

Abstract
Divorce is a common stressful event associated with both increased rates of depression and mortality. Given evidence of significant individual differences in depression following major life stressors, we examined if heterogeneous depression responses confer differential risk for mortality. Data from a population based longitudinal study was utilized to identify individuals who experienced divorce (n=559). Prospective trajectories of depression severity from before to after divorce were identified using latent growth mixture modeling, and rates of mortality between trajectories were compared as a distal outcome. Four trajectories demonstrated strongest model fit: resilience (67%), emergent depression (10%), chronic pre-to-post divorce depression (12%), and decreasing depression (11%). Mortality base rate was 9.7% by 6 years post-event, and depression that emerged due to divorce was associated with significantly greater mortality risk compared to resilient (OR, 2.46; 95% CI, 1.05–5.81) and to married individuals, while chronic depression was not associated with greater risk.
Keywords: Depression, Divorce, Resilience, Mortality, Latent Growth Mixture Modeling
Introduction
Divorce is a frequent and highly distressing life transition. Estimates of divorce in the United States range from 40–50% of all marriages (American Psychological Association, 2015) with approximately 2.5 million adults facing divorce a year (Arias, 2007). The process of a divorce usually entails myriad stressors, major financial, legal and logistical challenges, and adjustments on the emotional and social level (Sbarra, Emery, Beam, & Ocker, 2014; Sbarra, Hasselmo, & Bourassa, 2015).
Marital dissolution is a highly aversive event as it has been shown to significantly impact physical and psychological wellbeing. Yet, there is also evidence of considerable resilience following divorce (Mancini, Bonanno & Clark, 2011). At present, these diverse outcomes are poorly understood. Considering the frequency of divorce and the number of individuals directly or indirectly involved, it is crucial to more fully investigate the possible variations in divorce outcomes. To that end, in the current study we applied latent growth mixture modeling (LGMM) to a population data set to examine diverse, prospective trajectories of depression, including resilience and chronic symptoms, measured from before to after divorce. In addition, we examined both predictors and long-term consequences associated with those trajectories, including increased risk for premature mortality.
Premature mortality is one of the more provocative negative health outcomes associated with marital dissolution (Sbarra, Hasselmo & Nojopranoto, 2012). In a meta-analysis on the relationship between divorce and early death has shown that divorced adults have a 23 percent higher risk of dying before the next follow-up period than their married counterparts, which was even more pronounced for men than women (Sbarra, Law & Portley, 2011). Other negative health outcomes are also more prevalent among the divorced adult population (Lorenz, Wickrama, Conger & Elder, 2006), and studies have investigated a biological link between divorce and pathophysiology (Sbarra & Hazan, 2008). For instance, divorced adults are more likely to suffer from reactive blood pressure, which can lead to hypertension (Sbarra, Law, Lee, & Mason, 2009). Other health hazard commonly associated with divorced adults include disruptive sleep patterns, insomnia (Hajak, 2001), poor diet, reduced exercise (Eng, Kawachi, Fitzmaurice, & Rimm, 2005), increased body mass index (Sbarra et al., 2012), and substance abuse relapse (Dawson, Grant, Stinson, & Chou, 2006; Agrawal & Lynskey, 2009). These factors among others may explain increased risk for mortality associated with divorce.
Together, this body of literature provides a poor prognosis for those whose marriage ends in divorce. However, responses to divorce, like other major life stressors, have been shown to be heterogeneous with the majority of individuals coping well despite the event (Bonanno, Westphal, & Mancini, 2011). Such important individual differences in psychological functioning may further reflect individual differences in mortality associated with divorce.
In the current study, we utilize data from an ongoing national survey, the Health and Retirement Study (HRS) to identify heterogeneous trajectories of depression response to divorce. We further investigated the relationship between trajectory membership and subsequent mortality. Based on previous studies of divorce and other major life stressors, we hypothesized that resilience will be the modal outcome and that trajectories of elevated depression will be associated with greater rates of mortality.
