

Abstract
Objective:
A site-specific bone loading index was developed to predict post-menarcheal arm bone mass, geometry, areal density and non-bone lean mass using organized activity records.
Methods:
Two cohorts of post-menarcheal girls (A= 55, B= 48) met analysis inclusion criteria: 1) Whole body and non-dominant radius DXA scans +1.0 to +2.6 years post-menarche; 2) detailed, organized activity records available for 36 months prior to the focal DXA scan; 3) accompanying anthropometric data. DXA non-dominant arm and radius regions of interest (1/3, Ultradistal (UD)) were evaluated. An arm bone loading index (arm totBLI) was developed and refined to describe >50 activities. Separate regression analyses for Cohorts A&B tested explanatory value of arm totBLI for DXA outcomes, accounting for gynecological age, height and whole body non-bone lean mass.
Results:
In both cohorts, arm totBLI reflecting 3 years of peri-menarcheal activity exposure exhibited strong explanatory value for post-menarcheal radius and arm outcomes (squared semi-partial r =0.07-0.34, p<0.05), except Arm Area. For both cohorts and most outcomes, arm totBLI explained significant variance, even after adjusting for local muscle mass.
Conclusions:
In two independent cohorts, arm totBLI may consistently indicate osteogenic and sarcogenic properties of represented activities; additional research is necessary for further refinement and validation.
Keywords: Exercise, DXA, Bone-Muscle Interactions, Female, Puberty
Introduction
Quantification of human skeletal loading is challenging, particularly in pediatric studies and retrospective adult research evaluating activity-related adaptations in bone structure. Ideally, skeletal loading would be measured using gauges to observe stresses generated in the bone tissue during a variety of activities at variable frequencies, intensities and durations. However, use of stress gauges is highly invasive and therefore unsuitable for pediatric or long term human studies. Accelerometry provides an alternative method to quantify presumed skeletal stimulation generated via dynamic loading, but it can be unwieldy, with labor-intensive data analysis. Thus, most accelerometry studies evaluate “snapshots” of activity over short periods as a metric of long term exposure, which may not be an accurate reflection of habitual activity1. Furthermore, as accelerometric assessments reflect current movement patterns, their results do not necessarily reflect prior physical activity exposure. Accordingly, to quantify habitual physical activity exposure, researchers often rely upon physical activity records and questionnaires that are too general to account for site-specific skeletal loading.
To improve long term site-specific loading quantification, Dolan et al. developed a retrospective questionnaire to evaluate lifetime loading exposure for the hip and spine in premenopausal women2. Their research group quantified each activity in “Bone Loading Units”, defined as the sum of the load magnitude and load rate, with load rate weighted 3 times. Both the magnitude of loading forces and the rate of force application were scored between 1 (low) and 3 (high). Bone Loading Scores were generated from the Bone Loading Units. These scores incorporate frequency and duration of all activities, yielding cumulative and annual mean loading scores for recent annual mean lifetime activity exposure, as well as for specific periods (for example, elementary school or middle school). Working from the Bone Loading Units and Scores template, we applied a similar methodology to quantify site-specific loading at the non-dominant distal radius in existing data from our prospective, longitudinal DXA study of bone growth in relation to organized physical activity exposure.
The current analysis is unique, because in contrast to most pediatric activity studies, it specifically evaluates a non-dominant arm loading model in the context of multiple organized (structured) physical activities. This strategy differs from those of studies that evaluate the effects of a single activity on the arm (racquet sports, gymnastics, etc.). It also differs from lower extremity and spine loading models, as the spine and lower extremity are loaded by many activities of daily living (walking, standing), as well as most organized physical activities (soccer, baseball, dance, running, jumping, etc.). Because lower extremity loading is so commonplace, it is difficult to distinguish associations of one form of loading (focal activity or intervention) from those of another (daily living and other activities).
In contrast, the non-dominant arm is exposed to diverse patterns of use across various activities, summarized as follows. First, many activities do not specifically load the arms (e.g. running, dance, soccer). Second, some activities involve gripping to bear light loads (e.g. lacrosse, field hockey, baseball/softball, racquet sports), whereas others grip to bear heavy loads (e.g. weight-training, rowing, gymnastics). Third, some sports involve upper extremity impact loading (e.g. baseball/softball, racquet sports, hockey, boxing, gymnastics), whereas others do not (weight-training, rowing, etc.). Fourth, in most organized activities, the dominant arm is loaded preferentially (racquet sports, basketball, volleyball, golf, batting, etc.). Preferential use ranges from virtually 100% (racquet sports with single-handed backhand) to partial preference (lacrosse, basketball, hockey, etc.), to role-oriented use (softball/baseball: dominant arm throws and experiences the majority of batting loads (push vs. pull) and all throwing forces; non-dominant arm is impact-loaded by catching), to nearly symmetrical bilateral loading (rowing, weight-training, gymnastics, cycling). Thus, in terms of non-dominant arm loading, there is a broad spectrum of loading profiles for evaluation, culminating in the extreme loading model of artistic gymnastics. Artistic gymnastics loads both arms with the total body mass and extremely high impact forces, as well as gripping to bear the total body mass.
Our analyses specifically evaluate the distal radius for two main reasons. First, the distal radius is a major site of pediatric and adult fracture3. Second, the radius is the major load-bearing bone in the distal forearm4. If the distal radius can be loaded osteogenically and safely during growth and beyond, bone structure and strength may be optimized, reducing local fracture risk in adulthood. This idea is broadly supported by distal radius fragility fracture rates among male former elite athletes over the age of 50 years5. While the athletes’ fracture rates were higher during youth (presumably due to elevated competitive contact behavioral risk), over age 50, their fracture risk was lower than age-matched controls; risk reduction is important at advanced ages when fracture risk and impaired healing pose a greater threat to overall health and function5.
Thus, we developed and tested a novel sport-specific bone loading index for the non-dominant upper extremity in two independent samples of post-menarcheal girls. All included subjects had provided organized physical activity exposure records for 3 years prior to the focal DXA scan, for association of activity stimuli with musculoskeletal development between 2 years pre-menarche and 2.5 years post-menarche. This phase of physical maturation was chosen, because it is believed that girls accrue up to 40% of peak bone mass in the four years surrounding menarche6. We tested the hypothesis that an arm bone loading index (arm totBLI), specifically designed to quantify site-specific loading exposure, would predict DXA musculoskeletal outcomes 1 to 2.5 years post-menarche, setting the stage for adult status.
Data from two separate cohorts were evaluated in order to gauge consistency of the bone loading index’s predictive value across independently sampled groups (ie. as an indicator of validity and reproducibility). We hypothesized that arm totBLI would be a strong, significant predictor of post-menarcheal bone outcomes and arm non-bone lean mass, yielding similar explanatory value in both cohorts. We also hypothesized that arm totBLI would provide similar explanatory value to WBnbFFM and ARMnbFFM, reflecting the osteogenic effect of site-specific loading during the majority of peak bone accrual velocity, even after accounting for whole body and local muscle mass.
Methods
Subjects were drawn from existing cohorts of a longitudinal study of bone growth in relation to artistic gymnastics exposure7. See Figure 1 for details. Subjects had been recruited from local non-athletic clubs, athletic clubs, private schools and gymnastic training facilities, supplemented by parental contacts through the area hospital and medical school. The main distinction between the two cohorts was birth year range (Cohort A: 12/1985-1/1993; Cohort B: 5/1995 - 9/2004). Informed assent and parental consent were provided, and study protocols were approved by our local Institutional Review Board. Research was carried out in compliance with the Declaration of Helsinki. For inclusion in analyses, the following were required: 1) Whole body and non-dominant radius dual energy X-ray absorptiometry (DXA) scan data available at a gynecological age (years before/after menarche) between +1.0 and +2.6 years post-menarche; 2) detailed physical activity data available for at least 36 months prior to the focal DXA scan; 3) accompanying anthropometric data.
Figure 1.
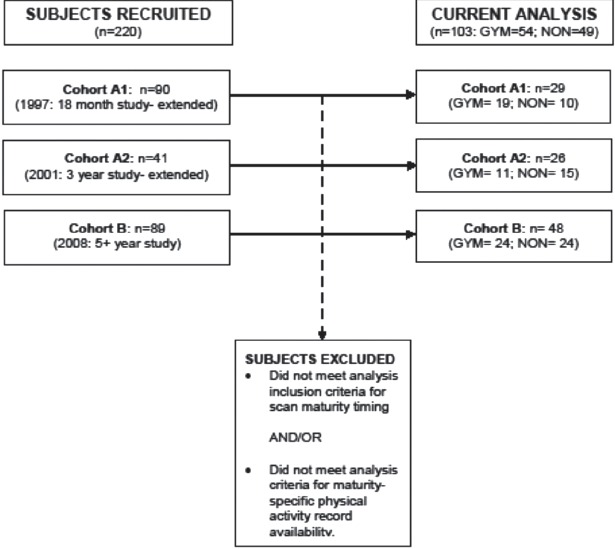
Recruitment and inclusion diagram.
