

Abstract
Our study investigated the relationship between BMI and bite size in a cafeteria setting. Two hundred and seventy one participants consumed one meal each. Participants were free to select any food provided by the cafeteria and could return for additional food as desired. Bite weights were measured with a table embedded scale. Data were analyzed with ANOVAs, regressions, Kolmogorov-Smirnov tests, and a repeated measures general linear model for quartile analysis. Obese participants were found to take larger bites than both normal (P=0.002) and overweight participants (p=0.017). Average bite size increased by 0.20 g per point increase in BMI. Food bites and drink bites were analyzed individually, showing 0.11 g/BMI and 0.23 g/BMI slopes, respectively. Quartiles of bites were also analyzed, and a significant interaction was found between normal and obese participants (p=0.034) such that the lower two quartiles were similar, but the upper two quartiles showed an increase in bite size for obese participants. The source of these effects could be the result of a combination of several uncontrolled factors.
Keywords: obesity, eating behavior, calorie intake, BMI, bite size
1. Introduction
The study of the microstructure of eating investigates physiological actions during consumption such as bite size (g), chewing rate (chews/swallow), eating rate (g/min or bites/min), and meal duration (min) [13, 27]. Differences in these measures between the lean and obese are sought to provide a basis for recommending behavior changes to treat obesity [25]. Example behaviors that have been studied include slowing eating rate [29, 30], chewing food more slowly [31], reducing visible portion size [1], and controlling bite size [26]. Many of these eating behaviors, including eating rate, bite size, and time each bite spends in the oral cavity, are inter-related [9, 10, 21].
This paper considers one specific component of the microstructure of eating, bite size, and relates this component to BMI. Previous studies have shown trends of larger sized bites for the obese compared to the lean, but were conducted in a laboratory setting and differences did not show statistical significance. For example, Hill and McCutcheon found a 0.8 g increase in bite size of donuts between the obese and non-obese, but the distributions of 7.1 ± 2.3 g (obese) and 6.3 ± 2.0 g were not statistically significantly different [14]. Spiegel reports a range of 0.2 to 2 g increase in average bite size of five different foods (chips, sandwich, bagel, cake, and cookie) between obese and non-obese participants, but again none of the differences reached statistical significance [25]. Park and Shin found a 0.2 to 0.4 g decrease in bite size of rice between obese and non-obese, but the study was designed to compare differences in gender and only compared 12 subjects in each group [20]. As noted by the authors of these studies, the inability to detect a bite size vs BMI difference may be due to a combination of the small size of the difference and an insufficient sample size to detect it. It may also be confounded by the limited number of foods tested.
The purpose of this study is to examine if the relationship between bite size and BMI seen in a laboratory setting can be observed in a less controlled environment. The secondary goal was to characterize the difference in bite size in terms of grams per BMI. The study took place in a cafeteria setting, and participants were free to select any food option available in the cafeteria that day. Each of the 271 participants’ meals were continuously weighed through use of scales embedded in the table with a cafeteria tray adhered to their tops. Video recording was used to provide visual verification of when bites were consumed.
2. Methods
2.1. Subjects
A total of 271 subjects (130 male, 141 female; age 18–75; BMI 17–46 kg/m2; ethnicity 189 Caucasian, 27 African-American, 2 American Indian or Alaska Native, 29 Asian or Pacific Islander, 11 Hispanic, and 13 Other) participated in the study. The participants were categorized into BMI groups, with 4 underweight (BMI < 18.5), 162 normal weight (18.5 ≤ BMI < 25), 66 overweight (25 ≤ BMI < 30), and 39 obese (BMI ≥ 30) determined by measured height and weight. Height and weight measures were taken in a laboratory before moving as a group to the cafeteria. Because only four underweight participants took place in this study, these four were excluded from categorical analysis of BMI. Each subject provided informed consent. The study was approved by the Clemson University Institutional Review Board for the protection of human subjects.
2.2. Food Selection
The data used in this study were recorded in the Harcombe Dining Hall of Clemson University. The facility seats up to 800 guests and provides hundreds of different foods and beverages. Subjects were free to select any available foods or beverages and make as many return trips as desired to obtain more food. Each such trip was referred to as a course. Participants selected 374 unique foods and beverages, and the most commonly selected items are summarized in previous articles [23, 24].
