

Abstract
Blunted positive affect is characteristic of depression. Altered positive affect regulation may contribute to this blunting, and two regulation strategies, dampening positive affect and positive rumination, have been implicated in depression. However, the conditions under which these strategies impart risk/protective effects prior to onset of depression are unknown. The current study examined 81 healthy children (age 7–10) at low and high risk for depression on the basis of maternal history of depression and tested how dampening and positive rumination interacted with the experience of recent positive life events to predict depressive symptoms. Children at high and low risk did not differ in their use of dampening or positive rumination. However, elevated use of dampening in the context of many positive life events predicted current depressive symptoms, and specifically anhedonic symptoms, in children at low-risk for depression. These findings held when controlling for negative rumination and negative life events. Positive rumination did not interact with positive life events but was associated with higher depressive symptoms in high-risk children. Results indicate that prior to the onset of depression, positive life events may impart risk when dampening positive affect is utilized in this context, while positive rumination may increase risk for depressive symptoms.
Keywords: Positive Affect Regulation, Dampening, Positive Rumination, Risk for Depression, Children
Dysregulated positive affect is implicated in many forms of child (Davis & Suveg, 2014), adolescent (Gilbert, 2012), and adult (Carl, Soskin, Kerns, & Barlow, 2013) psychopathology. One mental disorder with pronounced positive affect disturbance is depression, which is often characterized by anhedonia, or blunted positive affect and reduced interest and enjoyment in pleasurable daily activities (American Psychiatric Association, 2013). Although blunted positive affect is a cardinal symptom of depression, there is still a dearth of knowledge of how blunting of positive affect develops, including how positive affect regulation may contribute to this process.
The study of positive affect disturbance in depression has recently started to focus on the time course of positive affect (e.g., Davidson, 2015). Specifically, depression in adults is characterized by blunted in-the-moment liking or enjoyment of positive stimuli (for review, see Barch, Pagliaccio, & Luking, 2015) and a shorter subjective experience and neural response following positive stimuli (Heller et al., 2009; McMakin, Santiago, & Shirk, 2009). Moreover, treatments developed specifically to help maintain and savor positive affective states show great promise (McMakin, Siegle, & Shirk, 2011). Although initial evidence suggests similar positive affect disturbance in youth (Forbes & Dahl, 2012), most evidence has accumulated in adult populations. Thus, the developmental trajectories of positive affect disturbance remain unclear. One mechanism that may contribute to the development of positive affect disturbance in depression is maladaptive affect regulation.
A large body of work demonstrates that altered regulation of negative affect is associated with depression (e.g., Aldao, Nolen-Hoeksema, & Schweizer, 2010) and only more recently has literature started to examine the regulation of positive affect (du Pont, Welker, Gilbert, & Gruber, 2016). Dampening and positive rumination are two opposing strategies used specifically to regulate positive affect that have recently garnered interest. Dampening has been defined as the “tendency to respond to positive mood states with mental strategies to reduce the intensity and duration of the positive mood state” (Feldman, Joormann, & Johnson, 2008 p. 509). Dampening can be conceptualized as focusing on the negative aspects of the positive emotional state, or taking a “glass half empty” view of positive affect by thinking thoughts such as “these feelings won’t last,” or “I didn’t deserve to feel happy.” On the opposite end of the spectrum, positive rumination has been defined as the tendency to respond to positive mood states “with recurrent thoughts about positive self-qualities, positive affective experience, and one’s favorable life circumstances” (Feldman et al., 2008 p. 509). Positive rumination is associated with cyclical and repetitive thoughts centering on one’s current positive affective state, similar to how negative rumination involves responding to negative mood states by passively and repetitively focusing on one’s negative affective state (Nolen-Hoeksema, 1991). Positive rumination has been purported to help maintain or possibly increase positive affect, and is somewhat akin to savoring techniques (Bryant, 2003).
Dampening positive affect has been associated with elevated current depressive symptoms in non-clinical and community child and adult samples (Feldman et al., 2008; Nelis, Holmes, & Raes, 2015; Raes, Daems, Feldman, Johnson, & Van Gucht, 2009). Moreover, depressed and remitted depressed adults exhibit elevated dampening compared with healthy controls (Nelis et al., 2015; Raes, Smets, Nelis, & Schoofs, 2012). However, findings are inconclusive regarding the prospective association between dampening and onset of depressive symptoms in adults (Gilbert, Gruber, & Nolen-Hoeksema, 2013; Nelis et al., 2015; Raes et al., 2012) and no association has been found between dampening and future onset of depressive symptoms in children (Bijttebier, Raes, Vasey, & Feldman, 2012; Gentzler, Morey, Palmer, & Yi, 2013). Some have speculated that the tendency to dampen positive affect emerges only during or after experiencing depression and thus is more a ‘scar’ of past depression rather than a risk or vulnerability factor for the onset of future depression (Nelis et al., 2015). However, dampening could potentially be a vulnerability factor occurring prior to onset of depression, but only when the tendency to dampen positive affect is activated by specific environmental opportunities. Stated otherwise, dampening may operate in a cognitive diathesis-stress/opportunity manner (e.g., Hankin & Abramson, 2001; Kercher & Rapee, 2009), such that the cognitive effects of dampening are activated in specific contexts, such as when experiencing a positive life event (Nelis et al., 2015). Along this line of thinking, in order for the tendency of dampening to have any effect on symptoms, one might first need an environmental ‘prompt’ of a positive life event to then engage in dampening of the positive affect elicited by that life event.
The relationship between positive rumination and depression is less clear. On the one hand, it has not been associated with depressive symptoms in adults (S. L. Johnson, McKenzie, & McMurrich, 2008) and originally was theorized to be associated with manic rather than depressive symptomatology (Feldman et al., 2008). However, some work has demonstrated an inverse relationship between positive rumination and current depressive, and specifically anhedonic, symptoms in adults (Nelis et al., 2015; Raes et al., 2009; Werner-Seidler, Banks, Dunn, & Moulds, 2013). Moreover, lower positive rumination predicts the onset of elevated anhedonic symptoms in adults (Nelis et al., 2015) and remitted depressed adults who endorse elevated positive rumination endorse more positive affect during an experimental induction (Gilbert et al., 2013). Thus, there is some indication that positive rumination is a buffering or protective factor for depression, yet it is unknown whether positive rumination imparts these purported benefits in the context of positive life events and whether this is the case for youth populations.
