

Abstract
Background:
Vitamin D which is involved in the maintenance of bone mineral homeostasis has been found to portray various pleiotropic effects. Although it has been widely accepted that serum 25-hydroxy Vitamin D level above 30 ng/ml is considered optimal for the biological actions of Vitamin D, there is a need to explore the levels of Vitamin D reported among Indians from various regions of the country. Hence, this systematic review aims to appraise the status of Vitamin D levels reported from apparently healthy Indians across various parts of India.
Methodology:
A comprehensive literature search was carried out to identify the range of Vitamin D levels among apparently healthy individuals from various parts of India, with the search term “Vitamin D and India” in the search portals of PubMed, Google Scholar, Indmed, and ScienceDirect. A total of 2998 articles were retrieved by the above search strategy, of which only forty studies fulfilled the criteria to be included in the systematic review. Studies done in various states were compiled under the respective zones based on the classification of Indian zones as specified in Zonal maps of India.
Results:
The level of Vitamin D from all the forty included studies ranged from 3.15 ± 1.4 to 52.9 ± 33.7 ng/ml. The effect size of Vitamin D level was higher in the South Zone compared to other zones.
Conclusion:
The present study shows that Vitamin D deficiency is prevalent among apparently healthy Indians living in different regions of India, irrespective of their exposure to sunlight.
Keywords: Indians, supplementation, Vitamin D
INTRODUCTION
Vitamin D, a prohormone, is synthesized primarily by the photolysis of 7-dehydrocholesterol present in human skin by ultraviolet B radiation of wavelength 290–320 nm from sunlight [Figure 1]. Cod-liver oil, meat, egg, milk products, and mushrooms contribute toward dietary sources of Vitamin D in a meager quantity.[1] Apart from playing a vital role in the maintenance of bone mineral homeostasis, Vitamin D has been found to portray pleiotropic effects as an anti-inflammatory, antiapoptotic, and antifibrotic agent. Further, it has been shown to play a major role in the regulation of cardiac, renal. and immune functions. Vitamin D deficiency has been found to be associated with increased risk for occurrence of diseases such as diabetes, schizophrenia, and malignancies.[2,3,4,5,6]
Figure 1.

Vitamin D biosynthesis from sunlight
Vitamin D status of an individual is assessed by the level of serum 25-hydroxy (25-OH) Vitamin D, one of the major circulating metabolites of Vitamin D. According to a study done by Hollis to evaluate the biological effects of Vitamin D on calcium homeostasis, serum 25-OH Vitamin D level above 32 ng/ml is required for maintenance of bone health.[7] Correspondingly, another study by Heaney has found that maximum calcium absorption in the gut is achieved above 30 ng/ml of serum 25-OH Vitamin D.[8] These findings suggest to serum 25-OH Vitamin D level above 30 ng/ml as optimal for the biological actions of Vitamin D in an individual.
Currently, Vitamin D status is categorized based on Endocrine society guidelines as deficiency, insufficiency, and sufficiency based on serum 25-OH Vitamin D levels below 20 ng/ml (50 nmol/L), 21–29 ng/ml (52.5–72.5 nmol/L), and 30–100 ng/ml (75–250 nmol/L), respectively.[9] Although this classification is accepted widely, extensive efforts are being taken to interpret the basis of this criteria as most of the global populations are found to be Vitamin D deficient.[10]
A recently conducted systematic review to appraise Vitamin D level from population across the continents found that nearly one-third of the studies from all over the world had Vitamin D level <20 ng/ml (50 nmol/L).[11] Surprisingly, in spite of being a country of abundant sunshine, the prevalence of Vitamin D deficiency in India has been found to be nearly 70%–90% across all age groups.[12,13,14,15] The average level of serum 25-OH Vitamin D level among Indians is strikingly lesser than the recommended criteria of 20 ng/ml as per the studies reported from various parts of India.[16,17,18] One of the reasons for this could be that the normal reference range for Vitamin D level in Indians may be less than the criteria suggested. With the gaining momentum on the significance of Vitamin D level in promoting health, there is a need to explore the levels of 25-OH Vitamin D reported among Indians from various regions of the country. Hence, this systematic review aims to appraise the status of Vitamin D levels reported from apparently healthy Indians across various parts of India.
METHODOLOGY
A comprehensive literature search was carried out to identify the range of Vitamin D levels among apparently healthy individuals from various parts of India, with the search term “Vitamin D and India” in the search portals of PubMed, Google Scholar, IndMed, and ScienceDirect. All original research articles of community or hospital-based research done on Vitamin D levels of apparently healthy Indians published till June 30, 2015, were included in this study. From the retrieved articles, studies done among patients, pediatric age group, pregnant women, and lactating mothers were excluded from the study. Similarly, studies carried out on Indians living in foreign countries, case reports, in-vitro and animal studies were also excluded from the study. A total of 2998 articles were retrieved by the above search strategy of which only forty studies fulfilled the criteria to be included in the systematic review [Figure 2]. Studies done in various states were compiled under the respective zones based on the classification of Indian zones as specified in Zonal maps of India [Table 1].[19]
Figure 2.
