

Abstract
Treatment intensification to maximize disease control and reduced intensity approaches to minimize the risk of late sequelae have been evaluated in newly diagnosed Hodgkin lymphoma. The influence of these interventions on the risk of secondary malignant neoplasms, progression-free survival and overall survival is reported in the meta-analysis herein, based on individual patient data from 9498 patients treated within 16 randomized controlled trials for newly diagnosed Hodgkin lymphoma between 1984 and 2007. Secondary malignant neoplasms were meta-analyzed using Peto’s method as time-to-event outcomes. For progression-free and overall survival, hazard ratios derived from each trial using Cox regression were combined by inverse-variance weighting. Five study questions (combined-modality treatment vs. chemotherapy alone; more extended vs. involved-field radiotherapy; radiation at higher doses vs. radiation at 20 Gy; more vs. fewer cycles of the same chemotherapy protocol; standard-dose chemotherapy vs. intensified chemotherapy) were investigated. After a median follow-up of 7.4 years, dose-intensified chemotherapy resulted in better progression-free survival rates (P=0.007) as compared with standard-dose chemotherapy, but was associated with an increased risk of therapy-related acute myeloid leukemia/myelodysplastic syndromes (P=0.0028). No progression-free or overall survival differences were observed between combined-modality treatment and chemotherapy alone, but more secondary malignant neoplasms were seen after combined-modality treatment (P=0.010). For the remaining three study questions, outcomes and secondary malignancy rates did not differ significantly between treatment strategies. The results of this meta-analysis help to weigh up efficacy and secondary malignancy risk for the choice of first-line treatment for Hodgkin lymphoma patients. However, final conclusions regarding secondary solid tumors require longer follow-up.
Introduction
Hodgkin lymphoma (HL) is a lymphoid malignancy with an incidence of 3-4/100 000/year. Young adults are most often affected.1 At present, about 80% of patients achieve long-term remission after treatment with multi-agent chemotherapy optionally followed by radiotherapy (RT).2 Given the mostly young age at diagnosis and the excellent long-term prognosis, therapy-related late effects including secondary malignant neoplasms (SMN), cardiovascular disease and infertility have become increasingly important.3–6 Several recent clinical trials evaluated the possibility of reducing toxicity by limiting chemotherapy and RT without compromising efficacy.2 Conversely, some studies for patients with newly diagnosed advanced HL investigated intensified chemotherapy protocols to improve the clinical outcome of high-risk patients.2
SMN are divided into secondary hematological malignancies including therapy-related acute myeloid leukemia/myelodysplastic syndromes (t-AML/MDS) and secondary non-Hodgkin lymphomas (NHL) and the heterogeneous group of secondary solid tumors. An association between the use of alkylating agents and topoisomerase II inhibitors and the development of t-AML/MDS has been demonstrated.7–9 Both drug classes are included in first-line chemotherapy protocols such as adriamycin, bleomycin, vinblastine and dacarbazine (ABVD), bleomycin, etoposide, doxorubicin, cyclophosphamide, vincristine, procarbazine, and prednisone escalated (BEA-COPP) and vinblastine, doxorubicin, vincristine, bleomycin, mustard, etoposide, and prednisone (Stanford V).10–12 For secondary NHL, such associations have not been identified.13 The time interval between HL treatment and the occurrence of secondary hematological malignancies is usually short, ranging between four and ten years in most cases.9,13 In contrast, the risk of secondary solid tumors remains significantly increased for up to 25 years and more.3,4
In the meta-analysis herein, using individual patient data (IPD), SMN, progression-free survival (PFS) and overall survival (OS) of patients treated in randomized clinical trials comparing different treatment approaches (combined-modality treatment (CMT) vs. chemotherapy alone; more extended radiotherapy (RT) vs. involved-field RT (IF-RT); RT at higher doses vs. RT at 20 Gy; more vs. fewer cycles of the same chemotherapy protocol; standard-dose chemotherapy vs. intensified chemotherapy) were investigated. Acceptable chemotherapy regimens were ABVD or similar (e.g., mechlorethamine, vincristine, procarbazine and prednisone/doxorubicin, bleomycin and vincristine [MOPP/ABV]) or (for the last study question above) any dose-intensified chemotherapy randomly compared with a standard dose ABVD-like regimen.
Methods
Searches for randomized clinical trials including patients with newly diagnosed HL that compared treatment approaches according to the mentioned study questions and published from 1984 onwards were performed in March 2010 using the electronic literature databases Medline and Cochrane Central. Reference lists of all relevant retrieved publications and previous meta-analyses were searched. All identified articles were screened independently by two authors. Trials had to have enrolled at least 50 patients per treatment group and to have finished recruitment before or during 2007, to avoid trials with inadequate follow-up. Searches were repeated in April 2015.
IPD were requested from the investigators of the eligible trials, including birth date, sex, HL diagnosis date, stage at diagnosis, presence of B symptoms, randomization date, allocated treatment, remission status after first-line treatment, relapse date, date and type of SMN, death date and last follow-up date concerning clinical outcome and vital status.
Statistical methods
For quality control, each trial included in the meta-analysis was initially analyzed separately, comparing the treatment arms with respect to recruitment times, patient characteristics, complete remission rates, follow-up duration, PFS, OS and time to SMN. Results were compared with previous trial publications and inconsistencies were queried. Risk of bias was assessed for each trial according to the Cochrane recommendations.14 To assess completeness of follow-up, the median observation time was calculated using the Kaplan-Meier method with reverse censoring at death. The distribution of last information dates was quantified using the interquartile range of the dates of last information (IQR-DLI). This range includes the central 50% of last information dates and thus represents the extent to which patients in a given study are lost to follow up over a broad time interval. Large IQR-DLI values (absolute or relative to median follow-up) suggest poorer quality of follow up.