Method
Data
Analyses used data from the Health and Retirement Study (HRS), a longitudinal panel survey conducted every two years, starting from 1992 (Juster & Suzman, 1995). The study is collecting data on various socio-economic factors, physical and mental health from an older adult population. The HRS is sponsored by the National Institute on Aging and is conducted by the University of Michigan. HRS RAND data files version N were used for the analysis, as they offered a more streamlined version of the HRS across the biennial time points (Chien et al., 2015). Ten time points of data were analyzed, ranging from 1994 to 2012; the first wave was not included, as it did not use the same depression measure present in the other time points. Data was structured using a floating baseline design methodology (Galatzer-Levy, Bonanno, & Mancini, 2010).
Participants
At each time point HRS participants were asked numerous questions about demographic information, including marital status. We restricted our analyses to participants who experienced a divorce between data waves, identifying subpopulations that are heterogeneous in their longitudinal growth patterns of depression. For each participant, four consecutive time points (T1–T4) were used, including two observations prior to the divorce (T1 and T2), and two post facto observations (T3 and T4). To lower the risk of modeling spurious subpopulations, only participants with no missing depression scores immediately before and after the divorce were included in the analysis. The final sample consisted of 559 adult participants (57.1% female, 42.9% male), predominantly Caucasian (75.5% white, 24.5% non-white), and with a mean age of 57 (SD = 8) at the first observation. Mean years of education were 12 (SD = 3), and the median total non-housing wealth was $20,000 (IQR = 2,000–124,500). The average marriage duration was 20 years (SD = 14). For most of the participants this was their first experience of divorce (51.5% None; 37.6% One; 10.9% Two or more). A portion of the sample (14.8%) remarried within 6 year after the divorce.
Measures
Depression
Depressive symptoms were measured using the CESD-8 (Kohut, Berkman, Evans, & Cornoni-Huntley, 1993), a short form version of the Center for Epidemiologic Studies Depression (CESD) scale (Radloff, 1977). The CESD-8 is considered a reliable and valid instrument to assess depression in an older adult population (Karim, Weisz, Bibi, & ur Rehman, 2014). The CESD-8 score is the sum of the presence (+1) or absence (0) of six negative symptoms (feeling most of the time: depression, everything is an effort, sleep is restless, alone, sad, and could not get going), minus the presence (−1) of two positive symptoms (feeling most of the time: happy and enjoy life). A score of 4 was recommended by the HRS as cut-off for clinical depression (Steffick, 2000). CESD-8 data was available across the four time points for most of the subjects (66.4%), while 30.2% of the subjects were missing a CESD-8 scores at one time point, and 3.4% at two time points. The mean CESD-8 score before the divorce was 2.11 (SD = 2.48) at the first time point and 2.14 (SD = 2.35) at the second, while after the divorce event it was 2.13 (SD=2.39) at the third and 1.8 (SD = 2.27) at the fourth observations.
Chronic Health Conditions
The co-occurrence of medical conditions was assessed asking participants if a medical doctor told them they suffered from a health problem (Wallace & Herzog, 1995). Dichotomic variables indicated those participants that were diagnosed by a medical doctor with a health problem at the observation prior to the divorce. For the purpose of this study, we focused on the four health conditions with the highest mortality incidence (National Center for Health Statistics, 2016): heart disease (heart attack, coronary heart disease, angina, congestive heart failure, or other heart problems; 18.2% of sample), cancer (cancer or a malignant tumor of any kind except skin cancer; 9.5%), lung disease (chronic lung diseases except asthma such as chronic bronchitis or emphysema; 10.6%), and stroke (stroke or transient ischemic attack; 6.1%).
Mortality
Information on whether and when a participant died was collected from the National Death Index as part of the Health and Retirement Study. Cause of death was protected and not accessible for the present study. A dichotomic variable was created to identify the portion of our sample that died within 6 years subsequent to the divorce (9.7%).
Results
Latent Growth Mixture Modeling was performed using Mplus 7.1 (Muthén & Muthén, 2014), to identify the best fitting trajectories model of depressive symptoms, covering a period prior to the divorce (T1 and T2) and at two time points after (T3 and T4). Variances of the intercept and slope were allowed to be freely estimated, while the variance of the quadratic parameter was fixed to allow model convergence. Model solutions with an increasing number of classes were compared in relation to Akaike (AIC), Bayesian (BIC) and sample-size adjusted Bayesian (SSBIC) Information Criteria, relative Entropy, adjusted Lo-Mendell-Rubin (L-M-R LRT) and Parametric Bootstrapped (BLRT) Likelihood Ratio Test. A solution is deemed best based on these indices, explanatory properties, parsimony, and theoretical coherence (Muthén, 2003; Bonanno, 2004). Table S1 in the supplemental materials displays the relative model fit from one to five classes solutions for the unconditional LGMM. The four classes solution had the lowest Information Criteria and highest relative entropy compared to the solutions with significant BLRT and L-M-R LRT. Therefore, the four classes model was considered having the best fit, as well as interpretability. After determining the best fitting solution of depression growth trajectories (i.e. the unconditional model), demographic variables were nested as covariates to analyze class membership prediction (i.e. the conditional model).
