

Abstract
Purpose:
To analyze the current practice patterns of Indian pediatric ophthalmologists in the management of lens anomalies. This study was conducted in a tertiary eye care hospital and involved an online questionnaire survey for practicing pediatric ophthalmologists in India.
Methods:
A questionnaire was devised by the authors, which included the various options available for the management of lens anomalies in children. The questionnaire was sent to each of them using an online portal. Commercial software (Stata ver. 13.1; StataCorp, College Station, TX, USA) was used for statistical analysis.
Results:
In unilateral cataracts in children aged <6 months, 85.42% of surgeons did not prefer to insert an intraocular lens (IOL). In the age group of 6–12 months, almost half of them preferred to insert an IOL. In the age group of 12–24 months and >24 months, 92.63% and 88.54%, respectively, preferred to insert an IOL. In bilateral cataracts, in children aged <6 months, 91.84% of surgeons did not prefer to insert an IOL, whereas in the age group of 6–12 months, 69.39% did not prefer to insert an IOL. In the age group of 12–24 months and >24 months, 80.61% and 90.82%, respectively, preferred to insert an IOL. Seventy-four percent of surgeons preferred to use a single-piece hydrophobic acrylic IOL.
Conclusion:
The management of lens anomalies by pediatric ophthalmologists in India varies with laterality and appears to be comparable to that followed worldwide.
Keywords: Lens disease, online survey, pediatric, practice patterns
The prevalence of childhood cataracts in our country is 0.06% and accounts for 28% of childhood blindness.[1] Cataract surgery is the first step in the long journey of rehabilitation of these children and has improved dramatically in the recent decades. Worldwide, there are hardly any surveys to analyze the preferred practice patterns in the management of childhood cataracts. Those available were conducted in August 1997 and June 2001 by American Association for Pediatric Ophthalmology and Strabismus in the United States and Canada to ascertain perceptions regarding the use of intraocular lens (IOL) implants and contact lenses (CLs) for the correction of aphakia in infants.[2] We conducted an online survey with the aim of analyzing the practice patterns of Indian pediatric ophthalmologists in the management of childhood cataracts and ectopia lentis, which in turn would help us in formulating guidelines and providing education where required.
Methods
Approval for the study was obtained from the institutional review board, and the study was conducted within the Declaration of Helsinki. A close-ended questionnaire [Annexure 1 (237KB, pdf) ] was devised by the authors, which included the type of practice (private practice, trust hospital, medical college, and institution), years of experience (<5 years, 5–10 years, and >10 years), and the various options available for the management of lens anomalies in children. The participants were asked to choose the procedure they preferred to perform in their clinical practice. The e-mail addresses of the practicing pediatric ophthalmologists in India were obtained from the website of the Strabismus and Pediatric Ophthalmology Society of India. The questionnaire was sent to each of them using the SurveyMonkey portal. Statistical analyses were performed using commercial software (Stata ver. 13.1; StataCorp, College Station, TX, USA). All associations were analyzed using the Chi-square test. A P ≤ 0.05 was considered statistically significant.
Results
Of the 520 e-mails sent, 64 (12.3%) were not delivered. Of the 456 e-mails that were delivered, 99 (21.71%) doctors responded. Thirty-one percent of surgeons were in private practice, 19% in trust hospitals, 12% in medical colleges, and 37% in institutional practice. Thirty-seven percent had <5 years of experience, 26% had between 5 and 10 years of experience, and 36% had >10 years of experience.