Randomized comparisons for each study question were combined across the appropriate trials to obtain a pooled Peto’s odds ratio (OR) for SMN rates, with 95% confidence intervals (CI).15,16 Three types of SMN, i.e., t-AML/MDS, secondary NHL and secondary solid tumors were also analyzed separately.
Subgroup analyses were performed to investigate whether the SMN rates depended upon the stage according to Ann Arbor classification (early stages I and II vs. advanced stages III and IV), age (≤50 years vs. >50 years) and sex. Treatment subgroups were defined for the intensified chemotherapy question only (escalated BEACOPP vs. Stanford V vs. epidoxirubicin, bleomycin, and vinblastine/lomustine, doxorubicin, and vindesine (EBV/CAD)-based vs. chlorambucil, vinblastine, prednisolone and procarbazine (ChlVPP)-based). Results were displayed chronologically by recruitment period in order to reveal time period effects.
Sensitivity analyses were conducted excluding SMN that had occurred after HL recurrence: follow-up times were censored at HL recurrence. Further sensitivity analyses were performed as follows: firstly, SMN data were analyzed using a one-step Cox proportional hazards regression, stratified by trial, secondly, analyses were repeated with the exclusion of the less complete follow-up periods in each trial, censoring at the date at which 75% of surviving patients in the particular trial were still being followed, thirdly, overall SMN and separate secondary solid tumor analyses were repeated excluding non-melanoma skin cancers (NMSC), and finally, the cumulative incidence method, which considers non-SMN death as a competing risk, was employed.17,18
All analyses were performed in SAS (version 9.3) and RevMan (version 5.2).
Results
Results of the search
A total of 3515 references (excluding duplicates) published after 1984 were identified in 2010 and reviewed for eligibility. The majority did not meet the predefined criteria and were excluded for the following reasons: 1419 references did not concern HL patients, 1162 did not report a clinical trial, 161 reported on patients in the second-line setting, 98 reported non-randomized trials, 97 were review articles, and 53 were duplicates. Hence, 578 references fulfilled the predefined general eligibility criteria and were reassessed concerning the exact treatment comparison. A total of 21 randomized clinical trials for the first-line treatment of HL were identified, which included at least 50 patients per study arm and compared treatment modalities that matched with at least one of the five study questions. Data were received for 16 trials conducted between 1984 and 2007 (Figure 1).19–33 No data were received for four studies.34–37 One additional trial first published in 2013 was only found in the 2015 search, so IPD were not sought.38 One trial was split for analysis since the participating centers could choose between two alternative intensified chemotherapy regimens.32
Figure 1.

Search results (combined for both searches in 2010 and 2015). HL: Hodgkin lymphoma; IPD: individual patient data.
Characteristics of the included studies
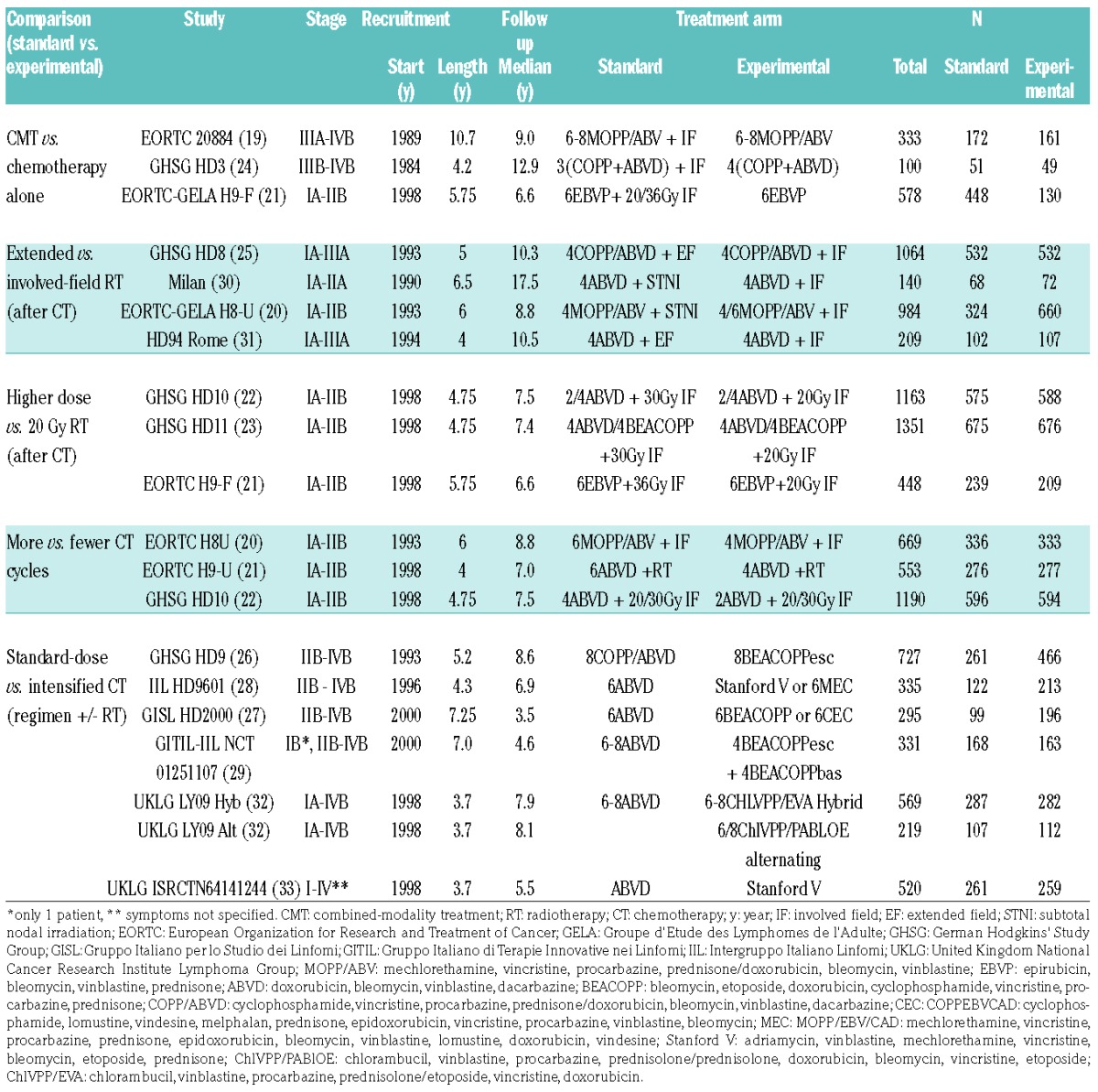
All included studies, grouped according to the study questions, are described in Table 1.
