

Abstract
In the last two years, an epidemic of 40 fatal heroin overdose cases has occurred in the Tampa area of Florida. Of these cases, 14 involved fentanyl and acetyl fentanyl. Victim demographics, case histories, toxicology findings, and causes and manners of death for all 40 deaths are presented. In 26 deaths in which acetyl fentanyl or fentanyl were not involved, free and total peripheral blood morphine concentrations were consistent with fatal heroin intoxications, averaging 0.16 mg/L and 0.35 mg/L, respectively. In the heroin cases with fentanyl present (n=7), the average free morphine concentration was 0.040 mg/L, the average total morphine concentration was 0.080 mg/L, and the average fentanyl concentration was 0.012 mg/L. In the cases with heroin, fentanyl, and acetyl fentanyl (n=3), the average free morphine concentration was 0.010 mg/L, the average total morphine concentration was 0.030 mg/L, the average fentanyl concentration was 0.018 mg/L, and the average acetyl fentanyl concentration was 0.008 mg/L. In the cases involving only acetyl fentanyl (without heroin or fentanyl, n=4), the average acetyl fentanyl concentration was 0.47 mg/L and the average acetyl norfentanyl concentration was 0.053 mg/L. The presented cases, with associated drug concentrations, case histories, demographics, and causes and manners of death may help provide assistance with the interpretation of the postmortem findings. Based on case circumstances, autopsy results, and toxicology results, it is evident that fentanyl and/or acetyl fentanyl, when present, contributed to the cause of death.
Keywords: Forensic pathology, Acetyl Fentanyl, Fentanyl, Heroin, Postmortem
INTRODUCTION
Heroin overdoses in the United States have been on the increase since 2007, with a dramatic increase reported in the last five years. The Centers for Disease Control and Prevention (CDC) report heroin overdoses tripled from 2010 to 2013 (1). Kentucky reported a 207% increase in heroin deaths, a 174% increase in heroin-related hospitalizations, and a 197% increase in heroin-related emergency department visits from 2010 to 2012 (2). Heroin deaths in Florida increased 78% in 2013 and 102% in the first six months of 2014 (3, 4).
Since late 2013, there have been alarming reports of heroin laced with fentanyl, acetyl fentanyl, and other fentanyl analogues, resulting in fatalities (5–10). More than 700 fentanyl and acetyl fentanyl related deaths have been reported, but the actual number is uncertain as many reports lack specific toxicology findings for fentanyl or acetyl fentanyl (5). Most of the fentanyl and acetyl fentanyl cases have occurred on the East coast of the United States. These deaths are believed to be the result of clandestinely manufactured fentanyl analogues being added to the heroin supply (5, 8, 10). This heroin market is currently largely controlled by Mexican drug traffickers (5).
Fentanyl was developed in 1960’s by Janssen Pharmaceuticals in Belgium as an intravenous anesthetic under the trade name of Sublimaze. Fentanyl is a high potency synthetic narcotic that is approximately 50 to 100 times more potent that morphine. Fentanyl pharmaceutical products currently available include an injectable formulation, oral transmucosal lozenges commonly referred to as “lollipops” (Actiq), transdermal patches (Duragesic), and effervescent buccal tablets (Fentora). Fentanyl is typically used for surgical anesthesia and severe chronic pain, with therapeutic plasma concentrations in the range of 0.002 to 0.005 mg/L. It is a mu opioid agonist with high lipid solubility, rapid onset of action, and short duration of action. Pharmacologic effects include analgesia, sedation, severe respiratory depression, seizures, coma, and hypotension. Other drug reactions include myosis, mood changes, euphoria, dysphoria, nausea, vomiting, and somnolence (11). Methyl fentanyl analogues differ in potency, with some being less potent than morphine and others being more potent than morphine (12, 13). The 3-methylfentanyl analog is possibly the deadliest of the fentanyl analogues, with an estimated potency of 6600 times greater than morphine (12).
Due to its wide availability as a prescribed drug, fentanyl has been abused and misused by health professionals, pain management patients, and recreational abusers (11). In addition, clandestinely manufactured fentanyl and fentanyl analogues have led to clusters of overdose deaths over the past several decades. In 1979, the first two fentanyl deaths associated with intravenous heroin addicts occurred in Orange County, California (13). Drug paraphernalia was found at the death scenes and the bodies displayed recent injection sites; though curiously, the toxicology findings were negative. As similar cases occurred throughout California, a Drug Enforcement Administration (DEA) investigation identified the drug being sold on the street under the name “China White” as α-methylfentanyl. Between 1979 and 1988, 112 cases of fentanyl and/or ten different fentanyl analogue deaths were confirmed in California, Oregon, Arizona, Nevada, and Pennsylvania (13–15). In 1988, a chemist in Pittsburgh, Pennsylvania produced and distributed 3-methylfentanyl, which led to multiple deaths immediately following its introduction into the illicit drug market (16, 17).
A second, bigger wave of fentanyl related deaths occurred between 2005 and 2007, with a total of 1013 deaths reported in the Midwest and Northeastern United States. Chicago reported 342 fatalities, the Detroit metropolitan area reported over 230 fatalities, and Minneapolis reported 23 fatalities, all due to fentanyl intoxication (18–21). Around the same time, an epidemic of 3-methylfentanyl deaths was reported in Europe (22). As a result, the DEA began regulating the precursor chemicals for fentanyl analogues, N-phenethyl-4-piperidone (NPP) and 4-anilino-N-phenethyl-4-piperidine (ANPP). In addition, a surveillance system comprised of officials from law enforcement, medical examiner/coroner systems, and public health departments was set up to help identify drug death trends and track outbreaks.
Since 2014, the Tampa area of the western coast of Florida (Hillsborough County) has experienced more than 40 heroin related deaths. This was a substantial increase from the previous five years in which there were three or fewer heroin related deaths per year from 2008 to 2013. Many of these fatalities have been associated with the combined use of heroin and fentanyl. Seven of these deaths involved acetyl fentanyl, a designer drug available from Internet drug sites or synthesized clandestinely which has no medical use in the United States. While there are no human studies, acetyl fentanyl was estimated to be 15 times more potent than morphine and one third as potent as fentanyl in mice (23). The chemical structures of fentanyl and acetyl fentanyl are presented in Figure 1. Case histories, demographics, toxicology findings and causes and manners of death in 40 of these drug deaths involving heroin and/or fentanyl and/or acetyl fentanyl are presented. The data include the blood concentrations of morphine (from heroin) and, if present, other drug findings.
Figure 1.
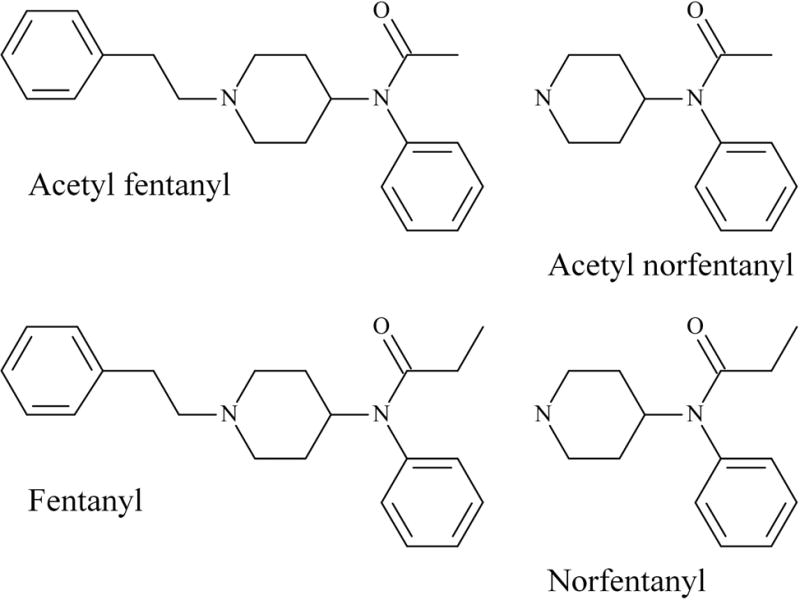
Chemical structures of acetyl fentanyl, fentanyl and their nor-metabolites.
