and the corresponding planned comparisons).
Table 1.
Description of Each Objective and the Comparisons Tested
| Objective | Group Comparisons | Outcome | Expected Result |
|---|---|---|---|
| Influence of the Fitbit… | |||
| On actual PA as reported in the e-diary | e-diary-only vs. e-diary+accelerometer | METS as reported via the e-diary | Greater average MET score in combined than in e-diary- only group. |
| On perceived total PA | Accelerometer-only vs. control | Perceived total PA (total METs from the IPAQ) | More perceived total PA in the Accelerometer-only group compared to control. |
| On perceived number of discrete exercise sessions | Accelerometer-only vs. control | Number of perceived discrete exercise sessions | No difference between groups |
| Influence of the e-diary… | |||
| On actual PA as measured by the accelerometer | accelerometer-only vs. e-diary+accelerometer | Average steps per day of study as measured via Fitbit | Greater average accelerometer steps in e-diary+accelerometer than in accelerometer-only group. |
| On perceived total PA | e-diary-only vs. control | Perceived total PA (total METs from the IPAQ) | More perceived total PA in the e-diary-only group compared to control. |
| On perceived number of discrete exercise sessions | e-diary-only vs. control | Number of perceived discrete exercise sessions | No difference between groups |
| Influence of each device on exercise intensity | |||
| Influence of each device on perceived mild, moderate, and vigorous PA | e-diary-only or accelerometer-only vs. control | Perceived mild, moderate, or vigorous PA (METS from the IPAQ) | More perceived mild, moderate, and vigorous PA in the e-diary-only and accelerometer-only groups compared to control. |
Results
Preliminary Analyses
Bivariate correlations are presented in Supplementary Table 1. Participant compliance with the protocol was evaluated; in addition to those removed from analyses because they were lost to follow-up (two participants) or did not complete their diaries on time or wear their accelerometers at least five days of the week (two from the e-diary-only group, three from the accelerometer-only group, and four from the combined group), two additional participants were removed from relevant analyses because height was not recorded correctly, leading to unrealistic BMI values. The final sample size (n = 146) included in the analyses had 35 participants in the accelerometer-only group, 34 in the daily-diary-only group, 36 in the combined group, and 41 in the control group. Approximately 60% of participants identified as White and almost 75% identified as female; on average participants were about 20 years old (19.39 years; ages ranged from 18–22 years) and normal weight (BMI = 23.72)
There were no significant differences between groups on age, or BMI (p-values > .05; See Table 2), indicating random assignment was successful, regarding potentially confounding variables. There were no significant differences in total perceived PA (F(3,142) = 1.89, p = 0.13, η2 = 0.04) or number of discrete exercise sessions (F(3, 142) = 0.98, p = 0.41) at baseline, meaning random assignment was successful in these outcome-related variables as well.
Table 2.
Sample Characteristics by Experimental Condition
| Total | Accelerometer-only | E-diary-only | E-diary + Accelerometer | Control | |
|---|---|---|---|---|---|
| Gender | |||||
| Female | 74.0% | 62.9% | 76.5% | 72.2% | 82.9% |
| Male | 26.0% | 37.1% | 23.5% | 27.8% | 17.1% |
| BMI (kg/m2) | 23.72±4.32 | 23.26±4.11 | 22.50±3.52 | 23.53±4.94 | 23.52±3.47 |
| Age (years) | 19.62±1.59 | 19.34±1.08 | 19.97±1.80 | 19.58±1.75 | 19.59±1.66 |
| Year in School | |||||
| Freshman | 32.2% | 31.4% | 23.5% | 38.9% | 34.1% |
| Sophomore | 37.7% | 37.1% | 32.4% | 33.3% | 46.3% |
| Junior | 15.8% | 17.1% | 26.5% | 13.9% | 7.3% |
| Senior | 14.4% | 14.3% | 28.6% | 23.8% | 12.2% |
| Ethnicity | |||||
| Hispanic | 7.5% | 2.9% | 5.9% | 13.9% | 7.3% |
| Non-Hispanic | 92.5% | 97.1% | 94.1% | 86.1% | 92.7% |
| Race | |||||
| White/Caucasian | 64.4% | 68.6% | 55.9% | 72.2% | 61.0% |
| Black/African American | 4.8% | 11.4% | 8.8% | 0.0% | 0.0% |
| Asian | 22.6% | 14.3% | 32.4% | 13.9% | 26.8% |
| Other | 8.2% | 5.7% | 2.9% | 13.9% | 12.2% |
| Discrete Exercise Sessions | 3.61±2.16 | 3.97±2.2 | 3.43±2.15 | 3.46±2.09 | 3.61±2.28 |
| Perceived Exercise | 489.7±469.3 | 579.0±568.1 | 464.2±373.7 | 555.1±547.5 | 376.1±348.8 |
Note. ANOVAS and chi2 tests were used to determine differences between groups. Results showed no between-group differences at the α=.05 significance level. Sample Characteristics are presented as mean ± standard deviation or percent
Influence of the Accelerometer
On PA reported in the e-diary over the week of the study (METS)
There was no significant difference (t(63) = −1.12, p = 0.27) in total METs measured by the e-diary-only and combined groups (see table 3).