Semi-annual measurement sessions yielded numerous data, including: 1) anthropometrics (e.g. height (cm), weight (kg), calculated body mass index (BMI, kg/m2)); 2) questionnaire-based records of menarche status and date of menarche; 3) calendar-based records of organized (structured) physical activity participation, listing activity-specific exposure in hours per week and accounting for time out of training >1 week (vacation, illness, injury). Free play was not evaluated due to concerns about accuracy of recall; the scheduled nature of structured/organized activities is preferred as an indicator of “routine” loading, from which deviations due to injury/illness are notable.
Whole body and non-dominant forearm DXA scans were performed, contemporaneous with the focal semi-annual measurement session, to yield bone projected area (cm2), bone mineral content (BMC, g) and areal bone mineral density (aBMD, g/cm2) for the non-dominant arm (whole body scan sub-region) and distal radius (1/3 and ultradistal forearm scan sub-regions). Whole body non-bone lean mass and arm non-bone lean mass were also evaluated (nbFFM: g, converted to kg for statistical analysis), with whole body percent fat evaluated as a subject characteristic. Cohort A scans were performed using a QDR4500W DXA scanner; Cohort B scans were performed using a cross-calibrated Discovery A scanner (Hologic, Waltham MA). Despite DXA scans occurring over dates spanning a 15 year period (2001 to 2015), more than 90% of DXA scans were performed by one of two long term staff DXA technologists using the same protocols. All scans were analyzed by the same investigator, using Apex software version 12.7.3.
As described elsewhere, DXA scan regions of interest were positioned to yield radius-specific outcomes (Hologic Discovery A Software v.12.7). The distal border of the DXA analysis box was placed distal to the ulnar side of the radial articular surface, ensuring congruent and consistent positioning, regardless of ulnar variance and physical maturity, as is appropriate for radius-specific growth studies (8, 9). Both ultradistal (UD, metaphyseal) and 1/3 (diaphyseal) regions of interest were evaluated.
In a sample of adult women, coefficients of variation were determined to be ≤1.3% for all radius outcomes (n=30) and <2.9% for all whole body outcomes (n=29), as scanned by the aforementioned pair of DXA technologists, using the Discovery A scanner. To evaluate inter-scanner variability, same-day “duplicate” scans were performed on the QDR 4500W and Discovery A scanners in approximately 130 female subjects aged 8 to 25 years old. These results demonstrated excellent agreement (Bland-Altman plots) but indicated sharper bone edge detection by the Discovery A scanner, as expected based on hardware improvements made between models [ASBMR abstract], with the exception of UD aBMD (virtually zero mean deviance, -0.0016 g/cm2). Despite scanner differences, coefficients of variation for QDR vs. Discovery A measurements were as follows: Radius outcomes RMSE CV ranged from 1.5% to 3.8%; Left arm non-bone lean mass RMSE was CV 7.5%; Total body non-bone lean mass RMSE CV was 1.9%. Regardless, inter-scanner discrepancies are minimally influential in the current analysis, because Cohort A regressions included only QDR scan results and Cohort B regressions included only Discovery A scan results.
Theory: basis for bone loading index formula
Bone loading scores were initially generated using activity records for the included subset of Cohort A (n=55), by a “committee” of exercise researchers and medical professionals. This committee included specialists in exercise science, orthopedic surgery, sports medicine and pediatric emergency medicine (JND, CAS, TAS, AOB, NMG). After additional data were collected for Cohort B, bone loading scores were expanded to accommodate these new physical activity records and the full range of prior activity records, with further refinement by exercise science specialists (JND, KAD). Subsequently, the revised algorithm (Table 1) and full range of activity-specific scores (Appendix 1) were reviewed and approved by the original committee members (TAS, CAS, AOB, NMG).
Table 1.
Non-dominant arm bone loading index: parameter descriptions.
| Factor | Level 0 | Level 1 | Level 2 | Level 3 | Level 4 | Level 5 |
|---|---|---|---|---|---|---|
| Magnitude | No gripping, no tension, no force generation, no added weight | Tension and/or force generation, but no additional weight besides arm | Gripping and/or bearing of very light mass such as ball or Frisbee | Gripping and/or bearing of moderate mass or small mass with use of a lever | Heavy mass is borne, such as partial body weight | Total body mass or greater is borne |
| Velocity | No load is borne beyond arm mass; no gripping | Static load application (isometric) or just arm pumping | Dynamic, loading but non-impact | Low impact | Blunted impact with elastic surface (e.g. racquet, lacrosse stick, basketball) | High impact against inelastic surface (e.g. bat, hard ball, ground) |
| Factor | Level 1 | Level 2 | Level 3 | Level 4 | Level 5 | Level 6 |
|---|---|---|---|---|---|---|
| Frequency | No gripping, no tension, no force generation,no added weight | Static loading | Infrequent loading | Intermittent loading with long rests | Intermittent loading with short rests | Nearly loading continuous |
| Non-dominance: 33% (primarily dominant arm loading), 66% (partial bilateral), 100% (bilateral). In dominant arm studies, the 33% and 66% factors should be modified accordingly. | ||||||
| armBLI=Σ [(Magnitude + Velocity) × Frequency × Training Exposure × Non-dominance]. | ||||||
Appendix 1.
Arm bone loading index factors and values for reported physical activities. (Based on 1-17 years of longitudinal records, age 7 to 29 years) (continuous on the next page).
| PHYSICAL ACTIVITY | Magnitude | Velocity | Frequency | Dom | BLI |
|---|---|---|---|---|---|
| Acrobatics | 5 | 5 | 3 | 1 | 30.0 |
| Archery | 4 | 1 | 4 | 1 | 20.0 |
| Badminton | 2 | 4 | 5 | 0.33 | 9.9 |
| Basketball | 2 | 4 | 4 | 0.66 | 15.8 |
| Batting | 3 | 5 | 5 | 0.66 | 26.4 |
| Biking (mountain) | 3 | 4 | 5 | 1 | 35.0 |
| Biking (road) | 3 | 4 | 2 | 1 | 14.0 |
| Biking (stationary) | 3 | 1 | 1 | 1 | 4.0 |
| Boxing (impact: targets, opponents) | 4 | 5 | 5 | 1 | 45.0 |
| Calisthenics | 4 | 2 | 4 | 1 | 24.0 |
| Cardio-kickboxing (no impact) | 1 | 1 | 5 | 1 | 10.0 |
| Cardio: Ski Machine (nordic-trac, gazelle, arc trainer) | 3 | 2 | 6 | 1 | 30.0 |
| Cheerleading (with tumbling) | 5 | 5 | 3 | 1 | 30.0 |
| Cheerleading (no tumbling) | 1 | 4 | 4 | 1 | 20.0 |
| Circuit training | 4 | 3 | 4 | 1 | 28.0 |
| Color Guard | 3 | 3 | 5 | 0.66 | 19.8 |
| Core strengthening | 4 | 1 | 2 | 1 | 10.0 |
| Dance/Aerobics | 1 | 1 | 3 | 1 | 6.0 |
| Discus/Shotput | 3 | 2 | 4 | 0.33 | 6.6 |
| Diving | 1 | 1 | 3 | 1 | 6.0 |
| Dry Land (diving cross-training) | 4 | 2 | 5 | 1 | 30.0 |
