

Abstract
Background
Until their phase-out between 2005 and 2013, polybrominated diphenyl ethers (PBDEs) were added to household products including furniture, rugs, and electronics to meet flammability standards. Replacement brominated flame retardant (BFR) chemicals, including 2-ethylhexyl-2,3,4,5 tetrabromobenzoate (TBB) and bis(2-ethylhexyl) 2,3,4,5-tetrabromophthalate (TBPH), which are components of the Firemaster 550® commercial mixture, are now being used to meet some flammability standards in furniture. The objective of this analysis was to evaluate the extent to which mothers and their children living in New York City are exposed to PBDEs, TBB, and TBPH.
Methods
We measured PBDEs, TBB, and TBPH using gas chromatography mass spectrometry in dust (n = 25) and handwipe (n = 11) samples collected between 2012 and 2013 from mothers and children living in New York City. We defined dust as enriched if the proportional distribution for a given BFR exceeded two-thirds of the total BFR content.
Results
We detected PBDEs and TBPH in 100% of dust and handwipe samples and TBB in 100% of dust samples and 95% of handwipe samples. Dust from approximately two-thirds of households was enriched for either PBDEs (n = 9) or for TBB + TBPH (n = 8). Overall, the median house dust concentration of TBB + TBPH (1318 ng/g dust) was higher than that of ΣPentaBDE (802 ng/g dust) and BDE-209 (1171 ng/g dust). Children generally had higher BFR handwipe concentrations compared to mothers (ΣPentaBDE: 73%, BDE-209: 64%, TBB + TBPH: 55%) and within households, BFR concentrations from paired maternal-child handwipes were highly correlated. Among mothers, we found a significant positive relation between house dust and handwipe BDE-209 and TBB + TBPH concentrations.
Conclusion
PBDEs, TBB and TBPH are ubiquitous in house dust and handwipes in a sample of mother-child pairs residing in New York City.
Keywords: Flame retardants, PBDEs, TBB, TBPH, Dust, Handwipe, Children
1. Introduction
Polybrominated diphenyl ethers (PBDEs) are a class of brominated flame retardant (BFR) chemicals that were widely added to furniture, textiles, electronics and other consumer products manufactured in the United States to meet fire safety standards passed in the 1970s [1]. Notably, while these standards do not mandate the use of PBDEs, they can be difficult to pass without the addition of flame retardant chemicals. Between 2004 and 2013, the three major commercial PBDE formulations (PentaBDE, OctaBDE and DecaBDE) were phased out of production in the United States owing to their environmental persistence and mounting evidence demonstrating their association with human health toxicity [2−5]. In 2013, residential fire safety standards were amended to allow upholstered furniture to pass a smolder test rather than the previously required open-flame test [6]. While compliance with the new standard is feasible without the use of flame retardant chemicals, research suggests manufacturers have sought out alternative flame retardants for use in residential furniture and furnishings. For example, proximate to the PentaBDE phase-out, Chemtura introduced Firemaster 550®, a commercial mixture comprised of several chemicals, including two brominated compounds: 2-ethylhexyl-2,3,4,5 tetrabromobenzoate (TBB: 35%) and bis(2-ethylhexyl) 2,3,4,5 tetrabromophthalate (TBPH: 15%). Studies examining the flame retardant content of furniture manufactured in the 2000s suggest Firemaster 550® was introduced as a replacement following the PBDE phase-out [7].
During manufacturing, PBDEs and Firemaster 550® are added, rather than chemically bound, to the consumer products that they are intended to protect. Over time these chemicals are released into the indoor environment where they sorb to house dust [8]. Young children have been shown to have higher serum PBDE concentrations compared to adults living in the same household; this pattern has been partially attributed to children's increased time spent on the floor and their frequent hand-to-mouth activity, which both lead to increased incidental ingestion of house dust [9]. Based on their shared chemical properties and commercial applications, we similarly expect TBB and TBPH to partition in dust; however, data supporting environmental transport and exposure patterns among young children are limited.
Our primary objectives of this study were to examine the associations between concentrations of PBDEs and alternative BFRs (TBB/TBPH) measured in house dust and handwipes collected from maternal-child pairs and to examine the relation between concentrations of these BFRs and several lifestyle and household factors. This is the first comparison of PBDEs, TBB and TBPH in dust and paired maternal-child handwipe samples. This study adds information about how adult versus child BFR exposure pathways may vary and whether TBB/TBPH exposure pathways parallel PBDE exposure pathways. The later have been previously well characterized, however, it is not known whether recommendations developed to minimize PBDE exposure from the indoor environment may also apply to TBB/TBPH.
