

Abstract
Objectives
To assess the value of new magnetic resonance imaging (MRI) techniques in cervical cancer.
Methods
We searched PubMed and MEDLINE and reviewed articles published from 1990 to 2016 to identify studies that used MRI techniques, such as diffusion weighted imaging (DWI), intravoxel incoherent motion (IVIM) and dynamic contrast enhancement (DCE) MRI, to assess parametric invasion, to detect lymph node metastases, tumour subtype and grading, and to detect and predict tumour recurrence.
Results
Seventy-nine studies were included. The additional use of DWI improved the accuracy and sensitivity of the evaluation of parametrial extension. Most studies reported improved detection of nodal metastases. Functional MRI techniques have the potential to assess tumour subtypes and tumour grade differentiation, and they showed additional value in detecting and predicting treatment response. Limitations included a lack of technical standardisation, which limits reproducibility.
Conclusions
New advanced MRI techniques allow improved analysis of tumour biology and the tumour microenvironment. They can improve TNM staging and show promise for tumour classification and for assessing the risk of tumour recurrence. They may be helpful for developing optimised and personalised therapy for patients with cervical cancer.
Teaching points
• Conventional MRI plays a key role in the evaluation of cervical cancer.
• DWI improves tumour delineation and detection of nodal metastases in cervical cancer.
• Advanced MRI techniques show promise regarding histological grading and subtype differentiation.
• Tumour ADC is a potential biomarker for response to treatment.
Keywords: Cervical cancer, DCE, DWI, IVIM, MRI
Introduction
Cervical cancer remains the fourth most common cancer in women worldwide [1], showing particularly high incidence in countries with low socioeconomic status. There is wide regional variation in the use of imaging modalities, and magnetic resonance imaging (MRI) in particular, in the work-up of cervical cancer. Accordingly, the FIGO classification [2], which is the internationally recognised staging system for cervical cancer, relies solely on clinical examination in assessing tumour stage. However, the current FIGO classification acknowledges the use of imaging methods as an adjunct for cervical cancer staging, and a number of studies have shown that imaging, especially MRI, is superior to clinical examination alone for correctly evaluating cervical carcinoma stage [3–7]. This is of particular importance in regard to the identification of parametrial invasion and the correct assessment of tumour size, given their important implications for the choice of treatment, i.e. fertility-sparing surgery versus neoadjuvant chemotherapy [8, 9].
Lymph node status is not part of the FIGO classification system; however, lymph node metastases are an important independent adverse prognostic factor [10]. The depth of stromal tumour invasion is associated with an increased risk for lymph node metastases [11]. Surgical lymph node dissection remains the “gold standard” for the diagnosis of lymph node metastases, but it may be associated with postoperative complication rates of up to 17% [12] and with unwanted side effects such as lymphoceles and wound infections. Therefore, preoperative assessment of lymph node stage using imaging may have great clinical importance.
Histological subtype and grade of differentiation may also determine the course of the disease, the therapeutic outcome and patient survival [10, 13]. Squamous cell carcinomas represent the majority of cervical cancer cases (ca. 69%) compared to adenocarcinomas (ca. 25%) [14, 15]. Whether clinical outcome differs between squamous cell carcinomas and adenocarcinomas still remains controversial. However, rare tumour subtypes like neuroendocrine tumours have an unfavourable prognosis [16]. Low-grade tumours are associated with favourable outcomes and lower tumour recurrence rates compared to high-grade tumours [17]. Although histopathological samples can be acquired easily by biopsy prior to surgery, tumour heterogeneity may lead to sampling errors in large tumours [18, 19].
Where available, conventional MRI is the preferred imaging modality for evaluating the local extent of cervical cancer due to its excellent soft tissue contrast [20, 21]. Recently developed MRI techniques, namely diffusion weighted imaging (DWI) [22] and dynamic contrast enhanced MRI (DCE-MRI)—also termed multiparametric MRI—are already part of the standard MR work-up for other tumour entities [23]. These techniques also show promise as complementary techniques for the assessment of cervical cancer, as they allow the assessment of the tumour microenvironment rather than solely relying on conventional anatomical measurements (e.g. tumour size, infiltration of surrounding structures, etc.).
There is increasing interest and research effort focused on these new techniques. This systematic review summarises the current status of knowledge on the value of multiparametric MRI for the non-invasive assessment of parametrial invasion, lymph node status, tumour grading/subtype differentiation and response to chemotherapy, which are considered the most important clinical features for selecting a personalised therapeutic approach for an individual patient.
Materials and methods
We adhered to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) Guidelines. A systematic literature search of PubMed and MEDLINE was conducted using the following search criteria: “MRI cervical cancer”, “DWI cervical cancer”, “DCE cervical cancer” and “IVIM cervical cancer”. The search was conducted on October 4, 2016, and it retrieved 2,393, 81, 66 and 6 references, respectively, for these searches. Only articles in English published in 1990–2016 were included. All articles were screened for relevance using the title and abstract. All study designs were eligible for inclusion. Studies on animals, duplicate studies and case reviews were excluded.
The resulting studies were reviewed independently by two authors (E.D. and A.M.H.). In the event of a disagreement about study inclusion, the two authors reached a consensus decision about inclusion after discussing whether the criteria for inclusion were fulfilled.
The primary eligibility criteria were that the articles reported on studies that examined the use of DWI, DCE-MRI or intravoxel incoherent motion (IVIM) for detecting parametrial invasion and lymph node metastases, determining tumour subtype and grading, and predicting tumour recurrence and therapeutic response.
The following data were extracted from full text articles: the study characteristics, including study design, year of publication, MRI sequences, histopathological findings and outcome(s). The final list of publications included 79 original research articles.
Conventional MRI for staging cervical cancer
MRI has no role in evaluating stage IA cervical cancer, because microscopic disease cannot be reliably detected [20]. However, MRI is the preferred imaging method for tumours of stage higher than IB2, since it allows a highly accurate assessment of the extent of tumour infiltration. MRI is superior to clinical staging for evaluating tumour size and location [3–7], and it improves the accuracy of FIGO staging by up to 96% [7].
The standard MRI protocol (Table 1) for cervical cancer includes T2-weighted imaging of the pelvis in different planes [20]. Axial and coronal planes are acquired obliquely, orientated to the plane of the cervical canal (Fig. 1). This allows for a more precise evaluation of tumour borders and parametrial invasion. T1- and T2-weighted sequences covering the whole abdomen and pelvis should be added to exclude identifiable lymph node metastases.
Table 1.
Proposed MRI protocol for cervical cancer staging
| Sequence | Technical aspects | Comments | |
|---|---|---|---|
| T1 axial | TSE/2D GRE | Whole abdomen and pelvis ST 5 mm | Assessment of lymph nodes and distant metastases |
| T2 coronal | SS-TSE | Whole abdomen and pelvis ST 5 mm | Assessment of lymph nodes and distant metastases |
| T2 sagittal | TSE | Small FOV ca. 0.5 × 0.5 mm in-plane resolution ST 3 mm | Tumour evaluation (size, extension), assessment of rectal and bladder infiltration |
| T2 axial oblique | TSE | Small FOV ca. 0.5 × 0.5 mm in-plane resolution ST 3 mm perpendicular to long axis of cervical canal | Tumour extension, assessment of parametrial invasion and rectal and bladder infiltration |
| T2 coronal oblique | TSE | Small FOV ca. 0.5 × 0.5 mm in-plane resolution ST 3 mm parallel to long axis of cervical canal | Tumour extension, assessment of parametrial invasion in a second imaging plane |
| DWI axial oblique | EPI | Small FOV ST 3 mm b values 100, 600, 1,000 s/mm2 | Tumour extension, assessment of parametrial invasion |
| Optional: multiphase 3D T1w fat-saturated sequences | GRE | ST 3 mm one native, four post-contrast scans | Alternatively DCE axial oblique (temporal resolution <10 s) |
Preparation: fasting (>4 h), antiperistaltic agents, moderately filled bladder
DCE dynamic contrast enhanced, DWI diffusion weighted imaging, EPI echo-planar imaging, FOV field of view, GRE gradient echo, ST slice thickness, TSE turbo spin echo, SS-TSE single-shot turbo spin echo
Fig. 1.
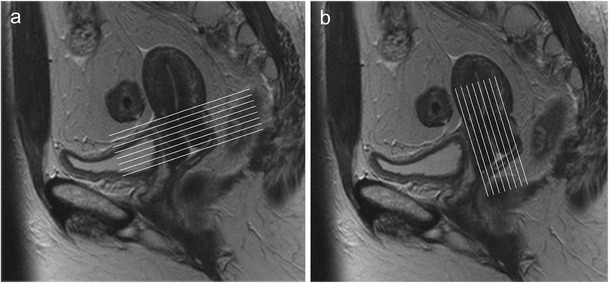
Sagittal T2-weighted image. The oblique axial (a) and coronal planes (b) are orientated to the plane of the cervical canal
Advanced MRI techniques
DWI and DCE-MRI have emerged as promising tools for characterising uterine malignancies [20, 24]. DWI is based on the principles of Brownian movement of water molecules, and it gives information about tissue structure on a microscopic level [24, 25]. Since solid tumours generally exhibit an increased cell count, the diffusion of water molecules is restricted in tumour tissue. In contrast, diffusion is less restricted, for example, in areas of tumour necrosis, where water molecules can move more freely. To quantify these differences in tissues, special MRI pulse sequences are applied to measure the movement of the water molecules. Additionally, an apparent diffusion coefficient (ADC) map can be constructed, which allows for an easy visual assessment of the tumour (Fig. 2). In the literature, low ADC values have been shown to correlate with tumour aggressiveness in various tumour entities, such as prostate cancer [23, 26].
