

Abstract
Background
Exposure to polychlorinated biphenyls (PCBs) is associated with depressive symptomatology. A cause of depressive symptoms is a disturbance in the neurotransmitter system of dopamine (DA). Animal as well as human studies report that PCBs can influence the DA system. This study examined whether PCB-related depressive symptoms are affected by DA metabolites in humans with high PCB body burden.
Methods
This study is part of the German HELPcB surveillance program (Health Effects in high Level exposure to PCB) for occupationally exposed workers and their relatives. Data was collected from 178 participants on two measurement time points (t1 and t2) with a one-year time lag in between the two time points. PCBs were analyzed in plasma via human biomonitoring and a validated questionnaire was used to identify existence and severity of depressive symptoms. As a surrogate for DA, we measured its metabolites homovanillic acid (HVA) and vanillylmandelic acid (VMA) in urine. Mediation analyses were performed to test whether the association between PCB exposure and severity of depressive symptoms is mediated by urinary concentration of DA metabolites HVA and VMA. The mediation was tested with the SPSS macro MEDIATE.
Results
We found a significant mediation over time for lower-chlorinated, higher-chlorinated and dioxin-like PCBs. The positive association between PCB exposure with severity of depressive symptoms was mediated by the main DA metabolite HVA. At t1 a higher exposure with PCBs was associated with lower concentration in urinary HVA. A reduced HVA concentration at t1 was correlated with increased depressive symptoms severity at t2. No meditations were found for VMA.
Conclusions
This work indicates that the association of PCB exposure and an increase of depressive symptoms after one year is mediated by the DA metabolite HVA as a surrogate for DA. These are first steps towards finding an explanation for an underlying neurochemical pathomechanism of PCB-related depressive symptomatology.
Electronic supplementary material
The online version of this article (10.1186/s12940-017-0316-3) contains supplementary material, which is available to authorized users.
Keywords: Polychlorinated biphenyls, Neurotoxicity, Neurotransmitter metabolites, Dopamine, Homovanillic acid, Vanillylmandelic acid, Depressive symptoms, Humans, Adults
Background
Polychlorinated biphenyls (PCBs) are a group of chemical substances, which had been commonly used in industrialized nations, because of their chemical and thermic stability, until their worldwide ban by the UNEP (United Nations Environment Programme) in 1995 [1]. PCBs can still be detected in the environment today, because of their high persistence. This high persistence is the reason why the general population has a background burden to PCBs with possible adverse health effects. Today individuals with higher PCB burden get primarily exposed to it in work contexts; for example during the recycling process of old electric devices produced prior to the ban of PCBs [2]. Exposure to PCBs has been associated with several adverse health effects, including: skin disease, abnormalities in liver function [3] and cancer [4]. Furthermore, preliminary results also suggest a potential negative impact on mental health. Peper et al. [5] found a moderate lower well-being in exposed teachers, who worked in a PCB contaminated school building. Seegal et al. [6] however report no correlation between PCBs and trait anxiety and depressive symptoms in former capacitor workers. In contrast, Kilburn et al. [7] found higher rates of depressive symptoms in PCB-exposed firefighters compared with a control group, but they found no direct association with PCB body burden. Conversely, Fitzgerald et al. [8] report a strong positive correlation between PCB body burden and depressive symptoms in elderly PCB exposed Hudson River residents. Similarly, in a prior longitudinal study, we found a higher risk for depressive syndrome in higher PCB-exposed individuals over a period of three years [9]. In summary, findings in the literature indicate a potential association of PCB exposure with depressive symptoms. The aim of this study is to explore potential neurophysiological mechanisms that link individual depressive symptoms to PCB exposure. Many mental disorders are associated with reduced concentrations in neurotransmitters. Especially in depression, lower levels of the monoamine neurotransmitters dopamine, serotonin and norepinephrine can be found [10]. For instance, a low dopamine (DA) level is associated with different types of depression [11] and depressive symptoms (i.e. motor-retardation; [12]). In this study, we focus on the neurotransmitter system of DA as possible path to explain the association of PCB exposure and depressive symptoms.
In the central nervous system (CNS), DA is produced in the presynaptic terminal and discharged from the vesicles into the synaptic cleft. It activates the DA receptors on the postsynaptic terminal and triggers an action potential. Thereafter, the DA transporter (DAT) takes the most of DA back into the presynaptic terminal, whereas another portion is metabolized into homovanillic acid (HVA) and vanillylmandelic acid (VMA) in the synaptic cleft. An alteration in the DA system may result in motor-retardation, a symptom that can also be seen in depressed patients [13]. Furthermore, clinically diagnosed depression is associated with lower levels of the metabolites HVA and VMA. Patients with DSM (Diagnostic and Statistical Manual of Mental Disorders) diagnosed depression show a lower HVA level in blood plasma than healthy controls [14]. Patients with clinically relevant depression have also been found to show a reduced VMA level in the cerebrospinal fluid (CSF) [15], and depressed patients at risk for suicide were found to demonstrate reduced HVA levels in their urine [16].
Neurotransmitter systems can be very sensitive to external influences, such as environmental toxicants like PCBs. A literature review shows that a significant body of research has already investigated the neurotoxic effects of PCBs in animals, and to a much lower extent in humans [17]. The majority of the mentioned studies in the review however examine neurodevelopmental effects, and research in adult humans with occupational exposure to PCBs is still rare until today. To the authors knowledge, Seegal et al. [18] and Putschögl et al. [19] are the only studies that investigate DA-related outcomes in occupational settings. Seegal et al. [18] found that an increase of PCB body burden is associated with a reduced DAT density, but this was only observed in women. Putschögl et al. [19] found a negative association between PCB body burden and urinary HVA as well as urinary VMA after work-related PCB exposure.
In this study, we examine whether DA level – reflected by urinary metabolite concentration – mediate the positive association of PCB body burden to depressive symptoms in individuals exposed to PCBs through their occupation (see Fig. 1). In the first hypothesis, we tested the direct path between PCB exposure and depressive symptoms. As reported in previous literature, we expect a positive association. In the mediation hypothesis we measure the urinary concentrations of the DA metabolites HVA and VMA as indicators for central DA level and hypothesize that there is an indirect path between the PCB body burden and depressive symptoms via alterations in the neurotransmitter DA reflected by urinary HVA and VMA level. Related to the indirect effect, we specifically postulate a negative association between PCB body burden and the DA metabolites HVA and VMA and between the DA metabolites and depressive symptoms. Extended to prior research, we further expect to find a cross-sectional as well as a longitudinal mediation between PCB body burden and depressive symptoms through DA metabolites HVA and VMA.
Fig. 1.
