

Abstract
Displaced tibial eminence fractures are commonly encountered in pediatric patients and are often considered to be functionally equivalent to an anterior cruciate ligament (ACL) rupture. While a variety of techniques are available for fixation of this injury, we describe an anchorless technique relying on suture fixation tied over a bone bridge. This technique also relies on two intra-articular Hewson suture passers to quickly and effectively pass and shuttle sutures through the ACL and tibial bone tunnels in order to reduce and fix the fracture fragment. We also briefly review various types of fixation used for tibial eminence fractures.
Displaced injuries of the tibial eminence may cause instability of the anterior cruciate ligament (ACL).1 These variants of an ACL injury can occur in pediatric and adult patients; however, the mechanism is often different in the 2 populations. In children and adolescents, injury occurs as a result of a sporting injury (similar to ACL tears in skeletally mature patients), while adults tend to obtain tibial eminence fractures during high-energy trauma such as a motor vehicle accident.2 In skeletally immature patients, the ACL is stronger than the incompletely ossified tibial eminence, leading to a bony avulsion when the knee is subjected to a valgus-external rotation force.1
Management of these injuries primarily depends on the amount of displacement of the fractured fragment.1 Nondisplaced or minimally displaced fractures can be treated with immobilization in a cast or splint, while surgical management is recommended when the avulsed tibial eminence is not anatomically reduced.1 Patients are assessed via plain radiographs, with magnetic resonance imaging used to further characterize the injury, amount of displacement, and possible involvement of the ACL. It is generally accepted that nondisplaced fractures, or fractures with only mild displacement of the anterior half of the tibial eminence, can be managed nonoperatively. Any fracture involving displacement of the entire tibial spine should undergo anatomic reduction and surgical fixation.3 Open treatment was described originally; however, with the advent of improved arthroscopic techniques, arthroscopic management has become increasingly common.4 Advantages of arthroscopy include smaller incisions, reduced soft-tissue damage, better pain control, quicker rehabilitation, ability to address concomitant intra-articular injuries such as meniscal tears, and ability to perform the surgery on an outpatient basis.1 A variety of methods for arthroscopic fixation have been described including Kirschner wires (K wires),5 staples,3 metal screws,6 suture anchors, and suture alone.2 We herein describe an arthroscopic anchorless technique that relies on suture fixation. A technique video is included for visual demonstration.
Surgical Technique
Please see accompanying Video 1.
Positioning and Portals
The patient is positioned supine on the operating table with the affected leg secured with a leg holder and the foot of the bed flexed down to allow the knee to bend freely. Standard anterolateral and anteromedial portals are made, and a diagnostic arthroscopy is performed. Because multiple transitions of camera and devices are often required, cannulas are recommended. In this case, the Arthrex PassPort Cannula (Arthrex, Naples, FL) is used in both portals.
Diagnostic Arthroscopy
It is important to begin the arthroscopy by lavaging out the joint, as hemarthrosis accompanies acute tibial spine fractures. The fracture bed is then gently explored, and any clotted blood or small, loose fragments of bone and soft tissue are carefully debrided, taking care not to comminute or unnecessarily thin the fragment (Fig 1).
Fig 1.
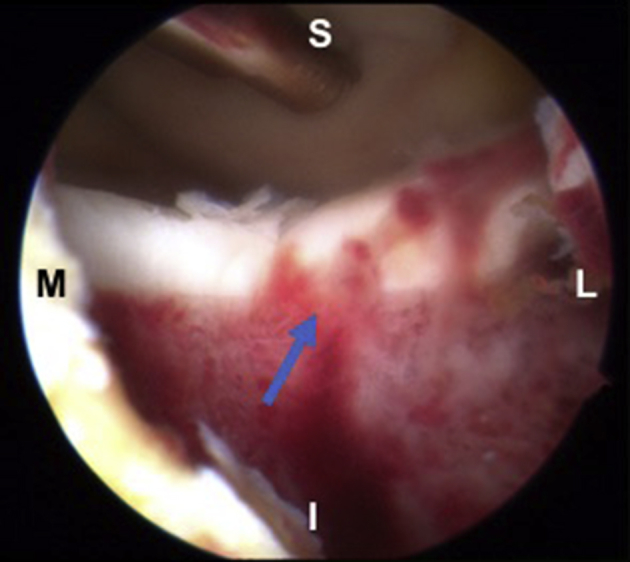
Viewing left knee from lateral portal. Fracture bed (blue arrow) preparation at the tibial fracture site following diagnostic arthroscopy. Standard patient orientation: top of image is toward the head (S), bottom is towards the foot (I), left side of image is medial (M), right is lateral (L).
