

Supplemental digital content is available in the article.
Key Words: SEDENTARY BEHAVIOR, AGING, MUSCLE STRENGTH, FUNCTIONAL HEALTH
ABSTRACT
Purpose
Television (TV) watching is the most prevalent sedentary leisure time activity in the United Kingdom. We examined associations between TV viewing time, measured over 10 yr, and two objective measures of physical capability, usual walking speed (UWS) and grip strength.
Methods
Community-based participants (n = 8623; 48–92 yr old) enrolled in the European Prospective Investigation of Cancer—Norfolk study attended a third health examination (3HC, 2006–2011) for measurement of maximum grip strength (Smedley dynamometer) and UWS. TV viewing time was estimated using a validated questionnaire (n = 6086) administered during two periods (3HC, 2006–2007; 2HC, 1998–2000). Associations between physical capability and TV viewing time category (<2, 2 < 3, 3 < 4, and ≥4 h·d−1) at the 3HC, 2HC, and using an average of the two measures were explored. Sex-stratified analyses were adjusted for age, physical activity, anthropometry, wealth, comorbidity, smoking, and alcohol intake and combined if no sex–TV viewing time interactions were identified.
Results
Men and women who watched the least TV at the 2HC or 3HC walked at a faster usual pace than those who watched the most TV. There was no evidence of effect modification by sex (Pinteraction = 0.09), and in combined analyses, participants who watched for <2 h·d−1 on average walked 4.29 cm·s−1 (95% confidence interval, 2.56–6.03) faster than those who watched for ≥4 h·d−1, with evidence of a dose–response association (Ptrend < 0.001). However, no strong associations with grip strength were found.
Conclusions
TV viewing time predicted UWS in older adults. More research is needed to inform public health policy and prospective associations between other measures of sedentariness, such as total sitting time or objectively measured sedentary time, and physical capability should be explored.
Current public health guidance recommends that older adults undertake at least 150 min·wk−1 of moderate-to-vigorous physical activity (MVPA) (6), along with muscle-strengthening activities at least twice per week. However, it is possible to meet these guidelines and still spend most of the time sedentary (4).
Sedentary behavior encapsulates time spent sitting or lying during wakeful hours, when energy expenditure is at or just above the basal metabolic rate (≤1.5 METs) (30). It has been proposed as an independent risk factor for poor health and has been associated with obesity, increased cardiometabolic risk, and mortality, independent of time spent in MVPA (36). These associations have been reported using both measures of total sitting time and measures of specific sedentary behaviors (21,40). Television (TV) watching in particular, a sedentary behavior reported by a large proportion of adults across all age groups and with high daily exposure (19), has been examined extensively. However, few studies have considered the potential effect of either overall sitting or specific sedentary behaviors on muscle strength and physical performance or “physical capability,” even though the disuse muscle atrophy associated with prolonged bed rest is familiar (23).
Objective markers of physical capability include grip strength, a correlate of general muscle strength, and performance measures such as usual walking speed (UWS). Maintenance of physical capability is an important part of healthy aging, and conditions associated with loss of physical capability, such as sarcopenia and frailty, are significant causes of late-life morbidity (5,8,9). Proposed interventions for sarcopenia include resistance exercise training, and its benefits are well established (27). However, not all older people are able to engage in such interventional exercise programs, and smaller changes to everyday lifestyle that may positively affect functional health should be explored.
To date, there is limited evidence on the association between overall sitting or specific sedentary behaviors such as TV watching and physical capability. Increased sedentary time, measured objectively using accelerometry, has been associated with reduced self-reported physical function in two cross-sectional studies on older adults, independent of time spent in MVPA (2,12). Longer total sitting time was also associated with worse self-reported physical functional health in a longitudinal study on women (31). Fewer studies have considered objectively measured physical capability, but two cross-sectional reports have associated lower physical capability with increased total sedentary time and TV viewing time (14,28).
To our knowledge, however, no studies have reported relations between prospectively measured TV viewing and objective measures of physical capability. Therefore, we examined the relation between TV viewing time, measured over a 10-yr exposure period, and current UWS and grip strength in men and women from a British prospective cohort study.
METHODS
Participants and study setting
The European Prospective Investigation of Cancer (EPIC)—Norfolk study recruited community-based men and women age 40–74 yr from general practice registers in and around Norwich, United Kingdom. A baseline health examination was completed by 25,639 people (1HC, 1993–1997), and participants have attended two further health examinations (2HC, 1998–2000; 3HC, 2006–2011) and answered detailed health and lifestyle questionnaires. Descriptions of the study design, follow-up, and representativeness of the cohort have been published elsewhere (18). All participants gave a written informed consent, and the study was approved by the Norfolk Local Research Ethics Committee and the East Norfolk and Waveney National Health Service Research Governance Committee.
At the 3HC, 8623 participants (now age 48–92 yr) attended a central research clinic and underwent tests of muscle strength and physical performance.
