

Abstract
Research on mindfulness interventions with adolescents has burgeoned over the last ten years, and findings have demonstrated increases in overall emotional wellbeing post-intervention. However, little is known about the differences between males and females in response to mindfulness interventions in this age group. In the present study we examine sex differences in outcomes of physiological stress markers during the Trier Social Stress Test (TSST) and emotional wellbeing measures before and after a mindfulness intervention (N = 15) with 10 female and 5 male adolescents. Additionally, we examine sex differences in course engagement and post-intervention use of mindfulness skills during the TSST. Overall, we found some evidence that females were more engaged than males in the class and also reported less stress post-intervention. We conclude by strongly encouraging future research in this area to more clearly elucidate the different ways in which adolescent males and females engage and respond to mindfulness interventions.
Introduction
Over the last ten years, research on mindfulness with adolescents has been burgeoning. Defined as being intentionally aware and non-judgmental toward one’s momentary experiences (Kabat-Zinn, 1994), mindfulness has been studied in adolescent populations through exploring associations between mindfulness and wellbeing, as well as investigating interventions in which training in mindfulness skills has been the primary focus. The first randomized clinical trial with adolescents reported decreases in psychological symptoms in a clinical sample of adolescents after a mindfulness training program (Biegel, Brown, Shapiro, & Schubert, 2009). The first review of mindfulness-based interventions (MBIs) with youth followed thereafter (Burke, 2010); this initial review of fifteen studies indicated that most of the mindfulness intervention studies with youth and adolescents thus far were feasibility studies, concluding that mindfulness interventions were feasible for this population. Burke (2010) proposed that research in the field move beyond feasibility studies and called for more robust research, specifically, large scale RCTs with active control groups.
Over the last five years, research in the field has continued to grow; two meta-analyses on MBIs with youth measured outcomes of general mindfulness interventions (Zoogman, Goldberg, Hoyt, & Miller, 2014) and school-based interventions (Zenner, Herrnleben-Kurz, & Walach, 2014). The former concluded that mindfulness interventions were advantageous over active controls, and larger effect sizes were evident in clinical samples and in psychological outcomes, such as depression and anxiety (Zoogman et al., 2014). The latter meta-analysis reported the largest effect sizes on outcomes such as stress, resilience and cognitive performance. In general, these recent meta-analyses echo results of meta-analyses of mindfulness interventions with adults, which also report small to medium effect sizes and positive outcomes for psychological symptoms (De Vibe, Bjørndal, Tipton, Hammerstrøm, & Kowalski, 2012; Khoury et al., 2013).
Despite this growth in research and findings indicating that MBIs are effective for adolescents, there has been no research which has investigated differential effects of MBIs for female and male adolescents. As males and females mature at different times and at different rates during adolescence, it is important that interventions are tailored to meet the emotional needs of both sexes. For example, as males mature later than females, a 13 year old boy would likely have a less developed emotional and cognitive repertoire than a 13 year old female. Further, as males and females are socialized to behave differently in learning environments (Eccles & Blumenfeld, 1985; Jones & Wheatley, 1990), they might benefit from different classroom techniques in learning mindfulness.
Mindfulness interventions created specifically for adolescents have recently emerged and have received some empirical scrutiny. One such mindfulness program is Learning to BREATHE (L2B; Broderick, 2013). L2B uses developmentally-appropriate activities and meditations to teach mindfulness skills and was adapted from the most empirically tested adult mindfulness program, Mindfulness-Based Stress Reduction, an 8-week program in which participants meet weekly to learn and practice mindfulness skills (Kabat-Zinn, 1990). Extensive research on MBSR has demonstrated positive physical and mental health outcomes in a multitude of domains (De Vibe et al., 2012; Goyal et al., 2014; Greeson, 2009; Hofmann, Sawyer, Witt, & Oh, 2010; Khoury et al., 2013), and research on L2B is beginning to show similar effects such as decreases in perceived stress, psychosomatic complaints, depression, and negative affect (Bluth, Campo, et al., 2015; Broderick & Metz, 2009; Metz et al., 2013). Although the format in which L2B is taught is flexible, L2B is generally offered to adolescents in a six session format in which adolescents meet weekly for one hour.
Although there is no conclusive evidence as to how much engagement (i.e., attendance, home practice) in a mindfulness course is needed to increase mindfulness, and thereby improve wellbeing outcomes, initial findings on mindfulness interventions with adolescents indicate that greater home practice is related to improvements in wellbeing (Britton et al., 2010; Huppert & Johnson, 2010). In studies with adolescents in other interventions (e.g., suicide prevention program), this has also been found to be the case (Hamilton & Klimes-Dougan, 2015). In adults, greater engagement in mindfulness training has been linked to improved outcomes in some studies (Carmody & Baer, 2008 De Vibe et al., 2013; Snippe, Nyklíček, Schroevers, & Bos, 2015; Speca, Carlson, Goodey, & Angen, 2000), although other studies report mixed results (Carlson, Speca, Patel, & Goodey, 2003; Davidson et al., 2003; Jain et al., 2007).
Despite the recent attention on the positive findings of mindfulness interventions, there has been limited research on the differential effect of sex on either engagement in MBIs or on outcomes of MBIs in adults and no research with adolescents. In one modified (7-week) MBSR course, female medical students reported significantly greater decreases in stress, mental distress, and subjective wellbeing compared to male medical students over the course of the intervention (De Vibe et al., 2013). Mental distress in men decreased from pre- to post- intervention, but did not reach statistical significance. Further, the facets of the mindfulness scale “non-reactivity” and “non-judging” changed significantly pre to post for females but not for males, suggesting that exploring these facets in future research may provide clarity as to that which is responsible for the differential change in outcomes between males and females. Authors posited that practicing mindfulness skills may have helped women handle their distress, but may have helped men become more aware of their level of distress, and suggested that men may need different types of mindfulness training.
In a review on MBIs for substance use disorders (Katz & Toner, 2012), findings indicated some sex differences in response to the interventions. For example, there was some evidence that women tended to “gravitate” more to the training than did men, and there was some indication of greater effectiveness for women. Findings from physiological data appeared to confirm these observations; changes in the hippocampi of women meditators differed from that of men in magnitude, laterality, and location on the hippocampus surface (Luders, Toga, Lepore, & Gaser, 2009). In relation to hypothalamus-pituitary-adrenal (HPA) axis activity (i.e., cortisol levels) during a conflict discussion task with young couples, Laurent et al. (2013) observed that women may benefit more from mindfulness interventions than men, although indicated that more research is needed to confirm this finding. Like Katz and Toner, they also suggest that the pathway through which mindfulness promotes wellbeing may be different for men than for women. Further, they suggest that it may be that the type of stressor that matters, in that mindfulness may be more beneficial in relation to interpersonal stressors rather than performance stressors, and for this reason, may be more relevant for women than men (Stroud, Salovey, & Epel, 2002). If this is the case, it would be expected that these sex differences in response to mindfulness interventions would emerge in adolescence (Laurent et al., 2013).
Further, there is a lacuna of research which investigates mechanisms of change in adolescent mindfulness interventions, although relationships between potential mediators and outcomes have been explored cross-sectionally in one study (Bluth & Blanton, 2014). This study posits that mindfulness and self-compassion, although distinct constructs, may interact to facilitate the development of each other and then promote positive emotional wellbeing. Self-compassion, defined as treating yourself with the same kindness and care as you would a good friend who was experiencing difficulty (Neff, 2003b), has been associated with positive mental health in numerous studies with adults (Neff & Dahm, 2014), and a meta-analysis reported large inverse associations between self-compassion and psychopathology (MacBeth & Gumley, 2012) and moderately large correlations between self-compassion and wellbeing (Zessin, Dickhäuser, & Garbade, 2015). Mindfulness training implicitly supports the development of self-compassion, and at least one practice taught in most MBIs involves cultivation of kindness towards oneself (Kabat-Zinn, 1990). Thus, it would be expected that a mindfulness intervention would result in increasing both mindfulness and self-compassion, which would then initiate a positive change in wellbeing. In fact, Baer et al. (2012) determined that change in mindfulness precedes change in perceived stress, and Snippe et al. (2015) reported that changes in mindfulness precede changes in positive and negative affect.
As males and females not only mature at different rates but have different developmental trajectories, and this is particularly evident during the adolescent period (Steinberg & Morris, 2001), it would not be surprising if specific mindfulness activities appeal to male and female adolescents differently and that these mindfulness activities were more or less effective depending on biological sex. Furthermore, sex differences and the use of mindfulness skills during stressful situations after mindfulness training have not been studied in adolescent populations. As mindfulness research with adolescents has conflated data from males and females, any sex-nuanced findings may inform and improve future interventions and research as MBIs can be tailored to the specific needs of male and female adolescents.
