

Abstract
Background
Survival after sudden cardiac arrest (SCA) remains low and tools for improved prediction of individuals at long-term risk for SCA are still awaited. Alternative short-term approaches aimed at pre-emptive risk stratification and prevention are needed.
Objective
To assess characteristics of symptoms in the four weeks prior to SCA, and whether the response to these symptoms may be associated with a better outcome.
Design
Ongoing prospective population-based study.
Setting
Population of approximately one million in the Northwestern US (2002–2012).
Patients
Middle-aged residents (35–65 years) suffering from SCA.
Measurement
Multiple sources assessment of symptoms in the four weeks preceding SCA and association with survival to hospital discharge.
Results
Of 839 SCA patients with comprehensive assessment of symptoms (51±12 years, 75% male), 430 patients (51%; 50% male vs. 53% female, P=0.59) experienced warning symptoms, mainly chest pain and dyspnea. In the majority of symptomatic patients (93%), symptoms recurred during the 24 hours preceding SCA. Only 81 patients (19%) called emergency medical services (911) to report symptoms prior to SCA; these were more likely to be patients with a history of heart disease (P<0.001) and/or continuous chest pain (P<0.001). Survival when 911 was called in response to symptoms was 32.1% (95%CI 21.8–42.4), compared to 6.0% (95%CI 3.5–8.5) in those who did not call (P<0.001). This association remained after considering potential confounders.
Limitations
Potential for recall and response bias; symptom assessment not available in 24% patients; missing data for some patients and SCA characteristics.
Conclusions
Warning symptoms are frequent prior to SCA but the vast majority of these are not acted upon. Emergent medical care was associated with survival in patients with symptoms, emphasizing a potential role for future approaches that enable short-term prevention of SCA.
Primary Funding Source
NHLBI.
Keywords: Sudden Death, Symptoms, Healthcare, Emergency Medical Services, Public Health, Epidemiology, Prevention
Introduction
Sudden cardiac arrest (SCA) is commonly perceived by the lay and medical communities as a sudden unexpected collapse, without warning. With more than 550,000 individuals of SCA occurring pre-hospital and in-hospital annually in the United States, SCA accounts for over half of cardiovascular mortality, and is a major public health issue.(1, 2)
Survival after SCA remains very low and stable (approximately 7%), despite major investments by the medical and research communities in this area over the past decades.(3) Furthermore, efforts to improve prediction of individuals at long-term risk for SCA are still awaited and in this context, alternative approaches aimed at pre-emptive risk stratification and prevention are needed.(1, 4, 5) Sentinel events preceding SCA may be of special interest, in light of recent advances in communication and remote transmission technologies.(6) (7) We hypothesized that “warning events” in the hours, days and weeks prior to SCA might identify a subgroup of SCA patients in whom timely and early intervention could impact outcome.
Investigation of SCA remains particularly challenging, especially since a great majority of patients die in the field, and consequently the information collected by Emergency Medical Services (EMS) is often restricted to data regarding the resuscitation process. Details of the past medical history of SCA patients (especially those who cannot be resuscitated) are thus usually sparse and very rarely considered systematically. In the Oregon-SUDS, we collected information on symptoms as well as clinical history for all SCA patients including those who died before reaching hospital.
We therefore conducted a comprehensive assessment of warning symptoms in the four weeks prior to SCA in a large prospective community based study of deceased and surviving SCA patients in the Portland, Oregon metropolitan area. We hypothesized that presence and response to warning symptoms may be associated with a better survival from SCA.
Methods
Setting, Definitions and Survey Methods
The Oregon Sudden Unexpected Death Study (Oregon-SUDS) is an ongoing community based prospective study of out of hospital SCA. Detailed methods have been published previously.(8–11) Briefly, since February 1, 2002,of SCA in the Portland Oregon metropolitan area were identified using multiple sources that included a two-tiered emergency medical response system, the medical examiner’s office and emergency departments of all local hospitals. This study was approved by the relevant Institutional Review Boards including Cedars-Sinai Medical Center, Los Angeles CA and Oregon Health and Science University, Portland, OR.
Sudden cardiac arrest was defined as an unexpected loss of the pulse without obvious extra-cardiac cause, occurring with a rapid collapse and with specific resuscitation records available. SCAs occurring in the setting of a prior terminal condition, such as malignancy not in remission or end-stage chronic obstructive lung disease, were excluded. At the time of adjudication, three physicians had access to lifetime medical history with all available hospital and outpatient medical records, including information on prior symptoms.
Variables considered in the present analysis included demographics, circumstances of occurrence as well as resuscitation data according to the revised Utstein style.(12) In addition to the data from EMS and the medical examiner, a working group of the Oregon-SUDS collected and assessed the lifetime past medical history for both deceased patients and survivors, including symptoms assessment prior to SCA, through review of records of all inpatient/outpatient visits from the Portland area hospitals. The principal outcome was survival to hospital discharge, available in all cases.
Assessment of Symptoms Prior to SCA
Characterization of symptoms and their frequency was performed during the four weeks prior to SCA, among patients aged 35–65 years, adjudicated from February 2002 to February 2012. The data on symptoms was collected by the Oregon-SUDS investigators based on information documented by the EMS team (in the field), intensivists or cardiologists (at the 16 hospitals), and physicians (in the community). Symptom assessment recorded on the EMS pre-hospital care report was derived from multiple sources, including information provided by family at the scene, witnesses, and survivors of SCA. In addition, available hospital and outpatient medical records for all patients were systematically analyzed for information regarding symptoms.
