

Abstract
Aging is associated with significant changes in structure and function of the kidney, even in the absence of age-related comorbidities. On the macrostructural level, kidney cortical volume decreases, surface roughness increases, and the number and size of simple renal cysts increase with age. On the microstructural level, the histologic signs of nephrosclerosis (arteriosclerosis/arteriolosclerosis, global glomerulosclerosis, interstitial fibrosis, and tubular atrophy) all increase with age. The decline of nephron number is accompanied by a comparable reduction in measured whole-kidney GFR. However, single-nephron GFR remains relatively constant with healthy aging as does glomerular volume. Only when glomerulosclerosis and arteriosclerosis exceed that expected for age is there an increase in single-nephron GFR. In the absence of albuminuria, age-related reduction in GFR with the corresponding increase in CKD (defined by an eGFR<60 ml/min per 1.73 m2) has been shown to associate with a very modest to no increase in age-standardized mortality risk or ESRD. These findings raise the question of whether disease labeling of an age-related decline in GFR is appropriate. These findings also emphasize the need for a different management approach for many elderly individuals considered to have CKD by current criteria.
Keywords: aging, glomerulosclerosis, nephrosclerosis, glomerular filtration rate, nephron number, kidney volume
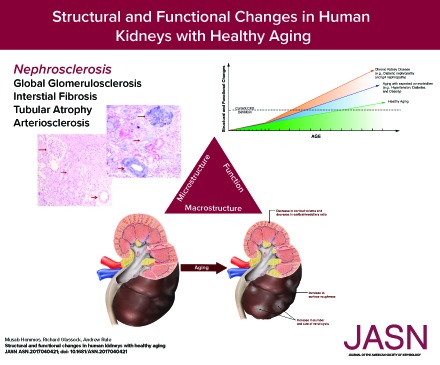
Any discussion of the aging kidney requires clarification as to what is meant by aging. Structural and functional changes in the kidney with aging can be divided into those seen with healthy aging, aging with expected comorbidity, and aging with the increased prevalence of specific kidney diseases (Figure 1). Because of the invasive nature of kidney biopsies and some kidney imaging tests, our ability to study structural changes with aging has been limited. Most kidney biopsies obtained for clinical care are in very select patients with overt kidney disease. There is also opportunity to study the renal parenchyma at death (autopsy or deceased donor biopsy); however, often, limited clinical and laboratory data are available, or structural changes from the morbid state preceding death overwhelm age-related findings.
Figure 1.

Structural and functional changes in the kidney from common co-morbidities or specific kidney diseases are additive to the underlying age-related changes that occur even in health. Healthy aging alone leads to nephrosclerosis with nephron loss and can be studied in living kidney donors. The added component of aging with expected comorbidity leads to more nephrosclerosis, larger glomeruli, and further nephron loss and can be studied in deceased kidney donors, certain autopsy settings, and patients who undergo a radical nephrectomy for a tumor. The added component of actual CKD becomes prevalent with aging and results in disease-specific changes that can be studied in patients undergoing clinically indicated biopsies for an overt nephropathy. The current single-threshold criteria-based CKD definition fails to distinguish between these three types of structural and functional changes with aging.
Unique to nephrology, there has been opportunity to specifically study healthy aging due to the comprehensive evaluation and selection on health that occurs with living kidney donors. The age range of living kidney donors spans six decades, providing a unique opportunity to study healthy aging in the absence of comorbidities. Also unique to living kidney donors is the opportunity to characterize macrostructure from a predonation computed tomography (CT) scan of the kidneys and microstructure from a biopsy of the donated kidney at transplant surgery. These studies have shown that, even in the absence of clinically evident comorbidities, there are substantial structural changes in the kidney that accompany a decline in kidney function. (Figure 2, Table 1).
Figure 2.

There are degenerative macro-structural changes that occur in the human kidney with even healthy aging. There is cortical volume loss, some increase in medullary volume (not shown), increase in surface roughness, increased sinus fat, and an increase in renal cysts. These findings can be attributed to underlying nephrosclerosis with nephron loss, hypertrophy of remaining tubules, and tubular diverticuli.
Table 1.