Although it has been hypothesized (Nelis et al., 2015; Raes et al., 2009) that dampening and positive rumination may be vulnerability and protective factors that exert their effects especially in response to positive life events, this has yet to be directly tested in children or adults. Related research demonstrates that efforts to ‘maximize’ one’s positive affect (akin to positive rumination) interact with daily positive events to predict maintained positive affect (Gentzler et al., 2013). Strategies that ‘minimize’ positive affect (akin to dampening) interact with daily positive events to predict internalizing and externalizing symptoms in community adolescents (Gentzler et al., 2013). Moreover, adaptive regulatory styles have been shown to interact with positive life events by buffering the effects of experiencing few positive events on depressive symptoms in children (Vines & Nixon, 2009). Taken together, initial findings demonstrate that dampening and positive rumination may be especially potent risk and protective factors in the context of positive life events.
Present Investigation
The present study aimed to test whether dampening and positive rumination act as vulnerability and protective factors, respectively, by interacting with recent positive life events to influence current depressive symptoms. In order to assess whether these affect regulation styles are vulnerability/protective factors that emerge prior to onset of depression, we tested this in children who have yet to experience a major depressive episode but who are at high-risk for developing depression due to their mother’s history of depression. It has been well established that maternal depression increases risk for developing depression and other related disorders in children (Goodman & Gotlib, 1999; Lieb, Isensee, Höfler, Pfister, & Wittchen, 2002). Thus, by including groups at low and high risk for depression based on maternal history of depression, we were able to examine how these opposing positive affect regulation strategies may be implicated in current depressive symptoms prior to the onset of a full major depressive episode. We hypothesized that in the context of experiencing relatively more positive events, dampening would predict elevated current depressive symptoms, as positive life events would provide a ‘prompt’ from which to engage in dampening. For positive rumination, we hypothesized that in the context of experiencing relatively more positive events, positive rumination would predict fewer depressive symptoms, as positive rumination would help children capitalize on and savor positive affect associated with these life events. We hypothesized that the interactive influence of dampening would occur only in the high-versus low-risk group given that high-risk children often exhibit difficulties regulating and recovering from affective states prior to onset of depression and thus may be more susceptible to utilizing dampening in response to positive life events (Goodman & Gotlib, 1999; Kovacs & Lopez-Duran, 2010). We hypothesized that the interactive influence of positive rumination with positive life events would occur in both the high- and low-risk groups, albeit operating through different mechanisms. Specifically, we hypothesized that the high-risk group would be more susceptible to utilize emotion regulation in the context of experiencing elevated affect (Kovacs & Lopez-Duran, 2010) and the low-risk group might be more apt to glean the purported protective benefits. As part of follow-up analyses, we also examined whether these findings remained when accounting for the effects of responding to negative affect, specifically, negative rumination, to understand whether underlying response styles may not depend on the valence of affect being regulated.
Methods
Participants
A total of 130 mothers with and without depression and their 7–10 year old children were recruited via brochures/flyers distributed in schools and throughout the St. Louis, Missouri community and via the Research Participant Registry at Washington University School of Medicine to participate in a larger study examining risk for depression in children. Prior to enrollment, mothers completed a phone screen to determine eligibility, and if eligible, mothers and children completed multiple in-person sessions, including a neuroimaging scan (data presented here from self-report measures administered at behavioral sessions). Prior to participation, all mothers included in the study provided written informed consent and all children included in the study provided written assent. Procedures were approved by the Washington University in St. Louis Institutional Review Board.
Maternal psychopathology was established using the Structured Clinical Interview for DSM Disorders (SCID; First, Spitzer, Gibbon, & Williams, 2007) and child psychopathology was assessed by both mother and child report using the Kiddie Schedule for Affective Disorders and Schizophrenia for School-Age Children (K-SADS; Kaufman et al., 1997). Masters-level clinicians, trained to reliability, conducted the assessments. Exclusion criteria for children included current or past internalizing or externalizing disorders, current or past psychotropic medication use, learning, motor, or major medical disorders, age beyond 7–10 years, gestational age < 35 weeks, maternal drug use during pregnancy, prohibition of candy intake, and braces (the latter two criteria for use in a neuroimaging task not examined here).
Eighty-one mother-child pairs met all inclusion criteria and completed self-report measures. Of these participants, 34 mothers experienced at least one past depressive episode and children of these mothers were denoted ‘high-risk.’ Forty-seven mothers exhibited no lifetime history of psychiatric diagnoses and children of these mothers were denoted ‘low-risk.’ High-risk mothers (mothers with a history of depression) experienced an average of 5.86 (SD = 10.86) previous depressive episodes and 11 mothers endorsed too many previous episodes to count. The average age of onset of mothers’ first depressive episode was 20.39 (SD =8.01). Eleven mothers (32%) endorsed a major depressive episode in the past month with 28 mothers (82%) experiencing at least one major depressive episode during their child’s lifetime. Comorbidities of mothers with a history of depression included 8 (24%) mothers with a lifetime anxiety disorder and 13 (38%) with lifetime substance abuse/dependence. Given the focus of the larger study was to assess vulnerability and protective factors in children at risk for depression, only psychiatrically healthy children were included. The average age of the healthy children was 8.91(SD= 1.17). The majority of children were White (n = 41, 51%), followed by African American (n = 30, 37%), biracial (n = 9, 11%), and other/unknown (n = 1, 1%). Average family income was between $51,000 – $60,000 per year.
Measures
Depressive symptoms
Child-reported depressive symptoms were assessed with the Child Depression Inventory-Child Version (CDI-C Kovacs, 1985). The CDI-C is a 27-item measure assessing depressive symptoms on a 3-point scale ranging from 0 (e.g., I have fun in many things) to 2 (e.g., nothing is fun at all). Age/gender normalized t-scores were used for all analyses. The anhedonia subscale of the CDI-C measures anhedonia as part of an endogenous depression, which included items measuring a loss of pleasure (i.e., anhedonia) and also sleep, appetite, and isolation. The negative mood subscale of the CDI-C measures sadness, worrying, crying, and difficulty making up ones’ mind.
Dampening and Positive Rumination
Dampening and positive rumination were measured in children using the Response to Positive Affect questionnaire (RPA; Feldman et al., 2008). The RPA is a 17-item self-reported measure that asks participants to rate how much they engage in different responses when they are feeling happy, excited, or enthused on a 1 (almost never) to 4 (almost always) scale. In children and adults, a two-factor model demonstrates the best fit to the data (Bijttebier et al., 2012; Nelis et al., 2016), reflecting subscales of dampening one’s positive emotion (e.g., think about things that could go wrong) and positive rumination (e.g., think about how happy you feel), the latter includes previously used emotion-focused and self-focused positive rumination. Good internal consistency was obtained for both dampening (α = 0.72) and positive rumination (α = 0.84) in the current sample.