2. Materials and methods
2.1. Study population
The study population consists of mothers and children enrolled in the Sibling-Hermano's birth cohort. Beginning in 2008, pregnant women were recruited from participants previously enrolled in the Columbia Center for Children's Environmental Health Mothers and Newborns Study, a prospective birth cohort started in 1998 [10]. At enrollment in the 2008 cohort women were between the ages of 27−44 years old. The cohort was originally established to study the effects of prenatal and childhood exposure to several environmental chemicals, therefore, for feasibility, information was collected only on the mother-child dyad. The study protocol was approved by the Institutional Review Board of the Columbia University Medical Center.
2.2. Household dust and handwipe sample collection
From February 2012 to January 2013, when children were approximately 3-years old, we collected dust and handwipe samples from 25 households located in Manhattan and the Bronx. Fig. 1 presents a schematic of all study samples collected.
Fig. 1.
Timeline of study enrollment and sample collection.
At the beginning of each study visit mothers gave written informed consent for themselves and for their child. Detailed sample collection methods are published elsewhere [11]. Briefly, a trained field technician vacuumed the surface area of the main living space using a commercial-grade Eureka canister vacuum cleaner fitted with a specially designed cellulose extraction thimble for dust collection. After 10-15 min (mean: 13 min, SD: 2.4 min), thimbles were removed, wrapped in aluminum foil and sealed in polyurethane bags until further processing. We collected dust field blanks in every 5th household by vacuuming 5 g of sodium sulfate powder from a clean aluminum foil surface. In the laboratory, we sieved dust samples to collect particles <500 μm in size, which we stored in clean amber glass jars at room temperature.
Detailed handwipe sample collection methods have been previously described [12]. Briefly, we wiped the entire palm and back surface of both hands from the base of the fingernails to the wrist with a 3 × 3 sterile gauze pad saturated with 3 mL of isopropyl alcohol. We replaced the used handwipe in a glass vial in an aluminum foil packet, covered it in bubble wrap and stored in a cooler for transport to our laboratory where samples were stored at −20 °C. We collected field blanks at 10% of randomly selected households by saturating a sterile gauze pad with isopropyl alcohol and placing it directly into an aluminum foil packet.
2.3. Household dust and handwipe analysis
Household dust (n = 25) and handwipe (n = 11) samples were analyzed for TBB, TBPH and 28 PBDE congeners using methods that have been previously reported [12,13]. Briefly, dust samples and handwipes were extracted with 50:50 hexane: dichloromethane and then purified using Floristic solid-phase extraction cartridges. Samples were spiked with isotopically labeled internal standards prior to extraction. Final analytic concentrations were determined using gas chromatography-mass spectrometry operated in electron capture negative ionization mode (GC/ECNI-MS). Laboratory blanks were included with each analytic run. Method limits of detection (MLD) were calculated using 3 times the standard deviation (SD) of the field blanks or as the laboratory limit of quantification (signal to noise ratio of 3) for congeners not detected in field blanks. Handwipes were only analyzed from a subset of participants due to resource constraints. The handwipes selected for analysis were collected between February and May 2012; these were the first 11 of the 25 households included in the study.
2.4. Questionnaire
At the time of sample collection, we conducted a structured interview to obtain information about personal characteristics (race/ethnicity, maternal age, marital status), lifestyle habits (maternal employment, smoking status, cleaning patterns, maternal-reported minutes since last hand wash) and household factors (clutter, type of floor covering, living conditions, material hardship). We additionally recorded the season that samples were collected.
2.5. Data analysis
To account for size differences in mother's versus children's hands, we normalized handwipe concentrations by hand surface area (ng/cm2), which we calculated from tracings of participant hands using an open-source program for estimating the area and perimeter of complex polygons (sketchandcalc.com). We blank-corrected samples by subtracting the average concentration detected in field blanks and replaced non-detected samples with the MLD divided by the square root of 2. We created a measure of ΣPentaBDE by summing BDEs 47, 99, 100, 153, 154 and co-eluting 85 and 155. We created a measure of alternative BFRs known to be included in some commercial mixtures (e.g. Firemaster 550®) by summing TBB and TBPH. We also focused analyses on BDE-209, which is the primary component of DecaBDE.
We examined relative proportions of ΣPentaBDEs, BDE-209 and TBB+ TBPH in house dust and identified households as enriched for TBB + TBPH or PBDEs based on whether the respective BFR proportional distribution exceeded two-thirds of the total BFR content. We performed bivariate logistic regression to determine if any characteristics predicted the likelihood of living in a PBDE or TBB + TBPH enriched household.
We examined summary statistics, including Spearman correlations, and used Wilcoxon signed rank and Kruskal-Wallis one-way analysis of variance tests to examine whether median house dust or handwipe BFR concentrations differed across several lifestyle and household characteristics. We considered values greater than the median plus 1.5 times the interquartile range as outliers. We conducted bivariate linear regression analyses to compare BFR concentrations in house dust to natural-log transformed concentrations in handwipes. All statistical analyses were performed using STATA (version 14.1).