2.3. Procedure
The main purpose of the data collection was to support algorithm development in wrist motion tracking to automatically detect and count bites [6, 24]. Participants wore wrist motion trackers on their dominant wrist. The trackers were tethered to external computers; this data is not used in this paper. A second purpose of the data collection was to compare an estimate of kilocalories consumed to kilocalories predicted by the participant. A prior work estimated kilocalories consumed through use of a digital photography technique [23, 32], and this estimate is used in this work to facilitate meal level analysis. The full details of participant recruitment and scheduling are described in these previous works. A third purpose of the data collection was to support algorithm development for detecting and weighing individual bites using a table embedded scale [18]. These weights are analyzed in this paper and their calculations are described below. The following focuses on the aspects of the procedure most pertinent to the analysis reported in this paper.
An instrumented table was constructed consisting of four place settings. Each setting had a scale embedded in the table with a cafeteria tray adhered to its top. After collecting foods and beverages, each participant placed their dishes on top of the fixed tray to facilitate continuous weighing of the tray’s contents during consumption. Digital cameras in the ceiling were positioned to record each participant, including the tray, upper torso and head.
The actions of participants were unrestricted, meaning they could eat with either or both hands, consume foods and beverages in any order, mix foods, and remove foods from the tray and consume multiple bites without returning it to the tray in between bites. Foods were not preselected nor were they pre-cut into controlled sizes. Portion sizes were provided according to the standards served in the dining hall, but participants were free to request multiple portions. Participants were seated in groups of up to 4 to encourage socializing, and other activities such as talking on the phone were not prohibited. In summary, the environment was intended to be as natural as possible while still affording the ability to collect data.
2.4. Measures
The main measure used in this paper is bites that could be individually weighed by the scale. The times of bites were determined by reviewers watching the synchronized video of the participants eating and marking the times at which a bite of food or drink was consumed, identified as the time when placed into the mouth [24]. For all 271 subjects, a total of 24,101 bites were annotated. However, not all these bites could be individually weighed. Because our environment was not controlled, multiple bites could be taken without scale interaction, actions could be taken too quickly for the scale to stabilize, and interactions with non-food items (such as a utensil, napkin, or dish) could interfere with weighing individual bites.
Our group developed an algorithm based upon the concept of the universal eating monitor (UEM) [15] that uses a more sophisticated signal analysis to identify bites during unrestricted eating [18]. The algorithm identified time periods when the scale weight is stable and analyzed the surrounding weight changes. The series of preceding and succeeding weight changes was compared against patterns for single food bites, food mass bites, and drink bites to determine if a scale interaction was due to a bite or some other activity. Our algorithm correctly detected and weighed 39% of bites [18]. An analysis of bites that could not be weighed compared to those that could revealed no statistically significant difference in average weight [18].
2.5. Statistical analyses
Statistical analyses were performed using Statistical Product and Service Solutions (SPSS version 24.0). Descriptive statistics were performed on all data including means, standard deviations, and standard error of the means. An analysis of variance (ANOVA) was used to analyze differences between bite weights for normal, overweight, and obese groups. Regressions were performed to find the relationship between participant BMI and bite weight for all bites, food bites, and drink bites. A repeated measures general linear model was used to determine the interaction between BMI categories and mean quartile bite weights with three between-subjects BMI levels (normal, overweight, and obese) and 4 within-subjects bite quartiles (0–25th percentile, 25–50th percentile, 50–75th percentile and 75th–100th percentile). Finally, Kolmogorov-Smirnov tests were used to compare distributions of meal level variables for each BMI group including total grams consumed, kilocalories consumed, number of bites, number of courses, and duration of meal.
3. Results
Figure 1 shows each participant’s average bite weight plotted against their BMI. The regression for this data has a slope of 0.20 (indicating an increase of 0.20 grams in bite size per single BMI point increase) with R2 = 0.035.
Figure 1.
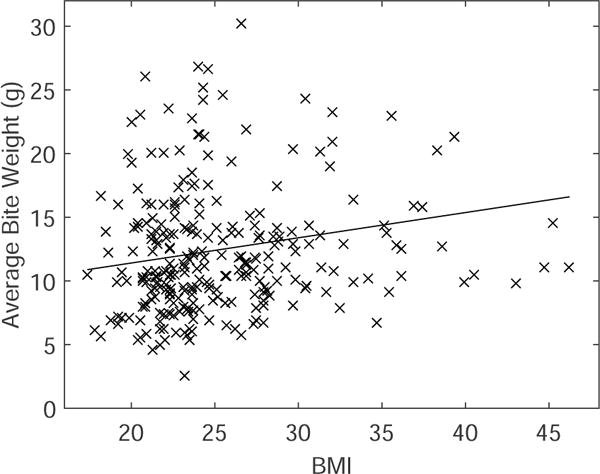
Plot comparing BMI to average bite weight per participant and trend line.