Table 3.
Means and Standard Deviations by Condition for Each Aspect of Physical Activity at Follow-Up.
| Accelerometer-only | E-diary-only | E-diary + Accelerometer | Control | Effect Size | |
|---|---|---|---|---|---|
| Actual PA from the e-diary or accelerometer | |||||
| METS (e-diary) | ----------- | 247.01±192.77a | 373.63±636.55a | ----------- | d=−.27 |
| Total steps/day (Accelerometer) | 9129.28±3192.45a | ----------- | 8253.04±2880.27a | ----------- | d=.29 |
| Perceived PA* | |||||
| METS (total PA; IPAQ) | 3866.58±423.07a | 2002.24±421.41b | 2392.68±410.41b | 2110.99±391.3b | η2 =.01 |
| Discrete exercise sessions | 3.43±0.34a | 3.85±0.34a | 4.22±0.33a | 3.69±0.32a | η2 =.10 |
| Perceived minutes per week at each intensityc | |||||
| Mild | 422.99±71.61a | 134.88±71.52b | 309.64±89.68ab | 206.42±66.52b | η2 =.06 |
| Moderate | 292.24±42.08a | 92.04±42.12b | 128.97±40.91b | 115.33±38.93b | η2 =.08 |
| Vigorous | 162.52±20.81a | 143.40±20.82a | 106.73±20.20a | 125.82±19.17a | η2 =.03 |
Note. Means with differing subscripts within rows are significantly different at the α=.05 significance value based on A-priori planned Comparisons
Models control for baseline exercise
On perceived total PA measured by the IPAQ at post-test (METS)
There was no difference in total PA between those in the e-diary-only group and those in the combined group (absolute mean difference = 390.44, SE = 589.76, p = 0.51). Compared to the control group, however, those in the accelerometer-only group did report significantly more self-reported total PA (absolute mean difference = 1755.60, SE = 580.06, p = 0.003) (see table 3).
On perceived number of discrete exercise sessions for the week
There was no difference in number of discrete exercise sessions between those in the e-diary-only group and those in the combined group (absolute mean difference = 0.38, SE = 0.48, p = 0.43). There was also no difference in number of discrete exercise sessions between those in the accelerometer-only group and those in the control group (absolute mean difference = 0.25, SE = .47, p = .59) (see table 3).
Influence of the e-diary
On PA measured by the accelerometer over the week of the study (average steps per day)
There was no significant difference (t(65) = 1.18, p = 0.24) in total steps measured by the accelerometer-only and combined groups (see table 3).
On perceived total PA measured by the IPAQ at post-test (METS)
Those in the combined group reported significantly less PA than those in the accelerometer-only group (absolute mean difference = 1473.90, SE = 586.80, p=0.013), but there was no difference in total PA between the e-diary-only group and the control group (absolute mean difference = 108.75, SE = 572.93, p=0.85). This suggests that the e-diary alone does not reduce self-reported total PA, but may mitigate the influence of the accelerometer on self-reported total PA (see table 3).
On perceived number of discrete exercise sessions for the week
There was no difference in number of discrete exercise sessions between those in the accelerometer-only group and those in the combined group (absolute mean difference = 0.79, SE = .48, p=.10). There was also no difference in number of discrete exercise sessions between those in the e-diary-only group and those in the control group (absolute mean difference = 0.16, SE = 0.47, p=0.73) (see table 3).