Fig. 2.
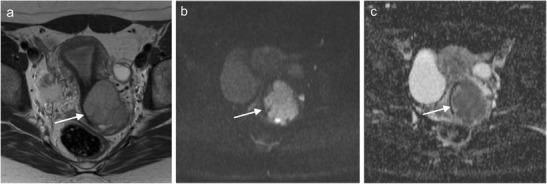
Axial T2-weighted image (a) and DWI image (b = 800) with ADC map (c) of a 36-year-old woman with stage IIB low-grade squamous cell cervical carcinoma. A hyperintense lesion is seen in the cervix (arrow), and there is disruption of the cervical stroma ring and parametrical invasion (a). The tumour shows high signal intensity on DWI (b), with corresponding low signal intensity on the ADC map (c)
IVIM is an extension of DWI that allows the assessment of perfusion characteristics in tumourous tissue by visualising the microscopic motions of water molecules [27]. This allows the determination of several different parameters, namely: D, the true molecular diffusion coefficient; D*, the perfusion-related fast diffusion coefficient, which correlates with blood flow; and f, the perfusion fraction, which is linked to the blood volume within tissue [18, 27–29]. Neither DWI nor IVIM require the administration of contrast agents and can therefore be used in patients with renal insufficiency [24].
DCE-MRI is a dynamic examination technique that depicts changes in signal intensity over time after injection of a standard paramagnetic contrast agent. DCE-MRI is used to characterise tumour microcirculation. DCE-MRI can be evaluated either semiquantitatively to determine parameters that describe changes in signal intensity over time, or quantitatively, which requires the use of pharmacokinetic models. Quantitative measurements can be used to analyse perfusion and permeability parameters, such as the volume transfer constant between plasma and the extracellular extravascular space (Ktrans), which correlates with vascular permeability. DCE-MRI is already implemented in MR protocols that are used to evaluate other tumour entities, such as prostate carcinoma, to improve tumour detection in treatment-naive and post-treatment patients [30].
Assessment of parametrial invasion
Conventional MRI has a reported diagnostic accuracy of 88.3–94%, a sensitivity of 38–100%, and a specificity of up to 92% in the assessment of parametrial invasion [31–34]. The signs of parametrial invasion on T2-weighted sequences include the disruption of the cervical stromal ring, spiculated tumour invasion and encasement of the periuterine vessels [35]. MRI can accurately exclude parametrial invasion, with a negative predictive value ranging from 94–100% [20, 36]. The intact hypointense stromal ring around the cervix on T2-weighted axial imaging represents the main sign for excluding parametrial invasion [37].
DWI further improves the assessment of parametrial invasion when it is added to conventional T2-weighted MRI [38–40]. Parametrial extension can be overestimated on T2-weighted images, especially in large tumours, which can induce changes in the surrounding stromal tissue due to tumour compression or increased inflammation [20, 41]. DWI reflects tumour cellularity, which helps differentiate between infiltrating tumour tissue and reactive changes. Park et al. [39] found that the fusion of DWI with T2-weighted images significantly (p < 0.05) increased diagnostic accuracy (reader 1, 90.1%; reader 2, 89.5%) compared to T2-weighted images alone (reader 1, 85.5%; reader 2, 83.6%). However, DWI is limited by poor anatomical detail and low spatial resolution; therefore, it should always be assessed in conjunction with T2-weighted images.
Studies have examined the correlation between low ADC values and tumour aggressiveness, including the presence of histopathological parametrial invasion [14, 42–44]. For example, Park et al. [44] found that patients with parametrial invasion had significantly lower tumour ADCs than those without and concluded that tumour ADC values are independent predictors of pathological parametrial invasion.
Detection of lymph node metastases
Conventional MRI relies on the criterion of size for assessing pelvic lymph node involvement. Lymph nodes are rated as suspicious if the short axis diameter is greater 1 cm. However, given the overlap in size between metastatic, hyperplastic and normal lymph nodes and the fact that micrometastases in small lymph nodes are not uncommon [21], conventional MRI is limited in lymph node assessment, even when accounting for FIGO stage [45]. The literature shows that the diagnostic accuracy of MRI is 67–95%, its sensitivity is 37–90%, and its specificity is 71–100% [21, 32, 46–54], even when other signs of metastatic disease, such as loss of normal lymph node architecture, rounder form, irregular borders and heterogeneous signal intensity, are considered.
DWI may represent a powerful adjunct for differentiating between metastatic and non-metastatic lymph nodes, as it reflects differences in cellularity and histopathology between benign and malignant lymph nodes [55, 56]. Several studies have reported that lymph node metastases have a higher degree of diffusion restriction than normal lymph nodes, and this can be assessed quantitatively using ADC values [57–64]. Choi et al. [61] found that measuring the minimal ADC in a lymph node had greater sensitivity for detecting metastases than measuring the short-axis diameter (86% vs 55%, p < 0.001). Similarly, Liu et al. [57] reported a sensitivity of 95.7% and a specificity of 96.5% for the detection of metastatic nodes. Yet the results in the literature are conflicting [60, 65–67], as Rizzo et al. [67] found no significant association between DWI parameters and the presence of lymph node metastasis. However, the authors suggested that their results might have been influenced by patient selection (early clinical stage) and small patient number. Another study reported an overlap in mean ADC values between malignant lymph nodes and hyperplastic lymph nodes, which reduced the diagnostic accuracy to 78.4% [60]. However, the patients in that study were excluded if all of their lymph nodes had a short axis diameter under 5 mm, and this may have influenced the results [60]. Although a meta-analysis by Shen et al. [55] confirmed the usefulness of DWI for differentiation between benign and metastatic lymph nodes, study heterogeneity—especially regarding the lack of standard protocol for DWI—limits the comparability of these results. Further prospective studies with standardised MRI protocol may offer more evidence regarding the value of DWI for nodal detection.
Compared with PET/CT, routine MRI without DWI is less sensitive and accurate for the detection of nodal metastases [49, 54, 68]. A meta-analysis published in 2010 which included 41 studies found that PET and PET/CT had a higher diagnostic performance compared with MRI and CT [69]. The addition of DWI may increase the diagnostic performance of MRI compared with PET/CT. Monteil et al. [70] reported that MRI which included DWI sequences is more precise than FDG PET/CT for detecting pelvic lymph node metastases, with a sensitivity, specificity, and diagnostic accuracy of 67%, 84% and 81% compared to 33%, 92% and 81% for PET/CT; although the differences were not as pronounced for para-aortic lymph nodes. Kitajima et al. [71] also reported that DWI had higher sensitivity than FDG PET/CT (83.3% vs 38.9%) but lower specificity (51.2% vs 96.3%) for detecting lymph node metastases. Although these studies show that the addition of DWI clearly improves sensitivity of MRI for the detection of nodal metastases, PET/CT still has a higher specificity of up to 97% [69]. Especially in cases of advanced disease, PET/CT has a high sensitivity (75-100%) and specificity (87-100%) [20] and can help demonstrate sites of unexpected disease such as supraclavicular lymph nodes [72].
In the future, lymph node-specific MR contrast agents could further improve the assessment of lymph node metastases. There are new MR contrast agents that are classified as nanoparticles that contain ultrasmall particles of iron oxide (USPIO). These agents are taken up by macrophages into lymph nodes [73]. Metastatic lymph nodes displace macrophages, thereby preventing USPIO uptake. USPIO increases the sensitivity of MRI up to 93% for the prediction of nodal metastases [73, 74], and it can also improve tumour conspicuity [75, 76].
Currently, there are no USPIO contrast agents that are approved by the U.S. Food and Drug Administration (FDA) or European Medicines Agency (EMA) for clinical MRI applications [77]. Several first-generation USPIOs, such as SHU 555 C (Supravist) and AMI-227, were discontinued or are still awaiting approval. Ferumoxytol, a second-generation USPIO, is an FDA-approved drug that is used to treat iron insufficiency anaemia in patients with chronic kidney disease. Its application as an MRI contrast agent remains off-label, and it is no longer authorised for use in the European Union.
Another contrast agent, gadofosveset trisodium, which binds to human serum albumin and which accumulates in benign lymph nodes, has shown great value in precise lymph node staging in rectal cancer MRI [78]. Thus, it may also be of value in staging cervical cancer.
Grading and subtype differentiation
The ADC has value in differentiating between normal uterine cervix stroma and cervical carcinoma [79–87]. Furthermore, the ADC shows potential for assessing pathological subtypes and for tumour grade differentiation [14, 60, 88–92]. A recent study [93] reported lower ADC values in poorly differentiated tumours compared to well/moderately differentiated tumours (p = 0.02). However, there were no significant differences between squamous cell carcinomas and adenocarcinomas (p = 0.1). In contrast, Xue et al. [92] retrospectively investigated ADC values in 53 patients with histopathologically proven cervical cancer and found a significant difference in the mean ADC values between adenocarcinomas and squamous cell carcinomas (p = 0.0074). However, there are currently no established ADC cutoff values as variations in MRI techniques and protocols can affect ADC values. In case of the previously mentioned studies, Winfield et al. [93] used a 3-T scanner with an endovaginal coil, resulting in higher signal-to-noise ratio and spatial resolution compared to a 1.5-T scanner with eight-channel phased-array body coil used in the study of Xue et al. This hinders comparisons between different centres and studies [94, 95].