| Elliptical | 3 | 2 | 6 | 1 | 30.0 |
| Field Hockey | 3 | 5 | 4 | 0.66 | 21.1 |
| Figure skating | 1 | 1 | 3 | 1 | 6.0 |
| Golf | 3 | 5 | 3 | 0.66 | 15.8 |
| Gymnastics | 5 | 5 | 4 | 1 | 40.0 |
| Gymnastics bars only | 5 | 3 | 4 | 1 | 32.0 |
| Gymnastics bars and beam only | 5 | 3 | 4 | 1 | 32.0 |
| Gymnastics bars and conditioning only | 5 | 3 | 4 | 1 | 32.0 |
| Gymnastics conditioning | 5 | 2 | 2 | 1 | 14.0 |
| Gymnastics Lower Extremity only | 1 | 1 | 0 | 1 | 0.0 |
| Gymnastics no bars | 5 | 5 | 4 | 1 | 40.0 |
| Gymnastics spotting | 3 | 2 | 3 | 0.66 | 9.9 |
| Hiking | 1 | 1 | 3 | 1 | 6.0 |
| Hockey (ice) | 3 | 5 | 4 | 0.66 | 21.1 |
| Horseback riding | 1 | 1 | 3 | 1 | 6.0 |
| Housework/Gardening (job) | 2 | 2 | 3 | 0.33 | 4.0 |
| Jacob's Ladder | 3 | 3 | 6 | 1 | 36.0 |
| Karate | 4 | 5 | 4 | 1 | 36.0 |
| Kayaking | 4 | 2 | 6 | 1 | 36.0 |
| Kickball | 1 | 3 | 1 | 0.66 | 2.6 |
| Kickboxing | 4 | 5 | 5 | 1 | 45.0 |
| Lacrosse | 3 | 4 | 4 | 0.66 | 18.5 |
| Marching Band | 2 | 1 | 2 | 0.66 | 4.0 |
| Marching Band (drums) | 2 | 5 | 5 | 1 | 35.0 |
| Mountain climbing | 1 | 1 | 3 | 1 | 6.0 |
| Mowing lawns (job) | 3 | 1 | 2 | 1 | 8.0 |
| Physical Therapy: Core | 4 | 1 | 2 | 1 | 10.0 |
| Physical Therapy: Lower Extremity | 0 | 0 | 0 | 1 | 0.0 |
| Physical Therapy: Upper Extremity | 3 | 2 | 4 | 1 | 20.0 |
| Pilates | 4 | 1 | 2 | 1 | 10.0 |
| Pitching | 2 | 2 | 5 | 0.33 | 6.6 |
| Plyometrics | 3 | 3 | 3 | 1 | 18.0 |
| Plyometrics (Lower Extremity only) | 0 | 0 | 0 | 1 | 0.0 |
| Powerlifting | 5 | 2 | 5 | 1 | 35.0 |
| Racquetball | 3 | 4 | 5 | 0.33 | 11.6 |
| Referee (soccer, basketball, field hockey, lacrosse) | 0 | 0 | 0 | 1 | 0.0 |
| Rock climbing | 4 | 1 | 6 | 1 | 30.0 |
| Rowing (boats, ergometer) | 4 | 2 | 6 | 1 | 36.0 |
| Running Sprints | 1 | 1 | 5 | 1 | 10.0 |
| Running XC (long distance) | 0 | 0 | 6 | 1 | 0.0 |
| Running Treadmill Sprints | 1 | 1 | 5 | 1 | 10.0 |
| Running Treadmill Long Distance | 0 | 0 | 6 | 1 | 0.0 |
| Shoveling | 3 | 3 | 6 | 0.66 | 23.8 |
| Skating (roller, ice, roller-blading) | 1 | 1 | 3 | 1 | 6.0 |
| Skiing, cross-country | 3 | 3 | 6 | 1 | 36.0 |
| Skiing, downhill | 2 | 1 | 3 | 1 | 9.0 |
| Snowboarding | 0 | 1 | 1 | 1 | 1.0 |
| Soccer | 1 | 1 | 3 | 1 | 6.0 |
| Softball/Baseball | 3 | 5 | 4 | 0.66 | 21.1 |
| Squash | 3 | 4 | 5 | 0.33 | 11.6 |
| Stairmaster (stair climbing) | 3 | 1 | 2 | 1 | 8.0 |
| Stretching | 1 | 1 | 1 | 1 | 2.0 |
| Swimming | 4 | 2 | 6 | 1 | 36.0 |
| Tae Kwon Do | 4 | 5 | 4 | 1 | 36.0 |
| Tennis | 3 | 4 | 5 | 0.33 | 11.6 |
| Track (indoor, unspecified) | 1 | 1 | 1 | 1 | 2.0 |
| Track (outdoor, unspecified) | 1 | 1 | 3 | 1 | 6.0 |
| Track and Field (jumping) | 1 | 1 | 3 | 1 | 6.0 |
| Track and Field (throwing) | 3 | 2 | 4 | 0.33 | 6.6 |
| Track and Field (long distance) | 0 | 0 | 1 | 1 | 0.0 |
| Trampoline | 1 | 1 | 3 | 1 | 6.0 |
| Tumbling | 5 | 5 | 4 | 1 | 40.0 |
| Ultimate Frisbee | 2 | 3 | 4 | 0.33 | 6.6 |
| Volleyball | 2 | 4 | 4 | 0.66 | 15.8 |
| Walking intervals | 0 | 0 | 0 | 1 | 0.0 |
| Weight-training, heavy | 4 | 2 | 5 | 1 | 30.0 |
| Weight-training, light | 3 | 2 | 5 | 1 | 25.0 |
| Weight-training, moderate | 3 | 2 | 5 | 1 | 25.0 |
| Weight-training Lower Extremity only, heavy | 0 | 0 | 0 | 1 | 0.0 |
| Weight-training Lower Extremity only, light | 0 | 0 | 0 | 1 | 0.0 |
| Weight-training Lower Extremity only, moderate | 0 | 0 | 0 | 1 | 0.0 |
| Weight-training Upper Extremity only, heavy | 4 | 2 | 5 | 1 | 30.0 |
| Weight-training Upper Extremity only, light | 3 | 2 | 5 | 1 | 25.0 |
| Weight-training Upper Extremity only, moderate | 3 | 2 | 5 | 1 | 25.0 |
| Wrestling | 4 | 3 | 4 | 1 | 28.0 |
| Yoga (no inversions) | 3 | 2 | 3 | 1 | 15.0 |
| Yoga (with inversions) | 4 | 2 | 4 | 1 | 24.0 |
Thus, the resultant non-dominant arm bone loading indices (armBLI) were developed to describe and grade >50 organized activities. The activity data were generated via longitudinal records (up to 17 years per subject), based on semi-annual reports of organized physical activity (hours per week) from over 200 subjects, age 8 to 29 years old. Thus, they include records from all included subjects from Cohorts A & B. On this basis, it is a fairly representative set of structured physical activities in which U.S. girls participate. Our armBLI is a modification of the bone loading index originally published by Dolan at al.2. Activities were graded based on: loading magnitude (0-5), velocity (0-5) (called rate by Dolan et al.) and frequency (1-6), incorporating an additional factor to specify degree of non-dominant arm involvement (exposure= 33%, 66% or 100% relative to dominant arm) (Table 1).
Load magnitude scoring was developed to reflect the mass of the forearm load. We substituted the term loading velocity for loading “rate” to avoid confusion with loading frequency. Loading velocity scoring was intended to reflect loading dynamism (e.g. impact vs. non-impact). We have used the term loading frequency to distinguish levels of infrequent vs. frequent site-specific loading. Unlike the Dolan index, in our algorithm, all factors were weighted equally.
Unique to our formula, the concept of “non-dominance” is related to loading frequency. Although many of these activities would seem to generate considerable osteogenic stimuli, our region of interest is the non-dominant arm. Accordingly, activities that primarily load the dominant arm will not stimulate non-dominant arm osteogenesis directly. On this basis, we have used the concept of “non-dominance” to approximate the stimulus dose conferred routinely by each activity. For activities that primarily use the dominant arm, the total bone loading units are multiplied by 0.33, to reduce the loading dose (e.g. racquet sports). For activities that often use the non-dominant arm, but still load the dominant arm preferentially, the total bone loading units are multiplied by 0.66 (e.g. basketball, volleyball, lacrosse). For activities in which arms are loaded symmetrically, the total bone loading units are multiplied by a factor of 1.0 (e.g. gymnastics, weight-training, rowing, yoga). These conventions refer specifically to our study design which evaluates the non-dominant arm; other study designs would need to modify this factor accordingly.
For each organized activity, arm bone loading units were generated, as detailed in Table 1. Arm bone loading units are equal to loading velocity plus loading magnitude; that sum is then multiplied by loading frequency and the activity-specific non-dominance factor (Table 1, Appendix 1). For each girl, totBLI is equal to the sum of bone loading units, multiplied by sport-specific hours, for all activities over a specified time period (e.g. totBLI=(tennis armBLI x 36 months tennis hrs) + (soccer armBLI x 36 months soccer hrs) + …). Thus, in this analysis, we evaluated a 3-year peri-menarcheal bone loading index (totBLI), representing 36 months of activity records for each subject.