Figure 2 plots the average bite weight of normal weight, overweight and obese participants with standard errors and number of participants per category. We found a significant main effect of BMI in which obese individuals had higher bite weights than normal weight individuals and overweight individuals. The mean bite sizes and standard errors for normal weight, overweight, and obese are 12.0±.39 g/bite, 12.4±.64, and 15.0±1.1, respectively. Significant differences were found between normal and obese (p=0.002) and overweight and obese (p=0.017). No significant difference was found between normal and overweight (p=.595).
Figure 2.
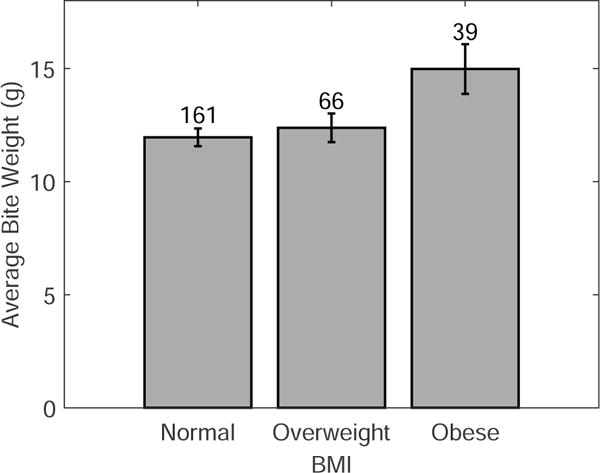
Average bite weight (±1 std err) and number of participants per BMI category.
Figure 3 shows the average bite weights across quartiles for each BMI group. Quartiles were determined by sorting all bites in each meal based on weight. The average bite weights for each quartile were found and compared across BMI groups. We found a significant interaction of BMI and quartile such that obese and normal weight individuals had similar bite weights in the lower quartiles, but obese individuals had larger bite weights in the upper quartiles (F[3,197] = 2.96, p=0.034). In addition, a similar interaction between overweight and obese approached significance (F[3,101] = 2.61, p=0.072). No significant difference was found between normal and overweight (F[3,224] = .73, p=.54).
Figure 3.
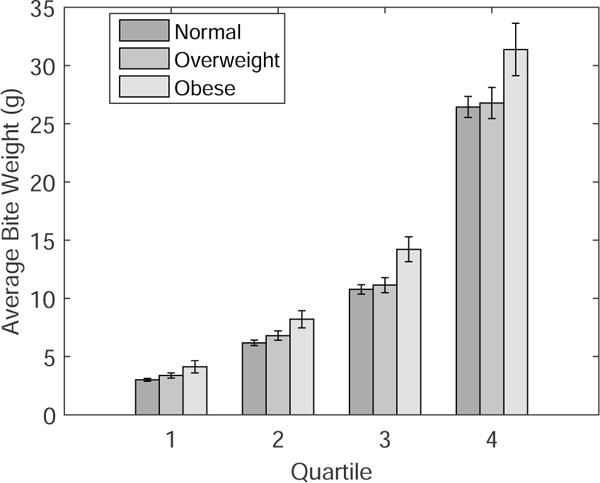
Mean bite weights (±1 std err) for each quartile of bites per BMI category.
In order to determine if the change in bite size with respect to BMI manifests itself at a meal level, Kolmogorov-Smirnov test were performed for several meal level variables shown in Table 1. No significant differences were found except for the percentage of drink bites consumed. For this variable, it was found that obese participants took a significantly larger percentage of drink bites than both normal (p=0.006) and overweight participants (p=0.013). Because of this, regressions for BMI and bite size were also performed for food bites and drink bites individually. For food bites, a slope of 0.11 g/BMI, with R2 = 0.029 was found, and for drink bites, a slope of 0.23 g/BMI was found, with R2 = 0.0084.
Table 1.
