

Abstract
Background:
Psoriasis is a chronic inflammatory disease of the skin that may affect the visible areas of body. Hence, the quality of life, self-esteem, and body image can be affected in psoriasis patients.
Objectives:
We aimed in the present study to assess the effects of psoriasis on the quality of life, self-esteem, and body image.
Materials and Methods:
The study included 92 patients with psoriasis, along with 98 control participants. The sociodemographic characteristics of the patients were assessed, their Psoriasis Area Severity Index (PASI) scores were calculated to determine the clinical severity of the psoriasis, and the values were recorded. In addition, Dermatology Life Quality Index (DLQI), Body Image Scale, and Rosenberg Self-Esteem Scale results were evaluated.
Results:
When the control and psoriasis groups were evaluated regarding the DLQI, self-esteem, and body image, quality of life was found to be more negatively affected in the psoriasis group than the controls, which was statistically significant (P < 0.001), and self-esteem (P < 0.001) and body image (P < 0.001) were found to be significantly lower. Educational status significantly affected self-esteem (P < 0.001) and body image (P = 0.021), however, quality of life was not significantly affected by this parameter (P = 0.345). PASI was positively correlated with the quality of life (r = 0.703) and self-esteem (r = 0.448), however, it was negatively correlated with the body image (r = −0.423).
Conclusions:
Psoriasis may negatively affect quality of life, self-esteem, and body image, and may also cause psychosocial problems. An assessment of new approaches on this issue may contribute to developments in the treatment of and rehabilitation from this disease.
Keywords: Body image, Psoriasis Area Severity Index, psoriasis, quality of life, self-esteem
Introduction
Psoriasis is a chronic inflammatory skin disease and may affect the visible areas of the body.[1] Therefore, patients are struggling with the disease during their daily activities and face various psychosocial problems. Self-esteem (SE) describes the belief and confidence in one's own worth, strengths, efficacy, and success; it is a subjective state of feeling formed by the individual's realistic evaluation of himself or herself.[2] Body image (BI) is a concept that includes the individual's subjective perceptions formed by his/her conscious or unconscious feelings and beliefs related with his/her own body; it changes throughout the person's life.
The aim of this study is to assess the effects of psoriasis on the quality of life, SE, and BI.
Materials and Methods
The study comprised 92 patients who were at least 18 years old and were diagnosed with plaque psoriasis either clinically or histopathologically; age, gender, and educational status-matched 98 healthy individuals served as control cases. The study was cross-sectional and consent of the ethics committee was obtained. The patients who could not read or write, who had an additional systemic or psychiatric disease, body mass index of ≥30 kg/m2, were pregnant, and who declined to complete the questionnaire were excluded. The control group was selected from healthy volunteers. The educational status of the contributors was classified as elementary school, secondary school, high-school, and university. Those who graduated from elementary and secondary schools were classified as having a low educational status, whereas those graduated from high-school and university were classified as having a high educational status. Psoriasis Area Severity Index (PASI) scores were interpreted; ≤5 mild psoriasis, 6–9 moderate psoriasis, and ≥10 severe psoriasis.
Dermatology Life Quality Index (DLQI) is a specific scale for dermatology and is composed of 10 questions. The lowest score for each question is 0 and the highest is 3. The meaning of DLQI scores were interpreted as 0–1, no effect at all on patient's life; 2–5, mild effect on patient's life; 6–10, moderate effect on patient's life; 11–20, considerable effect on patient's life; and 21–30, very severe effect on patient's life. A high score indicates an impaired quality of life. Its Turkish version was formulated by Öztürkcan et al.[3]
BI scale's validity and reliability studies were conducted by Hovardaoğlu in Turkey.[4] The lowest score that can be received is 40 and the highest is 200; a high score indicates an increase in the positive evaluation. Cases with scale scores below 135 are defined in the group with low BI, and those with scores ≥135 are defined in the group of high BI.
Rosenberg's Self-Esteem Scale's validity and reliability studies in Turkish were conducted by Çuhadaroğlu.[5] Considering the aim of the study, the first 10 statements on the scale were used to evaluate SE. Each item was answered on a 4-point scale, as follows: strongly agree, agree, disagree, and strongly disagree. According to the evaluation guide of the scale; 0–1 is high, 2–4 is moderate, and 5–6 is low.