Therefore, the purpose of this study is to explore whether there are differences in the way in which male and female adolescents engage with and respond to a mindfulness intervention. Due to the small sample size, these questions are exploratory, with the aim of determining whether further study of between-sex differences should be conducted. Specifically, our research questions explore 1) whether there is a difference in degree of engagement of male and female adolescents to a mindfulness intervention, 2) whether there is a difference in the effectiveness of a mindfulness intervention on male and female adolescents as measured by dimensions of self-reported wellbeing and physiological stress markers in response to a stress test, and 3) if males and females reported using different stress-reducing techniques during a laboratory stress test.
Method
Participants
Upon university IRB approval, we recruited participants through flyers in the community and university listservs. To be eligible, participants had to be between age 13 and 18, read and understand English, and score below 10 on the Kutcher Adolescent Depression Scale (KADS; LeBlanc, Almudevar, Brooks, & Kutcher, 2002). Further, adolescents were excluded if they endorsed an item on the scale indicating that they had thoughts of self-injury or suicide. In total, three adolescents were excluded because they scored above 10 on the KADS. The study psychologist contacted the parents of these adolescents to inform them of their score and the reasons for their exclusion in the study. The present study includes a subset of participants who were randomly assigned to the mindfulness intervention (N = 15; female n = 10; male n = 5). The group randomized to the healthy lifestyles control condition, which involved education on adolescent topics including sleep, exercise, nutrition, and peer relationships, was comprised initially of 10 females and 1 male. However, the male withdrew from the control group prior to completing the study. Given that the focus of the present study is to examine differences between male and female responses to the mindfulness intervention, the control group is not included in the present report. Participants randomized to the mindfulness group were 62% female; 33% of participants were age 13–14, 53% were age 15–16, and 13% were age 17–18; 19% were Black/African American, 75% were White, and 6% were Asian. Eighty percent of participants’ mothers and 87% of participants’ fathers had at least a college degree, and 20% of participants’ mothers and 13% of participants’ fathers had a doctorate or professional degree.
Procedure
Participants were told that they would attend a 6-week course that would help them contend with teenage stress. Prior to the course, participants attended a laboratory session in which their physiological stress response (i.e., blood pressure, heart rate, heart rate variability, cortisol) to the Trier Social Stress Test (TSST) was monitored. The TSST (Kirschbaum, Pirke, & Hellhammer, 1993; Martel et al., 1999; Rao, Hammen, Ortiz, Chen, & Poland, 2008) is an empirically-based, social evaluative lab social stressor which has demonstrated activation of the physiological stress response (i.e., hypothalamus-pituitary-adrenal axis [HPA] and autonomic nervous system [ANS]). Findings of previous studies indicate that those higher in trait mindfulness exhibit a lower cortisol response (Brown, Weinstein, & Creswell, 2012), and participants demonstrate less emotional reactivity (Britton, Shahar, Szepsenwol, & Jacobs, 2012) and less anxiety and distress (Hoge et al., 2013) post-mindfulness course.
Blood pressure (BP) and heart rate (HR) were taken seven times during the initial 20 minute pre-stress rest period (at minutes 0, 3, 5, 8, 14, 17, and 19) and heart rate variability (HRV) was monitored continuously for two 5-min intervals during the last 10 minutes of the 20 minute pre-stress rest period. Immediately following this rest period, participants provided a resting saliva sample for cortisol testing and completed the Spielberger State Anxiety Scale (SSAI; Spielberger, Gorsuch, Lushene, Vagg, & Jacobs, 1983). Next, participants were exposed to the TSST tasks. The TSST employed in the present study was modified for adolescents and required the participant to silently prepare (5 minutes) to give a speech about their ideal summer job (5 minutes) in front of a two person committee who responded with prepared questions if the participant stopped talking. This was immediately followed by a serial subtraction task requiring the participant to serially subtract seven starting from 2023 (5 minutes). The committee required the participant to restart at 2023 with each incorrect response. Blood pressure and HR were measured three times during each of the preparation, speech and serial subtraction tasks at 0, 2, and 4 minutes, and averaged to constitute mean task levels, and HRV was measured continuously for the entire 5-min preparation period. Participants provided a saliva sample and a state anxiety measure was completed again immediately after the TSST tasks. A 20-minute post-stress rest period followed in which HR and BP were measured seven times at minutes 0, 3, 5, 8, 14, 17, and 19, and averaged, and HRV was assessed continuously over two separate 5-minute intervals. Saliva samples were also provided two more times during the post-stress rest period at 10 minutes post-TSST tasks and 20 minutes post-TSST tasks. Further details for the measures and protocol for the laboratory session are reported elsewhere (Bluth, Roberson, et al., 2015).
During the test, blood pressure and heart rate were assessed via the Suntech Exercise BP monitor, Model 4240 (SunTech Medical Instruments, Inc., Raleigh, NC) which provided automated measurement of BP and HR during the session. Cortisol was assessed via saliva samples collected by passive drool, and heart rate variability was assessed using EKG data which was then exported into CardioEdit software (Brain–BodyCenter, University of Illinois at Chicago), which uses the Porges method (Porges, 1985) to obtain respiratory sinus arrhythmia (RSA), a measure of parasympathetic nervous system activity.
After the first laboratory session and three days prior to the beginning of the intervention, participants were emailed a link to an online survey comprised of the subjective measures. All surveys were completed prior to the first class. Upon completion of the intervention, participants were sent a second online survey, and then attended a second laboratory session which was identical to the first with the exception that they were given a different topic to speak about during the speech task of the TSST. Additionally, participants completed a post-lab questionnaire during this second lab which asked how this second lab experience was different than the first, and what stress techniques were used, if any, during the lab.
Adolescents were fully debriefed about the purpose of the TSST procedure following the second laboratory session. Participants were compensated $30 for completion of the initial baseline laboratory assessment and online survey, an additional $30 after the third class, and a final $40 after completion of the post-intervention laboratory assessment (see Figure 1 for study time frame).
Figure 1.
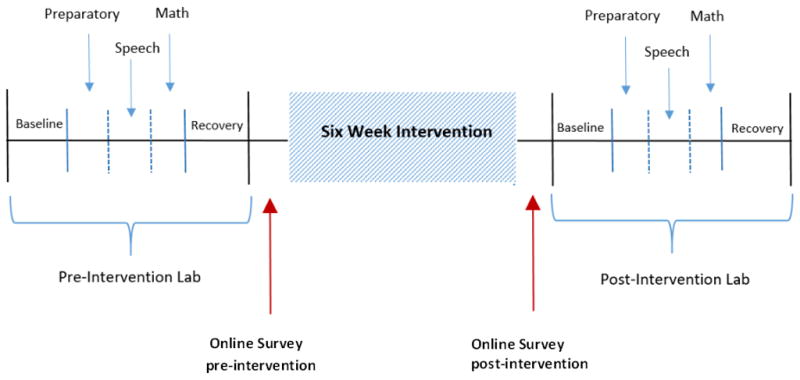
Study time frame
Intervention
Learning to BREATHE (L2B; Broderick, 2013) is a 6-week mindfulness course in which participants met for 1.5 hours weekly. L2B is adapted for adolescents from Mindfulness-Based Stress Reduction (MBSR), an 8-week mindfulness training course that has been empirically studied and validated (De Vibe et al., 2012; Greeson, 2009; Khoury et al., 2013). Similar to the adult MBSR program, guided mindful breathing, mindful movement, body scan, and mindful listening are included and practiced throughout the 6 weeks of classes. However, L2B differs from the adult program in that it incorporates developmentally-appropriate activities for adolescents. For example, meditations are shorter and adolescents learn through being actively engaged in lessons rather than the instructor explaining the outcomes of mindfulness practice (for a more detailed description of the intervention see Broderick, 2013). Complementing the weekly sessions, participants are given home practice assignments and encouraged to practice the mindfulness skills that learn in class that week. All classes were audiorecorded and transcribed. The instructor of this course was a long-time mindfulness practitioner (35+ years), former middle school classroom teacher, MBSR instructor, and had been teaching L2B for three years.
Measures
Course engagement
To assess how engaged participants were in the course, we used three markers of engagement: percent attendance over the 6 classes (# classes attended/# total classes), home practice completion (total # days homework was completed; students kept track on a daily basis of the practices they did each day at home and then at the beginning of each weekly class completed a form indicating the number of days that they practiced that week; an overall mean was computed for the 5 weeks that homework was assigned), and total content utterances (# of times adolescent spoke in class about the present class topic; this was counted from the transcribed classes. Note that if a participant attempted to engage another participant in an off-topic conversation, e.g., what they did the previous weekend, this was not counted as a “content utterance”). While each of these constructs tap into a different aspect of course engagement and may differ depending on individual characteristics (e.g., sex, personality), together they provide a more holistic measure of course engagement compared to a single measure.