Exercise Intensity
Results showed significant differences by treatment condition for perceptions of moderate PA (F(3, 142) = 4.78, p = 0.003, η2 = 0.09) and mild PA (F(3,142) = 3.11, p=0.03, η2 = 0.06) but no significant difference by treatment condition for vigorous PA (F(3,142) = 1.37, p = 0.25, η2 = 0.03). For moderate PA, those in the accelerometer-only group reported significantly more minutes of moderate activity than the control, combined or e-diary-only groups (p-values<0.01). For mild PA, the accelerometer-only group reported significantly more minutes of mild activity than the e-diary-only and the control groups (p-values < 0.02); Table 3).
Discussion
This study extends and supports the limited research on the practicality of using e-diaries and accelerometry in research. It is among the first to test whether these technologies influence, rather than just measure, actual PA as well as multiple aspects of perceived PA: total perceived PA; perceived number of discrete exercise sessions; and minutes of mild, moderate, and vigorous perceived PA.
Results partially supported the hypothesis that the consumer-available accelerometer would increase perceived and actual total PA. While there was no effect of wearing an accelerometer for a week on electronically measured PA, the accelerometers did influence perceptions of total PA, but only when they were worn alone. This supports literature that monitoring of behavior can influence perceptions of behavior, particularly when the individual is provided with feedback about the behavior (as with the accelerometer, but not with the e-diaries) (Clemes & Parker, 2009; Michie, Abraham, Whittington, McAteer, & Gupta, 2009). It also supports recent literature showing that feedback alone may not be sufficient for affecting significant behavior change (Behrens & Dinger, 2007; Davis & Loprinzi, 2016; Dusseldorp, van Genugten, van Buuren, Verheijden, & van Empelen, 2014).
It is worth noting that the Fitbit Zip, along with other Fitbit models or accelerometers, has the potential to provide more feedback than was given to our participants. For example, many devices including the Fitbit Zip can be synced to smartphone applications that provide graphs, badges, goals, estimates of calories burned, etc., which have the potential to change perceived and actual behaviour. Thus, our results demonstrate the possibility of using the Fitbit Zip to measure PA for a week without influencing it, but do not speak to whether using all of the tools provided by the Fitbit Zip and accompanying smartphone app can change behaviour.
Results did not support the second hypothesis, that the e-diary would increase perceived and electronically measured PA. The e-diary had no effect on actual PA, as measured by the accelerometer, or on self-reported total PA compared to the control group. Interestingly, since the combined group reported significantly lower perceived total PA than the accelerometer-only group at follow-up, the addition of the e-diary seems to have mitigated the effect of the accelerometer on perceptions of total PA. This is in contrast to previous literature showing that recording step counts increases physical activity (Clemes & Deans, 2012; Clemes & Parker, 2009). However, the distinction may be that participants did not write information from the accelerometer into the e-diary, since not everyone with an e-diary had an accelerometer. Instead, they wrote their estimates minutes of mild, vigorous, and moderate PA. This difference could explain why the diary tempered rather than reinforced the effect of the accelerometer.
Combining accelerometers with e-diaries is theoretically advantageous for researchers interested in measuring intentional and incidental PA using diary methods (e.g., Alahmari et al., 2016; Forrest, Smith, Fussner, Dodd, & Clerkin, 2016). It is promising to see that the use of the diary mitigated the effects of the accelerometer on participants’ self-reported activity at follow-up. Since there was no effect of any device on actual PA, the most likely explanation is that the feedback provided by the accelerometer inaccurately inflated perceived exercise. However, those in the combined group, also went through the steps each night of completing the e-diary (thinking through intentional vs. incidental activity; reviewing one’s actual exercise) and this may have anchored them back to reality.
Hypothesis three was supported: the number of self-reported discrete exercise sessions did not increase with either technology. Thus, these technologies do not seem to influence participants’ perceptions of their own number of discrete exercise sessions. This may be because while self-monitoring and feedback may encourage a slight increase in steps, they do not motivate going to the gym, which requires forethought and planning. The participant is likely cognizant of this fact and, as a result, perceptions of discrete exercise sessions remain realistic and not influenced by these technologies.