Symptoms were categorized as absent, present or not evaluable based on the extent of information available, and the agreement of investigators. Symptoms were considered “absent” when (i) there was no record of any medical consultation during the four weeks preceding SCA, (ii) at least one of the other sources specifically ascertained the absence of any complaints, and (iii) none of the other sources reported any symptoms. Symptoms were considered as “present” if they were documented by at least one of the above sources. Of note, symptoms starting immediately prior to the SCA event (symptoms with instantaneous collapse) were considered as “no symptoms” since they would have been unlikely to lead to any early intervention.
Symptoms were classified as (i) chest pain (sub-classified as typical and atypical), (ii) dyspnea, (iii) palpitations, (iv) syncope, and (v) other (including abdominal pain, nausea/vomiting, back pain and other miscellaneous symptoms). Finally, the presence of ongoing typical influenza-like symptoms was also evaluated. In cases of multiple symptoms (combined symptoms), chest pain was designated as the principal symptom when present. Time intervals from the onset of a symptom to SCA were categorized into four groups, where possible (98%): (i) within the first hour, (ii) within the hours before SCA (up to 24 hours), (iii) within the days before SCA (up to seven days), and (iv) within the weeks (up to four weeks) before SCA.
Symptoms were considered as not acted upon if patients or relatives/witnesses did not attempt to contact EMS (911) in response to symptoms that occurred prior to SCA.
Statistical Analysis
This report was prepared in compliance with the STROBE checklist for observational studies.(13,14) The characteristics of SCA were reported as mean (standard deviation), proportions, median and interquartile ranges, as appropriate. Comparisons between groups used the chi-square test for categorical variables and the Student t test for continuous variables. A logistic regression model was used to compare survival to hospital discharge by 911 call in those with symptoms. Covariates included age and sex, and meaningful independent variables according to Utstein guidelines(12). Missing values for covariates were accounted for using multiple imputations (mi impute) by chained equations. Imputation models included terms for age, gender, location, witnessed-CPR status, initial rhythm, timing, onset, diabetes, dyslipidemia, BMI, hypertension, current smoking, coronary artery disease, time to intervention, in addition to the outcome. We used ten imputations and Rubin’s rules to combine the results.(15,16) The results were similar to those from a complete cases analysis and so only results using multiply imputed data are presented as primary results. Sensitivity analyses were performed to assess the relationship between survival and 911 call, with additional adjustment for possible confounding due to hospital or time period (before and after 2005). Differences were assumed to be statistically significant for a two-tailed probability of P≤0.05. Ninety-five percent confidence intervals (CI) were calculated when appropriate. All data were analyzed using STATA software version v11.0 (Lakeway Drive, TX).
Role of Funding Sources
The funding source of the study had no role in the design, conduct, and analysis of this study and in the decision to submit the manuscript for publication.
Results
Frequency of Warning Signs and Associated Characteristics
Sixteen hospitals in the Portland metropolitan area were included, with the median number of patients per hospital of 71 (Q1:56 Q3:81). Overall, symptom data were not available for analysis in 260 (24%) patients, due to insufficient or conflicting documentation (Figure 1, Appendix 1). Reasons for not having symptom data included: (i) Absence of witness and relatives prior and at the time of SCA, as well as no medical report recorded in the area during the previous 4 weeks (166 patients), (ii) Witnesses/relatives unable to provide clear information in the absence of a specific medical record (69 patients), (iii) Information on symptoms provided by patients/witnesses/relatives considered as being too non-specific to make definite conclusions (23 patients), and finally (iv) Brain injury with significant cognitive dysfunction (2). Patients without symptom assessment were more likely to not have a witness (65.4% vs. 43.3%) (Appendix 2). The most common source for symptom information was the Oregon Emergency Medical Services, in 766 patients (91%) overall (Appendix 1), especially trained to get important information in the field.
Figure 1.
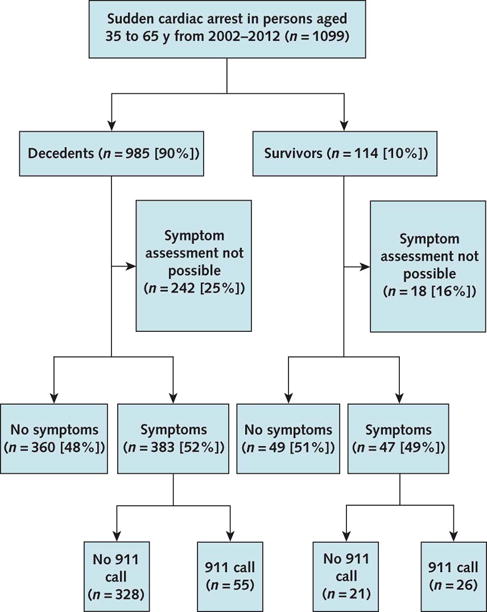
Flow Chart.
Of the 839 patients with symptoms assessment, 430 patients (51%) presented with at least one symptom within the four weeks prior to SCA (Figure 1), with very similar frequency in men and women (50 vs. 53%, P=0.59). A total of 51 patients (out of the 430 with symptoms) had consulted a family or specialist physician during the 4 preceding weeks.