METHODS
Postmortem blood, vitreous, and/or urine specimens were screened for volatiles by headspace gas chromatography, drugs of abuse by immunoassay (acetaminophen, barbiturates, benzodiazepines, cannabinoids, carisoprodol/meprobamate, benzoylecgonine, fentanyl, methadone, methamphetamine/MDMA, opiates, oxycodone, and salicylates), and alkaline extractable drugs by full scan gas chromatography mass spectrometry (GC/MS) (24). In all heroin cases with presumptive opiate positive immunoassay results, targeted testing for unconjugated and conjugated opiates including the heroin metabolite 6-monoacetylmorphine (6-MAM) was conducted by high performance liquid chromatography (HPLC) and tandem mass spectrometry (MS/MS) (25, 26). In many cases, if heroin was suspected, vitreous humor and urine were also analyzed to help detect the presence of 6-MAM. In the cases containing fentanyl and/or acetyl fentanyl, the immunoassay screens yielded presumptive fentanyl positive results (Immunalysis, Pomona, CA). Fentanyl and acetyl fentanyl immunoassay results were confirmed by full scan GC/MS analysis of alkaline blood extracts using an Rtx-5 (30 m × 0.25 mm × 0.25 μm) column (Restek, Bellefonte, PA). The initial oven temperature of 100°C was held for 1 minute, followed by a 15°C ramp to 230°C, then a 12°C ramp to 300°C followed by a 10 minute hold. Low fentanyl blood concentrations often made it necessary to evaluate the full scan data for fentanyl by extracting mass ions m/z 245, 189 and 146, Figure 2A. Fentanyl was quantitated using GC/MS in selected ion monitoring mode (SIM). Acetyl fentanyl was not initially detected in some cases. However when performing the SIM analysis for fentanyl, a compound containing a m/z 146 ion eluted approximately 30 seconds before fentanyl. When this m/z 146 ion was extracted out of the GC/MS full scan data, the other fentanyl related peak was identified and subsequently confirmed to be acetyl fentanyl, Figure 2B. Thereafter, all heroin cases from the past year were subsequently electronically searched using the GC/MS full scan data files for the ions associated with fentanyl and acetyl fentanyl to help identify previously unsuspected cases involving these drugs. Acetyl fentanyl was analyzed by a newly developed ultrahigh performance liquid chromatography tandem mass spectrometry (UPLC-MS/MS) method (27).
Figure 2.
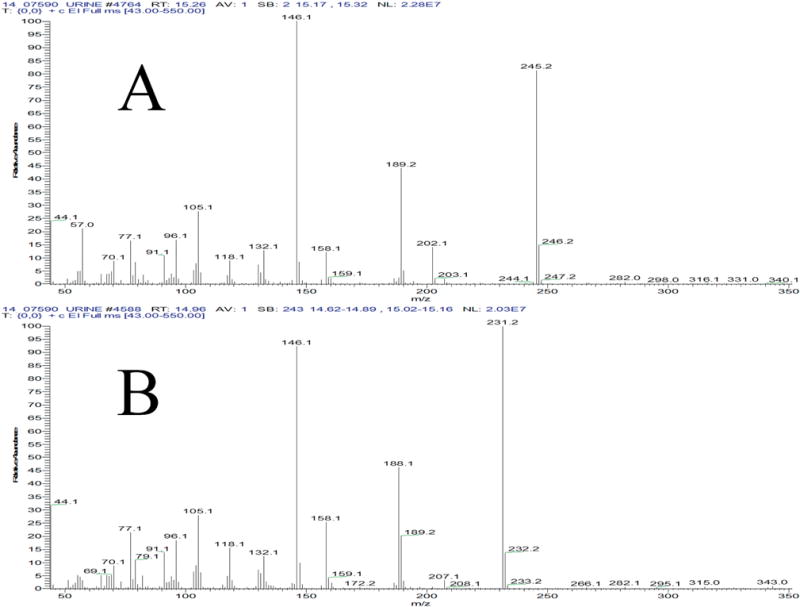
Electron impact gas chromatography mass spectrometry full scan mass spectra of fentanyl (A) and acetyl fentanyl (B).
RESULTS
The demographics of the victims in the 40 presented deaths from heroin and/or fentanyl abuse were as follows: 83% were male and 17% were female, average age was 36 years (range 19 to 57 years), and 88% were Caucasian and 12% were African American (in a county that is 75% Caucasian and 17% African American). All but one had a history of heroin abuse and/or evidence of intravenous drug use at the death scene such as powders, needles, syringes, tourniquets, and fresh track marks. Heroin use was evidenced by the toxicology findings of 6-MAM in 93% (37/40) of the deaths. Fentanyl was present in 27% (10/37) and acetyl fentanyl present in 11% (4/37) of these heroin cases. In only nine deaths was heroin the sole intoxicant. Polysubstance use was prevalent, as most cases had drugs of abuse other than opioids present. The most commonly detected drugs of abuse included alprazolam (12 cases), cocaine (9 cases), ethanol (7 cases), oxycodone (3 cases), methadone (3 cases), methamphetamine (3 cases), and hydromorphone (2 cases). Diphenhydramine, hydrocodone, citalopram, amitriptyline, nortriptyline, and morphine (without 6-MAM) were also found, each in a single death (see Tables 1 and 2). The deaths appeared to occur rapidly after drug administration as evidenced by powders, spoons, and syringes nearby (sometimes the syringe was extending from the decedents injection site). Two of the decedents were found dead in the same house with two unused lines of powdered drugs on the table, along with straws, presumably for insufflation. Most of the decedents were pronounced dead on scene, with only six of the decedents surviving long enough to be transported to local emergency departments.
Table 1.
