

Abstract
Objectives
To evaluate gender differences in outcomes in patents with ST-segment elevation myocardial infarction (STEMI) planned for primary percutaneous coronary intervention (PPCI).
Settings
A prespecified gender analysis of the multicentre, randomised, double-blind Administration of Ticagrelor in the catheterisation Laboratory or in the Ambulance for New ST elevation myocardial Infarction to open the Coronary artery.
Participants
Between September 2011 and October 2013, 1862 patients with STEMI and symptom duration <6 hours were included.
Interventions
Patients were assigned to prehospital versus in-hospital administration of 180 mg ticagrelor.
Outcomes
The main objective was to study the association between gender and primary and secondary outcomes of the main study with a focus on the clinical efficacy and safety outcomes. Primary outcome: the proportion of patients who did not have 70% resolution of ST-segment elevation and did not meet the criteria for Thrombolysis In Myocardial Infarction (TIMI) flow 3 at initial angiography. Secondary outcome: the composite of death, MI, stent thrombosis, stroke or urgent revascularisation and major or minor bleeding at 30 days.
Results
Women were older, had higher TIMI risk score, longer prehospital delays and better TIMI flow in the infarct-related artery. Women had a threefold higher risk for all-cause mortality compared with men (5.7% vs 1.9%, HR 3.13, 95% CI 1.78 to 5.51). After adjustment, the difference was attenuated but remained statistically significant (HR 2.08, 95% CI 1.03 to 4.20). The incidence of major bleeding events was twofold to threefold higher in women compared with men. In the multivariable model, female gender was not an independent predictor of bleeding (Platelet Inhibition and Patient Outcomes major HR 1.45, 95% CI 0.73 to 2.86, TIMI major HR 1.28, 95% CI 0.47 to 3.48, Bleeding Academic Research Consortium type 3–5 HR 1.45, 95% CI 0.72 to 2.91). There was no interaction between gender and efficacy or safety of randomised treatment.
Conclusion
In patients with STEMI planned for PPCI and treated with modern antiplatelet therapy, female gender was an independent predictor of short-term mortality. In contrast, the higher incidence of bleeding complications in women could mainly be explained by older age and clustering of comorbidities.
Clinical trial registration
NCT01347580;Post-results.
Keywords: myocardial infarction, STEMI, gender, primary PCI, ATLANTIC, ticagrelor
Strengths and limitations of this study.
All patients were planned for primary percutaneous coronary intervention (PPCI).
Current PPCI techniques and novel antiplatelet therapy were used.
Appropriate statistical methods used to adjust for baseline differences between genders.
Our analysis, although prespecified, is applicable to the population studied.
The large imbalance in the proportion of men and women included caused a reduced study power for definitely excluding significant differences in outcomes.
Introduction
Recent studies have provided evidence of gender differences in the pathophysiology and the clinical expression of atherosclerosis.1 Several registries in patients with ST-segment elevation myocardial infarction (STEMI) have consistently shown a considerably higher risk of adverse outcomes in women compared with men. Nevertheless, there are conflicting results regarding whether gender is an independent contributor to this observation or the higher risk in women depends on differences in baseline characteristics and comorbidities between genders.2–8 Although registries of patients with STEMI usually include large, unselected populations, they share some inherent limitations. Their results are certainly influenced by differences between genders in the use of timely reperfusion therapy and evidence-based drug therapies as well as undetected confounding factors.9 10 Therefore, reports of gender-based analyses of randomised controlled trials are of crucial importance in an effort to minimise inequality in the management and evaluate gender as a potential independent risk factor for adverse outcome. Only a few randomised trials of patients with STEMI treated with primary percutaneous coronary intervention (PPCI) have reported results in the context of gender.11 12 New treatments (eg, ticagrelor or prasugrel), special efforts to reduce bleeding (ie, increased use of radial arterial access, provisional rather than routine use of glycoprotein (GP) IIb/IIIa inhibitor), shorter delay times to reperfusion and a growing awareness regarding gender differences in the management and importance of adherences to evidence-based treatment could contribute to improved ischaemic and bleeding outcomes in female patients with STEMI.
In the Administration of Ticagrelor in the catheterisation laboratory or in the Ambulance for New ST elevation myocardial Infarction to open the Coronary artery (ATLANTIC) trial, prehospital administration of ticagrelor appeared to be safe but did not significantly improve outcome compared with in-hospital administration in patients with STEMI, treated with PPCI according to the current modern standards.13
We present a prespecified gender analysis of the ATLANTIC trial, with the aim of studying the association between gender and outcome.
Methods
The ATLANTIC study was an international, randomised, double-blind, placebo-controlled study with 30 days follow-up. The design of the study, inclusion and exclusion criteria, outcome definitions and principal results have previously been described.13 14 Briefly, 1862 patients presenting with STEMI, <6 hours after symptom onset, were included and randomised to prehospital (in the ambulance) versus in-hospital (in the catheterisation laboratory) treatment with a loading dose of ticagrelor (180 mg) in addition to aspirin and standard clinical care. All patients were to subsequently receive ticagrelor 90 mg twice daily for 30 days, after which it was recommended that ticagrelor should be continued for up to 12 months. Prehospital administration of a GP IIb/IIIa inhibitor was left to the physician’s discretion. Periprocedural use of parenteral anticoagulants was also left to the physician’s discretion, according to the local practice.
The proportion of patients who did not have ≥70% resolution of ST-segment elevation before PCI and/or did not meet the criteria for Thrombolysis In Myocardial Infarction (TIMI) flow 3 in the infarct-related artery (IRA) at initial angiography was the primary outcome of the ATLANTIC trial. Secondary outcomes (clinical efficacy outcomes) included the composite of death, MI, stent thrombosis, stroke or urgent revascularisation at 30 days and definite stent thrombosis at 30 days. Safety outcomes included major and minor bleeding over the 30-day treatment period. Bleeding risk was evaluated using the TIMI, Bleeding Academic Research Consortium (BARC) and Study of Platelet Inhibition and Patient Outcomes (PLATO) bleeding definitions.14
The main objective of our analysis was to study the association between gender and primary and secondary outcomes of the main study with a special focus on the clinical efficacy and safety outcomes. The interaction of gender subgroups with randomised treatment effects was also investigated.