Similar to discrete exercise sessions, vigorous exercise typically requires more forethought and planning than moderate or, especially, mild exercise. Following this logic, it is not surprising that the increases in perceptions of total PA observed in the accelerometer-only group were driven primarily by increases in self-reported mild and moderate PA, but not vigorous PA. Additionally, mild and moderate PA are not always identified as “exercise” to the extent that vigorous activity would be, especially since they may be part of daily activities and may not cause the participant to sweat, have a racing heart rate, or feel out of breath. Thus, the feedback provided by the accelerometer on mild and moderate PA may have surprised participants and led to inflated estimates of those intensities for those who did not also complete the e-diary.
Overall, findings from this study are encouraging for researchers interested in obtaining more accurate measurements of exercise but worried about potential reactance with novel devices. It is possible that prolonged use with the accelerometers or e-diaries would cause a change in behavior not observed after only one week and this possibility should be tested in future studies. However, research would predict that the greatest reactance would occur while the device was still novel and the influence of the device would actually reduce over time (Baron, Hirani, & Newman, 2015). Overall, the fact that neither the e-diaries nor the accelerometers increased self-reports of vigorous intentional PA or frequency of discrete exercise sessions is a promising result for researchers who want to use these methods to observe exercise, at least in healthy young adults. It is also promising to note that researchers who want to use an accelerometer without changing self-reports of behavior may be able to mitigate its effect by including some version of a daily diary that requires participants to think carefully about their exercise.
Findings from this study do not negate evidence that monitoring can change behavior (Michie et al., 2009), especially when people are motivated to improve their behaviour or in the context of behavioural interventions specifically designed to change behaviour. What our results show is that while monitoring can theoretically change behavior, it is also possible to measure PA without affecting behavior.
Strengths and Limitations
This study has several limitations that should be considered. While we attempted to keep the experience of those in all groups relatively similar by requiring everyone to come in for their baseline and follow-up sessions, everyone who wore the accelerometer had more extensive training from the researchers on how and when to wear the accelerometer. This added an additional five minutes on average to what those in the e-diary-only or control group experienced. This additional time with researchers at the baseline meeting may have influenced results; however the accelerometer-only group actually had higher self-reported exercise than the combined group who had the longest meetings. Another limitation is the use of a convenience sample of young, healthy, active adults. Physical activity measurements may have less of an effect on active versus sedentary adults. Further, technologies such as consumer-available accelerometers and electronic diaries may be more native to a young sample, leading to a more seamless integration into their experiences and, subsequently, fewer changes in their behavior than an older sample. For participants who already owned a Fitbit, using the device may have had a smaller impact on their behavior. We did not record prior or current ownership of a Fitbit; however, in a subsequent study, only two out of 135 participants reported that they owned a Fitbit, and these were not students as in the current sample but staff members. We also did not record whether participants had prior knowledge of step-count recommendations. While these limitations may affect the generalizability of our findings, it likely had little effect on internal validity, since participants were successfully randomized to groups. However, it would be interesting to examine the extent to which knowing step-count recommendations increases or tempers perceived and actual PA for those using an accelerometer. Finally, we measured only steps-per-day from the accelerometer without taking intensity into account. It is unlikely that using the device significantly influenced any intensity of exercise or we would have seen an overall effect. However, it is possible that using the device may have decreased one intensity (e.g., vigorous PA) and increased another (e.g., mild PA), thereby cancelling out their affects. We have no theoretical reason to expect this but future research could examine this possibility.
This study also had several strengths. Participants were randomized into each group, and random assignment appeared to be successful on the measured covariates/potential confounds. The study had very high retention rates, with over 92% of participants wearing the accelerometers and completing their diaries on time most days of the week. Because the accelerometer we used (the Fitbit) and daily diary are popular, relatively inexpensive ($60 for the Fitbit Zip, and use of Google Docs is free), and relatively simple to use as methods for collecting exercise data, these findings may be particularly useful for researchers with limited funding and practitioners who may want to suggest use of these methods to their patients. Another strength of this study was the measurement and calculations of self-reported and electronically assessed PA. Each device was used to estimate the relative influence of the other device. In the future, reducing the amount of feedback provided to participants, potentially by turning the face of the accelerometer away from participants or using devices that allow researchers to remove the feedback may further decrease the influence of the Fitbit on participants’ behavior (Burke et al., 2012).