In addition to DWI, IVIM may be useful for evaluating tumour differentiation and perfusion [18, 28, 93, 96]. IVIM perfusion parameters show moderate to good correlation with perfusion parameters derived from DCE-MRI in cervical cancer (r = 0.42–0.58; p = 0.003–0.038) [96]. Recently, mono-exponential DWI values (“classical” ADC values) were compared to IVIM model parameters in 42 cervical cancer patients, with both ADC and D (true molecular diffusion coefficient) showing lower values in poorly differentiated tumours than in well/moderately differentiated tumours [93]. To investigate differences between cancer tissue and normal cervical stroma, Lee et al. [28] compared the IVIM characteristics of 16 patients with cervical cancer with those of 17 healthy controls. Cervical cancer had lower perfusion and diffusion IVIM values compared to normal cervical tissue and leiomyoma tissue. Zhou et al. [18] reported higher perfusion at the tumour edge in high-grade tumours and found that D was significantly higher in G1 tumours than in G3 tumours. Moreover, the authors proposed that measuring tumour perfusion at the tumour edge might be better than measuring the whole tumour volume. Notably, during rapid tumour growth, cell proliferation often exceeds tumour angiogenesis, leading to poorly perfused central tumour areas and leading to tumour heterogeneity. Yamashita et al. [97] examined 62 cervical cancer patients using DCE-MRI. They found that areas with high contrast enhancement represented cancer cell fascicles and that poorly enhanced areas contained mainly fibrous tissue.
Tumour recurrence and therapeutic response
Differentiating residual tumour tissue or tumour recurrence from post-therapeutic tissue changes, such as inflammation and fibrosis, remains challenging using conventional MRI, as both scar tissue and residual tumour tissue can have similar signal intensities. The ideal time to predict therapy response is not yet defined. Some authors advocate early assessment 2 weeks after radiochemotherapy [98]. In difficult cases, functional imaging, including DWI and DCE, can be a useful addition. Mahajan et al. [99] examined 30 patients after hysterectomy with suspected local tumour recurrence. Additional multiparametric sequences, including DWI and DCE, increased the diagnostic accuracy to 100% compared to 70% accuracy with conventional MRI alone. Similarly, another study reported that a combination of T2-weighted images and DWI had a higher diagnostic accuracy in the detection of post-treatment tumour recurrence versus T2-weighted images alone (92.1% vs 73.6%, p = 0.016) [100].
The tumour ADC has been described as a potential biomarker for response to treatment. As noted above, the tumour ADC can be used to assess tumour grading, which can reflect tumour aggressiveness [92] and which is associated with treatment resistance. Several authors have compared pre-treatment ADC values in patients with versus without later tumour recurrence, finding that low pre-treatment ADC values seem to be a strong predictor of later tumour recurrence [22, 101–107]. Furthermore, changes in ADC values during chemotherapy, radiotherapy or chemoradiation may help evaluate the treatment response [42, 43, 108–123]. For example, Kuang et al. [42] examined 75 patients prior to, during and after therapy completion and found significantly higher ADCs in patients with complete response compared to those with partial response or stable disease after therapy completion. Accordingly, the ADC seems to be a good biomarker for monitoring the early tumour response [112, 113, 115, 117, 119, 122, 124], as increasing ADC values reflect increased diffusivity, possibly due to treatment-induced necrosis, apoptosis-induced cell death, loss of cell membrane integrity and increased extracellular space [42, 124, 125].
DWI may also have value as a predictor of long-term disease control. A recent study examined post-treatment DWI in 100 patients 1 month after completion of chemoradiation [126]. They found that the presence of residual tumour tissue determined on post-treatment T2-weighted images with the addition of DWI improved the prediction of disease progression up to 3 years after treatment, with a positive predictive value of 72.7% compared to 39.3% for T2-weighted images without DWI.
IVIM techniques may also be useful for predicting and monitoring tumour response, with results that are comparable to mono-exponential ADC modelling [120, 127]. However, so far only a few studies have investigated IVIM in this context. Zhu et al. [127] examined 21 patients who were receiving chemoradiation therapy and showed an increase of both f (the perfusion fraction) and D* (the pseudoperfusion coefficient) in the first weeks of chemoradiation therapy.
The value of DCE-MRI in predicting tumour response is well studied. Tumours with low perfusion characteristics are associated with tumour hypoxia, which represents a negative prognostic factor in cervical cancer [128]. In contrast, more oxygenated tumours may be more sensitive to radiation and chemotherapy, leading to a better prognosis [129, 130]. DCE-MRI can be used to predict the treatment response in cervical cancer [97, 117, 129, 131–146] and can show longitudinal changes in tumour perfusion during treatment [132, 142]. Mayr et al. [142] demonstrated that persistent low perfusion prior to, during and after radiotherapy correlates with a high risk of treatment failure; in contrast, patients with higher perfusion prior to therapy or with therapy-induced increases in initially low perfusion show a better outcome. According to Halle et al. [134], DCE-MRI can identify patients with hypoxia-related chemoresistance by correlating hypoxia-related gene sets with a previously determined prognostic DCE-MRI parameter (ABrix). Early identification of tumours with persistent low perfusion and, consequently, a higher chance of treatment failure warrants further investigation, as this could drive a change in treatment strategy and help the field move toward a more personalised treatment approach.
Limitations
There are limitations to DWI and DCE-MRI in that there are some technical issues and, most importantly, a lack of standardisation. The technical limitations include differences in modelling and the choice of b values for diffusion-weighted MRI, plus there are a large variety of pharmacokinetic models and sequences/contrast agent injection protocols used for DCE-MRI. Moreover, continuous technical advances and constant optimisation of MRI protocols according to the newest technical standards inadvertently reduce the comparability of MRI studies, as changes in resolution or the introduction of new advanced MRI techniques might allow for more precise tumour depiction. This had led to limited reproducibility and, since ADC values differ between various centres and with different MRI scanners, there are currently no established ADC cut-off values that allow for precise differentiation between, for example, tumour subtypes or grades [95]. Standardisation of MRI techniques is therefore considered critical for improving comparisons between studies.
Regarding the assessment of lymph node metastases, several studies excluded lymph nodes smaller than 5 mm, leading to selection bias. Node-by-node correlations between preoperative MRI and histopathological specimens present another problem. Lymph node position is generally labelled according to lymph node region, which limits the correlation between suspicious MRI findings and histopathological samples. In addition, the small size of some lymph nodes makes it difficult to precisely position a region of interest in order to measure, for example, ADC in a single lymph node.
Conclusions
Conventional MRI plays a key role in the evaluation of cervical cancer, showing good results for the assessment of tumour extent and parametrial invasion. New techniques, such as DWI, IVIM and DCE, show promise as tools for viewing cervical tumours and for quantitative analysis of tumour biology and the microenvironment. The addition of DWI improves the determination of tumour extension and the detection of lymph node metastases. Both DWI and DCE might provide further insights into tumour biology in terms of histological grading and subtype differentiation, and thereby help to assess the risk of tumour recurrence. Large multicentre prospective studies are needed to determine whether these new techniques can be used to develop optimised and personalised therapies for patients with cervical cancer.