Statistical analysis
Normality of data distributions was evaluated. Means and standard deviations for subject characteristics are presented for the total sample, Cohort A and Cohort B. T-tests assessed differences between cohorts, with variables ln-transformed, as needed. Physical activity hours and totBLI group differences were evaluated using Mann Whitney U-tests since the non-normal distributions were not improved using ln-transformation. For regression analyses, dependent variables were ln-transformed as necessary to improve normality of distributions.
We examined the explanatory value of totBLI for non-dominant arm DXA outcomes, measured approximately 1 to 2.5 years post-menarche, using multiple regression analyses. To assess the consistency of totBLI explanatory value, we performed separate regression analyses for Cohorts A and B (Tables 4 & 5). We systematically entered gynecological age, height, non-bone lean mass (nbFFM: total body or arm, as specified) and arm totBLI as independent variables. DXA bone outcomes and arm non-bone lean mass (ARMnbFFM) were dependent variables. Whole body nbFFM (WBnbFFM: Table 4) and ARMnbFFM (Table 5) were specifically evaluated in two sets of models, to evaluate the influence of whole body and local muscle mass, as lean mass is well-established as strong predictor of skeletal properties10-12. Presentation of data for models with ARMnbFFM as the dependent variable differs slightly (Table 4, WBnbFFM excluded; Table 5, WBnbFFM entered). ARM and WB nbFFM were not included as independent variables in the same models, thus their collinearity is not an issue in these analyses.
Table 2a.
Subject characteristics and group differences: general.
| Variable | Total Sample (n= 103) | Cohort A (n=55) | Cohort B (n=48) | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Mean | s. d. | Min | Max | Mean | s. d. | Min | Max | Mean | s. d. | Min | Max | |
| Chronological Age (yrs) | 14.8 | 1.2 | 11.3 | 17.9 | 15.1b | 1.1 | 13.0 | 17.9 | 14.4 | 1.2 | 11.3 | 17.2 |
| Gynecological Age (yrs) | 1.8 | 0.4 | 0.9 | 2.6 | 2.0c | 0.4 | 1.0 | 2.6 | 1.7 | 0.4 | 0.9 | 2.6 |
| Age at Menarche (yrs) | 12.9 | 1.1 | 9.5 | 15.8 | 13.1a | 1.1 | 11.1 | 15.8 | 12.7 | 1.2 | 9.5 | 15.3 |
| Height (cm) | 161.2 | 6.3 | 144.2 | 178.0 | 161.2 | 6.0 | 148.6 | 178.0 | 161.3 | 6.7 | 144.2 | 174.5 |
| Weight (kg) | 56.2 | 8.4 | 39.8 | 89.2 | 54.5 | 7.3 | 39.8 | 84.4 | 58.0a | 9.3 | 41.8 | 89.2 |
| Body Mass Index (kg/m2) | 21.6 | 2.7 | 15.6 | 30.9 | 21.0 | 2.6 | 15.6 | 30.9 | 22.2a | 2.8 | 17.6 | 30.5 |
| Whole Body Non-bone Lean | 39.9 | 4.8 | 28.7 | 55.3 | 38.9 | 4.1 | 28.7 | 51.8 | 41.0c | 5.3 | 31.0 | 55.3 |
| Mass (kg) | ||||||||||||
| Percent Body Fat (%) | 24.5 | 4.8 | 13.6 | 35.9 | 23.8 | 4.7 | 13.6 | 35.5 | 25.3 | 5.0 | 17.9 | 35.9 |
| 3 Year Mean Arm totBLI | 8.7 | 8.1 | 0.05 | 32.5 | 8.4 | 8.4 | 0.05 | 29.3 | 9.1 | 7.7 | 0.6 | 32.5 |
| 3 Year Physical Activity (h) | 1256.8 | 732.8 | 30.4 | 3299.6 | 1198.8 | 196.2 | 30.4 | 2972.0 | 1322.8 | 669.6 | 192.4 | 3299.6 |
| 3 Year Mean Physical | 9.5 | 9.2 | 0.2 | 86.3 | 8.3 | 5.5 | 0.2 | 20.6 | 9.2 | 4.7 | 1.3 | 22.9 |
| Activity (h/wk) | ||||||||||||
BLI= Bone Loading Index; T-test for all, except 3 Year BLI, PA, Mean PA (Mann-Whitney U); Bolded variables indicate significant cohort differences:
p<0.05;
p≤0.01;
p≤0.001.
Table 2b.
Subject characteristics and t-test results: non-dominant arm bone and lean mass dependent variables.
| Variable | Total Sample (n= 103) | Cohort A (n=55) | Cohort B (n=48) | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Mean | s. d. | Min | Max | Mean | s. d. | Min | Max | Mean | s. d. | Min | Max | |
| 1/3 Radius Area (cm2) | 2.59 | 0.25 | 2.05 | 3.24 | 2.54 | 0.26 | 2.05 | 3.18 | 2.64 | 0.23 | 2.13 | 3.24 |
| 1/3 Radius BMC (g) | 1.76 | 0.26 | 1.32 | 2.64 | 1.68 | 0.24 | 1.32 | 2.48 | 1.85b | 0.26 | 1.40 | 2.64 |
| 1/3 Radius aBMD (g/cm2) | 0.677 | 0.056 | 0.546 | 0.858 | 0.659 | 0.050 | 0.546 | 0.821 | 0.698c | 0.056 | 0.601 | 0.858 |
| UD Radius Area (cm2) | 3.26 | 0.30 | 2.64 | 4.05 | 3.21 | 0.27 | 2.68 | 3.87 | 3.32a | 0.32 | 2.64 | 4.05 |
| UD Radius BMC (g) | 1.43 | 0.30 | 0.81 | 2.44 | 1.38 | 0.30 | 0.81 | 2.14 | 1.49 | 0.29 | 1.08 | 2.44 |
| UD Radius aBMD (g/cm2) | 0.437 | 0.067 | 0.281 | 0.612 | 0.429 | 0.073 | 0.281 | 0.612 | 0.447 | 0.059 | 0.337 | 0.608 |
| Arm Area (cm2) | 174.53 | 24.12 | 126.04 | 239.14 | 163.74 | 19.97 | 126.04 | 234.51 | 186.90c | 22.63 | 150.45 | 239.14 |
| Arm BMC (g) | 131.55 | 27.21 | 86.82 | 237.59 | 118.88 | 20.62 | 86.82 | 179.31 | 146.07c | 26.73 | 108.63 | 237.59 |
| Arm aBMD (g/cm2) | 0.749 | 0.070 | 0.635 | 1.062 | 0.723 | 0.057 | 0.635 | 0.870 | 0.778c | 0.073 | 0.665 | 1.062 |
| Arm Non-bone Lean Mass (kg) | 1.98 | 0.37 | 1.36 | 3.72 | 1.83 | 0.26 | 1.36 | 2.43 | 2.15c | 0.40 | 1.52 | 3.72 |
UD= Ultradistal; Area= bone projected area; BMC= bone mineral content; aBMD= areal bone mineral density; Bolded variables indicate significant cohort differences:
p<0.05;
p≤0.01;
p≤0.001.
Table 3.
Number of participants and recorded hours in each activity, by cohort.