Experimental evidence suggests that consumer-available accelerometers and e-diaries may be used as non-reactive measures of behavior, specifically vigorous PA and discrete exercise session frequency. E-diaries may be used without influencing perceived and actual exercise but accelerometers that provide feedback may influence perceptions of behavior. Future research could further explore the role of feedback on self-reported behavior. Researchers could test whether accelerometers with less feedback (i.e., by turning off types of feedback or even turning the device away from participants) still cause increased self-reported PA. Researchers could also examine whether similar results emerge when using ecological momentary assessment to assess PA, which is similar to e-diaries but requires participants to report their behaviour multiple times throughout the day.
Conclusions
E-diaries and accelerometers provide many benefits such as more precise data collection in a natural setting. They are quickly becoming the gold-standard for measuring activity, and this study is among the first to test their influence on actual and perceived PA. Results showed that e-diaries had the least effect on behavior and therefore, they may be particularly useful for measuring PA. In addition to informing future research measuring behavior, these findings may also inform interventions to increase adherence to exercise regimens, as has been shown with other mobile devices (Burke et al., 2012)
Supplementary Material
Highlights.
Wearing an accelerometer daily increased perceived but not actual PA.
The accelerometer group reported more perceived mild & moderate but not vigorous PA.
Completing an e-diary daily did not change perceived or actual PA.
Neither the e-diary nor the accelerometer changed reported discrete exercise sessions.
Acknowledgments
this research was partially supported by the intramural research program of the National Institutes of Health, Eunice Kennedy Shriver National Institute of Child Health and Human Development and the department of psychology, Iowa State University. The authors also wish to acknowledge Katie Thompson, Margot Quinn, and Jessica Abrams for their assistance collecting data and Dr. Susan Persky and Dr. Kaigang Lee for their thoughtful comments, edits, and suggestions to this manuscript.
Footnotes
Publisher's Disclaimer: This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final citable form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.
The authors declare that they have no conflicts of interest.
References
- Adams SA, Matthews CE, Ebbeling CB, Moore CG, Cunningham JE, Fulton J, Hebert JR. The effect of social desirability and social approval on self-reports of physical activity. Am J Epidemiol. 2005;161(4):389–398. doi: 10.1093/aje/kwi054. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ainsworth BE, Macera CA, Jones DA, Reis JP, Addy CL, Bowles HR, Kohl HW., 3rd Comparison of the 2001 BRFSS and the IPAQ Physical Activity Questionnaires. Med Sci Sports Exerc. 2006;38(9):1584–1592. doi: 10.1249/01.mss.0000229457.73333.9a. [DOI] [PubMed] [Google Scholar]
- Alahmari AD, Kowlessar BS, Patel ARC, Mackay AJ, Allinson JP, Wedzicha JA, Donaldson GC. Physical activity and exercise capacity in patients with moderate COPD exacerbations. European Respiratory Journal. 2016 doi: 10.1183/13993003.01105-2015. [DOI] [PubMed] [Google Scholar]
- Baranowski T. Validity and Reliability of Self Report Measures of Physical Activity: An Information-Processing Perspective. Res Q Exerc Sport. 1988;59(4):314–327. doi: 10.1080/02701367.1988.10609379. [DOI] [Google Scholar]
- Baron J, Hirani S, Newman S. A mobile telehealth intervention for adults with insulin-requiring diabetes: early results of a mixed-methods randomized controlled trial. JMIR Res Protoc. 2015;4(1):e27. doi: 10.2196/resprot.4035. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Behrens TK, Dinger MK. Motion sensor reactivity in physically active young adults. Res Q Exerc Sport. 2007;78(2):1–8. doi: 10.1080/02701367.2007.10762229. [DOI] [PubMed] [Google Scholar]