Unconditional Model
Figure 1 graphically describes the four classes solution. The best log-likelihood value replicated, indicating that the model converged successfully with an entropy score of .86. Probability of distinct membership was high, with values ranging from .85 to .95.
Fig. 1.
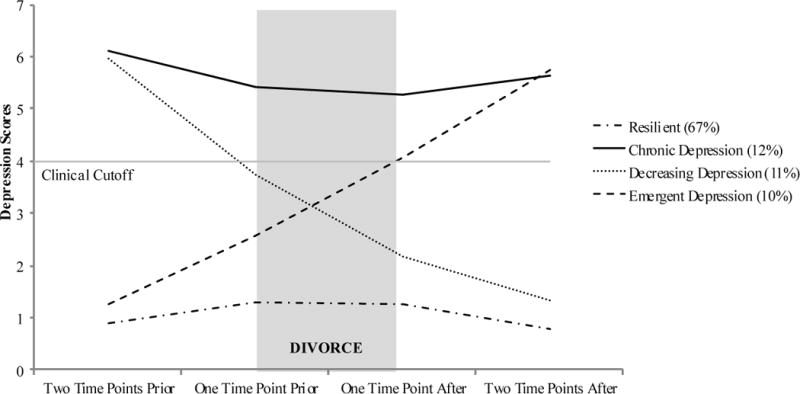
Mean CESD-8 depression scores for each trajectory group two time points before and two time points after the divorce (N = 559).
The majority of the sample (67%) was assigned to a growth trajectory with low values of depression throughout T1–T4, labeled “Resilient”. It was characterized by a low intercept (Est = .88, SE = .08, p ≤ .001), a flat slope (Est = .62, SE= .14, p ≤ .001), and also by a significant quadratic growth parameter (Est = −.22, SE = .04, p ≤ .001). The second largest class (12%) described a population with depression symptoms there were consistently above the clinical threshold across T1–T4, labeled “Chronic Depression”. It was characterized by a high intercept (Est = 6.11, SE = 0.33, p ≤ .001), flat slope (Est = −.96, SE = 0.46, p ≤ .05) and a non-significant quadratic parameter (Est = .27, SE = 0.14, p = .064). The “Decreasing Depression” class (11%) described a population with high starting values in depression, which become increasingly lower over time. It was characterized by a high intercept (Est = 5.96, SE = 0.34, p ≤ .001), a significant negative slope (Est = −2.57, SE = 0.51, p ≤ .001) and a borderline non-significant quadratic parameter (Est = .34, 7SE = 0.18, p= .053). The “Emergent Depression” (10%) described a trajectory with initially low depression symptoms that increase steadily from T1 to T4 and move above the clinical threshold. This trajectory was characterized by a low intercept (Est = 1.26, SE = .29, p ≤ .001), a borderline significant slope (Est= 1.19, SE = .63, p = .057) and a non-significant quadratic parameter (Est = .10, SE = .18, p = .577).
Predictors of trajectory membership
A conditional model was created to analyze the role of demographic, health, and marriage related variables as predictors of the class membership to the depression trajectories. Participants’ gender, ethnicity, initial age, non-housing wealth, chronic health conditions, length of marriage before divorce, and number of antecedent divorces were nested as covariates in the LGMM. Age, non-housing wealth, and length of marriage were standardized to assist model convergence. The presence of missing values in the covariates lowered the sample size available for the conditional model (N = 535), but the model successfully converged with an improved entropy score of .88. There were no substantial changes in the shape and proportions of the four classes when compared to the unconditional solution.