References
- 1.Ferlay J, Soerjomataram I, Dikshit R, et al. Cancer incidence and mortality worldwide: sources, methods and major patterns in GLOBOCAN 2012. Int J Cancer. 2015;136:E359–E386. doi: 10.1002/ijc.29210. [DOI] [PubMed] [Google Scholar]
- 2.Pecorelli S. Revised FIGO staging for carcinoma of the vulva, cervix, and endometrium. Int J Gynaecol Obstet. 2009;105:103–104. doi: 10.1016/j.ijgo.2009.02.012. [DOI] [PubMed] [Google Scholar]
- 3.Bleker SM, Bipat S, Spijkerboer AM, van der Velden J, Stoker J, Kenter GG. The negative predictive value of clinical examination with or without anesthesia versus magnetic resonance imaging for parametrial infiltration in cervical cancer stages IB1 to IIA. Int J Gynecol Cancer. 2013;23:193–198. doi: 10.1097/IGC.0b013e31827a4ad8. [DOI] [PubMed] [Google Scholar]
- 4.Dhoot NM, Kumar V, Shinagare A, Kataki AC, Barmon D, Bhuyan U. Evaluation of carcinoma cervix using magnetic resonance imaging: correlation with clinical FIGO staging and impact on management. J Med Imaging Radiat Oncol. 2012;56:58–65. doi: 10.1111/j.1754-9485.2011.02333.x. [DOI] [PubMed] [Google Scholar]
- 5.Kraljevic Z, Viskovic K, Ledinsky M, et al. Primary uterine cervical cancer: correlation of preoperative magnetic resonance imaging and clinical staging (FIGO) with histopathology findings. Coll Antropol. 2013;37:561–568. [PubMed] [Google Scholar]
- 6.Mitchell DG, Snyder B, Coakley F, et al. Early invasive cervical cancer: tumor delineation by magnetic resonance imaging, computed tomography, and clinical examination, verified by pathologic results, in the ACRIN 6651/GOG 183 Intergroup Study. J Clin Oncol. 2006;24:5687–5694. doi: 10.1200/JCO.2006.07.4799. [DOI] [PubMed] [Google Scholar]
- 7.Rajaram S, Sharma H, Bhargava SK, Tripathi RP, Goel N, Mehta S. Mapping the extent of disease by multislice computed tomography, magnetic resonance imaging and sentinel node evaluation in stage I and II cervical carcinoma. J Cancer Res Ther. 2010;6:267–271. doi: 10.4103/0973-1482.73342. [DOI] [PubMed] [Google Scholar]
- 8.Pareja R, Rendon GJ, Vasquez M, Echeverri L, Sanz-Lomana CM, Ramirez PT. Immediate radical trachelectomy versus neoadjuvant chemotherapy followed by conservative surgery for patients with stage IB1 cervical cancer with tumors 2cm or larger: a literature review and analysis of oncological and obstetrical outcomes. Gynecol Oncol. 2015;137:574–580. doi: 10.1016/j.ygyno.2015.03.051. [DOI] [PubMed] [Google Scholar]
- 9.Downey K, Jafar M, Attygalle AD, et al. Influencing surgical management in patients with carcinoma of the cervix using a T2- and ZOOM-diffusion-weighted endovaginal MRI technique. Br J Cancer. 2013;109:615–622. doi: 10.1038/bjc.2013.375. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Singh N, Arif S. Histopathologic parameters of prognosis in cervical cancer—a review. Int J Gynecol Cancer. 2004;14:741–750. doi: 10.1111/j.1048-891X.2004.014504.x. [DOI] [PubMed] [Google Scholar]
- 11.Zaino RJ, Ward S, Delgado G, et al. Histopathologic predictors of the behavior of surgically treated stage IB squamous cell carcinoma of the cervix. A Gynecologic Oncology Group study. Cancer. 1992;69:1750–1758. doi: 10.1002/1097-0142(19920401)69:7<1750::aid-cncr2820690717>3.0.co;2-s. [DOI] [PubMed] [Google Scholar]
- 12.Kohler C, Mustea A, Marnitz S, et al. Perioperative morbidity and rate of upstaging after laparoscopic staging for patients with locally advanced cervical cancer: results of a prospective randomized trial. Am J Obstet Gynecol. 2015;213(503):e501–e507. doi: 10.1016/j.ajog.2015.05.026. [DOI] [PubMed] [Google Scholar]
- 13.Katanyoo K, Sanguanrungsirikul S, Manusirivithaya S. Comparison of treatment outcomes between squamous cell carcinoma and adenocarcinoma in locally advanced cervical cancer. Gynecol Oncol. 2012;125:292–296. doi: 10.1016/j.ygyno.2012.01.034. [DOI] [PubMed] [Google Scholar]
- 14.Downey K, Riches SF, Morgan VA, et al. Relationship between imaging biomarkers of stage I cervical cancer and poor-prognosis histologic features: quantitative histogram analysis of diffusion-weighted MR images. AJR Am J Roentgenol. 2013;200:314–320. doi: 10.2214/AJR.12.9545. [DOI] [PubMed] [Google Scholar]
- 15.Ries LAG, Krapcho M, Stinchcomb DG, Howlader N, Horner MJ, Mariotto A et al (2007) SEER Cancer Statistics Review, 1975-2005. National Cancer Institute, Bethesda
- 16.Cohen JG, Kapp DS, Shin JY, et al. Small cell carcinoma of the cervix: treatment and survival outcomes of 188 patients. Am J Obstet Gynecol. 2010;203(347):e341–e346. doi: 10.1016/j.ajog.2010.04.019. [DOI] [PubMed] [Google Scholar]
- 17.Mangler M, Lanowska M, Kohler C, Vercellino F, Schneider A, Speiser D. Pattern of cancer recurrence in 320 patients after radical vaginal trachelectomy. Int J Gynecol Cancer. 2014;24:130–134. doi: 10.1097/IGC.0000000000000012. [DOI] [PubMed] [Google Scholar]
- 18.Zhou Y, Liu J, Liu C, et al. Intravoxel incoherent motion diffusion weighted MRI of cervical cancer—correlated with tumor differentiation and perfusion. Magn Reson Imaging. 2016;34:1050–1056. doi: 10.1016/j.mri.2016.04.009. [DOI] [PubMed] [Google Scholar]
- 19.Dominietto M, Rudin M. Could magnetic resonance provide in vivo histology? Front Genet. 2014;4:298. doi: 10.3389/fgene.2013.00298. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Sala E, Rockall AG, Freeman SJ, Mitchell DG, Reinhold C. The added role of MR imaging in treatment stratification of patients with gynecologic malignancies: what the radiologist needs to know. Radiology. 2013;266:717–740. doi: 10.1148/radiol.12120315. [DOI] [PubMed] [Google Scholar]
- 21.Balleyguier C, Sala E, Da Cunha T, et al. Staging of uterine cervical cancer with MRI: guidelines of the European Society of Urogenital Radiology. Eur Radiol. 2011;21:1102–1110. doi: 10.1007/s00330-010-1998-x. [DOI] [PubMed] [Google Scholar]
- 22.Gladwish A, Milosevic M, Fyles A, et al. Association of apparent diffusion coefficient with disease recurrence in patients with locally advanced cervical cancer treated with radical chemotherapy and radiation therapy. Radiology. 2016;279:158–166. doi: 10.1148/radiol.2015150400. [DOI] [PubMed] [Google Scholar]
- 23.Hotker AM, Mazaheri Y, Aras O, et al. Assessment of prostate cancer aggressiveness by use of the combination of quantitative DWI and dynamic contrast-enhanced MRI. AJR Am J Roentgenol. 2016;206:756–763. doi: 10.2214/AJR.15.14912. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Dhanda S, Thakur M, Kerkar R, Jagmohan P. Diffusion-weighted imaging of gynecologic tumors: diagnostic pearls and potential pitfalls. Radiographics. 2014;34:1393–1416. doi: 10.1148/rg.345130131. [DOI] [PubMed] [Google Scholar]
- 25.Bammer R. Basic principles of diffusion-weighted imaging. Eur J Radiol. 2003;45:169–184. doi: 10.1016/s0720-048x(02)00303-0. [DOI] [PubMed] [Google Scholar]
- 26.Woo S, Kim SY, Cho JY, Kim SH. Preoperative evaluation of prostate cancer aggressiveness: using ADC and ADC ratio in determining Gleason Score. AJR Am J Roentgenol. 2016;207:114–120. doi: 10.2214/AJR.15.15894. [DOI] [PubMed] [Google Scholar]
- 27.Le Bihan D, Breton E, Lallemand D, Aubin ML, Vignaud J, Laval-Jeantet M. Separation of diffusion and perfusion in intravoxel incoherent motion MR imaging. Radiology. 1988;168:497–505. doi: 10.1148/radiology.168.2.3393671. [DOI] [PubMed] [Google Scholar]
- 28.Lee EY, Yu X, Chu MM, et al. Perfusion and diffusion characteristics of cervical cancer based on intraxovel incoherent motion MR imaging-a pilot study. Eur Radiol. 2014;24:1506–1513. doi: 10.1007/s00330-014-3160-7. [DOI] [PubMed] [Google Scholar]
- 29.Le Bihan D. Intravoxel incoherent motion perfusion MR imaging: a wake-up call. Radiology. 2008;249:748–752. doi: 10.1148/radiol.2493081301. [DOI] [PubMed] [Google Scholar]