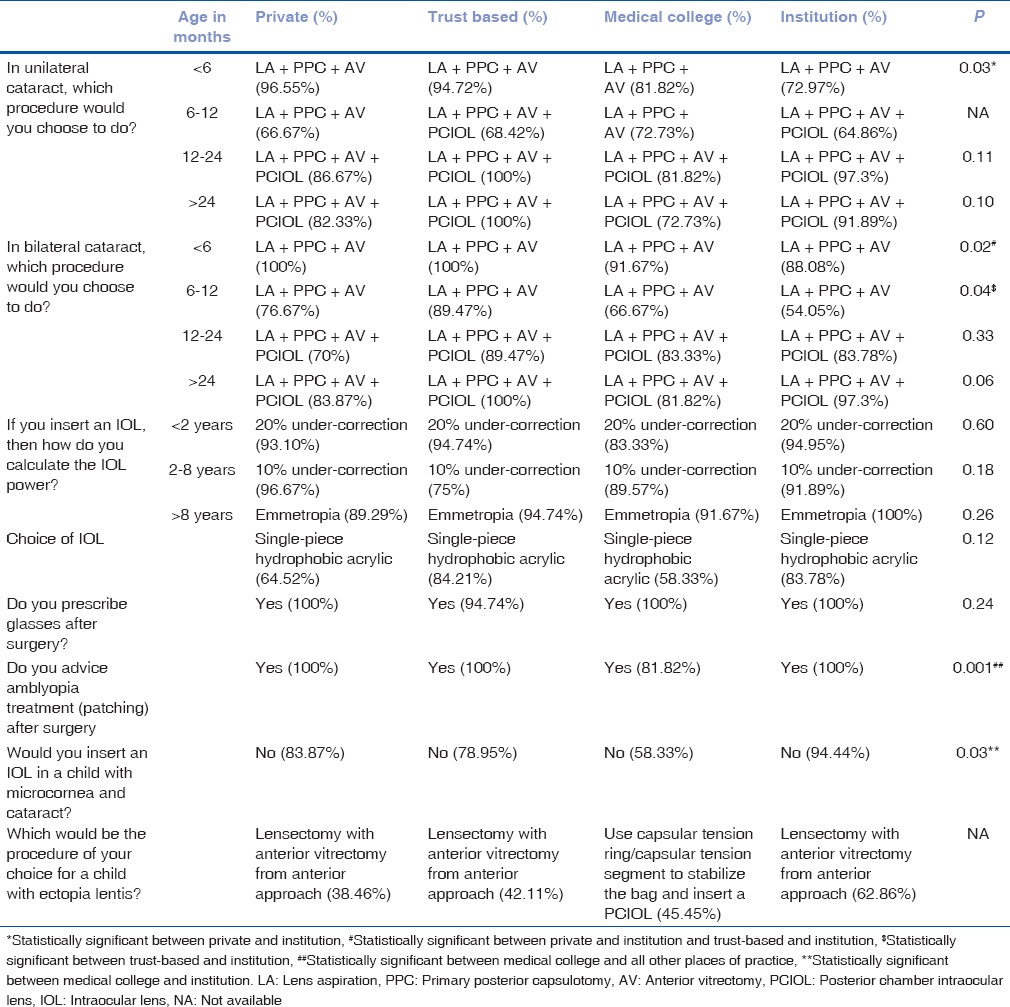
Choice of surgical procedure in unilateral and bilateral cataracts is shown in Tables 1 and 2. A single-piece hydrophobic acrylic IOL was preferred by 73.7% of surgeons, followed by 23.2% who preferred to use a three-piece hydrophobic acrylic IOL. For residual refractive errors, 99% prescribed glasses with 98% advising amblyopia treatment after surgery. Considering the preference for target IOL power, 92.78% of the surgeons undercorrected by 20% in the <2 years age group, 88.78% undercorrected by 10% in the 2–8 years age group, and 89.58% aimed for emmetropia in the >8 years age group. In children with microcornea and cataract, approximately 84% of surgeons did not prefer to insert an IOL. The number of children with ectopia lentis seen in a year ranged from 0 to 200 cases in this cohort. Table 3 shows the procedure of choice in children with ectopia lentis. Table 4 compares the most common procedure of choice with the number of years of experience, and Table 5 shows the most common procedure of choice in different types of practice.
Table 1.