TV viewing time
Participants answered a question on TV viewing behavior contained within a physical activity questionnaire (EPAQ2) (38) administered during the 3HC (2006–2007) and earlier during the 2HC (1998–2000). Only participants who had completed the EPAQ2 at the 2HC were resurveyed. Participants were asked to estimate the “hours of TV or video watched per day” and ticked the most appropriate response category (<1, 1–2, 2–3, 3–4, and >4 h·d−1) for a weekday before and after 6:00 p.m. and a weekend day before and after 6:00 p.m. Scores were summated and divided by seven to estimate daily TV viewing time.
Exactly the same question was asked at both time points, allowing TV viewing time during the 2HC and 3HC to be estimated and also an average of the two measures to be calculated, henceforth termed average TV viewing time. TV viewing time shows high repeatability (Cohen weighted kappa: men, 0.71; women, 0.74 (38)), is valid for ranking individuals with respect to objective physical activity measures (38), and has previously been independently associated with mortality (40) and incident cardiovascular diseases (39). TV viewing time at the 2HC and 3HC was highly correlated (Spearman rho: men, 0.72; women, 0.73), and average TV viewing time represented average exposure over the 10 yr preceding measurement of physical capability.
Physical capability measures
Measurements were made by trained research nurses, following standardized protocols (22). Grip strength was measured using a Smedley dynamometer (Scandidact, Kvistgaard, Denmark). Participants were allowed two trials with each hand, and the maximum strength (kg) recorded was used in analyses. The test was conducted, holding the dynamometer while standing or sitting if necessary, with the forearm held out in front.
UWS was estimated from the time taken to walk along a 4-m course using walking aids if necessary. Two timed walks were conducted, and the average time taken was used to estimate walking speed (cm·s−1).
Covariables
Total physical activity energy expenditure (PAEE) was measured using the EPAQ2 questionnaire, which asked about usual activity at home, work, during travel to and from work, and during leisure time over the past year. Time spent in each activity (h·wk−1) was multiplied the activity’s metabolic cost (MET), and scores were summated and divided by seven to represent average daily PAEE (38). Correlations between daily PAEE and TV viewing time were weak (Spearman rho: men = −0.16, P < 0.001; women = −0.15, P < 0.001).
Participants also completed a general health and lifestyle questionnaire (follow-up 4), which was mailed to participants with their 3HC invitation and asked, “Do you currently smoke cigarettes?” and “If you have stopped smoking, how old were you when you gave up?” In addition, the questionnaire asked, “In general, would you say you (and your family living with you) have enough money, just enough money, or not enough money?” Participants were categorized accordingly as current smokers, ex-smokers, or never smoked and those with more than enough, just enough, or not enough money. Participants also self-reported their alcohol consumption (units per week).
At the 3HC clinic appointment, weight was measured to the nearest 0.1 kg using digital scales (Tanita) and height was measured to the nearest 0.1 cm using a stadiometer (Chasmores, United Kingdom).
Comorbidity was estimated using information obtained since the study’s inception up to the 3HC visit. At baseline and during the 2HC, participants self-reported comorbidity. This information was combined with incident data over the follow-up period, captured through record linkage with hospital episode statistics, to estimate whether participants had ever experienced a stroke, cancer, diabetes and/or myocardial infarction. Comorbidity was included as a binary variable in analyses (yes/no).
Statistical analyses
Participants were described by category of average TV viewing time (<2, 2 < 3, 3 < 4, ≥4 h·d−1) using means (standard deviation [SD]), medians (interquartile range (IQR)), and frequencies (% (n)). Differences across TV time categories were evaluated using one-way ANOVA, Kruskal–Wallis, and chi-square tests.
Associations between average TV viewing time category and physical capability were explored using linear regression because grip strength and UWS were normally distributed. The highest category (≥4 h·d−1) was used as the referent category, so that regression coefficients (presented with 95% confidence intervals (CI)) represented the differences in UWS and maximum grip strength associated with less time spent watching TV. Analyses were repeated using TV viewing time measured at the 3HC and 2HC in separate models.
In addition, differences in physical capability per extra hour of average TV viewing time were evaluated.
Potential confounders were identified a priori from existing literature. All analyses were adjusted for age (model A). Subsequently, adjustments for comorbidity, alcohol intake, smoking status, current wealth, height, and weight (representing body size and composition) were made (model B). Lean mass and adiposity are important determinants of physical capability (16,29), and strong associations have been observed between TV viewing time and obesity (20). Adjustment was made for current wealth because socioeconomic position (SEP) is an important determinant of TV viewing time (32), but measures of SEP such as occupational social class and educational level are less consistently associated with muscle function than current wealth (26,34). Final models were also adjusted for PAEE to establish whether associations were independent of physical activity (model C).
Sex-specific analyses were performed first because TV viewing time has been associated differently with health outcomes in men compared with those in women (7,35), physical capability (particularly muscle strength) differs between sexes (22), and others have undertaken sex-stratified analyses (14). Analyses were combined if no sex–TV viewing time interactions were identified. Stata 12.0 was used for all analyses (StataCorp LP, College Station, TX).
Supplementary analyses
Associations between average TV viewing time and physical capability (grip strength and UWS) were evaluated after excluding those with comorbid disease at the 3HC.