- 30.Berman RM, Brown AM, Chang SD, et al. DCE MRI of prostate cancer. Abdom Radiol (NY) 2016;41:844–853. doi: 10.1007/s00261-015-0589-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Shweel MA, Abdel-Gawad EA, Abdel-Gawad EA, Abdelghany HS, Abdel-Rahman AM, Ibrahim EM. Uterine cervical malignancy: diagnostic accuracy of MRI with histopathologic correlation. J Clin Imaging Sci. 2012;2:42. doi: 10.4103/2156-7514.99175. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Chung HH, Kang SB, Cho JY, et al. Can preoperative MRI accurately evaluate nodal and parametrial invasion in early stage cervical cancer? Jpn J Clin Oncol. 2007;37:370–375. doi: 10.1093/jjco/hym036. [DOI] [PubMed] [Google Scholar]
- 33.Choi SH, Kim SH, Choi HJ, Park BK, Lee HJ. Preoperative magnetic resonance imaging staging of uterine cervical carcinoma: results of prospective study. J Comput Assist Tomogr. 2004;28:620–627. doi: 10.1097/01.rct.0000138007.77725.0a. [DOI] [PubMed] [Google Scholar]
- 34.Thomeer MG, Gerestein C, Spronk S, van Doorn HC, van der Ham E, Hunink MG. Clinical examination versus magnetic resonance imaging in the pretreatment staging of cervical carcinoma: systematic review and meta-analysis. Eur Radiol. 2013;23:2005–2018. doi: 10.1007/s00330-013-2783-4. [DOI] [PubMed] [Google Scholar]
- 35.Micco M, Sala E, Lakhman Y, Hricak H, Vargas HA. Role of imaging in the pretreatment evaluation of common gynecological cancers. Womens Health (Lond) 2014;10:299–321. doi: 10.2217/whe.14.19. [DOI] [PubMed] [Google Scholar]
- 36.Sahdev A, Sohaib SA, Wenaden AE, Shepherd JH, Reznek RH. The performance of magnetic resonance imaging in early cervical carcinoma: a long-term experience. Int J Gynecol Cancer. 2007;17:629–636. doi: 10.1111/j.1525-1438.2007.00829.x. [DOI] [PubMed] [Google Scholar]
- 37.Lien HH, Blomlie V, Iversen T, Trope C, Sundfor K, Abeler VM. Clinical stage I carcinoma of the cervix. Value of MR imaging in determining invasion into the parametrium. Acta Radiol. 1993;34:130–132. [PubMed] [Google Scholar]
- 38.Exner M, Kuhn A, Stumpp P, et al. Value of diffusion-weighted MRI in diagnosis of uterine cervical cancer: a prospective study evaluating the benefits of DWI compared to conventional MR sequences in a 3T environment. Acta Radiol. 2016;57:869–877. doi: 10.1177/0284185115602146. [DOI] [PubMed] [Google Scholar]
- 39.Park JJ, Kim CK, Park SY, Park BK. Parametrial invasion in cervical cancer: fused T2-weighted imaging and high-b-value diffusion-weighted imaging with background body signal suppression at 3 T. Radiology. 2015;274:734–741. doi: 10.1148/radiol.14140920. [DOI] [PubMed] [Google Scholar]
- 40.Downey K, Attygalle AD, Morgan VA, et al. Comparison of optimised endovaginal vs external array coil T2-weighted and diffusion-weighted imaging techniques for detecting suspected early stage (IA/IB1) uterine cervical cancer. Eur Radiol. 2016;26:941–950. doi: 10.1007/s00330-015-3899-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Valentini AL, Gui B, Micco M, et al. MRI anatomy of parametrial extension to better identify local pathways of disease spread in cervical cancer. Diagn Interv Radiol. 2016;22:319–325. doi: 10.5152/dir.2015.15282. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Kuang F, Yan Z, Wang J, Rao Z. The value of diffusion-weighted MRI to evaluate the response to radiochemotherapy for cervical cancer. Magn Reson Imaging. 2014;32:342–349. doi: 10.1016/j.mri.2013.12.007. [DOI] [PubMed] [Google Scholar]
- 43.Chopra S, Verma A, Kundu S, et al. Evaluation of diffusion-weighted imaging as a predictive marker for tumor response in patients undergoing chemoradiation for postoperative recurrences of cervical cancer. J Cancer Res Ther. 2012;8:68–73. doi: 10.4103/0973-1482.95177. [DOI] [PubMed] [Google Scholar]
- 44.Park JJ, Kim CK, Park SY, Park BK, Kim B. Value of diffusion-weighted imaging in predicting parametrial invasion in stage IA2-IIA cervical cancer. Eur Radiol. 2014;24:1081–1088. doi: 10.1007/s00330-014-3109-x. [DOI] [PubMed] [Google Scholar]
- 45.Hong KS, Ju W, Choi HJ, Kim JK, Kim MH, Cho KS. Differential diagnostic performance of magnetic resonance imaging in the detection of lymph node metastases according to the tumor size in early-stage cervical cancer patients. Int J Gynecol Cancer. 2010;20:841–846. doi: 10.1111/IGC.0b013e3181db5140. [DOI] [PubMed] [Google Scholar]
- 46.Park W, Park YJ, Huh SJ, et al. The usefulness of MRI and PET imaging for the detection of parametrial involvement and lymph node metastasis in patients with cervical cancer. Jpn J Clin Oncol. 2005;35:260–264. doi: 10.1093/jjco/hyi079. [DOI] [PubMed] [Google Scholar]
- 47.Manfredi R, Gui B, Giovanzana A, et al. Localized cervical cancer (stage <IIB): accuracy of MR imaging in planning less extensive surgery. Radiol Med. 2009;114:960–975. doi: 10.1007/s11547-009-0397-3. [DOI] [PubMed] [Google Scholar]
- 48.Reinhardt MJ, Ehritt-Braun C, Vogelgesang D, et al. Metastatic lymph nodes in patients with cervical cancer: detection with MR imaging and FDG PET. Radiology. 2001;218:776–782. doi: 10.1148/radiology.218.3.r01mr19776. [DOI] [PubMed] [Google Scholar]
- 49.Choi HJ, Roh JW, Seo SS, et al. Comparison of the accuracy of magnetic resonance imaging and positron emission tomography/computed tomography in the presurgical detection of lymph node metastases in patients with uterine cervical carcinoma: a prospective study. Cancer. 2006;106:914–922. doi: 10.1002/cncr.21641. [DOI] [PubMed] [Google Scholar]
- 50.Yang WT, Lam WW, Yu MY, Cheung TH, Metreweli C. Comparison of dynamic helical CT and dynamic MR imaging in the evaluation of pelvic lymph nodes in cervical carcinoma. AJR Am J Roentgenol. 2000;175:759–766. doi: 10.2214/ajr.175.3.1750759. [DOI] [PubMed] [Google Scholar]
- 51.Hawighorst H, Schoenberg SO, Knapstein PG, et al. Staging of invasive cervical carcinoma and of pelvic lymph nodes by high resolution MRI with a phased-array coil in comparison with pathological findings. J Comput Assist Tomogr. 1998;22:75–81. doi: 10.1097/00004728-199801000-00013. [DOI] [PubMed] [Google Scholar]
- 52.Scheidler J, Hricak H, Yu KK, Subak L, Segal MR. Radiological evaluation of lymph node metastases in patients with cervical cancer. A meta-analysis. JAMA. 1997;278:1096–1101. [PubMed] [Google Scholar]
- 53.Yoo SC, Kim WY, Yoon JH, et al. Accuracy of preoperative magnetic resonance imaging in assessing lymph node metastasis and myometrial invasion in patients with uterine cancer. Eur J Gynaecol Oncol. 2009;30:167–170. [PubMed] [Google Scholar]
- 54.Lv K, Guo HM, Lu YJ, Wu ZX, Zhang K, Han JK. Role of 18F-FDG PET/CT in detecting pelvic lymph-node metastases in patients with early-stage uterine cervical cancer: comparison with MRI findings. Nucl Med Commun. 2014;35:1204–1211. doi: 10.1097/MNM.0000000000000198. [DOI] [PubMed] [Google Scholar]
- 55.Shen G, Zhou H, Jia Z, Deng H. Diagnostic performance of diffusion-weighted MRI for detection of pelvic metastatic lymph nodes in patients with cervical cancer: a systematic review and meta-analysis. Br J Radiol. 2015;88:20150063. doi: 10.1259/bjr.20150063. [DOI] [PubMed] [Google Scholar]
- 56.He XQ, Wei LN. Diagnostic value of lymph node metastasis by diffusion-weighted magnetic resonance imaging in cervical cancer. J Cancer Res Ther. 2016;12:77–83. doi: 10.4103/0973-1482.148726. [DOI] [PubMed] [Google Scholar]
- 57.Liu Y, Liu H, Bai X, et al. Differentiation of metastatic from non-metastatic lymph nodes in patients with uterine cervical cancer using diffusion-weighted imaging. Gynecol Oncol. 2011;122:19–24. doi: 10.1016/j.ygyno.2011.03.023. [DOI] [PubMed] [Google Scholar]
- 58.Yu SP, He L, Liu B, Zhuang XZ, Liu MJ, Hu XS. Differential diagnosis of metastasis from non-metastatic lymph nodes in cervical cancers: pilot study of diffusion weighted imaging with background suppression at 3T magnetic resonance. Chin Med J (Engl) 2010;123:2820–2824. [PubMed] [Google Scholar]
- 59.Chen YB, Hu CM, Chen GL, Hu D, Liao J. Staging of uterine cervical carcinoma: whole-body diffusion-weighted magnetic resonance imaging. Abdom Imaging. 2011;36:619–626. doi: 10.1007/s00261-010-9642-4. [DOI] [PubMed] [Google Scholar]
- 60.Chen YB, Liao J, Xie R, Chen GL, Chen G. Discrimination of metastatic from hyperplastic pelvic lymph nodes in patients with cervical cancer by diffusion-weighted magnetic resonance imaging. Abdom Imaging. 2011;36:102–109. doi: 10.1007/s00261-009-9590-z. [DOI] [PubMed] [Google Scholar]