Structural and functional findings in the kidney with healthy aging
| Category | Age-related finding |
|---|---|
| Microstructural changes | Arteriosclerosis |
| Arteriolosclerosis | |
| Ischemic-appearing glomeruli (global deflation) | |
| Global glomerulosclerosis and obsolescence | |
| Interstitial fibrosis | |
| Tubular atrophy | |
| Decrease in nephron number | |
| Hypertrophy of remaining tubules | |
| Stable glomerular volume | |
| Macrostructural changes | Renal artery atherosclerosis and fibromuscular dysplasia |
| Decrease in cortical volume | |
| Increase in medullary volume until age 50 yr | |
| Increase in kidney surface roughness | |
| Increase in number of cysts | |
| Increase in size of cysts | |
| Functional changes | Decrease in total kidney GFR |
| Stable snGFR | |
| Stable single-nephron glomerular filtration capacity | |
| Stable and minimal urine albumin excretion (urine albumin-to-creatinine ratio will misleadingly increase from sarcopenia of aging) |
Macrostructural Changes
Kidney Volume
The length of the kidney is often assessed clinically (usually by ultrasound), but this only crudely captures the size of the kidney. A general population study of 1852 adults assessed kidney volume by magnetic resonance imaging. Total kidney volume decreases by about 16 cm3 per decade, although most of the decline occurred after the age of 60 years old. Small kidney volume (below the sex-specific tenth percentile among healthy adults) associates with older age, even after adjustment for other risk factors.1
A study of 1334 living kidney donors found kidney volume by CT scan to decline with age but only after the age of 50 years old, when it declines at 22 cm3 per decade.2 The angiographic phase of the contrast CT scan allows for separate measurement of the cortical volume and medullary volume of the kidneys. The kidney volume is 73% cortex and 27% medulla on average. Although cortical volume decreases with age, medullary volume actually increases with age until the age of 50 years old. The lack of change in total kidney volume with aging in adults up to 50 years old is explained by cortical volume loss being compensated for by medullary volume gain.
Renal Cysts and Tumors
Simple renal cysts increase with older age and are very common, particularly with high-resolution imaging modalities. The 95th percentile for number of kidney parenchymal cysts ≥5 mm for kidney donors ages 18–29 years old is one in men and one in women, but it increases to ten in men and four in women by ages 60–69 years old.3 Not only are there more parenchymal cysts with aging, but the size of the largest cyst increases with age. Other than simple renal cysts, hyperdense cysts, angiomyolipomas, parapelvic cysts (due to lymphatic dilations near the renal pelvis), and masses or cysts with features concerning for malignancy are all associated with older age.
Microstructural Changes
Nephrosclerosis
The term nephrosclerosis is used to describe findings in renal biopsy specimens that reveal a microstructural pattern of arteriosclerosis/arteriolosclerosis, focal global glomerulosclerosis (FGGS), tubular atrophy, and interstitial fibrosis. In terms of a mechanistic relationship, arteriosclerosis/arteriolosclerosis, defined as fibrous thickening and/or hyalinosis of the intima, is thought to lead to ischemia, resulting in global glomerulosclerosis with atrophy of the attached tubules and adjacent interstitial fibrosis.4 Nephrosclerosis is well known to be associated with hypertension,5 but it is also observed among healthy adults without hypertension or other relevant comorbidities. In a study of 1203 living kidney donors, nephrosclerosis was identified by the presence of two or more of the following: any glomerulosclerosis, any tubular atrophy, >5% interstitial fibrosis, and any luminal stenosis by arteriosclerosis.6 By this classification, nephrosclerosis increased from a prevalence of 2.7% among 18- to 29-year-old donors to a prevalence of 73% among 70- to 77-year-old donors. As a biopsy finding, age-related nephrosclerosis may be difficult to distinguish from chronic changes due to specific kidney diseases.7
Glomerulosclerosis
There has long been an interest in distinguishing age- from disease-related focal global glomerulosclerosis.8 Recently, the amount of glomerulosclerosis expected for a given age was described using normotensive kidney donors (Table 2).9 For example, the reference limit (95th percentile) for number of globally sclerotic glomeruli in a patient with 20 glomeruli on a kidney biopsy was 1.0 for a 20 year old but 5.5 for a 70 year old. Biopsies with abnormally higher amounts of globally sclerotic glomeruli were three times more likely to have glomeruli that were not sclerosed but had Bowman capsule thickening, pericapsular fibrosis, and capillary wrinkling (global deflation), features often attributed to ischemic injury. Donors with glomerulosclerosis that exceeded these age-based reference limits were also more likely to have hypertension or interstitial fibrosis on biopsy.
Table 2.
Upper reference limit (95th percentile) for the number of globally sclerotic glomeruli
| Age, yr | Total No. of Glomeruli Seen on Biopsy | |||||||
|---|---|---|---|---|---|---|---|---|
| 1 | 2 | 3–4 | 5–8 | 9–16 | 17–32 | 33–48 | 49–64 | |
| 18–29 | 0.5 | 0.5 | 0.5 | 0.5 | 1 | 1 | 1 | 1 |
| 30–34 | 0.5 | 0.5 | 0.5 | 0.5 | 1 | 1 | 1 | 1.5 |
| 35–39 | 0.5 | 0.5 | 0.5 | 0.5 | 1 | 1.5 | 2 | 2 |
| 40–44 | 0.5 | 0.5 | 0.5 | 1 | 1 | 2 | 2.5 | 3 |
| 45–49 | 0.5 | 0.5 | 1 | 1 | 1.5 | 2 | 3 | 4 |
| 50–54 | 1 | 1 | 1 | 1.5 | 2 | 3 | 5 | 5 |
| 55–59 | 1 | 1 | 1.5 | 1.5 | 2 | 3.5 | 4.5 | 6 |
| 60–64 | 1 | 1.5 | 1.5 | 2 | 2.5 | 4 | 5.5 | 7 |
| 65–69 | 1 | 2 | 2 | 2.5 | 3 | 4.5 | 6.5 | 8 |
| 70–74 | 1 | 2 | 2.5 | 3 | 4 | 5.5 | 7.5 | 9 |
| 75–77 | 1 | 2 | 2.5 | 3 | 4 | 6 | 8 | 9.5 |
Reference limits were developed using kidney biopsies at time of kidney transplant for 1847 carefully screened normotensive kidney donors.9
Challenging this notion that ischemia primarily explains age-related glomerulosclerosis, a study in 89 subjects found evidence that podocyte depletion can also lead to FGGS with aging.10 Older glomeruli showed a decreased density of podocytes due to both increased glomerular volume and a decrease in the number of podocytes per glomerulus. Older glomeruli also showed an increased podocyte detachment rate. A subset of these older glomeruli showed capillary wrinkling, tuft collapse, and periglomerular fibrosis. It is worth noting that this study sample was composed of living kidney donors, deceased kidney donors, and patients who had a radical nephrectomy for cancer.10 As discussed in the next section, an increase in glomerular volume is not seen in studies limited to living kidney donors. This highlights the importance of distinguishing the structural findings in healthy aging from the structural findings in aging with expected comorbidity (Figure 1).