Rumination
Rumination in the context of negative mood states was assessed using the Children’s Response Styles Questionnaire (CRSQ; Abela, Brozina, & Haigh, 2002). The CRSQ is a 25 item self-report measure that asks the child how they usually respond when they are sad from 0 (almost never) to 3 (almost always). In the current study we only included the 13-item rumination subscale (e.g., think why can’t I handle things better?), which demonstrated good internal consistency (α = 0.86).
Life events
Recent life events were assessed by child and mother report using a modified stressful life events checklist (J. H. Johnson & McCutcheon, 1980; Pagliaccio et al., 2014). Children were asked whether or not they have experienced a list of events in the last six months or ever in their lives that included events such as “moving to a new home,” “failing to make an athletic team,” and “increased absence of parents from home.” Mothers were asked the same questions regarding their child’s experience of life events. Some items were objectively negative (i.e., “death of a family member”) while some events were more ambiguous and could potentially be experienced as positive or negative (i.e., “change in parents’ financial status” or “moving to a new home”). For each event experienced, the child (and mother) rated the event as “good” or “bad.” The numbers of positive and negative life events were summed separately. Children endorsed experiencing 0 to 4 positive life events and 0 to 15 negative events in the past six months. Mothers endorsed their child experiencing 0 to 10 positive life events and 0 to 12 negative life events in the past six months. Inter-correlations among child- and maternal-report of positive and negative life events counts are presented in Table 2.
Table 2.
Bivariate correlations between predictor and dependent variables in entire sample of healthy children (N = 81).
| Measure | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 |
|---|---|---|---|---|---|---|---|---|
| 1. Dampening | – | |||||||
| 2. Positive Rumination | 0.24* | – | ||||||
| 3. Negative Rumination | 0.63** | 0.19 | – | |||||
| 4. Child Positive life events | 0.17 | 0.14 | 0.15 | – | ||||
| 5. Child Negative life events | 0.24* | 0.08 | 0.28* | 0.19 | – | |||
| 6. Mother Positive life events | 0.26* | 0.26* | 0.23* | .07 | 0.32** | – | ||
| 7. Mother Negative life events | 0.21 | 0.03 | 0.05 | .09 | 0.36** | 0.44** | – | |
| 8. CDI-Sum | 0.36** | 0.24* | 0.33** | 0.15 | 0.31** | 0.19 | 0.20 | – |
| 9. CDI-Anhedonia | 0.40** | 0.21 | 0.37** | 0.10 | 0.26* | 0.13 | 0.2 | 0.88** |
Note: Dampening = child-reported dampening positive affect; Positive rumination= child-reported positive rumination composite of self-focused and emotion-focused positive rumination; Negative Rumination = child-reported rumination in the context of negative moods; Child positive and negative life events= number of child-reported life events within the last six months; Mother positive and negative life events= number of mother-reported life events within the last six months; CDI Sum = child reported depressive symptoms total t-score; CDI Anhedonia= child reported anhedonia subscale t-score.
p < .05;
p < .01
Data analytic Plan
Preliminary analyses included missing data analysis, and Little’s MCAR test revealed that data from the self-report measures were missing at random (Schafer & Graham, 2002). If an entire questionnaire was missing it was not included in missing data imputation. Missing data were imputed using the expectation-maximum (EM) algorithm, which has been shown to be the preferred way of dealing with missing data over list-wise deletion or means substitution (Schafer & Graham, 2002). Predictors were visually examined for skew and were transformed when needed. We then examined group differences on demographic, predictor, and outcome variables between low- and high-risk groups utilizing t-tests and chi-square tests. Bivariate correlations were examined among demographic and predictors of interest.
To test our main hypothesis examining the interactive effects of dampening or positive rumination and experience of recent positive life events in children at low and high risk for depression, we performed hierarchical linear regressions including predictors of dampening (or positive rumination in separate regressions), recent positive life events, and risk status predicting child-reported depressive symptoms. Multicollinearity diagnostics from all regressions showed tolerance statistics within acceptable standards (no tolerance values below 0.1 or VIF values greater than 10.0; Myers, 1990). Step 1 included demographic control variables including ethnicity (dichotomized as white versus non-white), and centered variables for child age and family income (coded in 21 increments of $5,000 starting with 1= $1,000 to $5,000 and ending with 21= >$100,000). Step 2 included centered independent effects of dampening (or positive rumination), centered recent positive event scores, and risk status. Step 3 included all two-way interactions of the variables in Step 2. Lastly, Step 4 included the three-way interaction between dampening, recent positive events, and risk status. In the case of significant two-way interactions, simple slopes were tested. For significant three-way interactions, two-way interactions were examined separately in the two risk groups (high and low risk by maternal depression) and simple slopes were tested for significant two-way interactions.
Results
Descriptive Statistics and Participant Characteristics
Negative rumination exhibited positive skew and was thus square root transformed. Child and mother-reported positive and negative life events were also positively skewed and due to zero values (indicating no positive or negative life events endorsed in the last six months), we added to a constant of 1 and then used a natural logarithmic transformation. These transformed variables and all other variables were normally distributed. Children in the two risk groups did not significantly differ on any variables of interest (Table 1). Elevated child reported depressive symptoms were associated with younger child age, r = −.30, p = .007 and lower family income, r = −.41, p < .0001, and non-White children reported elevated depressive symptoms t(50.43) = 2.38, p = .01. Thus age, income, and ethnicity were included as covariates in regression analyses. For descriptive purposes, Table 2 presents bivariate correlations between all predictors and dependent variables.
Table 1.
Sample characteristics in children at low and high risk for depression.
| Low Risk (n = 47) |
High Risk (n = 34) |
|
|---|---|---|
| Demographics | ||
| Sex (% Female) | 47% | 53% |
| Age | 9.02 (1.13) | 8.77 (1.20) |
| Ethnicity (% White) | 57% | 68% |
| Family income | 12.18 (7.05) | 10.97 (7.35) |
| (monetary increment range) | ($56,000–$60,000) | ($46,000–$50,000) |
| Response to Positive Affect | ||
| Dampening | 13.32 (3.94) | 14.55 (4.17) |
| Positive Rumination | 24.57 (6.19) | 25.23 (5.59) |
| Negative Rumination | 1.67 (0.56) | 1.70 (0.57) |
| Life Events Checklist | ||
| Child Reported Positive events | 0.77 (1.00) | 0.91 (1.00) |
| Mother reported Positive events | 2.45(2.34) | 2.88 (2.01) |
| Child Reported Negative events | 2.26 (2.08) | 2.38 (2.08) |
| Mother Reported Negative events | 1.87 (2.45) | 2.44 (2.05) |
| Symptom Measurement | ||
| CDI Sum | 48.66 (10.31) | 52.54 (14.30) |
| CDI Anhedonia | 47.89 (10.31) | 51.74 (10.20) |
Note: Family income coded in 21 increments of $5,000 starting with 1= $1,000 to $5,000 and ending with 21= >$100,000. Positive rumination is a sum score of self-focused and emotion-focused positive rumination; Negative and positive life events are within the last six months; CDI Sum = child reported depressive symptoms total t-score; CDI Anhedonia= child reported anhedonia subscale t-score. All p’s > .05.