Provisional Fixation
The anterior intermeniscal ligament can block reduction, and in order to retract it, a PDS suture is shuttled around the ligament by passing it through an 18-gauge spinal needle inferior to the ligament and shuttling it out the anteromedial portal. The suture ends are held with a snap to retract the ligament throughout the case. The fracture fragment is then reduced with an ACL guide and temporarily fixed with a 0.062-in K wire that is percutaneously placed from a superolateral trajectory (Fig 2). To drill the tibial bone tunnels, a 1.5-cm incision is made along the anteromedial tibial surface, and an ACL guide is inserted through the anteromedial portal under direct visualization.
Fig 2.
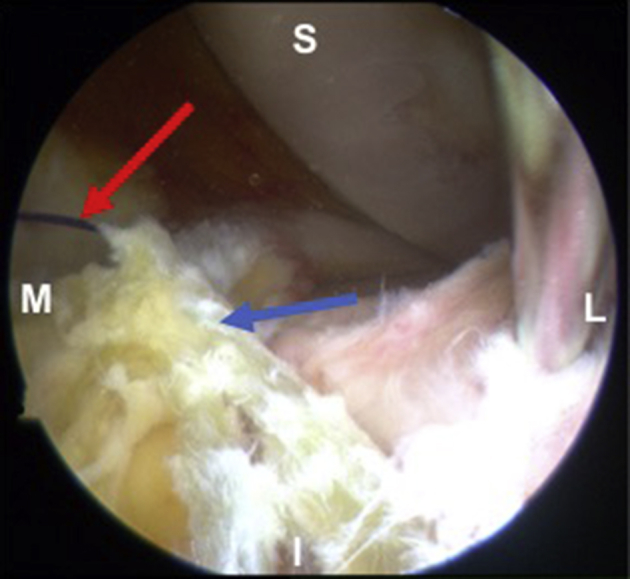
Viewing left knee from lateral portal. Assessment of tibial eminence reduction following insertion of K wire into the fracture fragment. Note the PDS stitch (red arrow) retracting intermeniscal ligament (blue arrow). Standard patient orientation: top of image is towards the head (S), bottom is towards the foot (I), left side of image is medial (M), right is lateral (L).
Preparation for Suture Passing
The tip of the ACL guide is placed just medial to the fracture fragment, approximately midway between the anterior and posterior aspect of the footprint. The ACL guide is secured against the anteromedial tibial surface at the medial aspect of the incision, and a pin is drilled. While taking care to avoid damaging the femoral condyles, the pin should be gently advanced and withdrawn multiple times to ensure a clear path. As soon as the guide pin is removed, a Hewson suture passer is advanced through the bone tunnel and maintained within the joint. The above process is repeated, now placing the ACL guide just lateral to the fracture fragment. A guide pin is drilled starting just laterally to the previously drilled tunnel through the same incision over the anteromedial tibia. This provides a bone bridge for later suture tying. A second Hewson suture passer is then advanced and maintained within the joint (Fig 3). A transpatellar portal is then made, and the arthroscope is inserted through this portal for the remainder of the case.
Fig 3.
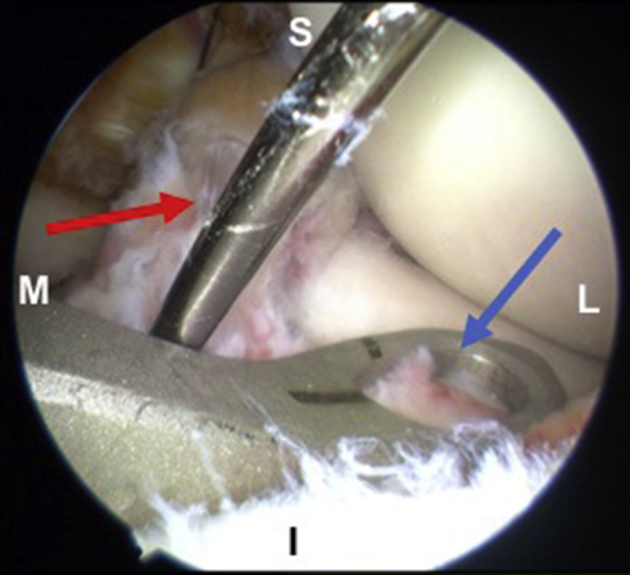
Viewing left knee from lateral portal. The anterior cruciate ligament (ACL) drill guide (blue arrow) is positioned both medially and laterally to the K wire (red arrow) in order to introduce a Hewson suture passer through the fracture fragment on both sides of the ACL. Standard patient orientation: top of image is towards the head (S), bottom is towards the foot (I), left side of image is medial (M), right is lateral (L).
