

Abstract
Objectives
Prevalence of diarrhoea and acute respiratory infection (ARI) is considerably high among South Asian children. The objective of this study is to compare the associations of sustainable household environment and knowledge of healthy practices with episodes of these diseases among the children in the region.
Design
The study analysed the latest, nationally representative and cross-sectional Demographic and Health Survey data.
Setting
Data from three countries were analysed: Bangladesh, Nepal and Pakistan.
Participants
Women aged between 12 and 49 years living in selected households provided information on 23 940 of their children under the age of 5 years.
Primary outcomes measures
The morbidity status of the children was recorded with respect to episodes of diarrhoea and/or ARI in the 2 weeks preceding data collection.
Results
Consuming unhygienic drinking water increased the risks of childhood diarrhoea, and use of solid fuel for indoor cooking increased the risk of ARI, across all three countries investigated. However, far more significant were the effects of mother’s education, with incomplete primary education leading to an odds of diarrhoea approaching twice that of a mother with secondary education or higher (OR 1.70 in Bangladesh, 95% CI 1.16 to 2.49).
Conclusions
Results from the current research underline the importance of developing and implementing integrated strategic plans for mothers and children in the countries investigated. Promoting hygienic water and sanitation facilities can help reduce the prevalence of childhood diarrhoea. Replacing indoor solid fuel cooking arrangements with cleaner fuel or more airy conditions can help reduce the prevalence of ARI. However, these strategies need to be integrated with education for women to raise the likelihood that reduced risks are actually realised.
Keywords: Public health <, Infectious Diseases, Community child health <, Paediatrics, Public Health, Statistics and Research Methods
Strengths and limitations of this study.
The study used some of the largest and most recent cross-sectional surveys conducted in the countries analysed.
Data from three countries were compared: Bangladesh (2014), Nepal (2011) and Pakistan (2012).
Information regarding the disease episodes is limited by its provision at a single point of time so that the seasonal variations in the prevalence of the disease episodes are not addressed in the analysis.
The disease episodes are limited by their determination on the basis of self-reporting of mothers over a short recall period (2 weeks).
The data sets do not represent same time point for the studied countries, although the largest time difference is only 3 years.
Introduction
Infectious diseases are responsible for approximately half of child deaths worldwide,1 where pneumonia and diarrhoea are two of the leading causes.2 3 Apart from deaths, several diarrhoeal episodes lead to long-term nutritional deficits, whereas childhood respiratory infections cause increased risk of reduced lung capacity.4 5 The greatest proportions of severe episodes of these infections are experienced in the south Asian and African regions and within these regions, the prevalence of these diseases is even higher for poorer countries and among disadvantaged children.6 7
Considering the consequences of diarrhoea and acute respiratory infection (ARI) episodes on mortality and long-term adverse health outcomes, numerous studies have been conducted to identify associated risk factors. Existing literature suggests that younger children are more likely to experience infectious diseases than older cohorts, and consequently, a higher proportion of diarrhoea and pneumonia-related deaths happen in the first 2 years of life.7–9 Due to differentials in food intake, standard of living and availability of healthcare facilities, urban–rural variations are also evident in childhood morbidity.10 11 Educated mothers are knowledgeable about healthy environments and possible risks of their children being exposed to infectious diseases, and hence, occurrence of infectious diseases is significantly associated with the educational status of mother.12–14 In addition to formal education, access to mass media helps to create awareness around communicable diseases.15–17 Furthermore, poorer individuals within impoverished settings face a relatively higher burden of infectious diseases, and children in wealthy families are more protected from diarrhoea and ARI.18–20
At the end of the Millennium Development Goals (MDG) in 2015, the development policies emphasised reducing the percentage of people living in households lacking a sustainable environment in terms of durable housing structure, sufficient living area, access to safe water and access to improved sanitation. These policies were developed considering the fact that a large proportion of diarrhoea-related mortality is attributable to either unsafe drinking water, inadequate sanitation or insufficient hygiene.21 Investigating 171 Demographic and Health Surveys (DHS) in 70 low-income and middle-income countries over the period 1986–2007, researchers22 concluded that access to improved sanitation and water was associated with lower risk of childhood diarrhoea. Similar relationships have been observed elsewhere.23–25 As a part of Goal 3 of the Sustainable Development Goals (SDG), the UN is aiming to end epidemics of water-borne and other communicable diseases by 2030. Goal 6 emphasises ensuring the availability of water and sanitation for all.26 A review of published articles27 concluded that residential crowding significantly increased the risk of severe respiratory disease. Using solid fuel for cooking is a major source of household air pollution and responsible for a variety of respiratory diseases.28–30
The main aim of this study was to advise on the relative importance of the SDG, in the light of evidence around the prevalence of diarrhoea and ARI among preschoolers from three south Asian countries—Bangladesh, Nepal and Pakistan. The first objective was to compare the prevalence of diarrhoea and ARI across the three countries. The second objective was to identify characteristics of children with relatively higher risks of diarrhoea and ARI. The third was to compare the association of potential predictors with the prevalence of diarrhoea and ARI. Of particular interest in the light of the SDG is the relative importance of sustainable household environment, in terms of safe drinking water and toilet facilities, compared with other predictors such as maternal education and household wealth. A second aim was to provide suggestions regarding the development of feasible and effective plans that fit with the SDG and are likely to reduce childhood diarrhoea and ARI in the region.
Data and methods
This study achieved the objectives by using the latest releases of nationally representative and cross-sectional DHS datasets from three south Asian countries—Bangladesh (2014), Nepal (2011) and Pakistan (2012). These developing countries are home to 400 million people (Bangladesh 169 million, Nepal 32 million and Pakistan 199 million)31 and share common historical, social and cultural background. In terms of per capita GDP, they trail the world (Pakistan 152nd, Bangladesh 156th and Nepal 172nd).32 Significant variations also exist among the countries in terms of child morbidity outcomes as well as a range of exposures to poverty and unhygienic household environment.