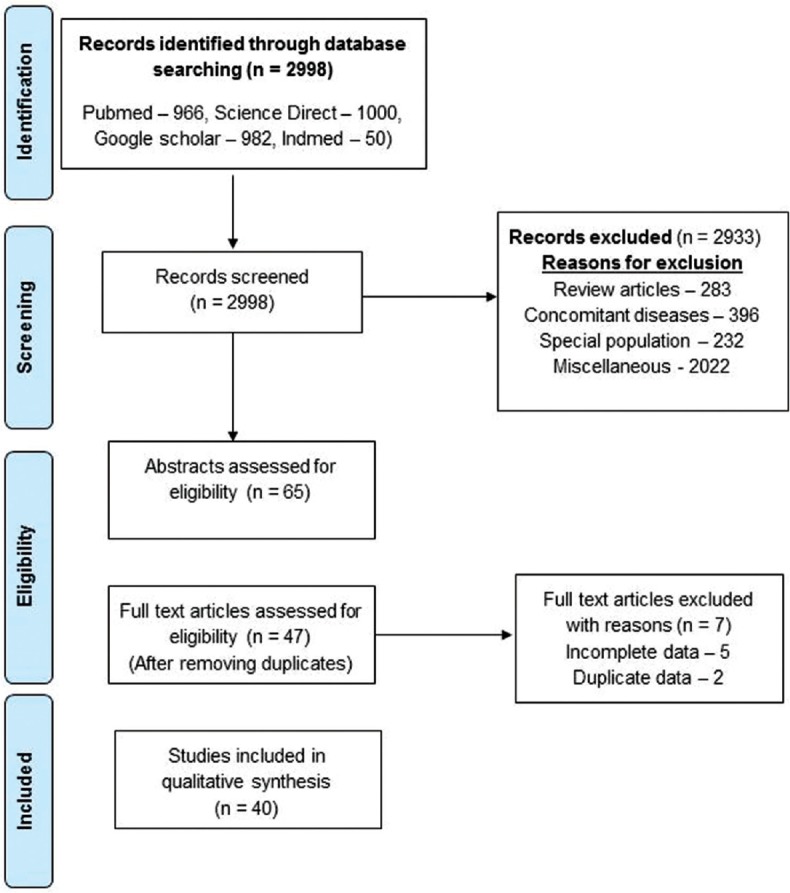
Flowchart describing the selection of studies for the systematic review
Table 1.
Various zones of India and the states included under them

RESULTS
A total of forty studies from all over India including North, East, West, and South Zones with a sample size of 19761 were analyzed. In all the forty studies, the criteria for Vitamin D deficiency were kept below 20 ng/ml. The age group of the participants from the studies included in the review ranged from 13 ± 3.1 to 65.8 ± 7.5 years. Among the various zones, North followed by South contributed majority of the studies. Out of forty studies, 24 studies were from North followed by nine studies from South Zone with less number of studies from East and West. Applying the criteria of our search strategy, we did not come across studies from North East and Central Zones [Table 2].
Table 2.
Baseline characteristics of apparently healthy individuals from various Vitamin D related studies done in India

The level of Vitamin D from all the forty included studies ranged from 3.15 ± 1.4 to 52.9 ± 33.7 ng/ml. The effect size of Vitamin D level was higher in the South Zone compared to other zones which were in almost in the same range of 12.3–14 ng/ml [Table 3]. Out of 40 studies included in the review, 14 (35%) studies had 25-OH Vitamin D level more than 20 ng/ml, of which one of the studies conducted in Chandigarh had Vitamin D level above 30 ng/ml. Majority of the North zone studies were from New Delhi followed by Lucknow and Chandigarh. Out of 24 studies done from North Zone, 22 studies had measured Vitamin D level using radioimmunoassay (RIA) while one study had used immunoassay the other one had used chemiluninescence assay. All the studies conducted from East Zone were only from Kolkata. The studies conducted from West Zone were from Mumbai and Pune. All the four studies from East Zone and three studies from West Zone had measured Vitamin D level using chemiluminescence and RIA methods, respectively. The South Zone studies were from Hyderabad, Tirupati, Vellore, and Nellore. Out of the ten studies done from South, seven studies had used RIA, two had used high-performance liquid chromatography, and one had used chemiluminescence to measure Vitamin D levels. One of the forty studies had samples taken from representatives of North, East, West, South, and Central zones and they had used RIA for the analysis of Vitamin D level [Table 2].
Table 3.
Overall effect size of Vitamin D from various parts of India

In random effect model, the effect size of Vitamin D level was found to higher in males compared to females as shown in Table 4. Similarly, the effect size of Vitamin D was found to be higher among middle-aged people compared to that of adolescents and those above 50 years of age. Those with normal body mass index (BMI) had a higher Vitamin D level compared to the population with higher BMI. People from rural areas had a higher Vitamin D level compared to those from urban areas. Vitamin D level was found to be higher during summer compared to that in winter [Table 4]. However, Vitamin D values except for summer and normal BMI were in the deficiency range of below 20 ng/ml. However, all these subgroups showed a larger difference in Vitamin D level in fixed-effect model compared to that of random-effect model [Figures 3 and 4].
Table 4.
