

Abstract
IMPORTANCE
Low-income minority children living in urban neighborhoods are at high risk for mental health problems and underachievement. ParentCorps, a family-centered, school-based intervention in prekindergarten, improves parenting and school readiness (ie, self-regulation and preacademic skills) in 2 randomized clinical trials. The longer-term effect on child mental health and academic performance is not known.
OBJECTIVE
To examine whether ParentCorps delivered as an enhancement to prekindergarten programs in high-poverty urban schools leads to fewer mental health problems and increased academic performance in the early elementary school years.
DESIGN, SETTING, AND PARTICIPANTS
This is a 3-year follow-up study of a cluster randomized clinical trial of ParentCorps in public schools with prekindergarten programs in New York City. Ten elementary schools serving a primarily low-income, black student population were randomized in 2005, and 4 consecutive cohorts of prekindergarten students were enrolled from September 12, 2005, through December 31, 2008. We report follow-up for the 3 cohorts enrolled after the initial year of implementation. Data analysis was performed from September 1, 2014, to December 31, 2015.
INTERVENTIONS
ParentCorps included professional development for prekindergarten and kindergarten teachers and a program for parents and prekindergarten students (13 two-hour group sessions delivered after school by teachers and mental health professionals).
MAIN OUTCOMES AND MEASURES
Annual teacher ratings of mental health problems and academic performance and standardized tests of academic achievement in kindergarten and second grade by testers masked to the intervention or control group randomization.
RESULTS
A total of 1050 children (4 years old; 518 boys [49.3%] and 532 girls [50.7%]) in 99 prekindergarten classrooms participated in the trial (88.1% of the prekindergarten population), with 792 students enrolled from 2006 to 2008. Most families in the follow-up study (421 [69.6%]) were low income; 680 (85.9%) identified as non-Latino black, 78 (9.8%) as Latino, and 34 (4.3%) as other. Relative to their peers in prekindergarten programs, children in ParentCorps-enhanced prekindergarten programs had lower levels of mental health problems (Cohen d = 0.44; 95% CI, 0.08–0.81) and higher teacher-rated academic performance (Cohen d = 0.21; 95% CI, 0.02–0.39) in second grade.
CONCLUSIONS AND RELEVANCE
Intervention in prekindergarten led to better mental health and academic performance 3 years later. Family-centered early intervention has the potential to prevent problems and reduce disparities for low-income minority children.
TRIAL REGISTRATION
clinicaltrials.gov Identifier: NCT01670227
Low-income minority children living in urban neighbor-hoods are at high risk for mental health problems and academic underachievement.1–4 Compelling evidence indicates that elimination of health disparities and the achievement gap requires meaningful engagement of families of children in the earliest years. Children’s brains are optimally programmed to benefit from high-quality experiences during early childhood. Accordingly, a strong early foundation provides the greatest potential for healthy development across domains.5
Substantial evidence indicates that nurturing relationships and predictable interactions with parents and other caregivers can buffer the effect of poverty-related stressors and adverse childhood experiences. Experimental prevention trials provide evidence in support of the causal role of parenting for a broad range of child outcomes.6 ParentCorps is a family-centered, school-based intervention that aims to help parents and teachers create safe, nurturing, and predictable environments for young children. It is delivered as an enhancement to prekindergarten (pre-K) in schools that serve large numbers of low-income children. Intervention includes professional development for pre-K and kindergarten teachers and a program offered to all families of pre-K students, implemented by mental health professionals and teachers during after-school hours. Previous cluster randomized clinical trials of ParentCorps found an effect on early childhood health and development.7–10 Expected changes occurred in the home and classroom environments based on parent and teacher report and observations by masked raters.10,11 The second trial evaluated the effect on kindergarten academic performance (ie, achievement test scores and teacher ratings), with effects observed across the full spectrum of baseline preacademic and self-regulation skills.8 For children with low self-regulation, additional intervention effects were detected on serious behavior problems at home (among boys),10 obesity,12 and health behaviors.12
This article reports results from the second trial on children’s mental health problems during a 3-year period. This study also evaluates whether the effect on kindergarten academic performance is maintained through second grade. We considered whether baseline self-regulation moderates intervention effects on mental health and academic performance. We hypothesized that relative to pre-K only, ParentCorps-enhanced pre-K would result in lower levels of mental health problems and higher academic performance. On the basis of previous findings, we expected that effects would be comparable or greater for children with low self-regulation and that family participation (ie, dose) would be associated with better outcomes.