Associations between average TV viewing time and timed chair stands (TCS) performance (time taken to perform five chair stands (s)) were also explored. This is a proxy measure for lower limb muscle strength, and 5368 participants with TV viewing time measurements were able to undertake this assessment (718 participants were unable to perform the test). The natural logarithm of TCS performance was used in analyses because the performance times were not normally distributed.
RESULTS
Of the 8623 participants who attended the 3HC, 6086 answered questions on TV viewing time. Those who did not were younger, more likely to be men, stronger (men), and heavier (see Table, Supplemental Digital Content 1, http://links.lww.com/MSS/A432, Men and women who attended the 3HC of EPIC Norfolk and had information on TV viewing time (measured at both 3HC and 2HC) compared with those who did not).
For those participants with TV viewing time, data were missing in some participants for height (n = 6), weight (n = 1), alcohol intake (n = 216), smoking status (n = 82), and current wealth (n = 329). Missing covariable data were more likely among women (P > 0.001), and those with missing data were older (men: 73.3 yr (SD, 7.8) vs 69.9 yr (SD, 8.1), P < 0.001; women: 70.4 yr (SD, 7.9) vs 68.2 yr (SD, 8.0), P < 0.001). A small number of participants without the relevant physical capability measurement were also excluded from respective analyses (grip strength, n = 102; UWS, n = 67).
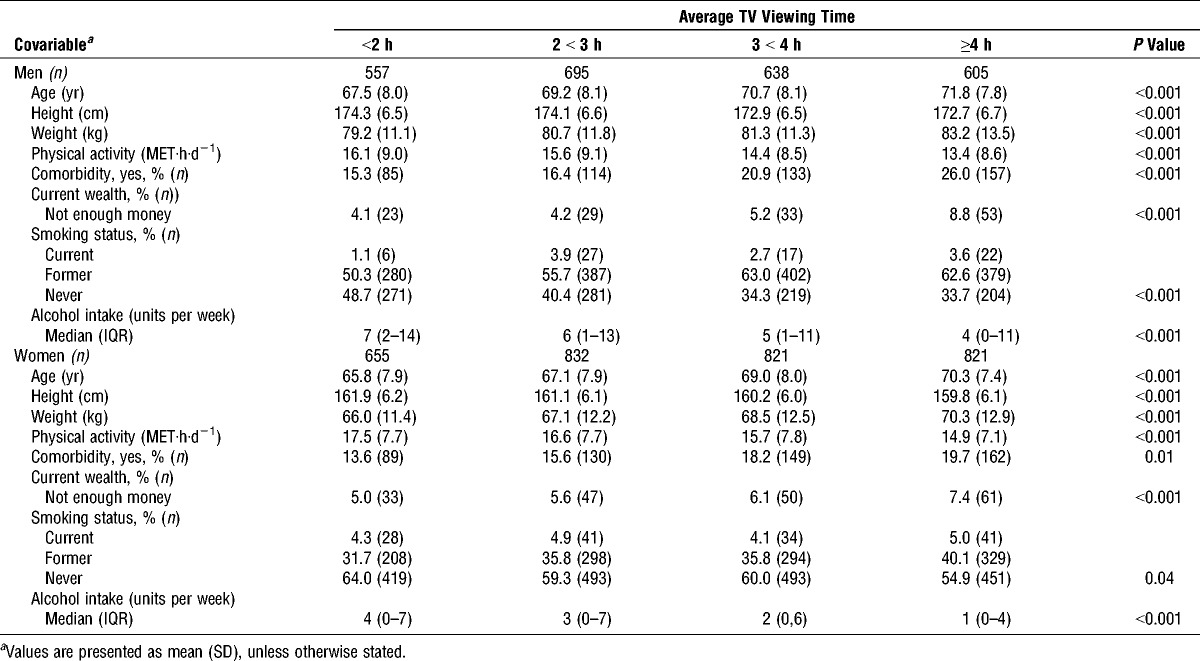
Men and women included in this study watched TV for 2.8 h·d−1 (SD, 1.3) and 2.9 h·d−1 (SD, 1.4), respectively, at the 2HC, 3.3 h·d−1 (SD, 1.5) and 3.4 h·d−1 (SD, 1.6) at the 3HC, and 3.0 h·d−1 (SD, 1.3) and 3.1 h·d−1 (SD, 1.4) on average over the 10-yr follow-up period. Those who watched more TV were older, heavier, smokers, less wealthy, consumed less alcohol, undertook less physical activity, and had greater comorbidity (Table 1).
TABLE 1.
The characteristics of men and women at the 3HC by average TV viewing time category.
UWS
Men and women who watched <2 h·d−1 of TV on average over the preceding 10 yr walked 4.09 and 4.34 cm·s−1 faster than those who watched for ≥4 h·d−1 (men: 95% CI, 1.45–6.74; women: 95% CI, 2.05–6.64), after multivariable adjustment (model C) (Table 2). There were significant trends across average TV viewing time categories, and every extra hour of average TV viewing time was associated with a decrease of 1.00 cm·s−1 and 1.44 cm·s−1 in UWS of men and women, respectively (men: 95% CI, 0.32–1.68; women, 95% CI, 0.87–2.02) (Table 3).