The trial design and protocol were approved by the national regulatory authorities in all the participating countries and by the local ethics committee or institutional review board at each participating site. All patients provided written informed consent.
Statistical analysis
Continuous variables are presented by their mean and SD or median and 25th−75th percentiles as appropriate. Categorical variables are presented as counts and percentages. Baseline and periprocedural characteristics were compared according to gender by χ2 tests for categorical variables and Student’s t-test or Mann-Whitney U test for continuous variables, depending on if the variable of interest was normally distributed or not. A p value <0.05 is considered to indicate statistical significance.
The incidence of events over time by gender is presented by Kaplan-Meier curves.
In order to study the association between gender and the clinical efficacy and safety outcomes, independent of randomised treatment as well as the possible interactions between gender and randomised treatment with respect to the outcomes, HRs with 95% CIs were derived from Cox proportional hazards models. In the unadjusted (crude) model, gender was the only explanatory variable whereas in the adjusted multivariable model, gender was forcibly included and the other variables were chosen by using a forward stepwise selection algorithm with a significant cut-off level of 0.05 for inclusion. Selection of covariates included in the multivariable analysis was based on previous studies3 4 6 15 and clinical experience. Univariate analysis was not performed. However, this is a common practice in observational studies and we included 18 covariates in our multivariable analysis that, we believe, incorporated all possible predictors of adverse outcomes in a STEMI population.
Adjustment variables included age, weight, prior MI, prior PCI, patient’s history of diabetes, hypertension, non-haemorrhagic stroke, gastrointestinal bleeding, time from symptom onset to pre-PCI ECG, admission Killip class (as a dichotomous variable 1/>1), baseline haemoglobin, estimated glomerular filtration rate (eGFR) according to the Modification of Diet in Renal Disease (MDRD) formula, access site, use of GP IIIb/IIa inhibitor, bivalirudin and unfractionated heparin (UFH), location of MI and revascularisation. To evaluate the importance of early mortality, a landmark analysis of the clinical efficacy outcomes was also performed from 48 hours after randomisation (arbitrarily defined) to the end of the study. In order to explore the importance of bleeding on the clinical efficacy outcomes, a separate analysis was also performed by censoring the patients who reported a PLATO major bleeding at the time of the onset of a bleeding event.
A comparable statistical process was used to compare gender differences in the effect of randomised treatment by constructing logistic regression models. ORs with 95% CIs were presented. The above process for Cox regression and logistic regression was also used to explore the interaction effect of gender and treatment.
For most of the variables included in the multivariable models, only few patients had missing data (<10 patients). However, 7% of patients had missing values for creatinine, 5% for haemoglobin and 4% for Killip class. The number of patients with complete data for multivariable Cox proportional hazard models of the primary outcome was 1613 (88%).
All the analyses were performed using SAS v.9.3.
Results
Baseline and periprocedural characteristics stratified by gender
Demographic and clinical characteristics
The study population consisted of 369 (20%) women. They were older (mean age 69 vs 59 years, p<0.01), had lower body mass index (BMI), higher TIMI risk score, more often had a history of hypertension, chronic obstructive pulmonary disease and stroke. Men had more frequent prior PCI. No difference was observed between genders with respect to acute heart failure (Killip class >1) and only a minority of patients presented with cardiogenic shock (table 1).
Table 1.
Baseline, clinical and periprocedural characteristics according to gender
| Characteristics | Women (n=369) | Men (n=1493) | p Value |
| Age, years; mean (SD) | 69 (13.0) | 59 (11) | <0.01 |
| Age ≥75 years | 153 (41.5) | 151 (10.1) | <0.01 |
| BMI, kg/m2; median (IQR) | 25.6 (22.5–29.1) | 26.5 (24.3–29.4) | <0.01 |
| Patient’s history of: | |||
| Diabetes mellitus | 48 (13.0) | 205 (13.7) | 0.72 |
| Hypertension | 190 (51.5) | 605 (40.5) | <0.01 |
| Dyslipidemia | 117 (31.7) | 536 (35.9) | 0.13 |
| Angina | 36 (9.8) | 157 (10.5) | 0.67 |
| Prior myocardial infarction | 24 (6.5) | 135 (9.0) | 0.67 |
| Prior PCI | 16 (4.3) | 124 (8.3) | <0.01 |
| Prior CABG | 1 (0.3) | 11 (0.7) | 0.32 |
| Prior non-haemorrhagic stroke | 8 (2.2) | 10 (0.7) | <0.01 |
| Chronic obstructive pulmonary disease | 22 (6.0) | 54 (3.6) | 0.04 |
| Gastrointestinal bleeding | 1 (0.3) | 16 (1.1) | 0.15 |
| Chronic renal disease | 7 (1.9) | 27 (1.8) | 0.91 |
| Index event information | |||
| First medical contact in ambulance | 280 (75.9) | 1132 (75.8) | 0.24 |
| Minutes from symptom onset to prehospital ECG, median (IQR) | 88 (49–169) | 70 (41–129) | <0.01 |
| Minutes from prehospital ECG to PCI, median (IQR) | 83 (68–101) | 80 (66–96) | 0.03 |
| Minutes from pre-PCI angiography to post-PCI angiography, median (IQR) | 36 (24–52) | 32 (23–45) | 0.03 |
| Received first loading dose | 369 (100) | 1488 (99.7) | 0.27 |
| Risk level at admission | |||
| Killip class | |||
| I | 332 (90.0) | 1349 (90.4) | 0.82 |
| IV | 2 (0,5) | 3 (0.2) | |
| TIMI risk score | |||
| 0–2 | 119 (32.2) | 1006 (67.4) | 0.01 |
| 3–6 | 231 (62.6) | 471 (31.5) | |
| >6 | 19 (5.1) | 16 (1.1) | |
| Culprit vessel | |||
| Left main artery | 4 (1.1) | 18 (1.2) | 0.63 |
| Left anterior descending artery | 141 (38.8) | 571 (39.0) | |
| Right coronary artery | 150 (41.3) | 590 (40.3) | |
| Left circumflex | 39 (10.7) | 196 (13.4) | |
| No culprit vessel identified | 28 (7.7) | 85 (5.8) | |
| Normal coronary angiography | 27 (7.4) | 76 (5.2) | 0.1 |
| Procedures for index event | |||
| Femoral access | 144 (39.7) | 445 (30.4) | <0.01 |
| Thromboaspiration | 160 (43.4) | 781 (52.3) | <0.01 |
| PCI | 309 (83.7) | 1321 (88.5) | 0.01 |
| With any stent | 288 (78.0) | 1248 (83.6) | 0.01 |
| With DES | 185 (50.1) | 761 (51.0) | 0.77 |
| Coronary artery bypass grafting | 4 (1.1) | 21 (1.4) | 0.63 |
| No revascularisation | 56 (15.2) | 151 (10.1) | <0.01 |
| Any glycoprotein IIb/IIIa inhibitor use | 115 (31.2) | 598 (40.1) | <0.01 |
| Glycoprotein IIb/IIIa inhibitor use before angiography | 14 (3.8) | 116 (7.8) | <0.01 |
| Intravenous anticoagulant prior to pre-PCI angiography | 231 (62.6) | 1027 (68.8) | 0.02 |
| Intravenous anticoagulant during hospitalisation* | 310 (84.0) | 1332 (89.2) | <0.01 |
| Heparin only | 135 (36.6) | 584 (39.1) | 0.02 |
| Bivalirudin only | 29 (7.9) | 65 (4.4) | 0.02 |
Variables presented as numbers (percentages) unless otherwise indicated.