| Sport | BLI | Cohort A | Cohort B | ||
|---|---|---|---|---|---|
| n=55 | Hours | n=48 | Hours | ||
| Acrobatics | 30.0 | 1 | 7.6 | 0 | 0 |
| Archery | 20.0 | 0 | 0 | 1 | 16 |
| Basketball | 15.8 | 14 | 4676.4 | 8 | 2367.2 |
| Biking (stationary) | 4.0 | 1 | 70 | 1 | 8.8 |
| Calisthenics | 24.0 | 9 | 494.8 | 2 | 24 |
| Cardio-kickboxing (no impact) | 10.0 | 1 | 12 | 0 | 0 |
| Cheerleading (with tumbling) | 30.0 | 2 | 930 | 3 | 1040 |
| Cheerleading (no tumbling) | 20.0 | 1 | 2242 | 1 | 692 |
| Circuit training | 28.0 | 1 | 44 | 0 | 0 |
| Color Guard | 19.8 | 4 | 1304 | 1 | 96 |
| Dance/Aerobics | 6.0 | 21 | 4492 | 13 | 4254.8 |
| Discus/Shotput | 6.6 | 0 | 0 | 1 | 48 |
| Diving | 6.0 | 1 | 192 | 3 | 982 |
| Dry Land (diving cross-training) | 30.0 | 0 | 0 | 1 | 60 |
| Elliptical/Nordic-trac/Arc-trainer | 30.0 | 4 | 104.8 | 1 | 3.2 |
| Field Hockey | 21.1 | 1 | 264 | 1 | 190 |
| Figure skating | 6.0 | 2 | 132 | 3 | 694 |
| Golf | 15.8 | 1 | 24 | 1 | 12 |
| Gymnastics | 40.0 | 26 | 34062 | 27 | 34017 |
| Gymnastics (bars & beam) | 32.0 | 0 | 0 | 1 | 68 |
| Gymnastics (bars &conditioning) | 32.0 | 0 | 0 | 2 | 394 |
| Gymnastics (conditioning) | 14.0 | 0 | 0 | 5 | 244 |
| Gymnastics (Legs only) | 0.0 | 0 | 0 | 1 | 102 |
| Gymnastics (no bars) | 40.0 | 0 | 0 | 1 | 34 |
| Gymnastics spotting | 9.9 | 0 | 0 | 1 | 5 |
| Hiking | 6.0 | 1 | 160 | 0 | 0 |
| Hockey (ice) | 21.1 | 1 | 310 | 0 | 0 |
| Horseback riding | 6.0 | 2 | 856.4 | 1 | 10 |
| Karate | 36.0 | 0 | 0 | 2 | 174 |
| Kickboxing | 45.0 | 1 | 100 | 0 | 0 |
| Lacrosse | 18.5 | 14 | 2902.4 | 5 | 1152 |
| Marching Band | 4.0 | 4 | 1106 | 2 | 448.4 |
| Marching Band (drums) | 35.0 | 1 | 22.4 | 0 | 0 |
| Physical Therapy Legs only | 0.0 | 0 | 0 | 2 | 32 |
| Physical Therapy Arms only | 20.0 | 0 | 0 | 1 | 2 |
| Rowing (Crew, Ergometer) | 36.0 | 2 | 181.6 | 1 | 351.6 |
| Running Sprints | 10.0 | 0 | 0 | 1 | 15.2 |
| Running Long Distance (XC) | 0.0 | 6 | 734.4 | 17 | 626.4 |
| Running Treadmill, Sprints | 10.0 | 0 | 0 | 1 | 1.6 |
| Running Treadmill, long distance | 0.0 | 0 | 0 | 2 | 34.4 |
| Skating (roller/ice/roller-blade) | 6.0 | 1 | 124 | 0 | 0 |
| Skiing (downhill) | 9.0 | 1 | 76 | 12 | 675.2 |
| Skiing (cross-country) | 36.0 | 0 | 0 | 4 | 72 |
| Snowboarding | 1.0 | 0 | 0 | 1 | 226 |
| Soccer | 6.0 | 14 | 4129.2 | 14 | 4615.6 |
| Softball/Baseball | 21.1 | 8 | 639.6 | 12 | 3412.4 |
| Swimming | 36.0 | 9 | 2136.4 | 13 | 374.4 |
| Tennis | 11.6 | 5 | 908.4 | 4 | 310 |
| Track (indoor) | 2.0 | 1 | 110 | 2 | 270.4 |
| Track (outdoor) | 6.0 | 15 | 1915.2 | 10 | 1649.6 |
| Track and Field (jumping events) | 6.0 | 0 | 0 | 1 | 4 |
| Trampoline | 6.0 | 0 | 0 | 1 | 96 |
| Tumbling | 40.0 | 1 | 200 | 3 | 66.4 |
| Ultimate Frisbee | 6.6 | 0 | 0 | 0 | 0 |
| Volleyball | 15.8 | 5 | 842.4 | 13 | 2810 |
| Walking intervals | 0.0 | 1 | 12 | 2 | 88.8 |
| Weight-training (heavy) | 30.0 | 0 | 0 | 1 | 48.8 |
| Weight-training (light ) | 25.0 | 0 | 0 | 0 | 0 |
| Weight-training (moderate) | 25.0 | 7 | 187.2 | 4 | 156 |
| Weight-training (arms, moderate) | 0.0 | 0 | 0 | 2 | 28 |
| Weight-training (legs, moderate) | 25.0 | 0 | 0 | 3 | 72 |
| Wrestling | 28.0 | 0 | 0 | 1 | 12 |
| Yoga (with inversions) | 24.0 | 1 | 8.8 | 0 | 0 |
Table 4.
Regression model statistics for non-dominant arm DXA adjusted for whole body lean mass.
| Radius DXA Output | Cohort A | Cohort B | ||||
|---|---|---|---|---|---|---|
| Adj. Model R2 | β [95% CI] SPCC | Adj. Model R2 | β [95% CI] SPCC | |||
| Whole Body nbFFM | 3 Year Arm totBLI | Whole Body nbFFM | 3 Year Arm totBLI | |||
| 1/3 Area | 0.28c |
0.022 [0.003,0.040] +0.27a |
0.012 [0.004,0.020] +0.36b |
0.46c |
0.032 [0.020,0.044] +0.56c |
0.008 [0.002,0.015] +0.26a |
| 1/3 BMC | 0.46c |
0.021 [0.005,0.037] +0.28b |
0.014 [0.007,0.021] +0.44c |
0.43c |
0.024 [0.010,0.038] +0.38c |
0.015 [0.007,0.023] +0.43c |
| 1/3 aBMD | 0.22b |
0.004 [-0.002,0.009] +0.16ns |
0.003 [0.001,0.006] +0.36b |
0.19b | 0.000 [-0.003,0.004] +0.02ns |
0.003 [0.001,0.006] +0.44b |
| UD Area | 0.41c | 0.017 [0.000,0.035] +0.200.06 |
0.011 [0.004,0.019] +0.32b |
0.53c |
0.035 [0.020,0.051] +0.46c |
0.012 [0.003,0.021] +0.28b |
| UD BMC | 0.50c |
0.025 [0.007,0.043] +0.27b |
0.020 [0.013,0.028] +0.52c |
0.68c |
0.019 [0.011,0.026] +0.43c |
0.014[0.010,0.018] +0.56c |
| UD aBMD | 0.47c |
0.005 [-0.001,0.010] +0.24a |
0.005 [0.003,0.007] +0.50c |
0.62c |
0.004 [0.002,0.007] +0.29b |
0.005 [0.003,0.006] +0.58c |
| Arm Area | 0.46c |
2.563 [1.33,3.80] +0.42c |
0.307 [-0.21,0.83] +0.12ns |
0.60c |
2.6 [1.55,3.64] +0.47c |
0.191 [-0.393,0.775] +0.06ns |
| Arm BMC | 0.52c |
2.79 [1.58,4.0] +0.44c |
0.826 [0.318,1.334] +0.31b |
0.70c |
0.022 [0.015,0.028] +0.51c |
0.007 [0.004,0.011] +0.31c |
| Arm aBMD | 0.51c |
0.005 [0.002,0.009] +0.30b |
0.004 [0.002,0.005] +0.51c |
0.54c |
0.007 [0.003,0.010] +0.38c |
0.005 [0.003,0.007] +0.52c |
| *Arm nbFFM | 0.23c | ------------- |
0.014 [0.006,0.021] +0.44c |
0.30c | ----------- |
0.024 [0.011,0.037] +0.45c |
Italic font indicates ln-transformed dependent variables. BMC= bone mineral content; aBMD= areal bone mineral density; Arm= Non-dominant Arm; nbFFM= non-bone lean mass. All models included gynecological age and height as independent variables (not shown), as well as whole body nbFFM and arm BLI, except models to explain Arm nbFFM (*lean mass excluded). For Adjusted Model R2 and t significance of β
p<0.05;
p≤0.01;
p≤0.001.
If 0.05 ≤ p ≤0.10, and for Arm totBLI, p is noted as parenthetic superscript, unless <0.001.
Table 5.
