

Abstract
Horizontal cleavage meniscus tears are a common orthopedic injury often treated with partial or total meniscectomy versus repair. This Technical Note presents a technique for all-inside repair with uniform compression of the superior and inferior leaflets by placement of multiple circumferential compression stitches using an all-inside self-retrieving suture passing device. The currently described technique provides several advantages for all-inside repair of a horizontal cleavage tear: (1) eliminates the need for a posterior incision, (2) minimizes the risk of neurovascular injury, (3) uses standard arthroscopy portals (or small modifications), and (4) requires only a single suture deployment with a self-retrieving device for each circumferential compression stitch. The resulting circumferential stitch provides uniform compression to the superior and inferior leaflets, promoting meniscal healing. This configuration has been shown to have the highest load to failure of all repair patterns.
Horizontal cleavage tears are common, accounting for approximately 32% of all meniscus tears.1 Once thought to have minimal healing capacity, these tears have traditionally been treated with partial or total menisectomy.2 Growing evidence supporting the role of the meniscus in knee stability, load distribution, and arthritis prevention has led to an increased effort for meniscal preservation.3, 4, 5 Some horizontal cleavage tears may be suitable for repair, but multiplanar tears with avascular flaps are not repairable.
Partial meniscectomy with single leaflet resection has been recommended to relieve symptoms, preserve meniscal tissue, and create a stable construct.6 However, testing has shown minimal biomechanical benefit for single leaflet resection because the total contact area decreases by 82% and the peak contact pressure is similar to that of dual leaflet resection.7, 8 In contrast, horizontal cleavage repair can restore contact pressures to near normal levels.8
Various techniques for repair of horizontal cleavage meniscus tears have been described that use the principles of anatomic reduction, biologic stimulation, and circumferential compression.9, 10 This Technical Note will present a technique for uniform compression of the superior and inferior leaflets by placement of multiple circumferential compression stitches using an all-inside self-retrieving suture passing device.
Indications and Contraindications
Indications for repair of horizontal cleavage tears continue to expand. Repair has shown excellent outcomes with healing rates comparable to other tear patterns in healthy young patients.11 Candidates for repair are young adults (<50) with intact ligaments and no arthritis who have persistent pain despite a period of nonoperative management including activity modification and physiotherapy.12 Conversely, inferior outcomes have consistently been shown with increasing age.11, 13 Contraindications to repair include patients with advanced age, osteoarthritis, instability, and unwillingness to comply with the rehabilitation protocol.12 Multiplanar tears with avascular flaps that are unlikely to heal are treated with partial meniscectomy.
Surgical Technique
Patient Positioning and Visualization
In addition to standard arthroscopy instrumentation, additional specialized equipment is required to perform this technique (Table 1). The patient is positioned supine on the operating table. The lower extremity is prepped and draped in the usual sterile fashion. A standard superomedial outflow portal is established. The inferolateral and inferomedial portals are carefully positioned for easy viewing and instrument passage. The inferolateral portal is created 1 cm lateral to the patellar tendon just distal to the inferior pole of the patella. This superior and lateralized position will allow the self-retrieving suture passing device to clear the tibial spines to access the mid-body of the meniscus. A standard inferolateral portal can be established if desired, followed by creation of an accessory anterolateral portal as described. The inferomedial portal is created under needle localization ensuring easy access to the posterior aspect of the medial meniscus. A diagnostic arthroscopy is performed.
Table 1.
Equipment Required to Perform a Horizontal Cleavage Meniscus Repair With a Self-retrieving Suture Passing Device
| Special Equipment Required for Meniscus Repair |
| Arthroscopic Biter |
| Arthroscopic Rasp |
| Ceterix NovoStitch |
| Knot Pusher |
| All-inside Suture Cutter |
| PassPort Cannula (Arthrex, Naples, FL) |
Meniscus Preparation
The horizontal cleavage tear is identified and carefully probed to determine the anterior and posterior extent of the tear and the quality of the meniscal tissue (Video 1). The avascular, nonrepairable central rim and frayed portions of the superior and inferior leaflets are debrided using an arthroscopic biter and a shaver. Biologic augmentation is achieved at the tear site by aggressively rasping within the tear back to the level of the peripheral capsule to access the blood supply. It is critical to observe capsular bleeding before proceeding with meniscal repair (Fig 1).
Fig 1.

Arthroscopic image viewed from the anterolateral portal showing a horizontal tear of the left medial meniscus after mechanical stimulation (rasping) to promote bleeding for biologic augmentation.