Results from the multinomial logistic regression indicated that when compared to the Resilient class, age was significantly lower for participants in the Chronic Depression (Est = −2.90, SE = 1.31, p ≤ 0.05) class and Decreasing Depression (Est = −3.11, SE = 1.48, p ≤ 0.05) classes; years of education were significantly lower for the Chronic Depression (Est = −0.68, SE = 0.17, p ≤ 0.001), Decreasing Depression (Est = −0.51, SE = 0.16, p ≤ 0.05), and Emergent Depression classes (Est = −0.40, SE = 0.19, p ≤ 0.05). The number of reported chronic health conditions were higher in the Chronic Depression class, having significantly more heart problems (Est = 1.24, SE = 0.40, p ≤ 0.05), and cancer (Est = 1.12, SE = 0.55, p ≤ 0.05) reported diagnoses. There were more also significantly more lung problems diagnoses in the Emergent Depression class (Est = 0.52, SE = 0.19, p ≤ 0.01).
The number of previous divorces, length of marriage, gender, ethnicity, and total non-housing wealth were not significant predictors of class membership. Table S2 in the online Supplemental Materials reports the estimates.
Mortality and Remarriage as distal outcomes of trajectory membership
A logistic regression analysis was performed to determine if participants’ trajectory assignments predicted post-divorce mortality. Fifty-four participants (9.7% of total sample) died during the six years subsequent to the divorce, with 34 participants assigned to the Resilient class (8.9% of class), 5 to Chronic Depression (7.4% of class), 5 to Decreased Depression (8.5% of class), and 10 to the Increased Depression class (19.6% of class). Participants’ class membership was regressed on mortality using Resilient as reference class, while controlling for gender, ethnicity, age, post-divorce non-housing wealth, and antecedent chronic health conditions (doctor’s diagnosed heart disease, cancer, lung disease, and stroke). Choice of covariates was based on previous literature findings that associated depressive symptoms trajectories and mortality (Galatzer-Levy & Bonanno, 2014), known risk factors (Fried et al., 1998; NCHS, 2016), as well as divorce and death (Sbarra et al., 2011). The likelihood ratio test of the full model against a constant only model was significant (χ2(11, N = 557) = 58.38,p ≤ .001), and odds ratios associated with each predictor are shown in Table 1. Results indicated that participants in the Emergent Depression class showed a significantly higher likelihood of mortality (OR, 2.46; 95% CI, 1.05–5.81) when compared to the resilient group. Being older, male, non-white, as well as having being diagnosed with hearth problems also significantly increased risk of death after divorce across all classes.
Table 1.
Odds Ratios for Class, Assets, Demographics, and Health Conditions as Predictors of Death (N = 557) and Remarriage (N = 511) by Six Years Following the Divorce.
| Mortality
|
Remarriage
|
|||
|---|---|---|---|---|
| Variable | OR | [95% CI] | OR | [95% CI] |
| Classa: | ||||
| Emergent Depression | 2.46* | [1.05, 5.81] | 0.44 | [0.15, 1.32] |
| Decreasing Depression | 1.19 | [0.42, 3.40] | 0.67 | [0.28, 1.62] |
| Chronic Depression | 0.85 | [0.30, 2.40] | 0.88 | [0.40, 1.93] |
| Age | 1.01*** | [1.00, 1.01] | 0.99 | [0.99, 1.00] |
| Assets | 1.00 | [1.00, 1.00] | 1.00* | [1.00, 1.00] |
| Ethnicity: Non-white | 2.64** | [1.36, 5.12] | 0.41* | [0.20, 0.82] |
| Gender: Male | 2.76** | [1.44, 5.32] | 1.80* | [1.09, 3.00] |
| Health Conditions: | ||||
| Cancer | 1.46 | [0.56, 3.83] | 0.21* | [0.04, 0.96] |
| Heart Problems | 2.12* | [1.07, 4.19] | 0.83 | [0.40, 1.72] |
| Lung Disease | 1.31 | [0.55, 3.14] | 1.08 | [0.47, 2.51] |
| Stroke | 0.59 | [0.17, 2.04] | 1.06 | [0.34, 3.36] |
Note. OR = Odd Ratio; 95% CI = 95% Confidence Interval.