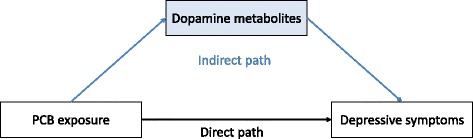
Hypothesized mediation model with direct and indirect path
Methods
Study population
This study was conducted as part of the long-term HELPcB (Health Effects in high Level exposure to PCB) surveillance program for former workers of a recycling company and surrounding companies with occupational PCB exposure and their relatives [20]. All participants received a yearly medical screening as part of the prevention program and the data used in this study was collected from two measurement time points in 2010 (t1) and 2011 (t2). Within these two measurement time points, 292 individuals participated at least at one measurement time (Fig. 2). In comparing drop-outs with the remaining participants, two reasons for a drop-out could be identified [21]. The first reason for remaining in the program was participants' satisfaction with the medical care. Participants who were more dissatisfied with the medical care in the program rather drop-out of the program. The second reason for leaving the program after t1 was related to problems in carrying out everyday tasks due to health problems. Participants who had fewer problems in carrying out their daily tasks rather left the program. A possible explanation may be that participants without or only few problems in carrying out their everyday tasks do not see the need to participate in the program. In total, 178 participants were included in this study, all of which participated in both measurement time points and did not take any dopamine-relevant medication such as antidepressants or Parkinson medication. The included participants did not significantly differ from the excluded ones in age, gender or liver function, nor in the PCB body burden, in depressive symptoms in terms of the sum score of the BDI or in the dopamine metabolites (data not shown). The mean age of the study population was 46.9 years (SD = 12.7 y), of which 155 (87.1%) were men and 23 (12.9%) women. In our study sample five (2.8%) participants left school without a degree, 71 (39.9%) had achieved a secondary school degree, 57 (32.0%) had a junior high school degree and 42 (23.6%) were awarded a university entrance diploma. The education status was unknown for three participants (1.7%).
Fig. 2.
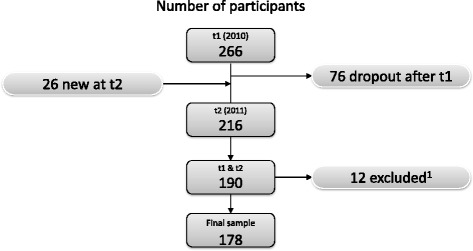
Flow-chart of the number of the study population. Note: t1 = measurement occasion 1, t2 = measurement occasion 2. 1excluded due to dopamine relevant medication, such as antidepressants or medication in Parkinson disease
Polychlorinated biphenyls
Data collection occurred at a university outpatient clinic for occupational medicine in the morning, where blood samples were collected from each participant for human biomonitoring. Participants were asked not to have breakfast before blood collection. The plasma was analyzed in our laboratory with gas chromatography and electron ionization-mass spectroscopy (please see Schettgen et al. [22, 23] for a detailed description of PCB detection in our study sample). To ensure the reproducibility as a marker for measurement quality of our results the between-day imprecision was determined. For this purpose, a quality control sample was analyzed in each analytical series and the mean values and standard deviation were determined for each congener. The results had a consistency of 5.9% to 7.4% with each other in the considered period indicating a good reproducibility. Furthermore, the accuracy of the determination of the indicator-PCBs in plasma was controlled by biannual successful participation in round robin exercises [24]. Six indicator PCB congeners (28, 52, 101, 138, 153 and 180) and twelve dioxin-like PCBs (77, 81, 105, 114, 118, 123, 126, 156, 157, 167, 169 and 189) were measured as part of the HELPcB program. From the above-mentioned dioxin-like PCBs, the four coplanar PCBs (77, 81, 126 and 169) were excluded from all analyses, as more than 80% of the participants showed values under the limit of detection (LOD). For a similar procedure see Lee et al. [25], Aminov et al. [26] or Fitzgerald et al. [8]. The LOD was 0.01 μg/L plasma and all values under the LOD were divided by two. With the remaining 14 PCB congeners three sum variables were created. According to the number of substituted chlorine atoms and the chemical structure, PCBs were categorized in lower-chlorinated biphenyls (LPCBs), higher-chlorinated biphenyls (HPCBs) and dioxin-like PCBs (dlPCBs). LPCBs have five or less substituted chlorine atoms and are more indicative of occupational exposure or exposure via inhalation, while HPCBs have more than five substituted chlorine atoms and instead reflect nutritional exposure and accumulate in the human adipose tissue over time. DlPCBs consist of lower- and higher-chlorinated PCBs but differ in their dioxin-like chemical structure. Therefore, we generated a third PCB group only with dlPCBs. The lower-chlorinated PCBs (PCB 28, PCB 52, PCB 101) were summed up into the variable LPCBs, the higher-chlorinated PCBs (PCB 138, PCB 153, PCB 180) to the variable HPCBs and the remaining dioxin-like PCBs (PCB 105, PCB 114, PCB 118, PCB 123, PCB 156, PCB 157, PCB 167 and PCB 189) to dlPCBs. For the dlPCBs no WHO toxic equivalency factor (WHO-TEF) was considered, because all used dlPCBs have the same WHO-TEF of 0.00003 [27]. To allow for clearer comparisons between the PCB body burden in our study sample and other study cohorts, we transformed the PCB variable from μg/L plasma in ng/g blood lipid and used the lipid-adjusted variables in all analyses. Cholesterol and triglycerides were detected in the serum and the total lipid level was calculated with the short formula from the CDC (Centers for Disease Control and Prevention [28]: total lipids = (2.27 * total cholesterol) + triglycerides +62.3 mg/dl). Afterwards we divided the PCBs in μg/L plasma by total lipids (g/L serum). The PCB body burden is stable over the measurement occasions. PCB level at t1 is highly correlated with PCB level at t2 (LPCBs: r = .96, p < .001; HPCBs: r = .98, p < .001; dlPCBs: r = .99; p < .001).
Transmitter metabolites
Urinary HVA and VMA as the main metabolites of the catecholamines DA are used as indicators to map out the central DA and NE concentration; a higher level of central DA is associated with more urinary metabolites [29, 30]. As a non-invasive method to assess neurotransmitter metabolism and turnover, random urinary samples were collected in the late morning between 9:00 a.m. and 11:00 a.m. The urine samples were stored at −20 °C and the concentration of HVA and VMA were detected via HPLC (high performance liquid chromatography). For a better interpretation of the metabolite concentration in random urine it is necessary to adjust for individual urine density [30, 31]. Therefore, Jaffe color reaction was used to analyze urinary creatinine concentrations and values are expressed as the ratio of HVA to creatinine and VMA to creatinine (HVA/Crea and VMA/Crea; both in μmol/g creatinine). Because the concentration of urinary DA-Metabolites depends to a large extent on liver function, albumin was determined as a marker for liver function in the serum. Furthermore, prior research reports that a higher concentration of urinary DA is associated with post-traumatic stress disorder [32]. In the current study, participants were asked how much they have been bothered by actual and prior traumatic experience.
Depressive symptoms
Depressive symptoms were measured using the updated version of Beck’s depression inventory (BDI-II; [33]). The BDI-II is a validated self-rating questionnaire that measures the severity of depressive symptoms and consists of 21 items with typical symptoms of depression such as “irritability” or “thoughts about suicide”. The participants were asked to specify how strong their symptoms were in the last two weeks. Each item has four options that range from 0 (the symptom is not manifested) until 3 (the symptom is strongly manifested). The internal consistencies were .91 at t1 and .92 at t2 thus showing a good reliability. To generate the outcome variable for each measurement occasion the answers from all BDI-II-items were added to a sum score. The sum scores can be interpreted as the severity of depressive symptomatology. In the following, we are referring to these outcome variables as “depressive symptoms”. Depressive symptoms at t1 highly correlate with depressive symptoms at t2 (r = .79, p < 001) and thus they are stable over time.
A statistical description of all relevant variables and their respective reference values are reported in Table 1.