Decedent’s Demographics, Case Histories, Toxicology Findings and the Causes and Manners of Death for the Heroin Cases Not Involving Fentanyl and/or Acetyl Fentanyl
| Case | Demographics | History | Toxicology Results | Cause and Manner of Death |
|---|---|---|---|---|
| 1 | 35 W/M | Decedent found dead on floor, used syringe and spoon with white residue nearby. | Morphine (free) 0.04 mg/L PB Morphine (total) 0.11 mg/L PB 6-MAM present VH, UR Diphenhydramine 0.10 mg/L PB Benzoylecgonine 0.04 mg/L PB |
Intoxication by heroin, cocaine and diphenhydramine Accident |
| 2 | 37 W/M | Decedent found dead in bathroom, syringe, spoon, baggies of heroin nearby. History of intravenous drug abuse. | Morphine (free) 0.29 mg/L PB Morphine (total) 0.46 mg/L PB 6-MAM present PB, VH, UR |
Intoxication by heroin Accident |
| 3 | 29 W/M | Decedent visiting with friends, heard struggling to breathe in bathroom. 911 called and police forced entry into bathroom. Decedent found dead on bathroom floor. Syringes and spoons nearby. | Morphine (free) 0.20 mg/L PB Morphine (total) 0.35 mg/L PB 6-MAM present PB |
Intoxication by heroin Accident |
| 4 | 57 W/M | Decedent found dead on floor in hotel room. Syringes and blood-stained rag found in trash can. | Morphine (free) 0.20 mg/L PB Morphine (total) 0.23 mg/L PB 6-MAM present PB Ethanol 0.14 g/dL PB |
Intoxication by heroin and ethyl alcohol Accident |
| 5 | 29 W/M | Decedent found dead in recliner. Syringes and white powdery substance nearby. Track marks under fingernails. History of heroin abuse. | Morphine (free) 0.04 mg/L PB Morphine (total) 0.55 mg/L PB 6-MAM present UR Ethanol 0.08 g/dL PB Cocaine 0.05 mg/L PB Cocaethylene 0.03 mg/L PB Benzoylecgonine 0.22 mg/L PB |
Intoxication by heroin, ethyl alcohol and cocaine Accident |
| 6 | 50 W/F | Decedent witnessed to snort an unknown white powder in car in parking lot. 911 called, advanced cardiac life support initiated, pronounced dead in emergency room. History of drug abuse. | Morphine (free) 0.18 mg/L PB Morphine (total) 0.31 mg/L PB 6-MAM present VH, UR Alprazolam 0.12 mg/L PB Amitriptyline 1.0 mg/L PB Nortriptyline 0.22 mg/L PB |
Intoxication by heroin Accident |
| 7 | 57 W/M | Decedent found dead on floor in apartment. Syringes and crack pipes nearby. History of crack cocaine and prescription drug abuse. | Morphine (free) 0.18 mg/L PB Morphine (total) 0.26 mg/L PB 6-MAM present PB, VH, UR Cocaine 0.12 mg/L PB Benzoylecgonine 3.6 mg/L PB |
Intoxication by heroin and cocaine Accident |
| 8 | 26 W/M | Decedent picked up by friend from his mother’s house. Reportedly, he was very “high.” Decedent wanted to sleep on friend’s sofa and was found dead the next day. Remote track marks in antecubital space. History of cocaine, heroin and prescription drug abuse. | Morphine (free) 0.06 mg/L PB Morphine (total) 0.33 mg/L PB 6-MAM present UR Cocaine 0.06 mg/L PB Benzoylecgonine 1.9 mg/L PB |
Intoxication by heroin and cocaine Accident |
| 9 | 38 W/M | Decedent found dead on bedroom floor. Syringe and spoon with residue nearby. History of intravenous heroin abuse. | Morphine (free) 0.35 mg/L PB Morphine (total) 0.76 mg/L PB 6-MAM present PB Cocaine 0.07 mg/L PB Benzoylecgonine 0.81 mg/L PB Alprazolam 0.03 mg/L PB |
Intoxication by heroin, cocaine and alprazolam Accident |
| 10 | 33 W/M | Decedent found dead in grassy area near highway in a state of decomposition. History of intravenous drug abuse. | Morphine (free) 0.12 mg/L PB Morphine (total) 0.12 mg/L PB 6-MAM present PB, UR Ethanol 0.11 g/dL PB |
Intoxication by heroin Accident |
| 11 | 35 W/M | Decedent found dead in bed, syringe in hand. Several syringes and a powdery substance on spoon nearby. History of heroin abuse. | Morphine (free) 0.14 mg/L PB Morphine (total) 0.19 mg/L PB 6-MAM present VH, UR Ethanol 0.05 g/dL PB |
Intoxication by heroin Accident |
| 12 | 37 W/M | Decedent at friend’s house when he “passed out.” Friend called 911 then left due to outstanding warrants. Paramedics arrived on scene, advanced cardiac life support was initiated, transported to emergency room where he was pronounced dead. History of heroin abuse. | Morphine (free) <0.02 mg/L PB Morphine (total) 0.10 mg/L PB 6-MAM present VH, UR |
Intoxication by heroin Accident |
| 13 | 46 W/M | Decedent found dead on living room floor. Used needle, spoon and white substance nearby. History of heroin abuse. | Morphine (free) 0.34 mg/L PB Morphine (total) 0.60 mg/L PB 6-MAM present PB, VH, UR |
Intoxication by heroin Accident |
| 14 | 19 W/M | Decedent said she was going to store with family dog. When she didn’t return, family found her seated in her parked car at the apartment complex office. 911 called, advanced cardiac life support initiated and pronounced dead in emergency room. History of heroin abuse. | Morphine (free) 0.02 mg/L PB Morphine (total) 0.04 mg/L PB 6-MAM present UR |
Intoxication by heroin Accident |
| 15 | 35 W/M | Decedent was at a gas station using heroin. Girlfriend picked him up. After driving ten to 15 minutes, girlfriend noticed him vomit and then stop breathing. 911 called, advanced cardiac life support initiated, pronounced dead in emergency room. History of heroin abuse. | Morphine (free) <0.02 mg/L PB Morphine (total) 0.02 mg/L PB 6-MAM present UR Oxycodone 0.20 mg/L PB Oxymorphone (total) 0.06 mg/L PB |
Intoxication by heroin and oxycodone Accident |
| 16 | 36 W/F | Decedent barricaded herself in bedroom for five hours. Boyfriend eventually gained entry and found her unresponsive. 911 called, advanced cardiac life support initiated, and transported to emergency room. Placed on ventilator in intensive care unit with poor prognosis and anoxic encephalopathy. Pronounced dead the next day. History of prescription drug abuse. | Morphine (free) 0.44 mg/L AB Morphine (total) 0.62 mg/L AB 6-MAM present VH, UR Alprazolam 0.02 mg/L AB Methadone 0.03 mg/L AB Hydromorphone (total) 0.02 mg/L AB |
Anoxic encephalopathy following resuscitation from cardiac arrest due to intoxication from heroin, methadone, alprazolam and hydromorphone Accident |
| 17 | 41 W/F | Decedent last seen by husband drinking and taking unknown amount of pills. Decedent found dead in bed the next morning. History of prescription drug abuse. | Morphine (free) 0.18 mg/L PB Morphine (total) 0.57 mg/L PB 6-MAM present PB Alprazolam 0.04 mg/L PB Oxycodone 0.08 mg/L PB Oxymorphone (total) 0.02 mg/L PB |
Intoxication by heroin, oxycodone and alprazolam Accident |