Downregulation of Positive Affect: Associations of Dampening with Symptoms
A hierarchical linear regression was conducted to examine the relationship between recent positive life events, dampening, and risk status with child-reported depressive symptoms (see Table 3). The covariates of ethnicity, age, and parent income (discussed above) were significant predictors in Step 1, F(3,77) = 8.39, R2 = 0.25, p < .0001. The addition of dampening, recent positive events, and risk status in Step 2 was not significant nor was Step 3 when two-way interactions of these variables were entered. However, when a three-way interaction between dampening, recent positive events, and risk status was entered in Step 4, the interaction significantly predicted depressive symptoms, Model 4: F(1,70) = 6.99, R2 = 0.38, ΔR2= .06, p = .01; Dampening × positive events × Risk, β = −0.36, p = .01.
Table 3.
Hierarchical multiple regression analyses predicting depressive and anhedonic symptoms from recent positive life events, risk status, dampening and positive rumination.
| Predictor | Dampening
|
Positive Rumination
|
|||||||
|---|---|---|---|---|---|---|---|---|---|
| CDI-Sum | CDI-Anhedonia | CDI-Sum | CDI-Anhedonia | ||||||
|
| |||||||||
| ΔR2 | β | ΔR2 | β | Predictor | ΔR2 | β | ΔR2 | β | |
| Step 1 | .25** | 64** | Step 1 | .25** | 64** | ||||
| Control Variablesa | Control Variablesa | ||||||||
| Step 2 | .06 | .03 | Step 2 | .03 | .02 | ||||
| Dampening | .23 | .13 | Positive Rumination | .12 | −.02 | ||||
| Positive Life Events | .03 | −.07 | Positive Life Events | .04 | −.06 | ||||
| Risk Status | .08 | .11 | Risk Status | .10 | .12 | ||||
| Step 3 | .02 | .01 | Step 3 | .08ˆ | .03 | ||||
| Dampening × Risk | .04 | −.02 | Pos Rumination × Risk | .30* | .18 | ||||
| Dampening × Positive Life Events | .05 | .09 | Pos Rumination × Positive Life Events | −.02 | .12 | ||||
| Risk × Positive Life Events | −.18 | −.09 | Risk × Positive Life Events | −.28* | −.15 | ||||
| Step 4 | .06** | .03* | Step 4 | .01 | .00 | ||||
| Dampening × Positive Life Events × Risk | −.36** | −.25* | Pos rumination × Positive Life Events × Risk | −.12 | .01 | ||||
Note. CDI Sum= child reported depressive symptoms total t-score; CDI Anhedonia= child reported anhedonia subscale t-score; Pos Rumination= Positive Rumination; Positive life events= number of child self-reported positive life events in the last six months.
Control variables for CDI-SUM included age, parent income, ethnicity (dummy coded White vs. Minority); Control variables for CDI-Anhedonia included previously mentioned control variables for CDI-SUM in addition to the CDI-Negative Mood subscale.
p = .05;
p < .05;
p < .01
To decompose this three-way interaction, we examined the two-way interaction (dampening × positive events) separately in the two risk groups. In the low-risk group, the interaction of dampening by positive events was significant in Step 3, F(1,40) = 6.83, R2 = 0.53, ΔR2= .08, p = .01, β = 0.30, p = .009, while this interaction was not significant in the high-risk group, F(1,27) = 1.81, R2 = 0.21 ΔR2= .05, p = .19, β = −0.24, p = .19 (Figure 1b). Simple slopes were tested in the dampening by positive events interaction that emerged in the low-risk group. Simple slopes revealed that, for the low-risk group, the influence of dampening on depressive symptoms was moderated by the number of positive life events (Figure 1a). Specifically, 1 standard deviation (SD) below the mean, (b= −0.78, SE = 0.66, t = −1.19, p = .24) and at the mean (b= 0.20, SE = 0.44, t = 0.46, p = .65) of positive life events did not interact with dampening to influence depressive symptoms, however for 1 SD above the mean of positive life events (b=1.18, SE = .49, t = 2.42, p = .02), dampening was associated with elevated depressive symptoms.
Figure 1.
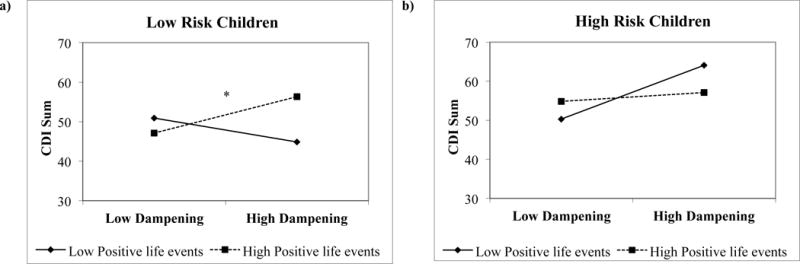
a–b Interaction of dampening positive affect and positive life events predicting depressive symptoms separated by risk group.
*Note: Interactions demonstrating 1 SD above and below the mean; CDI Sum = child reported depressive symptoms total t-score. (a) Simple slopes tests demonstrated a significant interaction between high dampening and 1 SD above the mean for positive events (high positive events), *p = .01 (b) interaction between dampening and positive life events not significant for high-risk children.
Upregulation of Positive Affect: Associations of Positive Rumination with Symptoms
A second hierarchical linear regression was conducted, to examine the relationship between recent positive life events, risk status, and positive rumination on child-reported depressive symptoms (see Table 3). As discussed above, the covariates of ethnicity, age, and parent income in Step 1 were significant, F(2,77) = 8.39, R2 = 0.25, p < .0001. Step 2 was not significant, however Step 3 was, F(3,71) = 2.72, R2 = 0.35, ΔR2= 0.08, p = .05, with two significant two-way interactions emerging: positive rumination by risk status (β = 0.30, p = .02) and positive life events by risk status (β = −0.28, p = .045). The three-way interaction added in Model 4 was not significant.