Table 1.
Sample characteristics in terms of exposure, biochemistry and outcome (N = 178)
| reference value | t1 | t2 | |||||
|---|---|---|---|---|---|---|---|
| Mean ± SD | Median | Range | Mean ± SD | Median | Range | ||
| LPCBsa | 3.9a,c | 402.8 ± 1887.5 | 21.2 | 1.3–19,345.0 | 303.4 ± 1493.2 | 12.8 | 1.4–14,090.4 |
| HPCBsa | 264.8a,c | 964.9 ± 1780.3 | 331.0 | 40.5–13,855.3 | 901.2 ± 1646.7 | 302.1 | 43.1–11,794.2 |
| dlPCBsa | 30.7a,c | 345.4 ± 775.3 | 62.2 | 7.0–6051.8 | 313.7 ± 756.6 | 53.6 | 8.3–6342.9 |
| HVA/creab | <42b;d | 19.8 ± 9.2 | 18.1 | 6.3–79.0 | 22.3 ± 12.8 | 19.2 | 10.0–115.1 |
| VMA/creab | <30b;d | 15.4 ± 5.7 | 14.6 | 7.0–46.0 | 15.8 ± 6.2 | 15.3 | 2.2–48.8 |
| depressive symptoms | 18e | 6.3 ± 6.4 | 5.0 | 0–38 | 6.6 ± 7.0 | 5.0 | 0–40 |
Note: LPCBs lower-chlorinated biphenyls (28, 52, 101), HPCBs higher-chlorinated biphenyls (138, 153, 180), dlPCBs dioxin-like polychlorinated biphenyls (105, 114, 118, 123, 156, 157, 167, 189), HVA homovanillic acid, VMA vanillylmandelic acid, crea creatinine, SD standard deviation, t1 measurement occasion 1, t2 measurement occasion 2
ain ng/g lipid
bin μmol/g Crea
cmedian of PCB exposure in the German general population; data source Schettgen et al. [23]
dintern laboratory reference value
ecut of value for clinically relevant depression [50]
Statistical analyses
As the PCB sum variables were not normally distributed, we log-transformed them with a natural logarithm. Possible control variables (i.e. sex, age, education, work status, traumatic experience, co-exposure, total lipids and albumin) were analyzed with a directed acyclic graph. The online tool DAGitty version 2.3 was used to generate the graph [34]. The resulting graph is reported in Additional file 1: Figure S1. As minimal sufficient adjustment set three control variables were identified: 1) albumin as marker for liver function, 2) age as an influencing factor of PCB body burden and 3) traumatic experience as influencing factor for depressive symptoms as well as HVA level. Thus, we controlled for age and albumin in testing hypothesis 1 and we added traumatic experiences in all mediation analyses (hypothesis 2). The variable depressive symptoms at t1was included as further control variable in the longitudinal mediation analyses.
We analyzed the direct path between PCB body burden and depressive symptoms with multiple linear regression analyses to test the first hypothesis. PCB body burden was included as the independent variable, depressive symptoms as the dependent variable and age and albumin as control variables. The second hypothesis was tested with mediation analysis. The direct association of PCBs and depressive symptoms (hypothesis 1) is mediated by the levels of urinary DA metabolites HVA/crea and VMA/crea; specifically, PCB exposure is negatively associated with urinary DA metabolites. Reduced DA metabolites are in turn associated with more depressive symptoms. To test a mediation three steps have to be carried out [35]. Testing the direct path in hypothesis 1 is the first step (see Fig. 1). In the second step, the association between PCB body burden and the mediator (i.e. DA metabolites HVA/crea and VMA/crea) has to be tested. If both associations are significant, a mediation as the representing indirect path between the predictor and the outcome can be tested in the final step; both, PCB body burden and the DA metabolites are included in one model as independent variables. The direct path (i.e. the predictor variable) should lose its significant association with the outcome variable after including the mediator variable into the model. If the direct path is still significant, although the mediator variable has a significant effect on the outcome, it is called a partial mediation. The indirect path of PCB body burden and depressive symptoms through DA metabolites was tested with the MEDIATION macro for SPSS of Hayes [36]. At each measurement time point, depressive symptoms was used as the dependent variable, the respective PCB sum variables were included as independent variables and the metabolites HVA/crea and VMA/crea as mediators. The mediation analyses were performed to test cross-sectional mediations at t1 and t2 as well as to test longitudinal mediations with PCB exposure at t1 to depressive symptoms at t2.
All analyses were performed with IBM SPSS 21 for windows [37]. Due to the postulated directed hypotheses, the one-sided level of significance (p < .05) was used for the regression analyses. In the mediation tests, the 90%-confidence interval would be the equivalent for testing one-sided. Two analyses were performed for each hypothesis (cross-sectional and longitudinal) and thus a 95%-confidence interval was used to correct the tested indirect paths for multiple testing.
Results
Two hypotheses were tested in this study. In the first hypothesis, the direct effect of PCB body burden on depressive symptoms was analyzed. We find significant positive associations between LPCBs and depressive symptoms as well as between dlPCBs and depressive symptoms for both measurement occasions (Table 2). The association between HPCBs and depressive symptoms is only significant at t2, but not at t1. Hypothesis one can be confirmed except for HPCBs at t1.
Table 2.
Results of multiple linear regression analyses to test the direct path of PCB body burden and depressive symptoms (controlled for age and albumin)
| IV | B | S.E. | β | t | p | R2 |
|---|---|---|---|---|---|---|
| LPCBs_t1 | 0.81 | .32 | .28 | 2.56 | .01 | .07 |
| HPCBs_t1 | 1.00 | .55 | .19 | 1.81 | .07 | .04 |
| dlPCBs_t1 | 0.99 | .44 | .24 | 2.24 | .03 | .06 |
| LPCBs_t2 | 0.76 | .34 | .23 | 2.21 | .03 | .16 |
| HPCBs_t2 | 1.37 | .56 | .24 | 2.47 | .02 | .14 |
| dlPCBs_t2 | 1.28 | .44 | .28 | 2.88 | .005 | .19 |
Notes: PCBs polychlorinated biphenyls, LPCBs lower-chlorinated PCBs, HPCBs higher-chlorinated PCBs, dlPCBs dioxin-like PCBs, t1 measurement occasion 1, t2 measurement occasion 2, IV independent variable, B unstandardized regression coefficient, S.E. standard error, β standardized regression coefficient, t t-value, p p-value (significance), R 2 explained variance
In the second hypothesis, the indirect effect of PCB body burden on depressive symptoms mediated by DA metabolites HVA/crea and VMA/crea was investigated. There are no significant cross-sectional mediations for HVA/crea; neither for t1 nor for t2, but significant indirect paths over time are identified for all three PCB groups (i.e. LPCBs, HPCBs and dlPCBs; see Table 3). Specifically, HVA/crea at t1 partially mediates the association between PCB exposure at t1 and depressive symptoms at t2. After including the mediator, the direct path remains significant (see Fig. 3).
Table 3.