Subject characteristics according to the presence or absence of warning symptoms are described in Table 1. Overall, characteristics of patients with and without symptoms prior to SCA were similar, including past medical history. Regarding circumstances of occurrence, patients with symptoms (vs. no symptoms) were more likely to be at home at the time of SCA (76 vs. 64%, P<0.001). Response times (between 911 call and EMS arrival) were similar in both groups (6.9±4.1 vs. 7.0±3.2 minutes, P=0.73), without a significant difference in the proportion with initial shockable rhythm (49 vs. 52%, P=0.40).
Table 1.
Characteristics of Sudden Cardiac Arrest Cases Based on Presence or Absence of Symptoms Prior to the Event.
| Absence of Symptoms N=409 |
Presence of Symptoms N=430 |
P value | |
|---|---|---|---|
| Demographic Data | |||
| Age — yr | |||
| Mean (SD) | 52.5 (8) | 52.6 (8) | 0.84 |
| Male Sex — no. (%) | 298 (76.0) | 320 (74.4) | 0.59 |
| Timing — no. (%) | 0.12* | ||
| Night (midnight to 6 am) | 21 (11.2) | 40 (17.2) | |
| Morning (6:00 am to 12:00 pm) | 52 (27.8) | 71 (30.4) | |
| Afternoon (12:00 pm to 6:00 pm) | 57 (30.5) | 62 (26.6) | |
| Evening (6:00 pm to midnight) | 57 (30.5) | 60 (25.8) | |
| Missing | 222 | 197 | |
| Type of Symptoms — no. (%) | |||
| Chest pain | 199 (46.3) | ||
| Dyspnea | 78 (18.1) | ||
| Syncope/palpitation | 22 (5.6) | ||
| Others | 127 (29.5) | ||
| Missing | 4 | ||
| ≥2 Known Cardiovascular Risk Factors no. (%) | 209 (51.4) | 224 (52.3) | 0.78 |
| Diabetes mellitus — no. (%) | 108 (27.5) | 95 (23) | 0.17* |
| Missing | 16 | 16 | |
| Dyslipidemia — no. (%) | 115 (29.3) | 117 (28.3) | 0.75* |
| Missing | 16 | 16 | |
| Systemic hypertension — no. (%) | 192 (48.9) | 196 (47.3) | 0.72* |
| Missing | 16 | 16 | |
| Body mass index — Mean (SD) | 31.2 (8) | 31.7 (9) | 0.69* |
| Missing | 105 | 105 | |
| Current smoking — no. (%) | 148 (53.6) | 204 (64.1) | 0.01* |
| Missing | 133 | 112 | |
| Known Heart Disease — no. (%) | 142 (34.7) | 159 (37.0) | 0.50 |
| Coronary artery disease no. (%) | 82 (29.4) | 105 (24.4) | 0.31 |
| Heart failure no. (%) | 61 (21.9) | 63 (19.9) | 0.56 |
| Atrial fibrillation no. (%) | 36 (12.9) | 32 (10.2) | 0.29 |
| Pacemaker no. (%) | 6 (2.1) | 2 (0.7) | 0.11 |
| ≥2 Known Cardiovascular Risk Factors and/or Heart Disease — | 246 (60.2) | 280 (65.1) | 0.14 |
| Coronary Artery Disease-related SCA* — no. (%) | 218 (79.3) | 240 (84.2) | 0.16* |
| Missing | 145 | 134 |
p-value obtained by using multiple imputation to account for missing data
SCA denotes Sudden Cardiac Arrest, SD, Standard Deviation.
Percentages were calculated on the basis of the total number of known events.
Characteristics of Symptoms and Temporal Pattern
The onset of cardiovascular symptoms is summarized in Figure 2. In most individuals (334; 80%), symptoms started more than one hour before SCA, including 147 with onset of symptoms more than 24 hours prior to SCA. Among those, 136 (93%) experienced recurrent new episodes of symptoms during the 24 hours preceding SCA.
Figure 2. Warning symptoms (chest pain, dyspnea, syncope/palpitations) among sudden cardiac arrest patients based on time period between onset of symptoms and occurrence of the event.

Of note, overall we were able to estimate onset of symptoms in 267 patients out of 299 of patients with chest pain, dyspnea, or syncope/palpitations.
Error bars correspond to 95% confidence intervals
The main symptom was chest pain, documented in 199 (46%) patients with symptoms, including intermittent typical angina in 151 (76%) of these. Coronary heart disease was previously identified in 28% of those patients with chest pain. Dyspnea was present in 78 patients (18%). Of these, congestive heart failure or pulmonary conditions were previously known in 32%. Syncope or palpitations were found in 22 patients (5%) with the first episode homogeneously distributed during the four-week period. In 86 patients (20%), symptomatology was related to abdominal or other complaints. Finally, typical ongoing influenza-like symptoms were observed in 41 patients (10%). A significant overlap of symptoms was observed, notably chest pain and dyspnea; 65 patients (33%) with chest pain developed concomitant acute dyspnea prior to SCA occurrence. Among patients without chest pain, none presented with more than one symptom.
The pattern of symptoms was significantly different between men and women (Table 2), with men experiencing more chest pain than women, whereas women experienced more dyspnea (P<0.001). When the analysis was restricted to cases of SCA with documented coronary artery disease, women still presented with a lower frequency of chest pain (32 vs. 58%, P=0.001).
Table 2.