Physiological markers
We measured blood pressure, heart rate, and cortisol during the stress tests to assess stress response. We assessed changes in cortisol by first normalizing the data using a log-transformation and then measuring the area under the curve with respect to increase (AUCi) using the formula from Pruessner, Hellhammer, Pruessner, & Lupien (2003). We examined change in HR and BP by establishing a mean systolic (SBP), diastolic (DBP), and heart rate (HR) value for each period during the TSST (i.e., baseline, preparatory, speech, math, recovery), and created cardiovascular reactivity scores for each period by subtracting the baseline value from the mean stressor value. For HRV, the two 5-minute HRV intervals in the baseline period were averaged, as were the two 5-minute HRV intervals in the recovery period.
The following subjective measures were collected during the online questionnaire which participants completed before and after the 6-week course unless otherwise indicated:
Mindfulness
The Children and Adolescent Mindfulness Measure (CAMM; Greco, Baer, & Smith, 2011) assesses moment-to-moment attention and acceptance of internal experiences. Participants indicate their responses ranging from 0 (never true) to 4 (always true). Higher scores indicating greater mindfulness. Factor analysis of the construction of this 10-item scale resulted in a one factor solution with a reported Cronbach’s alpha of 0.80 (Greco et al., 2011).
Self-compassion
Self-Compassion Scale (SCS; Neff, 2003a) is a 26-item measure in which response options ranged from 1 (Almost Never) to 5 (Almost Always). Higher score indicates greater self-compassion. Construct, content, and discriminant validity are well established (Neff, 2003a, 2015). Reported Cronbach alpha is .93 (Neff, 2003a; Neff, Kirkpatrick, & Rude, 2007).
Life satisfaction
Student’s Life Satisfaction Scale (SLSS; Huebner, 1991) is a 7-item scale which measures an overall evaluation of one’s life; response options ranged from 0 (never) to 3 (almost always). Higher scores indicate greater life satisfaction. Reported Cronbach alphas for adolescent samples are between .82 and .86 (Dew & Huebner, 1994; Gilman, Huebner, & Laughlin, 2000; Huebner, 1991).
Perceived stress
Perceived Stress Scale (PSS; S. Cohen, Kamarck, & Mermelstein, 1983), a 14-item scale, assesses the degree to which respondents find their lives “unpredictable, uncontrollable, and overloading”. Participant response options ranged from 0 (never) to 4 (very often). Construct validity in an adolescent sample has been established and reported Cronbach alpha is .86 (Martin, Kazarian, & Breiter, 1995).
Positive and negative affect
Positive and Negative Affect Schedule (PANAS; Watson, Clark, & Tellegen, 1988) contains two subscales: positive affect (PA; 10 words describing positive emotions) and negative affect (NA; 10 words describing negative emotions). Participants respond based on how they have felt over the previous few days using a 4-point scale ranging from 1 (very slightly or not at all) to 4 (most of the time). Higher scores indicate higher positive or negative affect. Reported Cronbach’s alphas range from .84 to .87 for negative affect and from .86 to .90 for positive affect (Watson et al., 1988). Discriminant and convergent validity have been established in adolescent samples (Dew & Huebner, 1994).
State anxiety
Spielberger State Anxiety Inventory (Spielberger et al., 1983) was assessed at two points during laboratory stress test immediately before and after the TSST; it is a widely used 20-item measure of state anxiety. Response options ranged from 1 (not at all) to 4 (very much so). Reported reliabilities range from .65 and .96 (Barnes, Harp, & Jung, 2002). State anxiety was calculated as post- stress test minus prestress test to account for variability in baseline stress.
The expectation and credibility scale
(Borkovec & Nau, 1972) is a 5-item questionnaire that assesses participants’ expectations of benefits of the course. This measure has been found to distinguish between standard psychotherapy treatments and treatments that are presumed to have no effect. As per usual protocol for this instrument, the measure was administered after the first class.
Use of mindfulness techniques during post-lab
Immediately following the second laboratory session, participants completed a questionnaire including two open-ended questions: “What stress techniques, if any, did you use during the lab?” and “How were your experiences today different from your last lab session?”
Data Analysis
SPSS 22 was used for all statistical analyses. To answer the first research question, we examined whether individuals’ participation in the classes (attendance, home practice completion, and utterances) differed by sex. We used Cohen’s d (J. Cohen, 1988) to examine the effect size of these differences. Effect size was interpreted using Cohen’s original standards (1988): small (d ≥.20), medium (d >.50), large (d >.80), and very large (d >1.30; Cohen, 1988). Because an effect size of d <.20 indicates an overlap in the two samples of > 92.0%, effect sizes less than .20 are usually considered as having no meaningful differences. However, a power analysis revealed that the present sample size could only detect an effect of 1.00 for the boys (n = 5) and an effect of .71 for the girls (n = 10). We also use effect sizes because this pilot study may be underpowered to examine differences based only on probability values (i.e., test statistics). Further, current statistical reporting guidelines (Cumming, 2014; Kline, 2013; Wilkinsion & APA Task Force for Statistical Inference, 1999) recommend interpreting results according to effect size and not statistical significance testing. Therefore, we interpret the findings with effect sizes only for which the study is powered (females, d ≥ .71; males, d ≥ 1.00. Additionally, we make recommendations for future research based on meaningful differences found according to Cohen’s recommendations (1988; i.e., d ≥.20).
To examine the second research question, we similarly examined and interpreted the effect size (Cohen’s d) and 95% confidence interval (CI) of the difference in stress reactivity (defined as mean stress level minus resting pre-stress level) from the pre-intervention lab stress testing session to the post-intervention stress testing session for females and males (means and standard deviation for all outcome variables by sex are presented in Table 1). The CI is reported to interpret precision within the sample population as well as likely significance level. That is, if the 95% CI straddles 0 then the associated statistical test would likely be non-significant. We use the same standards for interpreting Cohen’s d discussed in the first research question.
Table 1.
Means and Standard Deviations for males and females before and after the mindfulness intervention.
| Pre-Intervention M(SD) | Post-Intervention M(SD) | |||
|---|---|---|---|---|
|
| ||||
| Females | Males | Females | Males | |
| SBP – Baseline* | 109.86(8.18) | 110.48(9.80) | 105.61(7.37) | 108.86(11.67) |
| DBP- Baseline* | 64.99(4.26) | 64.86(4.17) | 62.80(5.50) | 56.48(2.74) |
| HR – Baseline* | 76.41(9.01) | 67.40(9.28) | 79.70(10.88) | 74.57(5.60) |
| SBP - Prep† | 12.01(8.73) | 9.18(5.32) | 17.32(10.85) | 12.41(6.60) |
| DBP- Prep† | 9.08 (4.98) | 7.61(7.52) | 12.63(6.54) | 12.51(4.75) |
| HR – Prep† | 18.22(14.72) | 9.67(10.55) | 17.13(10.60) | 11.50(8.56) |
| SBP - Speech† | 21.98(12.22) | 21.31(20.81) | 26.55(14.60) | 20.81(10.15) |
| DBP - Speech† | 15.28(5.14) | 13.28(6.90) | 13.93(9.43) | 14.28(8.70) |
| HR – Speech† | 20.19(14.34) | 15.67(7.56) | 21.33(16.67) | 18.90(11.49) |
| SBP - Math† | 18.01(10.48) | 16.58(9.95) | 20.82(12.26) | 17.01(8.16) |
| DBP - Math† | 11.75(4.04) | 12.08(8.07) | 11.97(7.02) | 13.51(9.01) |
| HR – Math† | 16.19(12.83) | 12.60(7.90) | 17.97(12.11) | 15.56(10.89) |
| SBP – Recovery* | 112.23(7.61) | 114.23(5.82) | 109.49(7.14) | 115.46(9.13) |
| DBP- Recovery* | 66.98(7.00) | 71.08(4.98) | 66.57(5.29) | 62.63(5.87) |
| HR – Recovery* | 79.40(9.56) | 70.03(8.10) | 84.08(10.58) | 77.66(9.90) |
| Anxiety* | 33.20(5.51) | 31.40(6.88) | 35.40(6.90) | 36.60(8.93) |
| HRV response* | −1.00(.88) | −.08(.48) | −.68(.75) | −.10(1.21) |
| HRV recovery* | .79(.78) | .17(.41) | .70(.96) | .43(.44) |
| Cortisol – Area under the curve* | .97(2.39) | .11(.72) | .11(2.14) | .41(1.26) |
| Mindfulness* | 30.60(5.12) | 38.40(7.80) | 33.00(3.50) | 35.20(5.22) |
| Self-Compassion* | 2.63(.56) | 3.26(.59) | 2.77(.57) | 3.03(.53) |
| Perceived Stress* | 29.20(4.16) | 24.00(8.48) | 31.50(6.59) | 24.00(6.44) |
| Life Satisfaction* | 3.56(.50) | 2.94(.30) | 2.50(.60) | 3.00(.39) |
| Positive Affect* | 31.30(7.80) | 30.00(5.20) | 30.90(5.30) | 36.40(4.04) |
| Negative Affect* | 22.60(5.66) | 19.60(7.23) | 22.60(4.90) | 16.80(4.87) |
Note. SBP – systolic blood pressure, DBP – diastolic blood pressure, HR – heart rate, HRV – heart rate variability
Raw score
Delta score from the baseline
Finally, for the third research question, we examined the qualitative responses of the techniques the participants used for stress reduction during the stress test. We performed a frequency count of the different types of techniques reported, and examined whether the frequency differed for males and females. To determine how the second lab experience differed from that of the first for both males and females, we read through responses and used content analysis to identify overarching themes (Hseih & Shannon, 2005). Since responses were limited in number (all but one participant responded, n =14) and brief, it was not necessary to use codes to analyze these data.