3. Results
3.1. Participant characteristics
Among the 25 households included in the study, mothers and children had mean ages of 32.2 (SD: 4.0) years and 3.3 (SD: 0.7) years, respectively. All mothers self-identified as African American (40%) or Dominican (60%). We detected no significant differences in household or lifestyle characteristics between the 11 households with and the 14 households without handwipe samples except that women were more likely to be employed in households where handwipes were collected (55% vs. 8%).
3.2. BFR concentrations in house dust
We detected 2 of the 4 PentaBDE congeners (BDE-47 and BDE-99), BDE-209, TBB, and TBPH in 100% of house dust samples (Supplemental Fig. 1). When examining relative BFR proportions, we identified three house dust patterns: TBB + TBPH enriched (n = 8), PBDE enriched (n = 9), and approximately equal levels of TBB + TBPH and PBDE (n = 8) (Supplemental Fig. 2). We identified no demographic or household variables that predicted BFR enrichment. PentaBDE congeners had moderate to high correlations with each other (rspearman= 0.48 to 0.94, p-values<0.05) while TBB and TBPH were highly correlated (rspearman = 0.72, p < 0.001); however, we found no correlation between PentaBDE, BDE-209, and TBB + TBPH. Overall, the median concentration of TBB + TBPH (1318 ng/g dust) was greater than that of PentaBDE (802 ng/g dust) and BDE-209 (1171 ng/g dust). As illustrated by Fig. 2, our sample included households with values greater than the median plus 1.5 times the interquartile range for each class of BFR (ΣPentaBDE: n = 5, households 5, 6,13, 16, and 21; BDE-209: n = 4, households 2, 8,13, and 18; TBB + TBPH: n = 4, households 22−25). We did not detect significantly different median concentrations across household or lifestyle characteristics for any of the 3 BFR classes examined (Table 1).
Fig. 2.
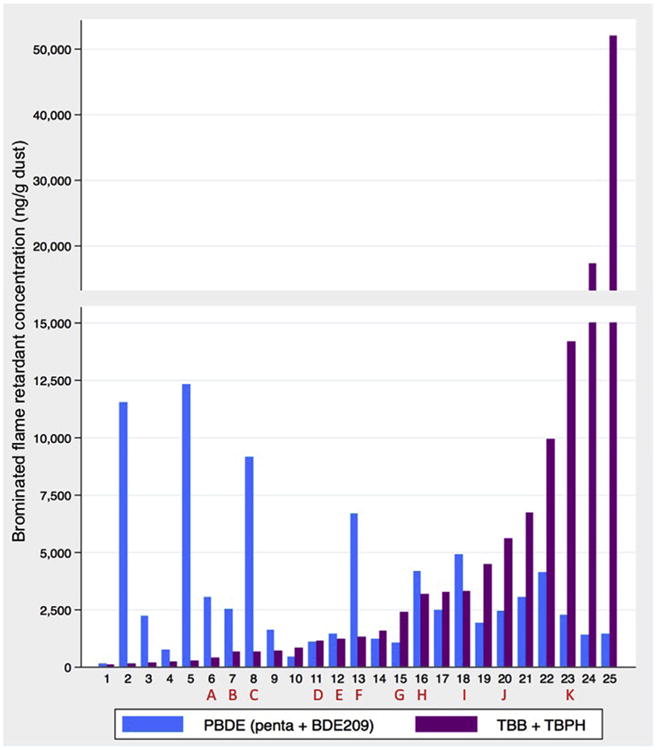
PBDE and TBB + TBPH concentrations in dust from New York City households, n = 25. Letters represent households where BFR concentrations were additionally measured in paired maternal-child handwipes. Penta represents the sum total of BDE congeners 47, 99, 100, 153, 154 and co-eluting 85 and 155.
Table 1.
Median BFR concentrations in dust from households in New York City, n = 25.