- Booth M. Assessment of physical activity: an international perspective. Res Q Exerc Sport. 2000;71(2 Suppl):S114–120. [PubMed] [Google Scholar]
- Burke LE, Styn MA, Sereika SM, Conroy MB, Ye L, Glanz K, Ewing LJ. Using mHealth technology to enhance self-monitoring for weight loss: a randomized trial. Am J Prev Med. 2012;43(1):20–26. doi: 10.1016/j.amepre.2012.03.016. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Caspersen CJ, Powell KE, Christenson GM. Physical activity, exercise, and physical fitness: definitions and distinctions for health-related research. Public Health Reports. 1985;100(2):126–131. Retrieved from http://www.ncbi.nlm.nih.gov/pmc/articles/PMC1424733/pdf/pubhealthrep00100-0016.pdf. [PMC free article] [PubMed] [Google Scholar]
- Clemes SA, Deans NK. Presence and duration of reactivity to pedometers in adults. Med Sci Sports Exerc. 2012;44(6):1097–1101. doi: 10.1249/MSS.0b013e318242a377. [DOI] [PubMed] [Google Scholar]
- Clemes SA, Matchett N, Wane SL. Reactivity: an issue for short-term pedometer studies? Br J Sports Med. 2008;42(1):68–70. doi: 10.1136/bjsm.2007.038521. [DOI] [PubMed] [Google Scholar]
- Clemes SA, Parker RA. Increasing our understanding of reactivity to pedometers in adults. Med Sci Sports Exerc. 2009;41(3):674–680. doi: 10.1249/MSS.0b013e31818cae32. [DOI] [PubMed] [Google Scholar]
- Conroy DE, Yang CH, Maher JP. Behavior Change Techniques in Top-Ranked Mobile Apps for Physical Activity. American Journal of Preventive Medicine. 2014;46(6):649–652. doi: 10.1016/j.amepre.2014.01.010. doi: http://dx.doi.org/10.1016/j.amepre.2014.01.010. [DOI] [PubMed] [Google Scholar]
- Cramer JA. Microelectronic systems for monitoring and enhancing patient compliance with medication regimens. Drugs. 1995;49(3):321–327. doi: 10.2165/00003495-199549030-00001. [DOI] [PubMed] [Google Scholar]
- Davis R, Loprinzi PD. Examination of Accelerometer Reactivity Among a Population Sample of Children, Adolescents, and Adults. J Phys Act Health. 2016:1–27. doi: 10.1123/jpah.2015-0703. [DOI] [PubMed] [Google Scholar]
- Dinger MK, Behrens TK, Han JL. Validity and Reliability of the International Physical Activity Questionnaire in College Students. American Journal of Health Education. 2006;37(6):337–343. doi: 10.1080/19325037.2006.10598924. [DOI] [Google Scholar]
- Dusseldorp E, van Genugten L, van Buuren S, Verheijden MW, van Empelen P. Combinations of techniques that effectively change health behavior: evidence from Meta-CART analysis. Health Psychol. 2014;33(12):1530–1540. doi: 10.1037/hea0000018. [DOI] [PubMed] [Google Scholar]
- Forrest LN, Smith AR, Fussner LM, Dodd DR, Clerkin EM. Using implicit attitudes of exercise importance to predict explicit exercise dependence symptoms and exercise behaviors. Psychology of Sport and Exercise. 2016;22:91–97. doi: 10.1016/j.psychsport.2015.06.006. doi: http://dx.doi.org/10.1016/j.psychsport.2015.06.006. [DOI] [PMC free article] [PubMed] [Google Scholar]
- French DP, Sutton S. Reactivity of measurement in health psychology: how much of a problem is it? What can be done about it? Br J Health Psychol. 2010;15(Pt 3):453–468. doi: 10.1348/135910710x492341. [DOI] [PubMed] [Google Scholar]
- Gettman LR, Pollock ML, Durstine JL, Ward A, Ayres J, Linnerud AC. Physiological Responses of Men to 1, 3, and 5 Day per Week Training Programs. Research Quarterly. American Alliance for Health, Physical Education and Recreation. 1976;47(4):638–646. doi: 10.1080/10671315.1976.10616722. [DOI] [PubMed] [Google Scholar]
- Guidelines for Data Processing and Analysis of the International Physical Activity Questionnaire (IPAQ) Short and Long Forms. 2005 Retrieved from http://www.institutferran.org/documentos/scoring_short_ipaq_april04.pdf.