B-coefficients for indirect path of PCB body burden to depressive symptoms trough dopamine metabolites HVA/crea and VMA/crea (bootstrapping with N = 5000)
| Indirect path | Effect | S.E. (boot) | BC Bootstrapping 95% CI | |
|---|---|---|---|---|
| Lower limit | Upper limit | |||
| Mediator HVA/crea | ||||
| LPCB_t1 ➔ HVA/crea_t1 ➔ depressive symptoms_t1 | −.01 | .04 | −.10 | .05 |
| LPCB_t2➔ HVA/crea_t2 ➔ depressive symptoms_t2 | −.001 | .06 | −.11 | .13 |
| LPCB_t1 ➔ HVA/crea_t1 ➔ depressive symptoms_t21 | .10 | .05 | .02 | .24 |
| LPCB_t1➔ HVA/crea_t2 ➔ depressive symptoms_t2 | .06 | .08 | −.04 | .31 |
| HPCB _t1➔ HVA/crea_t1 ➔ depressive symptoms_t1 | −.01 | .07 | −.21 | .10 |
| HPCB _t2➔ HVA/crea_t2 ➔ depressive symptoms_t2 | .03 | .08 | −.09 | .24 |
| HPCB _t1➔ HVA/crea_t1 ➔ depressive symptoms_t21 | .22 | .10 | .06 | .50 |
| HPCB _t1➔ HVA/crea_t2 ➔ depressive symptoms_t2 | .08 | .13 | −.10 | .49 |
| dlPCB_t1 ➔ HVA/crea_t1 ➔ depressive symptoms_t1 | −.01 | .05 | −.15 | .08 |
| dlPCB_t2 ➔ HVA/crea_t2 ➔ depressive symptoms_t2 | .02 | .07 | −.08 | .20 |
| dlPCB_t1 ➔ HVA/crea_t1 ➔ depressive symptoms_t21 | .17 | .08 | .05 | .36 |
| dlPCB_t1 ➔ HVA/crea_t2 ➔ depressive symptoms_t2 | .08 | .11 | −.06 | .41 |
| Mediator VMA/crea | ||||
| LPCB_t1 ➔ VMA /crea_t1 ➔ depressive symptoms_t1 | .00 | .01 | −.02 | .05 |
| LPCB_t2➔ VMA /crea_t2 ➔ depressive symptoms_t2 | −.00 | .02 | −.05 | .04 |
| LPCB_t1 ➔ VMA /crea_t1 ➔ depressive symptoms_t2 | .00 | .05 | −.06 | .10 |
| LPCB_t1➔ VMA /crea_t2 ➔ depressive symptoms_t2 | −.00 | .04 | −.09 | .08 |
| HPCB _t1➔ VMA /crea_t1 ➔ depressive symptoms_t1 | .00 | .03 | −.04 | .08 |
| HPCB _t2➔ VMA /crea_t2 ➔ depressive symptoms_t2 | .00 | .03 | −.06 | .08 |
| HPCB _t1➔ VMA /crea_t1 ➔ depressive symptoms_t2 | −.01 | .09 | −.08 | .21 |
| HPCB _t1➔ VMA /crea_t2 ➔ depressive symptoms_t2 | .00 | .07 | −.15 | .14 |
| dlPCB_t1 ➔ VMA /crea_t1 ➔ depressive symptoms_t1 | −.00 | .02 | −.59 | .04 |
| dlPCB_t2 ➔ VMA /crea_t2 ➔ depressive symptoms_t2 | .00 | .03 | −.05 | .07 |
| dlPCB_t1 ➔ VMA /crea_t1 ➔ depressive symptoms_t2 | .01 | .08 | −.07 | .17 |
| dlPCB_t1 ➔ VMA /crea_t2 ➔ depressive symptoms_t2 | .00 | .05 | −.10 | .12 |
Notes: PCBs polychlorinated biphenyls, LPCBs lower-chlorinated PCBs, HPCBs higher-chlorinated PCBs, dlPCBs dioxin-like PCBs, HVA homovanillic acid, VMA vanillylmandelic acid, crea creatinine, t1 measurement occasion 1, t2 measurement occasion 2, S.E. (boot) bootstrapped standard error, BC bias corrected, CI confidence interval; 1 significant mediations are in italic (p < .05)
Fig. 3.
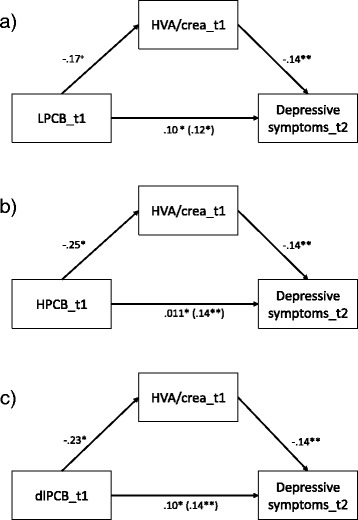
Illustration with standardized-b-coefficients of the longitudinal indirect paths of PCB to depressive symptoms through HVA/crea. Note: HPCB = higher-chlorinated PCBs, dioxin-like PCBs, HVA = homovanillic acid, t1 = measurement occasion 1, t2 measurement occasion 2; + = p < .10 (1-sided), * = p < .05 (1-sided)
Exposure with PCBs at t1 predicts depressive symptoms at t2. These direct effects are mediated by HVA/crea at t1. Detailed information regarding the analyses is reported in Tables 4, 5 and 6 and illustrations of the significant indirect paths with standardized beta coefficients are represented in Fig. 3. Thus, our longitudinal hypothesis can be partially confirmed for one indirect path via HVA/crea for all groups of PCBs (i.e. LPCBs, HPCBs and dlPCBs).
Table 4.
Results of the mediation analyses of LPCB body burden and depressive symptoms through HVA/crea using MEDIATE macro for SPSS [30]; controlled for age, albumin and traumatic experience
| Coefficient | SE | t | p | |
|---|---|---|---|---|
| Total effect model (DV = depressive symptoms_t2) | ||||
| LPCBs | .48 | .24 | 2.05 | .02 |
| Covariates | ||||
| Age | −.05 | .04 | −1.17 | .12 |
| Albumin | −.12 | .19 | −0.60 | .28 |
| Traumatic experience | 1.62 | 1.37 | 1.18 | .12 |
| Depressive symptoms_t1 | .75 | .09 | 8.60 | <.001 |
| Model fit | ||||
| R2 | .62 | <.001 | ||
| F | 26.67 | |||
| Effect of IV on HVA (mediator) | ||||
| LPCBs | −.75 | .50 | −1.50 | .07 |
| Effect of IV and mediator on depressive symptoms_t2 | ||||
| HVA/crea | −.13 | .05 | −2.61 | .01 |
| LPCBs | .38 | .23 | 1.67 | <.05 |
| Model fit | ||||
| R2 | .65 | <.001 | ||
| F | 24.92 | |||
| Homogeneity of regression (LPCB*HVA) | ||||
| R2 | .0004 | .38 | ||
| F | 0.10 | |||
Note: DV dependent variable, IV independent variable, t1 measurement occasion 1, t2 measurement occasion 2, LPCBs lower-chlorinated biphenyls, HVA homovanillic acid / creatinine, R 2 explained variance, F F-value, SE standard error, t t-value, p p-value (significance)
Table 5.