| N | ΣPentaBDEa (ng/g dust) | BDE-209 (ng/g dust) | TBB + TBPH (ng/g dust) | |
|---|---|---|---|---|
| Overall | 25 | 802.2 | 1171.4 | 1317.9 |
| Ethnicity | ||||
| Domican | 15 | 876.9 | 1142.7 | 1134.2 |
| African American | 10 | 772.2 | 1280.2 | 3226.9 |
| Education | ||||
| <High school | 6 | 816.0 | 1170.5 | 1781.8 |
| High school | 15 | 772.7 | 1388.9 | 1317.9 |
| >High school | 4 | 857.7 | 1426.9 | 2189.5 |
| Satisfied with living conditions | ||||
| Neutral | 5 | 802.2 | 1171.4 | 3271.3 |
| Somewhat satisfied | 12 | 834.8 | 1166.8 | 1226.1 |
| Very satisfied | 8 | 776.7 | 1265.8 | 1097.0 |
| Mother currently working | ||||
| No | 17 | 876.9 | 1169.6 | 1317.9 |
| Yes | 8 | 797.4 | 1541.6 | 1803.6 |
| Cluttered home | ||||
| No | 16 | 782.7 | 1170.5 | 1803.6 |
| Yes | 9 | 1230.5 | 1582.5 | 1317.9 |
| Home crowded with furniture | ||||
| No | 12 | 787.4 | 1298.1 | 974.0 |
| Yes | 13 | 876.9 | 1171.4 | 3164.4 |
| Flooring type | ||||
| Hardwood | 8 | 776.8 | 961.3 | 1855.3 |
| Carpet | 5 | 792.7 | 1582.5 | 646.5 |
| Linoleum | 8 | 979.4 | 1156.1 | 974.0 |
| Tile | 4 | 726.9 | 1943.8 | 5743.7 |
| Season of sampling | ||||
| Winter | 10 | 797.4 | 1504.6 | 1803.6 |
| Spring | 7 | 1045.7 | 1470.1 | 1134.2 |
| Summer | 5 | 663.7 | 349.5 | 1549.6 |
| Fall | 3 | 751.3 | 1171.4 | 3271.3 |
| Cleaning with vacuum | ||||
| No | 17 | 772.7 | 1169.6 | 1549.6 |
| Yes | 8 | 839.5 | 1485.7 | 964.9 |
| Cleaning with dustmop | ||||
| No | 15 | 802.2 | 1171.4 | 1134.2 |
| Yes | 10 | 826.7 | 1298.1 | 3217.8 |
| Cleaning with wetmop | ||||
| No | 11 | 889.6 | 1169.6 | 1549.6 |
| Yes | 14 | 782.7 | 1299.0 | 1065.9 |
ΣPentaBDE represents the sum total of BDE congeners 47, 99, 100, 153, 154 and co-eluting 85 and 155.
3.3. BFR concentrations in handwipes
Among the paired handwipe samples, BDE-47, BDE-99, BDE-100, and BDE-209 were detected in 100% of samples, while BDE-153 and BDE-154 were each detected in 82% and BDE-85/155 in 64%. TBPH was detected in all handwipe samples while TBB was detected in all but one sample. Within households, paired handwipe BFR concentrations were highly correlated (ΣPentaBDE rspearman = 0.83, BDE-209 rspearman = 0.59, TBB TBPH rspearman = 0.84). As illustrated by Fig. 3, children generally had higher PBDE concentrations than their mothers across households (median ΣPentaBDE mother: 0.19 ng/cm2 vs. child: 0.33 ng/cm2; median BDE-209 mother: 0.15 ng/cm2 vs. child: 0.27 ng/cm2) and within households (percent of households for which concentration in child handwipe exceeded paired maternal handwipe: ΣPentaBDE: 73% and BDE-209: 64%). However, among a subset of pairs, PBDE concentrations in the maternal handwipe was much greater than the paired child handwipe (Fig. 3: ΣPentaBDE: household “A”; BDE-209: household “C”). Children also had higher concentrations of TBB + TBPH than their mothers across households (median TBB + TBPH mother: 0.48 ng/cm2 vs. child: 0.86 ng/ cm2) and within households (percent of households for which concentration in child handwipe exceeded paired maternal hand-wipe: 55%). Given our small sample size, it is not surprising that we did not detect significantly different maternal or child handwipe concentrations by hand washing behavior, lotion use or any demographic characteristics, except that girls had significantly higher TBB + TBPH than boys (p = 0.02) (Table 2).
Fig. 3.
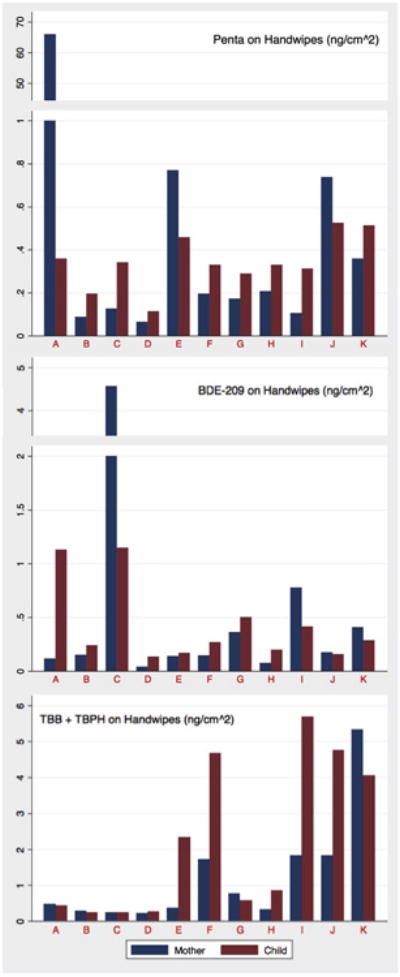
Comparison of BFR concentrations between paired maternal and child hand-wipes, n = 11. Concentrations are normalized to hand surface area (ng/cm2). Letters represent households. Penta represents the sum total of BDE congeners 47, 99, 100, 153, 154 and co-eluting 85 and 155.