Nephron Hypertrophy
Much has been written about how glomeruli hypertrophy in a variety of conditions, including obesity, diabetes, and surgical- or disease-related reductions in nephron mass.11–13 Actually, in these states, the entire nephron hypertrophies, but glomerulomegaly is just much more recognizable than the accompanying enlargement of tubules on a renal biopsy section.14 Because glomeruli only make up about 4% of the volume of the kidney cortex,15 it is enlargement of the tubules that leads to enlarged kidneys with comorbidities, such as obesity and diabetes.14,16 Because comorbidities become more prevalent with aging, glomerular enlargement with aging is usually seen in studies of deceased patients.17–19 However, studies limited to healthy living kidney donors have not found an increase in glomerular volume with aging.15,20,21
Other than glomerular volume, the total size of the nephron can be assessed a couple of other ways on kidney biopsy. One method is to average the profile (cross-sectional) area of tubules across a large region of the biopsy section to decrease error from the different orientations of tubules. Another method is on the basis of the principle that, as contiguous particles enlarge, their density decreases. Specifically, as nephrons hypertrophy, they disperse the glomeruli farther apart, increasing the volume (and cross-sectional area) of cortex per glomerulus. Thus, nephron size can be estimated by the average amount of cortex per glomerulus (more reasonably done in settings where there is minimal interstitial infiltrate or fibrosis). Both larger profile tubular area and larger cortex per glomerulus correlate with larger glomerular volume in a variety of populations.11,22,23 Although glomerular enlargement does not occur with healthy aging, hypertrophy of the tubules does occur. In living kidney donors, both profile tubular area and cortex area per glomerulus enlarge with aging.20 Nephrosclerosis is a volume-losing lesion (in particular, glomerulosclerosis and tubular atrophy) that brings nonsclerosed glomeruli closer together with aging. However, in regions where there is less nephrosclerosis, glomeruli are pushed farther apart with aging from hypertrophy of the remaining tubules.24
Nephron Number
It is well known from kidneys examined as autopsy specimens that nephron number decreases with aging.25,26 The rate of nephron loss per kidney has been estimated at about 6800 nephrons per kidney per year on the basis of autopsy series.17 A study in living kidney donors found that the rate of nephron loss was slightly less among healthy persons at 6200 nephrons per kidney per year.15 The mean number of nephrons (nonsclerosed glomeruli) per kidney decreased from 990,000 in 18–29 year olds to 520,000 in 70–75 year olds. Importantly, the loss of nephrons with aging was not fully accounted for by the increase in glomerulosclerosis with aging. Less than one third of the missing nephrons could be accounted for by the presence of globally sclerotic glomeruli. Complete loss of glomeruli with aging has long been suspected; Hayman et al.27 described in 1939 that “scars of destroyed glomeruli disappear without leaving recognizable traces.” Whether these lost glomeruli are fully reabsorbed or have simply atrophied to the point that they are not easily detected on a biopsy section is not fully clear. Regardless, detectable glomerulosclerosis on renal biopsy substantially under-represents the true loss of nephrons with aging.