Methods
Participants
Children entered pre-K and were enrolled in the trial at 4 years of age; this study followed up children at 5, 6, 7, and 8 years of age. The trial aimed to enroll all pre-K students in 4 consecutive years (September 12, 2005, through December 31, 2008); the only inclusion criterion was having an English-speaking caregiver (88 of 1280 children [6.9%] were ineligible). The major features of the design were reported earlier8,10 and are summarized herein. The published reports8,10 provide details on sample characteristics, indicate equivalent rates of study enrollment by condition and year, and suggest that randomization resulted in equivalent conditions with respect to baseline child, family, classroom, school, and neighborhood characteristics. Given evidence that schools require at least 1 year of capacity building for high-quality implementation,8,13 this study examines outcomes among children who were enrolled in pre-K after the first year of professional development and program implementation. All data were deidentified. The study was reviewed and approved by the Institutional Review Boards of the New York University School of Medicine and the New York City Department of Education. The study was introduced at pre-K orientation, and parents provided written informed consent. Data analysis for the follow-up study was performed from September 1, 2014, to December 31, 2015.
School Selection and Randomization
A cluster randomized clinical trial was conducted in 2 school districts in New York City. Schools were required to have a pre-K program with at least 2 classrooms (36 children) and a student population that was more than 80% black and more than 70% low income (ie, eligible for free lunch). Principals from the first 10 schools approached for the study agreed to participate; the trial schools are representative of all schools in the 2 districts (N = 34) with respect to demographics and state achievement test scores.8 To ensure approximately equal numbers of children in the 2 conditions, before randomization, schools were matched on size and split into pairs; within each pair, one school was randomized to the intervention group and the other to the control group. All 10 schools remained randomized to their groups throughout the study.
Intervention Conditions
All schools provided full-day or half-day pre-K for 4-year-olds and full-day kindergarten. In the intervention condition, schools received ParentCorps: (1) professional development for pre-K and kindergarten teachers, mental health professionals, and paraprofessionals and (2) programs for parents and pre-K students led by mental health professionals and teachers. The intervention aimed to help parents and teachers create safe, nurturing, and predictable environments at home and at school through the use of a specific set of evidence-based strategies, which in turn support children’s self-regulation skills. These foundational skills, along with continued use of evidence-based strategies by caregivers, are expected to promote mental health and school success.
Professional development included large-group experiential training (5 days in the first year; 2–3 days in subsequent years) and individual consultation (approximately 6 hours per year); pre-K teachers who chose to lead the program for students received additional training (2 days per year), coaching (1 hour per week for 13 weeks), and compensation for after-hours work.10
All families of pre-K students were invited to participate in 13 weekly 2-hour sessions for parents (Parenting Program; approximately 15 members) and concurrent sessions for children (Friends School) that were held at school, typically from 5 to 7 PM. During the Parenting Program, mental health professionals presented a specific set of strategies (eg, goal setting, attention during child-directed play, and helping children regulate emotions). Facilitators used a range of techniques (eg, role-play, discussion about video clips) to encourage participation, reflection, and consideration of cultural and contextual influences on parenting and child development. In Friends School, pre-K teachers used a consistent structure (eg, lessons, child-directed play) and a parallel set of strategies to promote self-regulation skills (eg, paying attention, identifying feelings).
Implementation of Intervention
All procedures were specified in manuals, and multimethod assessments indicated that fidelity was high (after capacity building, adherence was ≥90%10). Most families (257 of 423 [60.8%]) participated and, among participants, mean attendance was 7.30 of 13. The Parenting Program was engaging to parents from diverse backgrounds and those in greatest need of services as indicated by the lack of significant associations between participation and a broad range of baseline characteristics.10
Assessments and Definitions of Variables
Outcomes were teacher ratings of mental health problems and academic performance and achievement test scores. Teacher ratings of mental health were obtained on externalizing (ie, conduct problems, aggression, and hyperactivity) and internalizing (ie, anxiety, depression, and somatization) scales of the Behavior Assessment System for Children, Second Edition.14 Ratings were made at baseline and at the end of each year in pre-K through second grade (5 times with 4 teachers). Externalizing and internalizing scores were standardized based on age and sex and averaged to form an overall composite of mental health. Teachers also rated academic performance annually.8,15 Reading and math achievement were assessed twice—at the end of kindergarten and second grade—with the Kaufman Test of Educational Achievement (KTEA) Brief Form, Second Edition, by testers masked to condition.16 The Speed Developmental Indicators for the Assessment of Learning (DIAL) was administered in pre-K to provide a baseline indicator of preacademic skills.17 Self-regulation was assessed via masked observations during DIAL.