The DHS consists of a nationally representative sample of households obtained through a two-stage stratified sampling procedure. First, sample sizes in terms of number of households (for Bangladesh 18 000 households, for Nepal 10 826 households, for Pakistan 14 000 households) were calculated to provide reasonable precision for the survey indicators. In the first stage, each of the countries were divided into strata and a sample of enumeration areas (EAs) were selected independently from each stratum using probability proportional to size. The EAs were considered as the Primary Sampling Units. In the second stage, a systematic sampling technique was employed to select a fixed number of households from each of these EAs. Finally, ever-married women aged between 12 and 49 years living in the selected households were approached for interview to collect necessary information. The DHS enjoy high response rates and provide cleaned data for secondary analysis. This study excluded children from women who were not de-jure resident at the time of interview. Episodes of diarrhoea and ARI in 23 940 children (7760 from Bangladesh, 5140 from Nepal and 11 040 from Pakistan) under the age of 5 years and born to the selected women were analysed. To ensure the representativeness of the sample at various levels, sampling weights are included in the data for each sampling stage and cluster based on sampling probabilities. The sample weights were incorporated into the current analyses.
The surveys have attractive features that make them appealing for quantitative analysis: they collect information about the morbidity status of children and cover a wide range of variables regarding the children, their parents and the households they live in. The variables used in this study will be described in the next section.
Dependent and independent variables
The dependent variables in the study come from mother’s responses to questions on recent (within 2 weeks preceding the survey) episodes of diarrhoea and ARI of their children aged below 5 years. The DHS identify a child experiencing ARI by asking the mother whether the child has been ill in the 2 weeks preceding the survey with a cough accompanied by short, rapid breathing or by difficulty in breathing that the mother considered to be chest related.14 The children were categorised as those suffering or not experiencing these episodes within 2 weeks before the survey. Similarly, the DHS identify a child experiencing diarrhoea by asking the mother whether the child had diarrhoea in the last 2 weeks preceding the survey.
The set of independent variables considered as potential predictors were decided on using the existing literature, availability of information in the survey datasets and the knowledge of the researchers of the study region. To compare the prevalence of diarrhoea and ARI across age groups, children were categorised as those aged less than 1 year, between 1 and 3 years and from 3 to 5 years. A similar categorisation is used by other researchers.17 Households were also categorised as being in either an urban or rural setting. Educational attainment and access to mass media have been considered as a proxy of knowledge and understanding of mother regarding exposure to infectious diseases and their consequences on their children.15 16 Mothers were categorised as those with no or incomplete primary level, complete primary to incomplete secondary level and complete secondary or above level of education. Mothers were also classified on the basis of having or not having access to any of radio, television or newspapers.
Significant positive associations between household economic status and prevalence of infectious diseases were observed in previous studies.14 20 As a proxy of household economic status, this study used the wealth score created by the DHS and calculated using principal components analysis from variables comprising household construction materials (roof, ceiling and floor), possessions (televisions and bicycles) and dwelling characteristics (source of drinking water and sanitation facilities). Details about the calculation of the wealth scores is available.33 On the basis of wealth score, children were classified as those coming from a household classified as low (lower 40%), middle (middle 40%) and high (upper 20%) wealth categories.
Source of drinking water, type of toilet facility, crowding, type of cooking fuel and type of floor material were considered as indicators of sustainable household environment. Pipe, borehole, protected dug well, spring or rainwater are considered as improved sources of drinking water.33 Households were categorised as those having or not having an improved water source located on the premises. Sanitation using technologies such as flush toilet, ventilated pit latrine, traditional pit latrine with a slab or composting toilet were considered as improved. Households were categorised as those with ideal (improved unshared), moderate (unimproved unshared or improved shared) or worst (unimproved shared or no facility) toilet facilities. The number of adults per living room indicates crowding, and households were categorised as those with up to two adults per living room and two or more adults per living room. On the basis of existence of cooking practice, the households were categorised as ideal (cooking outside the house or not using solid fuel while cooking inside) or not ideal (using solid fuel while cooking inside the house). Finally, houses were categorised as having the floor made of mud or else. All information was extracted from the datasets mentioned in the previous section.
Statistical analysis
The dependent variables (prevalence of diarrhoea and ARI), as well as the predictor variables considered in the study, are categorical. Bivariate χ2 analyses were carried out to compare the prevalence of the diseases among the levels of the selected predictors.
Given the dichotomous nature of the dependent variables, multiple binary logistic regression models were fitted to assess the association between selected predictors on childhood morbidity. The model considers logarithm of odds (ratio of the probability of occurring to not occurring) as a linear additive function of the predictors. Exponentials of the estimated parameters referred as the OR estimate the changes in the odds with unit change in the predictors (for continuous predictor) or changes in the level of predictors compared with baseline (for categorical predictor).34 Separate multiple logistic regression models were fitted to the data from individual countries. To focus the models for each disease, the model for diarrhoea excluded the variable cooking fuel as predictor, whereas the model for ARI excluded source of drinking water and type of toilet facility as predictors. Statistical analysis was conducted in SPSS 21.035 using a weighted analysis to account for the survey weights and clustered structure of the sample.