| 18 | 30 W/M | Decedent had been acting “strangely” for the past two weeks using escort services for sex. On date of death, he was noted to be going in and out of bathroom frequently. Found dead on bedroom floor, pair of scissors in hand. Loose pills, straws, rolled up $20 bills and unknown rock substance found in room. | Morphine (free) 0.12 mg/L PB Morphine (total) 0.15 mg/L PB 6-MAM present PB, VH, UR Ethanol 0.17 g/dL PB |
Intoxication by heroin and ethyl alcohol Accident |
| 19 | 32 W/M | Decedent found dead in car. Needles throughout car. History of intravenous drug abuse. | Morphine (free) 0.12 mg/L PB Morphine (total) 0.39 mg/L PB 6-MAM present VH, UR Hydrocodone 0.02 mg/L PB Methamphetamine 0.50 mg/L PB Amphetamine <0.05 mg/L PB Citalopram 0.46 mg/L PB |
Intoxication by heroin, methamphetamine and hydrocodone Accident |
| 20 | 24 W/F | Decedent was using cocaine and drinking with friends. Friends notice her sleeping on floor and snoring heavily, found dead later that day. Track marks on right arm. | Morphine (free) 0.06 mg/L PB Morphine (total) 0.21 mg/L PB 6-MAM present PB Ethanol 0.15 g/dL PB Cocaethylene <0.02 mg/L PB Benzoylecgonine 0.28 mg/L PB |
Intoxication by heroin, cocaine and ethyl alcohol Accident |
| 21 | 34 W/M | Decedent at home with friends and witnessed to stop breathing. 911 called and pronounced dead. History of intravenous heroin abuse. | Morphine (free) 0.14 mg/L PB Morphine (total) 0.79 mg/L PB 6-MAM present VH Methamphetamine 1.6 mg/L PB Amphetamine 0.08 mg/L PB |
Anoxic encephalopathy following resuscitation from cardiac arrest due to intoxication by heroin and methamphetamine Accident |
| 22 | 27 W/F | Decedent went to friend’s apartment and friend let her stay the night. She was heard snoring around midnight and found dead the next morning. Used needles and heroin found nearby. History of heroin and intravenous drug abuse, prostitution, and drug arrests. | Morphine (free) 0.05 mg/L PB Morphine (total) 0.15 mg/L PB 6-MAM present PB Benzoylecgonine 1.9 mg/L PB |
Intoxication by heroin, ethyl alcohol, alprazolam and cocaine Accident |
| 23 | 22 W/M | Decedent found dead in bed with foam cone in mouth. Pipes, cans, and syringes nearby. History of intravenous heroin, cocaine and methamphetamine abuse. | Morphine (free) 0.17 mg/L HB Morphine (total) 0.27 mg/L HB 6-MAM present VH, UR Codeine present HB, VH, UR Alprazolam 0.03 mg/L HB Benzoylecgonine 0.06 mg/L HB |
Intoxication by heroin, cocaine and alprazolam Accident |
| 24 | 34 B/M | Decedent went to take a bath (normal at night). He was in bathroom for long time and found dead on bathroom floor. Use syringe nearby and fresh track mark on left arm. History of intravenous drug abuse. | Morphine (free) 0.15 mg/L PB Morphine (total) 0.31 mg/L PB 6-MAM present VH, UR Ethanol 0.17 g/dL PB Ethanol 0.20 g/dL VH |
Intoxication by heroin and ethyl alcohol Accident |
| 25 | 22 W/M | Decedent was at friend’s house, drank three beers, complained of being “itchy” and took a shower, still “itchy” and took another shower. Found dead in bedroom. No drug paraphernalia in house. History of cocaine, ecstasy, and marijuana use. | Morphine (free) 0.30 mg/L PB Morphine (total) 1.1 mg/L PB 6-MAM present VH, UR |
Intoxication by heroin Accident |
| 26 | 36 B/M | Decedent staying at friend’s house and went to bathroom. Friend heard water running for three hours, then heard water turned off and decedent never came out of bathroom. Found dead on bathroom floor, spoon with residue nearby. History of intravenous drug abuse. | Morphine (free) 0.43 mg/L PB Morphine (total) 0.56 mg/L PB Alprazolam 0.20 mg/L PB 6-MAM present PB, VH, UR |
Intoxication by heroin and alprazolam Accident |
M (male)
F (female)
W (white)
B (black)
PB (peripheral blood)
HB (heart blood)
AB (antemortem blood)
6-MAM (6-monoacetylmorphine)
UR (urine)
VH (vitreous humor)
Table 2.
Decedent’s Demographics, Case Histories, Toxicology Findings and the Causes and Manners of Death for Fentanyl and Acetyl Fentanyl Cases
| Case | Demographics | History | Toxicology Results | Cause and Manner of Death |
|---|---|---|---|---|
| 1 | 46 W/M | Decedent found dead on bedroom floor. History of prescription drug abuse. | Morphine (free) 0.03 mg/L PB Morphine (total) 0.06 mg/L PB 6-MAM present PB Fentanyl 0.020 mg/L PB Acetyl Fentanyl 0.009 mg/L PB Cocaine 0.07 mg/L PB Benzoylecgonine 0.97 mg/L PB |
Intoxication by heroin, fentanyl, acetyl fentanyl and cocaine Accident |
| 2 | 39 W/M | Decedent found dead in bed. Used needles, spoon and white powder nearby. History of heroin and cocaine abuse. | Morphine (free) negative PB Morphine (total) 0.02 mg/L PB 6-MAM present VH, UR Fentanyl 0.015 mg/L PB Acetyl Fentanyl 0.012 PB mg/L |
Intoxication by heroin, fentanyl and acetyl fentanyl Accident |
| 3 | 41 W/M | Decedent found dead in bathroom. Spoon, needle and syringe nearby. History of drug abuse. | Morphine (free) <0.02 mg/L PB Morphine (total) <0.02 mg/L PB 6-MAM present PB Alprazolam 0.03 mg/L PB Fentanyl 0.019 mg/L PB Acetyl Fentanyl 0.002 mg/L PB |
Intoxication by heroin, fentanyl, acetyl fentanyl and alprazolam Accident |
| 4 | 40 W/M | Decedent found dead in hotel room. Syringe and powder nearby. History of heroin abuse. | Morphine (free) 0.02 mg/L PB Morphine (total) 0.03 mg/L PB 6-MAM present PB Fentanyl 0.004 mg/L PB |
Intoxication by heroin and fentanyl Accident |
| 5 | 44 W/M | Decedent found dead in bathroom (in same house as case below). White powdery substance and straws on bedroom table. | Morphine (free) 0.02 mg/L PB Morphine (total) 0.04 mg/L PB 6-MAM present VH, UR Methadone 0.32 mg/L PB Alprazolam 0.03 mg/L PB Fentanyl 0.007 mg/L PB |
Intoxication by heroin, fentanyl, methadone and alprazolam Accident |
| 6 | 40 W/F | Decedent found dead in bedroom (in same house as case above). White powdery substance and straws on bedroom table. | Morphine (free) 0.05 mg/L PB Morphine (total) 0.08 mg/L PB 6-MAM present PB Methadone 0.40 mg/L PB Alprazolam 0.03 mg/L PB Fentanyl 0.038 mg/L HB |
Intoxication by heroin, fentanyl, methadone and alprazolam Accident |
| 7 | 53 W/M | Decedent found dead in chair. Syringe, spoon and three baggies of white powder nearby. History of intravenous drug abuse. | Morphine (free) 0.10 mg/L PB Morphine (total) 0.09 mg/L PB 6-MAM present PB, VH, UR Fentanyl 0.004 mg/L PB Methamphetamine 0.27 mg/L PB |
Intoxication by heroin, fentanyl and methamphetamine Accident |
| 8 | 40 W/M | Decedent found dead on bathroom floor. Spoon and syringe nearby. | Morphine (free) 0.02 mg/L PB Morphine (total) 0.06 mg/L PB 6-MAM present PB Hydromorphone (free) <0.02 PB Hydromorphone (total) 0.04 PB Fentanyl 0.015 mg/L PB |