Table 1.
Description of included studies.
Three aspects of the risk of bias (randomization, allocation concealment, attrition bias) according to the Cochrane scheme were judged to be low in 13 out of 16 trials, while randomization and allocation concealment were uncertain in two trials and considered high in one trial. High risk of bias due to lack of blinding applied to all trials with respect to SMN and PFS, OS was presumed to be entirely objective. Sixteen patients from two studies with no evaluable data after randomization were excluded from the meta-analysis.20,26 Those patients had also been excluded from the analyses of the respective study groups.
The median follow-up within the trials ranged between 3.5 and 17.6 years (overall median follow-up: 7.4 years). A histogram of follow-up times to SMN or last information is displayed in the Online Supplementary Figure S1; although 75% of patients had more than 5 years of follow-up, only 16% were followed beyond ten years. A comparison of the distribution of follow-up times between the treatment arms of the included studies yielded a significant difference according to the log-rank test (P=0.036) in only one out of 16 cases.
The IQR-DLI varied among trials from 0.4 to 6.6 years (median: 3.1 years). Studies with longer follow-up tended to have a wider scatter. The ratio between the IQR-DLI and the median follow-up varied between 0.05 and 0.59 (median: 0.34). Thus, in half of the included studies the central 50% of last information dates stretch over a time interval of at least three years or one third of the median follow-up duration.
Patient characteristics
IPD from 9498 patients treated within 16 randomized clinical trials for newly diagnosed HL were included. At the time of HL treatment, patients were aged between 14 and 75 according to inclusion criteria of the included studies (eight exceptions between ten and 87 years), median age was 33 years. During the course of follow-up, an SMN was reported for 438/9498 patients (4.6%), including 63 t-AML/MDS (0.7%), 86 secondary NHL (0.9%) and 276 (2.9%) secondary solid tumors. The sites most often affected were the breast (39/276), lung (35/276), skin (29/276) and bowel (colon, rectum) (23/276). In 13 patients (0.1%) diagnosed with an SMN, information on the tumor entity was lacking. Cumulative incidences of SMN at five, ten, 15 and 20 years (regarding death as a competing risk) were 2.4%, 5.8%, 13% and 23%, respectively.
Results of the treatment comparisons
(1) CMT vs. chemotherapy alone
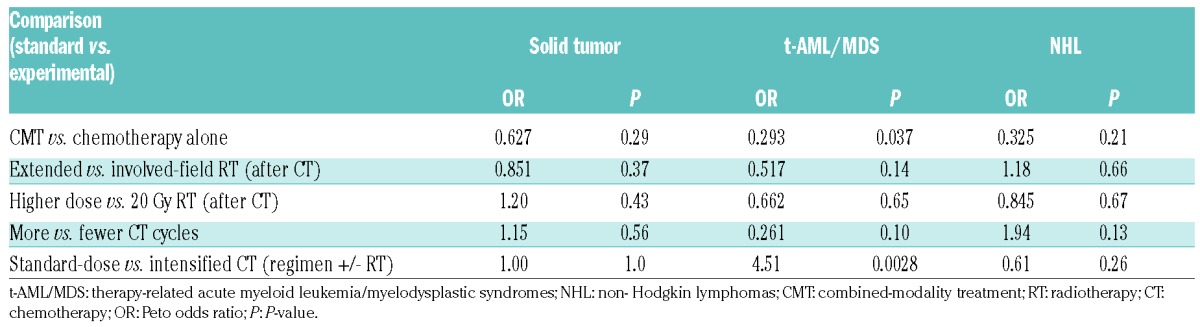
A total of 1011 patients treated within the European Organisation for Research and Treatment of Cancer (EORTC) 20884 (advanced stages), EORTC-Groupe D’Etude des Lymphomes de L’Adulte (GELA) H9-F (early stages) and the German Hodgkin Study Group (GHSG) HD3 (advanced stages) trials were analyzed. After a median follow-up of 7.8 years, 30/671 patients (4.5%) treated with CMT and 10/340 patients (2.9%) treated with chemotherapy alone had been diagnosed with an SMN. This difference was significant, favoring patients who had received chemotherapy only (P=0.010; Peto’s OR: 0.43, 95%-CI: 0.23–0.82) (Figures 2 and 3; Table 2). In particular, patients aged 50 and younger (P=0.04), female patients (P=0.01) and those with advanced stages (P=0.01) had a significantly reduced risk of developing an SMN when treated with chemotherapy alone. No reduced SMN rate with chemotherapy alone was observed among patients diagnosed with early stages (P=0.68). An analysis separately evaluating the incidence rates for t-AML/MDS, secondary NHL and secondary solid tumors revealed a risk reduction after chemotherapy alone solely for the development of t-AML/MDS (P=0.037), but not for secondary NHL and solid tumors (Table 3). The PFS and OS rates did not significantly differ between treatment groups (Table 2), however, there was some evidence of inferior tumor control with chemotherapy alone (HR: 1.31, 95%-CI: 0.99–1.73, P=0.06). Subgroup analyses indicated that stage and age were significant effect modifiers (interaction P-values were <0.0001 (stage) and 0.02 (age)). PFS was significantly impaired after chemotherapy alone in comparison with CMT for early-stage patients and patients aged ≤50 (Online Supplementary Tables S1, S2 and S3).