*Includes all intravenous medications given on the date of the qualifying ECG and/or index PCI.
BMI, body mass index; CABG, coronary artery bypass grafting; DES, drug-eluting stent; PCI, percutaneous coronary intervention; TIMI, Thrombolysis In Myocardial Infarction.
Time delays
Women had significantly longer delay times, both from symptom onset to prehospital ECG (median 88 vs 70 min, p<0.01) and from pre-PCI to post-PCI angiography (median 36 vs 32 min, p=0.03).
Procedural characteristics, angiographic findings and medication during the index event
Coronary angiography was more often performed by femoral access in women (39.7% vs 30.4%, p<0.01). The genders did not differ according to IRA, with the left anterior descending artery involved in 38% of women and 39% of men. PPCI, with or without stent, was performed significantly more often in men (88.5% vs 83.7%, p<0.01), whereas the use of drug-eluting stents was similar. Thromboaspiration, GP IIb/IIIa inhibitors and intravenous anticoagulants were used less often in women (table 1).
Association between gender and outcomes independent of randomised treatment
Female gender was associated with significantly higher risk for the composite outcome of death, MI, stroke, urgent revascularisation or definite acute stent thrombosis compared with male gender (6.8% vs 3.9%, crude HR 1.79, 95% CI 1.12 to 2.86) (figure 1). This difference was mainly driven by a threefold higher risk for all-cause mortality in women compared with men (5.7% vs 1.9%, HR 3.13, 95% CI 1.78 to 5.51). Although the difference was attenuated in the multivariable model, gender was still associated with all-cause mortality at 30 days (HR 2.08, 95% CI 1.03 to 4.20) (figure 2 and table 2). Landmark analysis for events occurring within 48 hours, and between 48 hours and 30 days showed that 38% of the women and 36% of the men who did not survive the first month died within 48 hours. Comparison after excluding patients from further analysis at the time point of a PLATO major bleeding event still revealed a statistically significant association between women and all-cause mortality (4.3% vs 1.4%. HR 3.20, 95% CI 1.67 to 6.13). Similar result was obtained after adjustment but the difference between genders did not reach statistical significance (HR 2.15, 95% CI 0.93 to 5.00).
Figure 1.
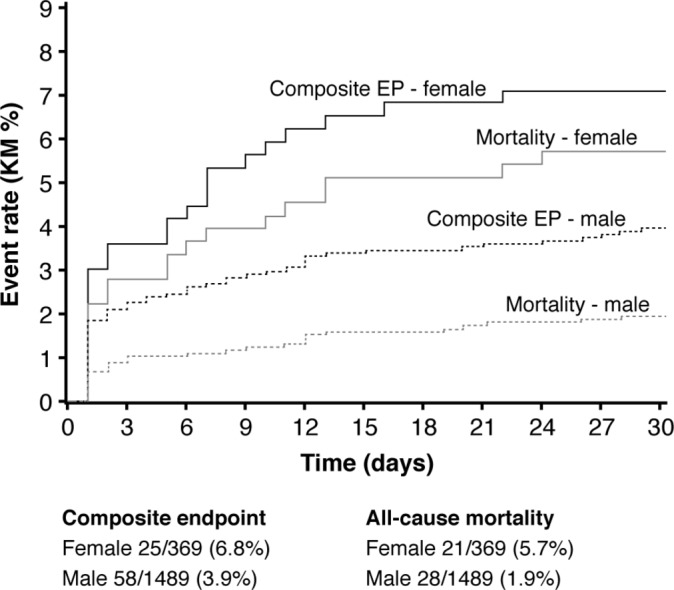
Cumulative Kaplan-Meier (KM) estimates of the incidence of the composite endpoint (EP) of death, MI, stroke, urgent revascularisation or definite acute stent thrombosis and all-cause mortality at 30 days by gender.
Figure 2.

Association between gender and clinical efficacy and safety outcomes independent of randomised treatment.
Table 2.