Statistical comparison of BMI groups across meal level variables including total grams consumed, kilocalories consumed, number of bites (both food and drink combined), number of courses, duration, and percent of total bites which were drink bites. Means ± standard errors shown.
| BMI | Grams | kCals | Bites | Courses | Duration (s) | Percent Drink |
|---|---|---|---|---|---|---|
| Normal | 818±27.1 | 1310±44 | 91.7±2.9 | 1.94±0.06 | 1290±34 | 16.5±1.18% |
| Overweight | 873±39.9 | 1210±61 | 87.4±4.6 | 1.85±0.09 | 1270±51 | 14.8±1.31% |
| Obese | 897±52.6 | 1330±103 | 80.1±5.4 | 1.95±0.13 | 1260±59 | 24.0±2.71% |
4. Discussion
The purpose of this study is to examine if the relationship between bite size and BMI seen in a laboratory setting can be observed in a less controlled environment. The secondary goal was to characterize the difference in bite size in terms of grams per BMI. Previous studies have indicated that a small effect of BMI on average bite size may be present. One study on donut consumption included 105 non-obese participants and 37 obese participants, where obesity was defined as more than 15% above optimal weight according to the Metropolitan Life Insurance Scale. This study indicated that one BMI index increase correlated to a 0.2 g bite size increase [14]. Another study consisted of 14 lean men and 12 obese men, where the BMI of lean participants ranged 19.5–25.8 and the BMI of obese participants ranged 31.8–54.5, consuming 5 different food types (chips, sandwich, bagel, cake, and cookie). The bite size differences with respect to food type ranged from approximately 0.02 – 0.15 g/BMI depending on the food consumed [26] (study 3). Our finding of a 0.20 g/BMI bite size increase was similar to both of these findings.
Differences in the microstructure of eating tend to be small. Finding these effects may require large sample sizes. One study with a smaller sample size (N = 28) indicated that participants with higher BMI appear to chew slightly longer than those with normal BMI, but there were not enough participants to demonstrate that the small effect was significant [31]. In contrast, one study examining 347 children [10] and another examining 254 participants [17] both found a significant, small effect between eating rate and BMI. Based on our results, the relationship between bite size and BMI is small and requires a large sample size in order to observe significance.
Most differences between groups in meal level variables were not significant. There did appear to be a trend indicating that obese individuals consumed fewer kilocalories than normal weight participants while eating approximately the same weight of food. This indicates that obese individuals may consume foods with a lower calorie density, although this speculation is based on results which were not found significant. We did find one significant meal level difference; the ratio of food and drink bites. Obese participants consumed 76.0% food and 24.0% drink bites, while normal weight participants consumed 83.5% food bites and 16.5% drink bites and overweight participants consumed 85.2% food bites and 14.8% drink bites. This finding explained some of the bite size increase we found, because across all bites, mean drink bite weight was significantly larger than mean food bite weight. However, the regressions performed for foods and drinks showed 0.11 g/BMI and 0.23 g/BMI increases respectively, indicating that the effect persists in both. The R-squared values we found for our BMI by bite weight regressions ranged from 0.0084-0.035 and suggest that bite size contributes only a very small amount (.85 – 3.5%) to the total variance in BMI. BMI is unlikely to be highly correlated with any single variable of the microstructure or macrostructure of eating. Rather, it is likely that many variables contribute small amounts to behaviors that collectively exert a larger influence on BMI.
Analyzing the data with respect to quartiles of bites and food selection, in an attempt to detect the source of this bite size by BMI interaction, yielded additional interesting results. The finding of a significant interaction between bite size, BMI group, and quartile indicated that the smallest half of bites for obese and normal weight individuals are similar, but the bite size difference results primarily from the largest half of bites consumed. An analysis of different foods would be interesting but is not supported by this study due to the fact that different foods were consumed at widely different frequencies based on subject choice.
Interventions to manipulate bite size have investigated several factors that can affect it. Increasing portion size has been shown to increase bite size in three studies [1, 3, 8]. In addition, one study found that bites of semi-solid foods were significantly smaller than bites of liquid consumption [5]. The presence of the child’s mother was shown to correlate to an increase in bite size in overweight children but not normal weight children [16]. Gender has also been found to affect bite size, with males taking larger bites than females [14, 20]. Thus, portion size, food viscosity, gender, and, in children, presence of a parent, could be controlled in future studies to help identify the source of the bite size by BMI correlation found. Finding a way to affect bite size could lead to additional effects on consumption. For example, one study showed that bite size has an effect on retro-nasal aroma release, which in turn contributes to meal termination [22]. In addition, two studies have shown that increasing bite size increases the amount of semisolid or liquid consumed in a meal [28, 33]. The present study demonstrates that the effect to eliminate is small (0.20 g/BMI) and that this number may be used as a goal in research on manipulating bite size.