Results
Due to the small sample size, we are presenting all results as potential indications of differences in the way male and female adolescents may engage in and respond to mindfulness interventions. These results should be interpreted with caution, and must be replicated with larger samples to make any conclusive determination as to these differences.
Preliminary analysis
To determine if the TSST induced a significant stress response, we conducted repeated measures analysis of variance (RM-ANOVA) with mean scores of the physiologic data and paired t-tests with mean scores of the SSAI separately for the pre-and post-intervention laboratory session. Results indicated that on average, the TSST induced a significant stress response (Table 2). We also examined results of a self-report credibility scale to determine if males and females had different expectations following the first class of the interventions. Results of independent t-tests indicated that there was no significant perceived difference in the expectations of the course between males and females following the first class Mfemales = 27.30 (SD = 6.82), Mmales = 25.2 (SD = 8.14), t(13) = −.53, p = .61. Cohen’s d = .29 [−.79, 1.37], indicated a small effect size, with females having a slightly greater belief in the positive outcome of the course than males.
Table 2.
Repeated measure ANOVA to examine stress response to TSST
| Measure | Pre-Intervention | Post-Intervention |
|---|---|---|
| Diastolic Blood Pressure | F(4,56) = 40.95, p < .05 | F(4,56) = 30.93, p < .05 |
| Systolic Blood Pressure | F(4,56) = 42.66, p < .05 | F(4,56) = 26.25, p < .05 |
| Heart Rate | F(4,56) = 20.12, p < .05 | F(4,56) = 23.77, p < .05 |
| Heart Rate Variability | F(2,28) = 10.17, p < .05 | F(2,28) = 4.71, p < .05 |
Note. All RM-ANOVA were significant indicating that the TSST did induce stress at both pre- and post-intervention.
Course Engagement
Initially, 11 females and 5 males were enrolled in the class. One female dropped out after the first session, and was not included in any analyses. In total, seven females attended six classes and three females attended five classes (Mfemales = 5.70, SD = .48). Three males attended six classes and two males attended five classes, (Mmales = 5.60, SD = .55); Cohen’s d = .20 (−.88, 1.23), indicating a small effect size, with females attending class slightly more than males.
Home practice frequency (i.e., number of days practicing mindfulness outside of the class) was provided by participants on weeks 2 through 6 (Mfemales = 4.42, SD = .43 days per week, and Mmales= 3.61, SD = .27 days per week). Cohen’s d for Mmales compared to Mfemales = 2.08 [.78, 3.40] indicated a very large effect with females completing more home practice than males. However, upon close examination of the home practice reports, data from one male participant seemed suspect because he was an outlier as he indicated that he practiced every day possible during the 5 week period. In comparison, in a previous mindfulness intervention study, two thirds of adolescents reported that they practiced once a week or less; in a second study no one practiced the full assigned amount and two-thirds failed to do their homework at least once; (see review: Zenner, Herrnleben-Kurz & Walach, 2014). In a third study, although daily practice was encouraged, participants practiced only an average of 2 days per week (Bluth, Gaylord, Campo, Mullarkey, & Hobbs, 2016). Therefore, we recalculated the male mean and effect size with his data excluded and found a very large effect size (Mmales,adjusted = 2.70, SD = .48 days/week; Mfemales = 4.42, SD = .43 days per week; Cohen’s d = 3.86 [2.11, 5.61]).Whether considering the data either with all five males or with excluding the male that was suspect, the effect size is large, indicating that females appeared to engage in the home practices much more frequently than males.
To determine the frequency of females’ and males’ contribution to class discussions in each class, we calculated a ratio for each class: total number of times males had a content utterance in class divided by the number of males present in that class, and the total number of times females had a content utterance in class divided by the number of females present in that class. We then averaged each value across the six classes for males and for females.. Over all six classes, the content utterances averaged Mfemales = 4.89 (SD = 2.58) and Mmales= 2.87 (SD = 1.57). Cohen’s d = .87 [−.25, 1.99] indicating a large effect size, with females contributing more in class discussions than males.
Physiologic Markers
For SBP during the preparation task, change in SBP reactivity from pre-intervention to post-intervention increased similarly for females (Cohen’s d = .48 [95% CI .21–.76]) and males (Cohen’s d = .49 [95% CI .08–.90]. During both the speech tasks, females showed an increase in SBP reactivity from pre- to post-intervention (Cohen’s d = .33 [95% CI −.12 –.79]) while males demonstrated no change (Cohen’s d = −.04 [95% CI −.71–.63]. Similarly, during the math task, females demonstrated an increase in SBP stress reactivity from pre- to post-intervention (Cohen’s d = .24 [95% CI −.38 –.87]) while males showed no change (Cohen’s d = .05 [95% CI −.73–.83].
Both females and males showed an increase in DBP reactivity to preparation from pre- to post-intervention (Cohen’s d = .59 [.04, 1.13]; and (Cohen’s d = .77 [−.44, 1.97], respectively). During the speech task, there was no change from pre-intervention to post-intervention for either females (Cohen’s d = −.16 [−.64, .38]) or males (Cohen’s d = .19 [−.50, .87]). Similarly, during the math task, the magnitude of DBP reactivity from pre- to post-intervention did not change for either females (Cohen’s d = .04 [−.62, .69]) or males (Cohen’s d =.17 [−.85, 1.19]).
For HR stress reactivity during preparation, neither females (Cohen’s d = −.08 [95% CI −.49–.33]) nor males (Cohen’s d = .19 [−1.03, 1.41]) demonstrated a difference in HR reactivity during preparation from pre- to post- intervention. According to Cohen’s d, HR reactivity during the speech test for females from pre- to post-intervention did not change (Cohen’s d = .07 [−.37, .52]) while HR reactivity increased slightly for males from pre- to post-intervention (Cohen’s d = .34 [−1.26, 1.93]). Similarly, HR reactivity during the math test from pre-to post-intervention did not change for females (Cohen’s d = .14 [−.13, .41]) while HR reactivity for males increased slightly (Cohen’s d = .31 [−.81, 1.43]).
HRV response to TSST was computed by subtracting the pre-stress HRV value from the preparatory HRV value. According to Cohen’s d, females had a small increase in HRV response to the TSST from pre- to post-intervention, indicating a decreased stress response (Cohen’s d = .37 [.03, .70]) whereas there was no change from pre- to post-intervention in HRV response in males (Cohen’s d = −.01 [−1.38, 1.36]).HRV recovery to TSST was computed by subtracting the preparatory HRV value from the post-stress HRV value. According to Cohen’s d, HRV recovery from the TSST did not change from pre- to post-intervention for females (Cohen’s d = −.10 [−.53, .33]) whereas HRV recovery increased somewhat for males (Cohen’s d = .62 [.23, 1.01]), suggesting a greater recovery in response to the intervention.
Change in cortisol output and anxiety also differed between males and females. Females evidenced a small decrease in cortisol output from pre-to post-intervention, according to Cohen’s d (Cohen’s d = −.38 [–1.35, .59]) indicating less of a stress response. Males had a small increase (Cohen’s d = .26 [95% CI −.43–.95]), indicating a small increase in stress response. Change in anxiety was measured by subtracting pre-stress self-reported anxiety from post-stress self-reported anxiety. Females self-reported a very large decrease in change in anxiety during the second TSST as compared to the first TSST, according to Cohen’s d (Cohen’s d = −1.77 [−3.02, .53]), while males only showed a medium decrease in change in anxiety (Cohen’s d = −.67 [−2.02, .68]).