Association between gender and clinical outcomes independent of randomised treatment
| Outcomes | Female (n=369) | Male (n=1489) | Crude HR (95% CI) (n included=1858) |
Adjusted HR (95% CI)* (n included=1613) |
p Value * |
| Patients with end point, n (%) | Patients with end point, n (%) | ||||
| Mortality and cardiovascular outcomes | |||||
| Composite of death/MI/stroke/urgent revascularisation/definite acute stent thrombosis | 25 (6.8) | 58 (3.9) | 1.79 (1.12to 2.86) | 1.32 (0.77to 2.27) | 0.32 |
| Composite of death/MI/urgent revascularisation | 23 (6.2) | 50 (3.4) | 1.91 (1.17 to 3.13) | 1.33 (0.75to 2.36) | 0.32 |
| All-cause mortality | 21 (5.7) | 28 (1.9) | 3.13 (1.78 to 5.51) | 2.08 (1.03to 4.20) | 0.04 |
| Myocardial infarction | 3 (0.8) | 14 (0.9) | 0.90 (0.26to 3.13) | 0.82 (0.23to 2.85) | 0.76 |
| Stroke | 3 (0.8) | 3 (0.2) | 4.18 (0.84to 20.70) | 4.14 (0.84to 20.51) | 0.08 |
| Urgent revascularisation | 2 (0.5) | 11 (0.7) | 0.75 (0.17to 3.38) | 0.69 (0.15to 3.11) | 0.63 |
| Definite acute stent thrombosis | 3 (0.8) | 10 (0.7) | 1.23 (0.34to 4.49) | 1.29 (0.35to 4.76) | 0.70 |
| Acute stent thrombosis (definite or probable) | 11 (3.0) | 30 (2.0) | 1.53 (0.77to 3.05) | 0.88 (0.39to 1.98) | 0.76 |
| Safety outcomes | |||||
| PLATO major bleeding† | 17 (4.6) | 33 (2.2) | 2.15 (1.20to 3.85) | 1.45 (0.73to 2.86) | 0.29 |
| TIMI major bleeding† | 10 (2.7) | 14 (0.9) | 2.95 (1.31to 6-65) | 1.28 (0.47to 3.48) | 0.63 |
| TIMI major or minor bleeding† | 18 (4.9) | 54 (3.6) | 1.38 (0.81to 2.35) | 0.94 (0.51to 1.74) | 0.85 |
| BARC type 3–5 (major) bleeding† | 16 (4.3) | 31 (2.1) | 2.15 (1.18to 3.93) | 1.45 (0.72to 2.91) | 0.30 |
| BARC type 2–5 (major or minor) bleeding† | 20 (5.4) | 56 (3.8) | 1.48 (0.89to 2.47) | 1.03 (0.57to 1.84) | 0.93 |
*HR (for female vs male) and p value calculated from logistic regression model including gender, age, weight, prior myocardial infarction, prior percutaneous coronary intervention, diabetes, hypertension, non-haemorrhagic stroke, gastrointestinal bleeding, time from symptom onset to prehospital ECG, admission Killip class, baseline haemoglobin, estimated glomerular filtration rate, access site, glycoprotein IIb/IIIa inhibitor, bivalirudin or unfractionated heparin use during index procedure, revascularisation and location of myocardial infarction
†Non-CABG-related bleeding occurring up to the date of the last study visit (to the maximum of 32 days) are included in the table.
BARC, Bleeding Academic Research Consortium; CABG, coronary artery bypass grafting; MI, myocardial infarction; PLATO, Study of Platelet Inhibition and Patient Outcomes; TIMI, Thrombolysis in Myocardial Infarction.
Female gender was associated with lower risk for TIMI flow <3 in the IRA at initial angiography (adjusted OR 0.67, 95% CI 0.47 to 0.96). The risk of incomplete ST-segment elevation resolution (<70%) before PCI did not differ significantly between the genders (adjusted OR 1.11, 95% CI 0.73 to 1.71). The risk of abnormal TIMI flow in the IRA and incomplete ST-segment elevation resolution after PCI was similar in both genders (figure 3).
Figure 3.

Association between gender and primary and secondary outcomes, independent of randomised treatment.
Women had significantly higher risk for major bleeding complications compared with men, irrespective of the bleeding definition used (30-day PLATO major bleeding 4.6% vs 2.2%, HR 2.15, 95% CI 1.18 to 3.85, TIMI major bleeding at 30 days 2.7% vs 0.9%, HR 2.95, 95% CI 1.31 to 6.65, BARC type 3–5 bleeding 4.3% vs 2.1%, HR 2.15, 95% CI 1.18 to 3.93) (figure 4). However, after adjustment for baseline and clinical characteristics, female gender was no longer an independent predictor of risk for bleeding at 30 days (table 2 and figure 2).
Figure 4.
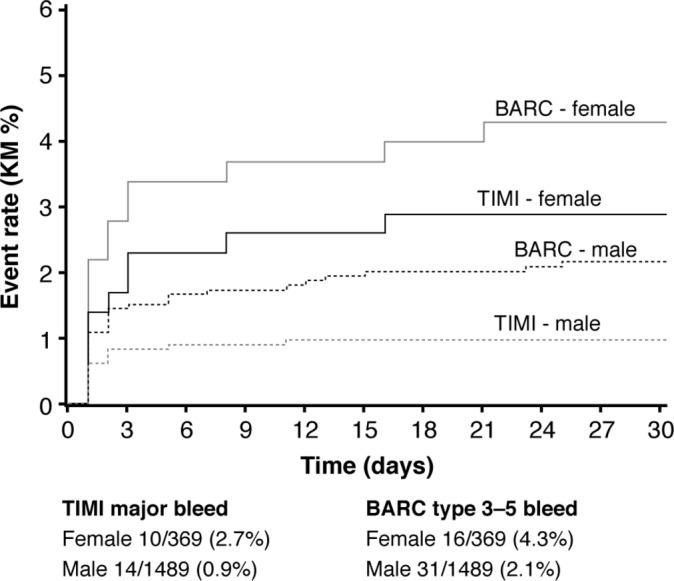
Cumulative Kaplan-Meier (KM) estimates of the incidence of the Thrombolysis In Myocardial Infarction (TIMI) major bleeding and Bleeding Academic Research Consortium (BARC) type 3–5 bleeding at 30 days by gender.