Results
Prevalence of diarrhoea was considerably lower for the children in Bangladesh (5.7%) with respect to Nepal (13.8%) and Pakistan (22.5%). A considerably higher percentage of children from Pakistan were experiencing ARI (15.9%) than Bangladesh (5.4%) and Nepal (4.6%). Percentages of children experiencing comorbidity (defined in this study as presence of both diarrhoea and ARI) were highest in Pakistan and lowest in Bangladesh (figure 1). Distributions of respondents for various levels of selected predictors are presented in table 1. Age distributions of children were consistent over the studied countries. Most of the children in the studied settings lived in rural areas, ranging from 70.3% in Pakistan to 90.6% in Nepal. The percentage of mothers with both lower (no or incomplete primary) and higher (completed secondary or higher) educational levels were highest in Pakistan (62.5% and 17.9%), whereas the percentage of mothers with no or incomplete primary level of education was lowest in Bangladesh (32.7%). The highest proportion of children whose mother had access to any mass media was from Nepal (84.4%). Among the studied countries, percentages of children from households using improved and unshared toilet facilities were lowest in Nepal (35.9%). Using solid fuel while cooking inside home was rare in Bangladesh (9.6%) and common in Nepal (57.4%) and Pakistan (59.8%). Among the studied settings, the percentage of children from household sharing more than two adults a room was highest (71.7%) in Pakistan.
Figure 1.
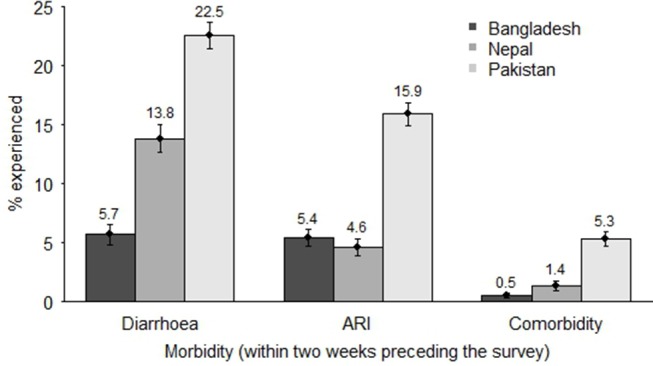
Percentage (with 95% CI) of children in Bangladesh, Nepal and Pakistan experiencing diarrhoea, ARI and comorbidity within 2 weeks preceding the survey. ARI, acute respiratory infection.
Table 1.
Percentages of respondents for various levels of the selected predictors in Bangladesh, Nepal and Pakistan
| Background characteristics | Percentages of respondents | ||
| Bangladesh (n=7760) | Nepal (n=5140) | Pakistan (n=11 040) | |
| Age of child, months | |||
| 0–11 | 19.5 | 19.9 | 19.8 |
| 12–35 | 41.2 | 39.2 | 39.4 |
| 36–59 | 39.3 | 40.9 | 40.8 |
| Type of place of residence | |||
| Rural | 74.4 | 90.6 | 70.3 |
| Urban | 25.6 | 9.4 | 29.7 |
| Mother’s education | |||
| Incomplete primary | 32.7 | 61.0 | 62.5 |
| Incomplete secondary | 51.5 | 25.3 | 19.6 |
| Secondary or higher | 15.8 | 13.7 | 17.9 |
| Access to electronic media | |||
| No access | 38.7 | 15.2 | 29.8 |
| Have access | 61.3 | 84.8 | 70.2 |
| Age of mother at the time of survey, years | |||
| 15–19 | 14.6 | 7.0 | 2.2 |
| 20–29 | 61.7 | 65.5 | 52.4 |
| 30–49 | 23.7 | 27.5 | 45.4 |
| Source of drinking water | |||
| Not improved/not in premises | 21.1 | 36.1 | 22.9 |
| Improved in premises | 78.9 | 63.9 | 77.1 |
| Toilet facility | |||
| Worst | 10.4 | 49.0 | 25.4 |
| Moderate | 26.7 | 15.0 | 11.5 |
| Ideal | 62.9 | 35.9 | 63.2 |
| No of adults per room | |||
| More than two adults | 40.9 | 43.2 | 71.7 |
| Up to two adults | 59.1 | 56.8 | 28.3 |
| Household cooking facility | |||
| Not ideal | 9.6 | 57.4 | 59.8 |
| Ideal | 90.4 | 42.6 | 40.2 |
| Household floor material | |||
| Mud | 68.9 | 75.4 | 47.3 |
| Not mud | 31.1 | 24.6 | 527 |
In the bivariate analyses, children experiencing episodes of ARI (within 2 weeks before the survey) were more likely to experience diarrhoea and vice-versa (table 2). Older children were significantly less likely to experience either episode than the younger. With the exception of episodes of ARI in Nepalese children, educational status of mother showed a significant association with the prevalence of the episodes of both infections. A mother’s access to mass media showed significant association with both episodes in Bangladesh only. Except for the prevalence of diarrhoea in Bangladesh, the wealth status of a household showed significant association with childhood diarrhoea and ARI. Significant associations between place of residence and prevalence of ARI were also observed for children in Bangladesh and Pakistan (p<0.05). In all except one setting, the source of drinking water did not show any significant association with diarrhoea or ARI, whereas type of toilet facility showed a significant association with the prevalence of diarrhoea in Nepal and Pakistan. The number of adults per living room showed a significant association with the prevalence of diarrhoea in Bangladesh and Nepal. Children from households using solid cooking fuel inside the house were significantly more likely to experience ARI with respect to those from households not using solid fuel for cooking inside the home.
Table 2.