Intoxication by heroin, fentanyl and hydromorphone Accident |
| 9 | 38 B/M | Decedent moved out of wife’s house two weeks prior due to domestic violence injunction. He returned to wife’s house while she was at work to walk the dog. Wife returned from work and found decedent dead on bathroom floor. Syringe and tourniquet nearby. History of intrave nous drug abuse. | Morphine (free) <0.02 mg/L PB Morphine (total) 0.03 mg/L PB 6-MAM present VH, UR Fentanyl 0.007 mg/L PB |
Intoxication by heroin and fentanyl Accident |
| 10 | 50 W/M | Decedent found dead on bathroom floor. Small red plastic baggie in toilet and syringe found in pocket. Recently released from prison. History of heroin abuse. | Morphine (free) 0.10 mg/L HB Morphine (total) 0.24 mg/L HB 6-MAM present VH, UR Fentanyl 0.016 mg/L HB |
Intoxication by heroin and fentanyl Accident |
| 11 | 55 W/M | Decedent found unresponsive in recliner. 911 called, advanced cardiac life support initiated and transported to emergency room. Admitted to intensive care unit and died next day. Oxycodone filled the day before with 60 pills, 30 remained. | Oxycodone 0.08 mg/L AB Oxymorphone (total) 0.02 mg/L AB Alprazolam <0.02 mg/L AB Acetyl Fentanyl 0.31 mg/L PB |
Intoxication by acetyl fentanyl and oxycodone Accident |
| 12 | 26 B/F | Decedent found dead in bathroom, sitting on toilet with needle in arm. History of intravenous heroin abuse. | Morphine (free) 0.03 mg/L PB Morphine (total) 0.07 mg/L PB Acetyl Fentanyl 0.40 mg/L PB |
Intoxication by acetyl fentanyl and morphine Accident |
| 13 | 30 W/M | Decedent found dead in bed in motel room. Last seen alive the night before by brother and seemed intoxicated. Needle marks in left arm, spoon and straws nearby. History of intravenous heroin abuse. | Alprazolam 0.02 mg/L PB Acetyl Fentanyl 0.56 mg/L PB |
Intoxication by acetyl fentanyl and alprazolam Accident |
| 14 | 28 W/M | Decedent found dead in bed in motel room. Razor blades, white powdery substances, straws, syringes and lighter nearby. History of heroin abuse. | Alprazolam 0.23 mg/L PB Acetyl Fentanyl 0.60 mg/L PB |
Intoxication by acetyl fentanyl and alprazolam Accident |
M (male)
F (female)
W (white)
B (black)
PB (peripheral blood)
HB (heart blood)
AB (antemortem blood)
6-MAM (6-monoacetylmorphine)
UR (urine)
VH (vitreous humor)
Victim demographics, case histories with cause and manner of death, and toxicology findings for 26 heroin deaths that did not also involve fentanyl and/or acetyl fentanyl are presented in Table 1. Similar data for 14 deaths involving fentanyl and/or acetyl fentanyl are presented in Table 2. In the 26 heroin deaths that did not also involve a fentanyl derivative, free and total peripheral blood morphine concentrations averaged 0.16 mg/L and 0.35 mg/L, respectively (Table 3). In general, these peripheral blood values are consistent with other reported studies of fatal heroin overdoses (28–32). Two of the cases (Table 1, Cases 12 and 14) had low morphine concentrations that may be indicative of delayed heroin deaths. In addition, the analysis of vitreous humor and urine was very useful to help identify the heroin metabolite, 6-MAM. 6-MAM appears to have a longer detection window in vitreous humor and urine, presumably due to the absence of plasma esterase activity (29–32). All the presented heroin cases had 6-MAM identified in at least one postmortem specimen. In contrast, in the heroin cases with fentanyl and acetyl fentanyl, morphine was either not detected or present at extremely low free and total peripheral blood concentrations, averaging 0.010 mg/L and 0.030 mg/L, respectively (Table 3). In the heroin cases involving fentanyl and acetyl fentanyl, the average fentanyl and acetyl fentanyl peripheral blood concentrations were 0.018 mg/L and 0.008 mg/L, respectively (Table 3). These data are consistent with reported lethal fentanyl intoxications and demonstrate that the fentanyl derivatives were the major intoxicants in these deaths (11, 13–15, 33–36). In the cases involving acetyl fentanyl where fentanyl was not detected nor was evidence of heroin use present, the average acetyl fentanyl peripheral blood concentration was 0.47 mg/L (range 0.31 to 0.60 mg/L, n=4) and the average acetyl norfentanyl concentration was 0.053 mg/L (range 0.02 to 0.086 mg/L, n=4) (Table 3). The higher blood concentrations of acetyl fentanyl compared to fentanyl may be due to victims administering larger doses of the acetyl analogue or be reflective of its lower potency compared to fentanyl; therefore, greater blood and/or brain concentrations of acetyl fentanyl may be required to cause death than those cases with fentanyl.
Table 3.
Average Peripheral Blood Drug Opioid Concentrations and Ranges (in Parentheses) in mg/L in Heroin Related Fatalities
| Type of case | Morphine (Free) |
Morphine (Total) |
Fentanyl | Norfentanyl | Acetyl Fentanyl | Acetyl Norfentanyl |
|---|---|---|---|---|---|---|
| Heroin n=26 |
0.160 (0.020–0.430) |
0.35 (0.040–1.10) |
||||
| Heroin and Fentanyl n=7 |
0.040 (none – 0.10) |
0.080 (0.030–0.90) |
0.012 (0.004–0.027) |
0.001 (0.002–0.003) |
||
| Heroin, Fentanyl and Acetyl Fentanyl n=3 |
0.010 (none – 0.030) |
0.030 (none – 0.060) |
0.018 (0.015–0.020) |
0.002 (0.001–0.003) |
0.008 (0.006–0.012) |
0.001 (0.001–0.002) |
| Acetyl Fentanyl n=4 |
0.470 (0.31–0.60) |
0.053 (0.002–0.086) |
DISCUSSION
The presented case demographics in Tables 1 and 2 are remarkably similar to the fentanyl and fentanyl analog epidemic in California in the 1980’s (13–15). California reported an average age of 32 years (range, 19 to 57 years), with victims being 78% male and 79% Caucasian. In addition, other similarities included evidence of drug use or drug paraphernalia at the death scenes with a suggestion of rapid demise after drug administration. California had five victims surviving long enough to be transported to a hospital, whereas this study had six such victims. Cocaine and alcohol were other commonly detected drugs. In addition, many of the decedents were found dead in bathrooms, bedrooms, and hotel rooms, in isolation, perhaps in an attempt to conceal drug use. However, the fatal fentanyl blood concentrations in the California epidemic were much lower with an average value of 0.003 mg/L compared to this study with an average fentanyl value of 0.018 mg/L. This could be due to a difference in analytical technique since the California fentanyl concentrations were based on radioimmunoassay testing and not GC/MS or HPLC-MS/MS.