The Resilient class was used as the reference class.
p ≤ 0.05;
p ≤ 0.01;
p ≤ 0.001
We next examined differences in mortality risk between trajectory memberships from the divorced sample and a sample of 500 continually married individuals randomly selected from the same database. The mortality rate for the continually married sample (9.6%) was highly similar to the mortality rate for the divorced sample (9.7%). Given that the married sample presented heterogeneous fluctuations of depression over time, we preformed a multinomial logistic regression analysis with the married sample as the reference class compared against the four trajectory classes from the divorced sample. In this analysis, we used the same choice of covariates as in the preceding logistic regression. The LRT of the model was significant (χ2(12, N = 925) = 113.88, p ≤ .001). Results indicated that divorced subjects from the Emergent Depression class had a significantly higher mortality risk (OR, 2.49; 95% CI, 1.06–5.85) when compared to their married counterparts. There were no significant differences in mortality outcomes between the married sample and the resilient, decreased depression and chronic depression trajectory groups. For full odds ratios for this analysis, see Table S3 in the supplementary materials.
A final multinomial logistic regression was performed to determine if differences in the longitudinal course of depressive symptoms were associated with the likelihood of remarriage. Within six years after the divorce 83 participants remarried (14.8% total sample). 63 of the remarried individuals were assigned to the Resilient Class (17.8% of class), 9 to the Chronic Depression (14.5%), 7 to the Decreased Depression (13.2%), and 4 to the Emergent Depression (9.3%) classes. The overall model fit was significant (χ2(11, N = 511) = 27.95, p ≤ .01), and results indicated that trajectory class membership was not a significant predictor of remarrying. A cancer diagnosis significantly decreased the likelihood of remarriage, whereas being male, white, and having more assets significantly increased it.
Discussion
The current work examined individual differences in depression response to divorce, along with demographics, health, remarriage, and mortality associated with those differences. We identified four heterogeneous psychological response trajectories. The majority of the sample (67%) was classified under the Resilient trajectory, indicating that these individuals maintained relatively stable psychological health following the stressor. The second largest class (12%) consisted of individuals with depression symptoms consistently above the clinical threshold, labeled Chronic Depression. It was followed by the Decreasing Depression (11%), a class of individuals whose condition improved steadily over time. The fourth common trajectory was Emergent Depression (10%), consisting of individual who were not depressed prior to the divorce became more depressed over time and had depression scores above the clinical threshold after the divorce. Nonetheless, despite the stressful nature of a divorce, the vast majority of individuals maintained a psychologically resilient outcome following the stressor.
We further investigated whether demographics and covariates related to health status, and marriage quality of participants were successful predictors of class membership of the depression trajectories. Results indicated that age, level of education and health conditions were significant predictors of depression class membership. Younger participants were more likely to be classified into the Chronic class compared to the Resilient class. These results indicate that younger people are more likely to be depressed leading up to their divorce. Considering the notion of younger divorcés further, it seems plausible that a divorce earlier in life can have more significant consequences. For instance, the economic burden often associated with divorce might more severely impact younger divorcees who are raising young children or in the process of establishing a career. Those with fewer years of education were more likely to be classified into all trajectories compared to the Resilient class indicating that lower levels of education are broadly associated with depression. This is consistent with previous findings that education is broadly protective in the context of stress. For instance, Mancini et al. (2011) found that those individuals with lower levels of education were more likely to fall into a trajectory of worsening depression after having gone through a divorce, suggesting that education is related to successfully cope with aversive events. Looking at health conditions, results indicated that individuals in the Chronic Depression and Emergent Depression classes reported a higher number of chronic health conditions than the individuals in the Resilient trajectory. Specifically, more heart problem and cancer diagnoses were reported in the Chronic Depression class, and more lung diseases in the Emergent Depression class. There is significant evidence that chronic health problems are associated with depression (Egede, 2007; Turvey, Schultz, Beglinger, & Klein, 2009). The finding that health problems are associated with emergent depression following divorce is novel to our knowledge and is consistent with the findings regarding increased rates of mortality among individuals on this trajectory.
Results indicated that the risk of mortality was higher for those on the emergent depression trajectory, when controlling for health conditions and key demographic factors that could account for the relationship between trajectory membership and mortality, including age, gender, ethnicity, and total non-housing assets. Participants who were already reporting depressive symptoms before the divorce did not show a higher risk of mortality, despite the higher incidence of heart problems, which was identified as another significant risk factor. These results were reproduced also when comparing the trajectory classes to a random sample of continually married individuals. There were no significant differences in mortality between the non-divorced and the resilient group. These findings are consistent with others demonstrating that the emergence of depression following a significant health stressor event such as myocardial infarction (Galatzer-Levy & Bonanno, 2014) is associated with mortality. However, to our knowledge, this is the first prospective study to demonstrate a relationship between a psychosocial stressor, the emergence of depression, and increased risk for mortality.