Suture Passing
A 45o angled suture passer (Quickpass SutureLasso, Arthrex) is then used to pass sutures (no. 2 Tigerstick/Fiberstick, Arthrex) through the ACL from lateral to medial at the most distal aspect, just proximal to the bone fragment. These sutures are threaded through each Hewson suture passer in turn as they transition across the knee joint (Fig 4). When all sutures (2 to 3) have been passed, the ends should be evened and pulled through the tibial tunnels via the Hewson suture passers. Each suture is then individually tied over the bone bridge made by the anterior tibial cortex. The surgeon can reinsert the ACL guide to provide compression to the tibial spine fracture and ensure maintenance of fracture reduction while an assistant ties the sutures. The K wire is removed, fracture reduction is checked, and the knee is taken through a range of motion to assess fracture stability and anterior impingement in full extension (Fig 5). The knee and wounds are irrigated and closed.
Fig 4.
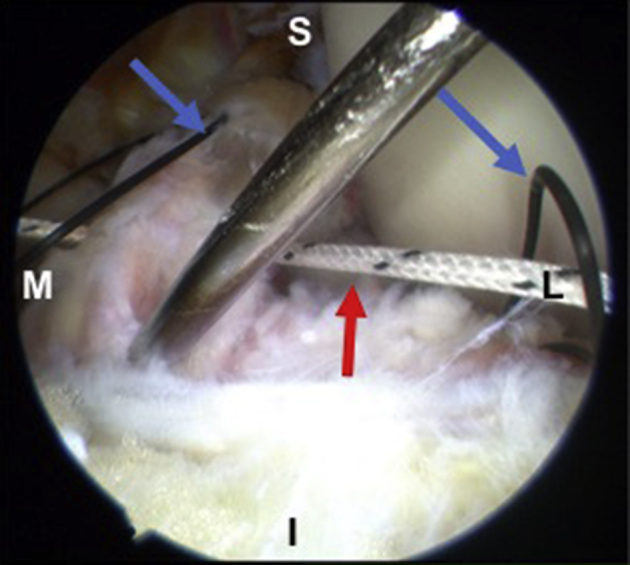
Viewing left knee from transpatellar portal. The first TigerStick (red arrow) suture is passed through both Hewson suture passers (blue arrows) and the ACL, using the fracture fragment as a bony bridge for reduction. Standard patient orientation: top of image is towards the head (S), bottom is towards the foot (I), left side of image is medial (M), right is lateral (L).
Fig 5.
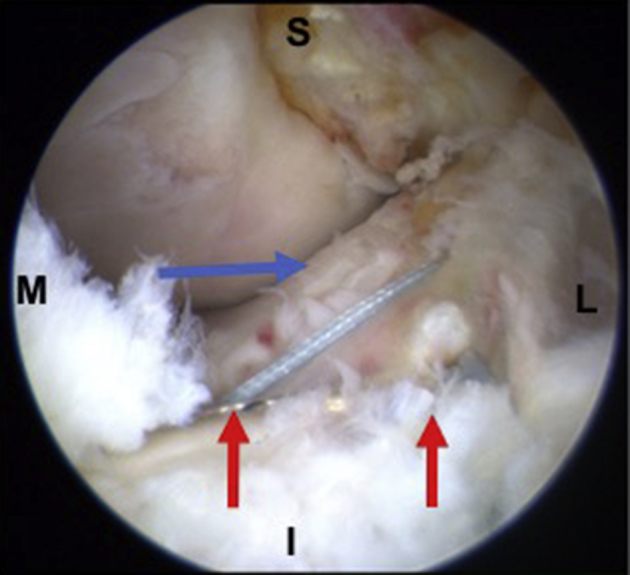
Viewing left knee from transpatellar portal. Final reduction of the tibial eminence via the anchorless double Hewson suture passer technique that we have described. The blue arrow shows the anterior cruciate ligament, while the red arrows show both limbs of the suture fixation. Standard patient orientation: top of image is towards the head (S), bottom is towards the foot (I), left side of image is medial (M), right is lateral (L).