Preference of surgical procedure in unilateral cataract
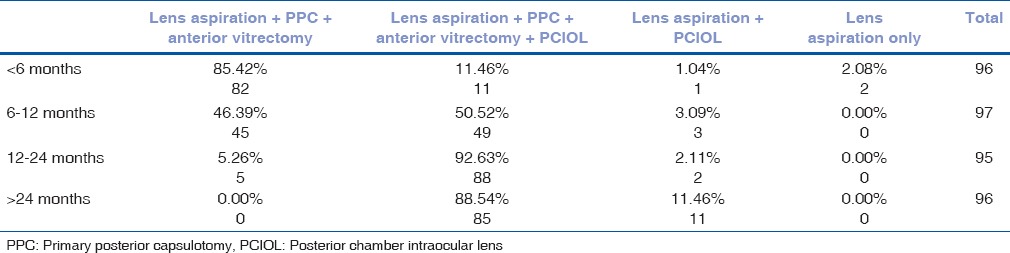
Table 2.
Preference of surgical procedure in bilateral cataract
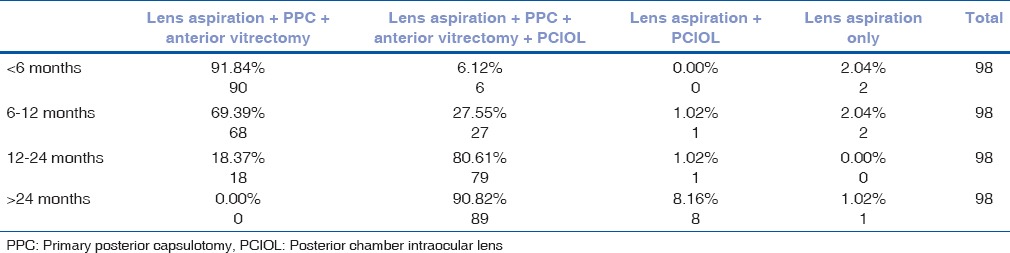
Table 3.
The procedure of choice in children with ectopia lentis

Table 4.
The most common procedure of choice when compared with the number of years of experience
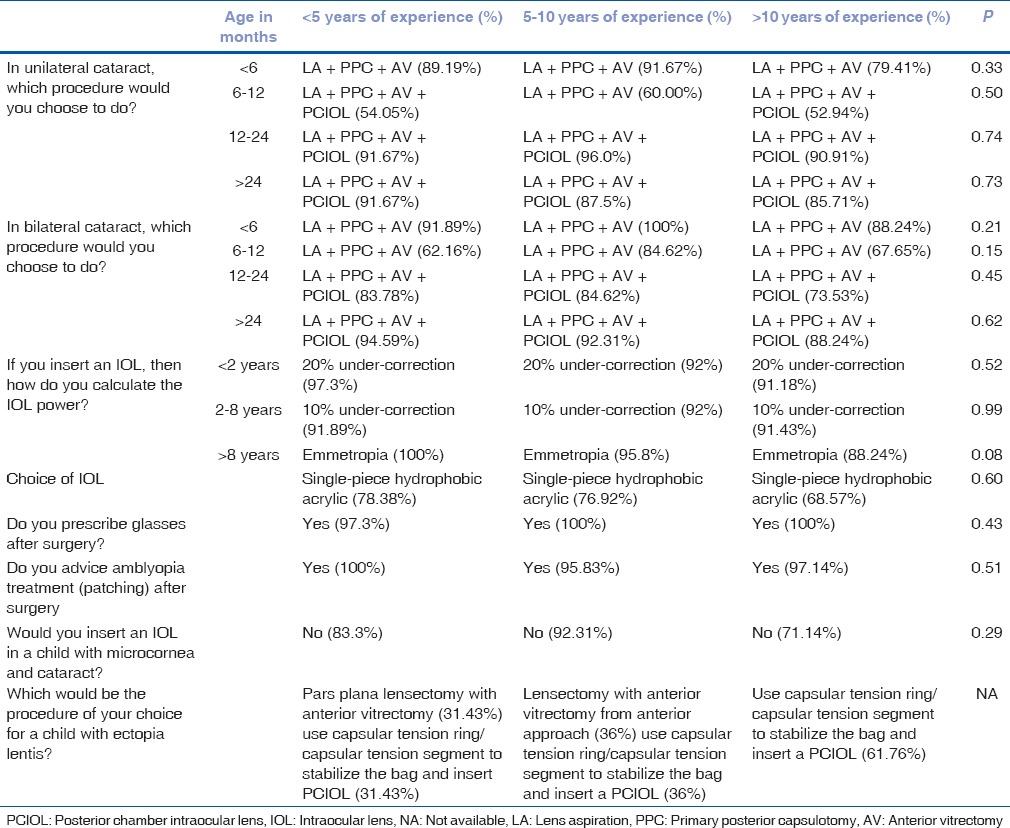
Table 5.