Statistical Analysis
Analyses assessed intervention-control differences on child-level outcomes and were based on the intention-to-treat principle (ie, all cases randomized at baseline were included in the analyses; multiple imputation was used to account for cases with missing data at follow-up). Effects were estimated with linear mixed-effects models using all available data.18 Post-intervention scores were modeled as a function of intervention, time, and the intervention × time interaction. Four post-intervention time points were available and analyzed for teacher-rated mental health problems and academic performance; 2 postintervention time points were available and analyzed for achievement tests. The intervention × time interaction was included in the model to assess whether change over time was different in the 2 conditions or conversely whether the magnitude of intervention-control difference varied with time. All analyses adjusted for the corresponding baseline indicator and cohort. The model accounted for between-subject (within school) correlation by including school-level random intercepts and slopes for time and within-subject (over time) correlation by including autocorrelated residual error terms. Statistical inference was based on 95% CIs; P values are reported only for interaction terms. Intervention effect sizes were interpreted by computing the Cohen d using model-based estimates of the parameters of interest (eg, intervention and control means) and SDs based on published norms or the mean across the 2 conditions at baseline.
To assess whether the intervention effect was the same across levels of baseline self-regulation, the model above was expanded to include the moderator (ie, self-regulation), moderator × intervention, moderator × time, and moderator × time × intervention interactions. As in previous reports,7,8 we considered children to have received full vs partial dose if parents participated in 5 or more sessions; 152 of 423 children (35.9%) received the full dose, and these families attended a mean of 10 sessions.10 We modeled postintervention outcomes as a function of dose (0, partial; 1, full; 2, control), time, and dose × time, adjusting for baseline and cohort as above.
A total of 409 of 792 children (51.6%) had complete data for all measures and times; 768 (97.0%) had baseline and at least 1 follow-up teacher rating, and 615 (77.7%) had at least 1 follow-up KTEA score. Teacher ratings were missing for 16 (2.0%), 111 (14.0%), 270 (34.1%), and 334 (42.2%) cases at follow-up from pre-K through second grade, respectively; the KTEA score was missing for 169 children (21.3%) in kindergarten and 348 (43.9%) in second grade. We used multiple imputations, assuming data were missing at random.19 The imputation made use of the joint distribution of all outcomes and the following demographic and baseline factors: cohort, school, sex, age, neighborhood poverty, DIAL screener, observed self-regulation, and teacher-rated adaptive behaviors. These factors were chosen because they are often associated with mental health, academic performance, and missingness. Using Markov chain Monte Carlo simulation, we minimally imputed the sample to achieve monotone missingness. We then sequentially imputed data for each wave using the predictive mean matching method separately for the intervention and control groups to account for the possibility of different missing data patterns by condition.20–22 Ten data sets were imputed. SAS statistical software (SAS Institute Inc) was used to perform the analysis.23
Results
Baseline Characteristics, Intervention Equivalence, and Participant Flow
The trial included 1050 children, representing 88.1% of eligible pre-K students, enrolled as 4 consecutive cohorts (518 boys [49.3%] and 532 girls [50.7%] in 99 pre-K classrooms). This follow-up study examines outcomes for the 3 cohorts that enrolled after the initial year of implementation (792 of 1050 children in the trial). Most families (421 [69.6%]) were low income; 680 (85.9%) identified as non-Latino black, 78 (9.8%) as Latino, and 34 (4.3%) as other. No differences were found between the conditions on any child or family demographic characteristic. Baseline testing of preacademic skills and masked observations of self-regulation were also comparable across condition; baseline differences were found in teacher ratings of mental health and performance (Table 1).
Table 1.
Baseline Characteristics of the Study Children and Families by Randomization Groupa
| Characteristic | Intervention (n = 5 Schools and 423 Children) |
Control (n = 5 Schools and 369 Children) |
|---|---|---|
| No. (%) of children | ||
| Male | 198 (46.8) | 179 (48.5) |
| Single parent | 158 (45.0) | 129 (43.4) |
| Parent unemployment | 130 (36.6) | 116 (39.3) |
| Low income | 236 (70.0) | 185 (69.0) |
| Parent educational level of high school diploma or lower | 174 (48.9) | 128 (43.6) |
| Black | 364 (86.1) | 316 (85.6) |
| Latino | 46 (10.9) | 32 (8.7) |
| Child school readiness at baseline, mean (SD) | ||
| Preacademic (test) | 98.18 (12.51) | 99.15 (13.34) |
| Self-regulation (observed) | 0.53 (0.55) | 0.46 (0.51) |
| Academic performance (teacher rated) | 64.37 (23.75) | 73.47 (18.83)b |
| Mental health problems (teacher rated) | 48.63 (7.73) | 44.74 (5.54)b |
Analyses of baseline equivalence adjusted for nesting of students within schools and used imputed data for child school readiness (n = 792); analyses used raw demographic data (the number of children ranged from 605 for income, to 651 for employment and education, and to 792 for sex and race).
