

Supplemental Digital Content is available in the text.
Summary:
Resection of tumors affecting the hip abductors can cause significant decrease in muscle strength and may lead to abnormal gait and poor function. We present a case report showing full functional recovery after resection of a synovial sarcoma affecting the right gluteus medius and minimus muscles with reconstruction free neurovascular latissimus dorsi muscle transplantation. The latissimus dorsi muscle was harvested following standard technique and fixed to the ilium and the greater trochanter. Receptor vessels were end-to-end anastomosed to the subscapular vessels followed by an end-to-end epineural suture between the superior gluteal nerve and the thoracodorsal nerve. A year after surgery, there is no evidence of recurrent disease; electromyographic analysis shows complete reinnervation of the latissimus dorsi muscle flap, and the patient has achieved full functional recovery. Free functional latisimus dorsi transfer could be considered as a viable reconstruction technique after hip abductors resection in tumor surgery.
The lower extremity is the most common location for soft-tissue sarcoma (STS), with around 5% located in the buttock. Resection of tumors in this location may necessitate en bloc removal of a considerable portion of the hip abductors, resulting in a significant decrease in muscle strength and may lead to abnormal gait and poor function.1,2 Manktelow and McKee3 first described the free neurovascular muscle transfer to restore finger function in 1978 and since then it has been applied mainly in upper extremity but also in craniofacial and, rarely, in lower extremity motor reconstructive surgeries. In lower extremity, the main indication is the functional reconstruction after quadriceps tumor resection with only 1 previous report of hip abductor reconstruction.4–6 We present the surgical technique and the electromyographic and clinical results that demonstrate full functional recovery after hip abductor resection with free neurovascular latissimus dorsi muscle transplantation.
CASE REPORT
A 43-year-old man presented to our outpatient clinic with a growing soft-tissue mass in the right buttock. His hip range of motion and walking were unaffected. Pelvic magnetic resonance imaging then revealed a 5-cm soft-tissue mass within the right gluteus medius muscle compatible with an STS (Fig. 1). Biopsy and chest computed tomography diagnosed a localized high-grade synovial sarcoma. The patient was given 3 doses of ifosfamide neoadjuvant chemotherapy without complications. Then, additionally to a wide resection of the right gluteus medius and minimus muscles, we proposed reconstruction with a free functional latissimus dorsi flap to diminish functional sequelae of severe hip abductor insufficiency (Fig. 2). Informed consent from the patient was obtained for publication of the case.
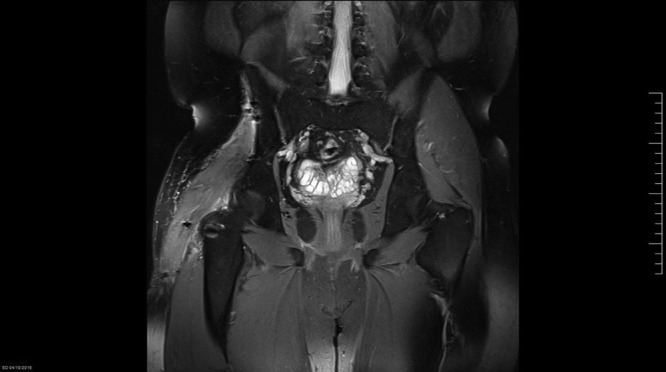
Fig. 1.

Preoperative MRI showing a 5-cm synovial sarcoma within the right gluteus medius muscle.
Fig. 2.
Postoperative MRI at 14 months showing complete resection of the right gluteus medius and minimus muscles and reconstruction with functional latissimus dorsi.
Surgical Technique
The patient was placed in a left lateral decubitus position. After identification and isolation of the superior gluteal vasculonervous bundle, gluteus medius and minimus muscles were resected including their insertion with a greater trochanter ostectomy. The latissimus dorsi muscle was harvested following standard technique applying tension suture markers at 5-cm intervals, which had been marked before its desinsertion and including an 8 × 4 cm skin paddle as a vascular postoperative monitor. After its tubulization, anchor screws (Arthrex) and 2 Trevira meshes (Implantcast GmbH, Buxtehude, Germany) were used to suture the muscle flap to the ilium and the greater trochanter with proper tension maintaining the hip at 30 degrees of abduction (Fig. 3).