The most common procedure of choice when compared with the place of practice
Discussion
Pediatric eyes are not small adult eyes. They have a developing visual system with unique needs based on their visual demands. One simply cannot extrapolate treatment options of various eye diseases in adults on to children. IOL implantation after cataract surgery in older children is widely accepted,[3] but the implantation of IOLs in those <2 years of age is still controversial[4] and challenging because the surgery has to be done during a period of growth and development in the pro-inflammatory environment of the infant eye.[5] There is an increased incidence of pupillary membranes requiring re-surgery with primary IOL implantation.[4] The Infant Aphakia Treatment Trial recommended leaving the eye aphakic in a child with unilateral cataract <7 months of age.[4] Primary IOL implantation should be reserved for situations where the cost and handling of CLs are deterrent enough to result in significant periods of uncorrected aphakia.[4] Birch et al.[6] reported that IOLs and aphakic CLs provide similar visual acuity development after surgery for unilateral cataracts. They suggested that IOLs may support better visual acuity development when compliance with CL wear is moderate to poor or when the cataract is extracted after 1 year of age. A recently conducted prospective study in the UK compared IOL implantation with CL correction in children under 2 years of age with either unilateral or bilateral cataracts and found that IOL implantation was associated with better vision in the bilateral group but not the unilateral group.[5] Another study by Magli et al.[7] showed that IOL implantation before 12 months of age may be useful in unilateral cataract; for bilateral cataract, simultaneous surgical aphakia, aphakic correction, and then IOL implantation at 2.5–3 years of age, together with anti-amblyopic therapy, are efficient methods to obtain visual recovery. Al Shamrani and Al Turkmani[3] propose that it is better not to implant an IOL in children <6 months of age, while IOL implantation is safe in children over 2 years of age. A retrospective analysis of 28 children (31 eyes) by Lundvall and Zetterström[8] showed that primary IOL implantation for congenital cataract in infants caused a high incidence of after-cataract with membrane formation requiring secondary surgery. In a review article, Ahmadieh and Javadi[9] said that IOL implantation in infants is associated with major complications and not recommended at present.
Recently, there has been an increasing trend toward the use of IOL for visual rehabilitation after cataract surgery in children <1 year of age.[10] Ram et al.[10] feel that primary IOL implantation with primary posterior capsulotomy (PPC) and anterior vitrectomy (AV) is safe in the first 2 years of life if performed meticulously. A retrospective study by Lu et al.[11] also shows that an IOL can be safely implanted in infants. Ninety-two and 85% of the pediatric ophthalmologists in India preferred to do a lens aspiration with PPC and AV in children <6 months of age in bilateral and unilateral cases, respectively, and 81% and 93% opted to insert an IOL in children >1 year of age in bilateral and unilateral cases, respectively. Almost half of them opted to do a lens aspiration with PPC and AV with IOL implantation in children 6–12 months of age in the unilateral cases and only 30% opted to insert an IOL in bilateral cases. This goes well with what is done worldwide.
It is now a well-established fact that hydrophobic foldable IOLs are preferred for children. In a worldwide survey, Wilson et al.[12] found that 69.0% of pediatric ophthalmologists used hydrophobic acrylic IOLs. Although poly methyl methacrylate (PMMA) lenses have the longest track record in children, hydrophobic foldable acrylic IOLs need a smaller incision, which has its own advantages. The single-piece design is said to have a greater ease of insertion and easier capsular bag placement. Compared with a three-piece design, the single-piece IOL has been shown to undergo less haptic deformation with capsular bag fibrosis following surgery and has been associated with lesser capsulorhexis ovaling.[13] The main disadvantage of using hydrophobic foldable IOLs is the cost (approximately $75), in contrast to PMMA lOLs, which are manufactured in several countries for $1–$2 each.[14] Seventy-four percent of surveyed surgeons in India preferred the use of a single-piece acrylic foldable IOL.