Association between gender and efficacy and safety of randomised treatment
Prehospital administration of ticagrelor compared with in-hospital administration resulted in a non-significant difference in the primary, secondary and safety outcomes. No significant interactions between randomised treatment and gender in terms of these outcomes were found in the unadjusted or adjusted model (test for interaction in the multivariable models; p=0.94 for all-cause mortality, p=0.55 for absence of TIMI flow grade 3 in the IRA at initial angiography, p=0.71 for absence of ≥70% resolution of pre-PCI ST-segment elevation, and p=0.31 for TIMI major bleeding at 30 days) (see online supplementary tables 1–3).
bmjopen-2016-015241supp001.pdf (247.1KB, pdf)
Discussion
In the present analysis, unadjusted data showed a significantly higher risk of short-term mortality and bleeding complications in women. After multivariable adjustment female gender remained an independent predictor of mortality, whereas advanced age and comorbidities could mainly explain the higher incidence of bleeding complications in women.
Undoubtedly, older age and clustering of comorbidities in women could explain a large part of the observed difference in short-term clinical outcomes in our study. However, the adjusted risk for death was still significantly higher in women. The contribution of gender, as independent risk factor, on adverse outcome may depend on the population studied. The age gap between genders in our population was substantially higher compared with previous studies, with a mean age difference of 10 years.12 16 In spite of appropriate statistical methods that were used for adjustment, adjustment for such age difference is awkward. Additionally, the age difference may indicate a selection bias. As identification and randomisation took place in the ambulance, young women with suspected STEMI were possibly not included in the study as alternative reasons for ST-segment elevation on prehospital ECG may have been considered more plausible in this group. Furthermore, a trend towards increased mortality with prehospital ticagrelor was observed in the ATLANTIC trial that was mainly attributed to a plausible imbalance between the two groups in terms of the severity of the presenting event. Given the low rate of all-cause mortality, unobserved confounders in elderly women with STEMI may have significantly contributed to our results and the findings of the main study. These factors may have a significant impact on the remaining higher adjusted risk for short-term mortality in women.
Previous observational studies in STEMI cohorts, without focus on patients treated with PPCI have shown a higher risk for early mortality in women.6 17 18 Significant differences in the rate of reperfusion therapy between genders and hidden confounders such as frailty in elderly women with STEMI may have influenced their results. Recent observational studies including patients treated with PPCI4 19 20 and prespecified gender analysis of randomised controlled trials11 12 16 21 22 have shown that the impact of gender on mortality could mainly be explained by differences in age and comorbidities between genders. On the contrary, an observational study and a meta-analysis have reported higher multivariable adjusted risk of early mortality in women with STEMI treated with PPCI.23 24 Differences in the population studied and in the covariates included in the multivariable analysis between studies may explain the conflicting results. Previous studies have clearly demonstrated the importance of body surface area and the eGFR on prognosis.25 26 In a meta-analysis, Berger et al showed that female gender was an independent predictor of early mortality in patients with STEMI. However, 30-day mortality was not statistically significant different between genders after additional adjustment for angiographic disease severity.27
In the present study, women had two to three times higher unadjusted risk for non-CABG-related bleedings, depending on the definition used. After adjustment for baseline characteristics, no significant difference remained. Female gender has previously been associated with higher risk for bleeding complications in patients with acute coronary syndrome.28–31 Known predictors of bleedings like advanced age, diabetes, hypertension, renal insufficiency and anaemia, are usually more often encountered in women with STEMI.15 Additionally, smaller body and vessel size, higher use of femoral access and overdosing of antithrombotic medication in women may explain the higher observed risk for bleeding. Procedural-related improvement such as increased use of radial access or smaller femoral sheaths and careful dose adjustment of antithrombotic medication, have resulted in a significant decline in the risk of bleeding/vascular complication during cardiovascular interventions the last years and have probably contributed to our results.32 The negative impact of bleedings on prognosis in patients with STEMI is well established.15 Our data showed that even after excluding patients from further analysis at the time of a PLATO major bleeding, the HR for early mortality in women versus men remained unchanged, implying that reducing the rate of major bleeding in women may improve their prognosis but is not the main reason for the observed difference between genders in the early mortality.
Some well-known gender disparities in the concomitant management of patients with STEMI remained unchanged. Women were less likely to be treated with GP IIb/IIIa inhibitors and thromboaspiration during PPCI despite lack of gender difference in protection from major adverse outcomes by GP IIb/IIIa inhibitors33 and benefit of thromboaspiration at the time when the study was conducted.34 Similar findings have been provided by large registries.7 8 Some of these lower rates of utilisation may be ‘appropriate’ given the higher TIMI 3 flow rates in the IRA pre-PPCI and lower rates of PPCI in women versus men. Furthermore, physician’s concern for higher risk of bleeding in older women with STEMI have certainly contributed to the lower use of GP IIb/IIIa inhibitors in women.
Although the impact of early reperfusion on mortality in patients with STEMI is now unquestionable,35 patients’ delay from symptom onset to prehospital ECG was not an independent predictor of mortality in our study, in agreement with results from previous gender analyses.36 37 A plausible explanation is an association between age and delay, and thus adjustment for age minimises the relative impact of delay. Furthermore, in PPCI, female gender has been associated with similar or even smaller infarct size than that in male gender, despite longer prehospital delays, indicating that other factors than larger infarct size secondary to longer prehospital delay mainly contribute to the observed higher unadjusted short-term mortality.36 The proportion of 30-day mortality that occurred within 48 hours of admission was similar in women and men (38% vs 36%, respectively) contrasting previous data where gender differences in early mortality were accounted for by excess very early (within 24–48 hours) deaths in women with STEMI.7 18 Cardiogenic shock and haemodynamic instability were key exclusion criteria in the ATLANTIC trial, which may have influenced these results. Cardiogenic shock has been shown to be more common in women and female gender has been highly associated with mortality in shock patients.20
In terms of ST-segment elevation resolution and TIMI flow 3 rates before and after PCI, no significant difference between genders was observed apart from a lower risk of abnormal coronary flow in IRA at initial angiography in women. The higher rate of TIMI flow 3 at initial angiography may be explained by the higher rate of normal coronary arteries as well as the less obstructive coronary artery disease in women with STEMI, which is in concordance with previous data.37
The analysis of the effect of gender on outcomes dependent on the randomised treatment showed no statistically significant interactions. Prehospital administration of ticagrelor did not improve pre-PCI or post-PCI coronary reperfusion as assessed by TIMI flow in IRA and resolution of ST elevation pre-PCI. Clinical efficacy outcomes were not significantly improved either. However, prehospital administration of ticagrelor was safe in both genders with similar rate of major and minor bleedings.