Associations between childhood morbidity (diarrhoea or ARI) in 2 weeks preceding the survey and background characteristics of children
| Background characteristics | Bangladesh | Nepal | Pakistan | |||
| % Diarrhoea | % ARI | % Diarrhoea | % ARI | % Diarrhoea | % ARI | |
| Childhood ARI/diarrhoea in last 2 weeks | ||||||
| Experienced | 9.8 | 9.3 | 30.1 | 10.1 | 30.2 | 23.7 |
| Not experienced | 5.4 | 5.1 | 13.1 | 3.8 | 20.4 | 13.6 |
| χ2 | 14.27* | 14.27* | 55.65* | 55.65* | 145.59* | 145.59* |
| Age of child, months | ||||||
| 0–11 | 6.4 | 7.7 | 18.3 | 5.6 | 30.2 | 18.1 |
| 12–35 | 6.8 | 6.0 | 19.0 | 6.0 | 27.2 | 17.9 |
| 36–59 | 4.1 | 3.5 | 6.7 | 2.9 | 14.2 | 12.8 |
| χ2 | 21.89* | 41.15* | 150.24* | 24.46* | 308.76* | 52.81* |
| Place of residence | ||||||
| Rural | 5.7 | 5.7 | 13.9 | 4.6 | 22.7 | 16.4 |
| Urban | 5.6 | 4.3 | 13.4 | 5.0 | 21.9 | 14.6 |
| χ2 | 0.01 | 5.66** | 0.07 | 0.12 | 0.89 | 5.84** |
| Mother’s educational status | ||||||
| Incomplete primary | 6.1 | 5.2 | 14.2 | 4.6 | 23.5 | 16.4 |
| Incomplete secondary | 6.0 | 6.1 | 14.8 | 5.1 | 23.0 | 16.3 |
| Secondary or higher | 3.8 | 3.3 | 10.5 | 4.1 | 18.5 | 13.4 |
| χ2 | 9.93* | 15.37* | 7.75† | 1.04 | 22.26* | 10.84* |
| Wealth status of household | ||||||
| Low | 6.3 | 6.5 | 13.5 | 4.7 | 23.5 | 15.6 |
| Middle | 5.3 | 5.2 | 15.0 | 5.5 | 23.6 | 17.0 |
| High | 5.2 | 3.3 | 11.8 | 2.2 | 17.1 | 13.7 |
| χ2 | 3.66 | 19.76* | 5.03 | 12.92* | 36.23* | 10.58* |
| Access to electronic media | ||||||
| No access | 6.4 | 6.0 | 15.8 | 4.7 | 23.2 | 15.9 |
| Have access | 5.2 | 5.0 | 13.5 | 4.6 | 22.2 | 15.8 |
| χ2 | 4.87† | 3.39 | 2.83 | 0.03 | 1.42 | 0.03 |
| Age of mother at the time of survey, years | ||||||
| 15–19 | 6.3 | 7.9 | 16.2 | 5.6 | 32.6 | 21.1 |
| 20–29 | 5.6 | 5.3 | 14.0 | 4.7 | 24.3 | 16.2 |
| 30–49 | 5.6 | 4.1 | 12.9 | 4.2 | 19.9 | 15.2 |
| χ2 | 0.86 | 20.72* | 2.64 | 1.47 | 43.87* | 7.09** |
| Source of drinking water | ||||||
| Unimproved/not in premises | 6.8 | 6.1 | 14.1 | 4.7 | 21.7 | 15.5 |
| Improved in premises | 5.4 | 5.2 | 13.7 | 4.6 | 22.7 | 16.0 |
| χ2 | 5.25† | 2.33 | 0.13 | 0.02 | 1.22 | 0.39 |
| Toilet facility | ||||||
| Worst | 6.1 | 7.3 | 15.5 | 4.8 | 24.2 | 15.5 |
| Moderate | 5.8 | 6.4 | 12.0 | 5.6 | 23.5 | 15.8 |
| Ideal | 5.6 | 4.6 | 12.3 | 4.1 | 21.8 | 16.0 |
| χ2 | 0.41 | 15.55* | 11.28* | 2.73 | 8.14** | 0.47 |
| No of adults per room | ||||||
| More than two adults | 5.0 | 5.3 | 14.8 | 4.8 | 22.7 | 15.7 |
| Up to two adults | 6.1 | 5.4 | 13.1 | 4.6 | 21.9 | 16.2 |
| χ2 | 3.93† | 0.07 | 3.18 | 0.13 | 0.78 | 0.49 |
| Household cooking fuel | ||||||
| Not ideal | 7.8 | 8.1 | 12.9 | 5.2 | 23.7 | 16.4 |
| Ideal | 5.4 | 5.1 | 15.1 | 3.8 | 20.6 | 15.1 |
| χ2 | 6.89* | 11.85* | 5.53** | 5.50** | 14.65* | 3.00† |
| Household floor material | ||||||
| Mud | 6.0 | 5.8 | 14.3 | 5.0 | 23.3 | 15.8 |
| Not mud | 4.9 | 4.4 | 12.5 | 3.6 | 21.7 | 15.9 |
| 3.57 | 7.19* | 2.50 | 4.35† | 3.83** | 0.03 | |
| Overall | 5.7 | 5.4 | 13.8 | 4.6 | 22.5 | 15.9 |
The figures for various levels of predictors represent the percentage of children experiencing disease
*p<0.01.
**p<0.05.
†p<0.1.
ARI, acute respiratory infection.
Adjusted ORs for experiencing diarrhoea and their associated CI for the predictor variables are presented in table 3. Once the effect of other variables was controlled for, in all the three countries, age of children and educational status of mother showed significant association with prevalence of diarrhoea. In Bangladesh, Nepal and Pakistan, children below 1 year of age were 63% (OR 1.63, CI 1.23 to 2.16), 219% (OR 3.19, CI 2.51 to 4.05) and 156% (OR 2.56, CI 2.26 to 2.91) more likely to experience diarrhoea with respect to those aged above 3 years (the reference category). With respect to the reference category, children aged between 1 and 3 years were also significantly more likely to experience diarrhoea. In Bangladesh, children from mothers with no or incomplete primary and incomplete secondary educational levels were 70% (OR 1.70, CI 1.16 to 2.49) and 69% (OR 1.69, CI 1.20 to 2.38) more likely to experience diarrhoea with respect to those from mothers with secondary or higher level of education. In Pakistan, children from households categorised as low and middle wealth status were significantly more likely to experience diarrhoea with respect to those with high economic status. However, for the children from Bangladesh and Pakistan, the wealth status of household was not significantly associated with the prevalence of diarrhoea (p>0.05). Children from households using worst toilet facilities (in terms of improvement and sharing status) were more likely to experience diarrhoea; however, the association is statistically significant for the children in Nepal only.