While performing this study in a cafeteria environment allowed us to investigate natural behaviors, there are also limitations on the implications of our findings. The cause of the increase in bite size as related to BMI cannot be determined. It may be due to a variety of factors including food selection, eating rate, and other differences in eating habits. Future studies should balance design on key variables of interest, such as food choices, in order to search for causal factors. For example, the importance of oro-sensory exposure time has been shown to affect eating rate and contribute to satiation [4, 7, 12]. Bite size has also been related to chews per bite, as this moderates the link between bite size and eating rate[7, 11, 12]. In addition, food selection and food texture could play a significant role in relating consumption to BMI [2, 19], and future studies could seek to control food options in order to investigate this effect. Another limitation of our study includes an uneven BMI distribution as a result of the use of a convenience sample, which could be controlled in future studies. Also, all participants ate in a group setting in a cafeteria environment and were free to eat as many courses as desired, so it is possible results could only hold in this environment. In addition, while we believe the table embedded scale algorithm used in this study is robust enough to be used for repeated analyses, only one meal was recorded per participant, so consistency measures within participants could not be analyzed in this work. Nevertheless, a significant effect of BMI on average bite size was found, and the effect was in the same range as effects found in prior laboratory studies.
In conclusion, this study has provided evidence that obese individuals take significantly larger bites than normal weight or overweight individuals in a cafeteria setting. This effect is small, 0.20 g/BMI. In addition, a significant interaction between quartile of bites and BMI was found such that obese individuals took larger bites in the larger two quartiles of bites than normal weight individuals. The source of these phenomena is unclear. Further studies should search for their cause.
Highlights.
Bite weight differences between BMI groups were observed in a cafeteria setting.
Obese participants took larger bites than normal (p=0.002) and overweight (p=0.017).
A 0.20 g/BMI bite size relationship was observed.
Food and drink bites showed 0.11 and 0.23 g/BMI increases, respectively.
Acknowledgments
The work in this paper is partially supported by the National Institutes of Health (NIH) grants 1R41DK091141-01A1 and 2R42DK091141-02.
Footnotes
Publisher's Disclaimer: This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final citable form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.
Bibliography
- 1.Almiron-Roig E, Tsiountsioura M, Lewis H, Wu J, Solis-Trapala I, Jebb S. Large portion sizes increase bite size and eating rate in overweight women. Physiology and Behavior. 2015;139:297–302. doi: 10.1016/j.physbeh.2014.11.041. [DOI] [PubMed] [Google Scholar]
- 2.Bolhuis D, Forde C, CHeng Y, Xu H, Martin N, de Graaf C. Slow Food: Sustained Impact of Harder Foods on the Reduction in Energy Intake over the Course of the Day. PLoS One. 2014;9(4):e93370. doi: 10.1371/journal.pone.0093370. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Burger K, Fisher J, Johnson S. Mechanisms Behind the Portion Size Effect: Visibility and Bite Size. Obesity. 2011;19:546–551. doi: 10.1038/oby.2010.233. [DOI] [PubMed] [Google Scholar]
- 4.de Graaf C. Texture and satiation: The role of oro-sensory exposure time. Physiology and Behavior. 2012;107:496–501. doi: 10.1016/j.physbeh.2012.05.008. [DOI] [PubMed] [Google Scholar]
- 5.de Wijk R, Zijlstra N, Mars M, de Graaf C, Prinz J. The effects of food viscosity on bite size, bite effort and food intake. Physiology and Behavior. 2008;95:527–532. doi: 10.1016/j.physbeh.2008.07.026. [DOI] [PubMed] [Google Scholar]