TABLE 2.
TV viewing time and UWS.
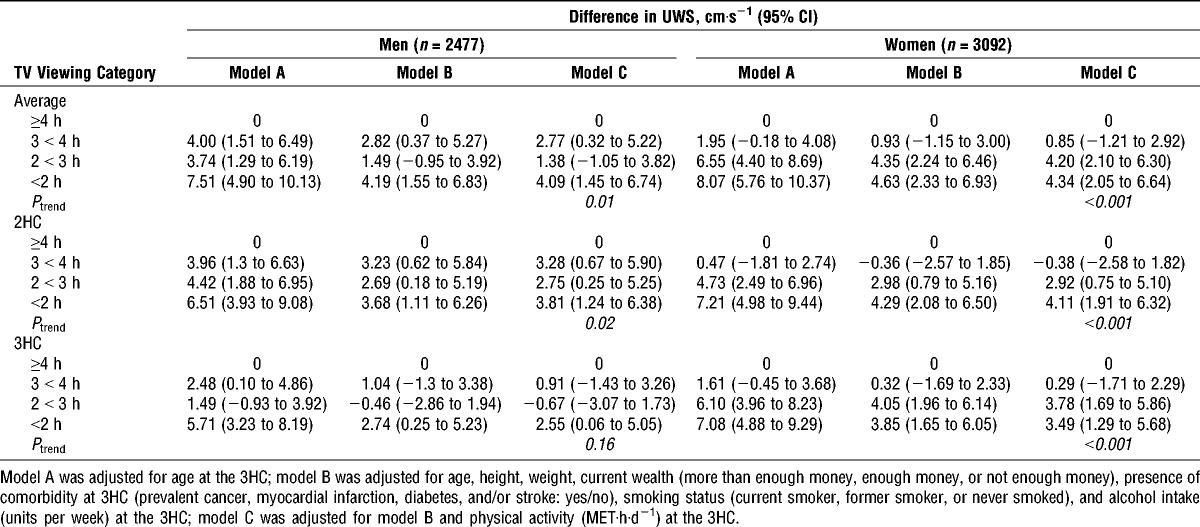
TABLE 3.
Differences in physical capability per extra hour of average daily TV viewing time.

There was no evidence of sex–TV viewing time interaction (P = 0.09) (Table 3). Therefore, men and women were considered together and UWS was 4.29 cm·s−1 faster (95% CI, 2.56–6.03) in participants who watched the least TV on average compared with that in participants who watched the most, after multivariable adjustment. A dose–response association was also evident (Ptrend < 0.001) (Fig. 1a).
FIGURE 1.
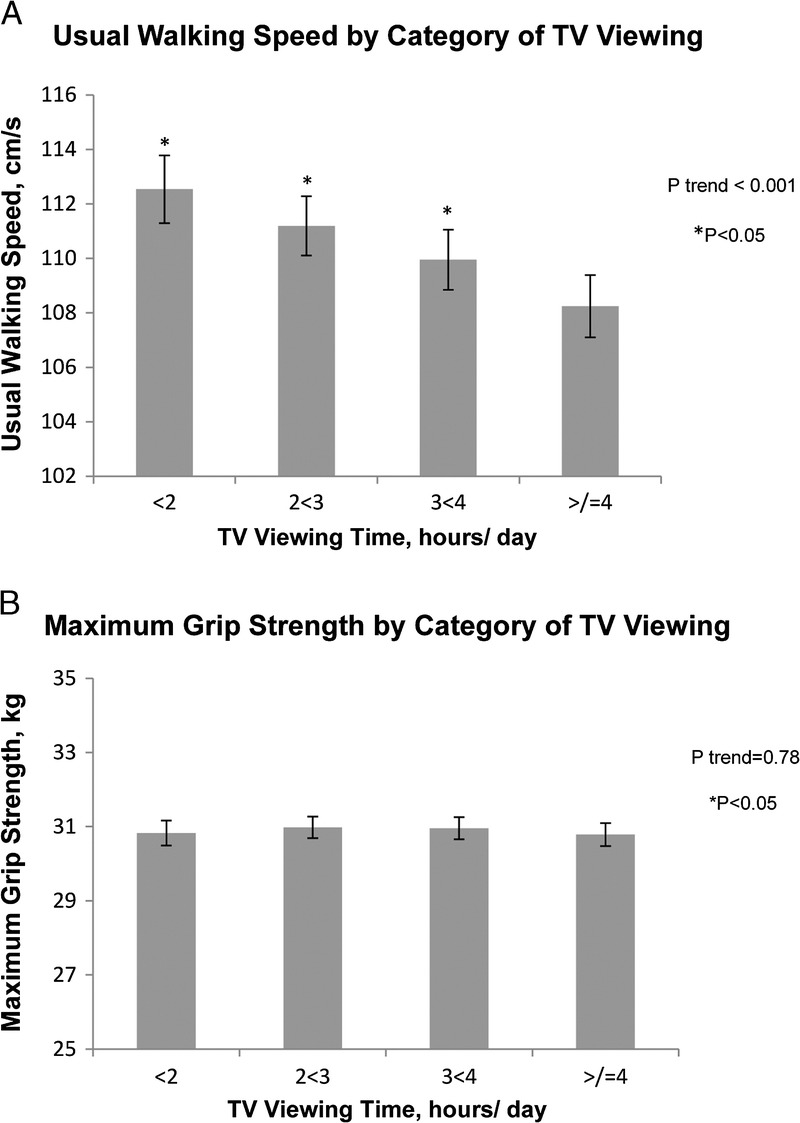
Mean UWS (A) and maximum grip strength (B) of participants by category of average TV viewing time over 10 yr of follow-up. Least square mean values were adjusted for sex, age, height, weight, physical activity (MET·h·d−1), current wealth (more than enough money, enough money, or not enough money), presence of comorbidity (prevalent cancer, myocardial infarction, diabetes, and/or stroke: yes/no), smoking status (current smoker, former smoker, or never smoked) and alcohol intake (units per week) at the 3HC. Bars indicate 95% CI.