Figure 2.

Additional radiotherapy, cumulative incidence of SMN (Peto meta-analysis). CI: confidence interval; O–E: observed minus expected; V: variance; I2 = measure of heterogeneity: EORTC: European Organization for Research and Treatment of Cancer; GHSG: German Hodgkins’ Study Group.
Figure 3.

Additional radiotherapy, cumulative incidence of SMN (Peto meta-analysis). Vertical bars depict approximate 95% confidence intervals (CI) for cumulative incidence rates. CT: chemotherapy; RT: radiotherapy.
Table 2.
Treatment effect and heterogeneity for secondary malignant neoplasms (SMN), overall survival (OS) and progression-free survival (PFS).

Table 3.
Summary of SMN results for each SMN type.
(2) More extended RT vs. involved field RT
A total of 2397 early-stage patients treated within the EORTC-GELA H8-U, the GHSG HD8, the Italian HD94 and the Milan trial were analyzed. After a median follow-up of 10.8 years, 91/1026 patients (8.9%) who had received RT to more extended fields and 96/1371 patients (7.0%) who had received IF-RT had been diagnosed with an SMN. This difference was not statistically significant (P=0.32; Peto’s OR: 0.86, 95%-CI: 0.64–1.16; Online Supplementary Figures S2 and S3). In addition, when separately analyzing the incidence rates of t-AML/MDS, secondary NHL and secondary solid tumors, there were no significant differences between the treatment groups. The same is true for the PFS and OS rates (Table 2). Subgroup analyses according to sex and age did not identify any heterogeneity of the treatment effect across any subgroups.
(3) RT at higher doses vs. RT at 20 Gy
A total of 2962 early-stage patients treated within the EORTC-GELA H9-F, GHSG HD10 and GHSG HD11 trials were analyzed. After a median follow-up of 7.4 years, 54/1489 patients (3.6%) who had RT at a dose of 30 Gy or 36 Gy and 56/1473 patients (3.8%) who had RT at a dose of 20 Gy had developed an SMN. Thus, the rate of SMN did not differ between the treatment groups (P=0.87; Peto’s OR: 1.03, 95%-CI: 0.71–1.50; Online Supplementary Figures S4 and S5). There were also no differences when the rates for t-AML/MDS, secondary NHL and secondary solid tumors were separately considered. The clinical outcome was similar in both treatment groups, with no differences in PFS and OS. Additional subgroup analyses according to sex and age did not identify differences between any subgroups.
(4) More vs. fewer cycles of the same chemotherapy protocol
A total of 2403 early-stage patients treated within the EORTC-GELA H8-U, EORTC-GELA H9-U and GHSG HD10 trials were analyzed. After a median follow-up of 7.8 years, 48/1201 patients (4.0%) who had been treated with more cycles and 53/1202 patients (4.4%) who had received fewer cycles of the same chemotherapy protocol had developed an SMN. This difference was not statistically significant (P=0.65; Peto’s OR: 1.10, 95%-CI: 0.74–1.62) (Online Supplementary Figures S6 and S7). Additionally, the SMN incidences did not differ between the patient groups when t-AML/MDS, secondary NHL and secondary solid tumors were considered separately. The clinical outcome after treatment with more or fewer cycles of the same chemotherapy was comparable, without any significant PFS and OS differences. Additional subgroup analyses according to sex and age did not identify differences between any subgroups.
(5) Standard-dose chemotherapy (ABVD or cyclophosphamide vincristine, procarbazine, and prednisone (COPP)/ABVD) vs. intensified chemotherapy
A total of 2996 advanced-stage patients treated within a Gruppo Italiano Terapie Innovative nei Linfomi (GITIL)-Intergruppo Italiano Linfomi (IIL) trial, the Gruppo Italiano per lo Studio dei Linfomi (GISL) HD2000 trial, the GHSG HD9 trial, the HD9601 trial from Italy and the British LY09 and ISRCTN64141244 trials were analyzed. The rates of RT were comparable in both treatment groups of the included studies with the exception of the ISRCTN64141244 and HD9601 trials, administering Stanford V as an intensified regimen. After a median follow-up of 6.7 years, 31/1305 patients (2.8%) who had received standard-dose chemotherapy (ABVD, COPP/ABVD) and 60/1691 patients (3.5%) treated with intensified chemotherapy protocols (escalated BEACOPP, Stanford V, ChlVPP/prednisolone, doxorubicin, bleomycin, vincristine, and etoposide (PABIOE), ChlVPP/etoposide, vincristine, and doxorubicin (EVA), MOPP/EBV/CAD, COPP/EBV/CAD) had developed an SMN. This difference was not statistically significant (P=0.15; Peto’s OR: 1.37, 95%-CI: 0.89–2.10; Figures 4 and 5). When considering t-AML/MDS, secondary NHL and secondary solid tumors separately, an increased risk to develop t-AML/MDS was seen for patients treated with intensified chemotherapy protocols (P=0.0028), whereas the incidence rates for secondary NHL and secondary solid tumors did not differ between the treatment groups (Table 3). Overall, tumor control was significantly better with intensified chemotherapy regimens as compared with standard-dose protocols (P=0.007; HR: 0.82, 95%-CI: (0.70 – 0.95)) while there were no significant differences in OS (P=0.12; HR: 0.85, 95%-CI: (0.70 – 1.04)). However, subgroup analyses revealed that patients aged ≤50, in particular, appear to benefit from more aggressive chemotherapy approaches as the improved PFS also translated into a better OS in these patients (P=0.02). In contrast with patients older than 50 years, patients aged ≤50 also had a significantly greater SMN risk with intensified chemotherapy protocols than with standard-dose chemotherapy (interaction P=0.02; treatment effect in younger subgroup: P=0.01). Additional subgroup analyses revealed differences between the different intensified protocols for PFS (interaction P<0.00001) and OS (interaction P=0.006). Patients treated with escalated BEACOPP had superior PFS and OS rates in comparison with those receiving standard-dose chemotherapy. For Stanford V, PFS was worse than with standard-dose chemotherapy. No PFS and OS differences in comparison with standard-dose chemotherapy were observed for ChlVPP/PABIOE, ChlVPP/EVA, MOPP/EBV/CAD and COPP/EBV/CAD. For SMN no interaction in chemotherapy subgroups were found (interaction P=0.06; Online Supplementary Table S3).