Table 3.
The adjusted ORs (CI) for the studied covariates from binary multivariable logistic regression models for children experiencing diarrhoea for Bangladesh, Nepal and Pakistan
| Variables (reference category) levels | OR of diarrhoea (95% CI) | ||
| Bangladesh | Nepal | Pakistan | |
| Age of child (36–59 months) | |||
| 0–11 | 1.63* (1.23 to 2.16) | 3.19* (2.51 to 4.05) | 2.56* (2.26 to 2.91) |
| 12–35 | 1.71* (1.36 to 2.14) | 3.29* (2.68 to 4.04) | 2.24* (2.01 to 2.50) |
| Place of residence (urban) | |||
| Rural | 0.87 (0.69 to 1.12) | 0.92 (0.68 to 1.25) | 0.83* (0.73 to 0.94) |
| Mother’s education (secondary or higher) | |||
| Incomplete primary | 1.70* (1.16 to 2.49) | 1.41** (1.03 to 1.93) | 1.27* (1.08 to 1.48) |
| Incomplete secondary | 1.69* (1.20 to 2.38) | 1.55* (1.14 to 2.10) | 1.19** (1.0 1 to 1.40) |
| Mother’s access to mass media (have access) | |||
| No access | 1.16 (0.91 to 1.48) | 1.07 (0.85 to 1.35) | 1.01 (0.90 to 1.13) |
| Age of mother at the time of survey (30–49 years) | |||
| 15–19 | 0.94 (0.67 to 1.30) | 0.83 (0.59 to 1.17) | 1.40** (1.05 to 1.86) |
| 20–29 | 0.94 (0.74 to 1.21) | 0.99 (0.81 to 1.20) | 1.17* (1.07 to 1.29) |
| Wealth status (high) | |||
| Low | 0.79 (0.48 to 1.30) | 0.71† (0.47 to 1.06) | 1.53* (1.23 to 1.91) |
| Middle | 0.78 (0.53 to 1.16) | 0.94 (0.66 to 1.33) | 1.49* (1.26 to 1.77) |
| Source of drinking water (hygienic in premises) | |||
| Unimproved or not in premises | 1.21 (0.96 to 1.53) | 1.10 (0.91 to 1.31) | 0.93 (0.83 to 1.04) |
| Toilet facility (ideal) | |||
| Worst | 1.06 (0.76 to 1.46) | 1.29** (1.04 to 1.59) | 1.10 (0.97 to 1.25) |
| Moderate | 1.03 (0.82 to 1.29) | 0.92 (0.70 to 1.20) | 1.01 (0.88 to 1.17) |
| No of adults per room (up to two adults per room) | |||
| More than two adults | 0.76* (0.62 to 0.93) | 1.12 (0.95 to 1.33) | 1.06 (0.95 to 1.17) |
| Household floor material (not mud) | |||
| Floor made of mud | 1.27 (0.89 to 1.81) | 1.11 (0.83 to 1.48) | 0.94 (0.82 to 1.08) |
*p<0.01.
**p<0.05.
†p<0.1.
Adjusted ORs for experiencing ARI with associated CI for the studied variables were presented in table 4. Like diarrhoea, younger children were significantly more likely to experience ARI than older children. In Bangladesh and Pakistan, children of mothers with incomplete primary or incomplete secondary level of education were more likely to experience ARI than those from secondary or higher level of education. In Pakistan, with respect to the children of mothers with secondary or higher level of education, those of mothers with incomplete primary and incomplete secondary level of education were 35% (OR 1.35, CI 1.13 to 1.62) and 24% (OR 1.24, CI 1.04 to 1.49) more likely to experience ARI. However, the relationship of maternal education and ARI of children is not significant in Nepal. In Bangladesh and Nepal, children from households categorised as low or middle wealth status were significantly more likely to experience ARI with respect to those with high status. However, the association of wealth with ARI was not significant for Nepal. In Bangladesh, children from households not using ideal cooking facilities (using solid fuel while cooking inside house) were 62% (OR 1.62, CI 1.22 to 2.16) more likely to experience ARI; however, the association was not statistically significant in Nepal and Pakistan (p>0.05). Over the countries, neither the degree of crowding nor the household floor material showed consistent association with either diarrhoea or ARI.
Table 4.