Statistical analysis
Data were statistically evaluated using the Statistical Package for the Social Sciences version 17.0 software (SPSS Inc, Chicago, Illinois, USA). Continuous data were expressed as mean and standard deviation, and categorical data were expressed as the frequency and percentage. A student's t-test was used for comparing continuous variables between the independent groups. Two independent categorical groups were compared using the Chi-square. The mean values were compared between groups using the analysis of variance (ANOVA) test, and correlations were determined using the Pearson's correlation analysis. P value of <0.05 was accepted to be significant.
Results
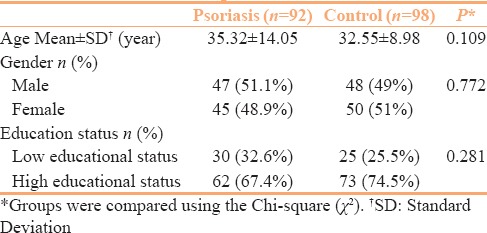
The mean ages of cases in the control and psoriasis groups were 32.55 ± 8.98 years and 35.32 ± 14.05 years, respectively. When groups were evaluated regarding the gender, 48 cases were males (49%) and 50 cases were females (51%) in the control group, whereas 47 cases were males (51.1%) and 45 cases were females (48.9%) in the psoriasis group. No statistically significant differences were determined between the groups regarding age and gender (P values of 0.109 and 0.772, respectively). Patients’ characteristics are presented in Table 1.
Table 1.
Participants characteristics
DLQI, SE, and BI data of the groups are presented in Table 2.
Table 2.
DLQI, self-esteem, and body image data of the groups

SE and BI were compared with regard to the status of education, and the group with a high level of education had significantly higher SE and BI evaluations compared with the group with low educational level (level of education-SE P = 0.000; level of education-BI P = 0.021). When quality of life was compared regarding educational levels, life quality was more widely affected in the group with low levels of education compared with the group with high educational levels; however, this difference was not significant statistically (P = 0.345).
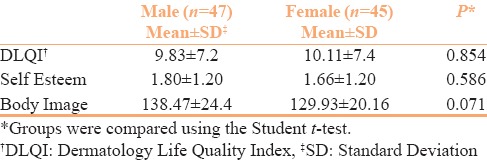
DLQI, SE, and BI differences between males and females in patients with psoriasis are presented in Table 3.
Table 3.
DLQI, self-esteem, and body image differences between males and females in patients with psoriasis
When quality of life was evaluated in relation to the PASI, life quality was moderately affected in the group with mild disease, however, life quality was widely affected in the groups with moderate and severe levels of disease. When the DLQI was compared regarding the PASI, life quality in the group with a lower PASI level was significantly better compared to cases existing with a high level (P < 0.001). When SE and BI were evaluated regarding the PASI values, SE and BI in the group with mild disease were found to be significantly higher compared to the groups with moderate and severe diseases (P < 0.001).
The correlations between PASI and quality of life, SE, and BI are presented in Table 4.
Table 4.
The correlations between PASI and quality of life, self-esteem, and body image

Discussion
Psoriasis affects both genders in equal frequencies and it can manifest at any age. The initial signs of the disease exist before the age of 40 years in 70% of the patients and most frequently in the 3rd decade.[6] In this study, similar to the reported literature, gender did not differ in a statistically significant manner in the psoriasis group (P > 0.05). DLQI is one of the most frequently used scales for determining life quality.[7] In a study by Balcı et al., the total score DLQI in the psoriasis group was 9.50 ± 6.10, and it was found to be 0.67 ± 0.80 in the control group.[8] Mazzotti et al. determined a DLQI score of 8.8 ± 6.1 in patients with psoriasis.[9] In the present study, the DLQI score in the group with psoriasis (9.97 ± 7.3) was also found to be significantly higher than that of the control participants (2.46 ± 2.8) (P < 0.001). This result revealed the existence of an inferior quality of life for the patients with psoriasis, compared with the healthy controls.