In relation to measures assessed after returning home after completion of the TSST, the following changes were noted. Females reported a medium increase in mindfulness from pre- to post-intervention (Cohen’s d = .54 [−.34, 1.43]) while males reported a small decrease (Cohen’s d = −.33 [−.65, .01]). Females reported a small increase in self-compassion (Cohen’s d = .24 [−.56, 1.03]). Males reported a small decrease (Cohen’s d = −.41 [−1.02, .20]) from pre- to post-intervention. Females reported a small increase in perceived stress from pre- to post-intervention (Cohen’s d = .38 [−.15, .92]). Perceived stress for males did not change (Cohen’s d = .00 [95% CI −1.29, 1.29]).. According to Cohen’s d, there was no change in self-reported life satisfaction for females (Cohen’s d = −.16 [−.67, .36]) or males (Cohen’s d = .16 [−.57, .89]). Positive affect for females did not change, according to Cohen’s d (Cohen’s d = −.06 [−.95, .83]) while males reported a very strong increase from pre- to post-intervention (Cohen’s d = 1.33 [.42, 2.24]). Females reported no change in negative affect from pre- to post-intervention (Cohen’s d = .00 [−.76, .76]) while males reported a small decrease (Cohen’s d = −.25 [−.47, .030]).
In the post-lab questionnaire, participants responded to an open ended question, “What stress reduction techniques, if any, did you use during the lab?” All females (10/10) indicated that they used some form of stress reduction technique that they had learned in class during the post-lab social stress test (e.g., body scan, three mindful breaths). In contrast, two males indicated that they did not use any stress techniques and three indicated that they used stress techniques that they had learned in class (e.g., mindful breathing).
Participants were also asked, “How were your experiences today different from your last lab session?” Eight of the females and three of the males indicated that they felt less nervous during the second lab. Typical comments included “I was much less stressed out about the tasks I had to complete. I was more carefree this time and didn’t worry so much. I learned from [the instructor] that you just have to let things be sometime” (female), and “Less stressful, easier, felt like it was shorter” (male). One male indicated, “I think the interview went better, but I messed up at about 420ish on the subtracting one, and when they told me I was incorrect and had to start over, I thought it was completely ridiculous and couldn’t keep a straight face to the rest of it.”
Discussion
As developmental differences and differences in timing and rates of pubertal maturation become apparent in early adolescence, the purpose of this study was to explore whether there might be differences in how male and female adolescents engage with and respond to a mindfulness intervention. There have been few studies on sex differences in mindfulness interventions with adults, and none that we could find with adolescents; for this reason, it is our hope that this initial exploratory investigation would shed light on whether this area of research should be further investigated with larger samples.
In relation to our first research question, we found effect size differences between males and females in their engagement of the mindfulness course. Specifically, females tended to be more engaged in the intervention than males, practiced mindfulness skills more frequently at home, and were more engaged in class discussions than males. Further, females seemed to be more attracted to the course than males as is indicated by differences in enrollment; 62% of participants were female. This may have been driven in part by the fact that females had a slightly greater belief in the credibility of the intervention than did their male counterparts, and therefore not only agreed to participate in the program but put forth more effort to engage with the program once they were enrolled. Another possibility may be due to developmental differences; since adolescent females mature earlier than males (Steinberg & Morris, 2001), they may have greater interest and understanding of a program that focuses on development of stress reduction techniques. Because of the development stage, females may have more of an aptitude to see the possibility of long-term benefits of such a program, while looking beyond the immediate future may be more challenging for adolescent males.
In our second research question, we explored the potential differential outcomes pertaining to how males and females change from pre-intervention to post-intervention on psychological and physiological variables of interest. Overall, it appears that only two variables changed pre to post when constrained by the parameters set by our power analysis: changes in anxiety in response to the TSST for females and positive affect for males. Females self-reported less increase in anxiety during the second TSST and the effect size for the change from pre- to post- was large. We did not have the statistical power to detect a change in anxiety during the TSST from pre- to post-intervention for males; however, a future study with a larger sample may be able to determine whether there is a change in anxiety pre- to post-intervention for males. Qualitative responses provided in the post-lab questionnaire confirmed the finding for females as most females indicated that they were less stressed during the second TSST than the first. Interestingly, for males and not females, positive affect increased substantially from pre- to post- intervention. It is possible that a mindfulness intervention is differentially effective for males and females as it may serve to decrease female anxiety while it increases male positive affect.
Future research may benefit by further exploring some of the possible sex differences which were meaningful according to Cohen’s recommendations (1988) but that our sample was not powered to detect. For example, for males, indicators of physiological stress response to the TSST demonstrated that males were more stressed during the post–intervention TSST; cortisol output was greater, change in HR was slightly greater during speech and math tasks, and change in SBP and DBP was slightly greater during the preparatory task post-intervention. However, we observed no change in HRV from pre- to post-intervention lab assessments, and no change in SBP or DBP during the speech or math tasks. Despite these increases in stress demonstrated by some of the physiological results, males self-reported less anxiety as a result of the TSST in the second (post) lab assessment, and this was further substantiated by their qualitative responses in the post-lab questionnaire. Further, results of the online survey indicated that males evidenced a small decrease in self-reported mindfulness and self-compassion as a result of the intervention, no change in life satisfaction or perceived stress, and a positive change in overall mood (i.e., increase in positive affect and decrease in negative affect). For males, a contributing factor of this mismatch of physiological and self-report stress measures may include that males, at this developmental age, are not as aware of the nuances of their emotional states as females. This mismatch for males might be further explained by their reduction in self-reported mindfulness and self-compassion.
Similarly, findings in females that had meaningful effect sizes (Cohen, 1988) may benefit by further investigation in future research. For example, females appeared to demonstrate a somewhat different depiction of intervention outcomes. First, findings from both cortisol and HRV data indicate that females were less stressed at the post-intervention lab assessment (with no change in HR). SBP and DBP showed some indication of greater stress during the second TSST as evidenced by small to medium effect size differences from the first lab assessment during the preparatory phase and small to medium effect size differences from the first lab assessment of SBP during speech and math tasks (no change in DBP). Findings from the online survey indicate an increase in both mindfulness and self-compassion for females, and no change in positive and negative affect. Contrary to these results, females also reported an increase in perceived stress and decrease in life satisfaction post-intervention. A contributing factor of this mismatch in results may be that females experience an increase in self-awareness (i.e., mindfulness) which make them more aware of their stress as a result of the intervention (White, 2012); this will be discussed in greater depth later. Though these preliminary analyses, limited by a small sample size, indicate some sex differences as a results of the mindfulness intervention, future research is needed to substantiate and further explore these findings.
The third research question addressed whether participants used any of the stress-reduction techniques that they had learned from the mindfulness course during the second TSST. We felt that this was an important question as it would provide some indication as to whether the skills that participants acquired would transfer to their daily experiences of stress. Here again we found what appeared to be a difference between that which was reported by males and females. Three of the five males indicated that they used a skill that had been introduced and practiced during the six-week course; however, all females indicated that they had used at least one of the mindfulness skills.
To summarize, it appears that both males and females experienced some degree of anticipatory stress upon beginning the second lab assessment. This is understandable, as having experienced the TSST previously, they may have anticipated stress and this may have been reflected in their increased change in SBP and DBP during the preparatory phase. Overall, the post-intervention TSST experience was less stressful relative to the first TSST experience for females than for males, as indicated by cortisol and HRV. This may be due to females’ greater use of stress-reduction techniques while experiencing the TSST. The intervention appeared to be effective in increasing mindfulness and self-compassion for females but not for males, did not improve perceived stress or life satisfaction for either males or females, and may have had some positive effect on mood for males.
There are a number of possible explanations for sex differences in response to this intervention. First, as assessed after the first class, females “believed” more in the potential value of the intervention, and this may have prompted their greater degree of engagement in the class, eventually leading to their increase in mindfulness and self-compassion, and subsequent use of these skills during the TSST. It is also possible that their greater degree of engagement in the course was due to developmental differences (i.e., greater maturity) than males. Another possible explanation for less engagement on the part of males is that there were twice as many females in the class and the instructor was also female; it is possible that males felt that they were in a “minority” and therefore felt intimidated and were less likely to participate. In other types of interventions, differences between how male and female adolescents respond to the interventions has been reported (Craig & Sprang, 2014; Hamilton & Klimes-Dougan, 2015) and degree of engagement of youth in mindfulness interventions has been related to outcomes (Huppert & Johnson, 2010). Further, in a conceptual model of Learning to BREATHE, Broderick and Jennings (2012) outline different ways in which adolescents respond to stress, articulating that some respond by disengaging. It is possible that during the TSST some males “disengaged” rather than employing mindfulness skills. As one male reflected in his post-questionnaire “…When they told me I was incorrect and had to start over, I thought it was completely ridiculous and couldn’t keep a straight face to the rest of it.” If used regularly in response to stress, disengagement (i.e., numbing one’s emotions) can lead to substance use, aggressive behavior, and cognitive distortion (Broderick & Jennings, 2012; Hayes, Wilson, Gifford, Follette, & Strosahl, 1996) and is therefore considered to not be a healthy response if used over the long-term.