Discussion
Our technique offers a reliable and effective method for arthroscopic repair of tibial eminence fractures without the need for suture anchors or any other type of intra-articular hardware (Table 1). One popular method for nonarthroscopic fixation involves reduction with K wires or cannulated screws.1 While this has proven to be an effective method of fixation, most investigators advocate for removal of the screws at approximately 6 to 12 months post operatively.7, 8, 9 Kocher et al. reported excellent clinical outcomes following cannulated screw fixation; however, the investigators noted that residual laxity of the ACL was present postoperatively.8 Arthroscopic suture anchor techniques are also popular. Vega et al. examined 7 patients who underwent fixation with a single, double-loaded suture anchor and had successful outcomes.10 One potential pitfall with a suture anchor technique, however, is the risk of either short-term or long-term pullout of the anchor; this risk is avoided with our technique. Cost may also be a consideration with suture anchor techniques.
Table 1.
Pearls and Pitfalls
| Pearls | Pitfalls |
|---|---|
| Retraction of the intermeniscal ligament with a PDS suture can aid visualization and prevent entrapment. | Inadequately tensioning the passed sutures used for fracture reduction can over-/underreduce the fracture fragment. |
| Use of arthroscopic cannulas helps avoid soft-tissue bridging and allows for quicker transfer of instruments. | Proper portal placement is essential to increase ease of suture passing. |
| Position loops of the Hewson suture passers in such a way that the angled suture passer can easily traverse both suture passers in one simple motion. | Skilled assistant is critical to drill bone tunnels, pass Hewson suture passers through the tunnels, and tie sutures. |
Anchorless techniques similar to ours have also been described in the literature. Ahn et al.11 performed suture fixation on 14 patients. At final follow-up, all patients had returned to athletics at their previous level. Additionally all patients had full range of motion, and 13/14 had negative Lachman tests. This technique differed from ours in that a PDS suture was passed through the ACL, after which drill holes in the tibia were made. An arthroscopic grasper was then passed through the drill holes, and each end of the suture was pulled through and tied.11 While this is an effective method, out technique eliminates the additional step of suture retrieval following suture passing because the 2 ends of the suture are already in the Hewson suture passers, which are passed through the tibial drill holes. Additionally, arthroscopic suture retrieval through the tibial drill holes may be difficult due to the amount of constraint encountered with an arthroscopic instrument in a bony drill hole. Huang et al. also describe a technique in which 4 PDS sutures are individually passed through 2 Hewson suture passers. The investigators then used the PDS as shuttle stitches for their final fixation.2 All 36 patients who underwent fixation with this technique went on to union within 3 months; additionally, no adverse effects such as loss of fixation or infection were reported.2
Our described technique has advantages as well as potential disadvantages compared with other fixation methods (Table 2). The technique described helps simplify suture management and minimize the steps needed to achieve fixation. Additionally, it obviates the need for intra-articular hardware and subsequent surgery for its removal. In patients with open physes, the described technique can be modified by using absorbable suture (e.g., PDS) instead of nonabsorbable suture. Alternatively, the technique can be modified to drill all-epiphyseal tunnels to avoid drilling across the physis.
Table 2.
Advantages and Disadvantages of Suture Fixation With Double Hewson Suture Passer
| Advantages | Disadvantages |
|---|---|
| Eliminates need for intra-articular hardware. | Passing suture through anterior cruciate ligament and 2 Hewson sutures simultaneously may be technically challenging. |
| Eliminates risk for suture anchor pullout in short and long term. | Fixation relies on using fracture fragment as bony bridge, may not hold reduction if fragment is comminuted. |
| Once suture is passed through Hewson suture passers, no further suture retrieval is required. | Misplacement of drill holes may lead to over-/underreduction. |
| Low cost: procedure could be completed simply with suture, eliminating need for implant associated cost. | Accessory incisions needed for tibial drill holes versus an all-inside suture anchor technique. |
| Good clinical evidence for positive outcomes with suture-only fixation.2, 1, 11 | |
| Can use nonabsorbable or absorbable sutures. |
Despite its ease of fracture reduction following suture passing, adequately threading the 45° suture passer through both Hewson suture passers and the ACL may be technically challenging. Comminuted fractures may also be difficult to control with this technique, although fixation of comminuted fractures with screws would also be challenging. While the authors agree that not every fracture may be amenable to this technique, we do believe that it is an efficient and effective method for treatment of tibial eminence fractures and is a suitable alternative fixation method for surgeons treating these injuries.
Footnotes
The authors report the following potential conflicts of interest or sources of funding: J.D.H. receives support from DePuy-Synthes. Full ICMJE author disclosure forms are available for this article online, as supplementary material.