For the positive rumination by risk status interaction, simple slopes tests revealed that the effect of positive rumination on depressive symptoms was only significant in the high-risk group. Specifically, those high-risk children who engaged in more positive rumination reported elevated depressive symptoms (b = 0.87, SE = 0.39, t = 2.25, p = .03) while positive rumination did not influence depressive symptoms in low-risk children (b = −0.06, SE = 0.30, t = 0.20, p = .85; see Figure 2). For the positive life events by risk status interaction, simple slopes tests were not significant for either the low risk group (b = −11.50, SE = 10.95, t = −1.05, p = .30) or the high-risk group (b = 10.95, SE = 8.57, t = 1.28, p = .21).
Figure 2.
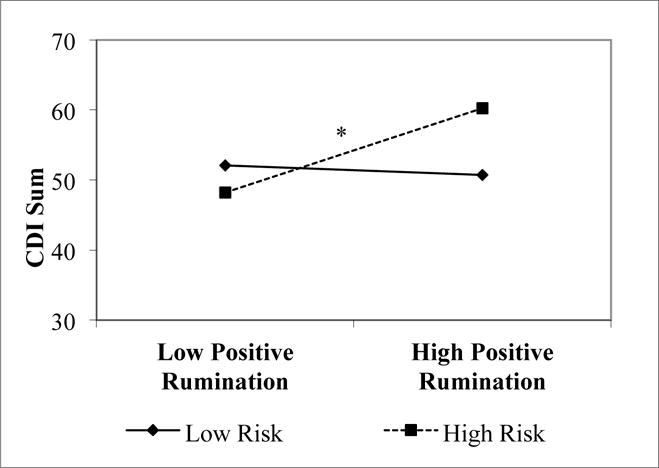
Interaction of positive rumination and risk on depressive symptoms.
*Note: CDI Sum = child reported depressive symptoms total t-score; simple slopes tests demonstrated a significant interaction between high positive rumination and high risk children, *p = .03.
Follow-up Analysis
We completed three follow-up analyses to better understand findings. The first examined whether findings would replicate when examining child-reported anhedonic symptoms. Regressions were run replacing child-reported depressive symptoms with the anhedonia subscale from the CDI while also controlling for the negative mood subscale from the CDI, to examine specificity with anhedonic symptoms. Again a three-way interaction emerged for dampening, positive life events and risk status in Step 4, F(1,69) = 6.46, R2 = 0.70, ΔR2= 0.03, β = −0.25, p = .01 (see Table 3). Results were similar to above when we examined the dampening by positive life events interaction separately in the two risk groups: only the low risk group exhibited a relationship between dampening and positive life events with depressive symptoms, F(1,39) = 6.74, R2 = 0.85, ΔR2= 0.05, β = 0.24, p = .01. Again, simple slopes tests revealed the same pattern as above: that for the low-risk children, only when experiencing positive events 1 SD above the mean (b = .73, SE = .30, t = 2.41, p = .02) was dampening associated with elevated anhedonic symptoms, but this was not the case at the mean (b = .13, SE = .26, t = .48, p = .63) or 1 SD below the mean of positive life events (b = −.47, SE = .39, t = −1.2, p = .23). For positive rumination, none of the steps in the regression significantly predicted anhedonic symptoms when controlling for negative mood symptoms, demonstrating that positive rumination does not appear to play a specific role in anhedonic symptoms, but instead relates to depressive symptoms more generally in the context of risk.
The second follow-up analysis aided in better understanding the independent effects of dampening and positive rumination above and beyond the tendency to ruminate in negative moods and the influence of negative life events. To do this, we completed the original regressions again, but also included additional control variables at Step 1: recent negative life event scores (centered) as well as negative rumination (centered). Outcomes included sum depressive symptoms and the anhedonia subscale (again controlling for the negative mood subscale). For dampening, even when controlling for rumination in the context of negative moods and the influence of negative life events, the patterns were parallel. Specifically, only Model 4 was significant, demonstrating again a three way interaction between dampening, positive life events and risk status for both sum depressive symptoms, F(1,68) = 8.02, R2 = 0.43, ΔR2= 0.07, β = −0.38, p = .006, and anhedonic symptoms, F(1,67) = 7.59, R2 = 0.72, ΔR2= 0.03, β = −0.27, p = .008. Follow-up analyses to decompose the interactions with dampening revealed parallel findings to above. For the positive rumination regressions, when the influence of rumination in the context of negative moods and negative life events were accounted for, none of the effects of positive rumination, positive life events or risk status on depressive or anhedonic symptoms were statistically significant (all p’s > .05).
Lastly, given that maternal and child report are often discrepant (De Los Reyes & Kazdin, 2005), we examined maternal report of child positive life events in the original hypothesized regressions above. Again, the same pattern of findings emerged. For dampening, there was a three-way interaction with dampening, positive life events and risk status for depressive symptoms, F(1,70) = 7.00, R2 = 0.38, ΔR2= 0.06, β = −0.48, p = .01 and anhedonic symptoms, F(1,69) = 6.46, R2 = 0.70, ΔR2= 0.03, β = −0.33, p = .01 with the same pattern of follow-up analyses and simple slopes tests. For positive rumination, the same two-way interaction of positive rumination and risk status was significant for sum depressive symptoms, F(1,71) = 2.72, R2 = 0.27, ΔR2= 0.08, p = .05, β = 0.30, p = .02
Discussion
The present investigation provides preliminary support for the association between dampening and positive rumination and current depressive symptoms in children, however the expected associations in children at high versus low risk for depression were not supported. Specifically, although dampening interacted with positive life events to predict concurrent depressive symptoms, and specifically anhedonic symptoms, this relationship was observed only within in the low-risk group. Moreover, positive rumination was hypothesized to be associated with fewer depressive symptoms in the context of positive life events across low and high-risk children. However, we found positive rumination to be associated with elevated depressive symptoms only in the high-risk children, where it did not interact with life events. The current study is the first to examine tendencies to dampen and ruminate on positive affect in children at risk for depression. Although findings revealed differing associations than anticipated, we demonstrate how two forms of positive affect regulation may influence current symptomatology, potentially increasing risk for the onset of a full depressive episode.