Warning symptoms among sudden cardiac arrests based on sex.
| Men N=320 |
Women N=110 |
Total | |
|---|---|---|---|
| Chest Pain | 173 (54) | 26 (24) | 199 |
| Dyspnea | 45 (14) | 33 (31) | 78 |
| Syncope/Palpitation | 14 (4) | 8 (7) | 22 |
| Others | 58 (18) | 28 (25) | 86 |
| Flu-like symptoms | 28 (9) | 13 (12) | 41 |
Missing Data (specific type of symptoms not assessable) in 4 patients, 2 among men and 2 among women).
Response to Symptoms and Relationship with Survival Outcome
Overall, among the 430 patients with preceding symptoms, 81 (19%) called EMS prior to SCA (Figure 1). Characteristics of patients based on their decision to call 911 are summarized in Table 3. Previous history of heart disease (P=0.001) and older age (P=0.021) were associated with 911 calls. Symptoms suggestive of cardiovascular conditions were more likely to be associated with 911 calls, especially continuous chest pain compared to all other symptoms (69 vs. 15%, P<0.001).
Table 3.
Characteristics and circumstances of sudden cardiac arrest based on whether or not 911 call was made in response to symptoms.
| Call N=81 |
No Call N=349 |
P Value | |
|---|---|---|---|
| Study Periods | 0.41 | ||
| 2002–2005 | 52 (64.2) | 198 (56.7) | |
| 2006–2009 | 18 (22.2) | 103 (29.5) | |
| 2010–2012 | 11 (13.6) | 48 (13.8) | |
| Demographic Data | |||
| Age — yr | |||
| Mean (SD) | 54.2 (7) | 52.2 (8) | 0.02 |
| Sex | 0.84 | ||
| Male — no. (%) | 61 (75.3) | 259 (74.2) | |
| Timing — no. (%) | 0.90* | ||
| Night (midnight to 6:00 am) | 11 (17.7) | 29 (17.0) | |
| Morning (6:00 am to 12:00 pm) | 16 (25.8) | 55 (32.1) | |
| Afternoon (12:00 pm to 6:00 pm) | 20 (32.3) | 42 (24.6) | |
| Evening (6:00 pm to midnight) | 15 (24.2) | 45 (26.3) | |
| Missing | 19 | 178 | |
| Known Heart Disease — no. (%) | 45 (55.6) | 114 (32.7) | <0.001 |
| Coronary artery disease | 28 (34.8) | 77 (22.1) | 0.01 |
| Type of Symptoms — no. (%) | <0.001 | ||
| Chest pain | 45 (55.6) | 154 (44.1) | |
| Dyspnea | 23 (28.4) | 55 (15.8) | |
| Syncope/palpitation | 6 (7.4) | 16 (7.4) | |
| Others | 7 (8.6) | 120 (34.4) | |
| Missing | 0 | 4 | |
| Onset of Symptoms — no. (%) | 0.56* | ||
| ≤one hour | 21 (28.8) | 57 (17.9) | |
| ≤one day | 32 (43.8) | 142 (44.5) | |
| ≤one week | 17 (23.3) | 108 (33.8) | |
| ≤one month | 3 (4.1) | 12 (3.8) | |
| Missing | 8 | 30 | |
| Home Occurrence — no. (%) | 49 (60.5) | 278 (79.7) | <0.001* |
| Missing | 0 | 2 | |
| Witnessed status— no. (%) | 74 (91.4) | 182 (52.6) | <0.001* |
| No witness | 7 (8.6) | 164 (47.4) | |
| Witnessed without CPR | 43 (53.1) | 135 (39) | |
| Witnessed with CPR | 31 (38.3) | 47 (13.6) | |
| Missing | 0 | 3 | |
| Time to Intervention | |||
| Call-to-EMS Arrival — Mean (SD), Min | 6.9 (4) | 7.0 (3) | 0.67* |
| Missing data | 16 | 133 | |
| Rhythm — no. (%) | 0.02* | ||
| Ventricular fibrillation/tachycardia | 42 (58.4) | 112 (45.7) | |
| Electromechanical dissociation | 25 (34.7) | 60 (24.5) | |
| Asystole | 5 (6.9) | 73 (29.8) | |
| Missing data | 10 | 103 |
p-value obtained by using multiple imputation to account for missing data
CPR denotes Cardiopulmonary Resuscitation, EMS, Emergency Medical Services, SCA, Sudden Cardiac Arrest, SD, Standard Deviation.
Percentages were calculated on the basis of the total number of known events.
Among the 81 patients with symptoms who called 911, 63 (78%) developed SCA before arrival of emergency medical responders, whereas 18 (22%) experienced SCA in the ambulance on the way to hospital. Overall, compared to patients who did not call 911 prior to SCA, patients who did call were more frequently witnessed (P=0.001), had a higher proportion of bystander cardiopulmonary resuscitation (P=0.001), and presented with a higher rate of initially shockable rhythm (P=0.02).
Survival to hospital discharge was 32.1% (95%CI 21.8–42.4), compared to 6.0% (95% CI 3.5–8.5) in those who did not call 911 (P<0.001). After adjustment for differences in patients and resuscitation variables, and multiple imputation for missing data, 911 call remained significantly associated with survival to hospital discharge (OR 4.82, 95%CI 2.23–10.43, P<0.001) (Appendix 3). A sensitivity analysis using complete case analysis found a significant association (OR 3.27, 95%CI 1.37–7.79, P=0.008) as did analyses that controlled for potential confounding due to hospital (OR 3.35, 95%CI 1.47–7.65, P=0.004) and the periods of time prior to and after year 2005 (OR 5.64, 95%CI 2.59–12.43, P=0.001).