Figure 4.

Intensified chemotherapy, secondary malignant neoplasms, forest plot for Peto Odds Ratios. CI: confidence interval; O–E: observed minus expected; V: variance, I2: measure of heterogeneity; ABVD: doxorubicin, bleomycin, vinblastine, dacarbazine.
Figure 5.

Intensified chemotherapy, cumulative incidence of SMN (Peto meta-analysis). Vertical bars depict approximate 95% confidence intervals (CI) for cumulative incidence rates. ABVD: doxorubicin, bleomycin, vinblastine, dacarbazine.
All of the main meta-analytic results are summarized in Table 2.
Sensitivity analyses agreed with the described main analyses. The results of sensitivity analyses concerning censoring of incomplete follow-up periods and exclusion of NMSC are summarized in Online Supplementary Tables S4 and S5.
Discussion
The meta-analysis herein, including 9498 patients treated within 16 randomized clinical trials for newly diagnosed HL between 1984 and 2007, represents one of the largest analyses of SMN, PFS and OS of HL patients based on randomized comparisons. The major findings were as follows: (1) after a median follow-up of 7.4 years, the overall SMN rate was 4.6%, (2) compared with patients receiving chemotherapy alone, an increased SMN rate was observed in patients receiving CMT, (3) patients with early-stage HL treated with CMT had a better PFS than patients treated with chemotherapy alone, (4) compared with patients receiving standard-dose chemotherapy, those receiving intensified chemotherapy protocols developed t-AML/MDS more often, and (5) compared with ABVD-like protocols, PFS and OS in advanced-stage patients were improved with escalated BEACOPP, but higher rates of SMN were observed.
The overall SMN rate of 4.6% in the meta-analysis here-in was lower than in previous reports. A meta-analysis from our group included a total of 9312 patients treated between 1962 and 2000. After median follow-up times ranging between four and 32 years for the considered trials, the overall SMN rate was 7.6%.39,40 A British analysis including 5798 patients treated between 1963 and 2001 reported an SMN rate of 7.9%.4 According to a Dutch study with a median follow-up of 19.1 years, the overall SMN rate was 23% and the risk for the development of an SMN was still increased 30 years after HL treatment.3 Two reasons likely contribute to the higher SMN rates in these previous analyses: (1) a relevant proportion of the expected secondary solid tumors that are often diagnosed ten or more years after HL treatment has not yet occurred in the patients included in the meta-analysis herein due to the limited median follow-up of 7.4 years, and (2) the SMN rate observed within the present meta-analysis is probably truly lower than the rates seen in the older analyses, since in recent years RT fields and doses were reduced and chemotherapy protocols were modified with the aim of decreasing the SMN risk.
In the meta-analysis herein, patients receiving CMT for HL had a significantly increased risk to develop an SMN when compared with chemotherapy alone. Figure 3 shows that at ten years after first-line treatment, the absolute cumulative SMN risks are approximately 3% and 10%, a risk difference of 7%. This result is in line with previous analyses such as the above mentioned British study, in which patients treated with chemotherapy alone had a significantly lower relative risk for the development of an SMN than patients receiving CMT.4 Subgroup analyses of the analysis herein considering t-AML/MDS, secondary NHL and secondary solid tumors separately, detected a significantly increased risk after CMT for t-AML/MDS only, but not for secondary NHL and secondary solid tumors. This finding is consistent with older reports, including a study from Italy comprising 1659 patients treated with RT alone, CMT or chemotherapy alone. At 15 years, the t-AML/MDS rate after CMT was significantly higher than after chemotherapy alone (P=0.05).41
According to the meta-analysis herein, patients diagnosed with early-stage HL had a better PFS after CMT than after chemotherapy alone. However, this finding has to be interpreted with caution as it derives from only one of the included trials. Nonetheless, similar data also came from the randomized EORTC/Lymphoma Study Association (LYSA)/Fondazione Italiana Linfomi (FIL) H10 study and the RAPID trial conducted in the UK. These studies evaluated the positron emission tomography (PET)-guided omission of consolidating RT after chemotherapy in patients with early-stage HL. Both studies additionally revealed a significantly increased event rate after chemotherapy alone in patients with a good response to chemotherapy resulting in a negative interim PET.42–44 Additional data supporting the use of CMT in early-stage HL come from a previous Cochrane systematic review including 1245 patients from five randomized studies and an analysis comprising 20600 patients registered in the U.S. National Cancer Data Base, both of which have not only demonstrated a better PFS but also an improved OS among patients treated with CMT compared with chemotherapy alone.45,46
In the meta-analysis herein, an increased t-AML/MDS rate was seen in patients receiving intensified chemotherapy compared with patients treated with standard-dose chemotherapy. This finding is consistent with other reports on t-AML/MDS after HL treatment. An analysis by the GHSG, including 11952 patients treated within prospective studies for newly diagnosed HL, demonstrated that patients receiving no BEACOPP or up to four cycles of escalated BEACOPP had significantly lower cumulative t-AML/MDS rates than patients treated with four or more cycles of escalated BEACOPP (0.3% vs. 0.7% vs. 1.7%; P<0.0001).7
For escalated BEACOPP, the increased t-AML/MDS risk contrasts with an improved clinical outcome. PFS (P<0.00001) and OS (P=0.0005) rates were better than those seen with standard-dose protocols, i.e., ABVD or COPP/ABVD. This is in line with the results of a network meta-analysis on the effect of the initial treatment strategy on the survival of patients with advanced HL. That analysis, which included a total of 9993 patients, revealed a survival advantage of 10% at five years for escalated BEA-COPP in comparison with ABVD.47
Generally, this meta-analysis provides high-quality evidence on SMN, PFS and OS among patients treated for HL, as the used data are from participants of large randomized trials for the first-line treatment of HL. However, the analysis has some limitations. With a median overall follow-up of 7.4 years, valid estimates are only possible for secondary hematological malignancies, whilst final conclusions regarding secondary solid tumors that often occur more than ten years after HL cannot be drawn. The long-term data of HL patients treated within clinical trials are therefore necessary but often difficult to obtain due to different factors, including a limited duration of insurance for study participants and a lack of funding sources. There is also some uncertainty about the completeness of SMN reporting which is of particular importance due to the small number of SMN events. Finally, for certain outcomes and study questions there was a considerable heterogeneity of up to 89% between the included trials, which signifies that the overall meta-analytic results may not apply in all situations.