- 61.Choi EK, Kim JK, Choi HJ, et al. Node-by-node correlation between MR and PET/CT in patients with uterine cervical cancer: diffusion-weighted imaging versus size-based criteria on T2WI. Eur Radiol. 2009;19:2024–2032. doi: 10.1007/s00330-009-1350-5. [DOI] [PubMed] [Google Scholar]
- 62.Park SO, Kim JK, Kim KA, et al. Relative apparent diffusion coefficient: determination of reference site and validation of benefit for detecting metastatic lymph nodes in uterine cervical cancer. J Magn Reson Imaging. 2009;29:383–390. doi: 10.1002/jmri.21635. [DOI] [PubMed] [Google Scholar]
- 63.Kim JK, Kim KA, Park BW, Kim N, Cho KS. Feasibility of diffusion-weighted imaging in the differentiation of metastatic from nonmetastatic lymph nodes: early experience. J Magn Reson Imaging. 2008;28:714–719. doi: 10.1002/jmri.21480. [DOI] [PubMed] [Google Scholar]
- 64.Lin G, Ho KC, Wang JJ, et al. Detection of lymph node metastasis in cervical and uterine cancers by diffusion-weighted magnetic resonance imaging at 3T. J Magn Reson Imaging. 2008;28:128–135. doi: 10.1002/jmri.21412. [DOI] [PubMed] [Google Scholar]
- 65.Klerkx WM, Veldhuis WB, Spijkerboer AM, et al. The value of 3.0 tesla diffusion-weighted MRI for pelvic nodal staging in patients with early stage cervical cancer. Eur J Cancer. 2012;48:3414–3421. doi: 10.1016/j.ejca.2012.06.022. [DOI] [PubMed] [Google Scholar]
- 66.Nakai G, Matsuki M, Inada Y, et al. Detection and evaluation of pelvic lymph nodes in patients with gynecologic malignancies using body diffusion-weighted magnetic resonance imaging. J Comput Assist Tomogr. 2008;32:764–768. doi: 10.1097/RCT.0b013e318153fd43. [DOI] [PubMed] [Google Scholar]
- 67.Rizzo S, Calareso G, Maccagnoni S, et al. Pre-operative MR evaluation of features that indicate the need of adjuvant therapies in early stage cervical cancer patients. A single-centre experience. Eur J Radiol. 2014;83:858–864. doi: 10.1016/j.ejrad.2014.01.029. [DOI] [PubMed] [Google Scholar]
- 68.Gonzalez-Benitez C, Zapardiel I, Salas PI, Diestro MD, Hernandez A, De Santiago J. Nodal involvement evaluation in advanced cervical cancer: a single institutional experience. Eur J Gynaecol Oncol. 2013;34:138–141. [PubMed] [Google Scholar]
- 69.Choi HJ, Ju W, Myung SK, Kim Y. Diagnostic performance of computer tomography, magnetic resonance imaging, and positron emission tomography or positron emission tomography/computer tomography for detection of metastatic lymph nodes in patients with cervical cancer: meta-analysis. Cancer Sci. 2010;101:1471–1479. doi: 10.1111/j.1349-7006.2010.01532.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 70.Monteil J, Maubon A, Leobon S, et al. Lymph node assessment with (18)F-FDG-PET and MRI in uterine cervical cancer. Anticancer Res. 2011;31:3865–3871. [PubMed] [Google Scholar]
- 71.Kitajima K, Yamasaki E, Kaji Y, Murakami K, Sugimura K. Comparison of DWI and PET/CT in evaluation of lymph node metastasis in uterine cancer. World J Radiol. 2012;4:207–214. doi: 10.4329/wjr.v4.i5.207. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 72.Mirpour S, Mhlanga JC, Logeswaran P, Russo G, Mercier G, Subramaniam RM. The role of PET/CT in the management of cervical cancer. AJR Am J Roentgenol. 2013;201:W192–W205. doi: 10.2214/AJR.12.9830. [DOI] [PubMed] [Google Scholar]
- 73.Rockall AG, Sohaib SA, Harisinghani MG, et al. Diagnostic performance of nanoparticle-enhanced magnetic resonance imaging in the diagnosis of lymph node metastases in patients with endometrial and cervical cancer. J Clin Oncol. 2005;23:2813–2821. doi: 10.1200/JCO.2005.07.166. [DOI] [PubMed] [Google Scholar]
- 74.Atri M, Zhang Z, Marques H, et al. Utility of preoperative ferumoxtran-10 MRI to evaluate retroperitoneal lymph node metastasis in advanced cervical cancer: Results of ACRIN 6671/GOG 0233. Eur J Radiol Open. 2015;2:11–18. doi: 10.1016/j.ejro.2014.11.002. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 75.Laghi A, Paolantonio P, Panebianco V, et al. Decrease of signal intensity of myometrium and cervical stroma after ultrasmall superparamagnetic iron oxide (USPIO) particles administration: an MR finding with potential benefits in T staging of uterine neoplasms. Invest Radiol. 2004;39:666–670. doi: 10.1097/00004424-200411000-00004. [DOI] [PubMed] [Google Scholar]
- 76.Keller TM, Michel SC, Frohlich J, et al. USPIO-enhanced MRI for preoperative staging of gynecological pelvic tumors: preliminary results. Eur Radiol. 2004;14:937–944. doi: 10.1007/s00330-004-2258-8. [DOI] [PubMed] [Google Scholar]
- 77.Shi Q, Pisani LJ, Lee YK, et al. Evaluation of the novel USPIO GEH121333 for MR imaging of cancer immune responses. Contrast Media Mol Imaging. 2013;8:281–288. doi: 10.1002/cmmi.1526. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 78.Heijnen LA, Lambregts DM, Martens MH, et al. Performance of gadofosveset-enhanced MRI for staging rectal cancer nodes: can the initial promising results be reproduced? Eur Radiol. 2014;24:371–379. doi: 10.1007/s00330-013-3016-6. [DOI] [PubMed] [Google Scholar]
- 79.Naganawa S, Sato C, Kumada H, Ishigaki T, Miura S, Takizawa O. Apparent diffusion coefficient in cervical cancer of the uterus: comparison with the normal uterine cervix. Eur Radiol. 2005;15:71–78. doi: 10.1007/s00330-004-2529-4. [DOI] [PubMed] [Google Scholar]
- 80.Hoogendam JP, Klerkx WM, de Kort GA, et al. The influence of the b-value combination on apparent diffusion coefficient based differentiation between malignant and benign tissue in cervical cancer. J Magn Reson Imaging. 2010;32:376–382. doi: 10.1002/jmri.22236. [DOI] [PubMed] [Google Scholar]
- 81.Payne GS, Schmidt M, Morgan VA, et al. Evaluation of magnetic resonance diffusion and spectroscopy measurements as predictive biomarkers in stage 1 cervical cancer. Gynecol Oncol. 2010;116:246–252. doi: 10.1016/j.ygyno.2009.09.044. [DOI] [PubMed] [Google Scholar]
- 82.Chen J, Zhang Y, Liang B, Yang Z. The utility of diffusion-weighted MR imaging in cervical cancer. Eur J Radiol. 2010;74:e101–e106. doi: 10.1016/j.ejrad.2009.04.025. [DOI] [PubMed] [Google Scholar]
- 83.Kilickesmez O, Bayramoglu S, Inci E, Cimilli T, Kayhan A. Quantitative diffusion-weighted magnetic resonance imaging of normal and diseased uterine zones. Acta Radiol. 2009;50:340–347. doi: 10.1080/02841850902735858. [DOI] [PubMed] [Google Scholar]
- 84.Charles-Edwards EM, Messiou C, Morgan VA, et al. Diffusion-weighted imaging in cervical cancer with an endovaginal technique: potential value for improving tumor detection in stage Ia and Ib1 disease. Radiology. 2008;249:541–550. doi: 10.1148/radiol.2491072165. [DOI] [PubMed] [Google Scholar]
- 85.Xue HD, Li S, Sun F, et al. Clinical application of body diffusion weighted MR imaging in the diagnosis and preoperative N staging of cervical cancer. Chin Med Sci J. 2008;23:133–137. doi: 10.1016/s1001-9294(09)60027-4. [DOI] [PubMed] [Google Scholar]
- 86.McVeigh PZ, Syed AM, Milosevic M, Fyles A, Haider MA. Diffusion-weighted MRI in cervical cancer. Eur Radiol. 2008;18:1058–1064. doi: 10.1007/s00330-007-0843-3. [DOI] [PubMed] [Google Scholar]
- 87.Kuang F, Yan Z, Li H, Feng H. Diagnostic accuracy of diffusion-weighted MRI for differentiation of cervical cancer and benign cervical lesions at 3.0T: comparison with routine MRI and dynamic contrast-enhanced MRI. J Magn Reson Imaging. 2015;42:1094–1099. doi: 10.1002/jmri.24894. [DOI] [PubMed] [Google Scholar]
- 88.Mainenti PP, Pizzuti LM, Segreto S, et al. Diffusion volume (DV) measurement in endometrial and cervical cancer: a new MRI parameter in the evaluation of the tumor grading and the risk classification. Eur J Radiol. 2016;85:113–124. doi: 10.1016/j.ejrad.2015.10.014. [DOI] [PubMed] [Google Scholar]
- 89.Kuang F, Ren J, Zhong Q, Liyuan F, Huan Y, Chen Z. The value of apparent diffusion coefficient in the assessment of cervical cancer. Eur Radiol. 2013;23:1050–1058. doi: 10.1007/s00330-012-2681-1. [DOI] [PubMed] [Google Scholar]
