

 This work is licensed under a
This work is licensed under a Abstract
Tumor-induced osteomalacia (TIO) is caused by the hormone fibroblast growth factor 23 (FGF-23). It is mainly produced in the tissue of mesenchymal tumors. Patients with TIO frequently suffer from a chronic decompensated pain syndrome and/or muscle weakness with postural deformity. Despite the severity of the disease, the diagnosis is frequently established late. In some cases, it takes several years to establish the condition. This case report concerning a 68-year old woman demonstrates the selective blood sampling for FGF-23 as path-breaking diagnostics to confirm the diagnosis of a neuroendocrine tumor.
Learning points:
Tumor-induced osteomalacia is a rare condition compared to other paraneoplastic syndromes.
It causes complex symptoms such as progressive reduction of physical capacity, exhaustion, fatigue, a decompensated pain syndrome of the musculoskeletal system and fractures of several bones.
Elevated serum levels of FGF-23 implicate massive phosphate elimination and resulting hypophosphatemia.
The diagnosis is often established over a period of several years because the localization of small FGF-23-producing tumors is complicated.
It is the combination of MRI and selective blood sampling for FGF-23 which permits reliable identification of tumors causing TIO and leads to accurate localization.
In a patient with generalized pain and reduced physical capacity, osteological parameters such as phosphate, 25-OH vitamin D3 and 1,25-(OH)2D3, as well as bone-specific alkaline phosphatase levels in serum should be determined. Hypophosphatemia should always lead to further diagnostic investigations aiming at the detection of an FGF-23-producing tumor.
Patient demographics: Adult, Female, White, Germany
Clinical overview: Bone, Tumours and neoplasia, FGF23, Osteomalacia, Tumour-induced osteomalacia, Paraneoplastic syndromes, Hypophosphataemia, Neuroendocrine tumour
Diagnosis & treatment: Osteomalacia, Hypophosphataemia, Back pain, Fatigue, Bone fracture(s), FGF23, MRI, Alkaline phosphatase (bone-specific), 25-hydroxyvitamin-D3, Calcitriol, Phosphate (serum), Bone scintigraphy, X-ray, Calcium (serum), CT scan, PET scan, Immunohistochemistry, Histopathology, Resection of tumour, Calcitriol, Phosphate supplements
Related disciplines: Neurology, Oncology, Surgery
Publication details: Novel diagnostic procedure, October, 2017
Background
This case report concerning a 68-year-old woman demonstrates the selective blood sampling for FGF-23 as path-breaking diagnostics to confirm the diagnosis of a neuroendocrine tumor which is often undetected due to its small dimension.
Case presentation
Introduction
Tumor-induced osteomalacia (TIO) is caused by the hormone fibroblast growth factor 23 (FGF-23). It is mainly produced in the tissue of mesenchymal tumors. Phosphate metabolism is markedly disrupted by the abnormal production of FGF-23, and phosphate is eliminated to a greater extent (1).
Phosphate and calcium are linked to each other in blood as a calcium–phosphate product. The reduction of serum phosphate levels impairs the calcification of bone, and the interplay of the musculoskeletal system is disrupted (1).
Patients with TIO frequently suffer from a chronic decompensated pain syndrome and/or muscle weakness with postural deformity (2).
Despite the severity of the disease, the diagnosis is frequently established late. In some cases, it takes several years to establish the condition (3). Diagnostic investigations in the region of the skull base by computed tomography (CT) and magnetic resonance imaging (MRI) are hindered by the small dimensions of mesenchymal tumors (4).
In 2004, Takeuchi et al. reported on selective venous blood sampling combined with MRI for the diagnosis of TIO.
The following case is presented with the purpose of facilitating and accelerating the detection of FGF-23-producing tumors in the future.