Overall effect size of Vitamin D based on age, gender, BMI and socioeconomic status from various parts of India

Figure 3.
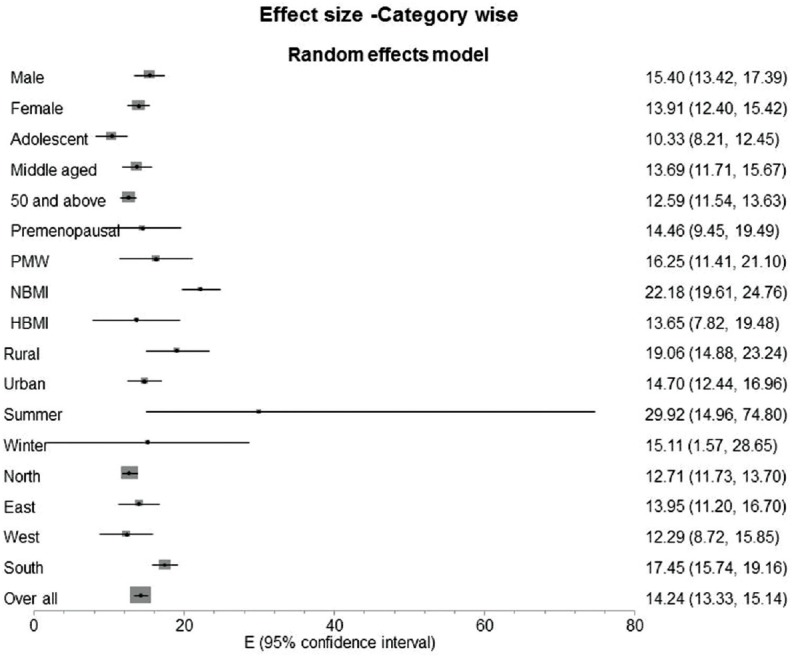
Effect size of Vitamin D using random-effects model
Figure 4.
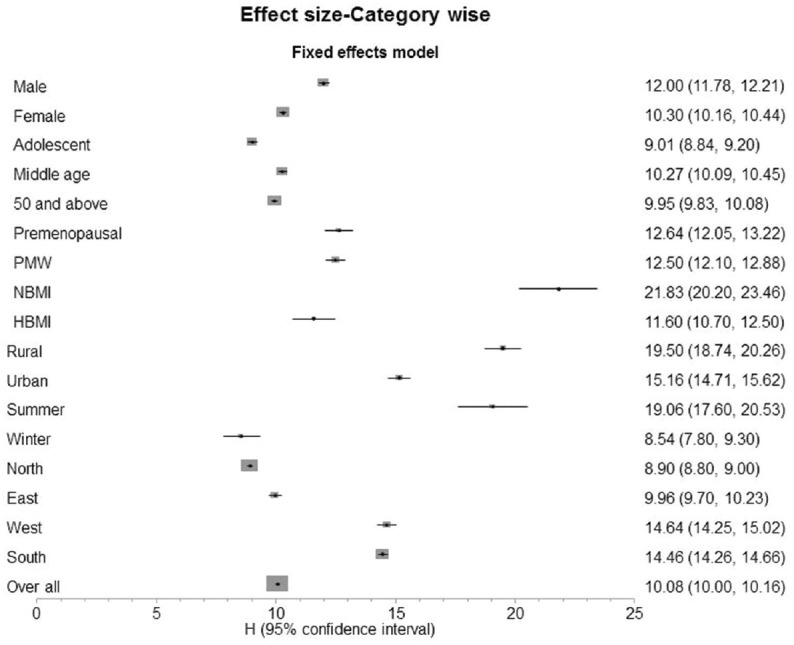
Effect size of Vitamin D using fixed-effects model
DISCUSSION
India, a nation of abundant sunshine, is surprisingly found to have massive burden of Vitamin D deficiency among the public irrespective of their locality.[13,14,20] Hence, we conducted a systematic review with the aim of evaluating the status of Vitamin D levels among apparently healthy population from various zones of India. Our study has shown the overall effect size of serum 25-OH Vitamin D level among Indians as 14.16 ng/ml (confidence interval [CI]: 13.27–15.05). This finding is similar to serum 25-OH Vitamin D concentration (14.35 ± 10.62 ng/ml [mean ± standard deviation [SD]) in a study conducted on apparently healthy middle-aged health-care professionals from various parts of India.[15] This review found a difference in the overall effect size of Vitamin D level among South Indians is (17.45 [15.74–19.16] ng/ml) compared to Indians from other parts of India which varied between 12.3 and 14 ng/ml. This could be attributed to more sunny weather in South India compared to other parts of India.