- 6.Dong Y, Hoover A, Scisco J, Muth E. A New Method for Measuring Meal Intake in Humans via Automated Wrist Motion Tracking. Applied Psychophysiology and Biofeedback. 2016;37:205–215. doi: 10.1007/s10484-012-9194-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Ferriday D, Bosworth M, Godinot N, Martin N, Forde C, Van Den Heuvel E, Appleton S, Mercer Moss F, Rogers P, Brunstrom J. Variation in the Oral Processing of Everyday Meals Is Associated with Fullness and Meal Size; A Potential Nudge to Reduce Energy Intake? Nutrients. 2016;8(5):315. doi: 10.3390/nu8050315. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Fisher J, Kral T. Super-size me: Portion size effects on young children’s eating. Physiology and Behavior. 2008;94:39–47. doi: 10.1016/j.physbeh.2007.11.015. [DOI] [PubMed] [Google Scholar]
- 9.Fogel A, Goh A, Fries L, Sadananthan S, Velan S, Michael N, Tint M, Fortier M, Chan M, Toh J, Chong Y, Tan K, Yap F, Shek L, Meaney M, Broekman B, Lee Y, Godfrey K, Chong M, Forde C. A description of an ‘obesogenic’ eating style that promotes higher energy intake and is associated with greater adiposity in 4.5 year-old children: Results from the GUSTO cohort. Physiology and Behavior. 2017;176:107–116. doi: 10.1016/j.physbeh.2017.02.013. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Fogel A, Goh A, Fries L, Sadananthan S, Velan S, Michael N, Tint M, Fortier M, Chan M, Toh J, Chong Y, Tan K, Yap F, Shek L, Meaney M, Broekman B, Lee Y, Godfrey K, Chong M, Forde C. Faster eating rates are associated with higher energy intakes during an Ad libitum meal, higher BMI and greater adiposity among 4.5 year old children Results from the GUSTO cohort. British Journal of Nutrition. 2017;117(7):1042–1051. doi: 10.1017/S0007114517000848. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Forde C, van Kuijk N, Thaler T, de Graaf C, Martin N. Oral processing characteristics of solid savoury meal components, and relationship with food composition, sensory attributes and expected satiation. Appetite. 2013;60:208–219. doi: 10.1016/j.appet.2012.09.015. [DOI] [PubMed] [Google Scholar]
- 12.Forde C, Leong C, Chia-Ming E, McCrickerd K. Fast or slow-foods? Describing natural variations in oral processing characteristics across a wide range of Asian foods. Food & Function. 2017;8:595–606. doi: 10.1039/c6fo01286h. [DOI] [PubMed] [Google Scholar]
- 13.Guss J, Kissileff H. Microstructural analyses of human ingestive patterns: from description to mechanistic hypotheses. Neuroscience and Biobehavioral Reviews. 2000;24:261–268. doi: 10.1016/s0149-7634(99)00079-2. [DOI] [PubMed] [Google Scholar]
- 14.Hill S, McCutcheon N. Contributions of Obesity, Gender, Hunger, Food Preference, and Body Size to Bite Size, Bite Speed, and Rate of Eating. Appetite. 1984;5:73–83. doi: 10.1016/s0195-6663(84)80026-4. [DOI] [PubMed] [Google Scholar]
- 15.Kissileff H, Klingsberg G, Van Itallie T. Universal eating monitor for continuous recording of solid or liquid consumption in man. American Journal of Physiology - Regulatory, Integrative and Comparative Physiology. 1980;238(R14–R22) doi: 10.1152/ajpregu.1980.238.1.R14. [DOI] [PubMed] [Google Scholar]
- 16.Laessle R, Uhl H, Lindel B, Müller A. Parental influences on laboratory eating behavior in obese and non-obese children. International Journal of Obesity. 2001;25:S60–S62. doi: 10.1038/sj.ijo.0801701. [DOI] [PubMed] [Google Scholar]
- 17.Llewellyn C, van Jaarsveld C, Boniface D, Carnell S, Wardle J. Eating rate is a heritable phenotype related to weight in children. American Journal of Clinical Nutrition. 2008;88:1560–1566. doi: 10.3945/ajcn.2008.26175. [DOI] [PubMed] [Google Scholar]