Psoriasis is an illness that involves both the skin and joints, and thus may negatively affect SE.[10] In the study of Kruger et al., psoriasis was identified as being related to the absence of SE.[11] Another study has reported that the association of poor SE with various psychopathologies such as sexual dysfunction disorders, anxiety, depression, and contemplating suicide occurs at high levels in patients with psoriasis.[12] In this study, being similar with the results in the literature.
Psoriasis affects the appearances of individuals, and thus it may result in changes in their attitudes towards their BI.[13] Khoury et al. investigated the effects of psoriasis on BI, and determined that psoriasis negatively affects both BI and sexuality.[14] BI was also identified to negatively affect individuals with head, neck, or breast cancer, colostomy, and obesity.[15] In the present study, BI was also found to be negatively affected by the patients with psoriasis.
Level of education and quality of life are factors that affect SE and BI. In the study by Üstündağ et al., SE scores were assessed to be higher in the group with a higher level of education (P < 0.05), whereas BI did not differ significantly between the groups (P > 0.05).[13] Kim et al. have also determined that no connection exists between the educational status and quality of life.[16] In this study, SE and BI in the patients with psoriasis were found to be better in the group with a high education levels; however, educational status was not determined to significantly affect the DLQI.
PASI scale is the gold standard used in evaluations for the severity of psoriasis.[17] In the study by Lin et al., the clinical severity of psoriasis was found to affect the quality of life in a negative manner.[18] In studies by Moradi et al. and Norlin et al., moderate correlations were determined between the PASI and DLQI (r = 0.58 and r = 0.51, respectively).[19,20] In the study by Khoury et al., 8 patients with severe to moderate psoriasis (PASI ≥10) were interviewed. Five thematic issues linked to the negative impact of psoriasis on patient body image were identified as body coverage, sexual inhibitions, the influence of social support, reduced exercise activity, and a negative self-image.[14] In the study by Kouris, SE of patients with PASI scores ≥15 was not significantly affected compared with patients whose PASI scores were <15 (P < 0.427).[21]
In the present study, PASI was found to positively correlate with the DLQI and SE, and a negative correlation was determined between the PASI and BI. Although duration of illness, the socioeconomic status, and annual family income are very important on patients’ life, they were not taken into account. Hence, these are accepted as a limitation of our study.
Conclusion
Psoriasis may affect the quality of life, SE, and BI in a negative manner, and may cause psychosocial problems. Novel approaches on this issue may contribute to thedevelopments being made in the treatment of and rehabilitation from this disease.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- 1.Nestle FO, Kaplan DH, Barker J. Psoriasis. N Engl J Med. 2009;361:496–509. doi: 10.1056/NEJMra0804595. [DOI] [PubMed] [Google Scholar]
- 2.Ho J, Lee A, Kaminsky L, Wirrell E. Self-concept, attitude toward illness and family functioning in adolescents with type 1 diabetes. Paediatr Child Health. 2008;13:600–4. doi: 10.1093/pch/13.7.600. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Oztürkcan S, Ermertcan AT, Eser E, Sahin MT. Cross validation of the Turkish version of dermatology life quality index. Int J Dermatol. 2006;45:1300–7. doi: 10.1111/j.1365-4632.2006.02881.x. [DOI] [PubMed] [Google Scholar]