P < .05.
The Figure shows the flow of the participants in the trial. Of the 792 students in this follow-up study, 78 (9.8%) were unavailable for follow-up (retention: 377 [89.1%] in the intervention group and 337 [91.3%] in the control group); 485 (61.2%) remained in study schools and had complete outcome data through second grade (254 [60.0%] in the intervention group and 231 [62.6%] in the control group). Children with data in second grade did not differ from those without data on demographic characteristics, baseline teacher ratings, or school readiness (P > .05).
Figure. Enrollment, Randomization, and Follow-up of Schools and Students.
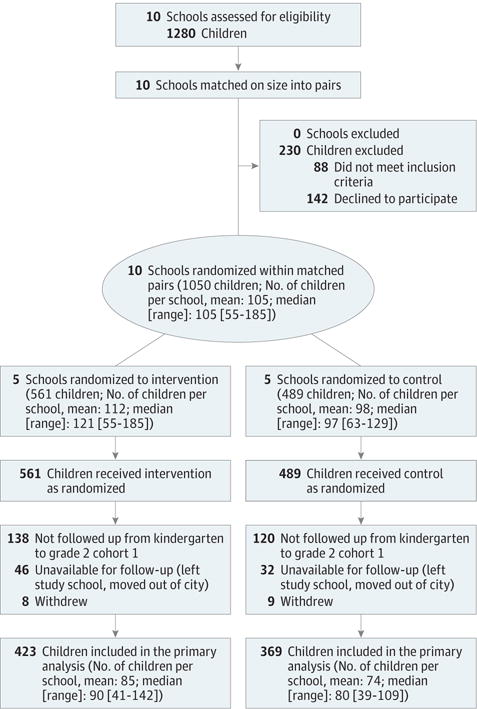
Primary analysis included all 792 children enrolled in cohorts 2 to 4 (intervention, 423; control, 369), including cases that withdrew or were unavailable for follow-up.
Mental Health Problems
The intervention × time interactions were significant, indicating that the magnitude of the effect on mental health increased over time (P = .003) (Table 2). From 5 to 8 years of age, problems increased substantially for children in control schools (5.64 points [or 0.56 SD] on a norm-referenced scale); in contrast, among intervention school children, problems remained relatively stable (decreased 0.99 points [−0.10 SD]). These diverging trajectories resulted in children in control schools having higher levels of mental health problems than those in intervention schools at 8 years of age (d = 0.44; 95% CI, 0.08–0.81). Post hoc examination of the 2 measures in the mental health composite revealed similar patterns, with substantial differences at 8 years of age on each domain (behavioral d = 0.36; emotional d = 0.42). The investigation of whether baseline self-regulation moderated the intervention effect revealed no evidence of moderation (intervention × time × self-regulation interaction: estimated = −0.36; 95% CI, −1.18 to 0.46; P = .38; intervention × self-regulation: estimated =−2.27; 95% CI, −7.66 to 3.12; P = .40). Overall, there was no dose-response relationship. However, among the subgroup of high-risk children (ie, low self-regulation), there was a 2-fold difference in the effect on mental health for children exposed to full dose vs partial dose (d = 0.81 vs 0.40).
Table 2.
Intervention Effect on Mental Health Problems and Academic Achievementa
| Effect | Estimate (95% CI) | |
|---|---|---|
| Mental Health Problems | Academic Performance | |
| Baseline measure of outcome | 0.73 (0.68 to 0.78) |
0.71 (0.66 to 0.76) |
| Time | 1.88 (0.85 to 2.92) |
−3.44 (−4.58 to −2.30) |
| Intervention | −4.42 (−8.09 to −0.75) |
5.99 (1.27 to 10.71) |
| Intervention × time | −2.21 (−3.67 to −0.75) |
1.17 (−0.49 to 2.84) |
| Condition (time) | ||
| Intervention | −0.33 (−1.36 to −0.70) |
−2.26 (−3.40 to −1.13) |
| Control | 1.88 (0.85 to 2.92) |
−3.44 (−4.58 to −2.30) |
| Cohen d for intervention-control difference in second grade, SD | 0.44 (0.08 to 0.81) |
0.21 (0.02 to 0.39) |
Four postintervention time points were included: spring of prekindergarten (time = −3), spring of kindergarten (time = −2), spring of first grade (time = −1), and spring of second grade (time = 0). All analyses controlled for cohort (ie, year of implementation). The estimate for intervention reflects the intervention-control difference in mean outcome in the spring of second grade (adjusting for baseline). The estimate for the intervention × time interaction indicates whether the magnitude of the intervention-control difference varies with time or, conversely, whether the change over time is different for the intervention vs control conditions.