Table 2.
Median BFR concentrations on handwipes from maternal-child pairs residing in New York City, n = 11.
| Mother (ng/cm2) | Child (ng/cm2) | |||||||
|---|---|---|---|---|---|---|---|---|
|
|
|
|||||||
| N | ΣPenta BDEa | BDE-209 | TBB + TBPH | N | ΣPenta BDEa | BDE-209 | TBB + TBPH | |
| Overall | 11 | 0.20 | 0.15 | 0.48 | 11 | 0.33 | 0.27 | 0.86 |
| Ethnicity | ||||||||
| Domican | 7 | 0.20 | 0.15 | 0.48 | 7 | 0.33 | 0.24 | 0.57 |
| African American | 4 | 0.17 | 0.59 | 1.08 | 4 | 0.34 | 0.35 | 2.45 |
| Sex | ||||||||
| Female | 11 | 0.20 | 0.15 | 0.48 | 6 | 0.39 | 0.18 | 3.20* |
| Male | 5 | 0.31 | 0.50 | 0.43 | ||||
| Minutes since handwash | ||||||||
| 0-60 | 7 | 0.19 | 0.15 | 0.48 | 2 | 0.33 | 0.23 | 2.78 |
| 61-120 | 2 | 0.42 | 0.48 | 1.83 | 3 | 0.19 | 0.24 | 0.26 |
| 120+ | 2 | 0.42 | 0.09 | 0.30 | 5 | 0.34 | 0.41 | 2.35 |
| Lotion use since handwash | ||||||||
| No | 7 | 0.17 | 0.36 | 0.77 | 9 | 0.34 | 0.27 | 0.86 |
| Yes | 4 | 0.75 | 0.13 | 0.43 | 2 | 0.21 | 0.27 | 2.98 |
p= 0.02.
ΣPentaBDE represents the sum total of BDE congeners 47, 99, 100, 153, 154 and co-eluting 85 and 155. Concentrations normalized to hand surface area (ng/cm2).
3.4. BFR concentration in house dust compared to handwipes
As illustrated by Fig. 4, for both BDE-209 and TBB + TBPH the associations between house dust and handwipe concentrations were stronger for mothers (BDE-209: β = 0.45 per 1000 ng/g dust, p = 0.002; TBB + TBPH: β = 0.24 per 1000 ng/g dust, p = 0.005) compared to children (BDE-209: β = 0.17 per 1000 ng/g dust, p=0.09; TBB + TBPH: β = 0.24 per 1000 ng/g dust, p = 0.005). For Σ PentaBDE, the relation between house dust and handwipe concentrations was positive but not significant for either mothers(β= 0.49 per 1000 ng/g dust, p = 0.50) or children (β= 0.02 per 1000 ng/g dust, p = 0.89).
Fig. 4.
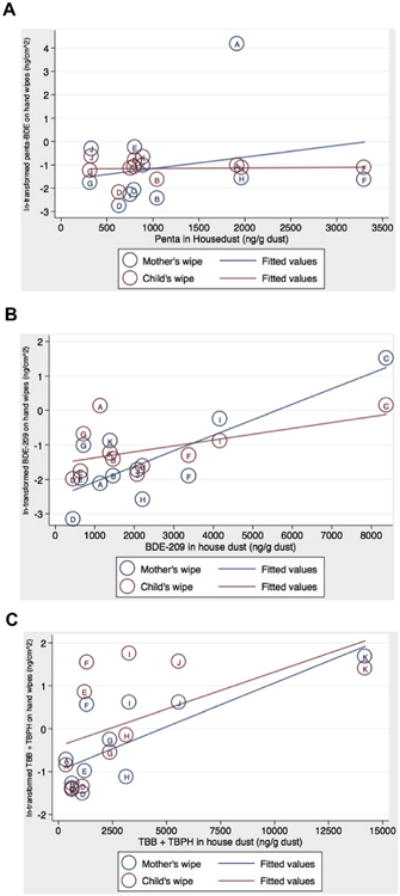
Comparison of BFRs measured in house dust and handwipes, n = 11 mother-child pairs. Letters represent households. Penta represents the sum total of BDE congeners 47, 99, 100, 153, 154 and co-eluting 85 and 155.