- 4.Hovardaoğlu S. Vücut algısı ölçeği. Psikiyatri, Psikoloji, Psikofarmakoloji (3P) Dergisi. 1993;1:26. [Google Scholar]
- 5.Cuhadaroğlu F. Adolesanlarda benlik saygısı. Uzmanlık tezi. Hacettepe Universitesi Tıp Fakültesi, Ankara. 1986 [Google Scholar]
- 6.Gürer MA, Adışen E. Psoriasis, Genel Bilgiler, Epidemiyoloji. Türkderm. 2008;42:15–7. [Google Scholar]
- 7.Finlay AY, Khan GK. Dermatology Life Quality Index (DLQI) - A simple practical measure for routine clinical use. Clin Exp Dermatol. 1994;19:210–6. doi: 10.1111/j.1365-2230.1994.tb01167.x. [DOI] [PubMed] [Google Scholar]
- 8.Balcı DD, İnandı T. Liken Planusta DYKİ. Türkderm. 2008;42:127–30. [Google Scholar]
- 9.Mazzotti E, Barbaranelli C, Picardi A, Abeni D, Pasquini P. Psychometric properties of the Dermatology Life Quality Index (DLQI) in 900 Italian patients with psoriasis. Acta Derm Venereol. 2005;85:409–13. doi: 10.1080/00015550510032832. [DOI] [PubMed] [Google Scholar]
- 10.Dewing KA. Management of patients with psoriatic arthritis. Nurse Pract. 2015;40:40–6. doi: 10.1097/01.NPR.0000461950.23292.18. [DOI] [PubMed] [Google Scholar]
- 11.Krueger G, Koo J, Lebwohl M, Menter A, Stern RS, Rolstad T. The impact of psoriasis on quality of life: Results of a 1998 National Psoriasis Foundation patient-membership survey. Arch Dermatol. 2001;137:280–4. [PubMed] [Google Scholar]
- 12.Russo PA, Ilchef R, Cooper AJ. Psychiatric morbidity in psoriasis: A review. Australas J Dermatol. 2004;45:155–9. doi: 10.1111/j.1440-0960.2004.00078.x. [DOI] [PubMed] [Google Scholar]
- 13.Üstündağ H, Demir N, Zengin N, Gül A. Stomalı Hastalarda Beden İmajı ve Benlik Saygısı. Turkiye Klinikleri J Med Sci. 2007;27:522–7. [Google Scholar]
- 14.Khoury LR, Danielsen PL, Skiveren J. Body image altered by psoriasis. A study based on individual interviews and a model for body image. J Dermatolog Treat. 2014;25:2–7. doi: 10.3109/09546634.2012.739278. [DOI] [PubMed] [Google Scholar]
- 15.Lipowska M, Lipowski M. Narcissism as a moderator of satisfaction with body image in young women with extreme underweight and obesity. PLoS One. 2015;10:e0126724. doi: 10.1371/journal.pone.0126724. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Kim WH, Cho YS, Yoo HM, Park IS, Park EC, Lim JG. Quality of life in Korean patients with inflammatory bowel diseases: Ulcerative colitis, Crohn disease and intestinal Behçet's disease. Int J Colorectal Dis. 1999;14:52–7. doi: 10.1007/s003840050183. [DOI] [PubMed] [Google Scholar]
- 17.Puzenat E, Bronsard V, Prey S, Gourraud PA, Aractingi S, Bagot M, et al. What are the best outcome measures for assessing plaque psoriasis severity? A systematic review of the literature. J Eur Acad Dermatol Venereol. 2010;24:10–6. doi: 10.1111/j.1468-3083.2009.03562.x. [DOI] [PubMed] [Google Scholar]
- 18.Lin TY, See LC, Shen YM, Liang CY, Chang HN, Lin YK. Quality of life in patients with psoriasis in northern Taiwan. Chang Gung Med J. 2011;34:186–96. [PubMed] [Google Scholar]
- 19.Moradi M, Rencz F, Brodszky V, Moradi A, Balogh O, Gulácsi L. Health status and quality of life in patients with psoriasis: An Iranian cross-sectional survey. Arch Iran Med. 2015;18:153–9. [PubMed] [Google Scholar]
- 20.Norlin JM, Steen Carlsson K, Persson U, Schmitt-Egenolf M. Analysis of three outcome measures in moderate to severe psoriasis: A registry based study of 2450 patients. Br J Dermatol. 2012;166:797–802. doi: 10.1111/j.1365-2133.2011.10778.x. [DOI] [PubMed] [Google Scholar]
- 21.Kouris A, Christodoulou C, Stefanaki C, Livaditis M, Tsatovidou R, Kouskoukis C, et al. Quality of life and psychosocial aspects in Greek patients with psoriasis: A cross-sectional study. An Bras Dermatol. 2015;90:841–5. doi: 10.1590/abd1806-4841.20154147. [DOI] [PMC free article] [PubMed] [Google Scholar]