Single-Nephron GFR
The mean single-nephron GFR (snGFR) can be estimated in kidney donors by dividing measured GFR (iothalamate clearance) by the number of nephrons in both kidneys.28 The snGFR in healthy adults is relatively stable across physiologic variation in sex and height. However, snGFR is increased with some CKD risk factors (obesity and family history of ESRD), and this seems to occur via larger nephron size on renal biopsy. Is aging associated with a stable snGFR (consistent with physiologic characteristics) or a higher snGFR (consistent with CKD risk factors)? It appears that snGFR is stable with healthy aging, despite the substantial loss of nephrons (over the age of 70 years old, this is less clear due to selection bias in the few allowed to donate). Nephrosclerosis on renal biopsy does associate with an increase in snGFR but only when nephrosclerosis exceeds that expected for age. Consistent with this finding, the single-nephron glomerular filtration capacity as determined from electron microscopy of glomeruli in living kidney donors also does not increase with age.21 Why glomeruli do not compensate for age-related nephron loss with larger size, higher single-nephron glomerular filtration capacity, and higher snGFR is not fully understood. Older glomeruli are capable of higher snGFR in the presence of CKD risk factors.28 There may be less metabolic demand for glomerular function with aging,29 possibly related to sarcopenia and decreased protein intake. Indexing GFR to metabolic rate instead of body surface area substantially attenuates the decline in GFR with age.30
Influence of Nephron Endowment on Renal Aging
It is well known that the number of nephrons present at birth is highly variable and that nephrogenesis is virtually complete at the end of gestation.31 Low birth weight is a good indicator of low nephron endowment.32 Compensation for low nephron endowment occurs in utero or shortly after birth, such that whole-kidney GFR is normal but at the expense of an increase in snGFR with glomerular enlargement. Indeed, lower nephron number with a family history of ESRD is associated with a compensatory increase in snGFR28 and larger glomeruli.20 Because of nephron loss with aging, those individuals with low nephron number at birth are expected to reach critical levels of nephropenia with pathophysiologic maladaptation at an earlier age. This may explain why low birth weight is a risk factor for CKD and ESRD.33
Relationship of Microstructure to Macrostructure with Aging
Detection of this mild but progressive nephrosclerosis with aging is difficult without a kidney biopsy. Nonetheless, nephrosclerosis leads to macrostructural findings on imaging studies, including a decrease in cortical volume, an even stronger decrease in the cortex-to-medulla volume ratio, an increase in the kidney surface roughness, and it may also contribute to parenchymal cysts.20 Glomerulosclerosis with aging seems to preferentially affect the more superficial nephrons for unclear reasons, although the deeper juxtamedullary nephrons hypertrophy to compensate.34 The increase in medullary volume (composed of the loops from juxtamedullary nephrons) with aging is also consistent with this compensation.2 Diverticula of renal tubules also become more frequent with aging,35 and these diverticula are likely the precursor lesion for age-related renal cysts.36
The age-related loss of cortical volume from nephrosclerosis is masked to some extent, by the age-related tubular hypertrophy.20 Because of this, cortical volume is a poor surrogate for nephron number. Between the ages of 18–29 and 70–75 years old, the mean number of nephrons decreases by 48%, whereas the cortical volume only decreases by 16%.15 Because medullary volume increases until about age 50 years old,2 total kidney volume is an even worse surrogate for nephron loss with aging than cortical volume.
Functional Changes with Aging
GFR Decline
GFR, approximated by urinary creatinine clearance, declined at about 0.75 ml/min per year in a longitudinal study of relatively normal men.37 This decline in GFR with aging remains evident, even in living kidney donors who are carefully evaluated for good health.38 Even in isolated indigenous populations with low rates of cardiovascular disease, a similar decline in GFR with aging is evident.39
The GFR correlates with cortical volume (or kidney volume).1,2 Thus, it is worth assessing whether GFR associates with the underlying structural determinants of cortical volume: nephrosclerosis, nephron size, and nephron number. Larger nephrons associate with higher snGFR, which leads to a higher GFR.28 Lower nephron number directly leads to lower GFR.15,20 Interestingly, nephrosclerosis and specifically, glomerulosclerosis do not have an age-independent association with GFR.6,20 This is explained by nephron loss from age-related nephrosclerosis leading to a proportional decline in GFR.15 However, nephron loss from nephrosclerosis beyond that expected for age associates with a compensatory increase in snGFR, such that GFR is at the level expected for age.28 Unlike GFR, urine albumin excretion does not change with healthy aging.6
Prevalence of CKD in the Elderly
The prevalence of CKD as currently defined by an eGFR<60 ml/min per 1.73 m2 or albuminuria (urine albumin-to-creatinine ratio >30 mg/g) persisting for 3 months or more is reportedly 13% of the United States adult population.40 However, the prevalence by these criteria markedly increases with age from 4% for adults ages 20–39 years old to 47% for adults ages 70 years old and older. This remarkable increase in the prevalence of criteria-defined CKD in elderly adults is due more to an eGFR decline than to increasing albuminuria. In young adults, 75% of such CKD is due to albuminuria, and 25% is due to eGFR<60 ml/min per 1.73 m2. Conversely, in older adults, 19% of such CKD is due to albuminuria, and 81% is due to eGFR<60 ml/min per 1.73 m2.40 Among most elderly adults with CKD, the rate of eGFR decline remains fairly slow, unless the eGFR is <30 ml/min per 1.73 m2.41 Thus, a fixed threshold of <60 ml/min per 1.73 m2, in the absence of abnormal albuminuria, may not be appropriate for defining CKD in the elderly. Indeed, the average measured GFR for a representative cohort of community-living adults >70 years of age is approximately 60 ml/min per 1.73 m2.42 Therefore, by criteria-based definitions, 50% of persons over age 70 years old might be labeled as having CKD; a substantial number of the elderly likely have only physiologic aging of the kidneys (Figure 1), which is not a disease per se.