The review found that the mean effect size of serum 25-OH Vitamin D level is less in females (13.91, CI: 12.40–15.42) compared to males (15.40, CI: 13.42–17.39). This value is similar to a study done in healthy volunteers of Kashmir valley by Zargar et al. which showed that mean (SD) serum 25-OH Vitamin D level among females is 13.77 (11.05).[24] Similarly, a study done among school children in New Delhi found boys having significantly higher 25-OH Vitamin D levels compared to females (P = 0.004).[26] Another study done to evaluate mean serum 25-OH Vitamin D values among adolescent boys and girls belonging to the same family near Lucknow, found that serum 25-OH Vitamin D in boys (67.5 ± 29.0 nmol/L) was higher than that in their sisters (31.3 ± 13.5 nmol/L, P < 0.001) during winter. This difference of Vitamin D level in adolescent girls compared to boys has been attributed to reduced exposure to sunlight, less nutrition as well as early marriage and pregnancy among girls.[27] Similarly, a study done by Ramakrishnan et al., in urban college students from North India, found a significant difference of Vitamin D sufficiency in men (86.4%) compared to women (64.4%) (P = 0.001) in summer. However, this was attributed to the use of sunscreen among women students.[38]
The review found middle-aged people to have higher Vitamin D level (13.69 [11.71–15.67] ng/ml) compared to adolescents (10.33 [8.21–12.45] ng/ml) and those aged above 50 years (12.59 [11.54–13.63] ng/ml). This finding was similar to the concentration of serum 25-(OH) Vitamin D (14.35 ± 10.62 ng/mL [mean ± SD]) from a study conducted in apparently healthy middle-aged health-care professionals from various parts of India.[15] Likewise, a study done among people aged above 50 years in North India, has reported that nearly 91.2% of people in this age group are Vitamin D deficient with a mean 25-OH Vitamin D level of 9.72 ± 7.75 ng/ml and a median value of 8.21 (0.18–100.0) ng/ml. The reason for a higher value in our study among those aged above 50 years could be a result of compiled Vitamin D level across the people from all regions of India.[17] The finding of the review with respect to the value in adolescents is in concurrence to a study done among 760 apparently healthy school children of 10–18 years belonging to both lower and upper socioeconomic status in New Delhi, with an unadjusted mean serum 25-OH value of 11.8 ± 7.2 ng/ml. However in the same study, mean serum 25-OH value adjusted for lower (n = 430) and upper socioeconomic status (n = 330) was found to be 10.4 ± 0.4 and 13.7 ± 0.4 respectively (P < 0.01). The authors had concluded the reason for this significant difference among the children belonging to upper social strata could be attributed to their nutritional source of Vitamin D and calcium rich foods.[26] On the contrary, a study done in college students from Chandigarh did not find association between socioeconomic status and Vitamin D level (P = 0.55).[38] Likewise, another study done in 62 obese Asian Indian children and adolescent in the age group of 6–17 years found that all of them were Vitamin D deficient with a mean serum 25-(OH) Vitamin D level of 8.5 ± 4.2 ng/ml.[25] These results illustrate that socioeconomic status, as well as nutritional status, does not alter Vitamin D level among the adolescents.
In our study, effect size of 25-OH Vitamin D level among postmenopausal women was found to be 16.25 ng/ml (CI: 11.41–21.1 ng/ml). This was similar to the level of Vitamin D (14.6 ± 7 ng/ml) as per the study done on postmenopausal women of the age group of 50–67 years by Harinarayan.[53] Our finding is also similar to a study done on postmenopausal women (n = 150) aged 50 years and above from Tamil Nadu, with mean 25-OH Vitamin D level of 20.85 (8.63) ng/ml.[50] One of the major reasons quoted for reduced Vitamin D level in this group of population is reduced exposure to sunlight owing to more indoor confinement.
The study found a significant difference in Vitamin D level among people with normal BMI (22.18 [19.61–24.76] ng/ml) compared to those with high BMI (13.65 [7.82–19.48] ng/ml). Even nondiabetic obese urban Asian Indians with increased total abdominal fat were found to be associated with Vitamin D insufficiency.[16] The inverse relationship between weight and Vitamin D level is attributed to unavailability of Vitamin D owing to its accumulation with in fat compartments in overweight people.[54] Vitamin D level was found to be higher in rural population (19.06 [CI: 14.88–23.24] ng/ml) compared to urban population (CI: 14.70 [12.44–16.96] ng/ml). The decline in outdoor activity and effluence is considered to be a reason for Vitamin D deficiency among urban population.[55] A study done in a village from North India found that 70% of rural population has Vitamin D deficiency with mean serum 25-OH Vitamin D level of 36.4 ± 22.5 nmol/L. This value was found to be higher than the mean 25-OH Vitamin D level of 13.5 ± 3.0 nmol/L among urban population. This difference was attributed to longer duration of exposure to sunlight in rural population.[23] There was a significant variation in Vitamin D level measured among studies conducted during summer (29.92 [−14.96–74.80] ng/ml) compared to the studies done in winter (15.11 [1.57–28.65] ng/ml) [Table 4]. Following administration of Vitamin D supplementation in a study done on apparently healthy Indian women with Vitamin D deficiency, the increase in mean serum 25-OH Vitamin D level was found to be higher during summer compared to that of winter.[20] Similarly, a study done in rural area of North India showed a significant difference (P < 0·001) in 25-OH Vitamin D level in girls and women during summer (55·5 ± 19·8 nmol/L, mean ± SD) compared to that of (winter 27·3 ± 12·3 nmol/L, mean ± SD).[27] Further, a study done in Chandigarh on college students showed the mean ± SD of 25-OH Vitamin D level during summer was 52.9 ± 33.7 ng/ml, with a median value of 48 ng/ml while the same in winter was 31.8 ± 21.1 ng/ml, with a median value of 30 ng/ml (P<.001). In the same study after excluding the subjects with features of healed rickets, the mean 25-OH Vitamin D level was found to be 55.0 ± 33.9 ng/ml and 31.8 ± 20.7 ng/ml at the end of summer as well as winter, respectively.[38]
CONCLUSION
The present study shows that Vitamin D deficiency is prevalent among apparently healthy Indians living in different regions of India, irrespective of their exposure to sunlight as per the current Institute of Medicine (IOM) recommendation of normal Vitamin D level. The deficiency is commonly seen among the Indians regardless of age, gender, menopausal status, residing in rural, or urban areas.