The adjusted ORs (CI) for the studied covariates from binary multivariable logistic regression models for children experiencing ARI for Bangladesh, Nepal and Pakistan
| Variables (reference category) levels | OR of ARI (95% CI) | ||
| Bangladesh | Nepal | Pakistan | |
| Age of child (36+ months) | |||
| 0–11 | 2.21* (1.66 to 2.92) | 1.99* (1.23 to 2.79) | 1.49* (1.30 to 1.72) |
| 12–35 | 1.74* (1.36 to 2.22) | 2.12* (1.54 to 2.91) | 1.49* (1.32 to 1.68) |
| Place of residence (urban) | |||
| Rural | 1.10 (0.83 to 1.45) | 0.66† (0.41 to 1.07) | 1.14† (0.98 to 1.34) |
| Mother’s education (secondary or higher) | |||
| Incomplete primary | 1.31 (0.88 to 1.96) | 0.86 (0.54–1.38) | 1.35* (1.13 to 1.62) |
| Incomplete secondary | 1.63* (1.14 to 2.33) | 1.02 (0.64 to 1.63) | 1.24** (1.04 to 1.49) |
| Mother’s access to mass media (have access) | |||
| No access | 0.96 (0.75 to 1.22) | 1.02 (0.69 to 1.49) | 0.99 (0.87 to 1.12) |
| Age of mother at the time of survey (30–49 years) | |||
| 15–19 | 1.47* (1.05 to 2.06) | 0.95 (0.55 to 1.64) | 1.29 (0.93 to 1.78) |
| 20–29 | 1.20 (0.91 to 1.57) | 1.01 (0.74 to 1.38) | 1.02 (0.91 to 1.13) |
| Wealth status (high) | |||
| Low | 2.25* (1.36 to 3.70) | 2.25** (1.08 to 4.69) | 0.94 (0.74 to 1.20) |
| Middle | 1.61* (1.08 to 2.41) | 2.68* (1.41 to 5.10) | 1.09 (0.90 to 1.31) |
| Household cooking fuel (ideal) | |||
| Not ideal | 1.62* (1.22 to 2.16) | 1.31† (0.96 to 1.79) | 1.01 (0.88 to 1.16) |
| No of adults per room (up to two adults per room) | |||
| More than two adults | 0.95 (0.77 to 1.17) | 1.03 (0.79 to 1.36) | 0.96 (0.86 to 1.08) |
| Household floor material (not mud) | |||
| Floor made of mud | 0.77 (0.55 to 1.08) | 1.04 (0.67 to 1.31) | 0.92 (0.79 to 1.07) |
*p<0.01.
**p<0.05.
†p<0.1.
ARI, acute respiratory infection.
Discussion
Prevalence of two major infectious diseases, diarrhoea and ARI, is relatively high among young children in the South Asian region. The study was conceived with objectives of comparing the association of potential predictors, in particular sustainable household environment and maternal education, on disease episodes among preschoolers from three South Asian countries, Bangladesh, Nepal and Pakistan.
The highest prevalence rates were in Pakistan for both diarrhoea and ARI, and in Nepal, for diarrhoea. Bangladesh is considered as a paradox in terms of good health outcomes despite economic poverty.36 37 Even the disadvantaged children from Bangladesh (from households categorised as poor and using unimproved water and toilet facilities) possess lower risk of experiencing diarrhoea with respect to economically advantaged children in Nepal and Pakistan. Similar outcomes have been reported,38 where it is mentioned that Pakistan lags behind the MDG in many aspects including child health. Though the prevalence of ARI is low in Nepal, prevalence of diarrhoea is higher in the country. This may have resulted from lack of sustainable household environment (defined as improved water source and hygienic sanitation) or knowledge of healthy practice of mother (measured by level of schooling).
Rural–urban setting was not found to have a significant effect on the prevalence of either diarrhoea or ARI. Source of drinking water, number of adults sharing a living room and floor materials all showed inconsistent effects on the prevalence of childhood diarrhoea across the countries studied.
In all the three studied countries, bivariate analyses showed that the presence of diarrhoea significantly increases the likelihood of the prevalence of ARI and vice-versa. However, it is important not to include diarrhoea in the multiple model of ARI prevalence and vice versa, because there is a high degree of overlap in risk factors for diarrhoea and ARI, for example, age of child, crowding, poor housing. Furthermore, the short recall period employed in the DHS (2 weeks) means that the data are clearly cross-sectional and the lag effect of one disease on another cannot be measured with the data at hand. Similar results were observed in previous studies where the epidemiology of diarrhoea and ARI overlapped. This is highly likely to be due to shared risk factors or compromised immune function.39–41 Health policy needs to take a holistic approach to combatting childhood infections due to the clear presence of comorbidity, at least in the case of diarrhoea and ARI shown in this article.
Younger children possess significantly higher risks of experiencing morbidity than older; the result is consistent with previous studies in Bangladesh and elsewhere.8 14 The immune system may not be developed at earlier ages, and younger children may be infected from unhygienic feeding practices (water, bottles, and so on) and unclean surroundings. Diarrhoea pathogens, like Escherichia coli, are commonly transmitted via impure water, unhygienic utensils or poor food handling.42 While crawling, children explore their immediate environment and may pick up infections. Inappropriate dietary supplementation may also hinder children’s developing immune system, which can be overcome through exclusive breastfeeding for recommended periods of time. Breastfeeding data are available in the DHS; however, it has not been included in the current analyses due to its high degree of confounding with age.
Of most interest is the result that maternal educational status showed significant positive influence on reducing the prevalence of diarrhoea and ARI, and that the effects are more evident when the educational attainment is at least secondary or higher.
Data limitations
Although the DHS adopted appropriate survey methodology to obtain a representative sample, the final sample does not guarantee complete representativeness at national and regional levels. DHS are cross-sectional surveys which collect information regarding the disease episodes for a single point of time. Such studies can yield information on association but not impact. The seasonal variations in the prevalence of the disease episodes are not addressed in the data. Moreover, the disease episodes are determined on the basis of self-reporting of mothers and not followed by any clinical examination. To reduce the reporting bias due to memory lapse, a short recall period (2 weeks) is considered while collecting morbidity related information. Children who were not de-jure resident at the time of the survey were excluded from the analysis. The exclusion may lead a bias to the outcomes; however, the amount of bias is likely to be small. Finally, the datasets do not represent same time point for the studied countries, though the largest time difference is only 3 years.