Mortality and Kidney Failure Risk with Age-Related Reductions in GFR
The CKD prognosis consortium assessed the risk of mortality by GFR and urine albumin across different age categories among over 2 million adults in 46 diverse cohort studies.43 One way of viewing the CKD prognosis consortium data is to identify the range of GFR associated with the lowest risk of mortality in the absence of abnormal albuminuria. By this approach, the lowest risk of mortality for ages 18–54 years old is with a GFR of 75 ml/min per 1.73 m2 and higher, but the lowest risk of mortality for ages >75 years old is with a GFR of 45–104 ml/min per 1.73 m2.44
An important development in the management of CKD has been the Kidney Failure Risk Equation validated in 31 different cohorts.45,46 This tool estimates the risk of kidney failure in the next 2 or 5 years on the basis of the patient age, sex, eGFR, urine albumin-to-creatinine ratio, and if available, serum calcium, phosphorous, bicarbonate, and albumin. Applying this tool in older patients can be very reassuring in many older patients with a criteria-based label of CKD. For example, a 65-year-old woman with an eGFR of 50 ml/min per 1.73 m2 and a urine albumin-to-creatinine ratio of 5 mg/g has a 0.1% risk of kidney failure in 2 years and a 0.3% risk in 5 years. It is worth noting that, with the Kidney Failure Risk Equation and other similar models,47,48 older patients have a much lower risk of progression to ESRD compared with younger patients with the same eGFR. A population-based study found that, among persons with an eGFR of 30–59 ml/min per 1.73 m2, the incidence of kidney failure was 3.0 per 100 person-years for elderly (age >65 years old) with proteinuria, 0.7 per 100 person-years for younger adults without proteinuria, and undetectably low for elderly without proteinuria.49
Conclusions and Perspectives
Because healthy aging is associated with structural changes in the kidney and a decrease in GFR without a substantive increase in the risk of ESRD or mortality, age-based modifications to the definition of CKD have been proposed. One definition includes a GFR<75 ml/min per 1.73 m2 in younger adults (age <40 years old)50 and a GFR<45 ml/min per 1.73 m2 in older adults (age >65 years old).51 More granular age–based thresholds on the basis of the 2.5th percentile of a reference population have also been developed to identify patients who have a GFR less than expected for their age.52,53
Beyond modifying the current disease labeling of older adults with merely physiologic kidney aging, specific management strategies that are of actual benefit to older patients with reduced GFR warrant attention. It is generally accepted that water-soluble, renally cleared medications should be dosed on the basis of the patient’s GFR (not indexed to body surface area). Nephrotoxic medications, such as nonsteroidal anti-inflammatory drug and iodinated radiocontrast, should be avoided, whenever possible, in patients with reduced GFR, regardless of the cause. Clinical trials of angiotensin blockers in younger adults with proteinuric CKD have been shown to cause a 30% reduction in the relative risk of ESRD. However, a simulation study in patients older than age 70 years old found that a GFR of 45–59 ml/min per 1.73 m2 without proteinuria had an estimated number needed to treat of 2500 to prevent ESRD in one patient.54 Thus, caution is warranted in applying standard CKD treatments, such as angiotensin blockers, to a physiologic decline in GFR.
Disclosures
None.
Acknowledgments
This work was supported with funding from National Institutes of Health, National Institute of Diabetes and Digestive and Kidney Diseases grant R01 DK090358.
Footnotes
Published online ahead of print. Publication date available at www.jasn.org.