In the initial cases in which fentanyl and/or acetyl fentanyl were detected, the deaths were unusual in that the decedent had a history of heroin use, with drug paraphernalia found at the scene, yet the blood morphine concentrations were remarkably low compared to other fatal heroin overdose deaths. It was evident that some additional intoxicant was involved in the case. Once fentanyl was identified and quantitated using selected ion monitoring, the presence of the earlier eluting compound with m/z 146 ion raised the suspicion of another fentanyl derivative. The ion of m/z 231, m/z 14 less than fentanyl, led to the identification of acetyl fentanyl. Many of the fentanyl analogues have common ions, therefore, it is prudent to obtain a full scan mass spectra to compare to certified reference materials for definitive identification.
At the time the autopsy and toxicology testing were completed on these cases, there were no published reports of acetyl fentanyl concentrations in human biological specimens, including postmortem tissues or fluids. Therefore, the determination that acetyl fentanyl contributed to the cause of death in some of these cases was based on autopsy findings, toxicology findings, individual case histories, and the likely pharmacological similarity of acetyl fentanyl to fentanyl. In the cases with acetyl fentanyl only, the acetyl fentanyl concentrations were incredibly high, requiring dilution for analysis. Three of the four acetyl fentanyl deaths occurred within two days of each other. In addition, the acetyl fentanyl concentrations were much higher than what had been seen in the previously reported fentanyl fatalities. This raised the suspicion that these more recent acetyl fentanyl cases appeared to be related to a new supply of drug in the area. Law enforcement was able to link the three cases to the same drug dealer. Since the time these cases were analyzed, there was a single case report of an acetyl fentanyl fatality with an acetyl fentanyl peripheral blood concentration of 0.26 mg/L, consistent with the acetyl fentanyl blood concentrations reported in Table 3 (37).
As with all postmortem cases, postmortem redistribution can influence the toxicology results as well as the interpretation of the toxicology results. Fentanyl is highly lipophilic, 80% plasma protein-bound with a high volume of distribution—all characteristics that would suggest that fentanyl would display significant postmortem redistribution (6, 38). The postmortem interval (from time of death to time of autopsy) could also potentially influence postmortem drug concentrations. The estimated postmortem interval for the presented cases was only four to twelve hours, so any influence from the postmortem interval was likely minimal. Several published reports have indicated postmortem fentanyl blood concentrations, whether specimens are obtained from the heart or femoral artery, are unreliable for the determination of the fentanyl blood concentration at the time of death and ascribing fentanyl overdose as a cause of death (39, 40). However, these assertions have been refuted by considering other physiological and pharmaceutical factors. In an extensive published review of the postmortem fentanyl literature, deaths involving the rapid administration of fentanyl or the administration of large bolus doses of fentanyl were found to have incomplete fentanyl distribution throughout the body tissues and fluids (41). Thus, nonequilibrium pharmacokinetics results in higher fentanyl heart blood concentrations than femoral blood values simply due to relative blood flow through the various vessels and organs prior to death. Further, in deaths in which fentanyl had been routinely administered by a transdermal patch in therapeutic concentrations, a situation in which equilibrium kinetics are most likely, no evidence of postmortem redistribution was observed and the blood concentrations were relatively equal throughout the body (41). A central blood to peripheral blood drug concentration ratio of approximately one demonstrates a minimal tendency towards postmortem redistribution (42). Central blood to peripheral blood fentanyl ratios of 1.2 and 0.95 were reported in studies of 166 cases and 18 cases, respectively (41), suggesting fentanyl has minimal postmortem redistribution. In a study evaluating 92 deaths involving the therapeutic use and abuse of fentanyl transdermal patches, a variable relationship between a given fentanyl dose and resultant postmortem blood concentration was observed (43). This published study, similar to the cases presented in Table 2, also noted that many of the fentanyl deaths involve polysubstance use and other potentially toxic drugs. Although this published study concluded that in many cases the postmortem fentanyl concentrations do not reliably predict antemortem blood concentrations, the authors noted that the lack of reliability of postmortem fentanyl blood concentrations does not preclude decision making as to the cause and manner of death in cases when fentanyl is present (43). Other factors such as drugs and drug paraphernalia at the death scene, circumstances surrounding the death, autopsy findings, and toxicology reports all contribute to the conclusion that fentanyl was a cause and/or significant contributor to the cause of death.
In reviewing these reported heroin deaths, it became evident that the drug supply in the Tampa area was constantly changing. At times, there would be only heroin overdose cases. At other times, there would be a cluster of deaths in a short period of time involving only acetyl fentanyl or heroin combined with fentanyl and/or acetyl fentanyl. On the other hand, several weeks could go by with no heroin deaths at all. To help law enforcement identify the suppliers of heroin in the area, detectives were notified immediately of any suspected heroin-related deaths and as soon as the toxicology results confirmed heroin, fentanyl, or acetyl fentanyl. There was nothing unique about the death scenes, drug packets, drug paraphernalia, or drug powders that could be visually identified that would indicate whether the administered powders contained heroin, acetyl fentanyl, fentanyl, or other drug mixtures. None of the presented cases had prescriptions for fentanyl or evidence of pharmaceutical fentanyl at the death scenes (patches, injectables, or oral lozenges). Several of the drug powders and syringes found at the death scenes were analyzed by either the toxicology laboratory, or the local forensic drug lab and they contained various mixtures of heroin, fentanyl, and/or acetyl fentanyl. Some of the powders contained little heroin with larger amounts of fentanyl and/or acetyl fentanyl. The differing amounts of heroin, fentanyl, and/or acetyl fentanyl in the actual drug powders and syringes at the death scenes may explain some of the differences observed in the concentrations of drugs identified in the toxicology reports.
CONCLUSION
Medical examiners, coroners, and postmortem toxicology laboratories should be cognizant of their cases in which the case history and circumstances suggest an opiate overdose-related death, yet the toxicology findings are negative or have only trace amounts of drugs detected. These cases could potentially contain fentanyl, acetyl fentanyl, or other fentanyl analogs such as butyryl fentanyl. The presented cases, with associated drug concentrations, case histories, demographics, and causes and manners of death may help provide assistance with the interpretation of the postmortem findings. In addition, the rapid identification of new or unusual drugs of abuse or illicit drug mixtures in fatal poisonings may aid law enforcement in the timely identification of new illicit drug sources, hopefully saving lives in the process.
Acknowledgments
FUNDING
This project was supported in part by the National Institutes of Health (NIH) grant P30DA033934.
Footnotes
FINANCIAL DISCLOSURE
The authors have indicated that they do not have financial relationships to disclose that are relevant to this manuscript
DISCLOSURES
The authors, reviewers, editors, and publication staff do not report any relevant conflicts of interest
Contributor Information
Julia Pearson, Hillsborough County Medical Examiner Department.
Justin Poklis, Department of Pharmacology and Toxicology, Virginia Commonwealth University.
Alphonse Poklis, Department of Pharmacology and Toxicology, Department of Pathology, and Department of Forensic Science, Virginia Commonwealth University.
Carl Wolf, Department of Pathology, and Department of Forensic Science, Virginia Commonwealth University.
Mary Mainland, Hillsborough County Medical Examiner Department.
Laura Hair, Hillsborough County Medical Examiner Department.
Kelly Devers, Hillsborough County Medical Examiner Department
Leszek Chrostowski, Hillsborough County Medical Examiner Department.
Elise Arbefeville, Hillsborough County Medical Examiner Department.
Michele Merves, Hillsborough County Medical Examiner Department.