4. Discussion
In this study, we examined levels of PBDEs and newer BFRs (TBB/TBPH) in house dust (n = 25) and paired maternal-child handwipes (n = 11). This is the first study to examine the distribution of both PBDE and TBB/TBPH concentrations in New York City homes and the first to examine paired maternal-child handwipe samples.
We detected PBDEs and TBB/TBPH in dust collected from 100% of households surveyed. This is consistent with the results from 4 U.S.-based studies (n = 30–81 participants) conducted between 2009 and 2012, which detected PBDEs and/or TBB/TBPH in 94–100% of house or office dust samples (Supplemental Table 1) [13–17]. The geometric mean house dust concentrations of ΣPentaBDE (816 ng/g) and BDE-209 (1051 ng/g) were lower in our samples compared to those collected from Massachusetts (ΣPentaBDE: 2167 ng/g, BDE-209: 4204 ng/g) and North Carolina (ΣPentaBDE: 1400–2153 ng/g, BDE-209:1280–2574 ng/g). The geometric mean TBB concentration was higher in our study (762 ng/g) compared to samples collected from North Carolina homes (97–315 ng/g), however, geometric mean TBPH concentrations were similar (New York: 590 ng/g, North Carolina: 365–604 ng/g). These findings may reflect differences in housing type (e.g., apartments vs. single family homes), demographics that may influence furniture and furnishing purchasing and replacement habits (e.g., ethnicity, socioeconomic factors), or time trends in flame retardant use (2009–2012 versus 2012–2013).
We found that house dust from approximately two-thirds of homes was enriched for either PBDEs or TBB + TBPH, supporting previous work that has suggested brominated flame retardant mixtures containing TBB and TBPH, such as Firemaster 550®, have been used as replacements for PBDEs in furniture and furnishings [7]. Moreover, across all households, the median TBB + TBPH concentration exceeded PBDE concentrations, suggesting that the magnitude of exposure to alternative BFRs may parallel or exceed exposure to PBDEs. Despite the recent PBDE phase-out, our detection of ΣPentaBDE and BDE-209 in 100% of samples is not surprising given that furniture is infrequently replaced.
Similar to house dust, we detected PBDEs and TBB + TBPH in 100% of paired maternal-child handwipe samples. No previous studies have measured BFR concentrations in paired maternal-child samples, however, the concentrations and detection frequencies reported here are consistent with results from studies measuring PBDEs or TBB/TBPH in samples collected from either children [13,16] or adults [14,15,17] (Supplemental Table 1).
In the present study, we found that while concentrations on the hands of mothers and their children were significantly correlated, toddlers generally had higher BFR concentrations (per unit hand surface area) than their mothers. Additionally, we found positive associations between BFRs measured in house dust (ng/g) and per unit hand surface area (ng/cm2), however, these associations were only statistically significant for BDE-209 and TBB + TBPH measured in maternal handwipes. These patterns suggest that while the indoor environment shared by mothers and their children may be an important source of BFR exposure, age-specific behaviors may contribute to differences in exposure pathways within the home. Studies have shown that the distribution of house dust particles size varies by the spatial positioning of the settled dust [18,19] and that concentrations of PentaBDE congeners, but not BDE-209 or TBB, vary by dust particle size, with higher concentrations typically detected in smaller size fractions [20]. These properties may partially explain our lack of a significant association between ΣPentaBDE measured in house dust and on handwipes, as dust on surfaces and handwipes may be characterized by different dust particle size distributions. This may be especially true for mothers, who may be in contact with dust on elevated surfaces more than dust on the floor. Additionally, it has been shown that plastic toys made with recycled materials may contain PBDEs [21] and that children who play primarily with plastic toys versus wood or metal toys have higher PBDE handwipe concentrations [22]. This suggests that PBDE hand residue levels may reflect direct contact with toys and partially explain our lack of an association between ΣPentaBDE concentrations in house dust and on child handwipes.