The increase in mindfulness and self-compassion in females post-intervention was expected, but the lack of improvement in other self-reported outcomes (i.e., perceived stress, life satisfaction, positive and negative affect) was surprising especially given the change in the former. To fully understand why this may have occurred, it is important to first consider the widely accepted temporal order of how change takes place in mindfulness interventions: through mindfulness training, one becomes more mindful and more self-compassionate, which allows one to respond more mindfully and with less self-judgment to events which take place in daily life, which in turn results in improvements in overall mental health (Baer, Carmody, et al., 2012; Baer, Lykins, & Peters, 2012; Carmody & Baer, 2008; Keng, Smoski, Robins, Ekblad, & Brantley, 2012). Adolescent females in our study demonstrated some improvements in mindfulness and self-compassion, reported using mindfulness tools during the TSST, but did not evidence improvements in mental health outcomes. According to Baer, Carmody & Hunsinger (2012), mindfulness increases in the first several weeks of a mindfulness intervention and perceived stress decreases after the fourth week; however, it may be that this trajectory is different for adolescents, particularly for adolescent females. These teens may need more time or a greater “dose” of mindfulness to evidence positive change in outcomes. The empirical question as to the necessary “dose” of mindfulness to evidence change would also benefit from further investigation in future studies.
It is particularly noteworthy that although there were increases in mindfulness and self-compassion in females, perceived stress and life satisfaction actually worsened from pre- to post-intervention. One possible explanation for this is that increasing awareness through development of mindfulness made these females more acutely aware of their suffering, and in the short term, they experienced greater discomfort, evidenced as a slight increase in perceived stress and decrease in life satisfaction. Similar results were reported in another study which utilized an all-female sample (White, 2012). This transient increase of stress (Hayes & Feldman, 2004) which may occur in the process of learning mindfulness has received little attention; in fact, turning toward difficult emotions and embracing them rather than avoiding them (i.e., disengaging) or over-identifying with them (i.e., ruminating or obsessing) is critical to learning and living mindfulness (Chödrön, 2007; Kabat-Zinn, 1990). It is possible that these nuances – this increase in mindfulness and slight decrease in some emotional wellbeing outcomes - may have been masked in previous studies that used significance testing rather than effect sizes, the latter of which elucidate smaller changes and the magnitude of that change in smaller sample sizes. It is possible that improvements in emotional wellbeing constructs may have emerged in follow-up assessments; future studies would benefit from conducting both short and long-term follow-up assessments at 1-month and 6-month intervals, for example.
In addition to conducting these follow-up assessments, another possible explanation for the lack of change in positive and negative affect in females is that the amount of increase in mindfulness and self-compassion experienced was not substantial enough to initiate detectable changes in these constructs. It may be the case that this 6-week intervention does not offer substantial instruction or practice to change female adolescents’ mood. External factors affecting mood (e.g., conflict with peers, academic pressures, challenging family relationships) may be too great and volatile during this developmental period to be overcome by the small changes in mindfulness and self-compassion that were evidenced here. Also, as this study was underpowered, it may be that there was not enough statistical power to detect changes. Replication with larger samples is essential prior to making any definitive statement about changes in constructs.
Males, however, did report positive changes in mood (i.e., positive and negative affect) despite the fact that they did not report increases in mindfulness or self-compassion. It may be that these positive changes in mood were determined by external factors; there is ample evidence that adolescent females experience daily events in a more negative light than males of the same age, and therefore experience greater negative mood, anxiety, and depression (Lewinsohn, Gotlib, Lewinsohn, Seeley, & Allen, 1998; Nolen-Hoeksema & Girgus, 1994). Alternatively, it is possible that the benefit of a mindfulness intervention is different for males and females as it improves males’ mood rather than their physiological stress response and other self-report measures. Future studies should investigate this possibility to determine if this is the case. Again, the lack of ample statistical power in this study may have prevented the detection of changes in these variables, and future studies should utilize a larger study that is powered to detect these differences.
Overall, there has been a paucity of research on sex differences in mindfulness interventions, although a recent review of mindfulness studies with adults with substance use challenges indicates that mindfulness training may be more appealing and effective for females than for males (Katz & Toner, 2012). Our study contributes to the literature by exploring the potential differences in engagement and outcomes a mindfulness intervention between adolescent males and females. However, due to the small sample size and lack of ample statistical power, we are unable to make any conclusive statement as to whether the intervention is more effective or appealing to females than males, yet believe that there is ample evidence to warrant further study with larger samples. It may be that mindfulness itself is effective for both male and female adolescents but the mechanism for change or the temporal order of change may differ by sex. Additionally, future research may reveal that the delivery and types of activities and meditations may need to be tailored to fit the differential developmental needs of male and female adolescents. Alternatively, it may be such that the different meditations or tools themselves (i.e., body scan versus mindful breathing) may be more effective for males, while other practices are completely ineffective. To date, these questions have not been investigated, and the field would benefit greatly from further study in these areas.
Limitations
This study has distinct limitations. First, the sample size was small and therefore underpowered to detect changes in variables. The lack of statistical power also limited analyses that we could perform (e.g., interactions among the variables). Second, as temporal order of changes in constructs may have been a factor in the lack of changes evidenced in some variables, our study would have been improved had we conducted follow-up measures. Third, there were twice as many females as males in the intervention, and the instructor was also female. This may have affected male engagement in class. Fourth, as we depended on unpaid volunteers to be the “committee members” who facilitated the TSST, they varied in both age and sex for each participant, and this may have had an effect on the level of stress experienced by the adolescents during the TSST. For example, it may be that adolescents are more intimidated by an older male, and less so by a younger female. In future studies it is recommended to have the committee members be consistent in age and sex for each participant.
In conclusion, we have found initial evidence that warrants further investigation as to whether a mindfulness intervention for adolescents may have differential effects for males and females. Future research is needed to further explore and explain sex differences on the effectiveness of a mindfulness intervention to reduce stress and improve coping strategies among this age group. Future research should focus on sex differences in mechanisms of change, temporal order of change, and classroom dynamics that may impact intervention outcomes. We strongly recommend more research in this area of study.
Acknowledgments
Funding for this project was provided through a Francisco J. Varela Award by the Mind and Life Foundation, grant number T32AT003378-04 from the National Center on Complementary and Alternative Medicine (NCCAM) and grant number R01MH099076 from the National Institute of Mental Health (NIMH) at the National Institutes of Health (NIH). Analyses and conclusions are the responsibility of the authors rather than the funders.
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Informed consent was obtained from all individual participants included in the study.
Footnotes
All authors declare that there is no conflict of interest.
Author Contributions
KB conceived of, designed, and executed the study, PR conducted the data analysis and wrote the results, SG collaborated with the design and data collection, and edited the manuscript.