Academic Performance
The intervention effect was significant, whereas the intervention × time interaction was not, suggesting that the magnitude of the effect on teacher-rated academic performance was maintained over time (P = .17) (Table 2). Although performance decreased in both conditions from 5 to 8 years of age, children in intervention schools performed higher than controls consistently over time (d = 0.21; 95% CI, 0.02–0.39). Similarly, for achievement tests, the intervention × time interaction was not significant (reading: estimated = −4.18; 95% CI, −10.30 to 1.95; P = .18; math: estimated = −2.44; 95% CI, −6.02 to 1.14; P = .18), suggesting that the effect on kindergarten achievement reported previously8 did not deteriorate substantially by second grade. On the basis of a reduced model (excluding the nonsignificant interaction term), reading test scores were marginally higher for children in intervention schools relative to controls (d = 0.32; 95% CI, −0.06 to 0.70); there was no discernible benefit for math achievement (d = 0.10; 95% CI, −0.03 to 0.23). There were no significant 2-way or 3-way interaction effects for any outcome (P > .10). For all 3 academic outcomes, the intervention effect was 1.5 to 3 times greater for children with full vs partial dose (performance: d = 0.26 vs 0.17; reading: d = 0.46 vs 0.24; math: d = 0.18 vs 0.06).
Discussion
This follow-up study examined intervention-control differences on mental health and academic performance through 8 years of age. In early childhood, intervention improved academic performance (teacher ratings and achievement tests) for all children and behavior problems among the highest-risk boys.8,10 At the 3-year follow-up, an effect was detectable for mental health (behavioral and emotional problems) and academic performance across baseline levels of risk (child self-regulation). For children enrolled in pre-K in control schools, mental health problems observable by teachers increased substantially (more than one-half SD) during the early school years. This pattern is consistent with the well-described accumulation of stressors and cascading negative consequences for health and development among children living in poverty.5 In sharp contrast, children in pre-K programs with ParentCorps had no increase in mental health problems over time. These different trajectories resulted in clinically meaningful differences by second grade (eg, controls were nearly twice as likely as children in intervention schools to score in the clinical range on a norm-referenced teacher rating scale). Of importance, because ParentCorps was delivered as an enhancement to pre-K, effects are over and above the benefits of pre-K (estimated to be one-third SD if high quality).24,25 Finally, the intervention effect can be compared with well-established gaps in outcomes for low-income minority children. For example, the effect of ParentCorps on academic performance is approximately half that of the black-white achievement gap (one-half SD).26,27
The intervention-control differences on mental health and academic performance remained across baseline levels of self-regulation observed during pre-K. In high-poverty urban schools, an estimated one-quarter of children enter school without adequate self-regulation.10,28,29 Although self-regulation facilitates on-task behavior and optimal management of attention, motivation, and stress reactivity while learning,30–32 children without these skills are much more likely to have negative interactions with teachers and peers and ultimately to develop emotional or behavioral problems that interfere with learning.33,34 ParentCorps’ focus on helping teachers and parents create safe, nurturing, and predictable environments is expected to soothe children’s physiologic stress response and allow for the acquisition of executive functioning skills.32 Although this study did not directly measure stress response, the plausibility of this mechanism is supported by the prior demonstration by Brotman et al35,36 that family-centered early intervention with low-income black and Latino families altered cortisol levels and prosocial and disruptive peer interactions.
Developmental theory provides a rationale for the expectation that a relatively brief intervention in early childhood could result in meaningful and sustained benefits for mental health and academic domains, especially among those at highest risk for problems.37,38 First, although no single factor predicting later outcomes has a large effect size, the accumulation of small effects over time can be great. Therefore, small increases in self-regulation and early learning can lead to large differences in mental health and academic performance. Second, there is a primacy of early influences such that they trigger cascades that become larger effects over time. Third, the development of mental health and school success is characterized by transactional influences across several domains. Therefore, by altering parent and teacher behaviors, self-regulation, and early learning, intervention yields broad and long-lasting effects.