Regression model statistics for non-dominant arm DXA adjusted for arm lean mass.
| Radius DXA Output | Cohort A | Cohort B | ||||
|---|---|---|---|---|---|---|
| Adj. Model R2 | β[95% CI]SPCC | Adj. Model R2 | β[95% CI]SPCC | |||
| Arm nbFFM | 3 Year Arm totBLI | Arm nbFFM | 3 Year Arm totBLI | |||
| 1/3 Area | 0.33c |
0.410 [0.146,0.674] +0.35b |
0.010 [0.002,0.018] +0.28a |
0.52c |
0.427 [0.284,0.570] +0.61c |
0.003 [-0.004,0.01] +0.08ns |
| 1/3 BMC | 0.46c |
0.386 [0.161,0.610] +0.35c |
0.012 [0.005,0.018] +0.36c |
0.50c |
0.362 [0.198,0.526] +0.46c |
0.010 [0.002,0.018] +0.26a |
| 1/3 aBMD | 0.23b |
0.061 [-0.019,0.142] +0.18ns |
0.003 [0.001,0.006] +0.30a |
0.20b | 0.017 [-0.028,0.063] +0.10ns |
0.003 [0.001,0.005] +0.36b |
| UD Area | 0.43c |
0.321 [0.060,0.581] +0.25a |
0.010 [0.002,0.017] +0.26a |
0.52c |
0.427 [0.229,0.624] +0.44c |
0.007 [-0.003,0.017] +0.14ns |
| UD BMC | 0.57c |
0.518 [0.272,0.765] +0.38c |
0.017 [0.010,0.024] +0.41c |
0.67c |
0.23 [0.136,0.322] +0.42c |
0.01 [0.007,0.016] +0.41c |
| UD aBMD | 0.54c |
0.116 [0.054,0.178] +0.35c |
0.004 [0.002,0.006] +0.39c |
0.62c |
0.052 [-0.019,0.085] +0.29b |
0.004 [0.002,0.006] +0.46c |
| Arm Area | 0.51c |
42.71 [25.12,60.30] +0.46c |
0.109 [-0.414,0.632] +0.04ns |
0.59c |
31.79 [18.71,44.87] +0.46c |
-0.203 [-0.854,0.448] -0.06ns |
| Arm BMC | 0.60c |
49.01 [32.60,65.43] +0.52c |
0.575 [0.09,1.06] +0.20a |
0.76c |
0.298 [0.223,0.373] +0.57c |
0.003 [0.000,0.007] +0.130.078 |
| Arm aBMD | 0.58c |
0.105 [0.059,0.152] +0.40c |
0.003 [0.002,0.005] +0.40c |
0.66c |
0.112 [0.074,0.150] +0.50c |
0.004 [0.002,0.005] +0.32c |
| *Arm nbFFM | 0.70c |
0.052 [0.041,0.064] +0.67c |
5.80 [0.80,10.80] +0.17a |
0.76c |
0.066 [0.052,0.080] +0.66c |
14.67 [6.70,22.64] +0.26c |
Italic font indicates ln-transformed dependent variables.
BMC= bone mineral content; aBMD= areal bone mineral density;
Arm= Non-dominant Arm; nbFFM= non-bone lean mass.
All models included gynecological age and height as independent variables (not shown), as well as Arm nbFFM and arm BLI, except models with Arm nbFFM* as the dependent variable, for which whole body nbFFM was entered.
For Adjusted Model R2 and t significance of β:
p<0.05;
p≤0.01;
p≤0.001.
If 0.05 ≤ p ≤0.10, and for Arm totBLI, p is noted as parenthetic superscript, unless <0.001.
Model adjusted R2 and significance are reported based on p thresholds (0.05, 0.01. 0.001). Beta coefficients with 95% confidence intervals and t significance of betas are reported for all variables. Semi-partial correlation coefficients (SPCCs) are reported in Tables 4-5 as metrics of explanatory value for all independent variables, squared to yield percent of variance explained (discussed in text).
Results
Subject characteristics of the total sample (n=103), Cohort A (n=55) and Cohort B (n=48) are presented in Tables 2a and 2b. No subject demonstrated primary amenorrhea (all subjects’ age at menarche <16.0 years). Although some girls demonstrated menstrual irregularity, this is not uncommon in girls at this maturity stage (all subjects’ gynecological ages were ≤2.6 years at time of DXA). At the time of the focal DXA scan, Cohort A was significantly older, with greater chronological and gynecological age than Cohort B (p≤0.002). However, Cohort B had a younger mean age at menarche (p=0.047), was significantly heavier (p=0.039) and had higher average BMIs (p=0.021), attributable to significantly greater non-bone lean mass (WBnbFFM, ARMnbFFM: p≤0.028) and greater bone outcomes (1/3 BMC, 1/3 aBMD, UD Area, ARMArea, ARMBMC, ARMaBMD: p<0.048; strong trends for 1/3 Area p=0.051, UD BMC p=0.063). There were no significant differences between cohorts for physical activity record-based variables.
Table 3 presents a breakdown of the number of subjects participating in reported activities, along with the total recorded hours of peri-menarcheal participation (36 months per subject, pooled), presented by cohort. The activities with the greatest percentage of participants and recorded hours of participation overall were gymnastics (52%, specifically targeted for the longitudinal study), dance/aerobics (33%) and soccer (27%) [Table 3]. Other activities with more than 1,000 hours of participation recorded are (from highest to lowest hours): cheerleading, lacrosse, softball/baseball, volleyball, track, swimming, marching band, color guard, cross-country running (long distance), tennis and diving.
It is important to note that most of the recorded activity represents elementary/middle school activity, as the majority of the girls were younger than high school age or early in high school at the time of DXA. Despite this early school age range, a wide variety of physical activities is represented by the two cohorts, including the most common competitive sports in which U.S. high school girls participate through school programs (track, basketball, volleyball, soccer, softball/baseball, cross-country running, tennis, swimming/diving, competitive spirit (cheerleading), lacrosse)13. Some of the activities are represented consistently across cohorts (gymnastics, soccer, track), whereas others are represented at disparate subject numbers and training hours in the two samples (basketball, softball/baseball, lacrosse).
For regression analyses, WBnbFFM models included gynecological age, height, WBnbFFM, and totBLI as independent variables (Tables 4 & 5). Gynecological age explained significant variance in only one model: Cohort A UD aBMD, accounting for WBnbFFM (not shown). Height also explained significant variance in few models (not shown). NbFFM and totBLI explained the majority of variance across models and cohorts.
After accounting for gynecological age, height, and WBnbFFM, totBLI explained 7% to 34% of variance for all bone outcomes (p<0.05), except ARM Area (Cohorts A & B). In comparison, WBnbFFM explained 6% to 31% of variance for all outcomes (p<0.05), except 1/3 aBMD (Cohorts A & B), and UD Area (Cohort A). Comparison of arm totBLI betas, significance and squared SPCCs indicated consistent significance and direction of relationships between arm totBLI and bone outcomes across Cohort A & Cohort B models. Cohort A & B squared SPCCs were within 15% of each other for BMC (1/3, UD, ARM), UD Area, ARM aBMD and ARMnbFFM, indicating consistent explanatory value in separate independent samples. By substituting WBnbFFM with ARMnbFFM, totBLI explained 4% to 21% of variance for all bone outcomes except ARM Area (Cohorts A&B), 1/3 Area (B) and UD Area (B) (Table 5). ARMnbFFM explained 6% to 37% of variance for all outcomes with the exception of 1/3 aBMD (Cohorts A & B).
Positive associations indicate that, as quantified using the totBLI algorithm, greater arm loading is associated with greater BMC (UD, 1/3, ARM), bone area (UD & 1/3) and areal density (UD, 1/3, ARM), even after accounting for whole body lean mass. Based on comparison of squared semi-partial correlation coefficients between totBLI and WBnbFFM in Cohort A, totBLI exhibits greater explanatory value than WBnbFFM for all variables other than Arm Area (totBLI=ns) and Arm BMC (9.6% vs. 19.4%). In Cohort B, totBLI exhibited stronger explanatory value than WBnbFFM for all but Arm BMC and all 3 Area variables (1/3, UD, Arm). As would be expected, as an index of local muscle mass, ARMnbFFM tended to demonstrate similar or greater explanatory value to that of arm totBLI for both Cohorts, yet arm totBLI retained significant explanatory value for most dependent variables, with particular potency for 1/3 and UD radius aBMD.
Discussion
Supporting our hypothesis, the peri-menarcheal arm bone loading index reflected site-specific osteogenic potency for a variety of organized activities. Interestingly, in both cohorts, loading index explanatory value rivaled that of whole body non-bone lean mass, exhibiting consistent significant positive associations with non-dominant radius bone mass, geometry and density at radius metaphysis and diaphysis sites. Arm totBLI also exhibited significant explanatory value for total arm BMC, aBMD and non-bone lean mass. Surprisingly, the significant, positive association between arm totBLI and most bone outcomes persisted even after accounting for the statistical relationship with non-bone lean mass; this persistence suggests that, for the represented activities, the osteogenic aspects of loading are not a function of local muscular factors alone.