The studies conducted in Massachusetts and North Carolina have consistently reported moderate positive correlations between BFR concentrations measured in house dust (ng/g dust) and on handwipes (ng/wipe) collected from adults (rspearman = ΣPentaBDE: 0.38; BDE-209: 0.33; TBB: 0.34; TBPH: 0.35) or children (rspearman = ΣPentaBDE: 0.31; TBB: 0.54) (Supplemental Table 2). In order to compare our findings to these previous studies, we re-examined our handwipe data on a mass basis. We found that when not adjusting for hand surface area, the correlation between BFRs in house dust and handwipes in our study was similar to previous studies for BDE-209 (rspearman child: 0.25, adult: 0.46) and TBPH (rspearman child: 0.39, adult: 0.49), however, we found stronger correlations for TBB (rspearman child: 0.81, adult: 0.75) and a weaker correlation for ΣPentaBDE among adults (rspearman: 0.09). In contrast to previous studies, among children we detected an inverse correlation between ΣPentaBDE measured in house dust and on handwipes (rspearman: −0.27). Given our small sample size, this is likely due to the strong inverse relation between ΣPentaBDE house dust and handwipe concentrations for the child living in “home F”, who had a small hand size relative to the other children in the study, but the highest house dust concentration.
We did not find associations between any household-level characteristic and house dust or handwipe concentrations. Increasing the frequency of house cleaning and hand washing is often cited as a method to reduce flame retardant exposure (e.g., https://www.epa.gov/assessing-and-managing-chemicals-under-tsca/reducing-your-childs-exposure-flame-retardant-chemicals), however, we found that neither time since last hand wash or frequency of house cleaning was associated with lower dust or handwipe concentrations. In a study of children aged 2–5 years, frequency of hand washing, specifically washing hands more than 5 times per day, was associated with lower concentrations of PBDE and Firemaster 550®-associated BFRs [16]. Unfortunately, we were unable to directly compare our findings to this study as we did not collect information about hand washing frequency. One recent study reported that toddler's handwipe concentrations of PBDEs were related more closely to behavioral characteristics (e.g., licking fingers, hours of sleep) than household characteristics (e.g., flooring type) [22]. While we do not have measures of behavioral characteristics in this sample, we also found that flooring type was not related to BFR concentrations.
One limitation of our study is that we did not examine other classes of flame retardants (e.g., organophosphate flame retardants, chlorinated flame retardants) that have also been used as PBDE replacements. Therefore, total exposure to flame retardants for mothers and children in New York City is likely underestimated by the measures reported here. Also, handwipe residues are an indicator of personal exposure but do not reflect internal dose, which could be assessed by measuring PBDEs in blood or metabolites of TBB and TBPH in urine. Other studies in toddlers have found that serum PentaBDE concentrations significantly correlate with both handwipe and house dust PentaBDE levels [13]. Finally, due to the small sample size, this study may have been unable to detect associations or trends between household characteristics and BFR concentrations in house dust and in handwipes.
Our study is the first to explore house dust and handwipe BFR concentrations among mothers and their toddlers. We found that the presence of PBDEs, TBB and TBPH was ubiquitous and that among the subset of homes with handwipe samples, toddlers tended to have higher hand residue concentrations than their mothers. Concentrations of BDE-209 and TBB + TBPH, but not PentaBDEs, measured in house dust were significantly associated with concentrations measured on the hands of mothers. Future research conducted on a larger sample size, is needed to understand how PBDEs and newer BFRs relate to each other in the indoor environment and to identify and evaluate modifiable factors, including individual behaviors, that may reduce BFR exposure among these potentially susceptible sub populations.
Supplementary Material
Acknowledgments
We acknowledge the assistance of Boris Cortes, Adnan Divjan, and Anastasiya Vasilyeva.
Sources of funding: This research was supported by: the Passport, Forsythia, and Fine Foundations, NIH R01 ES021806, R00 ES 017051, and P01 ES09089. During preparation of this manuscript, WJC was supported by NIEHS T32ES023772, NIEHS T32ES007322 and EPA FP-91779001.
Abbreviations
- BFR
brominated flame retardant
- MLD
method limit of detection
- PBDE
polybrominated diphenyl ether
- TBB
2-ethylhexyl-2,3,4,5- tetrabromobenzoate
- TBPH
bis(2-ethylhexyl) 2,3,4,5-tetrabromophthalate
Footnotes
Appendix A. Supplementary data
Supplementary data related to this article can be found at http://dx.doi.org/10.1016/j.emcon.2017.01.001.
References
- 1.Technical Bulletin 117. State of California Department of Consumer Affairs. North Highlands, CA: 1975. pp. 1–8. [Google Scholar]
- 2.G.L.C. Corportation. Great Lakes Chemical Corporation Completes Phase-out of Two Flame Retardants. Great Lakes Chemical Corportation; Indianapolic, IN: 2005. [Google Scholar]
- 3.EPA. DecaBDE phase-out initiative. [2015 February 20];2015 Available from: http://www.epa.gov/oppt/existingchemicals/pubs/actionplans/deccadbe.html.