Conclusion
This study focuses on three South Asian countries with relatively higher prevalence of childhood diarrhoea and ARI on the worldwide scale. Sustainable household environment, as mentioned in the SDG, in terms of flooring, water, toilet and cooking facilities was not found to have the greatest association with morbidity. Nor was wealth a main driver, as its association with childhood diarrhoea and ARI was only statistically significant in half of the settings considered in this paper. Of far more importance was the knowledge base of a child’s primary caregiver (typically the mother) regarding the potential risks of infection and the impacts of infection on survival and well-being. These results indicate that the SDG of good health and well-being needs to be tackled by incorporating quality health education along with the goals of clean water and sanitation for all and no poverty. According to our findings, maternal education could be effective in reducing child morbidity only when it is at complete secondary level or higher. An effective basic knowledge base formed through policies that incorporate health education in school curricula at primary and secondary level has a good chance of making an impact, especially since the female primary school enrolment rate in Nepal and Bangladesh is already above 90%. Alternative ways to develop knowledge of healthy practices among the mass population could be delivered through mass media. Well-developed motivational programs incorporating mass media, health professionals, community health workers, community leaders, government and non-government organisations may help improve population awareness of the causes and consequences of infectious diseases. These programs may be more essential for the countries like Pakistan where the percentages of children suffering infectious diseases are relatively higher and female school enrolment rate is relatively lower.
Supplementary Material
Footnotes
Contributors: MMH conceptualised the study and developed the methodology. Data interpretation was undertaken by both authors and they are responsible for the drafting of the final manuscript.
Competing interests: None declared.
Patient consent: Secondary analysis of publicly available, de-identified data involved, and so no consent sought.
Provenance and peer review: Not commissioned; externally peer reviewed.
Data sharing statement: Data are available upon request from the Demographic and Health Survey Program (https://dhsprogram.com/).
References
- 1. Liu L, Oza S, Hogan D, et al. Global, regional, and national causes of child mortality in 2000–13, with projections to inform post-2015 priorities: an updated systematic analysis. Lancet 2015. 2015;385:430–40. 10.1016/S0140-6736(14)61698-6 [DOI] [PubMed] [Google Scholar]
- 2. Bhutta ZA, Das JK, Walker N, et al. Interventions to address deaths from childhood pneumonia and diarrhoea equitably: what works and at what cost? Lancet 2013;381:1417–29. 10.1016/S0140-6736(13)60648-0 [DOI] [PubMed] [Google Scholar]
- 3. UNICEF. Pneumonia and diarrhea: tackling the deadliest diseases for the world’s poorest children. New York: UNICEF, 2012. [DOI] [PubMed] [Google Scholar]
- 4. Checkley W, Buckley G, Gilman RH, et al. Multi-country analysis of the effects of diarrhoea on childhood stunting. Int J Epidemiol 2008;37:816–30. 10.1093/ije/dyn099 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5. Edmond K, Scott S, Korczak V, et al. Long term sequelae from childhood pneumonia; systematic review and meta-analysis. PLoS One 2012;7:e31239. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6. Qazi S, Aboubaker S, MacLean R, et al. Ending preventable child deaths from pneumonia and diarrhoea by 2025. development of the integrated global action plan for the prevention and control of pneumonia and diarrhoea. Arch Dis Child 2015;100 (Suppl 1):S23–S28. 10.1136/archdischild-2013-305429 [DOI] [PubMed] [Google Scholar]
- 7. Walker CLF, Rudan I, Liu L, et al. Global burden of childhood pneumonia and diarrhea. Lancet 2013;381:1405–16. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8. Bbaale E. Determinants of diarrhoea and acute respiratory infection among under-fives in Uganda. Australas Med J 2011;4:400–9. 10.4066/AMJ.2011.723 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9. Budge PJ, Griffin MR, Edwards KM, et al. Acute viral respiratory illnesses in Andean children: a household-based cohort study. Ped Inf Dis J 2014;33:443. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10. Dostal M, Pastorkova A, Rychlik S, et al. Comparison of child morbidity in regions of Ostrava, Czech Republic, with different degrees of pollution: a retrospective cohort study. Environ Health 2013;12:74 10.1186/1476-069X-12-74 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11. Tumwine JK, Thompson J, Katua-Katua M, et al. Diarrhoea and effects of different water sources, sanitation and hygiene behaviour in East Africa. Trop Med Int Health 2002;7:750–6. 10.1046/j.1365-3156.2002.00927.x [DOI] [PubMed] [Google Scholar]
- 12. Mukhtar A, Mohamed Izham MI, Pathiyil RS. A survey of mothers' knowledge about childhood diarrhoea and its management among a marginalised community of Morang, Nepal. Australas Med J 2011;4:474–9. 10.4066/AMJ.2011.821 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13. Ghasemi AA, Talebian A, Alavi NM, Masoudi AN, et al. Knowledge of mothers in management of diarrhea in under-five children, in Kashan, Iran. Nurs Midwifery Stud 2013;1:158–62. 10.5812/nms.10393 [DOI] [Google Scholar]
- 14. Kamal MM, Hasan MM, Davey R. Determinants of childhood morbidity in Bangladesh: evidence from the demographic and health survey 2011. BMJ Open 2015;5:e007538 10.1136/bmjopen-2014-007538 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15. Wakefield MA, Loken B, Hornik RC. Use of mass media campaigns to change health behaviour. Lancet 2010;376:1261–71. 10.1016/S0140-6736(10)60809-4 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16. Asakitikpi AE. Acute diarrhoea: mothers’ knowledge of ORT and its usage in Ibadan metropolis, Nigeria. Ethno-Med 2010;4:125–30. [Google Scholar]