The primary source of Vitamin D being sunlight, it was assumed for a long time that a country like India with ample sunshine exposure all through the year will be devoid of Vitamin D deficiency. Conversely, studies done in Indian population was found to be portraying a diverse scenario.[13,14] One of the reasons for Vitamin D deficiency among Indians is ascribed to decreased synthesis of Vitamin D as a consequence of darker skin, use of sunscreen, indoor lifestyle, reduced intake of dietary products rich in Vitamin D, etc.[32] Hence, it is being suggested that Vitamin D supplementation has to be used widely among Indians to treat Vitamin D deficiency. It is also suggested to create awareness among the population regarding the prevalence of Vitamin D deficiency and the measures to be taken to avoid it by increasing exposure to sunlight, intake of Vitamin D rich diet as well as Vitamin D supplementation if required. Suggestions are given regarding fortification of food with Vitamin D through national healthcare programs.[56,57] However, before carrying out such programs, the effects of Vitamin D overdose resulting in hypercalcemia, calcium stones, metastatic calcification, etc., should be taken into consideration.[57] Studies recommend that serum 25-OH Vitamin D levels should be interpreted along with serum PTH levels. This is because Vitamin D deficient subjects with normal PTH levels are found to exhibit either no or less adverse effects on bone health. A study done in adolescents and adults to evaluate the relationship between serum 25-OH Vitamin D, PTH, and bone mineral density in Indians has suggested that possibly the increased serum PTH level determines bone health irrespective of serum 25-OH Vitamin D.[40] Recently, it has been reported that IOM reference values for Vitamin D normal level needs to be interpreted in an appropriate manner and Vitamin D deficiency need not be considered as a pandemic. It is also stated that unnecessary screening procedure, as well as Vitamin D supplementation, needs to be evaded.[10] The continuing deliberations have raised the concerns regarding the normal cutoff value of Vitamin D level as well as the need for Vitamin D supplementation in Indian population. Further, studies are needed to establish the normal value for serum 25-OH Vitamin D level in Indian population.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- 1.Jäpelt RB, Jakobsen J. Vitamin D in plants: A review of occurrence, analysis, and biosynthesis. Front Plant Sci. 2013;4:136. doi: 10.3389/fpls.2013.00136. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Shivakumar V, Kalmady SV, Amaresha AC, Jose D, Narayanaswamy JC, Agarwal SM, et al. Serum Vitamin D and hippocampal gray matter volume in schizophrenia. Psychiatry Res. 2015;233:175–9. doi: 10.1016/j.pscychresns.2015.06.006. [DOI] [PubMed] [Google Scholar]
- 3.McDonnell SL, Baggerly LL, French CB, Heaney RP, Gorham ED, Holick MF, et al. Incidence rate of type 2 diabetes is >50% lower in GrassrootsHealth cohort with median serum 25-hydroxyvitamin D of 41 ng/ml than in NHANES cohort with median of 22 ng/ml. J Steroid Biochem Mol Biol. 2016;155(Pt B):239–44. doi: 10.1016/j.jsbmb.2015.06.013. [DOI] [PubMed] [Google Scholar]
- 4.Zhu B, Zhu B, Xiao C, Zheng Z. Vitamin D deficiency is associated with the severity of COPD: A systematic review and meta-analysis. Int J Chron Obstruct Pulmon Dis. 2015;10:1907–16. doi: 10.2147/COPD.S89763. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Shui IM, Mucci LA, Kraft P, Tamimi RM, Lindstrom S, Penney KL, et al. Vitamin D-related genetic variation, plasma Vitamin D, and risk of lethal prostate cancer: A prospective nested case-control study. J Natl Cancer Inst. 2012;104:690–9. doi: 10.1093/jnci/djs189. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Lai YH, Fang TC. The pleiotropic effect of Vitamin D. ISRN Nephrol 2013. 2013:898125. doi: 10.5402/2013/898125. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Hollis BW. Circulating 25-hydroxyvitamin D levels indicative of Vitamin D sufficiency: Implications for establishing a new effective dietary intake recommendation for Vitamin D. J Nutr. 2005;135:317–22. doi: 10.1093/jn/135.2.317. [DOI] [PubMed] [Google Scholar]
- 8.Heaney RP. Vitamin D depletion and effective calcium absorption. J Bone Miner Res. 2003;18:1342. doi: 10.1359/jbmr.2003.18.7.1342. [DOI] [PubMed] [Google Scholar]