Strengths and limitations
The present study has some important limitations. Our results are applicable to the populations studied, patients with STEMI pretreated with ticagrelor and planned for primary PCI.
The ATLANTIC study population is from a randomised controlled trial, with inclusion and exclusion criteria contributing to differences relative to populations treated in routine clinical practice, and thereby limiting generalisability. However, the proportion of elderly patients (>75 years) was higher than in the PLATO trial, especially for women, and under-representation of women in clinical trials is a well-recognised problem. Moreover, the study was conducted at several centres and countries increasing external validity. Taken together, our results should be applied to a real-world STEMI population with caution.
Additionally, the ATLANTIC trial was not stratified by gender. The large imbalance in the proportion of men and women included, commonly encountered in a STEMI population, caused a reduced power for detecting or definitely excluding significant differences in some outcomes between the genders or to definitely exclude an interaction between gender and the randomised treatment.
The most important strength of our analysis is that patients were treated according to the current guidelines of STEMI, with PPCI as the reperfusion strategy of choice, administration of the modern ADP receptor blocker ticagrelor in addition to aspirin as soon as possible after the first medical contact, high use of radial access during catheterisation and adjuvant pharmacological treatment during PPCI with UFH or bivalirudin.38 Therefore, our study provides important information about differences and similarities between genders in patients with STEMI treated with current PCI techniques and pharmacological treatment.
Conclusion
In patients with STEMI, planned for PPCI and treated with modern antiplatelet therapy, female gender identifies a group of patients with high risk of early mortality in whom prompt efforts to improve outcome are warranted. Female gender was not an independent predictor of bleeding but advanced age and clustering of comorbidities in women could mainly explain their higher unadjusted risk for bleeding events compared with men. Prehospital administration of ticagrelor had a similar efficacy and safety profile in men and women with STEMI.
Supplementary Material
Acknowledgments
Statistical analysis was performed by Richard Cairns from Worldwide Clinical Trials UK. The authors would like to thank all patients who took part in this study. Editorial support was provided by Liz Anfield, Prime Medica, Knutsford, Cheshire.
Footnotes
Contributors: ES is responsible for the conception and design of the gender substudy of the ATLANTIC trial. DV is responsible for analyses and interpretation of the data and drafted the manuscript. SSL, JA, MJ, AC, MC, SGG, AWvH and GM have critically revised the manuscript and added important intellectual content. All authors have participated in the work and have read and approved the manuscript.
Funding: The main ATLANTIC trial was financed by AstraZeneca. Editorial support for this study was funded by AstraZeneca.
Competing interests: DV reports that he has no relationships relevant to the contents of this paper to disclose. SSL reports that she has no relationships relevant to the contents of this paper to disclose. JA reports receiving lecture fees from AstraZeneca. MJ reports receiving lecture fees from AstraZeneca and Sanofi. AC reports that he has no relationships relevant to the contents of this paper to disclose. MC reports that he has no relationships relevant to the contents of this paper to disclose. SGG reports receiving research grants and speaker/consulting honoraria from AstraZeneca, Daiichi-Sankyo, Eli Lilly, Sanofi, Bristol-Myers Squibb, Merck and The Medicines Company. AWvH reports receiving research and educational grants from Abbott, AstraZeneca, Eli Lilly/Daiichi-Sankyo, Merck/Correvio, Medtronic and The Medicines Company and speaker fees from Boehringer Ingelheim, Abbott, AstraZeneca, Eli Lilly/Daiichi-Sankyo, Merck/Correvio, Medtronic, The Medicines Company, Pfizer and SGM reports receiving research grants to the Institution or consulting/lecture fees from Acuitude, ADIR, Amgen, AstraZeneca, Bayer, Berlin Chimie AG, Boehringer Ingelheim, Bristol-Myers Squibb, Brigham Women’s Hospital, Cardiovascular Research Foundation, Celladon, CME resources, Daiichi-Sankyo, Eli Lilly, Europa, Fédération Française de Cardiologie, Gilead, Hopitaux Universitaires Genève, ICAN, Janssen-Cilag, Lead-Up, Medcon International, Menarini, Medtronic, MSD, Pfizer, Recor, Sanofi-Aventis, Stentys, The Medicines Company, TIMI Study Group, Universitat Basel, WebMD and Zoll Medical. ES reports receiving lecture fees from AstraZeneca.
Patient consent: Obtained.
Ethics approval: The trial design and protocol were approved by the national regulatory authorities in all the participating countries and by the local ethics committee or institutional review board at each participating site. All patients provided written informed consent.
Provenance and peer review: Not commissioned; externally peer reviewed.
Data sharing statement: No additional data are available.