Nonetheless, given the relevant proportion of HL patients that have already developed an SMN after a median observation of 7.4 years, the present report underscores the need for treatment approaches allowing a more accurate allocation to defined risk groups, in order to prevent overtreatment and reduce the risk of the development of potentially fatal SMN. At present, interim PET is considered the most promising tool to stratify treatment. Some mature results addressing this issue are already available and additional studies will be analyzed in the near future.48,49 The replacement of conventional chemotherapy by novel agents such as the CD30-directed antibody-drug conjugate brentuximab vedotin and antibodies targeting the programmed death cell protein 1 (PD-1) may also reduce the risk for the development of SMN.50,51
Supplementary Material
Acknowledgments
Further thanks go to the Cochrane Collaboration and in particular to the Cochrane Haematological Malignancies Review Group (coordinating editor: Dr. Nicole Skoetz, M.D.) for reviewing the protocol and draft of the Cochrane systematic review.
Footnotes
Funding
The authors would like to thank the Bundesministerium für Bildung und Forschung (German Federal Ministry of Education and Research, grant no. 01KG0921) for financial support.
Check the online version for the most updated information on this article, online supplements, and information on authorship & disclosures: www.haematologica.org/content/102/10/1748
References
- 1.Eichenauer DA, Engert A, Andre M, et al. Hodgkin’s lymphoma: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann Oncol. 2014;25 Suppl 3:iii70–75. [DOI] [PubMed] [Google Scholar]
- 2.Borchmann P, Eichenauer DA, Engert A. State of the art in the treatment of Hodgkin lymphoma. Nat Rev Clin Oncol. 2012; 9(8):450–459. [DOI] [PubMed] [Google Scholar]
- 3.Schaapveld M, Aleman BM, van Eggermond AM, et al. Second cancer risk up to 40 years after treatment for Hodgkin’s lymphoma. N Engl J Med. 2015; 373(26):2499–2511. [DOI] [PubMed] [Google Scholar]
- 4.Swerdlow AJ, Higgins CD, Smith P, et al. Second cancer risk after chemotherapy for Hodgkin’s lymphoma: a collaborative British cohort study. J Clin Oncol. 2011; 29(31):4096–4104. [DOI] [PubMed] [Google Scholar]
- 5.Aleman BM, van den Belt-Dusebout AW, De Bruin ML, et al. Late cardiotoxicity after treatment for Hodgkin lymphoma. Blood. 2007;109(5):1878–1886. [DOI] [PubMed] [Google Scholar]
- 6.Behringer K, Mueller H, Goergen H, et al. Gonadal function and fertility in survivors after Hodgkin lymphoma treatment within the German Hodgkin Study Group HD13 to HD15 trials. J Clin Oncol. 2013; 31(2):231–239. [DOI] [PubMed] [Google Scholar]
- 7.Eichenauer DA, Thielen I, Haverkamp H, et al. Therapy-related acute myeloid leukemia and myelodysplastic syndromes in patients with Hodgkin lymphoma: a report from the German Hodgkin Study Group. Blood. 2014;123(11):1658–1664. [DOI] [PubMed] [Google Scholar]
- 8.Koontz MZ, Horning SJ, Balise R, et al. Risk of therapy-related secondary leukemia in Hodgkin lymphoma: the Stanford University experience over three generations of clinical trials. J Clin Oncol. 2013; 31(5):592–598. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Leone G, Voso MT, Sica S, Morosetti R, Pagano L. Therapy related leukemias: susceptibility, prevention and treatment. Leuk Lymphoma. 2001;41(3–4):255–276. [DOI] [PubMed] [Google Scholar]
- 10.Bonadonna G, Zucali R, Monfardini S, De Lena M, Uslenghi C. Combination chemotherapy of Hodgkin’s disease with adriamycin, bleomycin, vinblastine, and imidazole carboxamide versus MOPP. Cancer. 1975;36(1):252–259. [DOI] [PubMed] [Google Scholar]
- 11.Diehl V, Sieber M, Ruffer U, et al. BEA-COPP: an intensified chemotherapy regimen in advanced Hodgkin’s disease. The German Hodgkin’s Lymphoma Study Group. Ann Oncol. 1997;8(2):143–148. [DOI] [PubMed] [Google Scholar]
- 12.Bartlett NL, Rosenberg SA, Hoppe RT, Hancock SL, Horning SJ. Brief chemotherapy, Stanford V, and adjuvant radiotherapy for bulky or advanced-stage Hodgkin’s disease: a preliminary report. J Clin Oncol. 1995;13(5):1080–1088. [DOI] [PubMed] [Google Scholar]
- 13.Rueffer U, Josting A, Franklin J, et al. Non-Hodgkin’s lymphoma after primary Hodgkin’s disease in the German Hodgkin’s Lymphoma Study Group: incidence, treatment, and prognosis. J Clin Oncol. 2001;19(7):2026–2032. [DOI] [PubMed] [Google Scholar]
- 14.Higgins JPT, Altman DG, Sterne JAC. Chapter 8: Assessing risk of bias in included studies. Cochrane Handbook for Systematic Reviews of Interventions (Editors: Higgins JPT, Green S.). 2011. [Google Scholar]