Results of the mediation analyses of HPCB body burden and depressive symptoms through HVA/crea using MEDIATE macro for SPSS [30]; controlled for age, albumin and traumatic experience
| Coefficient | SE | t | p | |
|---|---|---|---|---|
| Total effect model (DV = depressive symptoms_t2) | ||||
| HPCBs | .94 | .39 | 2.40 | .01 |
| Covariates | ||||
| Age | −.08 | .04 | −1.96 | .03 |
| Albumin | −.14 | .19 | −.72 | .27 |
| Traumatic experience | 1.61 | 1.36 | 1.19 | .12 |
| Depressive symptoms_t1 | .75 | .09 | 8.79 | <.001 |
| Model fit | ||||
| R2 | .62 | <.001 | ||
| F | 27.45 | |||
| Effect of IV on HVA (mediator) | ||||
| HPCBs | −1.84 | .82 | −2.24 | .02 |
| Effect of IV and mediator on depressive symptoms_t2 | ||||
| HVA/crea | −.12 | .05 | −2.40 | .01 |
| HPCBs | .71 | .39 | 1.82 | .04 |
| Model fit | ||||
| R2 | .65 | <.001 | ||
| F | 25.17 | |||
| Homogeneity of regression (HPCB*HVA) | ||||
| R2 | .002 | .25 | ||
| F | 0.47 | |||
Note: DV dependent variable, IV independent variable, t1 measurement occasion 1, t2 measurement occasion 2, HPCBs higher-chlorinated biphenyls, HVA homovanillic acid/creatinine, R 2 explained variance, F F-value, SE standard error, t t-value, p p-value (significance)
Table 6.
Results of the mediation analyses of dlPCB body burden and depressive symptoms through HVA/crea using MEDIATE macro for SPSS [30]; controlled for age, albumin and traumatic experience
| Coefficient | SE | t | p | |
|---|---|---|---|---|
| Total effect model (DV = depressive symptoms_t2) | ||||
| dlPCB | .80 | .31 | 2.56 | .02 |
| Covariates | ||||
| Age | −.06 | .04 | −1.56 | .07 |
| Albumin | −.14 | .19 | −.72 | .24 |
| Traumatic experience | 1.75 | 1.36 | 1.29 | .10 |
| Depressive symptoms_t1 | .74 | .09 | 8.62 | <.001 |
| Model fit | ||||
| R2 | .63 | <.001 | ||
| F | 27.86 | |||
| Effect of IV on HVA (mediator) | ||||
| dlPCB | −1.40 | .67 | −2.10 | .02 |
| Effect of IV and mediator on depressive symptoms_t2 | ||||
| HVA/crea | −.12 | .05 | −2.41 | .01 |
| dlPCB | .63 | .31 | 2.03 | .03 |
| Model fit | ||||
| R2 | .65 | <.001 | ||
| F | 25.53 | |||
| Homogeneity of regression (HPCB*HVA) | ||||
| R2 | .002 | .27 | ||
| F | 0.39 | |||
Note: DV dependent variable, IV independent variable, t1 measurement occasion 1, t2 measurement occasion 2, dlPCBs dioxine-like polychlorinated biphenyls; HVA = homovanillic acid / creatinine, R 2 explained variance, F F-value, SE standard error, t t-value, p p-value (significance)
For VMA/crea neither the cross-sectional nor the longitudinal indirect paths are significant. Thus, for VMA/crea the second hypothesis is not supported.
Discussion
Occupational and environmental exposures to PCBs have been associated with reduced well-being and depressive symptomatology [9]. In the present study, we investigated whether this effect is mediated through the urinary DA metabolites HVA and VMA. The mediations were tested cross-sectionally and longitudinally; cross-sectional results were non-significant. However, longitudinally LPCBs, HPCBs and dlPCBs showed a negative association with HVA at t1 and these reduced HVA levels were in turn associated with an increase in depressive symptoms at t2. An increase in LPCBs of 10 ng/g lipids results in one additional depressive symptom (of the 21 queried symptoms) through the mediator HVA. Respectively, an increase of approximately 5 ng/g lipids in HPCBs or in dlPCBs also results in one additional depressive symptom via the HVA as the mediator. These results indicate that PCB-related depressive symptomatology may be related to lower levels of central DA as they are reflected in lower levels of HVA.
The longitudinal mediation of PCB exposure via HVA/crea on depressive symptoms is in line with prior studies. Seegal et al. [38] exposed apes to different PCBs over 20 weeks and reported reduced DA concentrations in the striatum directly after the exposure. A system within the basal ganglia, the striatum, subserves motor, cognitive and limbic functions such as drive, learning, memory, emotion and vegetative regulation. Whilst there was a correlation between PCB exposure and the DA concentration directly after exposure, no correlation was found 24 and 44 weeks later, despite the DA concentration still being reduced. One explanation for these findings might be that PCBs cause irreversible damage to brain structures such as the death of dopaminergic neurons [38]. In fact, we also found a significant mediation only over time (after 56 weeks), but not cross-sectionally. Cell death of dopaminergic neurons can be a consequence of blocked vesicular monoamine transporter 2 (VMAT2). Richardson & Miller [39] report that an exposure with PCBs can cause lower reactivity of VMAT2. The authors suggested that DA cannot be transported in the vesicle and will be anaerobically metabolized in the presynapsis. Reactive oxygen species (ROS) will then be produced destroying the neuron and leading to cell death [40]. Finally, a reduced frequency of dopaminergic neurons will potentially lead to a reduced DA concentration in the striatum and cause depressive symptoms [13]. These findings may explain why we found mediations only occurring over time.
We did not identify any mediation of PCBs through VMA on depressive symptoms. A reason for this may be the metabolite itself. Primarily, HVA is the main metabolite of DA but VMA also of norepinephrine (NE). Although NE is transformed from DA, the results related to VMA may also be influenced by NE and its function as a stress hormone. NE is increased in moments of acute stress [41]. Paris et al. [42] report, that a thoracic computed tomography (CT) is associated with more psychological distress in asbestos exposed participants, who are aware of asbestos-related health risks. Thus, it can be argued that the examination itself triggers the perception of health risks related to PCB exposure in our cohort and this may be a source of stress for participants, and may therefore influence acute NE levels. This could make it difficult to identify an indirect effect via VMA. Furthermore, in our study we are not able to differentiate the separate effects of DA and NE related to VMA. Jimerson et al. [15] report a six times stronger reduced CSF-HVA level than CSF-VMA level in depressed participants. Thus, it is possible that our study population is too small to detect the weaker effect in VMA.
One strength of our study is that the found effects are free from a common-method bias typically discussed in psychological and social science research. Effects may be overestimated, due to the use of the same method to assess predictor and outcome variables. In the current study, different methods were used to assess predictor, mediator and outcome variable. PCBs were measured in blood plasma, DA metabolites in urine and depressive symptoms with a standardized screening questionnaire. Thus, a common-method-bias that overestimates our results can be excluded.
A systematic drop-out of study participants could also bias our results. There were many drop-outs in our study population, but analyses show, that there are no systematic differences in the relevant variables used in the current study. A strength of this study is the one year time lag between the measurement occasions. Depressive symptoms may be related to autumn and winter season [43]. Using yearly time intervals can reduce a possible bias due to seasonal influences on depressive symptomatology.