Lastly, exploring the covariate of remarriage by six years after the divorce, our analyses indicated that remarriage was not significantly related to trajectory class membership. Yet, it is noteworthy that the majority of individuals in the resilient class who fare well after divorce do not end up remarrying. Thus, there is a double-dissociation between remarriage and resilience.
In addition to the strengths of our study, there were also a number of limitations worth noting. As the HRS is a bi-annual data collection, short-term variations in depression may not have been registered. A more fine-grained assessment may provide a more detailed picture of the emergence of depression. Moreover, the study focused on a psychosocial stressor, which resulted in a relatively small mortality base rate over six years (9.7%) relative to mortality outcomes observed following major health events (e.g., Galatzer-Levy & Bonanno, 2014). Furthermore, the total number of deaths (54) was divided between trajectories, resulting in further small absolute numbers of deceased per class. Although our total sample size (N=557) was adequate for the statistical analyses’ overall power (Long & Freese, 2006), the estimated differences in trajectories’ outcomes are calculated from relative risk comparisons between these small per class numbers. Therefore, while the results are consistent with previous literature linking emergent depression trajectories with higher mortality risk (Galatzer-Levy & Bonanno, 2014; Morin, Galatzer-Levy, Maccallum & Bonanno, in press), interpretation of the effect sizes’ magnitude fosters caution. Moreover, the mean age of our sample was 57, which may limit the generalizability of our findings. For example, findings regarding mortality may not reproduce in significantly younger populations. A larger and more varied sample followed over a longer time period could have potentially resulted in a higher mortality base rate, a larger absolute number of deaths, and consequently more robust and generalizable findings.
Despite these limitations, this study adds significantly to a growing body of literature that has demonstrated heterogeneity in depression response to significant stressor events (Bonanno et al., 2002; Galatzer-Levy & Bonanno, 2012; Bonanno, Kennedy, Galatzer-Levy, Lude, & Elfström, 2012; Burton, Galatzer-Levy, & Bonanno, 2014; Galatzer-Levy & Bonanno, 2015; Maccallum, Galatzer-Levy, & Bonanno, 2015; Morin et al., in press; Stolove, Galatzer-Levy & Bonanno, in press). Our findings indicate that the majority of individuals cope well despite the significant adversity associated with divorce. We further demonstrate that illness and mortality are significantly elevated among individuals who develop clinically relevant depression following the divorce. Together, these results underscore the crucial importance of identifying heterogeneous patterns of outcome and in particular those individuals with marked increases in depression following divorce or other aversive events who are most likely to benefit from psychological and physiological interventions. Further work is needed to understand the link between mental and physical outcomes. Significant evidence now indicates that immune and inflammatory changes that are brought on by stress also influence the development of depressive symptoms (Kiecolt-Glaser, Derry, & Fagundes, 2015). Determining if the link between emergent depression and mortality is driven by individual differences in inflammatory response to divorce may represent a fruitful direction for further research.