References
- 1. Bairey Merz CN, Shaw LJ, Reis SE, et al. . Insights from the NHLBI-Sponsored Women’s Ischemia Syndrome Evaluation (WISE) Study: Part II: gender differences in presentation, diagnosis, and outcome with regard to gender-based pathophysiology of atherosclerosis and macrovascular and microvascular coronary disease. J Am Coll Cardiol 2006;47(3 Suppl):S21–9. 10.1016/j.jacc.2004.12.084 [DOI] [PubMed] [Google Scholar]
- 2. Mehta RH, Stebbins AS, Lopes RD, et al. . Comparison of incidence of bleeding and mortality of men versus women with ST-elevation myocardial infarction treated with fibrinolysis. Am J Cardiol 2012;109:320–6. 10.1016/j.amjcard.2011.09.012 [DOI] [PubMed] [Google Scholar]
- 3. Kytö V, Sipilä J, Rautava P. Gender and in-hospital mortality of ST-segment elevation myocardial infarction (from a multihospital nationwide registry study of 31,689 patients). Am J Cardiol 2015;115:303–6. 10.1016/j.amjcard.2014.11.001 [DOI] [PubMed] [Google Scholar]
- 4. Jakobsen L, Niemann T, Thorsgaard N, et al. . Sex- and age-related differences in clinical outcome after primary percutaneous coronary intervention. EuroIntervention 2012;8:904–11. 10.4244/EIJV8I8A139 [DOI] [PubMed] [Google Scholar]
- 5. Kang SH, Suh JW, Yoon CH, et al. . Sex differences in management and mortality of patients with ST-elevation myocardial infarction (from the korean acute myocardial Infarction National Registry). Am J Cardiol 2012;109:787–93. 10.1016/j.amjcard.2011.11.006 [DOI] [PubMed] [Google Scholar]
- 6. Lawesson SS, Alfredsson J, Fredrikson M, et al. . A gender perspective on short- and long term mortality in ST-elevation myocardial infarction--a report from the SWEDEHEART register. Int J Cardiol 2013;168:1041–7. 10.1016/j.ijcard.2012.10.028 [DOI] [PubMed] [Google Scholar]
- 7. de Boer SP, Roos-Hesselink JW, van Leeuwen MA, et al. . Excess mortality in women compared to men after PCI in STEMI: an analysis of 11,931 patients during 2000-2009. Int J Cardiol 2014;176:456–63. 10.1016/j.ijcard.2014.07.091 [DOI] [PubMed] [Google Scholar]
- 8. Leurent G, Garlantézec R, Auffret V, et al. . Gender differences in presentation, management and inhospital outcome in patients with ST-segment elevation myocardial infarction: data from 5000 patients included in the ORBI prospective french regional registry. Arch Cardiovasc Dis 2014;107:291–8. 10.1016/j.acvd.2014.04.005 [DOI] [PubMed] [Google Scholar]
- 9. Lawesson SS, Alfredsson J, Fredrikson M, et al. . Time trends in STEMI--improved treatment and outcome but still a gender gap: a prospective observational cohort study from the SWEDEHEART register. BMJ Open 2012;2:e000726 10.1136/bmjopen-2011-000726 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10. Pilgrim T, Heg D, Tal K, et al. . Age- and Gender-related disparities in primary percutaneous coronary interventions for acute ST-segment elevation myocardial infarction. PLoS One 2015;10:e0137047 10.1371/journal.pone.0137047 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11. Lansky AJ, Pietras C, Costa RA, et al. . Gender differences in outcomes after primary angioplasty versus primary stenting with and without abciximab for acute myocardial infarction: results of the Controlled Abciximab and Device Investigation to Lower Late Angioplasty complications (CADILLAC) trial. Circulation 2005;111:1611–8. 10.1161/01.CIR.0000160362.55803.40 [DOI] [PubMed] [Google Scholar]
- 12. Motovska Z, Widimsky P, Aschermann M. The impact of gender on outcomes of patients with ST elevation myocardial infarction transported for percutaneous coronary intervention: analysis of the PRAGUE-1 and 2 studies. Heart 2008;94:e5 10.1136/hrt.2006.110866 [DOI] [PubMed] [Google Scholar]
- 13. Montalescot G, van ’t Hof AW, Lapostolle F, et al. . Prehospital ticagrelor in ST-segment elevation myocardial infarction. N Engl J Med 2014;371:1016–27. 10.1056/NEJMoa1407024 [DOI] [PubMed] [Google Scholar]
- 14. Montalescot G, Lassen JF, Hamm CW, et al. . Ambulance or in-catheterization laboratory administration of ticagrelor for primary percutaneous coronary intervention for ST-segment elevation myocardial infarction: rationale and design of the randomized, double-blind administration of Ticagrelor in the cath lab or in the Ambulance for New ST elevation myocardial infarction to open the coronary artery (ATLANTIC) study. Am Heart J 2013;165:515–22. 10.1016/j.ahj.2012.12.015 [DOI] [PubMed] [Google Scholar]
- 15. Manoukian SV, Feit F, Mehran R, et al. . Impact of major bleeding on 30-day mortality and clinical outcomes in patients with acute coronary syndromes: an analysis from the ACUITY trial. J Am Coll Cardiol 2007;49:1362–8. 10.1016/j.jacc.2007.02.027 [DOI] [PubMed] [Google Scholar]
- 16. Wijnbergen I, Tijssen J, van ’t Veer M, et al. . Gender differences in long-term outcome after primary percutaneous intervention for ST-segment elevation myocardial infarction. Catheter Cardiovasc Interv 2013;82:379–84. 10.1002/ccd.24800 [DOI] [PubMed] [Google Scholar]
- 17. Champney KP, Frederick PD, Bueno H, et al. . The joint contribution of sex, age and type of myocardial infarction on hospital mortality following acute myocardial infarction. Heart 2009;95:895–9. 10.1136/hrt.2008.155804 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18. Jneid H, Fonarow GC, Cannon CP, et al. . Sex differences in medical care and early death after acute myocardial infarction. Circulation 2008;118:2803–10. 10.1161/CIRCULATIONAHA.108.789800 [DOI] [PubMed] [Google Scholar]
- 19. Jackson EA, Moscucci M, Smith DE, et al. . The association of sex with outcomes among patients undergoing primary percutaneous coronary intervention for ST elevation myocardial infarction in the contemporary era: insights from the Blue Cross Blue Shield of Michigan Cardiovascular Consortium (BMC2). Am Heart J 2011;161:106–12. 10.1016/j.ahj.2010.09.030 [DOI] [PubMed] [Google Scholar]