Clinical summary
A 68-year-old woman was admitted to the hospital in November 2010. At this time, she had pain in the lumbar region for about 22 months, with a progressive reduction of her physical capacity. Additionally, she reported exhaustion and fatigue. She had a decompensated pain syndrome of the musculoskeletal system, starting in the upper arms and spreading to the thighs and the hips. Any movement was associated with severe pain and required the use of forearm supports. X-rays revealed 11 vertebral body fractures, while scintigraphy showed fractures in both upper arms and thighs.
The patient’s blood chemistry revealed elevated alkaline phosphatase levels, markedly reduced phosphate and very low 1,25-(OH)2D3 levels. These findings led to the investigation of the patient’s FGF-23 levels, which were found to be markedly high.
A staging was initiated because a malignant condition was suspected. The suspicion of malignancy was not confirmed. A cerebral meningioma was diagnosed, but was initially not taken into account as a cause of the patient’s elevated FGF-23 levels.
TIO-specific diagnostic investigation
A bone metabolism and hormone analysis was initiated during the patient’s hospital stay in November 2010. The following conditions were found: massively reduced serum phosphate levels (0.48 mmol/L), elevated bone-specific alkaline phosphatase (109.00 μkg/L) and PTH (9.86 pmol/L), reduced serum levels of 25-OH-Vitamin D3 (48.0 nmol/L) and 1,25-(OH)2D3 (5.0 ng/L) and a serum calcium value of 2.36 mmol/L. Osteolyses and pathological space-occupying lesions were ruled out on MRI. Imaging investigations revealed severe osteomalacia (Looser’s transformation zones) with a pronounced remodeling of bones. Fractures of the femoral neck and the humerus on both sides, as well as multiple rib and vertebral body fractures were found.
These findings were viewed in unison and an FGF-23-producing tumor of uncertain location (CUP) was suspected. Serum levels of FGF-23 were markedly increased. A whole-body MRI and a CT scan failed to provide unequivocal information besides a meningioma in the olfactory groove on the right side (Fig. 1).
Figure 1.
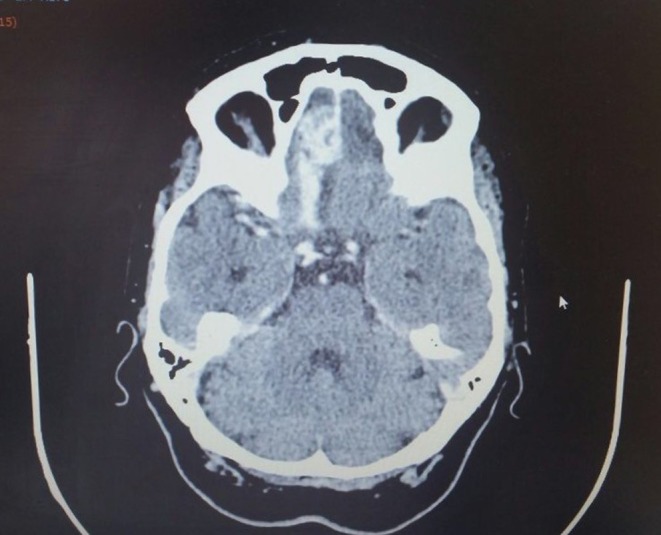
Axial CT of the patient, frontobasal meningioma in the olfactory groove on the right side. Secondary finding: subacute intracerebral hemorrhage in the frontal aspect on the right side in January 2011.
FDG PET/CT showed less enhancement of FDG in a contrast medium absorbing lesion frontobasal right which correlated with the meningioma.
DOTATATE PET revealed an uptake in the region mentioned earlier. Due to the fact that a less proportion of meningioma secrete phosphatonins, selective venous blood sampling was performed in June 2011 to determine the location of an FGF23-producing tumor.
A catheter was inserted into the corresponding veins at various locations with the aid of fluoroscopy, and blood samples were taken. FGF-23 was determined by ELISA. The highest FGF-23 values were noted in the right-sided jugular vein (1600 kRU/L), as shown in Fig. 2.
Figure 2.