Supplementary Material
References
- Agrawal A, Lynskey MT. Correlates of later-onset cannabis use in the National Epidemiological Survey on Alcohol and Related Conditions (NESARC) Drug and Alcohol Dependence. 2009;105:71–75. doi: 10.1016/j.drugalcdep.2009.06.017. [DOI] [PMC free article] [PubMed] [Google Scholar]
- American Psychological Association. Fact sheet on marriage & divorce. 2016 Retrieved from: http://www.apa.org/topics/divorce/
- Arias E. United States life tables, 2004. Hyattsville, MD: National Center for Health Statistics; 2007. (National Vital Statistics Reports, 56). [PubMed] [Google Scholar]
- Bonanno GA, Wortman CB, Lehman DR, Tweed RG, Haring M, Sonnega J, Nesse RM. Resilience to loss and chronic grief: a prospective study from preloss to 18-months postloss. Journal of personality and social psychology. 2002;83(5):1150. doi: 10.1037//0022-3514.83.5.1150. [DOI] [PubMed] [Google Scholar]
- Bonanno GA. Loss, trauma, and human resilience: have we underestimated the human capacity to thrive after extremely aversive events? American psychologist. 2004;59(1):20. doi: 10.1037/0003-066X.59.1.20. [DOI] [PubMed] [Google Scholar]
- Bonanno GA, Westphal M, Mancini AD. Resilience to loss and potential trauma. Annual Review of Clinical Psychology. 2011;7:1.1–1.25. doi: 10.1146/annurev-clinpsy-032210-104526. [DOI] [PubMed] [Google Scholar]
- Burton C, Galatzer-Levy IR, Bonanno GA. Treatment type and demographic characteristics as predictors for cancer adjustment: Prospective trajectories of depressive symptoms in a population sample. Health Psychology. 2015;34:602–609. doi: 10.1037/hea0000145. [DOI] [PubMed] [Google Scholar]
- Chien S, Campbell N, Chan C, Hayden O, Hurd M, Main R, Moldoff M. RAND HRS Data Documentation, Version O. 2015. [Google Scholar]
- Dawson DA, Grant BF, Stinson FS, Chou PS. Maturing out of alcohol dependence: The impact of transitional life events. Journal of Studies on Alcohol. 2006;67:195–203. doi: 10.15288/jsa.2006.67.195. [DOI] [PubMed] [Google Scholar]
- Egede LE. Major depression in individuals with chronic medical disorders: prevalence, correlates and association with health resource utilization, lost productivity and functional disability. General hospital psychiatry. 2007;29(5):409–416. doi: 10.1016/j.genhosppsych.2007.06.002. [DOI] [PubMed] [Google Scholar]
- Eng PM, Kawachi I, Fitzmaurice G, Rimm EB. Effects of marital transitions on changes in dietary and other health behaviours in US male health professionals. Journal of epidemiology and community health. 2005;59(1):56–62. doi: 10.1136/jech.2004.020073. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Long JS, Freese J. Regression models for categorical dependent variables using Stata. Stata press; 2006. [Google Scholar]
- Lorenz FO, Wickrama KAS, Conger RD, Elder GH., Jr The Short-Term and Decade-Long Effects of Divorce on Women’s Midlife Health. Journal of Health and Social Behavior. 2006;47(2):111–125. doi: 10.1177/002214650604700202. [DOI] [PubMed] [Google Scholar]
- Fried LP, Kronmal RA, Newman AB, Bild DE, Mittelmark MB, Polak JF, Cardiovascular Health Study Collaborative Research Group Risk factors for 5-year mortality in older adults: the Cardiovascular Health Study. Jama. 1998;279(8):585–592. doi: 10.1001/jama.279.8.585. [DOI] [PubMed] [Google Scholar]
- Galatzer-Levy IR, Bonanno GA, Mancini AD. From Marianthal to latent growth mixture modeling: A return to the exploration of individual differences in response to unemployment. Journal of Neuroscience, Psychology, and Economics. 2010;3(2):116. [Google Scholar]
- Galatzer-Levy IR, Bonanno GA. Beyond normality in the study of bereavement: Heterogeneity in depression outcomes following loss in older adults. Social Science & Medicine. 2012;74:1987–1994. doi: 10.1016/j.socscimed.2012.02.022. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Galatzer-Levy IR, Bonanno GA. Optimism and death predicting the course and consequences of depression trajectories in response to heart attack. Psychological Science. 2014 doi: 10.1177/0956797614551750. 0956797614551750. [DOI] [PubMed] [Google Scholar]
- Hajak G. Epidemiology of severe insomnia and its consequences in Germany. European Archives of Clinical Neuroscience. 2001;251:49–56. doi: 10.1007/s004060170052. [DOI] [PubMed] [Google Scholar]
- Juster FT, Suzman R. An overview of the Health and Retirement Study. Journal of Human Resources. 1995:S7–S56. [Google Scholar]