- 90.Liu Y, Ye Z, Sun H, Bai R. Grading of uterine cervical cancer by using the ADC difference value and its correlation with microvascular density and vascular endothelial growth factor. Eur Radiol. 2013;23:757–765. doi: 10.1007/s00330-012-2657-1. [DOI] [PubMed] [Google Scholar]
- 91.Liu Y, Bai R, Sun H, Liu H, Wang D. Diffusion-weighted magnetic resonance imaging of uterine cervical cancer. J Comput Assist Tomogr. 2009;33:858–862. doi: 10.1097/RCT.0b013e31819e93af. [DOI] [PubMed] [Google Scholar]
- 92.Xue H, Ren C, Yang J, et al. Histogram analysis of apparent diffusion coefficient for the assessment of local aggressiveness of cervical cancer. Arch Gynecol Obstet. 2014;290:341–348. doi: 10.1007/s00404-014-3221-9. [DOI] [PubMed] [Google Scholar]
- 93.Winfield JM, Orton MR, Collins DJ et al (2016) Separation of type and grade in cervical tumours using non-mono-exponential models of diffusion-weighted MRI. Eur Radiol. doi:10.1007/s00330-016-4417-0 [DOI] [PMC free article] [PubMed]
- 94.Thoeny HC, Forstner R, De Keyzer F. Genitourinary applications of diffusion-weighted MR imaging in the pelvis. Radiology. 2012;263:326–342. doi: 10.1148/radiol.12110446. [DOI] [PubMed] [Google Scholar]
- 95.Donati OF. Chong D, Nanz D, et al. Diffusion-weighted MR imaging of upper abdominal organs: field strength and intervendor variability of apparent diffusion coefficients. Radiology. 2014;270:454–463. doi: 10.1148/radiol.13130819. [DOI] [PubMed] [Google Scholar]
- 96.Lee EY, Hui ES, Chan KK, et al. Relationship between intravoxel incoherent motion diffusion-weighted MRI and dynamic contrast-enhanced MRI in tissue perfusion of cervical cancers. J Magn Reson Imaging. 2015;42:454–459. doi: 10.1002/jmri.24808. [DOI] [PubMed] [Google Scholar]
- 97.Yamashita Y, Baba T, Baba Y, et al. Dynamic contrast-enhanced MR imaging of uterine cervical cancer: pharmacokinetic analysis with histopathologic correlation and its importance in predicting the outcome of radiation therapy. Radiology. 2000;216:803–809. doi: 10.1148/radiology.216.3.r00se07803. [DOI] [PubMed] [Google Scholar]
- 98.Schreuder SM, Lensing R, Stoker J, Bipat S. Monitoring treatment response in patients undergoing chemoradiotherapy for locally advanced uterine cervical cancer by additional diffusion-weighted imaging: a systematic review. J Magn Reson Imaging. 2015;42:572–594. doi: 10.1002/jmri.24784. [DOI] [PubMed] [Google Scholar]
- 99.Mahajan A, Engineer R, Chopra S, et al. Role of 3T multiparametric-MRI with BOLD hypoxia imaging for diagnosis and post therapy response evaluation of postoperative recurrent cervical cancers. Eur J Radiol Open. 2016;3:22–30. doi: 10.1016/j.ejro.2015.11.003. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 100.Lucas R, Lopes Dias J, Cunha TM. Added value of diffusion-weighted MRI in detection of cervical cancer recurrence: comparison with morphologic and dynamic contrast-enhanced MRI sequences. Diagn Interv Radiol. 2015;21:368–375. doi: 10.5152/dir.2015.14427. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 101.Erbay G, Onal C, Karadeli E, Guler OC, Arica S, Koc Z (2016) Predicting tumor recurrence in patients with cervical carcinoma treated with definitive chemoradiotherapy: value of quantitative histogram analysis on diffusion-weighted MR images. Acta Radiol. doi:10.1177/0284185116656492 [DOI] [PubMed]
- 102.Himoto Y, Fujimoto K, Kido A, et al. Pretreatment mean apparent diffusion coefficient is significantly correlated with event-free survival in patients with International Federation of Gynecology and Obstetrics stage Ib to IIIb cervical cancer. Int J Gynecol Cancer. 2015;25:1079–1085. doi: 10.1097/IGC.0000000000000445. [DOI] [PubMed] [Google Scholar]
- 103.Heo SH, Shin SS, Kim JW, et al. Pre-treatment diffusion-weighted MR imaging for predicting tumor recurrence in uterine cervical cancer treated with concurrent chemoradiation: value of histogram analysis of apparent diffusion coefficients. Korean J Radiol. 2013;14:616–625. doi: 10.3348/kjr.2013.14.4.616. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 104.Micco M, Vargas HA, Burger IA, et al. Combined pre-treatment MRI and 18F-FDG PET/CT parameters as prognostic biomarkers in patients with cervical cancer. Eur J Radiol. 2014;83:1169–1176. doi: 10.1016/j.ejrad.2014.03.024. [DOI] [PubMed] [Google Scholar]
- 105.Marconi DG, Fregnani JH, Rossini RR, et al. Pre-treatment MRI minimum apparent diffusion coefficient value is a potential prognostic imaging biomarker in cervical cancer patients treated with definitive chemoradiation. BMC Cancer. 2016;16:556. doi: 10.1186/s12885-016-2619-0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 106.Nakamura K, Joja I, Nagasaka T, et al. The mean apparent diffusion coefficient value (ADCmean) on primary cervical cancer is a predictive marker for disease recurrence. Gynecol Oncol. 2012;127:478–483. doi: 10.1016/j.ygyno.2012.07.123. [DOI] [PubMed] [Google Scholar]
- 107.Zhou G, Chen X, Tang F, Zhou J, Wang Y, Wang Z. The value of diffusion-weighted imaging in predicting the prognosis of stage IB-IIA cervical squamous cell carcinoma after radical hysterectomy. Int J Gynecol Cancer. 2016;26:361–366. doi: 10.1097/IGC.0000000000000613. [DOI] [PubMed] [Google Scholar]
- 108.Bae JM, Kim CK, Park JJ, Park BK. Can diffusion-weighted magnetic resonance imaging predict tumor recurrence of uterine cervical cancer after concurrent chemoradiotherapy? Abdom Radiol (NY) 2016;41:1604–1610. doi: 10.1007/s00261-016-0730-y. [DOI] [PubMed] [Google Scholar]
- 109.Das S, Chandramohan A, Reddy JK, et al. Role of conventional and diffusion weighted MRI in predicting treatment response after low dose radiation and chemotherapy in locally advanced carcinoma cervix. Radiother Oncol. 2015;117:288–293. doi: 10.1016/j.radonc.2015.10.006. [DOI] [PubMed] [Google Scholar]
- 110.Fu C, Bian D, Liu F, Feng X, Du W, Wang X. The value of diffusion-weighted magnetic resonance imaging in assessing the response of locally advanced cervical cancer to neoadjuvant chemotherapy. Int J Gynecol Cancer. 2012;22:1037–1043. doi: 10.1097/IGC.0b013e31825736d7. [DOI] [PubMed] [Google Scholar]
- 111.Kim HS, Kim CK, Park BK, Huh SJ, Kim B. Evaluation of therapeutic response to concurrent chemoradiotherapy in patients with cervical cancer using diffusion-weighted MR imaging. J Magn Reson Imaging. 2013;37:187–193. doi: 10.1002/jmri.23804. [DOI] [PubMed] [Google Scholar]
- 112.Liu Y, Sun H, Bai R, Ye Z. Time-window of early detection of response to concurrent chemoradiation in cervical cancer by using diffusion-weighted MR imaging: a pilot study. Radiat Oncol. 2015;10:185. doi: 10.1186/s13014-015-0493-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 113.Makino H, Kato H, Furui T, Morishige K, Kanematsu M. Predictive value of diffusion-weighted magnetic resonance imaging during chemoradiotherapy for uterine cervical cancer. J Obstet Gynaecol Res. 2014;40:1098–1104. doi: 10.1111/jog.12276. [DOI] [PubMed] [Google Scholar]
- 114.Nakamura K, Kajitani S, Joja I, et al. The posttreatment mean apparent diffusion coefficient of primary tumor is superior to pretreatment ADCmean of primary tumor as a predictor of prognosis with cervical cancer. Cancer Med. 2013;2:519–525. doi: 10.1002/cam4.100. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 115.Ni X, Tong Y, Xiao Y, Liao J, Chen Y, Wang M. Diffusion-weighted magnetic resonance imaging in predicting the radiosensitivity of cervical cancer. Int J Clin Exp Med. 2015;8:13836–13841. [PMC free article] [PubMed] [Google Scholar]
- 116.Onal C, Erbay G, Guler OC. Treatment response evaluation using the mean apparent diffusion coefficient in cervical cancer patients treated with definitive chemoradiotherapy. J Magn Reson Imaging. 2016;44:1010–1019. doi: 10.1002/jmri.25215. [DOI] [PubMed] [Google Scholar]
- 117.Park JJ, Kim CK, Park SY, et al. Assessment of early response to concurrent chemoradiotherapy in cervical cancer: value of diffusion-weighted and dynamic contrast-enhanced MR imaging. Magn Reson Imaging. 2014;32:993–1000. doi: 10.1016/j.mri.2014.05.009. [DOI] [PubMed] [Google Scholar]