Some studies have advocated the use of capsular tension ring/capsular tension segment (CTR/CTS) children with subluxed lenses.[15] We found 44.68% of surgeons preferred to use a CTR/CTS in unilateral cases and 21.74% in bilateral cases [Table 3]. Surgeons generally opt not to perform a PPC when using a CTR/CTS because of the technical challenge of opening the posterior capsule in the same procedure as the implantation of a capsular tension device.[15] Therefore, one of the most common complications which occurs after a pediatric cataract surgery with CTR/CTS is the visual axis opacification which requires a second surgery.[15] A higher number of surgeons preferred this method in unilateral cases when compared to bilateral as spectacle correction cannot be used to treat unilateral aphakia and CL wear has its own drawbacks such as keratitis, corneal neovascularization, noncompliance, frequent lens change, and cost. In contrast, bilateral cases can be easily managed by spectacle correction. For this reason, it appears that 44.12% of surgeons preferred to just do a lensectomy in unilateral cases and 72.82% preferred the same in bilateral cases.
Although studies have shown that scleral fixated IOLs (SFIOLs) are well tolerated in the pediatric population,[16] concerns regarding the long-term stability of the suture material (10-0 polypropylene) have been raised.[17] They indicate that, over time, there is a possibility of 10-0 polypropylene suture degradation, resulting in spontaneous subluxation of the IOLs. To reduce this complication, Price et al.[18] recommend the use of 9-0 polypropylene suture. However, larger bore sclerostomies will be required for the same with an increased potential for leakage. The thicker suture is also technically more difficult to rotate and bury.[17] There are reports on the use of 7-0 polytetrafluoroethylene suture (Gore-TexR) to fixate the IOLs to the sclera in adults.[19] The long-term safety and efficacy of this suture in the eye, especially in the pediatric age group, are yet to be determined. For the above reasons, it seems prudent that very few surgeons preferred SFIOL (10.64% in bilateral cases and 4.35% in unilateral cases [Table 3]) in our study.
In recent years, iris fixation of IOLs to correct aphakia has gained popularity[20] and proposes to be technically less challenging and faster than transscleral fixation. In our study, we found that only 1% of surgeons preferred iris fixated IOLs. The reason for this could be because early dislocation of iris fixated IOLs is still possible and appears to be attributed to either too little iris incorporated in the knot or too tight a knot, resulting in the IOL tearing free from the iris.[21] Late dislocation is possible in both (iris fixated and scleral fixated) techniques secondary to suture failure.[21]
Although there was no statistically significant difference when we correlated the most common procedure done with the number of years of experience, in unilateral and bilateral cataracts in children <6 months of age, surgeons with >10 years of experience preferred to insert an IOL. Furthermore, a larger percentage of surgeons with >10 years' experience opted to insert an IOL in microcornea and in unilateral ectopia lentis. Pediatric cataract surgeries are technically more challenging; smaller the age, the more difficult it becomes. Hence, it is reasonable to assume that a surgeon becomes more confident with experience and hence tends to take up more challenging cases as the number years in practice increases.
In unilateral and bilateral cataracts in children aged <6 months and 6–12 months, the most common procedure performed by surgeons, irrespective of their place of practice, was lens aspiration + PPC + AV; however, the tendency to insert an IOL in a younger child appears to be more common among surgeons in institutions (statistically significant between private practice and institution [P = 0.03] in unilateral cataracts in children <6 months and statistically significant between private practice and institution and trust-based and institution [P = 0.02] in bilateral cataracts in children <6 months [Table 5]). This could be attributed to the fact that such institutions have multiple subspecialties working together under one roof with a good support system in case of difficulties or complications. We also found statistically significant difference in the answer to the question, “Do you start amblyopia treatment after surgery?” Only 80% of surgeons in medical colleges started patching as compared to 100% of surgeons in other practices (P = 0.003). In addition, a greater number of surgeons in medical colleges tended to insert an IOL in children with microcornea (P = 0.03). The reason for this is not very clear.