- 20. Suessenbacher A, Doerler J, Alber H, et al. . Gender-related outcome following percutaneous coronary intervention for ST-elevation myocardial infarction: data from the austrian acute PCI registry. EuroIntervention 2008;4:271–6. 10.4244/EIJV4I2A47 [DOI] [PubMed] [Google Scholar]
- 21. Husted S, James SK, Bach RG, et al. . The efficacy of ticagrelor is maintained in women with acute coronary syndromes participating in the prospective, randomized, PLATelet inhibition and patient outcomes (PLATO) trial. Eur Heart J 2014;35:1541–50. 10.1093/eurheartj/ehu075 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22. De Luca G, Gibson CM, Gyöngyösi M, et al. . Gender-related differences in outcome after ST-segment elevation myocardial infarction treated by primary angioplasty and glycoprotein IIb-IIIa inhibitors: insights from the EGYPT cooperation. J Thromb Thrombolysis 2010;30:342–6. 10.1007/s11239-010-0451-y [DOI] [PubMed] [Google Scholar]
- 23. Benamer H, Tafflet M, Bataille S, et al. . Female gender is an independent predictor of in-hospital mortality after STEMI in the era of primary PCI: insights from the greater Paris area PCI registry. EuroIntervention 2011;6:1073–9. 10.4244/EIJV6I9A187 [DOI] [PubMed] [Google Scholar]
- 24. Pancholy SB, Shantha GP, Patel T, et al. . Sex differences in short-term and long-term all-cause mortality among patients with ST-segment elevation myocardial infarction treated by primary percutaneous intervention: a meta-analysis. JAMA Intern Med 2014;174:1822–30. 10.1001/jamainternmed.2014.4762 [DOI] [PubMed] [Google Scholar]
- 25. Peterson ED, Lansky AJ, Kramer J, et al. . Effect of gender on the outcomes of contemporary percutaneous coronary intervention. Am J Cardiol 2001;88:359–64. 10.1016/S0002-9149(01)01679-4 [DOI] [PubMed] [Google Scholar]
- 26. Sederholm Lawesson S, Tödt T, Alfredsson J, et al. . Gender difference in prevalence and prognostic impact of renal insufficiency in patients with ST-elevation myocardial infarction treated with primary percutaneous coronary intervention. Heart 2011;97:308–14. 10.1136/hrt.2010.194282 [DOI] [PubMed] [Google Scholar]
- 27. Berger JS, Elliott L, Gallup D, et al. . Sex differences in mortality following acute coronary syndromes. JAMA 2009;302:874–82. 10.1001/jama.2009.1227 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28. Steg PG, Huber K, Andreotti F, et al. . Bleeding in acute coronary syndromes and percutaneous coronary interventions: position paper by the Working Group on Thrombosis of the european Society of Cardiology. Eur Heart J 2011;32:1854–64. 10.1093/eurheartj/ehr204 [DOI] [PubMed] [Google Scholar]
- 29. Mehran R, Pocock SJ, Nikolsky E, et al. . A risk score to predict bleeding in patients with acute coronary syndromes. J Am Coll Cardiol 2010;55:2556–66. 10.1016/j.jacc.2009.09.076 [DOI] [PubMed] [Google Scholar]
- 30. Becker RC, Bassand JP, Budaj A, et al. . Bleeding complications with the P2Y12 receptor antagonists clopidogrel and ticagrelor in the PLATelet inhibition and patient outcomes (PLATO) trial. Eur Heart J 2011;32:2933–44. 10.1093/eurheartj/ehr422 [DOI] [PubMed] [Google Scholar]
- 31. Mathews R, Peterson ED, Chen AY, et al. . In-hospital major bleeding during ST-elevation and non-ST-elevation myocardial infarction care: derivation and validation of a model from the ACTION Registry®-GWTG™. Am J Cardiol 2011;107:1136–43. 10.1016/j.amjcard.2010.12.009 [DOI] [PubMed] [Google Scholar]
- 32. Ahmed B, Piper WD, Malenka D, et al. . Significantly improved vascular complications among women undergoing percutaneous coronary intervention: a report from the Northern New England Percutaneous Coronary intervention registry. Circ Cardiovasc Interv 2009;2:423–9. 10.1161/CIRCINTERVENTIONS.109.860494 [DOI] [PubMed] [Google Scholar]
- 33. Cho L, Topol EJ, Balog C, et al. . Clinical benefit of glycoprotein IIb/IIIa blockade with Abciximab is independent of gender: pooled analysis from EPIC, EPILOG and EPISTENT trials. Evaluation of 7E3 for the Prevention of ischemic complications. Evaluation in percutaneous transluminal coronary angioplasty to improve Long-Term Outcome with Abciximab GP IIb/IIIa blockade. evaluation of platelet IIb/IIIa inhibitor for stent. J Am Coll Cardiol 2000;36:381–6. [DOI] [PubMed] [Google Scholar]
- 34. Vlaar PJ, Svilaas T, van der Horst IC, et al. . Cardiac death and reinfarction after 1 year in the Thrombus aspiration during percutaneous coronary intervention in acute myocardial infarction study (TAPAS): a 1-year follow-up study. Lancet 2008;371:1915–20. 10.1016/S0140-6736(08)60833-8 [DOI] [PubMed] [Google Scholar]
- 35. De Luca G, Suryapranata H, Ottervanger JP, et al. . Time delay to treatment and mortality in primary angioplasty for acute myocardial infarction: every minute of delay counts. Circulation 2004;109:1223–5. 10.1161/01.CIR.0000121424.76486.20 [DOI] [PubMed] [Google Scholar]
- 36. Sadowski M, Gasior M, Gierlotka M, et al. . Gender-related differences in mortality after ST-segment elevation myocardial infarction: a large multicentre national registry. EuroIntervention 2011;6:1068–72. 10.4244/EIJV6I9A186 [DOI] [PubMed] [Google Scholar]
- 37. Otten AM, Maas AH, Ottervanger JP, et al. . Is the difference in outcome between men and women treated by primary percutaneous coronary intervention age dependent? gender difference in STEMI stratified on age. Eur Heart J Acute Cardiovasc Care 2013;2:334–41. 10.1177/2048872612475270 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38. Wessler JD, Stant J, Duru S, et al. . Updates to the ACCF/AHA and ESC STEMI and NSTEMI guidelines: putting guidelines into clinical practice. Am J Cardiol 2015;115(5 Suppl):23A–8. 10.1016/j.amjcard.2015.01.004 [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
bmjopen-2016-015241supp001.pdf (247.1KB, pdf)