References
- 1.Roseman DA, Hwang SJ, Oyama-Manabe N, Chuang ML, O’Donnell CJ, Manning WJ, Fox CS: Clinical associations of total kidney volume: The Framingham Heart Study. Nephrol Dial Transplant 32: 1344–1350, 2017 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Wang X, Vrtiska TJ, Avula RT, Walters LR, Chakkera HA, Kremers WK, Lerman LO, Rule AD: Age, kidney function, and risk factors associate differently with cortical and medullary volumes of the kidney. Kidney Int 85: 677–685, 2014 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Rule AD, Sasiwimonphan K, Lieske JC, Keddis MT, Torres VE, Vrtiska TJ: Characteristics of renal cystic and solid lesions based on contrast-enhanced computed tomography of potential kidney donors. Am J Kidney Dis 59: 611–618, 2012 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Robbins SL, Kumar V, Cotran RS: Robbins and Cotran Pathologic Basis of Disease, 8th Ed., Philadelphia, Saunders/Elsevier, 2010, pp xiv [Google Scholar]
- 5.Hughson MD, Puelles VG, Hoy WE, Douglas-Denton RN, Mott SA, Bertram JF: Hypertension, glomerular hypertrophy and nephrosclerosis: The effect of race. Nephrol Dial Transplant 29: 1399–1409, 2014 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Rule AD, Amer H, Cornell LD, Taler SJ, Cosio FG, Kremers WK, Textor SC, Stegall MD: The association between age and nephrosclerosis on renal biopsy among healthy adults. Ann Intern Med 152: 561–567, 2010 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Sethi S, D’Agati VD, Nast CC, Fogo AB, De Vriese AS, Markowitz GS, Glassock RJ, Fervenza FC, Seshan SV, Rule A, Racusen LC, Radhakrishnan J, Winearls CG, Appel GB, Bajema IM, Chang A, Colvin RB, Cook HT, Hariharan S, Herrera Hernandez LP, Kambham N, Mengel M, Nath KA, Rennke HG, Ronco P, Rovin BH, Haas M: A proposal for standardized grading of chronic changes in native kidney biopsy specimens. Kidney Int 91: 787–789, 2017 [DOI] [PubMed] [Google Scholar]
- 8.Kaplan C, Pasternack B, Shah H, Gallo G: Age-related incidence of sclerotic glomeruli in human kidneys. Am J Pathol 80: 227–234, 1975 [PMC free article] [PubMed] [Google Scholar]
- 9.Kremers WK, Denic A, Lieske JC, Alexander MP, Kaushik V, Elsherbiny HE, Chakkera HA, Poggio ED, Rule AD: Distinguishing age-related from disease-related glomerulosclerosis on kidney biopsy: The Aging Kidney Anatomy study. Nephrol Dial Transplant 30: 2034–2039, 2015 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Hodgin JB, Bitzer M, Wickman L, Afshinnia F, Wang SQ, O’Connor C, Yang Y, Meadowbrooke C, Chowdhury M, Kikuchi M, Wiggins JE, Wiggins RC: Glomerular aging and focal global glomerulosclerosis: A podometric perspective. J Am Soc Nephrol 26: 3162–3178, 2015 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Tsuboi N, Koike K, Hirano K, Utsunomiya Y, Kawamura T, Hosoya T: Clinical features and long-term renal outcomes of Japanese patients with obesity-related glomerulopathy. Clin Exp Nephrol 17: 379–385, 2013 [DOI] [PubMed] [Google Scholar]
- 12.Tsuboi N, Utsunomiya Y, Hosoya T: Obesity-related glomerulopathy and the nephron complement. Nephrol Dial Transplant 28[Suppl 4]: iv108–iv113, 2013 [DOI] [PubMed] [Google Scholar]
- 13.Tsuboi N, Utsunomiya Y, Kanzaki G, Koike K, Ikegami M, Kawamura T, Hosoya T: Low glomerular density with glomerulomegaly in obesity-related glomerulopathy. Clin J Am Soc Nephrol 7: 735–741, 2012 [DOI] [PubMed] [Google Scholar]
- 14.Thomson SC, Vallon V, Blantz RC: Kidney function in early diabetes: The tubular hypothesis of glomerular filtration. Am J Physiol Renal Physiol 286: F8–F15, 2004 [DOI] [PubMed] [Google Scholar]
- 15.Denic A, Lieske JC, Chakkera HA, Poggio ED, Alexander MP, Singh P, Kremers WK, Lerman LO, Rule AD: The substantial loss of nephrons in healthy human kidneys with aging. J Am Soc Nephrol 28: 313–320, 2017 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Hayslett JP, Kashgarian M, Epstein FH: Functional correlates of compensatory renal hypertrophy. J Clin Invest 47: 774–799, 1968 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Hoy WE, Douglas-Denton RN, Hughson MD, Cass A, Johnson K, Bertram JF: A stereological study of glomerular number and volume: Preliminary findings in a multiracial study of kidneys at autopsy. Kidney Int Suppl 83: S31–S37, 2003 [DOI] [PubMed] [Google Scholar]
- 18.Fulladosa X, Moreso F, Narváez JA, Grinyó JM, Serón D: Estimation of total glomerular number in stable renal transplants. J Am Soc Nephrol 14: 2662–2668, 2003 [DOI] [PubMed] [Google Scholar]
- 19.Abdi R, Slakey D, Kittur D, Racusen LC: Heterogeneity of glomerular size in normal donor kidneys: Impact of race. Am J Kidney Dis 32: 43–46, 1998 [DOI] [PubMed] [Google Scholar]