Discussion
To the best of our knowledge, this study is the first comprehensive evaluation of the extent to which a patient’s or their family’s response to symptoms in the four weeks preceding SCA, is associated with survival. Several key points emerge from this study. Firstly, there is a relatively high frequency of warning signs preceding SCA in middle age, when evaluation is extended to the four weeks preceding SCA. Second, these symptoms appear to be frequently ignored or minimized by patients in the community, with at least two-thirds of affected individuals not seeking urgent medical care, given that the vast majority of symptoms reoccurred during the 24 hour time period preceding SCA. Finally, our findings suggest that an early 911 call among patients with symptoms is associated with better survival, especially since in the majority of patients symptoms recurred in the hours immediately preceding SCA. These findings suggest that there may be potential for enhancing short-term prevention of SCA in the future.
The term “sudden” has classically suggested that collapse occurred without warning. Although previous community-based studies that investigated the circumstances preceding SCA have documented the existence of early warning symptoms in some patients,(17,18) these studies were mainly focused on symptoms occurring very shortly before witnessed SCA; and findings were limited to those collected in the field by EMS providers, and finally likely to underestimate the potential window for timely intervention. It is noteworthy that the vast majority of our patients with symptoms who eventually developed SCA, did not call for emergent care. This is a particularly striking finding when you consider the fact that the majority (>90%) of those who first experienced symptoms during the days and weeks before SCA, experienced recurrent symptoms during the hours preceding the event. Not surprisingly, patients with continuous symptoms or with known heart disease appear more likely to call 911, probably because of a better awareness of warning signs. However, two thirds of such patients did not call 911, identifying major room for improvement.(19)
Our findings emphasize the need to encourage efforts that target public awareness of SCA as a largely fatal event. It is important to reinforce knowledge of prodromal symptoms of SCA in the general public as well as patients affected by heart disease and their family members. The recent impressive advances in mobile telecommunication technologies leave open the possibility that these developments could help improve management of SCA patients with warning symptoms, potentially affording a unique opportunity for early intervention.(6) This may be particularly helpful in the subgroup of patients with known heart disease. It is conceivable that in this patient sub-group instant transmission of point-of-care ECGs and development of automated algorithms could enable comparison with baseline recordings stored in the mobile device.(6,7) Also, immediate geo-localization and identifying the location of the closest automatic external defibrillator are all technically feasible and potentially could be beneficial in this setting. Thus, targeted public education to enhance timely reporting of symptoms combined with development of systematic strategies for response to these symptoms, may lead to new paradigms for short-term prevention of SCA. Our results also demonstrate that 12% of patients had consulted a physician within the 30 days prior SCA, and were investigated with a systematic work-up. These results also point out the intrinsic difficulty in estimating risk of SCA even in symptomatic patients, and should motivate more focused investigation in this area.
In contrast with what has been previously suggested for women,(20,21) a significant proportion of women in our series also had cardiac symptoms in the weeks prior to SCA. The overall frequency of symptoms was similar between men and women, challenging to some extent the traditional concept that SCA may be more difficult to predict or prevent in women. The pattern of symptoms, however, differed significantly, with less chest pain among women, even when our analysis was restricted to cases with definite coronary artery disease. Those results appear consistent with recent findings regarding sex differences in sentinel symptoms prior to myocardial infarction.(22–24)
While the concept that an early call to EMS improves survival seems intuitive, our findings emphasize that patients who called 911 prior to SCA more frequently had a witnessed arrest (22% in front of EMS), had a higher rate of cardiopulmonary resuscitation and higher propensity for presenting with a shockable rhythm. All these factors have been associated with better survival.(3) The fact that early 911 call remains associated with better survival after multiple adjustments on patients’ characteristics as well as circumstances of SCA, points to the need to further investigate the mechanisms of this association.
The findings of pre-existing symptoms correlating with higher chance of presenting with shockable rhythms (ventricular fibrillation/tachycardia, as opposed to PEA or asystole) are of interest and are likely explained by three factors. Published studies suggest that the patterns of prodromal symptoms we observed prior to sudden death (out-of-hospital) were overall similar to symptoms observed prior to non-fatal myocardial infarction,(25)suggesting a high proportion of coronary ischemia patients. We and others have previously reported a higher likelihood of shockable rhythms in patients with coronary disease.(26) Finally, the higher frequency of witnessed events and bystander CPR especially in the 911 call group is also likely to have contributed to the higher prevalence of shockable rhythms in patients with pre-existing symptoms.(27)
Although our results are derived from a unique and comprehensive survey of SCA survivors and decedents, several limitations warrant consideration. First, since symptom ascertainment was not possible for (24%) of our population, there is a potential for bias. In addition, there was missing data for many potential confounders. Multiple imputation methodology was used to handle data that was missing for the covariates Second, because our population is comprised of patients who eventually developed SCA, the benefit of any early symptom alerts on outcomes may be underestimated, since a number of patients with symptoms and timely appropriate medical management may eventually not have developed SCA. Thirdly, we acknowledge that the specificity of identified symptoms, possibly in combination with other factors, to predict imminent SCA needs further evaluation in order to finally improve “short-term” risk stratification. The ultimate goal would be to optimize triage by EMS or other health care providers. In this regard, our preliminary findings suggest that a combination of chest pain and dyspnea may be especially frequent, a finding that appears to be in agreement with previous reports indicating that the development of acute heart failure along with myocardial ischemia increases the risk of ventricular arrhythmias.(28) Fourth, although EMS remain the most important source of information collected on site, and EMS personnel of the Portland area, have been systematically receiving specialized training for information gathering in the specific setting of SCA since the early 90s, we acknowledge that our results with respect to the proportion of patients with symptoms may be subject to some recall as well as response bias. However, the influence of this potential response bias is likely to be low since in the setting of SCA in general but also in this evaluation, the proportion of survivors included in the symptoms assessment evaluation is quite small (5.6% in our study). Further, the influence of symptoms (leading to earlier 911 call) on survival is unlikely to be significantly affected by this bias since information on 911 calls was directly ascertained from the EMS system and did not rely on patient/family recall. Finally, such an observational study cannot establish a causal association, and underlying mechanisms behind this association between early 911 call and survival need further investigation.