Some of the limitations of our study must be mentioned. Though e-mails were sent to 520 surgeons, only 99 responded. One reason could be that respondents were not encouraged to provide accurate or honest answers in an online survey.[22] The other reason for this low response rate could be that this society was, till about 3 years earlier, a society made up largely of strabismologists. Thus, it may not represent the practice patterns followed by the entire community of pediatric ophthalmologists in India. Further, general cataract surgeons who perform pediatric cataract surgeries have not been included in this study.
Conclusion
The management of lens anomalies by pediatric ophthalmologists in India varies with laterality, experience, and type of practice and appears to be comparable to those trends seen worldwide.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- 1.Kemmanu V, Hegde K, Giliyar SK, Shetty BK, Kumaramanickavel G, McCarty CA, et al. Prevalence of childhood blindness and ocular morbidity in a rural pediatric population in Southern India: The Pavagada Pediatric Eye Disease Study-1. Ophthalmic Epidemiol. 2016;23:185–92. doi: 10.3109/09286586.2015.1090003. [DOI] [PubMed] [Google Scholar]
- 2.Lambert SR, Lynn M, Drews-Botsch C, DuBois L, Wilson ME, Plager DA, et al. Intraocular lens implantation during infancy: Perceptions of parents and the American Association for Pediatric Ophthalmology and Strabismus members. J AAPOS. 2003;7:400–5. doi: 10.1016/j.jaapos.2003.08.004. [DOI] [PubMed] [Google Scholar]
- 3.Al Shamrani M, Al Turkmani S. Update of intraocular lens implantation in children. Saudi J Ophthalmol. 2012;26:271–5. doi: 10.1016/j.sjopt.2012.05.005. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Infant Aphakia Treatment Study Group. Lambert SR, Lynn MJ, Hartmann EE, DuBois L, Drews-Botsch C, et al. Comparison of contact lens and intraocular lens correction of monocular aphakia during infancy: A randomized clinical trial of HOTV optotype acuity at age 4-5 years and clinical findings at age 5 years. JAMA Ophthalmol. 2014;132:676–82. doi: 10.1001/jamaophthalmol.2014.531. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Solebo AL, Russell-Eggitt I, Cumberland PM, Rahi JS British Isles Congenital Cataract Interest Group. Risks and outcomes associated with primary intraocular lens implantation in children under 2 years of age: The ioLunder2 cohort study. Br J Ophthalmol. 2015;99:1471–6. doi: 10.1136/bjophthalmol-2014-306394. [DOI] [PubMed] [Google Scholar]
- 6.Birch EE, Cheng C, Stager DR, Jr, Felius J. Visual acuity development after the implantation of unilateral intraocular lenses in infants and young children. J AAPOS. 2005;9:527–32. doi: 10.1016/j.jaapos.2005.07.008. [DOI] [PubMed] [Google Scholar]
- 7.Magli A, Fimiani F, Bruzzese D, Carelli R, Giani U, Iovine A, et al. Congenital cataract extraction with primary aphakia and secondary intraocular lens implantation in the posterior chamber. Eur J Ophthalmol. 2008;18:903–9. doi: 10.1177/112067210801800608. [DOI] [PubMed] [Google Scholar]
- 8.Lundvall A, Zetterström C. Primary intraocular lens implantation in infants: Complications and visual results. J Cataract Refract Surg. 2006;32:1672–7. doi: 10.1016/j.jcrs.2006.05.004. [DOI] [PubMed] [Google Scholar]
- 9.Ahmadieh H, Javadi MA. Intra-ocular lens implantation in children. Curr Opin Ophthalmol. 2001;12:30–4. doi: 10.1097/00055735-200102000-00006. [DOI] [PubMed] [Google Scholar]