Several limitations of the study deserve consideration. First, the trial included a relatively small number of schools, which decreases power (effective number of participants is decreased because of clustering within a school). Second, although there was no evidence that children who left study schools were different from those who remained, they may have differed on unmeasured characteristics. Third, despite randomization, the conditions differed with respect to baseline teacher ratings, which makes comparison between conditions more difficult. We note that alternative analyses (mixed-effects models applied to baseline score as an outcome rather than including baseline as a covariate) resulted in highly similar inferences about intervention-control differences over time. Fourth, it is possible that teacher ratings were biased. Inter vention may have sensitized teachers such that they perceived children differently than their colleagues in control schools. However, second grade teachers were not involved in the intervention and were unaware of families’ level of participation during pre-K, and the intervention-control difference in academic performance (as rated by pre-K through second grade) was consistent with the favorable pattern observed for the objective reading achievement tests (kindergarten and second grade). Fifth, although careful examination of family participation revealed that a broad range of factors was not associated with dose (eg, parental depression, ethnicity, and child school readiness),10 unmeasured characteristics may be.
As ParentCorps is implemented independently by school districts in New York City and other urban centers, it will be important to determine whether it can be implemented with fidelity and whether effects on mental health and academic performance are replicated for diverse populations. Further study of mechanisms underlying change will be critical to advance developmental and intervention theory and for continuous program improvements.
Conclusions
Children in schools with ParentCorps had more positive trajectories for mental health and academic performance. Findings suggest that family-centered intervention during pre-K has the potential to mitigate the effect of poverty-related stressors on healthy development and thereby reduce racial and socioeconomic disparities.
Key Points.
Question
Does ParentCorps delivered as an enhancement to prekindergarten programs in high-poverty, urban schools lead to fewer mental health problems and increased academic performance in the early elementary school years?
Findings
In this follow-up of a randomized clinical trial, relative to their peers in prekindergarten programs, children in ParentCorps-enhanced prekindergarten programs had significantly lower levels of teacher-rated mental health problems and higher academic performance in second grade.
Meaning
Family-centered early intervention has the potential to promote mental health and academic performance and reduce disparities for low-income minority children.
Acknowledgments
Funding/Support: This study was funded by grants R305F050245 and R305A100596 from the US Department of Education, Institute of Education Sciences, and grant 1R01MH077331-01 from the National Institute of Mental Health (Dr Brotman).
Role of the Funder/Sponsor: The US Department of Education, Institute for Education Sciences, and National Institute of Mental Health funded the design and conduct of the study; collection, management, analysis, and interpretation of the data; and preparation of the manuscript. They had no role in the decision to submit the manuscript for publication.
Footnotes
Correction: This article was corrected on November 7, 2016, to fix the Funding/Support section.
Author Contributions: Dr Brotman had full access to all the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis.
Study concept and design: Brotman, Dawson-McClure, Kamboukos, Calzada, Petkova.
Acquisition, analysis, or interpretation of data: Brotman, Dawson-McClure, Kamboukos, Huang, Goldfeld, Petkova.
Drafting of the manuscript: Brotman, Dawson-McClure, Huang, Petkova.
Critical revision of the manuscript for important intellectual content: All authors.
Statistical analysis: Huang, Petkova.
Obtained funding: Brotman, Dawson-McClure, Huang, Calzada.
Administrative, technical, or material support: Brotman, Dawson-McClure, Kamboukos, Calzada.
Study supervision: Brotman, Dawson-McClure, Kamboukos.
Conflict of Interest Disclosures: Payments for the purchase of ParentCorps materials, training, and technical assistance are made to the Department of Population Health at the New York University Langone Medical Center to cover costs for materials and faculty and staff salaries associated with training and technical assistance. Any revenue generated from sales and training support further development of ParentCorps. No other disclosures were reported.
References
- 1.Cataldi EF, Laird J, Kewalramani A. High school dropout and completion rates in the United States: 2007 (NCES 2009064) http://nces.ed.gov/pubs2009/2009064.pdfPublished 2009. Accessed December 17, 2015.