Meniscus Repair With Circumferential Compression Stitches
Meniscal repair is performed in a posterior to anterior direction. A PassPort cannula (Arthrex, Naples, FL) is placed in the anteromedial portal to prevent soft-tissue bridging during knot tying. A suture is preloaded within the Ceterix Novostitch (Ceterix Orthopedics, Menlo Park, CA) self-retrieving suture passing device, which is advanced through the PassPort cannula to the posterior meniscus under arthroscopic visualization. The upper jaw is positioned over the superior leaflet of the meniscus tear with the tip of the instrument at the meniscocapsular junction. The lower jaw is then advanced under the inferior leaflet. The needle is then deployed advancing the suture limb beyond the meniscocapsular junction. The suture is retrieved by the upper jaw of the Ceterix suture passing device and carefully removed from the joint. An arthroscopic knot is tied with the assistance of a knot pusher at the meniscocapsular junction on the superior surface of the meniscus. Suture limbs are then cut using an arthroscopic cutter. The circumferential stitch applies uniform compression on the inferior and superior leaflets (Fig 2).
Fig 2.

Arthroscopic images of the medial compartment of a left knee. An anterolateral viewing portal shows placement of a circumferential compression stitch using the Ceterix Novostitch device through an anteromedial working portal. (A) The upper jaw is placed over the superior aspect of the meniscus and advanced to the meniscocapsular junction. (B) The lower jaw is advanced under the inferior leaflet of the meniscus tear. (C) After the suture has been passed through the meniscus with free limbs superior and inferior to the meniscus tear. (D) After the 2 suture limbs have been tied arthroscopically forming a circumferential compression stitch.
The tear is sequentially stabilized by placing similar circumferential compression stitches at 5 mm intervals. The empty suture cartridge is removed and replaced with a new cartridge before each stitch. As the repair advances anteriorly toward the mid-body of the meniscus, the ipsilateral portal will no longer allow the correct trajectory for suture placement. The PassPort cannula is removed from the ipsilateral portal and positioned in the contralateral portal to allow better trajectory to the body of the meniscus. The entire tear is repaired (Fig 3) and a probe is used to confirm the stability of the final construct (Fig 4). Several important pearls and pitfalls should be considered when repairing a horizontal cleavage tear with circumferential compression fixation (Table 2).
Fig 3.

Arthroscopic images of a medial meniscus horizontal cleavage repair in a left knee. (A) Viewing is from the anterolateral portal using the anteromedial portal for instrument passage while repairing the posterior third of the medial meniscus. (B) Viewing is from the anteromedial portal using the anterolateral portal for instrument passage while repairing the mid-body of the meniscus.
Fig 4.

Arthroscopic image viewing from the anteromedial portal with the probe inserted from the anterolateral portal showing repair of a horizontal cleavage meniscus tear in a left knee using circumferential compression stitches.
Table 2.
Pearls and Pitfalls of the Described Technique
| Pearls | Pitfalls |
|---|---|
| Aggressive meniscal rasping to achieve capsular bleeding. This will provide biologic augmentation to the repair site increasing the chance for meniscal healing | Failure to stimulate bleeding at the repair site |
| Accessory portals created under spinal needle localization allowing easy instrument passage over the tibial spine and under the femoral condyle | Instrumentation passage through standard portals resulting in iatrogenic cartilage damage |
| Advancing the Ceterix device to abut the peripheral capsule before deployment to circumferentially capture the entire tear | Failure to capture the entire tear within the circumferential compression stitch. This does not allow for compression of the peripheral meniscus at the tear site |
| PassPort cannula placement to prevent soft-tissue bridging during arthroscopic knot tying | Soft tissue bridging |
All arthroscopy equipment is removed. The portal incisions are closed with an absorbable suture followed by Steri-Strips, sterile gauze, and a compressive dressing. The knee is locked in full extension in a rehabilitation brace.
Rehabilitation
Weeks 0 to 4
A knee immobilizer is worn during ambulation; partial weight bearing using crutches with the knee in full extension; antiedema strategies; range of motion exercises; and core and lower extremity strengthening exercises. Range of motion is limited to 90° to avoid stress on the posterior horn repair with femoral rollback.
Weeks 4 to 8
Discontinue the knee immobilizer; progress to weight bearing as tolerated (wean crutches); continue range of motion exercises, gait training, and core and lower extremity strengthening exercises. Range of motion is increased as tolerated, but no loading at flexion angles greater than 90°.