The current strategy and analysis differs from most upper extremity loading studies that commonly compare bone traits of non-athletes against those of subjects with substantial exposure to specific activity types during growth and/or early adulthood (e.g. gymnastics (weight-bearing/impact), racquet sports (impact), weight-training (weight-bearing))14-19. We designed the analysis to reflect site-specific loading via a range of physical activities, including a variety of doses of artistic gymnastics over the exposure period. Specific inclusion of artistic gymnasts was intended to amplify loading effect sizes (greater correlation coefficients), as follows: 1) gymnast studies exaggerate loading exposure differentials at the non-dominant distal radius, because most activities preferentially load the lower extremities and/or the dominant arm; 2) gymnastics training is experienced over a broad range of exposures (3 year means, 0 to 24 hours per week), thereby expanding the range of loading exposures beyond most samples of the general populace. The broad range of non-gymnastic activities represented, at variable doses within and between cohorts, provided a large degree of variability in loading types (muscular, external loads, impact loads), magnitudes and frequencies. Thus, the overall composition of our subject population allowed assessment of arm totBLI as a measure of osteogenic potential for a wide range of activities during the maturational period represented. Furthermore, arm totBLI explained 19% to 20% of variance in arm non-bone lean mass, with 3% to 7% of ARMnbFFM variance explained even after accounting for the statistical effects of whole body lean mass. This indicates that arm totBLI is valuable for prediction of muscular as well as skeletal adaptations to exercise-related loading.
The bone loading history questionnaire (BLHQ) developed by Dolan et al. was the primary basis for our armBLI2. They used activity-specific ground reaction force data compiled from other sources and reported by Groothausen et al.20 as the basis for the activity-specific bone loading units. They tested two versions of the BLHQ (hip and spine) in a sample of 80 pre-menopausal women, representing low, moderate and high activity levels (mean age 31 years, range 18-45 years old). BLHQ results were evaluated as predictors of femoral neck and lumbar spine aBMD, using both partial correlation (continuous data) and logistic regression analyses (BLHQ and aBMD tertiles)2. After adjusting for BMI, both hip and spine versions of the BLHQ were significantly and positively correlated with femoral neck aBMD (partial correlation coefficients: r=+0.32 and r=+0.34, respectively). Furthermore, after adjusting for age, oral contraceptive use, calcium intake and BMI, odds of low hip aBMD were higher in individuals in the lowest tertiles for recent hip loading AND total and recent spine loading2. Neither BLHQ format predicted lumbar spine aBMD or tertile successfully. Compared to the results of Dolan et al., after adjusting for gynecological age, height and total body non-bone lean mass, our partial correlation results tended to be of higher magnitude (partial r= +0.35 to +0.72) and were statistically significant for all but ARM Area (+0.10 to +0.17). This strong explanatory value is a positive finding, particularly as our BLI are based on perceived “average” site-specific arm loading patterns rather than ground reaction forces measured at the lower extremity or general acceleration profiles. Application of site-specific acceleration profiles recorded during common activities may yield even stronger associations in future bone loading index algorithm analyses.
Weeks and Beck developed the bone-specific physical activity questionnaire (BPAQ) to quantify loading at the hip and spine21. In 20 male and 20 female adults (mean age 24.5, range 18-30), they used force plates to measure ground reaction forces during a series of movement protocols, as a basis for estimation of activity-specific dynamic loading profiles that were incorporated into the BPAQ predictive algorithm. These subjects completed the BPAQ and other questionnaires, including the BLHQ, but only the recent phase of the BPAQ was evaluated. Clinically relevant bone traits were assessed in these same subjects, including but not limited to areal BMD of the lumbar spine, femoral neck, trochanter and whole body, as well as calcaneal ultrasound attenuation. In males, the recent phase of the BPAQ successfully predicted numerous bone properties for femoral neck, lumbar spine and whole body regions of interest (r2= 36% to 68% of variance). However, in young adult females, BPAQ results were not significant predictors of clinically relevant bone outcomes for any of the 10 tested properties for lumbar spine, femoral neck, trochanter or total body regions of interest; only calcaneal ultrasound properties were predicted successfully by the “past loading” component of the BPAQ (48% of variance, p<0.05)21. In comparison, our arm totBLI exhibited significant explanatory value, explaining 7% to 34% of variance in 8/9 bone parameters evaluated, after adjusting for the effects of gynecological age, height and non-bone lean mass.
There are several possible reasons for the differences between our findings and those of the studies of Dolan et al.2 and Weeks and Beck21. First, use of the non-dominant arm loading model and inclusion of gymnasts exaggerates loading diversity, providing high variability to test the arm totBLI algorithm. In the BLHQ and BPAQ studies, limited variability in loading exposure may have been problematic, particularly at sites for which loading via activities of daily living may be more influential over time. Second, activity data for the other two studies were collected retrospectively, which may have increased recall bias; in contrast, our activity data were recorded prospectively at semi-annual intervals over the 3-year period. It is possible that arm totBLI explanatory value would diminish if tested using a lifetime loading history design. Third, the other two studies evaluated adult subjects who may have accumulated more influential confounding effects over time (e.g. long-term dietary and hormonal variations). In particular, the Dolan study included subjects in the peri-menopausal range who may be subject to bone loss, which may be accelerated or slowed as a function of unmeasured factors (diet, parity, breast-feeding, etc.). In contrast, our study design specifically targeted peri-menarcheal loading exposure to amplify the measurable influence of loading on bone development. Also, we restricted subject physical maturity (estrogen exposure) to a narrow gynecological age range to limit the cumulative effects of inter-subject variability in estrogen dose. Strategic gynecological age limitation appeared to be successful, as gynecological age only exhibited significant independent explanatory value in one regression model (Cohort B, UD aBMD, WBnbFFM-adjusted). Finally, in the Weeks and Beck study, BPAQ explanatory value was likely limited by small sample size; however, male analyses yielded significant correlations, supporting the idea that a broad range of loading types and exposures may be most critical to effective algorithm testing. We cannot compare arm totBLI results against those of the other algorithms directly, as neither the BLHQ nor the BPAQ was designed to evaluate upper extremity loading exposure.
Limitations
While increasing the variability of physical activity in this study, inclusion of gymnasts in the study population may also represent a limitation; it is difficult to specifically evaluate the osteogenic value of all included organized activities, since observed effects may be dominated by gymnastics exposure (~50% of subjects participated in gymnastics during the 36 month period). The arm totBLI is limited by the lack of quantitative assessments for each of its components (magnitude, velocity, frequency, exposure dose); we relied on qualitative categorization of activity characteristics and activity reports, with the latter being subject to possible recall bias. Similarly, the current activity index cannot contrast the relative osteogenic potency of multiple loading bouts interspersed with rest periods versus exposure administered in a single bout.
Nonetheless, as hypothesized, armBLI exhibited relatively consistent explanatory value across 2 cohorts, despite significant cohort differences in maturity and anthropometrics, as well as a possibility of subtle cohort differences in activity profiles. Significantly higher lean mass among Cohort B subjects appeared linked to high explanatory value for most bone area outcomes. The fact that this association appears to persist despite accounting for height associations within all models may indicate a particularly strong relationship between lean mass and bone width (periosteal expansion) in Cohort B. It is possible that this finding reflects activity profile differences (sport choice and participation rates) and/or a secular trend for greater lean mass and bone area for height in more recent birth years.
The positive association between cumulative armBLI and ultradistal areal BMD suggests greater bone density with greater loading exposure, but greater out of plane depth cannot be ruled out as the underlying cause of higher observed aBMD (greater periosteal expansion rather than greater volumetric density). Numerous reports indicate that periosteal expansion is the primary mode of radial diaphysis loading adaptation, often accompanied by a widened intramedullary cavity; because this structural adaptation may limit or reduce volumetric density, areal density may not increase significantly with loading22. In particular, if adaptive expansion is primarily medial-lateral rather than postero-anterior9,23-25, volumetric density advantages may be underestimated using PA DXA.
In this preliminary analysis, dietary and hormonal variables were not evaluated as factors in bone development, although we limited the influence of estrogen exposure by restricting gynecological age to a narrow range and incorporating this variable into our regression equations. Future studies should be performed to quantify the key components of the bone loading index. Subsequent analyses should validate the resultant algorithms against observed associations between loading exposure and well-specified bone traits in a larger sample, preferably accounting for potential influence of dietary and hormonal variation. Our current findings support the use of the peri-menarcheal exposure period and associated post-menarcheal outcome data for this purpose. Finally, indices of bone mass, geometry and density were limited to standard 2D DXA outcomes; use of pQCT or high resolution pQCT may provide more specific information on 3D bone structure, microstructure and indices of theoretical strength in relation to loading exposure. Future studies should evaluate data from these skeletal imaging modalities in relation to loading exposure during this key maturity phase.