Fig. 3.
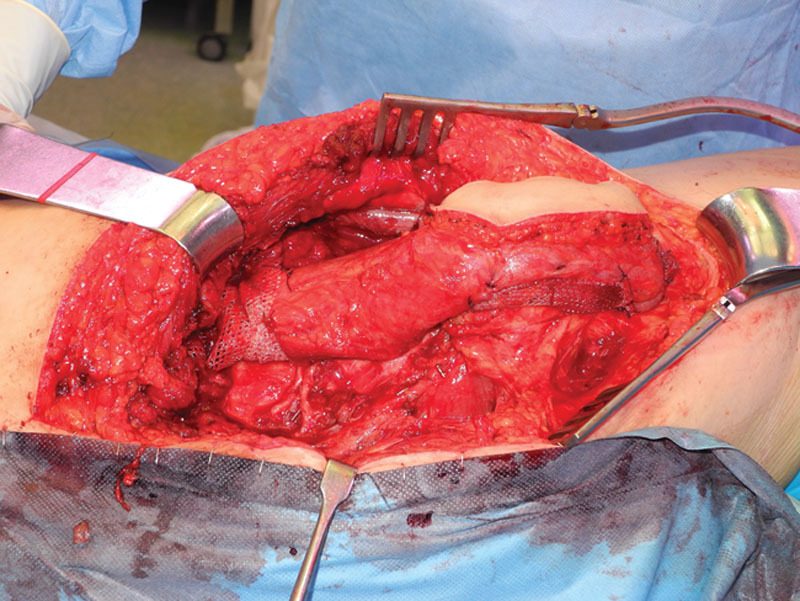
Intraoperative image showing the latissimus dorsi muscle with the skin paddle, placed in the ilium and greater trochanter with the mesh. The vascular pedicle can be observed in the bottom left margin of the image.
Receptor vessels were end-to-end anastomosed to the subscapular vessels followed by an end-to-end epineural suture between the superior gluteal nerve and the thoracodorsal nerve. There were no intraoperative complications.
Postoperative Care
The definitive biopsy confirmed synovial sarcoma with negative margins. Surgical wounds healed uneventfully. Six weeks after surgery, standard adjuvant radiotherapy was applied to the postoperative tumor bed in a schedule of 1.8 Gy/fraction, 5 fractions per week and for 6 weeks, for a total dose of 63 Gy. Physical therapy was initiated after the first week. The patient regained partial abductor strength after 2 months walking without aids and with minor limp, then progressing to full muscle strength at 4 months. A year after surgery, there is no evidence of disease, electromyographic analysis shows complete reinnervation of the latissimus dorsi muscle flap (Fig. 4), the patient has achieved M5 abductor strength, walking without limp, and he can even run short distances (see video, Supplemental Digital Content 1, which displays the patient 1 year after surgery, http://links.lww.com/PRSGO/A535).
Fig. 4.
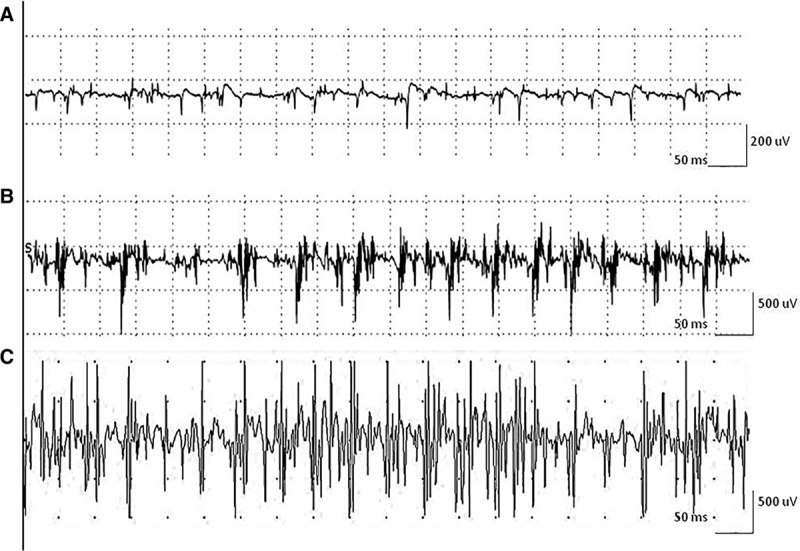
Needle electromyography findings in latissimus dorsi muscle at 3 (A), 6 (B), and 16 (C) months after surgical repair. A, Total denervation of latissimus dorsi muscle at 3 months of evolution, with profuse spontaneous activity in the form of fibrillation and positive waves and absence of voluntary activity. B, Early signs of reinnervation at 6 months, with few polyphasic and low amplitude MUPs. C, Abundant signs of reinnervation at 16 months with nearly interferential pattern of activation. MUPs, motor unit potentials.