- Karim J, Weisz R, Bibi Z, ur Rehman S. Validation of the Eight-Item Center for Epidemiologic Studies Depression Scale (CES-D) Among Older Adults. Current Psychology. 2014:1–20. [Google Scholar]
- Kiecolt-Glaser JK, Derry HM, Fagundes CP. Inflammation: depression fans the flames and feasts on the heat. American Journal of Psychiatry. 2015;172(11):1075–1091. doi: 10.1176/appi.ajp.2015.15020152. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kohout FJ, Berkman LF, Evans DA, Cornoni-Huntley J. Two shorter forms of the CES-D depression symptoms index. Journal of aging and health. 1993;5(2):179–193. doi: 10.1177/089826439300500202. [DOI] [PubMed] [Google Scholar]
- Maccallum F, Galatzer-Levy IR, Bonanno GA. Trajectories of depression following spousal and child bereavement: A comparison of the heterogeneity in outcomes. Journal of Psychiatric Research. 2015;69:72–79. doi: 10.1016/j.jpsychires.2015.07.017. [DOI] [PubMed] [Google Scholar]
- Mancini AD, Bonanno GA, Clark AE. Stepping off the hedonic treadmill. Individual differences in response to major life events. Journal of Individual Differences. 2011;32:144–152. [Google Scholar]
- Morin RT, Galatzer-Levy IR, Maccallum F, Bonanno GA. Multiple health events do not reduce resilience when compared with single events. Health Psychology. doi: 10.1037/hea0000481. (in press) [DOI] [PubMed] [Google Scholar]
- Muthén B. Statistical and substantive checking in growth mixture modeling: comment on Bauer and Curran (2003) 2003 doi: 10.1037/1082-989X.8.3.369. [DOI] [PubMed] [Google Scholar]
- Muthén LK, Muthén BO. Mplus (Version 7.3)[computer software] Los Angeles, CA: Muthén & Muthén; 2014. pp. 1998–2014. [Google Scholar]
- National Center for Health Statistics, Centers for Disease Control, & Preventi, editor. Health, United States, 2015, With Special Feature on Racial and Ethnic Health Disparities. Government Printing Office; 2016. [PubMed] [Google Scholar]
- Radloff LS. The CES-D scale a self-report depression scale for research in the general population. Applied psychological measurement. 1977;1(3):385–401. [Google Scholar]
- Sbarra DA, Emery RE, Beam CR, Ocker BL. Marital dissolution and major depression in midlife: A propensity score analysis. Clinical Psychological Science. 2014;2(3):249–257. doi: 10.1177/2167702613498727. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Sbarra DA, Hasselmo K, Bourassa KJ. Divorce and health: Beyond individual differences. Current Directions in Psychological Science. 2015;24:109–113. doi: 10.1177/0963721414559125. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Sbarra DA, Hasselmo K, Nojopranoto W. Divorce and death: A case for health psychology. Social and Personality Psychology Compass. 2012;12:905–919. doi: 10.1111/spc3.12002. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Sbarra DA, Hazan C. Coregulation, dysregulation, self-regulation: An integrative analysis and empirical agenda for understanding adult attachment, separation, loss, and recovery. Personality and Social Psychology Review. 2008;12(2):141–167. doi: 10.1177/1088868308315702. [DOI] [PubMed] [Google Scholar]
- Sbarra DA, Law RW, Lee LA, Mason AE. Marital dissolution and blood pressure reactivity: Evidence for the specificity of emotional intrusion, hyperarousal and task-related emotional difficulty. Psychosomatic Medicine. 2009;71:532–540. doi: 10.1097/PSY.0b013e3181a23eee. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Sbarra DA, Law RW, Portley RM. Divorce and Death A Meta-Analysis and Research Agenda for Clinical, Social, and Health Psychology. Perspectives on Psychological Science. 2011;6(5):454–474. doi: 10.1177/1745691611414724. [DOI] [PubMed] [Google Scholar]
- Steffick DE. Documentation of affective functioning measures in the Health and Retirement Study. Ann Arbor, MI: University of Michigan; 2000. [Google Scholar]
- Stolove CA, Galatzer-Levy IR, Bonanno GA. Emergence of depression following job loss prospectively predicts lower rates of reemployment. Psychiatry Research. doi: 10.1016/j.psychres.2017.03.036. (in press) [DOI] [PubMed] [Google Scholar]
- Turvey CL, Schultz SK, Beglinger L, Klein DM. A longitudinal community-based study of chronic illness, cognitive and physical function, and depression. The American Journal of Geriatric Psychiatry. 2009;17(8):632–641. doi: 10.1097/jgp.0b013e31819c498c. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wallace RB, Herzog AR. Overview of the health measures in the Health and Retirement Study. Journal of Human Resources. 1995:S84–S107. [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.