First, our findings provide partial and preliminary support of a cognitive diathesis-stress/opportunity model of dampening. Specifically, when children at low-risk for developing depression experienced many recent positive life events and also engaged in more dampening of their positive affect, they experienced higher self-reported depressive symptoms. This finding held when controlling for the influence of negative life events and the tendency to ruminate in negative mood states, and also replicated using mother-reported recent positive life events. These findings partially support our hypothesis that in the context of many positive life events, these events may act as a “prompt” by which the process of dampening is activated and takes effect. However, we hypothesized that dampening would confer vulnerability in this manner in children at high (not low) risk for depression. Dampening positive affect may have stronger effects in low-risk children, as dampening is a more nuanced process that occurs in what might usually be thought of as a buffering context—experiencing positive life events. In the context of positive events, if low-risk children engage in dampening, they might not be able to glean the benefits of the positive life events. In fact, dampening positive affect in the context of a positive life event may lead to faster positive affect attenuation, which could increase risk for later depressive symptoms. Although speculative, it might be that over multiple instances of dampening positive events, these low-risk children who utilize more dampening start to accumulate risk by repeatedly attenuating their positive affective experience.
With regards to positive rumination, this regulatory style did not interact with life events to confer protection from depressive symptoms across low- and high-risk children as originally hypothesized. Conversely, positive rumination was associated with elevated depressive (but not anhedonic) symptoms only in the high-risk children. We were surprised by this counter-intuitive result, although the current literature demonstrates inconclusive and mixed findings with regards to protective versus symptom related associations with positive rumination (Bijttebier et al., 2012; Gilbert et al., 2013; Raes et al., 2009). One speculation for our findings is that the underlying response style of ruminating confers risk for depressive symptoms in high-risk children no matter if occurring in positive or negative mood states. Specifically, a large body of literature demonstrates that ruminating in a negative mood increases risk for depression in youth (Rood, Roelofs, Bögels, Nolen-Hoeksema, & Schouten, 2009) and follow-up analyses in the current study demonstrated that when controlling for negative rumination, the associations between positive rumination and depressive symptoms in the high-risk group no longer remained. Related, it should also be noted that when examining bivariate correlations between positive and negative rumination in the current sample, positive rumination and negative rumination were not correlated in the low risk group (r = .07, p = .63), yet were positively correlated in the high-risk group (r = 0.35, p = .04) (combined correlations shown in Table 2). Given that the basic process of ruminating involves a repetitive and passive cognitive style that is associated with difficulties in cognitive inhibition and executive control (Joormann, 2010; Quinn & Joormann, 2015), future research may benefit from understanding whether positive rumination is associated with similar underlying cognitive styles as negative rumination, which might clarify previous discrepant results and provide reason for how the adaptive use of positive rumination may go awry. In particular, it might be that children at high-risk have been exposed to depressed mothers who engage in higher levels of negative rumination and related cognitive styles and these underlying cognitive styles might provide one means by which positive rumination potentially becomes maladaptive.
Our findings provide preliminary clinical implications with regards to how children regulate their positive affect. First, helping children savor their positive life events, rather than dampening the positive affect associated with positive life events, may be important to reduce risk for onset of depressive symptoms. Relatedly, the context of experiencing a positive life event may be a pertinent target for modifying maladaptive positive affect regulation. Second, further research is needed to understand the protective versus detrimental effects of positive rumination on depressive symptoms in children. Although positive rumination may be adaptive (e.g., Nelis et al., 2015), positive rumination may also trigger basic cognitive ruminative processes that increase depressive symptoms. Thus, it will be important for future research to clarify whether treatments aimed at helping children savor positive affect may need to be attentive to avoiding inadvertently triggering ruminative tendencies. Moreover, given that these children are about to enter adolescence, which is characterized by decreased positive affect (Larson, Moneta, Richards, & Wilson, 2002) and increased onset of psychopathology (Kessler, Chiu, Demler, & Walters, 2005), teaching adaptive ways to regulate positive affect early may have longer term benefits.
It should be noted that across groups of children at low and high risk for depression, there were no differences in tendencies to dampen positive affect or engage in positive rumination, indicating that the experience of positive life events may be an important context to examine these regulation strategies. Moreover, there were no overall group differences in depressive symptoms and only psychiatrically healthy children were included, which reduced variability and severity of depressive symptoms in the sample. This latter point limits generalizability to more severe clinical levels of depressive symptoms, but may also demonstrate that even at normative ranges of depressive symptoms, dampening and positive rumination may play nuanced roles in increasing vulnerability prior to the onset of depression.
Findings from the current study should be interpreted within the confines of several limitations. First, the study was cross-sectional and thus we cannot conclude whether dampening and positive rumination are predictive of future onset of depressive symptoms nor can we conclude that the depressive symptoms endorsed by the children are associated with increased onset of a full depressive episode. Future research is needed to prospectively examine the association of these regulation strategies with incidence and maintenance of depression in high-risk samples. Secondly, we only examined these affect regulation strategies in relation to depressive symptoms. Dampening has been associated with increased non-suicidal self-injury in adolescents (Burke et al., 2015) and predicts onset of elevated manic symptoms (Gilbert et al., 2013). Future work would benefit by examining the transdiagnostic implications of dampening in predicting maladaptive positive affect functioning and onset of different forms of symptomatology. Third, our primary analysis used all child-reported measures. Although younger children’s report is more consistent with other informants compared to that of adolescents (De Los Reyes & Kazdin, 2005), and we did replicate analyses using maternal reported recent life events, using all child report in the primary analyses could have led to inflated correlations between variables. Fourth, the measure of life events included negative events and ambiguous events and few objectively positive events. This led to a positively skewed positive life events indicator as many children reported experiencing no positive events in the previous six months. This low number of endorsed positive life events and resulting positive skew limits the generalizability of findings as it is probable that many experienced positive life events were not accounted for. Future research would benefit by examining a more encompassing measure of solely objective positive events. Moreover, future research would benefit by using experience sampling methods to assess how dampening or ruminating on these positive life events influences positive affect in the moment. Fifth, the sample size was modest and results should be interpreted with caution. Future research would benefit by replicating findings in larger samples as well as examining associations in children and adolescents who are currently or have already experienced a major depressive episode, to understand whether dampening interacts with positive life events to maintain or increase relapse rates in depression in developmental populations.
In sum, in children at low risk for depression, dampening was associated with higher depressive symptoms in the presence of many recent positive life events. This finding was above and beyond the influence of negative life events and negative rumination and appeared to be specific to symptoms of anhedonia. These associations of dampening with depressive symptoms may demonstrate one pathway by which positive affect comes to be attenuated in depression. Moreover, positive rumination appears to be associated with elevated depressive symptoms only for high-risk children. Positive rumination may not be an adaptive regulation strategy for high-risk children. However, identifying other ways to help children experience their positive affect to the greatest extent (without dampening it or ruminating on it) will be important to identify as possible targets of treatment and prevention.