Similar and consistent trends were seen between TV viewing time measured at either the 2HC or 3HC and UWS (Table 2).
Grip strength
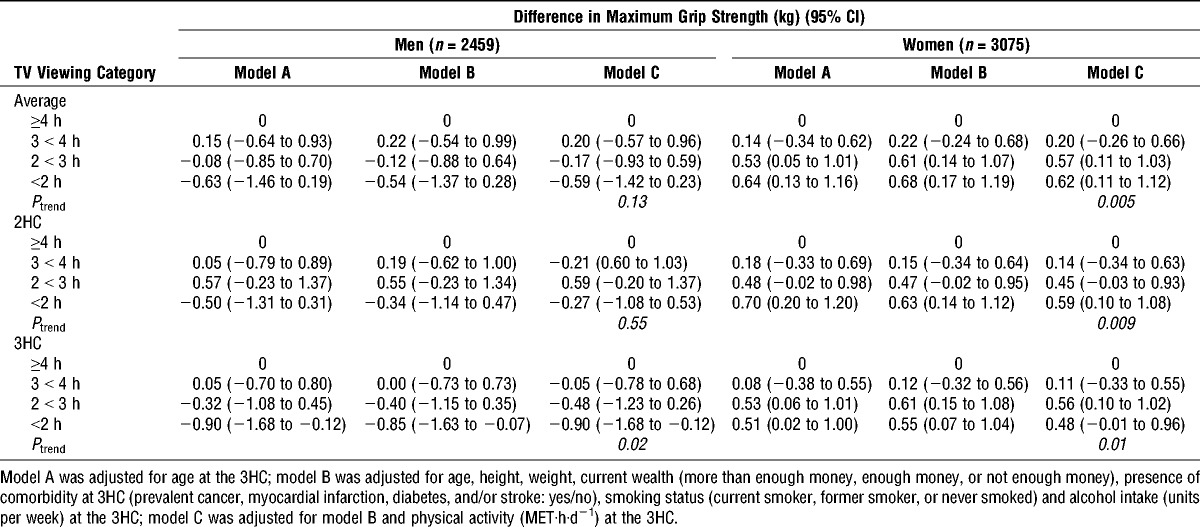
Average TV viewing time was not associated with grip strength in men, and only a weak association was observed in women (Tables 3 and 4). Women who watched TV for <2 h·d−1 on average were 0.62 kg stronger than those who watched for ≥4 h·d−1 (95% CI, 0.11–1.12), after multivariable adjustment (model C) (Table 4). There was significant trend across average TV viewing time categories, and for every extra hour of average TV viewing time, grip strength decreased by 0.21 kg (95% CI, 0.08–0.34) (Table 3).
TABLE 4.
TV viewing time and maximum grip strength.
Despite the suggestion of differences between sexes, there was no statistical evidence of interaction between sex and average TV viewing time (P = 0.28) (Table 3) and the differences in grip strength across TV viewing time categories in women were small. In analyses considering men and women together, no overall association was observed (Fig. 1b).
Similarly, there were no consistent or strong associations between grip strength and TV viewing time measured at either the 2HC or 3HC (Table 4).
Supplementary analyses
Associations between average TV viewing time and both UWS and grip strength were reexamined after excluding 1019 participants with at least one comorbid disease. The results did not change our conclusions. UWS was 4.76 cm·s−1 (95% CI, 2.85–6.68) faster in participants (n = 4566, both sexes combined) who watched the least TV on average over the previous 10 yr compared with that in participants who watched the most, with linear increase in UWS associated with decreasing TV viewing time (Ptrend < 0.001). No associations with grip strength were observed (n = 4531, both sexes combined; Ptrend = 0.97).
No associations between TCS and average TV viewing time were observed (see Table, Supplemental Digital Content 2, http://links.lww.com/MSS/A433, Difference in TCS performance (%) by category of average TV viewing time (measured using the EPAQ2 administered during the 2HC and 3HC)).