FGF-23 levels at various locations, determined by selective venous blood sampling. Based on Putz/Pabst: Sobotta. Atlas der Anatomie des Menschen (Atlas of Human Anatomy), 21. Aufl. (21st edition), Urban & Fischer, 2000.
This value was 14.5-fold higher than the upper normal range for FGF-23 (26–110 kRU/L). Compared to serum values in the left-sided jugular vein, it was increased by 110 kRU/L.
Owing to the markedly elevated FGF-23 levels in the cerebral vascular system, the meningioma visualized on the imaging investigations was regarded as a possible source of FGF-23 production.
TIO-specific therapy
The patient’s hypophosphatemia was balanced by drug therapy. Treatment with calcitriol and phosphate led to a marked alleviation of her initial symptoms.
Weidner et al. and Crouzet et al. report a prompt improvement in their patients’ clinical symptoms after resection of FGF-23-producing tumors. Therefore, the indication for resection of the meningioma was established in our patients. In August 2011, we performed microsurgical tumor resection of the known cerebral space-occupying lesion on the right side in the olfactory groove, corresponding to the region of the highest serum FGF-23 levels on selective blood sampling. Histological investigation revealed the expected meningioma. Additionally, the tumor contained cells of a mesenchymal chondrosarcoma responsible for FGF-23 secretion.
Immediately after complete resection, the patient’s FGF-23 level was initially in the normal range (76 kRU/L), but rose two months after the intervention. Figure 3 shows the renewed rise in FGF-23 levels after the first resection. An endoscopic-assisted microsurgical resection was then performed at the skull base on 24 February, 2012. Immunohistochemistry confirmed a recurrence of the previously diagnosed tumor.
Figure 3.

FGF-23 levels in kRU/L over time (2011/2012).
Immediately post surgery and thereafter, the patient’s metabolic parameters, such as calcium phosphate and bone-specific alkaline phosphatase, were normal. As shown in Fig. 3, the production of FGF-23 dropped initially and then rose to pathological levels.
After the initial resection, the patient’s bone metabolism parameters in serum and the postoperative control scintigraphy revealed increasing bone consolidation with mild to moderately increased bone remodeling in the subcapital fractures of both upper arms and thighs (Fig. 4).
Figure 4.
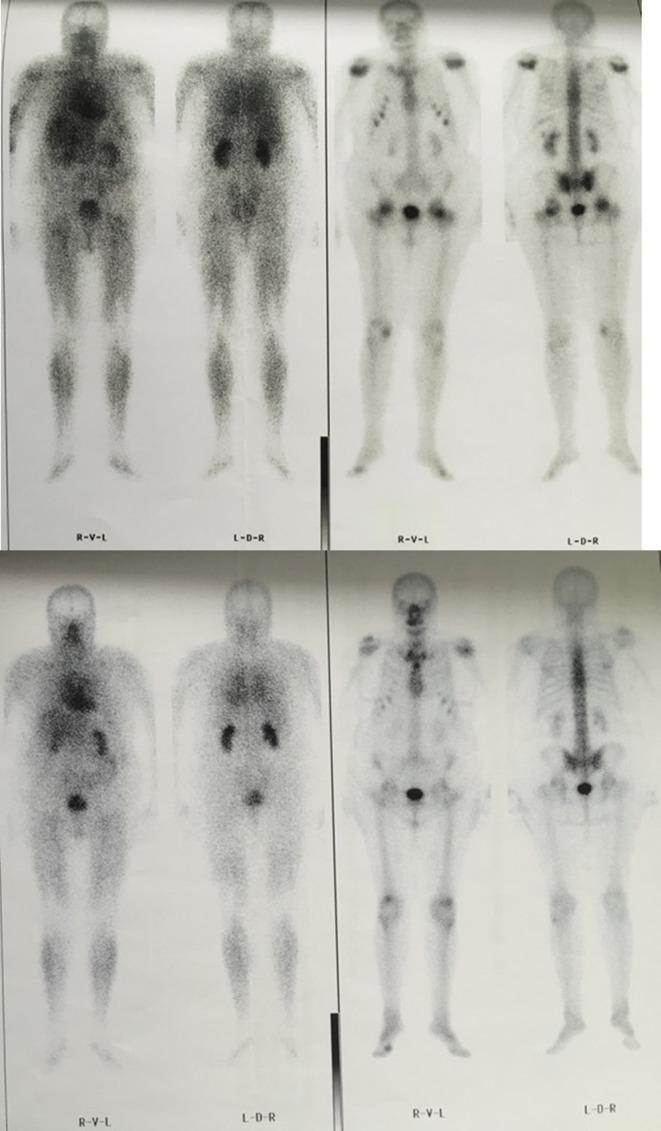
The patient’s bone scintigraphy showing a reduction in the intensity of bone remodeling, ‘adult rickety rosary’ sign and ‘tie sign of sternum’ in October 2014 (below) compared to a bone scintigraphy in 2010 (above).