Acknowledgments
This study was funded by the Sidney R. Baer Jr. Foundation; Brain and Behavior Research Foundation and the National Institute of Mental Health (MH097335).
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. This article does not contain any studies with animals performed by any of the authors.
Informed consent was obtained form all individual participants included in the study.
Footnotes
Kirsten Gilbert declares that she has no conflict of interest. Katherine Luking declares that she has no conflict of interest. David Paggliaccio declares that he has no conflict of interest. Joan Luby declares that she has no conflict of interest. Deanna Barch declares that she has no conflict of interest.
References
- Abela JRZ, Brozina K, Haigh EP. An Examination of the response styles theory of depression in third and seventh grade children: A short-term longitudinal study. Journal of Abnormal Child Psychology. 2002;30:515–527. doi: 10.1023/a:1019873015594. [DOI] [PubMed] [Google Scholar]
- Aldao A, Nolen-Hoeksema S, Schweizer S. Emotion-regulation strategies across psychopathology: A meta-analytic review. Clinical Psychology Review. 2010;30:217–237. doi: 10.1016/j.cpr.2009.11.004. [DOI] [PubMed] [Google Scholar]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders. 5th. Arlington, VA: American Psychiatric Publishing; 2013. [Google Scholar]
- Barch DM, Pagliaccio D, Luking KR. Mechanisms underlying motivational deficits in psychopathology: Similarities and differences in depression and schizophrenia. In: Simpson EH, Balsam PD, editors. Behavioral Neuroscience of Motivation. Vol. 27. Heidelberg Switzerland: Springer; 2015. pp. 411–450. [DOI] [PubMed] [Google Scholar]
- Bijttebier P, Raes F, Vasey MW, Feldman GC. Responses to positive affect predict mood symptoms in children under conditions of stress: A prospective study. Journal of Abnormal Child Psychology. 2012;40:381–389. doi: 10.1007/s10802-011-9579-2. [DOI] [PubMed] [Google Scholar]
- Bryant FB. Savoring Beliefs Inventory (SBI): A scale for measuring beliefs about savouring. Journal of Mental Health. 2003;12(2):175–196. doi: 10.1080/0963823031000103489. [DOI] [Google Scholar]
- Burke TA, Stange JP, Hamilton JL, Cohen JN, O’Garro-Moore J, Daryanani I, Alloy LB. Cognitive and Emotion-Regulatory Mediators of the Relationship Between Behavioral Approach System Sensitivity and Nonsuicidal Self-Injury Frequency. Suicide and Life-Threatening Behavior. 2015:495–504. doi: 10.1111/sltb.12145. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Carl JR, Soskin DP, Kerns C, Barlow DH. Positive emotion regulation in emotional disorders: A theoretical review. Clinical Psychology Review. 2013;33(3):343–360. doi: 10.1016/j.cpr.2013.01.003. [DOI] [PubMed] [Google Scholar]
- Davidson RJ. Comment: Affective chronometry has come of age. Emotion Review. 2015:1–3. doi: 10.1177/1754073915590844. 1754073915590844. [DOI] [Google Scholar]
- Davis M, Suveg C. Focusing on the positive: A review of the role of child positive affect in developmental psychopathology. Clinical Child and Family Psychology Review. 2014;17:97–124. doi: 10.1007/s10567-013-0162-y. [DOI] [PubMed] [Google Scholar]
- De Los Reyes A, Kazdin AE. Informant Discrepancies in the Assessment of Childhood Psychopathology: A Critical Review, Theoretical Framework, and Recommendations for Further Study. Psychological Bulletin. 2005;131(4):483–509. doi: 10.1037/0033-2909.131.4.483. [DOI] [PubMed] [Google Scholar]
- du Pont A, Welker K, Gilbert KE, Gruber J. The emerging field of positive emotion dysregulation. In: Vohs KD, Baumeister RF, editors. Handbook of Self-Regulation: Research, Theory and Applications. 3rd. New York: Guiford; 2016. pp. 364–379. [Google Scholar]
- Feldman GC, Joormann J, Johnson SL. Responses to positive affect: A self-report measure of rumination and dampening. Cognitive Therapy and Research. 2008;32:507–525. doi: 10.1007/s10608-006-9083-0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- First MB, Spitzer RL, Gibbon M, Williams J. Structured Clinical Interview for DSM-IV-TR Axis I Disorders, Research Version, Patient Edition (SCID-VP) New York: Biometrics Research, New York State Psychiatric Institude; 2007. [Google Scholar]
- Forbes EE, Dahl RE. Research Review: Altered reward function in adolescent depression: what, when and how? Journal of Child Psychology and Psychiatry. 2012;53(1):3–15. doi: 10.1111/j.1469-7610.2011.02477.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gentzler AL, Morey JN, Palmer CA, Yi CY. Young Adolescents’ Responses to Positive Events: Associations With Positive Affect and Adjustment. The Journal of Early Adolescence. 2013;33(5):663–683. doi: 10.1177/0272431612462629. [DOI] [Google Scholar]
- Gilbert K. The neglected role of positive emotion in adolescent psychopathology. Clinical Psychology Review. 2012;32(6):467–481. doi: 10.1016/j.cpr.2012.05.005. [DOI] [PubMed] [Google Scholar]
- Gilbert K, Gruber J, Nolen-Hoeksema S. Positive emotion dysregulation across mood disorders: How amplifying versus dampening predicts emotional reactivity and illness course. Behavior Research and Therapy. 2013;51:736–741. doi: 10.1016/j.brat.2013.08.004. [DOI] [PubMed] [Google Scholar]
- Goodman SH, Gotlib IH. Risk for psychopathology in the children of depressed mothers: A developmental model for understanding mechanisms of transmission. Psychological Review. 1999;106(3):458–490. doi: 10.1037/0033-295x.106.3.458. [DOI] [PubMed] [Google Scholar]
- Hankin BL, Abramson LY. Development of gender differences in depression: An elaborated cognitive vulnerability–transactional stress theory. Psychological Bulletin. 2001;127(6):773–796. doi: 10.1037/0033-2909.127.6.773. [DOI] [PubMed] [Google Scholar]
- Heller AS, Johnstone T, Shackman AJ, Light SN, Peterson MJ, Kolden GG, Davidson RJ. Reduced capacity to sustain positive emotion in major depression reflects diminished maintenance of fronto-striatal brain activation. Proceedings of the National Academy of Sciences. 2009;106(52):22445–22450. doi: 10.1073/pnas.0910651106. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Johnson JH, McCutcheon SM. Assessing life stress in older children and adolescents: Preliminary findings with the Life Events Checklist. Stress and anxiety. 1980;7:111–125. [Google Scholar]