In summary, a high proportion of middle-aged men and women in the community had warning symptoms prior to SCA, but the vast majority of these are not acted upon. Because timely response to such symptoms was associated with an increase in survival, our results highlight the potential importance of developing new community-based strategies for short-term prevention of SCA. Further studies are needed to improve risk-stratification among those patients with symptoms, as well as investigations of whether early intervention based on symptoms may improve outcomes or even prevent SCA occurrence.
Acknowledgments
We gratefully acknowledge the assistance of all EMS personnel (American Medical Response, Portland/Gresham fire departments), the Oregon State Medical Examiner’s office and the hospitals in the Portland Oregon metro area. Also, we would like to thank Drs Wulfran Bougouin (Paris Sudden Death Expertise Center, Paris, France) and Prof David S. Celermajer (Sydney Medical School, Sydney, Australia) for their critical review of the manuscript.
Funding: Funded in part by National Heart Lung and Blood Institute R01HL105170 and R01HL122492 to S.S.C. E.M. was a Visiting Faculty Scientist at the Cedars-Sinai Heart Institute funded by research grant support from the Philip Foundation, the Bettencourt Schueller Foundation, the French Society of Cardiology, the Foundation for Medical Research (FRM) and the French National Institute of Health and Medical Research.
Appendix 1. Primary Sources for Sudden Cardiac Arrest Symptom Information
| Patients with one Source: | 602 (72%) |
| EMS | 549 |
| ICU | 39 |
| Cardiology | 8 |
| MD Consult | 6 |
| Patients with two Sources: | 137 (17%) |
| EMS + ICU | 80 |
| EMS+MD Consult | 45 |
| Cardiology+ICU | 12 |
| Patients with more than two Sources: | 92 (11%) |
| EMS + ICU + Cardiology | 92 |
Identification of sources of information was possible in 831 (out of 839).
EMS denotes emergency medical services, ICU intensive care unit
Appendix 2. Patients Characteristics and Circumstances of Sudden Cardiac Arrest by Symptom Assessment
| Patients without symptom assessment N=260 (%) |
Patients with symptom assessment N=839 (%) |
P value | |
|---|---|---|---|
| Demographic Data | |||
| Age — yr | |||
| Mean(SD) | 54.1(7) | 52.6(8) | 0.04 |
| Male Sex — no. | 194 (74.6) | 631 (75.2) | 0.85 |
| Timing — no. | 0.15 | ||
| Night (midnight to 06:00 am) | 14 (14.3) | 61 (14.5) | |
| Morning (6:00 am to 12:00 pm) | 25 (25.5) | 123 (29.3) | |
| Afternoon (12:00 pm to 6:00 pm) | 39 (39.8) | 119 (28.3) | |
| Evening (6:00pm to midnight) | 20 (20.4) | 117 (25.9) | |
| Missing | 162 | 419 | |
| ≥2 Known Cardiovascular Risk Factor | 139 (54.9) | 433 (51.9) | 0.39 |
| Missing | 7 | 4 | |
| Known Heart Disease — no. | 95 (36.5) | 301 (35.9) | 0.85 |
| Coronary artery disease | 53 (20.4) | 198 (23.6) | 0.28 |
| ≥2 Known Cardiovascular Risk Factor and/or Heart Disease — no. | 167 (64.2) | 526 (62.7) | 0.65 |
| Coronary Artery Disease-related SCA* — no. | 111 (79.9) | 458 (80.5) | 0.08 |
| Missing | 121 | 279 | |
| Home Occurrence — no. | 162 (62.8) | 586 (70.2) | 0.03 |
| Missing | 2 | 4 | |
| Witnessed status— | |||
| No witness | 168 (65.4) | 361 (43.3) | <0.001 |
| Witnessed without CPR | 58 (22.6) | 301 (36.1) | |
| Witnessed with CPR | 31(12.1) | 172 (20.6) | |
| Missing | 3 | 5 | |
| Call-to-EMS Arrival — Mean(SD), Min | 6.9(3) | 6.9(4) | 0.80 |
| Missing | 91 | 296 | |
| Rhythm — no. | 0.56 | ||
| Ventricular fibrillation/tachycardia | 78 (44.1) | 312 (50.2) | 0.15 |
| Missing | 83 | 218 |
Appendix 3. Independent factors associated with survival to hospital discharge
| OR | [95%CI] | P Value | |
|---|---|---|---|
| Age (per year increase) | 1.06 | 1.0–1.12 | 0.04 |
| Male gender (per min increase) | 0.31 | 0.14–0.76 | 0.01 |
| Time of intervention | 0.98 | 0.88–1.09 | 0.68 |
| Witnessed status | 1.53 | 0.89–2.63 | 0.12 |
| No witnessed | 1 | ||
| Witnessed | 3.28 | 0.90–11.90 | 0.07 |
| Witnessed and bystander CPR | 4.28 | 1.32–13.77 | 0.02 |
| Public Location | 1.62 | 0.95–2.78 | 0.08 |
| Shockable rhythm | 16.21 | 5.48–47.90 | <0.001 |
| 911 call prior to SCA | 4.82 | 2.23–10.44 | <0.001 |
Missing values (time to intervention, witnessed status, public location shockable rhythm) were imputed using multiple imputations by chained equations.