References
- Baer RA, Carmody J, Hunsinger M. Weekly change in mindfulness and perceived stress in a mindfulness-based stress reduction program. Journal of Clinical Psychology. 2012;68(7):755–765. doi: 10.1002/jclp.21865. [DOI] [PubMed] [Google Scholar]
- Baer RA, Lykins EL, Peters JR. Mindfulness and self-compassion as predictors of psychological wellbeing in long-term meditators and matched nonmeditators. The Journal of Positive Psychology. 2012;7(3):230–238. [Google Scholar]
- Baer RA, Lykins ELB, Peters JR. Mindfulness and self-compassion as predictors of psychological wellbeing in long-term meditators and matched nonmeditators. The Journal of Positive Psychology. 2012;7(3):230–238. doi: 10.1080/17439760.2012.674548. [DOI] [Google Scholar]
- Barnes LLB, Harp D, Jung WS. Reliability generalizations of scores on the Spielberger state-trait anxiety inventory. Educational and Psychological Measurement. 2002;62(4):603–615. [Google Scholar]
- Biegel G, Brown K, Shapiro S, Schubert C. Mindfulness-based stress reduction for the treatment of adolescent psychiatric outpatients: A randomized clinical trial. Journal of Clinical and Consulting Psychology. 2009;77(5):855–866. doi: 10.1037/a0016241. [DOI] [PubMed] [Google Scholar]
- Bluth K, Blanton P. Mindfulness and self-compassion: Exploring pathways of adolescent wellbeing. Journal of Child and Family Studies. 2014;23(7):1298–1309. doi: 10.1007/s10826-013-9830-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bluth K, Campo RA, Pruteanu-Malinici S, Reams A, Mullarkey M, Broderick PC. A School-Based Mindfulness Pilot Study for Ethnically Diverse At-Risk Adolescents. Mindfulness. 2016;7(1):90–104. doi: 10.1007/s12671-014-0376-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bluth K, Gaylord SA, Campo RA, Mullarkey MC, Hobbs L. Making friends with yourself: a mixed methods pilot study of a mindful self-compassion program for adolescents. Mindfulness. 2016;7(2):479–492. doi: 10.1007/s12671-015-0476-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bluth K, Roberson PNE, Gaylord SA, Faurot KR, Grewen KM, Arzon S, Girdler SS. Does self-compassion protect adolescents from stress? Journal of Child and Family Studies. 2015;25(4):1098–1109. doi: 10.1007/s10826-015-0307-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Borkovec TD, Nau SD. Credibility of analogue therapy rationales. Journal of Behavior Therapy & Experimental Psychiatry. 1972;3(4):257–260. [Google Scholar]
- Britton W, Bootzin R, Cousins J, Hasler B, Peck T, Shapiro S. The contribution of mindfulness practice to a multicomponent behavioral sleep intervention following substance abuse treatment in adolescents: A treatment-development study. Substance Abuse. 2010;31(2):86–97. doi: 10.1080/08897071003641297. [DOI] [PubMed] [Google Scholar]
- Britton WB, Shahar B, Szepsenwol O, Jacobs WJ. Mindfulness-based cognitive therapy improves emotional reactivity to social stress: results from a randomized controlled trial. Behavior Therapy. 2012;43(2):365–380. doi: 10.1016/j.beth.2011.08.006. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Broderick P. Learning to BREATHE: A mindfulness curriculum for adolescents to cultivate emotion regulation, attention, and performance. Oakland, CA: New Harbinger Press; 2013. [Google Scholar]
- Broderick PC, Jennings PA. Mindfulness for adolescents: A promising approach to supporting emotion regulation and preventing risky behavior. New directions for youth development. 2012;2012(136):111–126. doi: 10.1002/yd.20042. [DOI] [PubMed] [Google Scholar]
- Broderick PC, Metz S. Learning to BREATHE: A pilot trial of a mindfulness curriculum for adolescents. Advances in school mental health promotion. 2009;2(1):35–46. [Google Scholar]
- Brown KW, Weinstein N, Creswell JD. Trait mindfulness modulates neuroendocrine and affective responses to social evaluative threat. Psychoneuroendocrinology. 2012;37(12):2037–2041. doi: 10.1016/j.psyneuen.2012.04.003. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Burke CA. Mindfulness-based approaches with children and adolescents: A preliminary review of current research in an emergent field. Journal of Child and Family Studies. 2010;19(2):133–144. doi: 10.1007/s10826-009-9282-x. [DOI] [Google Scholar]
- Carlson LE, Speca M, Patel KD, Goodey E. Mindfulness-based stress reduction in relation to quality of life, mood, symptoms of stress, and immune parameters in breast and prostate cancer outpatients. Psychosomatic Medicine. 2003;65(4):571–581. doi: 10.1097/01.psy.0000074003.35911.41. [DOI] [PubMed] [Google Scholar]
- Carmody J, Baer RA. Relationships between mindfulness practice and levels of mindfulness, medical and psychological symptoms and well-being in a mindfulness-based stress reduction program. Journal of Behavioral Medicine. 2008;31(1):23–33. doi: 10.1007/s10865-007-9130-7. [DOI] [PubMed] [Google Scholar]
- Chödrön P. The places that scare you: A guide to fearlessness in difficult times. Shambhala Publications; 2007. [Google Scholar]
- Cohen J. Statistical power analysis for the behavioral sciences. 2. Hillsdale, NJ: Erlbaum; 1988. [Google Scholar]
- Cohen S, Kamarck T, Mermelstein R. A global measure of perceived stress. Journal of Health and Social Behavior. 1983;24(4):385–396. [PubMed] [Google Scholar]
- Craig CD, Sprang G. Gender differences in trauma treatment: Do boys and girls respond to evidence-based interventions in the same way? Violence and Victims. 2014;29(6):927–939. doi: 10.1891/0886-6708.vv-d-13-00016. [DOI] [PubMed] [Google Scholar]
- Cumming G. The new statistics: Why and how. Psychological Science. 2013;25:7–29. doi: 10.1177/0956797613504966. http://dx.doi.org/10.1177/0956797613504966. [DOI] [PubMed] [Google Scholar]
- Davidson RJ, Kabat-Zinn J, Schumacher J, Rosenkranz M, Muller D, Santorelli SF, … Sheridan JF. Alterations in brain and immune function produced by mindfulness meditation. Psychosomatic Medicine. 2003;65(4):564–570. doi: 10.1097/01.psy.0000077505.67574.e3. [DOI] [PubMed] [Google Scholar]
- De Vibe M, Bjørndal A, Tipton E, Hammerstrøm KT, Kowalski K. Mindfulness based stress reduction (MBSR) for improving health, quality of life, and social functioning in adults. Campbell Systematic Reviews. 2012;8(3):1–128. [Google Scholar]
- De Vibe M, Solhaug I, Tyssen R, Friborg O, Rosenvinge JH, Sorlie T, Bjorndal A. Mindfulness training for stress management: a randomised controlled study of medical and psychology students. BMC Medical Education. 2013;13(1):107. doi: 10.1186/1472-6920-13-107. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Dew T, Huebner ES. Adolescents perceived quality of life: An exploratory investigation. Journal of School Psychology. 1994;32(2):185–199. [Google Scholar]
- Eccles JS, Blumenfeld P. Classroom experiences and student gender: Are there differences and do they matter? In: Wilkinson LC, Marrett CB, editors. Gender influences in classroom interaction. Orlando: Academic Press; 1985. pp. 79–114. [Google Scholar]
- Gilman R, Huebner ES, Laughlin J. A first study of the multidimensional students’ life satisfaction scale with adolescents. Social Indicators Research. 2000;52(2):135–160. [Google Scholar]
- Goyal M, Singh S, Sibinga EM, Gould NF, Rowland-Seymour A, Sharma R, … Haythornthwaite JA. Meditation programs for psychological stress and well-being: a systematic review and meta-analysis. JAMA Internal Medicine. 2014;174(3):357–368. doi: 10.1001/jamainternmed.2013.13018. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Greco LA, Baer RA, Smith GT. Assessing mindfulness in children and adolescents: development and validation of the Child and Adolescent Mindfulness Measure (CAMM) Psychological assessment. 2011;23(3):606–614. doi: 10.1037/a0022819. [DOI] [PubMed] [Google Scholar]
- Greeson JM. Mindfulness Research Update: 2008. Complementary Health Practice Review. 2009;14(10):10–18. doi: 10.1177/1533210108329862. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hamilton E, Klimes-Dougan B. Gender differences in suicide prevention responses: Implications for adolescents based on an illustrative review of literature. International Journal of Environmental Research on Public Health. 2015;12(3):2359–2372. doi: 10.3390/ijerph120302359. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hayes AM, Feldman G. Clarifying the construct of mindfulness in the context of emotion regulation and the process of change in therapy. Clinical Psychology: science and practice. 2004;11(3):255–262. [Google Scholar]
- Hayes SC, Wilson KG, Gifford EV, Follette VM, Strosahl K. Experiential avoidance and behavioral disorders: a functional dimensional approach to diagnosis and treatment. Journal of Consulting and Clinical Psychology. 1996;64(6):1152. doi: 10.1037//0022-006x.64.6.1152. [DOI] [PubMed] [Google Scholar]