Weeks 8 to 16
Proprioceptive training; core and lower extremity strengthening exercises; nonimpact aerobic conditioning when walking with normal gait mechanics. No loading at flexion angles greater than 90°.
Four Months
Initiation of return to sport program. No restrictions.
Discussion
Horizontal cleavage meniscus tears are a common orthopedic injury1 that are often treated with a partial or total meniscectomy.2 This is likely due to the long-held belief that horizontal cleavage tears have minimal capacity to heal. However, clinical reports on horizontal cleavage tear repair have challenged this belief by showing good results.14, 15 A clinical healing rate of 78% was reported in a recent systematic review examining 9 independent studies.11 The authors concluded that the healing rate after horizontal cleavage tear repair is similar to repair of other tear patterns.
Several techniques have been described for repair of horizontal cleavage meniscus tears including open, inside-out, and all-inside repairs.9, 10, 15 All-inside repairs provide the advantages of decreased needle stick injury, reduced surgical time, and less technical difficulty when compared with an inside-out technique.16, 17, 18 Furthermore, no difference in functional outcomes, complications, or overall failure rate has been shown.16, 17, 18 The introduction of self-retrieving suture passing devices such as the Ceterix Novostitch and Knee Scorpion (Arthrex) has expanded the indications for all-inside repair enabling circumferential compression stitch formation with a single deployment of the instrument. The resulting circumferential stitch provides uniform compression to the superior and inferior leaflets, promoting meniscal healing (Fig 5). This configuration has also been shown to have the highest load to failure of all repair patterns.19
Fig 5.
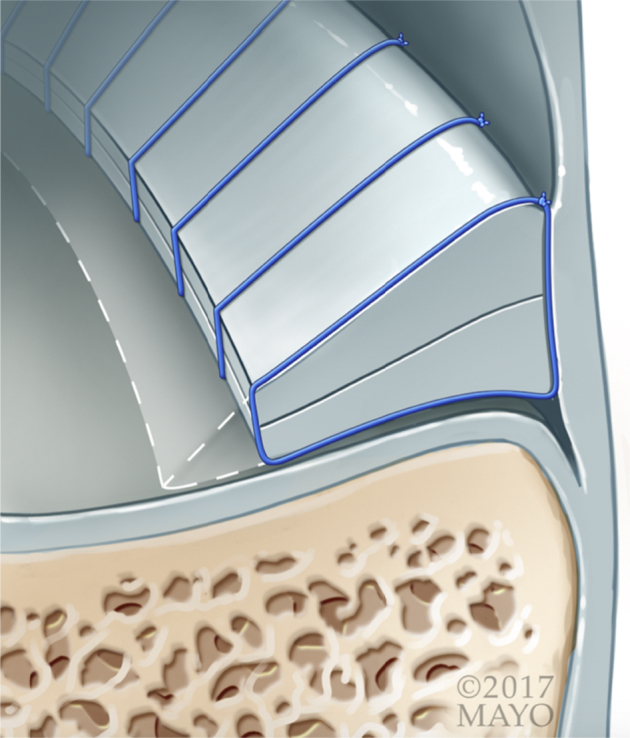
Schematic image showing the concept of circumferential compression stitch fixation for the treatment of a horizontal cleavage meniscus tear.
The currently described technique provides several advantages for all-inside repair of a horizontal cleavage tear (Table 3): (1) eliminates the need for a posterior incision, (2) minimizes the risk of neurovascular injury, (3) uses standard arthroscopy portals (or small modifications), and (4) requires only a single suture deployment with a self-retrieving device for each circumferential compression stitch. Limitations of the described technique include increased direct cost associated with the self-retrieving suture passing device and the need for arthroscopic knot tying that increases the technical difficulty of the procedure. Patient selection is paramount because this technique is not suitable for degenerative meniscal tears and arthritis due to poor outcomes in this patient population.11, 13
Table 3.