- 15.Peto R, Pike MC, Armitage P, et al. Design and analysis of randomized clinical trials requiring prolonged observation of each patient. I. Introduction and design. Br J Cancer. 1976;34(6):585–612. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Peto R, Pike LC, Armitage P, et al. Design and analysis of randomized clinical trials requiring prolonged observation of each patient. II. analysis and examples. Bri J Cancer. 1977;35(1):1–39. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Pepe MS, Mori M. Kaplan-Meier, marginal or conditional probability curves in summarizing competing risks failure time data? Stat Med. 1993;12(8):737–751. [DOI] [PubMed] [Google Scholar]
- 18.Tai BC, Machin D, White I, Gebski V. Competing risks analysis of patients with osteosarcoma: a comparison of four different approaches. Stat Med. 2001;20(5):661–684. [DOI] [PubMed] [Google Scholar]
- 19.Aleman BM, Raemaekers JM, Tirelli U, et al. Involved-field radiotherapy for advanced Hodgkin’s lymphoma. N Engl J Med. 2003;348(24):2396–2406. [DOI] [PubMed] [Google Scholar]
- 20.Ferme C, Eghbali H, Meerwaldt JH, et al. Chemotherapy plus involved-field radiation in early-stage Hodgkin’s disease. N Engl J Med. 2007;357(19):1916–1927. [DOI] [PubMed] [Google Scholar]
- 21.Thomas J, Ferme C, Noordijk EM, et al. Results of the EORTC-GELA H9 randomized trials: The H9-F trial (comparing 3 radiation dose levels) and H9-U trial (comparing 3 chemotherapy schemes) in patients with favorable or unfavorable early stage Hodgkin’s lymphoma (HL). Haematologica. 2007; 92(Supplement 5): abstract C010. [Google Scholar]
- 22.Engert A, Plutschow A, Eich HT, et al. Reduced treatment intensity in patients with early-stage Hodgkin’s lymphoma. N Engl J Med. 2010;363(7):640–652. [DOI] [PubMed] [Google Scholar]
- 23.Eich HT, Diehl V, Gorgen H, et al. Intensified chemotherapy and dose-reduced involved-field radiotherapy in patients with early unfavorable Hodgkin’s lymphoma: final analysis of the German Hodgkin Study Group HD11 trial. J Clin Oncol. 2010;28(27):4199–4206. [DOI] [PubMed] [Google Scholar]
- 24.Diehl V, Loeffler M, Pfreundschuh M, et al. Further chemotherapy versus low-dose involved-field radiotherapy as consolidation of complete remission after six cycles of alternating chemotherapy in patients with advance Hodgkin’s disease. German Hodgkins’ Study Group (GHSG). Ann Oncol. 1995;6(9):901–910. [DOI] [PubMed] [Google Scholar]
- 25.Engert A, Schiller P, Josting A, et al. Involved-field radiotherapy is equally effective and less toxic compared with extended-field radiotherapy after four cycles of chemotherapy in patients with early-stage unfavorable Hodgkin’s lymphoma: results of the HD8 trial of the German Hodgkin’s Lymphoma Study Group. J Clin Oncol. 2003;21(19):3601–3608. [DOI] [PubMed] [Google Scholar]
- 26.Diehl V, Franklin J, Pfreundschuh M, et al. Standard and increased-dose BEACOPP chemotherapy compared with COPP-ABVD for advanced Hodgkin’s disease. N Engl J Med. 2003;348(24):2386–2395. [DOI] [PubMed] [Google Scholar]
- 27.Federico M, Luminari S, Iannitto E, et al. ABVD compared with BEACOPP compared with CEC for the initial treatment of patients with advanced Hodgkin’s lymphoma: results from the HD2000 Gruppo Italiano per lo Studio dei Linfomi Trial. J Clin Oncol. 2009;27(5):805–811. [DOI] [PubMed] [Google Scholar]
- 28.Gobbi PG, Levis A, Chisesi T, et al. ABVD versus modified Stanford V versus MOPPE-BVCAD with optional and limited radiotherapy in intermediate- and advanced-stage Hodgkin’s lymphoma: final results of a multicenter randomized trial by the Intergruppo Italiano Linfomi. J Clin Oncol. 2005;23(36):9198–9207. [DOI] [PubMed] [Google Scholar]
- 29.Viviani S, Zinzani PL, Rambaldi A, et al. ABVD versus BEACOPP for Hodgkin’s lymphoma when high-dose salvage is planned. N Engl J Med. 2011;365(3):203–212. [DOI] [PubMed] [Google Scholar]
- 30.Bonadonna G, Bonfante V, Viviani S, Di Russo A, Villani F, Valagussa P. ABVD plus subtotal nodal versus involved-field radiotherapy in early-stage Hodgkin’s disease: long-term results. J Clin Oncol. 2004; 22(14):2835–2841. [DOI] [PubMed] [Google Scholar]
- 31.Anselmo AP, Cavalieri E, Osti FM, et al. Intermediate stage Hodgkin’s disease: preliminary results on 210 patients treated with four ABVD chemotherapy cycles plus extended versus involved field radiotherapy. Anticancer Res. 2004;24(6):4045–4050. [PubMed] [Google Scholar]
- 32.Johnson PW, Radford JA, Cullen MH, et al. Comparison of ABVD and alternating or hybrid multidrug regimens for the treatment of advanced Hodgkin’s lymphoma: results of the United Kingdom Lymphoma Group LY09 Trial (ISRCTN97144519). J Clin Oncol. 2005;23(36):9208–9218. [DOI] [PubMed] [Google Scholar]
- 33.Hoskin PJ, Lowry L, Horwich A, et al. Randomized comparison of the stanford V regimen and ABVD in the treatment of advanced Hodgkin’s Lymphoma: United Kingdom National Cancer Research Institute Lymphoma Group Study ISRCTN 64141244. J Clin Oncol. 2009;27(32):5390–5396. [DOI] [PubMed] [Google Scholar]