- 9.Holick MF, Binkley NC, Bischoff-Ferrari HA, Gordon CM, Hanley DA, Heaney RP, et al. Evaluation, treatment, and prevention of Vitamin D deficiency: An Endocrine Society clinical practice guideline. J Clin Endocrinol Metab. 2011;96:1911–30. doi: 10.1210/jc.2011-0385. [DOI] [PubMed] [Google Scholar]
- 10.Manson JE, Brannon PM, Rosen CJ, Taylor CL. Vitamin D deficiency – Is there really a pandemic? N Engl J Med. 2016;375:1817–20. doi: 10.1056/NEJMp1608005. [DOI] [PubMed] [Google Scholar]
- 11.Hilger J, Friedel A, Herr R, Rausch T, Roos F, Wahl DA, et al. Asystematic review of Vitamin D status in populations worldwide. Br J Nutr. 2014;111:23–45. doi: 10.1017/S0007114513001840. [DOI] [PubMed] [Google Scholar]
- 12.Harinarayan CV, Ramalakshmi T, Venkataprasad U. High prevalence of low dietary calcium and low Vitamin D status in healthy South Indians. Asia Pac J Clin Nutr. 2004;13:359–64. [PubMed] [Google Scholar]
- 13.Harinarayan CV, Ramalakshmi T, Prasad UV, Sudhakar D, Srinivasarao PV, Sarma KV, et al. High prevalence of low dietary calcium, high phytate consumption, and Vitamin D deficiency in healthy South Indians. Am J Clin Nutr. 2007;85:1062–7. doi: 10.1093/ajcn/85.4.1062. [DOI] [PubMed] [Google Scholar]
- 14.Shivane VK, Sarathi V, Bandgar T, Menon P, Shah NS. High prevalence of hypovitaminosis D in young healthy adults from the Western part of India. Postgrad Med J. 2011;87:514–8. doi: 10.1136/pgmj.2010.113092. [DOI] [PubMed] [Google Scholar]
- 15.Beloyartseva M, Mithal A, Kaur P, Kalra S, Baruah MP, Mukhopadhyay S, et al. Widespread Vitamin D deficiency among Indian health care professionals. Arch Osteoporos. 2012;7:187–92. doi: 10.1007/s11657-012-0096-x. [DOI] [PubMed] [Google Scholar]
- 16.Bhatt SP, Misra A, Sharma M, Guleria R, Pandey RM, Luthra K, et al. Vitamin D insufficiency is associated with abdominal obesity in urban Asian Indians without diabetes in North India. Diabetes Technol Ther. 2014;16:392–7. doi: 10.1089/dia.2013.0303. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Marwaha RK, Tandon N, Garg MK, Kanwar R, Narang A, Sastry A, et al. Vitamin D status in healthy Indians aged 50 years and above. J Assoc Physicians India. 2011;59:706–9. [PubMed] [Google Scholar]
- 18.Harinarayan CV, Sachan A, Reddy PA, Satish KM, Prasad UV, Srivani P. Vitamin D status and bone mineral density in women of reproductive and postmenopausal age groups: A cross-sectional study from South India. J Assoc Physicians India. 2011;59:698–704. [PubMed] [Google Scholar]
- 19.Zonal Maps of India|India Zonal Map. [Last cited on 2016 May 10]. Available from: http://www.mapsofindia.com/zonal/
- 20.Malhotra N, Mithal A, Gupta S, Shukla M, Godbole M. Effect of Vitamin D supplementation on bone health parameters of healthy young Indian women. Arch Osteoporos. 2009;4:47–53. doi: 10.1007/s11657-009-0026-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Vupputuri MR, Goswami R, Gupta N, Ray D, Tandon N, Kumar N. Prevalence and functional significance of 25-hydroxyvitamin D deficiency and Vitamin D receptor gene polymorphisms in Asian Indians. Am J Clin Nutr. 2006;83:1411–9. doi: 10.1093/ajcn/83.6.1411. [DOI] [PubMed] [Google Scholar]
- 22.Goswami R, Gupta N, Goswami D, Marwaha RK, Tandon N, Kochupillai N. Prevalence and significance of low 25-hydroxyvitamin D concentrations in healthy subjects in Delhi. Am J Clin Nutr. 2000;72:472–5. doi: 10.1093/ajcn/72.2.472. [DOI] [PubMed] [Google Scholar]
- 23.Goswami R, Kochupillai N, Gupta N, Goswami D, Singh N, Dudha A. Presence of 25(OH) D deficiency in a rural North Indian village despite abundant sunshine. J Assoc Physicians India. 2008;56:755–7. [PubMed] [Google Scholar]
- 24.Zargar AH, Ahmad S, Masoodi SR, Wani AI, Bashir MI, Laway BA, et al. Vitamin D status in apparently healthy adults in Kashmir Valley of Indian subcontinent. Postgrad Med J. 2007;83:713–6. doi: 10.1136/pgmj.2007.059113. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Khadgawat R, Thomas T, Gahlot M, Tandon N, Tangpricha V, Khandelwal D, et al. The effect of puberty on interaction between Vitamin D status and insulin resistance in obese Asian-Indian children. Int J Endocrinol 2012. 2012:173581. doi: 10.1155/2012/173581. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Marwaha RK, Tandon N, Reddy DR, Aggarwal R, Singh R, Sawhney RC, et al. Vitamin D and bone mineral density status of healthy schoolchildren in Northern India. Am J Clin Nutr. 2005;82:477–82. doi: 10.1093/ajcn.82.2.477. [DOI] [PubMed] [Google Scholar]