The longitudinally indirect effects may be weak. However, it needs to be considered that also many control variables were included. In the longitudinal analyses it was controlled for age, Albumin, traumatic experience and depressive symptoms at t1. Including depressive symptoms at t1 was necessary for the identification of the longitudinal indirect effect on depressive symptoms at t2, but this variable can explain much of the variance of depressive symptoms at t2. Therefore, it is a strength of the present study that we found significant mediations although we controlled for depressive symptoms at t1. This allows interpreting the results regarding the levels of DA metabolite HVA at t1 as an induced change in depressive symptoms at t2.
In epidemiologic research about hazardous substance exposure, it is necessary to discuss possible co-exposure to other substances. PCBs may be not the only hazardous substance that our study population is exposed to. The WHO TEQ for dioxins and furans was analyzed in our study cohort. However a co-exposure to other toxins does not produce an open backdoor-path in the DAG (see Additional file 1: Figure S1), because there is no association of dioxins and furans with depression; thus it is not part of the minimal adjustment set.
It is also important to note that the urinary metabolites may have originated in physiological structures other than the brain. For instance, only 12% of the urinary HVA originates from central DA [44]. Further, 94% of the urinary VMA originate from the liver [29] and PCBs are suspected to influence hepatic function [3]. The different sources of HVA and VMA may reduce the capacity of the study to detect a stronger effect on the outcome variable. Nevertheless, the use of urinary metabolites is a non-invasive method and we controlled for albumin as marker for liver function and also liver dysfunction in all analyses. Thus, abnormalities in liver function cannot explain the indirect effect of HVA related to depressive symptoms. Albumin is also a possible marker of longitudinal alcohol consumption, but by including albumin as control variable, we also controlled for longitudinal alcohol consumption. Furthermore, it has been reported that the measurement of HVA in blood correlates with renal clearance. Lambert et al. [45] conclude that blood concentration of HVA does not necessarily reflect the metabolism of DA but also depends on the amount of renal clearance. By measuring the urinary HVA we are able to control for renal clearance and urine density by adjusting for creatinine.
Finally, a controversial discussion in the literature focuses on the “dopamine hypothesis”, which states that low DA concentration may also cause depressive symptoms. It has been argued that DA is only relevant in certain forms of depressive symptoms (i.e. motor retardation [13]). Nevertheless, in our data there were no specific symptoms responsible for the association. This was true of symptoms related to motor activity as well as other symptoms measured (post hoc tests not shown in tables).
When interpreting the present findings, it is important to keep in mind that our study sample had a higher exposure to PCBs compared to other study samples where the impact of PCB exposure on mental health has been investigated (see Additional file 1: Table S1). This might explain why we were able to detect such small effects. Our work provides the first insight into a potential mechanism by which high-level PCB exposure influences the DA neurotransmitter system and increases symptoms over time. Yet, the pathophysiology of depression involves a complex interaction of neurotransmitters, hormones or behavioral factors. In order to address this complexity, future research should assess serotonin, which also plays a role in the development of depressive symptoms according to drug studies [46]. Additionally, the impact of other organ systems such as the thyroid gland should be considered, since PCBs have been argued to disturb thyroid hormones [47] and hypothyroidism is associated with depressive symptoms [48]. Finally, psychological mechanisms should also be considered when investigating the development of depressive symptoms after hazardous substance exposure. In a review, it was reported that patients show more depressive symptoms short time after getting the information of higher risk for developing a chronic disease [49]. A hazardous substance exposure might be threatening, because individuals are aware of the increased risk for developing a severe illness (i.e. cancer). Thus, this knowledge might cause a perceived health threat and may also play a role in developing mental syndromes [7, 9].
Conclusion
We were able to support prior findings that a high PCB body burden is associated with more depressive symptoms. Furthermore, this study gives first hints that the relationship between all types of PCB exposure (LPCB, HPCB and dlPCB) with depressive symptoms may be mediated by alterations in DA metabolism over time. This study encourages further research to investigate the impact of PCBs on other monoamine neurotransmitters, in order to learn more about underlying pathomechanisms of PCBs and mental health.
Acknowledgements
Special thanks go to the staff of the Out-patient Clinic of Occupational Medicine at the university hospital RWTH Aachen for their collaboration in patient recruitment and data collection as well as to Dr. Roland Hansen and his team from the laboratory of the University Hospital RWTH Aachen. We further thank all reviewers for their helpful comments to prior drafts of this manuscript.
Funding
This work was supported by the Institution for Statutory Accident Insurance and Prevention in the Energy, Textile, Electrical, and Media Industry (BGETEM), Cologne, Germany [grant number 360328]. The University Hospital Aachen, RWTH Aachen University, Germany was awarded an unrestricted grant to carry out this research.
Availability of data and materials
The datasets analyzed during the current study are not publicly available. In the agreements of the HELPcB program, participant- and health-related raw data are not allowed to be shared, but anonymized data of the scales are available from the corresponding author upon reasonable request.
Abbreviations
- BDI-II
Beck’s depression inventory II (German version)
- CDC
Centers for disease control and prevention
- Crea
Creatinine
- CSF
Cerebrospinal fluid
- DA
Dopamine
- DAT
Dopamine transporter
- dlPCBs
Dioxin-like polychlorinated biphenyls
- DSM-IV
Diagnostic and Statistical Manual of Mental Disorders IV
- HELPcB
Health effects in high level exposure to PCB
- HPCBs
Higher chlorinated biphenyls
- HPLC
High performance liquid chromatography
- HVA
Homovanillic acid
- LOD
Limit of detection
- LPCBs
Lower chlorinated biphenyls
- NE
Norepinephrine
- PCBs
Polychlorinated biphenyls
- VMA
Vanillylmandelic acid
Additional file
Directed acyclic graph to identify relevant control variables. Table S1. Mean PCB exposure of our study cohort in comparison to other study cohorts; sorted by PCB exposure (DOCX 89 kb)
Authors’ contributions
All authors revised the manuscript and gave substantial intellectual input during the preparation process. PMG performed the psychological screening, wrote the first draft of the manuscript, analyzed and interpreted the data and created the figures and Tables. MG performed the medical examinations and the medical interviews in the HELPcB program. TS analyzed the PCBs and supported the examination and interpretation of the PCB values related to references. FMP supported the data collection and coordinated the analyses of the neurotransmitter metabolites in the urine samples. TK performed medical examinations and designed the HELPcB program. BF designed the neuropsychological part of the HELPcB program and provided professional advice in neuropsychology. JL performed the psychological screening and supported statistical data analyses and provided professional advice in health psychology, data interpretation and result discussion. All authors read and approved the final manuscript.
Ethics approval and consent to participate
The HELPcB program was approved by the local ethics committee of the Medical Faculty of the RWTH Aachen University (EK 176/11). Informed consent was obtained from all participants included in the study.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Footnotes
Electronic supplementary material
The online version of this article (10.1186/s12940-017-0316-3) contains supplementary material, which is available to authorized users.
Contributor Information
Petra Maria Gaum, Phone: +49 241 80 89040, Email: pgaum@ukaachen.de, http://www.arbeitsmedizin.ukaachen.de.
Monika Gube, Email: monika.gube@staedteregion-aachen.de.
Thomas Schettgen, Email: tschettgen@ukaachen.de.
Franziska Maria Putschögl, Email: franziska.putschoegl@zi-mannheim.de.
Thomas Kraus, Email: tkraus@ukaachen.de.
Bruno Fimm, Email: bfimm@ukaachen.de.