- 2.Freedman DS, Srinivasan SR, Harsha DW, Webber LS, Berenson GS. Relation of body fat patterning to lipid and lipoprotein concentrations in children and adolescents: the Bogalusa Heart Study. Am J Clin Nutr. 1989;50(5):930–939. doi: 10.1093/ajcn/50.5.930. [DOI] [PubMed] [Google Scholar]
- 3.Muntner P, He J, Cutler JA, Wildman RP, Whelton PK. Trends in blood pressure among children and adolescents. JAMA. 2004;291(17):2107–2113. doi: 10.1001/jama.291.17.2107. [DOI] [PubMed] [Google Scholar]
- 4.Ogden CL, Carroll MD, Curtin LR, Lamb MM, Flegal KM. Prevalence of high body mass index in US children and adolescents, 2007–2008. JAMA. 2010;303(3):242–249. doi: 10.1001/jama.2009.2012. [DOI] [PubMed] [Google Scholar]
- 5.National Scientific Council on the Developing Child. Establishing a level foundation for life: mental health begins in childhood: working paper 6. http://www.developingchild.harvard.edu Published 2012. Accessed December 12, 2015.
- 6.Sandler IN, Schoenfelder EN, Wolchik SA, MacKinnon DP. Long-term impact of prevention programs to promote effective parenting: lasting effects but uncertain processes. Annu Rev Psychol. 2011;62:299–329. doi: 10.1146/annurev.psych.121208.131619. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Brotman LM, Calzada E, Huang KY, et al. Promoting effective parenting practices and preventing child behavior problems in school among ethnically diverse families from underserved, urban communities. Child Dev. 2011;82(1):258–276. doi: 10.1111/j.1467-8624.2010.01554.x. [DOI] [PubMed] [Google Scholar]
- 8.Brotman LM, Dawson-McClure S, Calzada EJ, et al. Cluster (school) RCT of ParentCorps: impact on kindergarten academic achievement. Pediatrics. 2013;131(5):e1521–e1529. doi: 10.1542/peds.2012-2632. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Brotman LM, Kingston S, Bat-Chava Y, Calzada EJ, Caldwell M. Training school personnel to facilitate a family intervention to prevent conduct problems. Early Educ Dev. 2008;19(4):622–642. [Google Scholar]
- 10.Dawson-McClure S, Calzada E, Huang KY, et al. A population-level approach to promoting healthy child development and school success in low-income, urban neighborhoods: impact on parenting and child conduct problems. Prev Sci. 2015;16(2):279–290. doi: 10.1007/s11121-014-0473-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Dawson-McClure S, Calzada EJ, Huang KY, Kamboukos D, Brotman LM. Promoting High Quality Early Childhood Classroom Environments and Family Engagement Through Culturally-Informed Preventive Intervention for Children Living in Low-Income, Urban Communities. Washington, DC: Society for Prevention Research; 2011. [Google Scholar]
- 12.Brotman LM, Dawson-McClure S, Huang KY, et al. Early childhood family intervention and long-term obesity prevention among high-risk minority youth. Pediatrics. 2012;129(3):e621–e628. doi: 10.1542/peds.2011-1568. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Borman G, Hewws G, Brown S. Comprehensive school reform and achievement: a meta-analysis. Rev Educ. 2003;73(2):125–130. doi: 10.3102/00346543073002125. [DOI] [Google Scholar]
- 14.Reynolds CR, Kamphaus RW. Behavior Assessment System for Children - 2. Minneapolis, MN: Pearson Inc; 2004. [Google Scholar]
- 15.Miller LS, Klein RG, Piacentini J, et al. The New York Teacher Rating Scale for disruptive and antisocial behavior. J Am Acad Child Adolesc Psychiatry. 1995;34(3):359–370. doi: 10.1097/00004583-199503000-00022. [DOI] [PubMed] [Google Scholar]
- 16.Kaufman AS, Kaufman NL. Kaufman Test of Educational Achievement. 2nd. Circle Pines, MN: AGS Publishing; 2005. [Google Scholar]
- 17.Mardell-Czudnowski C, Goldenberg D. Developmental Indicators for the Assessment of Learning - 3. Monterey, CA: AGS Publishing; 1998. [Google Scholar]
- 18.Diggle PJ, Heagerty P, Liang KY, Zeger SL. Analysis of Longitudinal Data. New York, NY: Oxford University Press; 2005. [Google Scholar]
- 19.Schafer JL, Graham JW. Missing data: our view of the state of the art. Psychol Methods. 2002;7(2):147–177. [PubMed] [Google Scholar]
- 20.Schenker N, Taylor JMG. Partially parametric techniques for multiple imputation. Comput Stat Data Anal. 1996;22(4):425–446. [Google Scholar]
- 21.Heitjan DF, Roderick JAL. Multiple imputation for the fatal accident reporting system. J R Stat Soc Ser C. 1991;40(1):13–29. [Google Scholar]
- 22.Little R, Rubin D. Statistical Analysis With Missing Data. New York, NY: John Wiley & Sons Inc; 2002. [Google Scholar]
- 23.SAS (R) 9 [computer program] Cary, NC: SAS Institute Inc; 2009. [Google Scholar]
- 24.Frede EC, Jung K, Barnett WS, Figueras A. The APPLES Blossom: Abbott Preschool Program Longitudinal Effects Study (APPLES), Preliminary Results Through 2nd Grade. New Brunswick: National Institute for Early Education Research, Graduate School of Education, Rutgers, the State University of New Jersey; 2009. [Google Scholar]
- 25.Yoshikawa H, Weiland C, Brooks-Gunn J, et al. Investing in our future: the evidence base on preschool education. 2013 http://fcd-us.org/resources/evidence-base-preschool Accessed December 17, 2015.