- 4.Fromme H, et al. Brominated flame retardants - exposure and risk assessment for the general population, Int. J Hyg Environ Health. 2016;219(1):1–23. doi: 10.1016/j.ijheh.2015.08.004. [DOI] [PubMed] [Google Scholar]
- 5.Linares V, Belles M, Domingo JL. Human exposure to PBDE and critical evaluation of health hazards. Arch Toxicol. 2015;89(3):335–356. doi: 10.1007/s00204-015-1457-1. [DOI] [PubMed] [Google Scholar]
- 6.Technical Bulletin 117-2013. State of California, Department of Consumer Affairs; Sacramento, CA: 2013. pp. 1–13. [Google Scholar]
- 7.Stapleton HM, et al. Novel and high volume use flame retardants in US couches reflective of the 2005 PentaBDE phase out. Environ Sci Technol. 2012;46(24):13432–13439. doi: 10.1021/es303471d. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Alaee M, et al. An overview of commercially used brominated flame retardants, their applications, their use patterns in different countries/regions and possible modes of release. Environ Int. 2003;29(6):683–689. doi: 10.1016/S0160-4120(03)00121-1. [DOI] [PubMed] [Google Scholar]
- 9.Lunder S, et al. Significantly higher polybrominated diphenyl ether levels in young U.S. children than in their mothers. Environ Sci Technol. 2010;44(13):5256–5262. doi: 10.1021/es1009357. [DOI] [PubMed] [Google Scholar]
- 10.Perera FP, et al. Effect of prenatal exposure to airborne polycyclic aromatic hydrocarbons on neuro development in the first 3 years of life among inner-city children. Environ Health Perspect. 2006;114(8):1287–1292. doi: 10.1289/ehp.9084. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Allen JG, et al. Critical factors in assessing exposure to PBDEs via house dust. Environ Int. 2008;34(8):1085–1091. doi: 10.1016/j.envint.2008.03.006. [DOI] [PubMed] [Google Scholar]
- 12.Stapleton HM, et al. Measurement of polybrominated diphenyl ethers on hand wipes: estimating exposure from hand-to-mouth contact. Environ Sci Technol. 2008;42(9):3329–3334. doi: 10.1021/es7029625. [DOI] [PubMed] [Google Scholar]
- 13.Stapleton HM, et al. Serum PBDEs in a North Carolina toddler cohort: associations with handwipes, house dust, and socioeconomic variables. Environ Health Perspect. 2012;120(7):1049–1054. doi: 10.1289/ehp.1104802. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Hoffman K, et al. Urinary tetrabromobenzoic acid (TBBA) as a biomarker of exposure to the flame retardant mixture Firemaster(R) 550. Environ Health Perspect. 2014;122(9):963–969. doi: 10.1289/ehp.1308028. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Hoffman K, et al. Monitoring indoor exposure to organophosphate flame retardants: hand wipes and house dust. Environ Health Perspect. 2015;123(2):160–165. doi: 10.1289/ehp.1408669. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Stapleton HM, et al. Flame retardant associations between children's handwipes and house dust. Chemosphere. 2014;116:54–60. doi: 10.1016/j.chemosphere.2013.12.100. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Watkins DJ, et al. Exposure to PBDEs in the office environment: evaluating the relationships between dust, handwipes, and serum. Environ Health Per-spect. 2011;119(9):1247–1252. doi: 10.1289/ehp.1003271. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Cao ZG, et al. Particle size: a missing factor in risk assessment of human exposure to toxic chemicals in settled indoor dust. Environ Int. 2012;49:24–30. doi: 10.1016/j.envint.2012.08.010. [DOI] [PubMed] [Google Scholar]
- 19.Muenhor D, Harrad S. Within-room and within-building temporal and spatial variations in concentrations of polybrominated diphenyl ethers (PBDEs) in indoor dust. Environ Int. 2012;47:23–27. doi: 10.1016/j.envint.2012.06.001. [DOI] [PubMed] [Google Scholar]
- 20.Al-Omran LS, Harrad S. Distribution pattern of legacy and “novel” bromi-nated flame retardants in different particle size fractions of indoor dust in Birmingham, United Kingdom. Chemosphere. 2016;157:124–131. doi: 10.1016/j.chemosphere.2016.05.041. [DOI] [PubMed] [Google Scholar]
- 21.Chen SJ, et al. Brominated flame retardants inchildren's toys: concentration, composition, and children's exposure and risk assessment. Environ Sci Technol. 2009;43(11):4200–4206. doi: 10.1021/es9004834. [DOI] [PubMed] [Google Scholar]
- 22.Hoffman K, et al. Toddler's behavior and its impacts on exposure to poly-brominated diphenyl ethers. J Expo Sci Environ Epidemiol. 2016 Mar 9; doi: 10.1038/jes.2016.11. http://dx.doi.org/10.1038/jes.2016.1. [DOI] [PMC free article] [PubMed]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.