Jessica Lang, Email: jlang@ukaachen.de.
References
- 1.UNEP – United Nations Environment Programme: Decision 18/32 of the UNEP Governing Council: Persistent Organic Pollutants. 1995. http://www.pops.int/documents/background/gcdecision/18_32/gc1832en.html. Accessed 13 July 2017.
- 2.Wolff MS. Occupational exposure to polychlorinated biphenyls (PCBs) Environ Health Persp. 1985;60:133–138. doi: 10.1289/ehp.8560133. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Longnecker MP, Rogan WJ, Lucier G. The human health effects of DDT (dichlorodiphenyltrichloroethane) and PCBs (polychlorinated biphenyls) and an overview of organochlorines in public health. Annu Rev Publ Health. 1997. https://doi.org/10.1146/annurev.publhealth.18.1.211. [DOI] [PubMed]
- 4.Lauby-Secretan B, Loomis D, Grosse Y, El Ghissassi F, Bouvard V, Benbrahim-Tallaa L, et al. Carcinogenicity of polychlorinated biphenyls and polybrominated biphenyls. Lancet Oncol. 2013. doi:10.1016/S1470-2045(13)70104-9. [DOI] [PubMed]
- 5.Peper M, Klett M, Morgenstern R. Neuropsychological effects of chronic low-dose exposure to polychlorinated biphenyls (PCBs): a cross-sectional study. Environ. Health. 2005. doi:10.1186/1476-069X-4-22. [DOI] [PMC free article] [PubMed]
- 6.Seegal RF, Fitzgerald EF, McCaffrey RJ, Shrestha S, Hills EA, Wolff MS, et al. Tibial bone lead, but not serum polychlorinated biphenyl, concentrations are associated with neurocognitive deficits in former capacitor workers. J Occup Environ Med. 2013. doi:10.1097/JOM.0b013e318285f3fd. [DOI] [PubMed]
- 7.Kilburn KH, Warsaw RH, Shields MG. Neurobehavioral dysfunction in firemen exposed to polychlorinated biphenyls (PCBs): possible improvement after detoxification. Arch Environ Health. 1989. doi:10.1080/00039896.1989.9935904. [DOI] [PubMed]
- 8.Fitzgerald EF, Belanger EE, Gomez MI, Cayo M, McCaffrey RJ, Seegal RF, et al. Polychlorinated biphenyl exposure and neuropsychological status among older residents of upper hudson river communities. Environ Health Persp. 2008. doi:10.1289/ehp.10432. [DOI] [PMC free article] [PubMed]
- 9.Gaum PM, Esser A, Schettgen T, Gube M, Kraus T, Lang J. Prevalence and incidence rates of mental syndromes after occupational exposure to polychlorinated biphenyls. Int. J. Hyg. Environ. Health. 2014. https://doi.org/10.1016/j.ijheh.2014.04.001. [DOI] [PubMed]
- 10.Delgado PL. Depression: the case for a monoamine deficiency. J Clin Psychiatry. 2000;61(Suppl 6):7–11. [PubMed] [Google Scholar]
- 11.Dunlop BW, Nemeroff CB. The role of dopamine in the pathophysiology of depression. Arch Gen Psychiatry. 2007. doi:10.1001/archpsyc.64.3.327. [DOI] [PubMed]
- 12.Willner P. Dopamine and depression: a review of recent evidence. 1. Empirical studies. Brain Res Rev. 1983. doi:10.1016/0165-0173(83)90005-X. [DOI] [PubMed]
- 13.Brown AS, Gershon S. Dopamine and depression. J Neural Transm. 1993. https://doi.org/10.1007/bf01245227. [DOI] [PubMed]
- 14.Lambert G, Johansson M, Ågren H, Friberg P. Reduced brain norepinephrine and dopamine release in treatment-refractory depressive illness. Arch Gen Psychiatry. 2000;57:787–793. doi: 10.1001/archpsyc.57.8.787. [DOI] [PubMed] [Google Scholar]
- 15.Jimerson DC, Gordon EK, Post RM, Goodwin FK. Central noradrenergic function in man: vanillylmandelic acid in CSF. Brain Res. 1975. doi:10.1016/0006-8993(75)90051-7. [DOI] [PubMed]
- 16.Roy A, Karoum F, Pollack S. Marked reduction in indexes of dopamine metabolism among patients with depression who attempt suicide. Arch. Gen. Psychiatry. 1992;49:447–450. doi: 10.1001/archpsyc.1992.01820060027004. [DOI] [PubMed] [Google Scholar]
- 17.Faroon O, Jones D, De Rosa C. Effects of polychlorinated biphenyls on the nervous system. Toxicol. Ind. Health. 2000. doi:10.1177/074823370001600708. [DOI] [PubMed]
- 18.Seegal RF, Marek KL, Seibyl JP, Jennings DL, Molho ES, Higgins DS, et al. Occupational exposure to PCBs reduces striatal dopamine transporter densities only in women: a β-CIT imaging study. Neurobiol Dis. 2010;2010. doi:10.1016/j.nbd.2010.01.009. [DOI] [PMC free article] [PubMed]
- 19.Putschögl FM, Gaum PM, Schettgen T, Gube M, Kraus T, Lang J. Effects of occupational exposure to polychlorinated biphenyls on urinary metabolites of neurotransmitters: a cross-sectional and longitudinal perspective. Int J Hyg Environ Health. 2015. doi:10.1016/j.ijheh.2015.03.009. [DOI] [PubMed]
- 20.Kraus T, Gube M, Lang J, Esser A, Sturm W, Fimm B, et al. Surveillance program for former PCB-exposed workers of a transformer and capacitor recycling company, family members, employees of surrounding companies, and area residents – executive summary. J Toxicol Env Health, Part A. 2012. doi:10.1080/15287394.2012.709377. [DOI] [PubMed]
- 21.Gaum PM, Esser A, Schettgen T, Gube M, Kraus T, Lang J. Untersuchung der drop-out-Raten bei einem langjährig angelegten arbeitsmedizinischen Vorsorgeprogramm (investigation of drop-out-rates in a long-term occupational health surrveillance programm) In: Schmitz-Spanke S, editor. Dokumentation der 56. Jahrestagung der DGAUM. München: DGAUM; 2016. pp. 581–585. [Google Scholar]
- 22.Schettgen T, Gube M, Alt A, Fromme H, Kraus T. Pilot study on the exposure of the German general population to non-dioxin-like and dioxin-like PCBs. Int J Hyg Environ Health. 2011. doi:10.1016/j.ijheh.2011.04.002. [DOI] [PubMed]
- 23.Schettgen T, Gube M, Esser A, Alt A, Kraus T. Plasma polychlorinated biphenyls (PCB) levels of workers in a transformer recycling company, their family members, and employees of surrounding companies. J Toxicol Env Health, Part A. 2012. doi:10.1080/15287394.2012.674905. [DOI] [PubMed]
- 24.G-EQUAS: The German external quality assessment scheme. 2017. http://www.g-equas.de/. Accessed 11 Apr 2017.