References
- 1.Rudd RA, Paulozzi LJ, Bauer MJ, et al. Increases in heroin overdose deaths - 28 States 2010 to 2012. MMWR Morb Mortal Wkly Rep. 2014 Oct 3;63(39):849–54. [PMC free article] [PubMed] [Google Scholar]
- 2.Slavova S, Bunn T, Lambert J. Drug overdose deaths in Kentucky, 2000–2013 [Internet] Lexington (KY): Kentucky Injury Prevention and Research Center; 2015. Mar, p. 17. cited 2015 Jun 4. Available from: http://www.mc.uky.edu/kiprc/projects/ddmarpdak/pdf/KyDrugOverdoseDeaths-2000–2013.pdf. [Google Scholar]
- 3.Drugs identified in deceased persons by Florida medical examiners - 2013 annual report [Internet] Tallahassee: Florida Department of Law Enforcement; 2014. Oct, p. 49. cited 2015 Jun 4. Available from: http://www.fdle.state.fl.us/Content/getdoc/05c6ff97-00cc-49b2-9ca5-5dacd4539b1a/2013-Annual-Drug-Report-(2).aspx. [Google Scholar]
- 4.Drugs identified in deceased persons by Florida medical examiners - interim report 2014 [Internet] Tallahassee: Florida Department of Law Enforcement; 2015. Apr, p. 32. cited 2015 Jun 4. Available from: http://www.fdle.state.fl.us/Content/Medical-Examiners-Commission/MEC-Publications-and-Forms/Documents/2014-Interim-Drug-Report-FINAL.aspx. [Google Scholar]
- 5.National heroin threat assessment summary [Internet] U.S. Drug Enforcement Administration; 2015. p. 12. cited 2015 Jun 4. Available from: http://www.dea.gov/divisions/hq/2015/hq052215_National_Heroin_Threat_Assessment_Summary.pdf. [Google Scholar]
- 6.Centers for Disease Control and Prevention (CDC) Acetyl fentanyl overdose fatalities–Rhode Island, March–May 2013. MMWR Morb Mortal Wkly Rep. 2013 Aug 30;62(34):703–4. [PMC free article] [PubMed] [Google Scholar]
- 7.Mercado-Crespo MC, Sumner SA, Spelke MB, et al. Notes from the field: increase in fentanyl-related overdose deaths - Rhode Island, November 2013–March 2014. MMWR Morb Mortal Wkly Rep. 2014 Jun 20;63(24):531. [PMC free article] [PubMed] [Google Scholar]
- 8.DEA [Internet] Washington: U.S. Drug Enforcement Administration; 2015. Mar 18, (DEA issues nationwide alert on fentanyl as threat to health and public safety). c2015. [cited 2015 Jun 1]. Available from: http://www.dea.gov/divisions/hq/2015/hq031815.shtml. [Google Scholar]
- 9.Lozier M, Boyd M, Stanley C, et al. Acetyl Fentanyl, a Novel Fentanyl Analog, Causes 14 Overdose Deaths in Rhode Island, March–May 2013. J Med Toxicol. 2015 Jun;11(2):208–17. doi: 10.1007/s13181-015-0477-9. http://dx.doi.org/10.1007/s13181-015-0477-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Stogner JM. The potential threat of acetyl fentanyl: legal issues, contaminated heroin, and acetyl fentanyl “disguised” as other opioids. Ann Emerg Med. 2014 Dec;64(6):637–9. doi: 10.1016/j.annemergmed.2014.07.017. http://dx.doi.org/10.1016/j.annemergmed.2014.07.017. [DOI] [PubMed] [Google Scholar]
- 11.Poklis A. Fentanyl: a review for clinical and analytical toxicologists. J Toxicol Clin Toxicol. 1995;33(5):439–47. doi: 10.3109/15563659509013752. http://dx.doi.org/10.3109/15563659509013752. [DOI] [PubMed] [Google Scholar]
- 12.Van Bever WF, Niemegeers CJ, Janssen P. A Synthetic analgesics. Synthesis and pharmacology of the diastereoisomers of N-(3-methyl-1-(2-phenylethyl)-4-piperidyl)-N-phenylpropanamide and N-(3-methyl-1-(1-methyl-2-phenylethyl)-4-piperidyl)-N-phenylpropanamide. J Med Chem. 1974 Oct;17(10):1047–51. doi: 10.1021/jm00256a003. http://dx.doi.org/10.1021/jm00256a003. [DOI] [PubMed] [Google Scholar]
- 13.Henderson GL. Designer drugs: past history and future prospects. J Forensic Sci. 1988 Mar;33(2):569–75. [PubMed] [Google Scholar]
- 14.Henderson GL. Blood concentrations of fentanyl and its analogs in overdose victims. Proc West Pharmacol Soc. 1983;26:287–90. [PubMed] [Google Scholar]
- 15.Henderson G. Fentanyl - related deaths: demographics, circumstances and toxicology of 112 cases. J Forensic Sci. 1991 Mar;36(2):422–33. [PubMed] [Google Scholar]
- 16.Baum R. Designer drugs: underground chemists play a deadly trade. Chem Eng News. 1985 Sep;9:7–16. [Google Scholar]
- 17.Hibss J, Perper J, Winek CL. An outbreak of designer drug-related deaths in Pennsylvania. JAMA. Feb;265(8):1991. 27, 1011–3. doi: 10.1001/jama.265.8.1011. http://dx.doi.org/10.1001/jama.265.8.1011. [DOI] [PubMed] [Google Scholar]
- 18.Centers for Disease Control and Prevention (CDC) Nonpharmaceutical fentanyl-related deaths–multiple states, April 2005–March 2007. MMWR Morb Mortal Wkly Rep. 2008 Jul 25;57(29):793–6. [PubMed] [Google Scholar]
- 19.Schumann H, Erickson T, Thompson T, et al. Fentanyl epidemic in Chicago, Illinois and surrounding Cook County. Clin Toxicol (Phila) 2008 Jul;46(6):501–6. doi: 10.1080/15563650701877374. http://dx.doi.org/10.1080/15563650701877374. [DOI] [PubMed] [Google Scholar]
- 20.Thompson JG, Baker AM, Bracey AH, et al. Fentanyl concentrations in 23 postmortem cases from the Hennepin County medical examiner’s office. J Forensic Sci. 2007 Jul;52(4):978–81. doi: 10.1111/j.1556-4029.2007.00481.x. http://dx.doi.org/10.1111/j.1556-4029.2007.00481.x. [DOI] [PubMed] [Google Scholar]
- 21.Martin M, Hecker J, Clark R, et al. China White epidemic: an eastern United States emergency department experience. Ann Emerg Med. 1991 Feb;20(2):158–64. doi: 10.1016/s0196-0644(05)81216-8. http://dx.doi.org/10.1016/s0196-0644(05)81216-8. [DOI] [PubMed] [Google Scholar]
- 22.Ojanperä I, Gergov M, Liiv M, et al. An epidemic of fatal 3-methylfentanyl poisoning in Estonia. Int J Legal Med. 2008 Sep;122(5):395–400. doi: 10.1007/s00414-008-0230-x. http://dx.doi.org/10.1007/s00414-008-0230-x. [DOI] [PubMed] [Google Scholar]
- 23.Higashikawa Y, Suzuki S. Studies on 1-(2-phenethyl)-4-(N-propionylanilino)piperidine (fentanyl) and its related compounds. VI. Structure-analgesic activity relationship for fentanyl, methyl-substituted fentanyls and other analogues. Forensic Toxicol. 2008 Jun;26(1):1–5. http://dx.doi.org/10.1007/s11419-007-0039-1. [Google Scholar]