- 20.Denic A, Alexander MP, Kaushik V, Lerman LO, Lieske JC, Stegall MD, Larson JJ, Kremers WK, Vrtiska TJ, Chakkera HA, Poggio ED, Rule AD: Detection and clinical patterns of nephron hypertrophy and nephrosclerosis among apparently healthy adults. Am J Kidney Dis 68: 58–67, 2016 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Tan JC, Busque S, Workeneh B, Ho B, Derby G, Blouch KL, Sommer FG, Edwards B, Myers BD: Effects of aging on glomerular function and number in living kidney donors. Kidney Int 78: 686–692, 2010 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Elsherbiny HE, Alexander MP, Kremers WK, Park WD, Poggio ED, Prieto M, Lieske JC, Rule AD: Nephron hypertrophy and glomerulosclerosis and their association with kidney function and risk factors among living kidney donors. Clin J Am Soc Nephrol 9: 1892–1902, 2014 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Koike K, Tsuboi N, Utsunomiya Y, Kawamura T, Hosoya T: Glomerular density-associated changes in clinicopathological features of minimal change nephrotic syndrome in adults. Am J Nephrol 34: 542–548, 2011 [DOI] [PubMed] [Google Scholar]
- 24.Rule AD, Semret MH, Amer H, Cornell LD, Taler SJ, Lieske JC, Melton LJ 3rd, Stegall MD, Textor SC, Kremers WK, Lerman LO: Association of kidney function and metabolic risk factors with density of glomeruli on renal biopsy samples from living donors. Mayo Clin Proc 86: 282–290, 2011 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.McNamara BJ, Diouf B, Douglas-Denton RN, Hughson MD, Hoy WE, Bertram JF: A comparison of nephron number, glomerular volume and kidney weight in Senegalese Africans and African Americans. Nephrol Dial Transplant 25: 1514–1520, 2010 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Hoy WE, Ingelfinger JR, Hallan S, Hughson MD, Mott SA, Bertram JF: The early development of the kidney and implications for future health. J Dev Orig Health Dis 1: 216–233, 2010 [DOI] [PubMed] [Google Scholar]
- 27.Hayman JM Jr, Martin JW Jr, Miller M: Renal function and the number of glomeruli in the human kidney Arch Intern Med 64: 69–83, 1939 [Google Scholar]
- 28.Denic A, Mathew J, Lerman LO, Lieske JC, Larson JJ, Alexander MP, Poggio E, Glassock RJ, Rule AD: Single nephron glomerular filtration rate in healthy adults. N Engl J Med 376: 2349–2357, 2017 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Nyengaard JR, Bendtsen TF: Glomerular number and size in relation to age, kidney weight, and body surface in normal man. Anat Rec 232: 194–201, 1992 [DOI] [PubMed] [Google Scholar]
- 30.Daugirdas JT, Meyer K, Greene T, Butler RS, Poggio ED: Scaling of measured glomerular filtration rate in kidney donor candidates by anthropometric estimates of body surface area, body water, metabolic rate, or liver size. Clin J Am Soc Nephrol 4: 1575–1583, 2009 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Luyckx VA, Perico N, Somaschini M, Manfellotto D, Valensise H, Cetin I, Simeoni U, Allegaert K, Vikse BE, Steegers EA, Adu D, Montini G, Remuzzi G, Brenner BM; Writing Group of the Low Birth Weight and Nephron Number Working Group : A developmental approach to the revention of hypertension and kidney disease: A report from the Low Birth Weight and Nephron Number Working Group [published online ahead of print March 9, 2017]. Lancet doi: 10.1016/S0140-6736(17)30576-7 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Luyckx VA, Brenner BM: Birth weight, malnutrition and kidney-associated outcomes--a global concern. Nat Rev Nephrol 11: 135–149, 2015 [DOI] [PubMed] [Google Scholar]
- 33.White SL, Perkovic V, Cass A, Chang CL, Poulter NR, Spector T, Haysom L, Craig JC, Salmi IA, Chadban SJ, Huxley RR: Is low birth weight an antecedent of CKD in later life? A systematic review of observational studies. Am J Kidney Dis 54: 248–261, 2009 [DOI] [PubMed] [Google Scholar]
- 34.Newbold KM, Sandison A, Howie AJ: Comparison of size of juxtamedullary and outer cortical glomeruli in normal adult kidney. Virchows Arch A Pathol Anat Histopathol 420: 127–129, 1992 [DOI] [PubMed] [Google Scholar]
- 35.Darmady EM, Offer J, Woodhouse MA: The parameters of the ageing kidney. J Pathol 109: 195–207, 1973 [DOI] [PubMed] [Google Scholar]
- 36.Baert L, Steg A: Is the diverticulum of the distal and collecting tubules a preliminary stage of the simple cyst in the adult? J Urol 118: 707–710, 1977 [DOI] [PubMed] [Google Scholar]
- 37.Lindeman RD, Tobin J, Shock NW: Longitudinal studies on the rate of decline in renal function with age. J Am Geriatr Soc 33: 278–285, 1985 [DOI] [PubMed] [Google Scholar]