- 26.Konstantopoulos S, Hedges L. How large an effect can we expect from school reforms? Teach Coll Rec. 2008;110(8):1611–1638. [Google Scholar]
- 27.Chatterji M. Reading achievement gaps, correlates and moderators of early reading achievement: evidence from the Early Childhood Longitudinal Study (ECLS) Kindergarten to First Grade sample. J Educ Psychol. 2006;98(3):489–507. [Google Scholar]
- 28.Iruka IU, Gardner-Neblett N, Matthews JS, Donna-Marie C. Preschool to kindergarten transition patterns for African American boys. Early Child Res Q. 2014;29(2):106–117. [Google Scholar]
- 29.Raver CC, Morris P. Invited Symposium I; integrating prevention science, policy and practices to support high-quality universal pre-K. Paper presented at: Society for Prevention Research; May 27, 2015; Washington, DC. [Google Scholar]
- 30.Rhoades B, Warren H, Domitrovich C, Greenberg M. Examining the link between preschool social-emotional competence and first grade achievement: the role of attention skills. Early Child Res Q. 2011;26(2):182–191. [Google Scholar]
- 31.Izard C, Fine S, Schultz D, Mostow A, Ackerman B, Youngstrom E. Emotion knowledge as a predictor of social behavior and academic competence in children at risk. Psychol Sci. 2001;12(1):18–23. doi: 10.1111/1467-9280.00304. [DOI] [PubMed] [Google Scholar]
- 32.Ursache A, Blair C, Raver C. The promotion of self-regulation as a means of enhancing school readiness and early achievement in children at risk for school failure. Child Dev Perspect. 2012;6(2):122–128. doi: 10.1111/j.1750-8606.2011.00209.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Arnold DH, Ortiz C, Curry JC, et al. Promoting academic success and preventing disruptive behavior disorders through community partnership. J Community Psychol. 1999;27(5):589–598. [Google Scholar]
- 34.McEvoy A, Welker R. Antisocial behavior, academic failure, and school climate: a critical review. J Emot Behav Disord. 2000;8(3):130–140. [Google Scholar]
- 35.Brotman LM, Gouley KK, Chesir-Teran D, Dennis T, Klein RG, Shrout P. Prevention for preschoolers at high risk for conduct problems: immediate outcomes on parenting practices and child social competence. J Clin Child Adolesc Psychol. 2005;34(4):724–734. doi: 10.1207/s15374424jccp3404_14. [DOI] [PubMed] [Google Scholar]
- 36.Brotman LM, Gouley KK, Huang KY, Kamboukos D, Fratto C, Pine DS. Effects of a psychosocial family-based preventive intervention on cortisol response to a social challenge in preschoolers at high risk for antisocial behavior. Arch Gen Psychiatry. 2007;64(10):1172–1179. doi: 10.1001/archpsyc.64.10.1172. [DOI] [PubMed] [Google Scholar]
- 37.Masten AS, Roisman GI, Long JD, et al. Developmental cascades: linking academic achievement and externalizing and internalizing symptoms over 20 years. Dev Psychol. 2005;41(5):733–746. doi: 10.1037/0012-1649.41.5.733. [DOI] [PubMed] [Google Scholar]
- 38.McClain DB, Wolchik SA, Winslow E, Tein J-Y, Sandler IN, Millsap RE. Developmental cascade effects of the New Beginnings Program on adolescent adaptation outcomes. Dev Psychopathol. 2010;22(4):771–784. doi: 10.1017/S0954579410000453. [DOI] [PMC free article] [PubMed] [Google Scholar]