DISCUSSION
TV watching is the most prevalent sedentary leisure time activity in the United Kingdom, with approximately one in three adults watching ≥4 h·d−1 (19). Associations between more time spent watching TV and several health outcomes such as obesity, the metabolic syndrome, diabetes, and mortality have been established (15). This has made sedentary behaviors such as TV viewing an attractive potential target for public health intervention, and the feasibility of reducing sedentary time in older adults, in whom TV viewing is even more prevalent (19) is already being tested (11).
However, few studies have considered the effect of sedentary behaviors, such as TV viewing, on physical capability despite the importance of maintaining physical functional health in later life. We observed that community-based older adults who spend the least time watching TV walk at a faster usual pace than those who watch the most TV. This association was observed in both men and women, with no evidence of effect modification by sex. Importantly, this association persisted when TV viewing time was measured 10 yr before UWS and after accounting for a range of covariables, including physical activity. Men and women who watched on average the least TV over the 10-yr exposure period walked 4 cm·s−1 faster than those who watched the most TV. This equates to 4-yr difference in age, on the basis of cross-sectional associations of UWS with age (22), and is likely to represent meaningful difference in functional health (24) particularly because walking speed has been proposed as the “sixth vital sign” of health (10).
Aging skeletal muscles are characterized by reduced myofiber numbers, size, and contractile function. Mechanisms driving these changes are likely to be multifactorial in origin (25), but sedentary behavior could play a part. The expressions of proteins involved in ubiquitin–proteasome pathways, which promote proteolysis and skeletal muscle cell atrophy, are up-regulated in rat models of sedentariness (13). In addition, time spent sitting or lying down is the only state associated with absence of muscle contractile activity (15), and other physiological consequences on muscle metabolism, distinct from the effects of exercise, have been identified (1). Thus, although we cannot conclusively establish causality, it is possible that sedentary behavior could affect muscle function.
However, strong and consistent associations between grip strength and TV viewing time were not observed. Isometric muscle strength encapsulates only one aspect of muscle function, and low performance may be present without low strength or vice versa, a concept acknowledged in working definitions of muscle conditions such as sarcopenia (5). In addition, limitations with our exposure measure and/or measure of muscle strength may have precluded associations being found. We could not evaluate associations between muscle strength and either the total amount of sedentary time or the pattern of sedentary behavior (e.g., fragmented vs continuous), which may be an important factor (3). In addition, differences in grip strength may not completely represent the variation in strength of other muscle groups, e.g., quadriceps, which may be more important for functional performance (37). We did consider associations between TV viewing time and TCS performance, a proxy measure for lower limb muscle strength, but again found no association. However, the least physically capable were unable to take part in the TCS test, truncating the range of performance captured, and it is not a direct measure of lower limb strength.
It should also be considered that TV viewing time does represent global sedentary behavior (33) and may be a marker of parameters other than “sitting.” For example, TV watching may lead to unhealthier eating patterns (17) and TV viewing time is also highly correlated to many socioeconomic factors (SEP) (32). Although we were able to adjust for many confounding factors, residual confounding could still be important and others have suggested this as an explanation for associations between TV watching and health. For example, Hamer and Stamatakis (14) found different associations between grip strength and measures of sedentary behavior, depending on the context within which the “sedentariness” occurred. Internet usage (yes/no) was associated with stronger grip strength but more time spent watching TV with weaker grip strength, potentially indicating different confounding structures for both types of sedentary behavior. However, this measure of internet usage did not quantify the time spent in this activity, which could limit its usefulness as a marker of sedentariness.
Our study was limited by missing data for TV viewing time, and those participants without TV viewing time were comparatively younger and heavier with stronger grip strength (in men). This presents an unusual picture, with predictors of “missingness” including factors associated with good health. This is likely due to the contribution of a study design factor to the missing data. Several thousand participants who had decided not to take part in the 2HC but wished to remain in the study were invited to the 3HC. These participants had not completed the EPAQ2 administered during the 2HC and were additionally not resurveyed. It is difficult to anticipate the bias introduced by missing data, and our results must be considered in light of this limitation.
Our study had several strengths. Data were available for a large number of men and women from a wide age group who had been well characterized. In addition, the prospective design allowed measurement of the exposure at repeated intervals including 10 yr before assessment of physical capability. This reduces, although does not eliminate, concern over reverse causality because it is unlikely that current physical function could predict TV viewing behavior 10 yr earlier.
CONCLUSIONS
TV viewing time was prospectively associated with UWS, a proposed vital sign of functional health, in community-based older adults. These findings may have a significant effect on public health policy (6). Other studies with prospective measures of total sitting time, or objective measures that allow estimation of the pattern of sedentary behavior, should further investigate relations between sedentariness and physical capability.
Supplementary Material
Acknowledgments
V. L. K. declares a Wellcome Trust clinical training fellowship (092077/Z/10/Z), and K. W., a British Heart Foundation intermediate basic science research fellowship (FS/12/58/29709). The EPIC–Norfolk study was supported by program grants from the Medical Research Council (G9502233, G0401527) and Cancer Research UK (C864/A8257). A grant from Research into Ageing (262) funded the 3HC clinic.