- 38.Poggio ED, Rule AD, Tanchanco R, Arrigain S, Butler RS, Srinivas T, Stephany BR, Meyer KH, Nurko S, Fatica RA, Shoskes DA, Krishnamurthi V, Goldfarb DA, Gill I, Schreiber MJ Jr: Demographic and clinical characteristics associated with glomerular filtration rates in living kidney donors. Kidney Int 75: 1079–1087, 2009 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Hollenberg NK, Rivera A, Meinking T, Martinez G, McCullough M, Passan D, Preston M, Taplin D, Vicaria-Clement M: Age, renal perfusion and function in island-dwelling indigenous Kuna Amerinds of Panama. Nephron 82: 131–138, 1999 [DOI] [PubMed] [Google Scholar]
- 40.Coresh J, Selvin E, Stevens LA, Manzi J, Kusek JW, Eggers P, Van Lente F, Levey AS: Prevalence of chronic kidney disease in the United States. JAMA 298: 2038–2047, 2007 [DOI] [PubMed] [Google Scholar]
- 41.Hemmelgarn BR, Zhang J, Manns BJ, Tonelli M, Larsen E, Ghali WA, Southern DA, McLaughlin K, Mortis G, Culleton BF: Progression of kidney dysfunction in the community-dwelling elderly. Kidney Int 69: 2155–2161, 2006 [DOI] [PubMed] [Google Scholar]
- 42.Ebert N, Jakob O, Gaedeke J, van der Giet M, Kuhlmann MK, Martus P, Mielke N, Schuchardt M, Tolle M, Wenning V, Schaeffner ES: Prevalence of reduced kidney function and albuminuria in older adults: The Berlin Initiative Study. Nephrol Dial Transplant 32: 997–1005, 2017 [DOI] [PubMed] [Google Scholar]
- 43.Hallan SI, Matsushita K, Sang Y, Mahmoodi BK, Black C, Ishani A, Kleefstra N, Naimark D, Roderick P, Tonelli M, Wetzels JF, Astor BC, Gansevoort RT, Levin A, Wen CP, Coresh J; Chronic Kidney Disease Prognosis Consortium : Age and association of kidney measures with mortality and end-stage renal disease. JAMA 308: 2349–2360, 2012 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.Denic A, Glassock RJ, Rule AD: Structural and functional changes with the aging kidney. Adv Chronic Kidney Dis 23: 19–28, 2016 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45.Tangri N, Grams ME, Levey AS, Coresh J, Appel LJ, Astor BC, Chodick G, Collins AJ, Djurdjev O, Elley CR, Evans M, Garg AX, Hallan SI, Inker LA, Ito S, Jee SH, Kovesdy CP, Kronenberg F, Heerspink HJ, Marks A, Nadkarni GN, Navaneethan SD, Nelson RG, Titze S, Sarnak MJ, Stengel B, Woodward M, Iseki K; CKD Prognosis Consortium : Multinational assessment of accuracy of equations for predicting risk of kidney failure: A meta-analysis. JAMA 315: 164–174, 2016 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46.Tangri N, Stevens LA, Griffith J, Tighiouart H, Djurdjev O, Naimark D, Levin A, Levey AS: A predictive model for progression of chronic kidney disease to kidney failure. JAMA 305: 1553–1559, 2011 [DOI] [PubMed] [Google Scholar]
- 47.Grams ME, Li L, Greene TH, Tin A, Sang Y, Kao WH, Lipkowitz MS, Wright JT, Chang AR, Astor BC, Appel LJ: Estimating time to ESRD using kidney failure risk equations: Results from the African American Study of Kidney Disease and Hypertension (AASK). Am J Kidney Dis 65: 394–402, 2015 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 48.Echouffo-Tcheugui JB, Kengne AP: Risk models to predict chronic kidney disease and its progression: A systematic review. PLoS Med 9: e1001344, 2012 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 49.Obi Y, Kimura T, Nagasawa Y, Yamamoto R, Yasuda K, Sasaki K, Kitamura H, Imai E, Rakugi H, Isaka Y, Hayashi T: Impact of age and overt proteinuria on outcomes of stage 3 to 5 chronic kidney disease in a referred cohort. Clin J Am Soc Nephrol 5: 1558–1565, 2010 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 50.Pottel H, Hoste L, Delanaye P: Abnormal glomerular filtration rate in children, adolescents and young adults starts below 75 mL/min/1.73 m2. Pediatr Nephrol 30: 821–828, 2015 [DOI] [PubMed] [Google Scholar]
- 51.Glassock R, Delanaye P, El Nahas M: An age-calibrated classification of chronic kidney disease. JAMA 314: 559–560, 2015 [DOI] [PubMed] [Google Scholar]
- 52.van den Brand JA, van Boekel GA, Willems HL, Kiemeney LA, den Heijer M, Wetzels JF: Introduction of the CKD-EPI equation to estimate glomerular filtration rate in a Caucasian population. Nephrol Dial Transplant 26: 3176–3181, 2011 [DOI] [PubMed] [Google Scholar]
- 53.Benghanem Gharbi M, Elseviers M, Zamd M, Belghiti Alaoui A, Benahadi N, Trabelssi el H, Bayahia R, Ramdani B, De Broe ME: Chronic kidney disease, hypertension, diabetes, and obesity in the adult population of Morocco: how to avoid “over”- and “under”-diagnosis of CKD. Kidney Int 89: 1363–1371, 2016 [DOI] [PubMed] [Google Scholar]
- 54.O’Hare AM, Hotchkiss JR, Kurella Tamura M, Larson EB, Hemmelgarn BR, Batten A, Do TP, Covinsky KE: Interpreting treatment effects from clinical trials in the context of real-world risk information: End-stage renal disease prevention in older adults. JAMA Intern Med 174: 391–397, 2014 [DOI] [PMC free article] [PubMed] [Google Scholar]