- 25.Lee DH, Lind PM, Jacobs DR Jr, Salihovic S, van Bavel B, Lind L. Polychlorinated biphenyls and organochlorine pesticides in plasma predict development of type 2 diabetes in the elderly. Diabetes Care. 2011. doi:10.2337/dc10-2116/-/DC1. [DOI] [PMC free article] [PubMed]
- 26.Aminov Z, Haase R, Rej R, Schymura MJ, Santiago-Rivera A, Morse G, DeCaprio A, Carpenter DO. Diabetes prevalence in relation to serum concentrations of polychlorinated biphenyl (PCB) congener groups and three chlorinated pesticides in a native American population. Environ. Health Perspect. 2016. doi:10.1289/ehp.1509902. [DOI] [PMC free article] [PubMed]
- 27.Van den Berg MSB, Denison L, De Vito M, Farland M, Feeley W, Fiedler MHH, Hanberg H, Haws A, Rose L, Safe M, Schrenk S, Tohyama DCT, Tuomisto A, Tysklind J, Walker M, Peterson NRE. The 2005 WorldHealth organization reevaluation of human and mammalian toxic equivalency factors for dioxins and dioxin-like compounds. Toxicol Sci. 2006. https://doi.org/10.1093/toxsci/kfl055. [DOI] [PMC free article] [PubMed]
- 28.Bernert JT, Turner WE, Patterson DG Jr, Needham LL. Calculation of serum "total lipid" concentrations for the adjustment of persistent organohalogen toxicant measurements in human samples. Chemosphere. 2007. https://doi.org/10.1016/j.chemosphere.2007.02.043. [DOI] [PubMed]
- 29.Eisenhofer G, Kopin IJ, Goldstein DS. Catecholamine metabolism: a contemporary view with implications for physiology and medicine. Pharmacol Rev. 2004. https://doi.org/10.1124/pr.56.3.1. [DOI] [PubMed]
- 30.Amin F, Davidson M, Davis KL. Homovanillic acid measurement in clinical research: a review of methodology. Schizophrenia Bull. 1992. https://doi.org/10.1093/schbul/18.1.123. [DOI] [PubMed]
- 31.Cole M, Craft AW, Parker L, Bell S, Seviour JA, McGill AC, Dale G. Urinary creatinine adjusted reference ranges for homovanillic and vanillylmandelic acid in children and adults. Clin Chim Acta. 1995;1995. doi:10.1016/0009-8981(95)06031-1. [DOI] [PubMed]
- 32.Delahanty DL, Raimonde AJ, Spoonster E. Initial posttraumatic urinary cortisol levels predict subsequent PSTD symptoms in motor vehicle accident victims. Biol Psychiatry. 2000;48:940. doi: 10.1016/S0006-3223(00)00896-9. [DOI] [PubMed] [Google Scholar]
- 33.Hautzinger M, Keller F, Kuehner C. Beck depressions-Inventar BDI II. Frankfurt am main: Harcourt test services. 2006. [Google Scholar]
- 34.Textor J, Hardt J, Knueppel S. DAGitty: a graphical tool for analyzing causal diagrams. Epidemiology. 2011. 10.1097/EDE.0b013e318225c2be. [DOI] [PubMed]
- 35.Baron RM, Kenny DA. The moderator-mediator variable distinction in social psychological research: conceptual, strategic, and statistical considerations. J. Pers. Soc. Psychol. 1986;51(6):1173. doi: 10.1037/0022-3514.51.6.1173. [DOI] [PubMed] [Google Scholar]
- 36.Hayes AF, Preacher KJ. Statistical mediation analysis with a multicategorical independent variable. Brit J Math Stat Psy. 2014. doi:10.1111/bmsp.12028. [DOI] [PubMed]
- 37.IBM Corp. Released 2012. IBM SPSS statistics for windows, version 21.0. Armonk: IBM Corp.
- 38.Seegal RF, Bush B, Brosch KO. Decrease in dopamine concentrations in adult, non-human promate brain persist following removal from polychlorinated biphenyls. Toxicology. 1994. doi:10.1016/0300-483X(94)90054-X. [DOI] [PubMed]
- 39.Richardson JR, Miller GW. Acute exposure to Aroclor 1061 or 1260 differentially affects dopamine transporter and vesicular monoamine transporter 2 levels. Toxicol Lett. 2004. doi:10.1016/j.toxlet.2003.12.006. [DOI] [PubMed]
- 40.Hatcher-Martin JM, Gearing M, Steenland K, Levey AI, Miller GW, Pennell KD. Association between polychlorinated biphenyls and Parkinson’s disease neuropathology. Neurotoxicology. 2012. doi:10.1016/j.neuro.2012.08.002. [DOI] [PMC free article] [PubMed]
- 41.Goddard AW, Ball SG, Martinez J, Robinson MJ, Yang CR, Russell JM, Shekhar A. Current perspectives of the roles of the central norepinephrine system in anxiety and depression. Depress Anxiety. 2010. doi:10.1002/da.20642. [DOI] [PubMed]
- 42.Paris C, Maurel M, Luc A, Stoufflet A, Pairon JC, Letoumeux M. CT scan screening is associated with increased distress among subjects of the APExS. BMC Public Health. 2010;10:647. doi: 10.1186/1471-2458-10-647. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.Kurlansik SL, Ibay AD. Seasonal affective disorder. Indian J Clin Pract. 2013;24(7):607. [Google Scholar]
- 44.Lambert GW, Eisenhofer G, Cox HS, Horne M, Kalff V, Kelly M, Jennings GL, Esler MD. Direct determination of homovanillic acid release from the human brain, an indicator of central dopaminergic activity. Life Sci. 1991. doi:10.1016/0024-3205(91)90593-Z. [DOI] [PubMed]
- 45.Lambert GW, Eisenhofer G, Esler MD. The influence of aging on the plasma concentration and renal clearance of homovanillic acid. Psychoneuroendocrino. 1994;1:33–41. doi: 10.1016/0306-4530(94)90057-4. [DOI] [PubMed] [Google Scholar]
- 46.Van Praag HM. Neurotransmitters and CNS disease - depression. Lancet. 1982. doi:10.1016/S0140-6736(82)90115-5.
- 47.Eguchi A, Nomiyama K, Tue NM, Trang PTK, Viet PH, Takahashi S, Tanabe S. Residue profiles of organohalogen compounds in human serum from e-waste recycling sites in North Vietnam: association with thyroid hormone levels. Environ. Res. 2015. doi:10.1016/j.envres.2015.01.007. [DOI] [PubMed]
- 48.Guimarães JMN, de Souza LC, Baima J, Sichieri R. Depression symptoms and hypothyroidism in a population-based study of middle-aged Brazilian women. J affect disorders. 2009. doi:10.1016/j.jad.2008.12.012. [DOI] [PubMed]
- 49.Shaw C, Abrams K, Marteu TM. Psychological impact of predicting individuals’ risks of illness: a systematic review. Soc Sci Med. 1999. doi:10.1016/S0277-9536(99)00244-0. [DOI] [PubMed]
- 50.Arnau RC, Meagher MW, Norris MP, Bramson R. Psychometric evaluation of the Beck depression inventory-II with primary care medical patients. Health Psychol. 2001. doi:10.1037//0278-6133.20.2.112. [DOI] [PubMed]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
The datasets analyzed during the current study are not publicly available. In the agreements of the HELPcB program, participant- and health-related raw data are not allowed to be shared, but anonymized data of the scales are available from the corresponding author upon reasonable request.