- 27.Sahu M, Bhatia V, Aggarwal A, Rawat V, Saxena P, Pandey A, et al. Vitamin D deficiency in rural girls and pregnant women despite abundant sunshine in Northern India. Clin Endocrinol (Oxf) 2009;70:680–4. doi: 10.1111/j.1365-2265.2008.03360.x. [DOI] [PubMed] [Google Scholar]
- 28.Goswami R, Marwaha RK, Gupta N, Tandon N, Sreenivas V, Tomar N, et al. Prevalence of vitamin D deficiency and its relationship with thyroid autoimmunity in Asian Indians: A community-based survey. Br J Nutr. 2009;102:382–6. doi: 10.1017/S0007114509220824. [DOI] [PubMed] [Google Scholar]
- 29.Tandon N, Marwaha RK, Kalra S, Gupta N, Dudha A, Kochupillai N. Bone mineral parameters in healthy young Indian adults with optimal Vitamin D availability. Natl Med J India. 2003;16:298–302. [PubMed] [Google Scholar]
- 30.Agarwal N, Mithal A, Dhingra V, Kaur P, Godbole MM, Shukla M. Effect of two different doses of oral cholecalciferol supplementation on serum 25-hydroxy-vitamin D levels in healthy Indian postmenopausal women: A randomized controlled trial. Indian J Endocrinol Metab. 2013;17:883–9. doi: 10.4103/2230-8210.117237. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Agarwal N, Mithal A, Kaur P, Dhingra V, Godbole MM, Shukla M. Vitamin D and insulin resistance in postmenopausal Indian women. Indian J Endocrinol Metab. 2014;18:89–93. doi: 10.4103/2230-8210.126583. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Gupta A, Prabhakar S, Modi M, Bhadada SK, Lal V, Khurana D. Vitamin D status and risk of ischemic stroke in North Indian patients. Indian J Endocrinol Metab. 2014;18:721–5. doi: 10.4103/2230-8210.139241. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Garg MK, Marwaha RK, Tandon N, Bhadra K, Mahalle N. Relationship of lipid parameters with bone mineral density in Indian population. Indian J Endocrinol Metab. 2014;18:325–32. doi: 10.4103/2230-8210.131165. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Tandon VR, Sharma S, Mahajan S, Raina K, Mahajan A, Khajuria V, et al. Prevalence of vitamin d deficiency among Indian menopausal women and its correlation with diabetes: A first Indian cross sectional data. J Midlife Health. 2014;5:121–5. doi: 10.4103/0976-7800.141188. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Marwaha RK, Tandon N, Shivaprasad C, Kanwar R, Mani K, Aggarwal R, et al. Peak bone mineral density of physically active healthy Indian men with adequate nutrition and no known current constraints to bone mineralization. J Clin Densitom. 2009;12:314–21. doi: 10.1016/j.jocd.2009.05.004. [DOI] [PubMed] [Google Scholar]
- 36.Priyambada L, Bhatia V, Singh N, Bhatia E. Serum 25 hydroxyvitamin D profile after single large oral doses of cholecalciferol (Vitamin D3) in medical staff in North India: A pilot study. J Postgrad Med. 2014;60:52–6. doi: 10.4103/0022-3859.128812. [DOI] [PubMed] [Google Scholar]
- 37.Arya V, Bhambri R, Godbole MM, Mithal A. Vitamin D status and its relationship with bone mineral density in healthy Asian Indians. Osteoporos Int. 2004;15:56–61. doi: 10.1007/s00198-003-1491-3. [DOI] [PubMed] [Google Scholar]
- 38.Ramakrishnan S, Bhansali A, Bhadada SK, Sharma R, Walia R, Ravikiran M, et al. Vitamin D status and its seasonal variability in healthy young adults in an Asian Indian urban population. Endocr Pract. 2011;17:185–91. doi: 10.4158/EP10155.OR. [DOI] [PubMed] [Google Scholar]
- 39.Nagpal J, Pande JN, Bhartia A. A double-blind, randomized, placebo-controlled trial of the short-term effect of Vitamin D3 supplementation on insulin sensitivity in apparently healthy, middle-aged, centrally obese men. Diabet Med. 2009;26:19–27. doi: 10.1111/j.1464-5491.2008.02636.x. [DOI] [PubMed] [Google Scholar]
- 40.Garg MK, Tandon N, Marwaha RK, Menon AS, Mahalle N. The relationship between serum 25-hydroxy vitamin D, parathormone and bone mineral density in Indian population. Clin Endocrinol (Oxf) 2014;80:41–6. doi: 10.1111/cen.12248. [DOI] [PubMed] [Google Scholar]