Advantages and Disadvantages of the Described Technique
| Advantages | Disadvantages |
|---|---|
| Preserves meniscal tissue when compared with resection | Requires arthroscopic knot tying |
| Only a single deployment of the instrument is required to place circumferential compression stitches | Risk of chondral damage with passage of a suture passing device |
| Does not require a posterior incision | Increased direct operative cost |
Footnotes
The authors report the following potential conflicts of interest or sources of funding: A.J.K. receives consultancy fees from Arthrex; has grants/grants pending from Arthritis Foundation, Ceterix, and Histogenics; and receives payment for lectures including service on speakers bureaus from Arthrex. D.B.F.S. is a member of the editorial or governing board of Cartilage; receives consultancy fees from Cartiheal, Smith & Nephew, and Vericel (paid consultant); and grants/grants pending from Arthrex, Ivy Sports, and Smith & Nephew (research support). M.J.S. is a board member of American Journal of Sports Medicine; receives consultancy fees from Arthrex; and has grants/grants pending from Stryker. Full ICMJE author disclosure forms are available for this article online, as supplementary material.
Supplementary Data
The patient is positioned supine and a horizontal cleavage medial meniscus tear in a left knee is repaired using the Ceterix self-retrieving suture passing device. The anterolateral portal is used for viewing, whereas the anteromedial portal is the working portal during repair of the posterior third of the meniscus. The meniscus is prepared using mechanical stimulation to promote bleeding from biologic augmentation at the tear site. This is performed using a combination of a rasp and a shaver. Mechanical stimulation is performed peripherally to the level of the capsule. After the meniscus has been prepared, a self-retrieving suture passing device is advanced through the anteromedial portal and a stitch is passed at the meniscocapsular junction. The suture is captured and removed from the joint surrounding the inferior and superior leaflets of the horizontal meniscus tear. An arthroscopic knot is tied over the superior aspect of the meniscus uniformly compressing the meniscus tear. An arthroscopic suture cutter is used to remove the free ends of the suture. Sequential sutures are placed at 5 mm increments. Each suture is placed with the suture passing device oriented perpendicular to the meniscus. As the repair advances anteriorly, this requires alternating the portals to view from the anteromedial portal while passing sutures throughout the anterolateral portal. After stabilizing the tear, a probe is inserted to confirm that the inferior and superior leaflets have been compressed and that the meniscus is stable. Circumferential compression stitches are placed at 5 mm intervals through the posterior third and mid-body of the meniscus.
References
- 1.Metcalf M.H., Barrett G.R. Prospective evaluation of 1485 meniscal tear patterns in patients with stable knees. Am J Sports Med. 2004;32:675–680. doi: 10.1177/0095399703258743. [DOI] [PubMed] [Google Scholar]
- 2.Yim J.H., Seon J.K., Song E.K. A comparative study of meniscectomy and nonoperative treatment for degenerative horizontal tears of the medial meniscus. Am J Sports Med. 2013;41:1565–1570. doi: 10.1177/0363546513488518. [DOI] [PubMed] [Google Scholar]
- 3.Nelson C.G., Bonner K.F. Inside-out meniscus repair. Arthrosc Tech. 2013;2:e453–e460. doi: 10.1016/j.eats.2013.07.006. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Shoemaker S.C., Markolf K.L. The role of the meniscus in the anterior-posterior stability of the loaded anterior cruciate-deficient knee. Effects of partial versus total excision. J Bone Joint Surg Am. 1986;68:71–79. [PubMed] [Google Scholar]
- 5.Hede A., Larsen E., Sandberg H. The long term outcome of open total and partial meniscectomy related to the quantity and site of the meniscus removed. Int Orthop. 1992;16:122–125. doi: 10.1007/BF00180200. [DOI] [PubMed] [Google Scholar]
- 6.Kim J.G., Lee S.Y., Chay S., Lim H.C., Bae J.H. Arthroscopic meniscectomy for medial meniscus horizontal cleavage tears in patients under age 45. Knee Surg Relat Res. 2016;28:225–232. doi: 10.5792/ksrr.2016.28.3.225. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Haemer J.M., Wang M.J., Carter D.R., Giori N.J. Benefit of single-leaf resection for horizontal meniscus tear. Clin Orthop Relat Res. 2007;457:194–202. doi: 10.1097/BLO.0b013e3180303b5c. [DOI] [PubMed] [Google Scholar]