Footnotes
No Conflict of Interest
Reproducible Research Statement
Study protocol: Available from Dr. Sumeet S. Chugh (e-mail, sumeet.chugh@cshs.org).
Statistical code: Not available.
Data set: Not available.
References
- 1.Go AS, Mozaffarian D, Roger VL, Benjamin EJ, Berry JD, Blaha MJ, Dai S, Ford ES, Fox CS, Franco S, Fullerton HJ, Gillespie C, Hailpern SM, Heit JA, Howard VJ, Huffman MD, Judd SE, Kissela BM, Kittner SJ, Lackland DT, Lichtman JH, Lisabeth LD, Mackey RH, Magid DJ, Marcus GM, Marelli A, Matchar DB, McGuire DK, Mohler ER, 3rd, Moy CS, Mussolino ME, Neumar RW, Nichol G, Pandey DK, Paynter NP, Reeves MJ, Sorlie PD, Stein J, Towfighi A, Turan TN, Virani SS, Wong ND, Woo D, Turner MB, American Heart Association Statistics Committee and Stroke Statistics Subcommittee Heart disease and stroke statistics–2014 update: a report from the American Heart Association. Circulation. 2014;129:e28–e292. doi: 10.1161/01.cir.0000441139.02102.80. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Adabag AS, Luepker RV, Roger VL, Gersh BJ. Sudden cardiac death: epidemiology and risk factors. Nat Rev Cardiol. 2010;7(4):216–25. doi: 10.1038/nrcardio.2010.3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Sasson C, Rogers MA, Dahl J, Kellermann AL. Predictors of survival from out-of-hospital cardiac arrest: a systematic review and meta-analysis. Circ Cardiovasc Qual Outcomes. 2010;3(1):63–81. doi: 10.1161/CIRCOUTCOMES.109.889576. [DOI] [PubMed] [Google Scholar]
- 4.Pauker SG, Estes NA, Salem DN. Preventing sudden cardiac death: can we afford the benefit? Ann Intern Med. 2005;142(8):664–6. doi: 10.7326/0003-4819-142-8-200504190-00015. [DOI] [PubMed] [Google Scholar]
- 5.Achtelik M. Preventing sudden cardiac death. Ann Intern Med. 2005;143(10):756. doi: 10.7326/0003-4819-143-10-200511150-00017. author reply. [DOI] [PubMed] [Google Scholar]
- 6.Steinhubl SR, Muse ED, Topol EJ. Can mobile health technologies transform health care? JAMA. 2013;310(22):2395–6. doi: 10.1001/jama.2013.281078. [DOI] [PubMed] [Google Scholar]
- 7.Topol EJ. Transforming medicine via digital innovation. Sci Transl Med. 2010;2(16):16cm4. doi: 10.1126/scitranslmed.3000484. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Noheria A, Teodorescu C, Uy-Evanado A, Reinier K, Mariani R, Gunson K, et al. Distinctive profile of sudden cardiac arrest in middle-aged vs. older adults: A community-based study. Int J Cardiol. 2013 doi: 10.1016/j.ijcard.2013.04.207. doi:pii:S0167-5273(13)00890-5 [Epub ahead of print] [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Chugh SS, Jui J, Gunson K, Stecker EC, John BT, Thompson B, et al. Current burden of sudden cardiac death: multiple source surveillance versus retrospective death certificate-based review in a large U.S. community. J Am Coll Cardiol. 2004;44(6):1268–75. doi: 10.1016/j.jacc.2004.06.029. [DOI] [PubMed] [Google Scholar]
- 10.Narayanan K, Reinier K, Uy-Evanado A, Teodorescu C, Chugh H, Marijon E, et al. Frequency and determinants of implantable cardioverter defibrillator deployment among primary prevention candidates with subsequent sudden cardiac arrest in the community. Circulation. 2013;128(16):1733–8. doi: 10.1161/CIRCULATIONAHA.113.002539. [DOI] [PubMed] [Google Scholar]
- 11.Teodorescu C, Reinier K, Uy-Evanado A, Ayala J, Mariani R, Wittwer L, et al. Survival advantage from ventricular fibrillation and pulseless electrical activity in women compared to men: the Oregon Sudden Unexpected Death Study. Journal of Interventional Cardiac Electrophysiology: An International Journal of Arrhythmias and Pacing. 2012;34(3):219–25. doi: 10.1007/s10840-012-9669-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Jacobs I, Nadkarni V, Bahr J, Berg RA, Billi JE, Bossaert L, et al. Cardiac arrest and cardiopulmonary resuscitation outcome reports: update and simplification of the Utstein templates for resuscitation registries. A statement for healthcare professionals from a task force of the international liaison committee on resuscitation (American Heart Association, European Resuscitation Council, Australian Resuscitation Council, New Zealand Resuscitation Council, Heart and Stroke Foundation of Canada, InterAmerican Heart Foundation, Resuscitation Council of Southern Africa) Resuscitation. 2004;63(3):233–49. doi: 10.1016/j.resuscitation.2004.09.008. [DOI] [PubMed] [Google Scholar]