Supplemental Data
Brief case presentation followed by technique for anchorless tibial eminence fracture fixation using the double Hewson suture passer technique. Following diagnostic arthroscopy of patient's left knee, the fracture site is debrided and preliminary reduction is obtained. Reduction is held with a K wire. An anterior cruciate ligament (ACL) drill guide is introduced, and drill holes are made both medially and laterally to the ACL within the fracture fragment in order to introduce the Hewson suture passers into the knee. A 45 degree suture passer is used to pass the TigerStick stitch from lateral to medial through the Hewson suture passers and the ACL. This step is repeated until adequate fixation is obtained (2 to 3 stitches). The Hewson suture passers are then withdrawn and the suture is tied over a bone bridge on the anterior tibial cortex.
References
- 1.Osti L., Buda M., Soldati F., Del Buono A., Osti R., Maffulli N. Arthroscopic treatment of tibial eminence fracture: A systematic review of different fixation methods. Br Med Bull. 2016;118:73–90. doi: 10.1093/bmb/ldw018. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Huang T.-W., Hsu K.-Y., Cheng C.-Y. Arthroscopic suture fixation of tibial eminence avulsion fractures. Arthroscopy. 2008;24:1232–1238. doi: 10.1016/j.arthro.2008.07.008. [DOI] [PubMed] [Google Scholar]
- 3.Kobayashi S., Terayama K. Arthroscopic reduction and fixation of a completely displaced fracture of the intercondylar eminence of the tibia. Arthroscopy. 1994;10:231–235. doi: 10.1016/s0749-8063(05)80100-8. [DOI] [PubMed] [Google Scholar]
- 4.Lubowitz J.H., Elson W.S., Guttmann D. Part II. Arthroscopic treatment of tibial plateau fractures: Intercondylar eminence avulsion fractures. Arthroscopy. 2005;21:86–92. doi: 10.1016/j.arthro.2004.09.031. [DOI] [PubMed] [Google Scholar]
- 5.McLennan J.G. The role of arthroscopic surgery in the treatment of fractures of the intercondylar eminence of the tibia. J Bone Joint Surg Br. 1982;64:477–480. doi: 10.1302/0301-620X.64B4.6896515. [DOI] [PubMed] [Google Scholar]
- 6.Senekovic V., Veselko M. Anterograde arthroscopic fixation of avulsion fractures of the tibial eminence with a cannulated screw: Five-year results. Arthroscopy. 2003;19:54–61. doi: 10.1053/jars.2003.50012. [DOI] [PubMed] [Google Scholar]
- 7.Reynders P., Reynders K., Broos P. Pediatric and adolescent tibial eminence fractures: Arthroscopic cannulated screw fixation. J Trauma. 2002;53:49–54. doi: 10.1097/00005373-200207000-00011. [DOI] [PubMed] [Google Scholar]
- 8.Kocher M.S., Foreman E.S., Micheli L.J. Laxity and functional outcome after arthroscopic reduction and internal fixation of displaced tibial spine fractures in children. Arthroscopy. 2003;19:1085–1090. doi: 10.1016/j.arthro.2003.10.014. [DOI] [PubMed] [Google Scholar]
- 9.Osti L., Merlo F., Liu S.H., Bocchi L. A simple modified arthroscopic procedure for fixation of displaced tibial eminence fractures. Arthroscopy. 2000;16:379–382. doi: 10.1016/s0749-8063(00)90082-3. [DOI] [PubMed] [Google Scholar]
- 10.Vega J.R., Irribarra L.A., Baar A.K., Iñiguez M., Salgado M., Gana N. Arthroscopic fixation of displaced tibial eminence fractures: A new growth plate-sparing method. Arthroscopy. 2008;24:1239–1243. doi: 10.1016/j.arthro.2008.07.007. [DOI] [PubMed] [Google Scholar]
- 11.Ahn J.H., Yoo J.C. Clinical outcome of arthroscopic reduction and suture for displaced acute and chronic tibial spine fractures. Knee Surg Sport Traumatol Arthrosc. 2005;13:116–121. doi: 10.1007/s00167-004-0540-6. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Brief case presentation followed by technique for anchorless tibial eminence fracture fixation using the double Hewson suture passer technique. Following diagnostic arthroscopy of patient's left knee, the fracture site is debrided and preliminary reduction is obtained. Reduction is held with a K wire. An anterior cruciate ligament (ACL) drill guide is introduced, and drill holes are made both medially and laterally to the ACL within the fracture fragment in order to introduce the Hewson suture passers into the knee. A 45 degree suture passer is used to pass the TigerStick stitch from lateral to medial through the Hewson suture passers and the ACL. This step is repeated until adequate fixation is obtained (2 to 3 stitches). The Hewson suture passers are then withdrawn and the suture is tied over a bone bridge on the anterior tibial cortex.