- 8.Koh J.L., Yi S.J., Ren Y., Zimmerman T.A., Zhang L.Q. Tibiofemoral contact mechanics with horizontal cleavage tear and resection of the medial meniscus in the human knee. J Bone Joint Surg Am. 2016;98:1829–1836. doi: 10.2106/JBJS.16.00214. [DOI] [PubMed] [Google Scholar]
- 9.Saliman J.D. The circumferential compression stitch for meniscus repair. Arthrosc Tech. 2013;2:e257–e264. doi: 10.1016/j.eats.2013.02.016. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Pujol N., Bohu Y., Boisrenoult P., Macdes A., Beaufils P. Clinical outcomes of open meniscal repair of horizontal meniscal tears in young patients. Knee Surg Sports Traumatol Arthrosc. 2013;21:1530–1533. doi: 10.1007/s00167-012-2099-y. [DOI] [PubMed] [Google Scholar]
- 11.Kurzweil P.R., Lynch N.M., Coleman S., Kearney B. Repair of horizontal meniscus tears: A systematic review. Arthroscopy. 2014;30:1513–1519. doi: 10.1016/j.arthro.2014.05.038. [DOI] [PubMed] [Google Scholar]
- 12.Hutchinson I.D., Moran C.J., Potter H.G., Warren R.F., Rodeo S.A. Restoration of the meniscus: Form and function. Am J Sports Med. 2014;42:987–998. doi: 10.1177/0363546513498503. [DOI] [PubMed] [Google Scholar]
- 13.Tengrootenhuysen M., Meermans G., Pittoors K., van Riet R., Victor J. Long-term outcome after meniscal repair. Knee Surg Sports Traumatol Arthrosc. 2011;19:236–241. doi: 10.1007/s00167-010-1286-y. [DOI] [PubMed] [Google Scholar]
- 14.Accadbled F., Cassard X., Sales de Gauzy J., Cahuzac J.P. Meniscal tears in children and adolescents: Results of operative treatment. J Pediatr Orthop B. 2007;16:56–60. doi: 10.1097/BPB.0b013e328010b707. [DOI] [PubMed] [Google Scholar]
- 15.Rubman M.H., Noyes F.R., Barber-Westin S.D. Arthroscopic repair of meniscal tears that extend into the avascular zone. A review of 198 single and complex tears. Am J Sports Med. 1998;26:87–95. doi: 10.1177/03635465980260013301. [DOI] [PubMed] [Google Scholar]
- 16.Grant J.A., Wilde J., Miller B.S., Bedi A. Comparison of inside-out and all-inside techniques for the repair of isolated meniscal tears: A systematic review. Am J Sports Med. 2012;40:459–468. doi: 10.1177/0363546511411701. [DOI] [PubMed] [Google Scholar]
- 17.Fillingham Y.A., Riboh J.C., Erickson B.J., Bach B.R., Jr., Yanke A.B. Inside-out versus all-inside repair of isolated meniscal tears. Am J Sports Med. 2017;45:234–242. doi: 10.1177/0363546516632504. [DOI] [PubMed] [Google Scholar]
- 18.Ayeni O., Peterson D., Chan K., Javidan A., Gandhi R. Suture repair versus arrow repair for symptomatic meniscus tears of the knee: A systematic review. J Knee Surg. 2012;25:397–402. doi: 10.1055/s-0032-1313752. [DOI] [PubMed] [Google Scholar]
- 19.Aşík M., Sener N. Failure strength of repair devices versus meniscus suturing techniques. Knee Surg Sports Traumatol Arthrosc. 2002;10:25–29. doi: 10.1007/s001670100247. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
The patient is positioned supine and a horizontal cleavage medial meniscus tear in a left knee is repaired using the Ceterix self-retrieving suture passing device. The anterolateral portal is used for viewing, whereas the anteromedial portal is the working portal during repair of the posterior third of the meniscus. The meniscus is prepared using mechanical stimulation to promote bleeding from biologic augmentation at the tear site. This is performed using a combination of a rasp and a shaver. Mechanical stimulation is performed peripherally to the level of the capsule. After the meniscus has been prepared, a self-retrieving suture passing device is advanced through the anteromedial portal and a stitch is passed at the meniscocapsular junction. The suture is captured and removed from the joint surrounding the inferior and superior leaflets of the horizontal meniscus tear. An arthroscopic knot is tied over the superior aspect of the meniscus uniformly compressing the meniscus tear. An arthroscopic suture cutter is used to remove the free ends of the suture. Sequential sutures are placed at 5 mm increments. Each suture is placed with the suture passing device oriented perpendicular to the meniscus. As the repair advances anteriorly, this requires alternating the portals to view from the anteromedial portal while passing sutures throughout the anterolateral portal. After stabilizing the tear, a probe is inserted to confirm that the inferior and superior leaflets have been compressed and that the meniscus is stable. Circumferential compression stitches are placed at 5 mm intervals through the posterior third and mid-body of the meniscus.