We would like to thank the participants, general practitioners and the many administrative and research staff who make the EPIC-Norfolk study possible.
V. L. K. analyzed and interpreted the data and drafted the manuscript with contributions from K.W., K.T.K., and A.A.S.K.T.K., N.J.W., and R.L. contributed to study concepts and design, and K. T. K., N. J. W., and R. L. contributed to participant recruitment, data collection, and management.
For the remaining authors, no conflicts of interest were declared.
The results of the present study do not constitute endorsement by the American College of Sports Medicine.
Footnotes
Supplemental digital content is available for this article. Direct URL citations appear in the printed text and are provided in the HTML and PDF versions of this article on the journal’s Web site (www.acsm-msse.org).
REFERENCES
- 1. Bey L, Hamilton MT. Suppression of skeletal muscle lipoprotein lipase activity during physical inactivity: a molecular reason to maintain daily low-intensity activity. J Physiol. 2003; 551 (Pt 2): 673– 82. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2. Buman MP, Hekler EB, Haskell WL, et al. Objective light-intensity physical activity associations with rated health in older adults. Am J Epidemiol. 2010; 172 (10): 1155– 65. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3. Chastin SFM, Ferriolli E, Stephens NA, Fearon KCH, Greig C. Relationship between sedentary behaviour, physical activity, muscle quality and body composition in healthy older adults. Age Ageing. 2012; 41 (1): 111– 4. [DOI] [PubMed] [Google Scholar]
- 4. Craft LL, Zderic TW, Gapstur SM, et al. Evidence that women meeting physical activity guidelines do not sit less: an observational inclinometry study. Int J Behav Nutr Phys Act. 2012; 9: 122. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5. Cruz-Jentoft AJ, Baeyens JP, Bauer JM, et al. Sarcopenia: European consensus on definition and diagnosis: report of the European Working Group on Sarcopenia in Older People. Age Ageing. 2010; 39 (4): 412– 23. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Department of Health. Start Active, Stay Active: A Report on Physical Activity from the Four Home Countries’ Chief Medical Officers. 2011. Available from: http://www.dh.gov.uk/en/Publicationsandstatistics/Publications/PublicationsPolicyAndGuidance/DH_128209. [Google Scholar]
- 7. Dunstan DW, Salmon J, Healy GN, et al. Association of television viewing with fasting and 2-h postchallenge plasma glucose levels in adults without diagnosed diabetes. Diabetes Care. 2007; 30 (3): 516– 22. [DOI] [PubMed] [Google Scholar]
- 8. Fielding RA, Vellas B, Evans WJ, et al. Sarcopenia: an undiagnosed condition in older adults. Current consensus definition: prevalence, etiology, and consequences. International Working Group on Sarcopenia. J Am Med Dir Assoc. 2011; 12 (4): 249– 56. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9. Fried LP, Tangen CM, Walston J, et al. Frailty in older adults: evidence for a phenotype. J Gerontol A Biol Sci Med Sci. 2001; 56 (3): M146– 56. [DOI] [PubMed] [Google Scholar]
- 10. Fritz S, Lusardi M. White paper: “walking speed: the sixth vital sign”. J Geriatr Phys Ther. 2009; 32 (2): 46– 9. [PubMed] [Google Scholar]
- 11. Gardiner PA, Eakin EG, Healy GN, Owen N. Feasibility of reducing older adults’ sedentary time. Am J Prev Med. 2011; 41 (2): 174– 7. [DOI] [PubMed] [Google Scholar]
- 12. Gennuso KP, Gangnon RE, Matthews CE, Thraen-Borowski KM, Colbert LH. Sedentary behavior, physical activity, and markers of health in older adults. Med Sci Sports Exerc. 2013; 45 (8): 1493– 500. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13. Glass DJ. Skeletal muscle hypertrophy and atrophy signaling pathways. Int J Biochem Cell Biol. 2005; 37 (10): 1974– 84. [DOI] [PubMed] [Google Scholar]
- 14. Hamer M, Stamatakis E. Screen-based sedentary behavior, physical activity, and muscle strength in the English longitudinal study of ageing. PLoS One. 2013; 8 (6): e66222. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15. Hamilton MT, Hamilton DG, Zderic TW. Role of low energy expenditure and sitting in obesity, metabolic syndrome, type 2 diabetes, and cardiovascular disease. Diabetes. 2007; 56 (11): 2655– 67. [DOI] [PubMed] [Google Scholar]
- 16. Hardy R, Cooper R, Aihie Sayer A, et al. Body mass index, muscle strength and physical performance in older adults from eight cohort studies: the HALCyon programme. PLoS One. 2013; 8 (2): e56483. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17. Harris JL, Bargh J a, Brownell KD. Priming effects of television food advertising on eating behavior. Health Psychol. 2009; 28 (4): 404– 13. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18. Hayat SA, Luben R, Keevil VL, et al. Cohort profile: a prospective cohort study of objective physical and cognitive capability and visual health in an ageing population of men and women in Norfolk (EPIC-Norfolk 3). Int J Epidemiol. 2013; 1– 10. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19. Health and Social Care Information Center. Health Survey for England 2008. Volume 1: Physical Activity and Fitness. Leeds (United Kingdom): The NHS Information Centre for Health and Social Care; 2009. [Google Scholar]