Outcome
Owing to the laboratory values and the patient’s stable clinical condition, her drug therapy could be reduced. High-precision radiation with a cyberknife or stereotaxy was planned, but was then discarded because of the patient’s stable condition and the MRI of the head performed in September 2012, which ruled out the presence of a tumor.
Discussion
TIO, which is a rare condition compared to other paraneoplastic syndromes, is based on elevated serum levels of FGF-23 (2, 4). By inhibiting the co-transporter system and massive phosphate elimination, this type of tumor induces hypophosphatemia. Phosphate and calcium absorptions are reduced by the impaired activity of 1-alpa-hydroxylase in the kidney and consequently lowered calcitriol levels. Stimulation of renal 24-hydroxylase causes additional inactivation of 1,25-(OH)2D3 (5). The predominant function of calcitriol is to regulate the calcium absorption in the gut.
FGF-23-producing tumors are most frequently found in the craniofacial region in the paranasal sinuses (2). Though many such tumors arise from nasopharynx and the surroundings, they are not uncommon in the small bones of the extremities.
In the case presented here, the diagnosis was established over a period of two years. A further seven months elapsed until surgery was performed, revealing a TIO due to an FGF-23-producing mesenchymal tumor. Due to the patient’s complex symptoms, several medical specialties were involved in the diagnosis. Interestingly, it was finally the patient’s musculoskeletal decompensated pain syndrome, as described by Takeshi et al., which led to her being referred to the department of rheumatology.
MRI and PET/CT are useful investigations for tumor-specific diagnosis (6). However, it is the combination of MRI and selective blood sampling for FGF-23, which permits reliable identification of tumors causing TIO. According to Panagiota et al., it would not be appropriate to establish the diagnosis by selective blood sampling alone without imaging procedures (7). The clinical case presented here confirms the assumption that a combination of radiological procedures and selective blood sampling for FGF-23 leads to accurate localization of the tumor.
The purpose of selective venous sampling in TIO is to localize the tumor in image negative patients. In this particular patient, SVS was performed as meningioma is not a usual cause of TIO.
According to Ogura et al., resection is the most effective treatment of TIO (8). Takeshi et al. reported complete remission after extensive neurosurgical resection. In contrast, partial resection led to transient and incomplete remission with delayed healing (9).
We conclude that in a patient with generalized pain and reduced physical capacity, osteological parameters such as phosphate, 25-OH vitamin D3 and 1,25-(OH)2D3, as well as bone-specific alkaline phosphatase levels in serum should be determined. Hypophosphatemia should always lead to further diagnostic investigations aiming at the detection of an FGF-23-producing tumor. As described earlier, surgical resection may serve as a curative measure.
Declaration of interest
The authors declare that they have no competing interests and no conflicts of interest. The authors have full control of all primary data and agree to allow the journal to review their data if required.
Funding
This research did not receive any specific grant from any funding agency in the public, commercial or not-for-profit sector.