- Hofmann SG, Sawyer AT, Witt AA, Oh D. The effect of mindfulness-based therapy on anxiety and depression: A meta-analytic review. Journal of Consulting and Clinical Psychology. 2010;78(2):169. doi: 10.1037/a0018555. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hoge EA, Bui E, Marques L, Metcalf CA, Morris LK, Robinaugh DJ, … Simon NM. Randomized controlled trial of mindfulness meditation for generalized anxiety disorder: effects on anxiety and stress reactivity. Journal of Clinical Psychiatry. 2013;74(8):786–792. doi: 10.4088/JCP.12m08083. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hseih HF, Shannon SE. Three approaches to qualitative content analysis. Qualitative Health Research. 2005;15(9):1277–1288. doi: 10.1177/1049732305276687. [DOI] [PubMed] [Google Scholar]
- Huebner ES. Initial Development of the Student’s Life Satisfaction Scale. School Psychology International. 1991;12(3):231–240. doi: 10.1177/0143034391123010. [DOI] [Google Scholar]
- Huppert F, Johnson D. A controlled trial of mindfulness training in schools: The importance of practice for an impact of well-being. Journal of Positive Psychology. 2010;5(4):264–274. [Google Scholar]
- Jain S, Shapiro SL, Swanick S, Roesch SC, Mills PJ, Bell I, Schwartz GE. A randomized controlled trial of mindfulness meditation versus relaxation training: effects on distress, positive states of mind, rumination, and distraction. Annals of behavioral medicine. 2007;33(1):11–21. doi: 10.1207/s15324796abm3301_2. [DOI] [PubMed] [Google Scholar]
- Jones MG, Wheatley J. Gender differences in teacher-student interactions in science classrooms. Journal of Research in Science Teaching. 1990;27(9):861–874. [Google Scholar]
- Kabat-Zinn J. Full Catastrophe Living. New York: Random House; 1990. [Google Scholar]
- Kabat-Zinn J. Wherever you go, there you are: Mindfulness in Everyday Life. New York: Hyperion; 1994. [Google Scholar]
- Katz D, Toner B. A systematic review of gender differences in the effectiveness of mindfulness-based treatments for substance use disorders. Mindfulness. 2012;4(4) doi: 10.1007/s12671-012-0132-3. [DOI] [Google Scholar]
- Keng SL, Smoski MJ, Robins CJ, Ekblad AG, Brantley JG. Mechanisms of change in mindfulness-based stress reduction: Self-compassion and mindfulness as mediators of intervention outcomes. Journal of Cognitive Psychotherapy. 2012;26(3):270–280. [Google Scholar]
- Khoury B, Lecomte T, Fortin G, Masse M, Therien P, Bouchard V, … Hofmann SG. Mindfulness-based therapy: a comprehensive meta-analysis. Clinical Psychology Review. 2013;33(6):763–771. doi: 10.1016/j.cpr.2013.05.005. [DOI] [PubMed] [Google Scholar]
- Kirschbaum C, Pirke KM, Hellhammer DH. The ‘Trier Social Stress Test’ -- a tool for investigating psychobiological stress responses in a laboratory setting. Neuropsychobiology. 1993;28(1–2):76–81. doi: 10.1159/000119004. [DOI] [PubMed] [Google Scholar]
- Kline RB. Beyond significance testing: Statistics reform in the behavioral sciences. 2. Washington, DC: APA Books; 2013. [Google Scholar]
- Laurent H, Laurent S, Hertz R, Egan-Wright D, Granger DA. Sex-specific effects of mindfulness on romantic partners’ cortisol responses to conflict and relations with psychological adjustment. Psychoneuroendocrinology. 2013;38(12):2905–2913. doi: 10.1016/j.psyneuen.2013.07.018. [DOI] [PubMed] [Google Scholar]
- LeBlanc JC, Almudevar A, Brooks SJ, Kutcher S. Screening for adolescent depression: comparison of the Kutcher Adolescent Depression Scale with the Beck depression inventory. Journal of Child Adolescent Psychopharmacology. 2002;12(2):113–126. doi: 10.1089/104454602760219153. [DOI] [PubMed] [Google Scholar]
- Lewinsohn PM, Gotlib IH, Lewinsohn M, Seeley JR, Allen NB. Gender differences in anxiety disorders and anxiety symptoms in adolescents. Journal of abnormal psychology. 1998;107(1):109. doi: 10.1037//0021-843x.107.1.109. [DOI] [PubMed] [Google Scholar]
- Luders E, Toga A, Lepore N, Gaser C. The underlying anatomical correlates of long-term meditation: Larger hippocampal and frontal volumes of gray matter. Neuroimage. 2009;45(3):672–678. doi: 10.1016/j.neuroimage.2008.12.061. [DOI] [PMC free article] [PubMed] [Google Scholar]
- MacBeth A, Gumley A. Exploring compassion: a meta-analysis of the association between self-compassion and psychopathology. Clinical Psychology Review. 2012;32(6):545–552. doi: 10.1016/j.cpr.2012.06.003. [DOI] [PubMed] [Google Scholar]
- Martel F, Hayward C, Lyons D, Sanborn K, Varady S, Schatzberg A. Salivary cortisol levels in socially phobic adolescent girls. Depression and Anxiety. 1999;10(1):25–27. doi: 10.1002/(sici)1520-6394(1999)10:1<25::aid-da4>3.0.co;2-o. [DOI] [PubMed] [Google Scholar]
- Martin R, Kazarian S, Breiter H. Perceived stress, life events, dysfunctional attitudes, and depression in adolescent psychiatric inpatients. Journal of Psychopathology and Behavioral Assessment. 1995;17(1):81–95. [Google Scholar]
- Metz S, Frank J, Reibel D, Cantrell T, Sanders R, Broderick P. The effectiveness of the Learning to BREATHE program on adolescent emotion regulation. Research in Human Development. 2013;10(3):252–272. [Google Scholar]
- Neff KD. The development and validation of a scale to measure self-compassion. Self and Identity. 2003a;2(3):223–250. doi: 10.1080/15298860390209035. [DOI] [Google Scholar]
- Neff KD. Self-compassion: An alternative conceptualization of a healthy attitude toward oneself. Self and Identity. 2003b;2(2):85–101. [Google Scholar]
- Neff KD. The self-compassion scale is a valid and theoretically coherent measure of self-compassion. Mindfulness. 2015;7(1) doi: 10.1007/s12671-015-0479-3. [DOI] [Google Scholar]
- Neff KD, Dahm KA. Self-Compassion: What it is, what it does, and how it relates to mindfulness. In: Ostafin BD, Robinson MD, Meier BP, editors. Handbook of mindfulness and self-regulation. New York: Springer; 2014. pp. 121–137. [Google Scholar]
- Neff KD, Kirkpatrick KL, Rude SS. Self-compassion and adaptive psychological functioning. Journal of Research in Personality. 2007;41(1):139–154. doi: 10.1016/j.jrp.2006.03.004. [DOI] [Google Scholar]
- Nolen-Hoeksema S, Girgus JS. The emergence of gender differences in depression during adolescence. Psychological Bulletin. 1994;115(3):424. doi: 10.1037/0033-2909.115.3.424. [DOI] [PubMed] [Google Scholar]
- Porges SW. Method and apparatus for evaluating rhythmic oscillations in a periodic physiological response system. 4,510,944 US Patent. 1985
- Pruessner M, Hellhammer DH, Pruessner JC, Lupien SJ. Self-reported depressive symptoms and stress levels in healthy young men: associations with the cortisol response to awakening. Psychosomatic Medicine. 2003;65(1):92–99. doi: 10.1097/01.psy.0000040950.22044.10. [DOI] [PubMed] [Google Scholar]
- Rao U, Hammen C, Ortiz LR, Chen LA, Poland RE. Effects of early and recent adverse experiences on adrenal response to psychosocial stress in depressed adolescents. Biological psychiatry. 2008;64(6):521–526. doi: 10.1016/j.biopsych.2008.05.012. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Snippe E, Nyklíček I, Schroevers MJ, Bos EH. The temporal order of change in daily mindfulness and affect during mindfulness-based stress reduction. Journal of Counseling Psychology. 2015;62(2):106. doi: 10.1037/cou0000057. [DOI] [PubMed] [Google Scholar]
- Speca M, Carlson LE, Goodey E, Angen M. A randomized, wait-list controlled clinical trial: The effect of a mindfulness meditation-based stress reduction program on mood and symptoms of stress in cancer outpatients. Psychosomatic Medicine. 2000;62(5):613–622. doi: 10.1097/00006842-200009000-00004. [DOI] [PubMed] [Google Scholar]
- Spielberger CD, Gorsuch RL, Lushene RE, Vagg PR, Jacobs GA. Manual for the State-Trait Anxiety Inventory. Palo Alto, CA: Consulting Psychologists Press, Inc; 1983. [Google Scholar]
- Steinberg L, Morris AS. Adolescent development. Journal of Cognitive Education and Psychology. 2001;2(1):55–87. [Google Scholar]
- Stroud LR, Salovey P, Epel ES. Sex differences in stress responses: social rejection versus achievement stress. Biological psychiatry. 2002;52(4):318–327. doi: 10.1016/s0006-3223(02)01333-1. [DOI] [PubMed] [Google Scholar]
- Watson T, Clark L, Tellegen A. Development and validation of brief measures of positive and negative affect: The PANAS scales. Journal of Personality and Social Psychology. 1988;54(6):1063–1070. doi: 10.1037//0022-3514.54.6.1063. [DOI] [PubMed] [Google Scholar]
- White LS. Reducing stress in school-age girls through mindful yoga. Journal of Pediatric Health Care. 2012;26(1):45–56. doi: 10.1016/j.pedhc.2011.01.002. [DOI] [PubMed] [Google Scholar]
- Wilkinson L APA Task Force for Statistical Inference. Statistical methods in psychology journals: Guidelines and explanations. American Psychologist. 1999;54(8):594–604. [Google Scholar]
- Zenner C, Herrnleben-Kurz S, Walach H. Mindfulness-based interventions in schools-a systematic review and meta-analysis. Frontiers in Psychology. 2014;5(603):1–20. doi: 10.3389/fpsyg.2014.00603. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Zessin U, Dickhäuser O, Garbade S. The relationship between self-compassion and well-being: A meta-analysis. Applied Psychology: Health and Well-Being. 2015;7(3):340–364. doi: 10.1111/aphw.12051. [DOI] [PubMed] [Google Scholar]
- Zoogman S, Goldberg S, Hoyt W, Miller L. Mindfulness interventions with youth: A meta-analysis. Mindfulness. 2014 doi: 10.1007/s12671-013-0260-4. [DOI] [Google Scholar]