- 10.Ram J, Brar GS, Kaushik S, Sukhija J, Bandyopadhyay S, Gupta A, et al. Primary intraocular lens implantation in the first two years of life: Safety profile and visual results. Indian J Ophthalmol. 2007;55:185–9. doi: 10.4103/0301-4738.31937. [DOI] [PubMed] [Google Scholar]
- 11.Lu Y, Ji YH, Luo Y, Jiang YX, Wang M, Chen X, et al. Visual results and complications of primary intraocular lens implantation in infants aged 6 to 12 months. Graefes Arch Clin Exp Ophthalmol. 2010;248:681–6. doi: 10.1007/s00417-010-1310-4. [DOI] [PubMed] [Google Scholar]
- 12.Wilson ME, Elliott L, Johnson B, Peterseim MM, Rah S, Werner L, et al. AcrySof acrylic intraocular lens implantation in children: Clinical indications of biocompatibility. J AAPOS. 2001;5:377–80. doi: 10.1067/mpa.2001.119786. [DOI] [PubMed] [Google Scholar]
- 13.Pandey SK, Werner L, Wilson ME, Jr, Izak AM, Apple DJ. Capsulorhexis ovaling and capsular bag stretch after rigid and foldable intraocular lens implantation: Experimental study in pediatric human eyes. J Cataract Refract Surg. 2004;30:2183–91. doi: 10.1016/j.jcrs.2004.02.079. [DOI] [PubMed] [Google Scholar]
- 14.Shah A, Spalton DJ, Gilbert C, Vasavada A, Boyce JF, Minassian D, et al. Effect of intraocular lens edge profile on posterior capsule opacification after extracapsular cataract surgery in a developing country. J Cataract Refract Surg. 2007;33:1259–66. doi: 10.1016/j.jcrs.2007.03.044. [DOI] [PubMed] [Google Scholar]
- 15.Kim EJ, Berg JP, Weikert MP, Kong L, Hamill MB, Koch DD, et al. Scleral-fixated capsular tension rings and segments for ectopia lentis in children. Am J Ophthalmol. 2014;158:899–904. doi: 10.1016/j.ajo.2014.08.002. [DOI] [PubMed] [Google Scholar]
- 16.Vote BJ, Tranos P, Bunce C, Charteris DG, Da Cruz L. Long-term outcome of combined pars plana vitrectomy and scleral fixated sutured posterior chamber intraocular lens implantation. Am J Ophthalmol. 2006;141:308–12. doi: 10.1016/j.ajo.2005.09.012. [DOI] [PubMed] [Google Scholar]
- 17.Luk AS, Young AL, Cheng LL. Long-term outcome of scleral-fixated intraocular lens implantation. Br J Ophthalmol. 2013;97:1308–11. doi: 10.1136/bjophthalmol-2013-303625. [DOI] [PubMed] [Google Scholar]
- 18.Price MO, Price FW, Jr, Werner L, Berlie C, Mamalis N. Late dislocation of scleral-sutured posterior chamber intraocular lenses. J Cataract Refract Surg. 2005;31:1320–6. doi: 10.1016/j.jcrs.2004.12.060. [DOI] [PubMed] [Google Scholar]
- 19.Das S, Nicholson M, Deshpande K, Kummelil MK, Nagappa S, Shetty BK, et al. Scleral fixation of a foldable intraocular lens with polytetrafluoroethylene sutures through a Hoffman pocket. J Cataract Refract Surg. 2016;42:955–60. doi: 10.1016/j.jcrs.2016.06.018. [DOI] [PubMed] [Google Scholar]
- 20.Kavitha V, Balasubramanian P, Heralgi MM. Posterior iris fixated intraocular lens for pediatric traumatic cataract. Middle East Afr J Ophthalmol. 2016;23:215–8. doi: 10.4103/0974-9233.171777. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Buckley EG. Pediatric sutured intraocular lenses: Trouble waiting to happen. Am J Ophthalmol. 2009;147:3–4. doi: 10.1016/j.ajo.2008.08.033. [DOI] [PubMed] [Google Scholar]
- 22.Wright KB. Researching Internet-based populations: Advantages and Disadvantages of Online Survey Research, Online Questionnaire Authoring Software Packages, and Web Survey Services. J Comp Med Commun. 2005;10:[Epub ahead of print]. [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.