- 17. Singh A, Singh MN. Diarrhoea and acute respiratory infections among under-five children in slums: evidence from India. PeerJ PrePrints 2014;2:e208v1. [Google Scholar]
- 18. Nundy S, Gilman RH, Xiao L, Ortega YR, Cabrera L, et al. Wealth and its associations with enteric parasitic infections in a low-income community in Peru: use of principal component analysis. Am J Trop Med Hyg 2011;84:38–42. 10.4269/ajtmh.2011.10-0442 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19. Hatt LE, Waters HR. Determinants of child morbidity in Latin America: a pooled analysis of interactions between parental education and economic status. Soc Sci Med 2006;62:375–86. 10.1016/j.socscimed.2005.06.007 [DOI] [PubMed] [Google Scholar]
- 20. Giashuddin MS, Kabir M, Hasan M. Economic disparity and child nutrition in Bangladesh. Indian J Pediatr 2005;72:481–7. 10.1007/BF02724424 [DOI] [PubMed] [Google Scholar]
- 21. Dora C, Haines A, Balbus J, et al. Indicators linking health and sustainability in the post-2015 development agenda. Lancet 2015;385:380–91. 10.1016/S0140-6736(14)60605-X [DOI] [PubMed] [Google Scholar]
- 22. Fink G, Günther I, Hill K. The effect of water and sanitation on child health: evidence from the demographic and health surveys 1986–2007. Int J Epidemiol 2011;40:1196–204. 10.1093/ije/dyr102 [DOI] [PubMed] [Google Scholar]
- 23. Speich B, Croll D, Fürst T, et al. Effect of sanitation and water treatment on intestinal protozoa infection: a systematic review and meta-analysis. Lancet Infect Dis 2016;16:87–99. 10.1016/S1473-3099(15)00349-7 [DOI] [PubMed] [Google Scholar]
- 24. Fuller JA, Westphal JA, Kenney B, et al. The joint effects of water and sanitation on diarrhoeal disease: a multicountry analysis of the demographic and Health surveys. Trop Med Int Health 2015;20:284–92. 10.1111/tmi.12441 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25. Shahnawaz K, Kumar M, Singh S, et al. Ncidence of diarrh e a l diseases among children in Kishanganj district of bihar. J Med Dent Sci 2014;3:3040–7. 10.14260/jemds/2014/2241 [DOI] [Google Scholar]
- 26. Sustainable Development Knowledge Platform, 2015. https://sustainabledevelopment.un.org/ (accessed 1 Sep 2016).
- 27. Colosia AD, Masaquel A, Hall CB, et al. Residential crowding and severe respiratory syncytial virus disease among infants and young children: a systematic literature review. BMC Infect Dis 2012;12:95 10.1186/1471-2334-12-95 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28. Lim SS, Vos T, Flaxman AD, et al. A comparative risk assessment of burden of disease and injury attributable to 67 risk factors and risk factor clusters in 21 regions, 1990–2010: a systematic analysis for the Global Burden of Disease Study 2010. Lancet 2012;380:2224–60. 10.1016/S0140-6736(12)61766-8 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29. Fatmi Z, White F. A comparison of 'cough and cold' and pneumonia: risk factors for pneumonia in children under 5 years revisited. Int J Infect Dis 2002;6:294–301. 10.1016/S1201-9712(02)90164-5 [DOI] [PubMed] [Google Scholar]
- 30. Chafe ZA, et al. Household cooking with solid fuels contributes to ambient PM2.5 air pollution and the burden of disease. Diss. University of British Columbia 2015. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31. Central Intelligence Agency. The world factbook. https://www.cia.gov/library/publications/the-world-factbook/ (accessed 28 Oct 2016).
- 32. World GDP (Nominal) Ranking, 2015. http://statisticstimes.com/economy/world-gdp-ranking.php (accessed 28 Oct 2016).
- 33. National Institute of Population Research and Training (NIPORT), Mitra and Associates, ICF International. Bangladesh demographic and health survey2014. Dhaka, Bangladesh, and Rockville, Maryland, USA: NIPORT, Mitra and Associates, and ICF International; 2016. [Google Scholar]
- 34. Hosmer Jr DW, Lemeshow S. Applied logistic regression: John Wiley & Sons, 2004. [Google Scholar]
- 35. IBM Corp. IBM SPSS Statistics for Windows, Version 22.0. Armonk, NY: IBM Corp; 2013. [Google Scholar]
- 36. Chowdhury AM, Bhuiya A, Chowdhury ME, et al. The Bangladesh paradox: exceptional health achievement despite economic poverty. Lancet 2013;382:1734 10.1016/S0140-6736(13)62148-0 [DOI] [PubMed] [Google Scholar]
- 37. Nasrin D, Wu Y, Blackwelder WC, et al. Health care seeking for childhood diarrhea in developing countries: evidence from seven sites in Africa and Asia. Am J Trop Med Hyg 2013;89:3–12. 10.4269/ajtmh.12-0749 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38. Rizvi A, Bhatti Z, Das JK, et al. Pakistan and the millennium development goals for maternal and child health: Progress and the way forward. Paediatr Int Child Health 2015;35:287–97. 10.1080/20469047.2015.1109257 [DOI] [PubMed] [Google Scholar]
- 39. Black RE, Morris SS, Bryce J. Where and why are 10 million children dying every year? Lancet 2003;361:2226–34. 10.1016/S0140-6736(03)13779-8 [DOI] [PubMed] [Google Scholar]
- 40. Walker CL, Perin J, Katz J, et al. Diarrhea as a risk factor for acute lower respiratory tract infections among young children in low income settings. J Glob Health 2013;3:60–7. 10.7189/jogh.03.010402 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41. Schmidt WP, Cairncross S, Barreto ML, et al. Recent diarrhoeal illness and risk of lower respiratory infections in children under the age of 5 years. Int J Epidemiol 2009;38:766–72. 10.1093/ije/dyp159 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42. Black RE. Diarrheal diseases and child morbidity and mortality. Popul Dev Rev 1984;10:141–61. 10.2307/2807959 [DOI] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.