Author contribution statement
Prof. Dr Med. Hans-Christof Schober: Head physician, Department of Internal medicine and Endocrinology, TIO-specific diagnostic investigation; Prof. Dr Med. Christian Kneitz: Head physician, Department of Internal Medicine, Rheumatology/Immunology, TIO-specific diagnostic investigation; Dr Med. Franziska Fieber: Resident physician, Department of Internal Medicine, Rheumatology/Immunology; Dr Med. Kathrin Hesse: Resident physician, Department of Internal Medicine and Endocrinology; Prof. Dr Med. Henry Schroeder: Director Department of Neurosurgery, location of surgical resection.
References
- 1.Fukomoto S, Yamashita T. 2001. Fibroblast growth factor (FGF)-23 and hypophosphatemic rickets/osteomalacia. Endocrine Journal 48 603–610. ( 10.1507/endocrj.48.603) [DOI] [PubMed] [Google Scholar]
- 2.Folpe AL, Fanburg-Smith JC, Billings SD, Bisceglia M, Bertoni F, Cho JY, Econs MJ, Inwards CY, Jan de Beur SM, Mentzel T, et al. 2004. Most osteomalacia-associated mesenchymal tumors are a single histopathologic entity: an analysis of 32 cases and comprehensive review of literature. American Journal of Surgical Pathology 28 1–30. ( 10.1097/00000478-200401000-00001) [DOI] [PubMed] [Google Scholar]
- 3.Schapira D, Ben Izhak O, Nachtigal A, Burstein A, Shalom RB, Shagrawi I, Best LA. 1995. Tumor-induced osteomalacia. Seminars in Arthritis and Rheumatism 25 35–46. ( 10.1016/S0049-0172(95)80016-6) [DOI] [PubMed] [Google Scholar]
- 4.Jane de Beur SM, Streeten SA, Civelek AC, McCarthy EF, Uribe L, Marx SJ, Onobrakpeya O, Raisz LG, Watts NB, Sharon M, et al. 2002. Localisation of mesenchymal tumours by somatostatin receptor imaging. Lancet 359 761–763. ( 10.1016/S0140-6736(02)07846-7) [DOI] [PubMed] [Google Scholar]
- 5.Mirams M, Robinson BG, Mason RS, Nelson AE. 2004. Bone as a source of FGF-23: regulation by phosphate? Bone 35 1192–1199. [DOI] [PubMed] [Google Scholar]
- 6.Dupond JL, Mahmmedi H, Prie D, Collin F, Gil H, Blagosklonov O, Ricbourg B, Meaux-Ruault N, Kantelip B. 2005. Oncogenic osteomalacia: diagnostic importance of fibroblast growth factor 23 and F-18 fluorodeoxyglucose PET/CT scan for the diagnosis and follow up in one case. Bone 36 375–378. ( 10.1016/j.bone.2005.01.001) [DOI] [PubMed] [Google Scholar]
- 7.Andreopoulou P, Dumitrescu CE, Kelly MH, Brillante BA, Cutler Peck CM, Wodajo FM, Chang R, Collins MT. 2011. Selective venous catheterization for the localization of phosphaturic mesenchymal tumors. Journal of Bone and Mineral Research 26 1295–1302. ( 10.1002/jbmr.316) [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Ogura E, Kageyama K, Fukomoto S, Yagihashi N, Fukuda Y, Kikuchi T, Masuda M, Suda T. 2008. Development of tumor-induced osteomalacia in subcutaneous tumor, defined by venous blood sampling of fibroblast growth factor-23. Internal Medicine 47 637–641. ( 10.2169/internalmedicine.47.0761) [DOI] [PubMed] [Google Scholar]
- 9.Uno T, Kawai K, Kunii N, Fukumoto S, Shibahara J, Motoi T, Saito N. 2011. Osteomalacia caused by skull base tumors: report of 2 cases. Neursurgery 69 239–244. ( 10.1227/NEU.0b013e31821867f7) [DOI] [PubMed] [Google Scholar]