Conclusion
Overall, our findings, based on peri-menarcheal activity exposure in 2 independent cohorts of young post-menarcheal subjects, indicate that this index of site-specific bone loading provides important, consistent explanatory value for most non-dominant arm DXA musculoskeletal outcomes, even after accounting for effects of physical maturity, body size and total body lean mass, factors with known associations to musculoskeletal outcomes. The current arm loading index may be a useful tool for other research studies evaluating the role of physical activity in upper extremity musculoskeletal adaptation.
Acknowledgements
Data collection: JD, TS, NG. Conception and design: JD, TS, NG, AB, KD, CS, PR. Analysis and interpretation of data: JD, KD, PR. Drafting and revision: JD, TS, NG, AB, KD, CS, PR. Approved final version: JD, TS, KD, PR, CS, NG, AB. JD takes responsibility for the integrity of the data analysis. We would like to acknowledge the assistance of Jill A. Kanaley, Ph.D. (data collection); Cathy Riley and Eileen Burd (DXA technologists); Sue Hemingway and Tina Craig (Study Coordinators). Also, we would like to thank all of the research participants and their parents. This research was funded by NIAMS (R03 AR047613, RO1 AR54145), the Orthopedic Research and Education Foundation, SUNY Upstate Medical University and the University of Wisconsin, Madison (Department of Orthopedics and Rehabilitation; School of Medicine and Public Health).
Footnotes
Edited by: F. Rauch
References
- 1.Dowthwaite J, Benevento E, Xu M, Goldfain A, Mohan C, Mehrotra K, et al. Long-term organized activity records are more appropriate for skeletal growth studies than detailed “snapshot” monitoring. Med Sci Sports Exerc. 2013;45(Suppl 1):312. ACSM Thurs D-17, abstract 1379. [Google Scholar]
- 2.Dolan SH, Williams DP, Ainsworth BE, Shaw JM. Development and reproducibility of the bone loading history questionnaire. Med Sci Sports Exerc. 2006;38:1121–31. doi: 10.1249/01.mss.0000222841.96885.a8. [DOI] [PubMed] [Google Scholar]
- 3.Nellans KW, Kowalski E, Chung KC. The epidemiology of distal radius fractures. Hand Clin. 2012;28:113–25. doi: 10.1016/j.hcl.2012.02.001. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Palmer AK, Werner FW. Biomechanics of the distal radioulnar joint. Clin Orthop. 1984;187:26–35. [PubMed] [Google Scholar]
- 5.Tveit M, Rosengren BE, Nyquist F, Nilsson JA, Karlsson MK. Former male elite athletes have lower incidence of fragility fractures than expected. Med Sci Sports Exerc. 2013;45:405–10. doi: 10.1249/MSS.0b013e318274fdf3. [DOI] [PubMed] [Google Scholar]
- 6.McKay HA, Bailey DA, Mirwald RL, Davison KS, Faulkner RA. Peak bone mineral accrual and age at menarche in adolescent girls:a 6-year longitudinal study. J Pediatr. 1998;133:682–7. doi: 10.1016/s0022-3476(98)70112-x. [DOI] [PubMed] [Google Scholar]
- 7.Dowthwaite JN, Rosenbaum PF, Scerpella TA. Site-specific advantages in skeletal geometry and strength at the proximal femur and forearm in young female gymnasts. Bone. 2012;50:1173–83. doi: 10.1016/j.bone.2012.01.022. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Scerpella TA, Dowthwaite JN, Rosenbaum PF. Sustained skeletal benefit from childhood mechanical loading. Osteoporos Int. 2011;22:2205–10. doi: 10.1007/s00198-010-1373-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Dowthwaite JN, Flowers PP, Scerpella TA. Agreement between pQCT- and DXA-derived indices of bone geometry, density, and theoretical strength in females of varying age, maturity, and physical activity. J Bone Miner Res. 2011;26:1349–57. doi: 10.1002/jbmr.322. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Rauch F, Bailey DA, Baxter-Jones A, Mirwald R, Faulkner R. The ‘muscle-bone unit’ during the pubertal growth spurt. Bone. 2004;34:771–5. doi: 10.1016/j.bone.2004.01.022. [DOI] [PubMed] [Google Scholar]
- 11.Ho-Pham LT, Nguyen UD, Nguyen TV. Association Between Lean Mass, Fat Mass, and Bone Mineral Density:A Meta-analysis. J Clin Endocrinol Metab. 2014;99:30–8. doi: 10.1210/jc.2014-v99i12-30A. [DOI] [PubMed] [Google Scholar]
- 12.Ka K, Rousseau MC, Lambert M, O’Loughlin J, Henderson M, Tremblay A, et al. Association between lean and fat mass and indicators of bone health in prepubertal caucasian children. Horm Res Paediatr. 2013;80:154–62. doi: 10.1159/000354043. [DOI] [PubMed] [Google Scholar]
- 13.2012-13 High school athletic survey results: 10 most popular girls programs [Internet] [updated 1/30/14; cited 1/30/14]; [Google Scholar]
- 14.Haapasalo H, Kannus P, Sievanen H, Heinonen A, Oja P, Vuori I. Long-term unilateral loading and bone mineral density and content in female squash players. Calcif Tissue Int. 1994;54:249–55. doi: 10.1007/BF00295946. [DOI] [PubMed] [Google Scholar]
- 15.Heinonen A, Sievanen H, Kannus P, Oja P, Vuori I. Site-specific skeletal response to long-term weight training seems to be attributable to principal loading modality:a pQCT study of female weightlifters. Calcif Tissue Int. 2002;70:469–74. doi: 10.1007/s00223-001-1019-9. [DOI] [PubMed] [Google Scholar]
- 16.Kontulainen S, Sievanen H, Kannus P, Pasanen M, Vuori I. Effect of long-term impact-loading on mass, size, and estimated strength of humerus and radius of female racquet-sports players:a peripheral quantitative computed tomography study between young and old starters and controls. J Bone Miner Res. 2003;18:352–9. doi: 10.1359/jbmr.2003.18.2.352. [DOI] [PubMed] [Google Scholar]
- 17.Dowthwaite JN, Scerpella TA. Distal radius geometry and skeletal strength indices after peripubertal artistic gymnastics. Osteoporos Int. 2011;22:207–16. doi: 10.1007/s00198-010-1233-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Ducher G, Jaffre C, Arlettaz A, Benhamou CL, Courteix D. Effects of long-term tennis playing on the muscle-bone relationship in the dominant and nondominant forearms. Can J Appl Physiol. 2005;30:3–17. doi: 10.1139/h05-101. [DOI] [PubMed] [Google Scholar]
- 19.Nikander R, Sievanen H, Uusi-Rasi K, Heinonen A, Kannus P. Loading modalities and bone structures at nonweight-bearing upper extremity and weight-bearing lower extremity:a pQCT study of adult female athletes. Bone. 2006;39:886–94. doi: 10.1016/j.bone.2006.04.005. [DOI] [PubMed] [Google Scholar]
- 20.Groothausen J, Siemer H, Kemper HCG, Twisk J, Welten DCW. Influence of peak strain on lumbar bone mineral density:an analysis of 15-year physical activity in young males and females. Pediatr Exerc Sci. 1997;9:159–73. [Google Scholar]
- 21.Weeks BK, Beck BR. The BPAQ:a bone-specific physical activity assessment instrument. Osteoporos Int. 2008;19:1567–77. doi: 10.1007/s00198-008-0606-2. [DOI] [PubMed] [Google Scholar]
- 22.Dowthwaite JN, Scerpella TA. Skeletal geometry and indices of bone strength in artistic gymnasts. J Musculoskelet Neuronal Interact. 2009;9:198–214. [PMC free article] [PubMed] [Google Scholar]
- 23.Dowthwaite JN, Flowers PP, Spadaro JA, Scerpella TA. Bone geometry, density, and strength indices of the distal radius reflect loading via childhood gymnastic activity. J Clin Densitom. 2007;10:65–75. doi: 10.1016/j.jocd.2006.10.003. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Dowthwaite JN, Hickman RM, Kanaley JA, Ploutz-Snyder RJ, Spadaro JA, Scerpella TA. Distal radius strength:A comparison of DXA-derived vs pQCT-measured parameters in adolescent females. J Clin Densitom. 2009;12:42–53. doi: 10.1016/j.jocd.2008.06.001. [DOI] [PubMed] [Google Scholar]
- 25.Dowthwaite JN, Hickman RM, Spadaro JA, Scerpella TA. Gymnastic loading and distal radius cross-sectional asymmetry. J Musculoskelet Neuronal Interact. A2008;8:355–5. IBMS Sun Valley Skeletal Tissue Biology Workshop abstract. [Google Scholar]