- Johnson SL, McKenzie G, McMurrich S. Ruminative responses to negative and positive affect among students diagnosed with bipolar disorder and major depressive disorder. Cognitive Therapy and Research. 2008;32:702–713. doi: 10.1007/s10608-007-9158-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Joormann J. Cognitive Inhibition and Emotion Regulation in Depression. Current Directions in Psychological Science. 2010;19(3):161–166. doi: 10.1177/0963721410370293. [DOI] [Google Scholar]
- Kaufman J, Birmaher B, Brent D, Rao UMA, Flynn C, Moreci P, Ryan N. Schedule for Affective Disorders and Schizophrenia for School-Age Children-Present and Lifetime Version (K-SADS-PL): Initial reliability and validity data. Journal of the American Academy of Child & Adolescent Psychiatry. 1997;36(7):980–988. doi: 10.1097/00004583-199707000-00021. [DOI] [PubMed] [Google Scholar]
- Kercher A, Rapee R. A Test of a Cognitive Diathesis—Stress Generation Pathway in Early Adolescent Depression. Journal of Abnormal Child Psychology. 2009;37(6):845–855. doi: 10.1007/s10802-009-9315-3. [DOI] [PubMed] [Google Scholar]
- Kessler RC, Chiu WT, Demler O, Walters EE. Prevalence, severity, and comorbidity of 12-month DSM-IV disorders in the National Comorbidity Survey Replication. Archives of General Psychiatry. 2005;62:617–627. doi: 10.1001/archpsyc.62.6.617. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kovacs M. The Children’s Depression Inventory (CDI) Psychopharmacology Bulletin. 1985;21:995–1124. [PubMed] [Google Scholar]
- Kovacs M, Lopez-Duran N. Prodromal symptoms and atypical affectivity as predictors of major depression in juveniles: implications for prevention. Journal of Child Psychology and Psychiatry. 2010;51(4):472–496. doi: 10.1111/j.1469-7610.2010.02230.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Larson R, Moneta G, Richards MH, Wilson S. Continuity, stability, and change in daily emotional experience across adolescence. Child Development. 2002;73(4):1151–1165. doi: 10.1111/1467-8624.00464. [DOI] [PubMed] [Google Scholar]
- Lieb R, Isensee B, Höfler M, Pfister H, Wittchen H. Parental major depression and the risk of depression and other mental disorders in offspring: A prospective-longitudinal community study. Archives of General Psychiatry. 2002;59(4):365–374. doi: 10.1001/archpsyc.59.4.365. [DOI] [PubMed] [Google Scholar]
- McMakin DL, Santiago CD, Shirk SR. The time course of positive and negative emotion in dysphoria. The Journal of Positive Psychology. 2009;4(2):182–192. doi: 10.1080/17439760802650600. [DOI] [PMC free article] [PubMed] [Google Scholar]
- McMakin DL, Siegle G, Shirk S. Positive affect stimulation and sustainment (PASS) module for depressed mood: A preliminary investigation of treatment-related effects. Cognitive Therapy and Research. 2011;35(3):217–226. doi: 10.1007/s10608-010-9311-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Myers R. Classical and modern regression with applications. 2nd. Boston, MA: Duxbury; 1990. [Google Scholar]
- Nelis S, Holmes E, Raes F. Response styles to positive affect and depression: Concurrent and prospective associations in a community sample. Cognitive Therapy and Research. 2015;39(4):480–491. doi: 10.1007/s10608-015-9671-y. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Nelis S, Luyckx K, Feldman G, Bastin M, Raes F, Bijttebier P. Assessing response styles to positive affect: One or two dimensions of positive rumination in the Responses to Positive Affect questionnaire? Personality and Individual Differences. 2016;89:40–46. doi: 10.1016/j.paid.2015.09.031. [DOI] [Google Scholar]
- Nolen-Hoeksema S. Responses to depression and their effects on the duration of depressive episodes. Journal of Abnormal Psychology. 1991;100:569–582. doi: 10.1037/0021-843X.100.4.569. [DOI] [PubMed] [Google Scholar]
- Pagliaccio D, Luby JL, Bogdan R, Agrawal A, Gaffrey MS, Belden AC, Barch DM. Stress-System Genes and Life Stress Predict Cortisol Levels and Amygdala and Hippocampal Volumes in Children. Neuropsychopharmacology. 2014;39(5):1245–1253. doi: 10.1038/npp.2013.327. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Quinn ME, Joormann J. Stress-Induced Changes in Executive Control Are Associated With Depression Symptoms: Examining the Role of Rumination. Clinical Psychological Science. 2015 doi: 10.1177/2167702614563930. [DOI] [Google Scholar]
- Raes F, Daems K, Feldman GC, Johnson SL, Van Gucht D. A psychometric evaluation of the Dutch version of the responses to positive affect questionnaire. Psychologica Belgica. 2009;49(4) doi: 10.5334/pb-49-4-293. [DOI] [Google Scholar]
- Raes F, Smets J, Nelis S, Schoofs H. Dampening of positive affect prospectively predicts depressive symptoms in non-clinical samples. Cognition & Emotion. 2012;26(1):75–82. doi: 10.1080/02699931.2011.555474. [DOI] [PubMed] [Google Scholar]
- Rood L, Roelofs J, Bögels SM, Nolen-Hoeksema S, Schouten E. The influence of emotion-focused rumination and distraction on depressive symptoms in non-clinical youth: A meta-analytic review. Clinical Psychology Review. 2009;29:607–616. doi: 10.1016/j.cpr.2009.07.001. [DOI] [PubMed] [Google Scholar]
- Schafer JL, Graham JW. Missing data: Our view of the state of the art. Psychological Methods. 2002;7(2):147–177. doi: 10.1037//1082-989x.7.2.147. [DOI] [PubMed] [Google Scholar]
- Vines L, Nixon RDV. Positive attributional style, life events and their effect on children’s mood: Prospective study. Australian Journal of Psychology. 2009;61(4):211–219. doi: 10.1080/00049530802579507. [DOI] [Google Scholar]
- Werner-Seidler A, Banks R, Dunn BD, Moulds ML. An investigation of the relationship between positive affect regulation and depression. Behaviour Research and Therapy. 2013;51(1):46–56. doi: 10.1016/j.brat.2012.11.001. [DOI] [PubMed] [Google Scholar]