- 34.Nachman JB, Sposto R, Herzog P, et al. Randomized comparison of low-dose involved-field radiotherapy and no radiotherapy for children with Hodgkin’s disease who achieve a complete response to chemotherapy. J Clin Oncol. 2002;20(18):3765–3771. [DOI] [PubMed] [Google Scholar]
- 35.Kung FH, Schwartz CL, Ferree CR, et al. POG 8625: a randomized trial comparing chemotherapy with chemoradiotherapy for children and adolescents with Stages I, IIA, IIIA1 Hodgkin Disease: a report from the Children’s Oncology Group. J Pediatr Hematol Oncol. 2006;28(6):362–368. [DOI] [PubMed] [Google Scholar]
- 36.Laskar S, Gupta T, Vimal S, et al. Consolidation radiation after complete remission in Hodgkin’s disease following six cycles of doxorubicin, bleomycin, vinblastine, and dacarbazine chemotherapy: is there a need? J Clin Oncol. 2004;22(1):62–68. [DOI] [PubMed] [Google Scholar]
- 37.Gerhartz HH, Schwenke H, Bazarbashi S, et al. Randomised comparison of COPP/ABVD versus dose- and time-escalated COPP/ABVD with GM-CSF support for advanced Hodgkin s disease. Proc Am Soc Clin Oncol. 1997;16:8a. [Google Scholar]
- 38.Gordon LI, Hong F, Fisher RI, et al. Randomized phase III trial of ABVD versus Stanford V with or without radiation therapy in locally extensive and advanced-stage Hodgkin lymphoma: an intergroup study coordinated by the Eastern Cooperative Oncology Group (E2496). J Clin Oncol. 2013;31(6):684–691. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Franklin JG, Paus MD, Pluetschow A, Specht L. Chemotherapy, radiotherapy and combined modality for Hodgkin’s disease, with emphasis on second cancer risk. Cochrane Database Syst Rev. 2005; (4):CD003187. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Franklin J, Pluetschow A, Paus M, et al. Second malignancy risk associated with treatment of Hodgkin’s lymphoma: meta-analysis of the randomised trials. Ann Oncol. 2006;17(12):1749–1760. [DOI] [PubMed] [Google Scholar]
- 41.Brusamolino E, Anselmo AP, Klersy C, et al. The risk of acute leukemia in patients treated for Hodgkin’s disease is significantly higher aft [see bined modality programs than after chemotherapy alone and is correlated with the extent of radiotherapy and type and duration of chemotherapy: a case-control study. Haematologica. 1998; 83(9):812–823. [PubMed] [Google Scholar]
- 42.Raemaekers JM, Andre MP, Federico M, et al. Omitting radiotherapy in early positron emission tomography-negative stage I/II Hodgkin lymphoma is associated with an increased risk of early relapse: Clinical results of the preplanned interim analysis of the randomized EORTC/LYSA/FIL H10 trial. J Clin Oncol. 2014;32(12):1188–1194. [DOI] [PubMed] [Google Scholar]
- 43.Radford J, Illidge T, Counsell N, et al. Results of a trial of PET-directed therapy for early-stage Hodgkin’s lymphoma. N Engl J Med. 2015;372(17):1598–1607. [DOI] [PubMed] [Google Scholar]
- 44.Andre MPE, Girinsky T, Federico M, et al. Early positron emission tomography response-adapted treatment in stage I and II Hodgkin Lymphoma: final results of the randomized EORTC/LYSA/FIL H10 Trial. J Clin Oncol. 2017;35(16):1786–1794. [DOI] [PubMed] [Google Scholar]
- 45.Herbst C, Rehan FA, Skoetz N, et al. Chemotherapy alone versus chemotherapy plus radiotherapy for early stage Hodgkin lymphoma. Cochrane Database Syst Rev. 2011;(2):CD007110. [DOI] [PubMed] [Google Scholar]
- 46.Olszewski AJ, Shrestha R, Castillo JJ. Treatment selection and outcomes in early-stage classical Hodgkin lymphoma: analysis of the National Cancer Data Base. J Clin Oncol. 2015;33(6):625–633. [DOI] [PubMed] [Google Scholar]
- 47.Skoetz N, Trelle S, Rancea M, et al. Effect of initial treatment strategy on survival of patients with advanced-stage Hodgkin’s lymphoma: a systematic review and network meta-analysis. Lancet Oncol. 2013; 14(10):943–952. [DOI] [PubMed] [Google Scholar]
- 48.Engert A, Haverkamp H, Kobe C, et al. Reduced-intensity chemotherapy and PET-guided radiotherapy in patients with advanced stage Hodgkin’s lymphoma (HD15 trial): a randomised, open-label, phase 3 non-inferiority trial. Lancet. 2012; 379(9828):1791–1799. [DOI] [PubMed] [Google Scholar]
- 49.Johnson P, Federico M, Kirkwood A, et al. Adapted Treatment Guided by Interim PET-CT Scan in Advanced Hodgkin’s Lymphoma. N Engl J Med. 2016; 374(25):2419–2429. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 50.Younes A, Gopal AK, Smith SE, et al. Results of a pivotal phase II study of brentuximab vedotin for patients with relapsed or refractory Hodgkin’s lymphoma. J Clin Oncol. 2012;30(18):2183–2189. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 51.Younes A, Santoro A, Shipp M, et al. Nivolumab for classical Hodgkin’s lymphoma after failure of both autologous stem-cell transplantation and brentuximab vedotin: a multicentre, multicohort, single-arm phase 2 trial. Lancet Oncol. 2016; 17(9):1283–1294. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.