- 13.Vandenbroucke JP, von Elm E, Altman DG, Gøtzsche PC, Mulrow CD, Pocock SJ, Poole C, Schlesselman JJ, Egger M, STROBE initiative Strengthening the Reporting of Observational Studies in Epidemiology (STROBE): explanation and elaboration. Ann Intern Med. 2007;147(8):W163–94. doi: 10.7326/0003-4819-147-8-200710160-00010-w1. [DOI] [PubMed] [Google Scholar]
- 14.Vandenbroucke JP. The making of STROBE. Epidemiology. 2007;18(6):797–9. doi: 10.1097/EDE.0b013e318157725d. [DOI] [PubMed] [Google Scholar]
- 15.White IR, Royston P, Wood AM. Multiple imputation using chained equations: Issues and guidance for practice. Stat Med. 2011;30(4):377–99. doi: 10.1002/sim.4067. [DOI] [PubMed] [Google Scholar]
- 16.Sterne JA, White IR, Carlin JB, Spratt M, Royston P, Kenward MG, Wood AM, Carpenter JR. Multiple imputation for missing data in epidemiological and clinical research: potential and pitfalls. BMJ. 2009;338:b2393. doi: 10.1136/bmj.b2393. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Nishiyama C, Iwami T, Kawamura T, Kitamura T, Tanigawa K, Sakai T, et al. Prodromal symptoms of out-of-hospital cardiac arrests: a report from a large-scale population-based cohort study. Resuscitation. 2013;84(5):558–63. doi: 10.1016/j.resuscitation.2012.10.006. [DOI] [PubMed] [Google Scholar]
- 18.Muller D, Agrawal R, Arntz HR. How sudden is sudden cardiac death? Circulation. 2006;114(11):1146–50. doi: 10.1161/CIRCULATIONAHA.106.616318. [DOI] [PubMed] [Google Scholar]
- 19.Meischke H, Dulberg EM, Schaeffer SS, Henwood DK, Larsen MP, Eisenberg MS. ‘Call fast, Call 911’: a direct mail campaign to reduce patient delay in acute myocardial infarction. Am J Public Health. 1997;87(10):1705–9. doi: 10.2105/ajph.87.10.1705. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Kannel WB, Wilson PW, D’Agostino RB, Cobb J. Sudden coronary death in women. Am Heart J. 1998;136(2):205–12. doi: 10.1053/hj.1998.v136.90226. [DOI] [PubMed] [Google Scholar]
- 21.Albert CM, Chae CU, Grodstein F, Rose LM, Rexrode KM, Ruskin JN, et al. Prospective study of sudden cardiac death among women in the United States. Circulation. 2003;107(16):2096–101. doi: 10.1161/01.CIR.0000065223.21530.11. [DOI] [PubMed] [Google Scholar]
- 22.Graham MM, Westerhout CM, Kaul P, Norris CM, Armstrong PW. Sex differences in patients seeking medical attention for prodromal symptoms before an acute coronary event. Am Heart J. 2008;156(6):1210–6 e1. doi: 10.1016/j.ahj.2008.07.016. [DOI] [PubMed] [Google Scholar]
- 23.Moriel M, Gavrielov-Yusim N, Gottlieb S. Cardiac symptoms in women and men. JAMA Intern Med. 2013;173(20):1929. doi: 10.1001/jamainternmed.2013.9788. [DOI] [PubMed] [Google Scholar]
- 24.Khan NA, Daskalopoulou SS, Karp I, Eisenberg MJ, Pelletier R, Tsadok MA, et al. Sex differences in acute coronary syndrome symptom presentation in young patients. JAMA Intern Med. 2013;173(20):1863–71. doi: 10.1001/jamainternmed.2013.10149. [DOI] [PubMed] [Google Scholar]
- 25.Alonzo AA, Simon AB, Feinleib M. Prodromata of myocardial infarction and sudden death. Circulation. 1975;52(6):1056–62. doi: 10.1161/01.cir.52.6.1056. [DOI] [PubMed] [Google Scholar]
- 26.Teodorescu C, Reinier K, Dervan C, Uy-Evanado A, Samara M, Mariani R, Gunson K, Jui J, Chugh SS. Factors associated with pulseless electric activity versus ventricular fibrillation: the Oregon sudden unexpected death study. Circulation. 2010;122:2116–22. doi: 10.1161/CIRCULATIONAHA.110.966333. [DOI] [PubMed] [Google Scholar]
- 27.Cobb LA, Weaver WD, Fahrenbruch CE, Hallstrom AP, Copass MK. Community-based interventions for sudden cardiac death. Impact, limitations, and changes. Circulation. 1992;85(1 Suppl):I98–102. [PubMed] [Google Scholar]
- 28.Bougouin W, Marijon E, Puymirat E, Defaye P, Celermajer DS, Le Heuzey JY, et al. Incidence of sudden cardiac death after ventricular fibrillation complicating acute myocardial infarction: a 5-year cause-of-death analysis of the FAST-MI 2005 registry. Eur Heart J. 2014;35(2):116–22. doi: 10.1093/eurheartj/eht453. [DOI] [PubMed] [Google Scholar]