- 24.Flammia DD, Bateman HR, Saady JJ, Christensen ED. Tissue distribution of molidone in a multidrug overdose. J Anal Toxicol. 2004 Sep;28(6):533–6. doi: 10.1093/jat/28.6.533. http://dx.doi.org/10.1093/jat/28.6.533. [DOI] [PubMed] [Google Scholar]
- 25.Dams R, Murphy CM, Choo RE, et al. LC-atmospheric pressure chemical ionization-MS/MS analysis of multiple illicit drugs, methadone, and their metabolites in oral fluid following protein precipitation. Anal Chem. 2003 Feb 15;75(4):798–804. doi: 10.1021/ac026111t. http://dx.doi.org/10.1021/ac026111t. [DOI] [PubMed] [Google Scholar]
- 26.Rook E, Hillebrand MJ, Rosing H, et al. The quantitative analysis of heroin, methadone and their metabolites and the simultaneous detection of cocaine, acetylcodeine and their metabolites in human plasma by high-performance liquid chromatography coupled with tandem mass spectrometry. J Chromatogr B Analyt Technol Biomed Life Sci. 2005 Sep 25;824(1–2):213–21. doi: 10.1016/j.jchromb.2005.05.048. http://dx.doi.org/10.1016/j.jchromb.2005.05.048. [DOI] [PubMed] [Google Scholar]
- 27.Poklis J, Poklis A, Wolf C, et al. Postmortem tissue distribution of acetyl fentanyl, fentanyl and their respective nor-metabolites analyzed by ultrahigh performance liquid chromatography with tandem mass spectrometry. Forensic Sci Int. 2015 Dec;257:435–41. doi: 10.1016/j.forsciint.2015.10.021. http://dx.doi.org/10.1016/j.forsciint.2015.10.021. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Drummer OH. Postmortem toxicology of drugs of abuse. Forensic Sci Int. 2004 Jun 10;142(2–3):101–13. doi: 10.1016/j.forsciint.2004.02.013. http://dx.doi.org/10.1016/j.forsciint.2004.02.013. [DOI] [PubMed] [Google Scholar]
- 29.Wyman J, Bultman S. Postmortem distribution of heroin metabolites in femoral blood, liver, cerebrospinal fluid, and vitreous humor. J Anal Toxicol. 2004 May-Jun;28(4):260–3. doi: 10.1093/jat/28.4.260. http://dx.doi.org/10.1093/jat/28.4.260. [DOI] [PubMed] [Google Scholar]
- 30.Rees KA, Pounder DJ, Osselton MD. Distribution of opiates in femoral blood and vitreous humour in heroin/morphine-related deaths. Forensic Sci Int. 2013 Mar 10;226(1–3):152–9. doi: 10.1016/j.forsciint.2013.01.002. http://dx.doi.org/10.1016/j.forsciint.2013.01.002. [DOI] [PubMed] [Google Scholar]
- 31.Pragst F, Spiegel K, Leuschner U, Hager A. Detection of 6-acetylmorphine in vitreous humor and cerebrospinal fluid–comparison with urinary analysis for proving heroin administration in opiate fatalities. J Anal Toxicol. 1999 May-Jun;23(3):168–72. doi: 10.1093/jat/23.3.168. http://dx.doi.org/10.1093/jat/23.3.168. [DOI] [PubMed] [Google Scholar]
- 32.Pearson J, Saady J. Utility of vitreous humor in investigations of heroin-related deaths. J Anal Toxicol. 2003 Apr;27(3):199. [Google Scholar]
- 33.Edinboro LE, Poklis A, Trautman D, et al. Fatal fentanyl intoxication following excessive transdermal application. J Forensic Sci. 1997 Jul;42(4):741–3. [PubMed] [Google Scholar]
- 34.Anderson DT, Muto JJ. Duragesic transdermal patch: postmortem tissue distribution of fentanyl in 25 cases. J Anal Toxicol. 2000 Oct;24(7):627–34. doi: 10.1093/jat/24.7.627. http://dx.doi.org/10.1093/jat/24.7.627. [DOI] [PubMed] [Google Scholar]
- 35.Kuhlman JJ, Jr, McCaulley R, Valouch TJ, Behonick GS. Fentanyl use, misuse, and abuse: a summary of 23 postmortem cases. J Anal Toxicol. 2003 Oct;27(7):499–504. doi: 10.1093/jat/27.7.499. http://dx.doi.org/10.1093/jat/27.7.499. [DOI] [PubMed] [Google Scholar]
- 36.Martin TL, Woodall KL, McLellan BA. Fentanyl-related deaths in Ontario, Canada: toxicological findings and circumstances of death in 112 cases 2002–2004. J Anal Toxicol. 2006 Oct;30(8):603–10. doi: 10.1093/jat/30.8.603. http://dx.doi.org/10.1093/jat/30.8.603. [DOI] [PubMed] [Google Scholar]
- 37.McIntyre IM, Trochta A, Gary RD, et al. An acute acetyl fentanyl fatality: a case report with postmortem concentrations. J Anal Toxicol. 2015 Jul-Aug;39(6):490–4. doi: 10.1093/jat/bkv043. http://dx.doi.org/10.1093/jat/bkv043. [DOI] [PubMed] [Google Scholar]
- 38.Prouty RW, Anderson WH. The forensic science implications of site and temporal influences on postmortem blood-drug concentrations. J Forensic Sci. 1990 Mar;35(2):243–70. [PubMed] [Google Scholar]
- 39.Luckenbill K, Thompson J, Middleton O, et al. Fentanyl postmortem redistribution: preliminary findings regarding the relationship among femoral blood and liver and heart tissue concentrations. J Anal Toxicol. 2008 Oct;32(8):639–43. doi: 10.1093/jat/32.8.639. http://dx.doi.org/10.1093/jat/32.8.639. [DOI] [PubMed] [Google Scholar]
- 40.Olson KN, Luckenbill K, Thompson J, et al. Postmortem redistribution of fentanyl in blood. Am J Clin Pathol. 2010 Mar;133(3):447–53. doi: 10.1309/AJCP4X5VHFSOERFT. http://dx.doi.org/10.1309/ajcp4x5vhfsoerft. [DOI] [PubMed] [Google Scholar]
- 41.McIntyre IM, Anderson DT. Postmortem fentanyl concentrations: a review. J Forensic Res. 2012;3:157. http://dx.doi.org/10.4172/2157-7145.1000157. [Google Scholar]
- 42.Dalpe-Scott M, Degouffe M, Garbutt D, Drost M. A comparison of drug concentrations in postmortem cardiac and peripheral blood in 320 cases. Canadian Soc Forensic Sci J. 1995;28(2):113–21. http://dx.doi.org/10.1080/00085030.1995.10757474. [Google Scholar]
- 43.Gill J, Lin P, Nelson L. Reliability of postmortem fentanyl concentrations in determining the cause of death. J Med Toxicol. 2013 Mar;9(1):34–41. doi: 10.1007/s13181-012-0253-z. http://dx.doi.org/10.1007/s13181-012-0253-z. Erratum in: J Med Toxicol. 2015 Sep; 11(3):382. http://dx.doi.org/10.1007/s13181-014-0427-y. [DOI] [PMC free article] [PubMed] [Google Scholar]