Video Graphic 1.

See video, Supplemental Digital Content 1, which displays the patient 1 year after surgery. A total active hip abduction and flexion is displayed without Trendelenburg sign, http://links.lww.com/PRSGO/A535.
DISCUSSION
STSs occur predominantly in the lower extremities, mainly in the thigh, and occasionally in the gluteal region. Advances in surgical techniques have made wide buttockectomy the procedure of choice preferentially over internal/external hemipelvectomy. Depending on the size, location, and depth, resection can affect not only the gluteus maximus but also the medius and minimus, causing severe abduction deficiency and abnormal Trendelemburg gait.1,2 This was evident from the immediate postoperative period when our patient was unable to abduct the hip and required crutches for walking due to the local muscle deficiency caused by the resection.
We opted for a free functional latissimus dorsi transfer as a first option for reconstruction. Less complex techniques such as the muscleplasty described by Whiteside require remnant muscle stumps of the gluteus medius to offer guarantee to the suture repair and are also more appropriate for low demand older patients. Pedicled ascent of the vastus lateralis would debilitate the quadriceps and was left as a second option in case the free flap failed.7 We also opted for the latissimus dorsi over a gracilis muscle transfer due to higher muscle power and better versatility to reconstruct the hip abductors. This reconstruction enabled the patient to fully recover hip abduction even against moderate resistance and functionally allowed him to recover unaided walking and running short distances. This excellent result enables the free functional latissimus dorsi transfer to be considered a viable reconstruction technique for hip abductors resection in tumor surgery.
Supplementary Material
Footnotes
Disclosure: The authors have no financial interest to declare in relation to the content of this article. The Article Processing Charge was paid for by the authors pertaining to Vall d’Hebron Research Institute (VHIR).
Supplemental digital content is available for this article. Clickable URL citations appear in the text.
REFERENCES
- 1.Soyfer V, Corn BW, Bickels J, et al. Primary high-grade soft-tissue sarcoma of the buttock: a rare but distinct clinical entity. Br J Radiol. 2016;89:20151017. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Behranwala KA, Barry P, A’Hern R, et al. Buttock soft tissue sarcoma: clinical features, treatment, and prognosis. Ann Surg Oncol. 2003;10:961–971.. [DOI] [PubMed] [Google Scholar]
- 3.Manktelow RT, McKee NH. Free muscle transplantation to provide active finger flexion. J Hand Surg Am. 1978;3:416–426.. [DOI] [PubMed] [Google Scholar]
- 4.Pritsch T, Malawer MM, Wu CC, et al. Functional reconstruction of the extensor mechanism following massive tumor resections from the anterior compartment of the thigh. Plast Reconstr Surg. 2007;120:960–969.. [DOI] [PubMed] [Google Scholar]
- 5.Muramatsu K, Ihara K, Doi K, et al. Functional neuro-vascularized muscle transfer for oncological reconstruction of extremity sarcoma. Surg Oncol. 2012;21:263–268.. [DOI] [PubMed] [Google Scholar]
- 6.Ihara K, Kishimoto T, Kawai S, et al. Reconstruction of hip abduction using free muscle transplantation: a case report and description of the technique. Ann Plast Surg. 2000;45:177–180.. [DOI] [PubMed] [Google Scholar]
- 7.Whiteside LA. Surgical technique: Gluteus maximus and tensor fasciae latae transfer for primary deficiency of the abductors of the hip. Clin Orthop Relat Res. 2014;472:645–653.. [DOI] [PMC free article] [PubMed] [Google Scholar]