- 41.Baidya A, Chowdhury S, Mukhopadhyay S, Ghosh S. Profile of Vitamin D in a cohort of physicians and diabetologists in Kolkata. Indian J Endocrinol Metab. 2012;16(Suppl 2):S416–7. doi: 10.4103/2230-8210.104113. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Dutta D, Maisnam I, Shrivastava A, Sinha A, Ghosh S, Mukhopadhyay P, et al. Serum Vitamin-D predicts insulin resistance in individuals with prediabetes. Indian J Med Res. 2013;138:853–60. [PMC free article] [PubMed] [Google Scholar]
- 43.Maisnam I, Dutta D, Mukhopadhyay S, Chowdhury S. Lean mass is the strongest predictor of bone mineral content in type-2 diabetes and normal individuals: An Eastern India perspective. J Diabetes Metab Disord. 2014;13:90. doi: 10.1186/s40200-014-0090-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.Basu S, Gupta R, Mitra M, Ghosh A. Prevalence of vitamin d deficiency in a pediatric hospital of Eastern India. Indian J Clin Biochem. 2015;30:167–73. doi: 10.1007/s12291-014-0428-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45.Kadam N, Chiplonkar S, Khadilkar A, Divate U, Khadilkar V. Low bone mass in urban Indian women above 40 years of age: Prevalence and risk factors. Gynecol Endocrinol. 2010;26:909–17. doi: 10.3109/09513590.2010.487604. [DOI] [PubMed] [Google Scholar]
- 46.Multani SK, Sarathi V, Shivane V, Bandgar TR, Menon PS, Shah NS. Study of bone mineral density in resident doctors working at a teaching hospital. J Postgrad Med. 2010;56:65–70. doi: 10.4103/0022-3859.65272. [DOI] [PubMed] [Google Scholar]
- 47.Shivane VK, Sarathi V, Lila AR, Bandgar T, Joshi SR, Menon PS, et al. Peak bone mineral density and its determinants in an Asian Indian population. J Clin Densitom. 2012;15:152–8. doi: 10.1016/j.jocd.2011.12.007. [DOI] [PubMed] [Google Scholar]
- 48.Amarendra Reddy G, Kulkarni B, Shatrugna V, Thilak Ravindra Reddy P, Nagalla B, Ajeya Kumar P, et al. Bone mass of overweight affluent Indian youth and its sex-specific association with body composition. Arch Osteoporos. 2009;4:31–9. doi: 10.1007/s11657-009-0024-x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 49.Yasovanthi J, Venkata Karunakar K, Sri Manjari K, Pulla Reddy B, Ajeya Kumar P, Sesha Charyulu M, et al. Association of Vitamin D receptor gene polymorphisms with BMD and their effect on 1, 25-dihydroxy vitamin D3 levels in pre- and postmenopausal South Indian women from Andhra Pradesh. Clin Chim Acta. 2011;412:541–4. doi: 10.1016/j.cca.2010.11.035. [DOI] [PubMed] [Google Scholar]
- 50.Paul TV, Thomas N, Seshadri MS, Oommen R, Jose A, Mahendri NV. Prevalence of osteoporosis in ambulatory postmenopausal women from a semiurban region in Southern India: Relationship to calcium nutrition and Vitamin D status. Endocr Pract. 2008;14:665–71. doi: 10.4158/EP.14.6.665. [DOI] [PubMed] [Google Scholar]
- 51.Shetty S, Kapoor N, Naik D, Asha HS, Prabu S, Thomas N, et al. Osteoporosis in healthy South Indian males and the influence of life style factors and vitamin d status on bone mineral density. J Osteoporos 2014. 2014:723238. doi: 10.1155/2014/723238. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 52.Bachali S, Dasu K, Ramalingam K, Naidu JN. Vitamin d deficiency and insulin resistance in normal and type 2 diabetes subjects. Indian J Clin Biochem. 2013;28:74–8. doi: 10.1007/s12291-012-0239-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 53.Harinarayan CV. Prevalence of Vitamin D insufficiency in postmenopausal South Indian women. Osteoporos Int. 2005;16:397–402. doi: 10.1007/s00198-004-1703-5. [DOI] [PubMed] [Google Scholar]
- 54.Wortsman J, Matsuoka LY, Chen TC, Lu Z, Holick MF. Decreased bioavailability of Vitamin D in obesity. Am J Clin Nutr. 2000;72:690–3. doi: 10.1093/ajcn/72.3.690. [DOI] [PubMed] [Google Scholar]
- 55.Agarwal KS, Mughal MZ, Upadhyay P, Berry JL, Mawer EB, Puliyel JM. The impact of atmospheric pollution on Vitamin D status of infants and toddlers in Delhi, India. Arch Dis Child. 2002;87:111–3. doi: 10.1136/adc.87.2.111. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 56.Vieth R, Carter G. Difficulties with Vitamin D nutrition research: Objective targets of adequacy, and assays for 25-hydroxyvitamin D. Eur J Clin Nutr. 2001;55:221–2. doi: 10.1038/sj.ejcn.1601145. [DOI] [PubMed] [Google Scholar]
- 57.Lhamo Y, Chugh PK, Tripathi CD. Vitamin D supplements in the Indian market. Indian J Pharm Sci. 2016;78:41–7. doi: 10.4103/0250-474x.180248. [DOI] [PMC free article] [PubMed] [Google Scholar]