- Hordern MD, Dunstan DW, Prins JB, Baker MK, Singh MAF, Coombes JS. Exercise prescription for patients with type 2 diabetes and pre-diabetes: A position statement from Exercise and Sport Science Australia. Journal of Science and Medicine in Sport. 2012;15(1):25–31. doi: 10.1016/j.jsams.2011.04.005. doi: http://dx.doi.org/10.1016/j.jsams.2011.04.005. [DOI] [PubMed] [Google Scholar]
- King AC, Hekler EB, Grieco LA, Winter SJ, Sheats JL, Buman MP, Cirimele J. Harnessing Different Motivational Frames via Mobile Phones to Promote Daily Physical Activity and Reduce Sedentary Behavior in Aging Adults. PLoS ONE. 2013;8(4):e62613. doi: 10.1371/journal.pone.0062613. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kooiman TJ, Dontje ML, Sprenger SR, Krijnen WP, van der Schans CP, de Groot M. Reliability and validity of ten consumer activity trackers. BMC Sports Sci Med Rehabil. 2015;7:24. doi: 10.1186/s13102-015-0018-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- McAuley E, Blissmer B. Self-Efficacy Determinants and Consequences of Physical Activity. Exercise and Sport Sciences Reviews. 2000;28(2):85–88. Retrieved from http://journals.lww.com/acsm-essr/Fulltext/2000/28020/Self_Efficacy_Determinants_and_Consequences_of.8.aspx. [PubMed] [Google Scholar]
- Michie S, Abraham C, Whittington C, McAteer J, Gupta S. Effective techniques in healthy eating and physical activity interventions: a meta-regression. Health Psychol. 2009;28:690–701. doi: 10.1037/a0016136. [DOI] [PubMed] [Google Scholar]
- Motl RW, McAuley E, Dlugonski D. Reactivity in baseline accelerometer data from a physical activity behavioral intervention. Health Psychol. 2012;31(2):172–175. doi: 10.1037/a0025965. [DOI] [PubMed] [Google Scholar]
- Physical Activity Guidelines for Americans. United States Department of Helath and Human Services. 2008 Retrieved from https://health.gov/paguidelines.
- Piazza PV, Deminèiere JM, Maccari S, Mormède P, Moal ML, Simon H. Individual reactivity to novelty predicts probability of amphetamine self-administration. Behavioural Pharmacology. 1990;1(4):339–346. doi: 10.1097/00008877-199000140-00007. Retrieved from http://journals.lww.com/behaviouralpharm/Fulltext/1990/00140/Individual_reactivity_to_novelty_predicts.7.aspx. [DOI] [PubMed] [Google Scholar]
- Rhodes RE, de Bruijn GJ. Automatic and motivational correlates of physical activity: does intensity moderate the relationship? Behav Med. 2010;36(2):44–52. doi: 10.1080/08964281003774901. [DOI] [PubMed] [Google Scholar]
- Riekert K, Rand C. Electronic Monitoring of Medication Adherence: When Is High-Tech Best? Journal of Clinical Psychology in Medical Settings. 2002;9(1):25–34. doi: 10.1023/A:1014131928789. [DOI] [Google Scholar]
- Shephard RJ. Limits to the measurement of habitual physical activity by questionnaires. British Journal of Sports Medicine. 2003;37(3):197–206. doi: 10.1136/bjsm.37.3.197. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Sutton S, Kinmonth AL, Hardeman W, Hughes D, Boase S, Prevost AT, Farmer A. Does electronic monitoring influence adherence to medication? Randomized controlled trial of measurement reactivity. Ann Behav Med. 2014;48(3):293–299. doi: 10.1007/s12160-014-9595-x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Swain DP, Franklin BA. Comparison of Cardioprotective Benefits of Vigorous Versus Moderate Intensity Aerobic Exercise. The American Journal of Cardiology. 2006;97(1):141–147. doi: 10.1016/j.amjcard.2005.07.130. doi: http://dx.doi.org/10.1016/j.amjcard.2005.07.130. [DOI] [PubMed] [Google Scholar]
- Tanasescu M, Leitzmann MF, Rimm EB, Willett WC, Stampfer MJ, Hu FB. Exercise type and intensity in relation to coronary heart disease in men. JAMA. 2002;288(16):1994–2000. doi: 10.1001/jama.288.16.1994. Retrieved from http://jama.jamanetwork.com/data/Journals/JAMA/4853/JOC20649.pdf. [DOI] [PubMed] [Google Scholar]
- Thomas JM, Dourish CT, Higgs S. Effects of awareness that food intake is being measured by a universal eating monitor on the consumption of a pasta lunch and a cookie snack in healthy female volunteers. Appetite. 2015;92:247–251. doi: 10.1016/j.appet.2015.05.034. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Vandoni M, Correale L, Del Bianco M, Marin L, Codrons E. Does reactivity to accelerometers occur in a single trial? Brief report in a sample of young adults. J Health Psychol. 2016 doi: 10.1177/1359105316628758. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.