- 18.Mattfeld R, Muth E, Hoover A. Measuring the consumption of individual solid and liquid bites using a table embedded scale during unrestricted eating. IEEE Journal of Biomedical and Health Informatics. 2016:1–1. doi: 10.1109/JBHI.2016.2632621. vol PP. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.McCrickerd K, Lim C, Leong C, Chia E, Forde C. Texture-Based Differences in Eating Rate Reduce the Impact of Increased Energy Density and Large Portions on Meal Size in Adults. The Journal of Nutrition. 2017;147(6):1208–1217. doi: 10.3945/jn.116.244251. [DOI] [PubMed] [Google Scholar]
- 20.Park S, Shin W. Differences in eating behaviors and masticatory performances by gender and obesity status. Physiology and Behavior. 2015;138:69–74. doi: 10.1016/j.physbeh.2014.10.001. [DOI] [PubMed] [Google Scholar]
- 21.Robinson E, Almiron-Roig E, Rutters F, de Graaf C, Forde C, Smith C, Nolan S, Jebb S. A systematic review and meta-analysis examining the effect of eating rate on energy intake and hunger. American Journal of Clinical Nutrition. doi: 10.3945/ajcn.113.081745. ajcn-081745. [DOI] [PubMed] [Google Scholar]
- 22.Ruijschop R, Zijlstra N, Boelrijk A, Dijkstra A, Burgering M, de Graaf C, Westerterp-Plantenga M. Effects of bite size and duration of oral processing on retro-nasal aroma release - features contributing to meal termination. British Journal of Nutrition. 2011;105:307–315. doi: 10.1017/S000711451000320X. [DOI] [PubMed] [Google Scholar]
- 23.Salley J, Hoover A, Wilson M, Muth E. Comparison between Human and Bite-Based Methods of Estimating Caloric Intake. Journal of the Academy of Nutrition and Dietetics. 2016;116:1568–4577. doi: 10.1016/j.jand.2016.03.007. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Shen Y, Salley J, Muth E, Hoover A. Assessing the Accuracy of a Wrist Motion Tracking Method for Counting Bites Across Demographic and Food Variables. IEEE Journal of Biomedical and Health Informatics. 2016;21:599–606. doi: 10.1109/JBHI.2016.2612580. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Spiegel T, Kaplan J, Tomassini A, Stellar E. Bite Size, Ingestion Rate, and Meal Size in Lean and Obese Women. Appetite. 1993;21:131–145. doi: 10.1016/0195-6663(93)90005-5. [DOI] [PubMed] [Google Scholar]
- 26.Spiegel T. Rate of intake, bites, and chews – the interpretation of lean - obese differences. Neuroscience and Biobehavioral Reviews. 2000;24:229–237. doi: 10.1016/s0149-7634(99)00076-7. [DOI] [PubMed] [Google Scholar]
- 27.Stellar E, Shrager E. Chews and swallows and the microstructure of eating. American Journal of Clinical Nutrition. 1985;42(5):973–982. doi: 10.1093/ajcn/42.5.973. [DOI] [PubMed] [Google Scholar]
- 28.Weijzen P, Smeets P, de Graaf C. Sip size of orangeade: effects on intake and sensory-specific satiation. British Journal of Nutrition. 2009;102:1091–1097. doi: 10.1017/S000711450932574X. [DOI] [PubMed] [Google Scholar]
- 29.Westerterp-Plantenga M, Westerterp K, Nicolson N, Mordant A, Schoffelen P, ten Hoor F. The shape of the cumulative food intake curve in humans, during basic and manipulated meals. Physiology and Behavior. 1990;47:569–576. doi: 10.1016/0031-9384(90)90128-q. [DOI] [PubMed] [Google Scholar]
- 30.Westerterp-Plantenga M. Eating behavior in humans, characterized by cumulative food intake curves - a review. Neuroscience and Biobehavioral Reviews. 2000;24:239–248. doi: 10.1016/s0149-7634(99)00077-9. [DOI] [PubMed] [Google Scholar]
- 31.White A, Venn B, Lu L, Rush E, Gallo L, Yong J, Farella M. A comparison of chewing rate between overweight and normal BMI individuals. Physiology and Behavior. 2015;145:8–13. doi: 10.1016/j.physbeh.2015.03.028. [DOI] [PubMed] [Google Scholar]
- 32.Williamson D, Allen H, Martin P, Alfonso A, Gerald B, Hunt A. Comparison of digital photography to weighed and visual estimation of portion sizes. Journal of the American Dietetic Association. 2003;103(9):1139–1145. doi: 10.1016/s0002-8223(03)00974-x. [DOI] [PubMed] [Google Scholar]
- 33.Zijlstra N, de Wijk R, Mars M, Stafleu A, de Graaf C. Effect of bite size and oral processing time of a semisolid food on satiation. American Journal of Clinical Nutrition. 2009;90:269–275. doi: 10.3945/ajcn.2009.27694. [DOI] [PubMed] [Google Scholar]