- 118.Rizzo S, Buscarino V, Origgi D et al (2016) Evaluation of diffusion-weighted imaging (DWI) and MR spectroscopy (MRS) as early response biomarkers in cervical cancer patients. Radiol Med. doi:10.1007/s11547-016-0665-y [DOI] [PubMed]
- 119.Somoye G, Harry V, Semple S, et al. Early diffusion weighted magnetic resonance imaging can predict survival in women with locally advanced cancer of the cervix treated with combined chemo-radiation. Eur Radiol. 2012;22:2319–2327. doi: 10.1007/s00330-012-2496-0. [DOI] [PubMed] [Google Scholar]
- 120.Wang YC, Hu DY, Hu XM, et al. Assessing the early response of advanced cervical cancer to neoadjuvant chemotherapy using intravoxel incoherent motion diffusion-weighted magnetic resonance imaging: a pilot study. Chin Med J (Engl) 2016;129:665–671. doi: 10.4103/0366-6999.177995. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 121.Wu Y, Yu D, Bai XL, Zhu W, Su N. MRI in the synchronic chemoradiotherapy of cervical squamous cell carcinoma. Eur J Gynaecol Oncol. 2016;37:380–383. [PubMed] [Google Scholar]
- 122.Zhang Y, Chen JY, Xie CM, et al. Diffusion-weighted magnetic resonance imaging for prediction of response of advanced cervical cancer to chemoradiation. J Comput Assist Tomogr. 2011;35:102–107. doi: 10.1097/RCT.0b013e3181f6528b. [DOI] [PubMed] [Google Scholar]
- 123.Fu ZZ, Peng Y, Cao LY, Chen YS, Li K, Fu BH. Value of apparent diffusion coefficient (ADC) in assessing radiotherapy and chemotherapy success in cervical cancer. Magn Reson Imaging. 2015;33:516–524. doi: 10.1016/j.mri.2015.02.002. [DOI] [PubMed] [Google Scholar]
- 124.Fu C, Feng X, Bian D, et al. Simultaneous changes of magnetic resonance diffusion-weighted imaging and pathological microstructure in locally advanced cervical cancer caused by neoadjuvant chemotherapy. J Magn Reson Imaging. 2015;42:427–435. doi: 10.1002/jmri.24779. [DOI] [PubMed] [Google Scholar]
- 125.Levy A, Caramella C, Chargari C, et al. Accuracy of diffusion-weighted echo-planar MR imaging and ADC mapping in the evaluation of residual cervical carcinoma after radiation therapy. Gynecol Oncol. 2011;123:110–115. doi: 10.1016/j.ygyno.2011.06.009. [DOI] [PubMed] [Google Scholar]
- 126.Park JJ, Kim CK, Park BK. Prediction of disease progression following concurrent chemoradiotherapy for uterine cervical cancer: value of post-treatment diffusion-weighted imaging. Eur Radiol. 2016;26:3272–3279. doi: 10.1007/s00330-015-4156-7. [DOI] [PubMed] [Google Scholar]
- 127.Zhu L, Zhu L, Shi H, et al. Evaluating early response of cervical cancer under concurrent chemo-radiotherapy by intravoxel incoherent motion MR imaging. BMC Cancer. 2015;16:79. doi: 10.1186/s12885-016-2116-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 128.Fyles A, Milosevic M, Hedley D, et al. Tumor hypoxia has independent predictor impact only in patients with node-negative cervix cancer. J Clin Oncol. 2002;20:680–687. doi: 10.1200/JCO.2002.20.3.680. [DOI] [PubMed] [Google Scholar]
- 129.Zahra MA, Tan LT, Priest AN, et al. Semiquantitative and quantitative dynamic contrast-enhanced magnetic resonance imaging measurements predict radiation response in cervix cancer. Int J Radiat Oncol Biol Phys. 2009;74:766–773. doi: 10.1016/j.ijrobp.2008.08.023. [DOI] [PubMed] [Google Scholar]
- 130.Hameeduddin A, Sahdev A. Diffusion-weighted imaging and dynamic contrast-enhanced MRI in assessing response and recurrent disease in gynaecological malignancies. Cancer Imaging. 2015;15:3. doi: 10.1186/s40644-015-0037-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 131.Torheim T, Groendahl AR, Andersen EK et al (2016) Cluster analysis of dynamic contrast enhanced MRI reveals tumor subregions related to locoregional relapse for cervical cancer patients. Acta Oncol. doi:10.1080/0284186x.2016.1189091:1-5 [DOI] [PubMed]
- 132.Mayr NA, Yuh WT, Magnotta VA, et al. Tumor perfusion studies using fast magnetic resonance imaging technique in advanced cervical cancer: a new noninvasive predictive assay. Int J Radiat Oncol Biol Phys. 1996;36:623–633. doi: 10.1016/s0360-3016(97)85090-0. [DOI] [PubMed] [Google Scholar]
- 133.Lund KV, Simonsen TG, Hompland T, Kristensen GB, Rofstad EK. Short-term pretreatment DCE-MRI in prediction of outcome in locally advanced cervical cancer. Radiother Oncol. 2015;115:379–385. doi: 10.1016/j.radonc.2015.05.001. [DOI] [PubMed] [Google Scholar]
- 134.Halle C, Andersen E, Lando M, et al. Hypoxia-induced gene expression in chemoradioresistant cervical cancer revealed by dynamic contrast-enhanced MRI. Cancer Res. 2012;72:5285–5295. doi: 10.1158/0008-5472.CAN-12-1085. [DOI] [PubMed] [Google Scholar]
- 135.Andersen EK, Hole KH, Lund KV, et al. Pharmacokinetic parameters derived from dynamic contrast enhanced MRI of cervical cancers predict chemoradiotherapy outcome. Radiother Oncol. 2013;107:117–122. doi: 10.1016/j.radonc.2012.11.007. [DOI] [PubMed] [Google Scholar]
- 136.Andersen EK, Hole KH, Lund KV, et al. Dynamic contrast-enhanced MRI of cervical cancers: temporal percentile screening of contrast enhancement identifies parameters for prediction of chemoradioresistance. Int J Radiat Oncol Biol Phys. 2012;82:e485–e492. doi: 10.1016/j.ijrobp.2011.05.050. [DOI] [PubMed] [Google Scholar]
- 137.Hompland T, Lund KV, Ellingsen C, Kristensen GB, Rofstad EK. Peritumoral interstitial fluid flow velocity predicts survival in cervical carcinoma. Radiother Oncol. 2014;113:132–138. doi: 10.1016/j.radonc.2014.09.011. [DOI] [PubMed] [Google Scholar]
- 138.Andersen EK, Kristensen GB, Lyng H, Malinen E. Pharmacokinetic analysis and k-means clustering of DCEMR images for radiotherapy outcome prediction of advanced cervical cancers. Acta Oncol. 2011;50:859–865. doi: 10.3109/0284186X.2011.578586. [DOI] [PubMed] [Google Scholar]
- 139.Huang Z, Mayr NA, Lo SS, et al. Characterizing at-Risk Voxels by Using Perfusion Magnetic Resonance Imaging for Cervical Cancer during Radiotherapy. J Cancer Sci Ther. 2012;4:254–259. doi: 10.4172/1948-5956.1000151. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 140.Huang Z, Yuh KA, Lo SS, et al. Validation of optimal DCE-MRI perfusion threshold to classify at-risk tumor imaging voxels in heterogeneous cervical cancer for outcome prediction. Magn Reson Imaging. 2014;32:1198–1205. doi: 10.1016/j.mri.2014.08.039. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 141.Yuh WT, Mayr NA, Jarjoura D, et al. Predicting control of primary tumor and survival by DCE MRI during early therapy in cervical cancer. Invest Radiol. 2009;44:343–350. doi: 10.1097/RLI.0b013e3181a64ce9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 142.Mayr NA, Wang JZ, Zhang D, et al. Longitudinal changes in tumor perfusion pattern during the radiation therapy course and its clinical impact in cervical cancer. Int J Radiat Oncol Biol Phys. 2010;77:502–508. doi: 10.1016/j.ijrobp.2009.04.084. [DOI] [PubMed] [Google Scholar]
- 143.Mayr NA, Yuh WT, Jajoura D, et al. Ultra-early predictive assay for treatment failure using functional magnetic resonance imaging and clinical prognostic parameters in cervical cancer. Cancer. 2010;116:903–912. doi: 10.1002/cncr.24822. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 144.Mayr NA, Huang Z, Wang JZ, et al. Characterizing tumor heterogeneity with functional imaging and quantifying high-risk tumor volume for early prediction of treatment outcome: cervical cancer as a model. Int J Radiat Oncol Biol Phys. 2012;83:972–979. doi: 10.1016/j.ijrobp.2011.08.011. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 145.Hawighorst H, Knapstein PG, Knopp MV, et al. Uterine cervical carcinoma: comparison of standard and pharmacokinetic analysis of time-intensity curves for assessment of tumor angiogenesis and patient survival. Cancer Res. 1998;58:3598–3602. [PubMed] [Google Scholar]
- 146.Kim JH, Kim CK, Park BK, Park SY, Huh SJ, Kim B. Dynamic contrast-enhanced 3-T MR imaging in cervical cancer before and after concurrent chemoradiotherapy. Eur Radiol. 2012;22:2533–2539. doi: 10.1007/s00330-012-2504-4. [DOI] [PubMed] [Google Scholar]