- 20. Jakes RW, Day NE, Khaw KT, et al. Television viewing and low participation in vigorous recreation are independently associated with obesity and markers of cardiovascular disease risk: EPIC-Norfolk population-based study. Eur J Clin Nutr. 2003; 57 (9): 1089– 96. [DOI] [PubMed] [Google Scholar]
- 21. Katzmarzyk PT, Church TS, Craig CL, Bouchard C. Sitting time and mortality from all causes, cardiovascular disease, and cancer. Med Sci Sports Exerc. 2009; 41 (5): 998– 1005. [DOI] [PubMed] [Google Scholar]
- 22. Keevil VL, Hayat S, Dalzell N, et al. The physical capability of community-based men and women from a British cohort: the European Prospective Investigation into Cancer (EPIC)-Norfolk study. BMC Geriatr. 2013; 13 (1): 93. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23. Kortebein P, Symons TB, Ferrando A, et al. Functional impact of 10 days of bed rest in healthy older adults. J Gerontol A Biol Sci Med Sci. 2008; 63 (10): 1076– 81. [DOI] [PubMed] [Google Scholar]
- 24. Kwon S, Perera S, Pahor M, et al. What is a meaningful change in physical performance? Findings from a clinical trial in older adults (the LIFE-P study). J Nutr Health Aging. 2009; 13 (6): 538– 44. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25. Matthews GDK, Huang CLH, Sun L, Zaidi M. Translational musculoskeletal science: is sarcopenia the next clinical target after osteoporosis? Ann N Y Acad Sci. 2011; 1237: 95– 105. [DOI] [PubMed] [Google Scholar]
- 26. Mohd Hairi F, Mackenbach JP, Andersen-Ranberg K, Avendano M. Does socio-economic status predict grip strength in older Europeans? Results from the SHARE study in non-institutionalised men and women aged 50+. J Epidemiol Community Health. 2010; 64 (9): 829– 37. [DOI] [PubMed] [Google Scholar]
- 27. Peterson MD, Rhea MR, Sen A, Gordon PM. Resistance exercise for muscular strength in older adults: a meta-analysis. Ageing Res Rev. 2010; 9 (3): 226– 37. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28. Santos DA, Silva AM, Baptista F, et al. Sedentary behavior and physical activity are independently related to functional fitness in older adults. Exp Gerontol. 2012; 47 (12): 908– 12. [DOI] [PubMed] [Google Scholar]
- 29. Sayer AA, Syddall HE, Dennison EM, et al. Grip strength and the metabolic syndrome: findings from the Hertfordshire Cohort Study. QJM. 2007; 100 (11): 707– 13. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Sedentary Behaviour Research Network: Standardized use of the terms “sedentary” and “sedentary behaviours”. Appl Physiol Nutr Metab. 2012; 37: 540– 2. [DOI] [PubMed] [Google Scholar]
- 31. Seguin R, Lamonte M, Tinker L, et al. Sedentary behavior and physical function decline in older women: findings from the Women’s Health Initiative. J Aging Res. 2012;2012:271589. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32. Stamatakis E, Hillsdon M, Mishra G, Hamer M, Marmot M. Television viewing and other screen-based entertainment in relation to multiple socioeconomic status indicators and area deprivation: the Scottish Health Survey 2003. J Epidemiol Community Health. 2009; 63 (9): 734– 40. [DOI] [PubMed] [Google Scholar]
- 33. Sugiyama T, Healy GN, Dunstan DW, Salmon J, Owen N. Is television viewing time a marker of a broader pattern of sedentary behavior? Ann Behav Med. 2008; 35 (2): 245– 50. [DOI] [PubMed] [Google Scholar]
- 34. Syddall H, Evandrou M, Cooper C, Sayer AA. Social inequalities in grip strength, physical function, and falls among community dwelling older men and women: findings from the Hertfordshire Cohort Study. J Aging Health. 2009; 21 (6): 913– 39. [DOI] [PubMed] [Google Scholar]
- 35. Thorp AA, Healy GN, Owen N, et al. Deleterious associations of sitting time and television viewing time with cardiometabolic risk biomarkers: Australian Diabetes, Obesity and Lifestyle (AusDiab) study 2004–2005. Diabetes Care. 2010; 33 (2): 327– 34. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36. Tremblay MS, Colley RC, Saunders TJ, Healy GN, Owen N. Physiological and health implications of a sedentary lifestyle. Appl Physiol Nutr Metab. 2010; 35 (6): 725– 40. [DOI] [PubMed] [Google Scholar]
- 37. Vittasalo JT, Era P, Leskinen A-L, Heikkinen E. Muscular strength profiles and anthropometry in random samples of men aged 31–35, 51–55 and 71–75 years. Ergonomics. 1985; 28 (11): 1563– 74. [Google Scholar]
- 38. Wareham NJ, Jakes RW, Rennie KL, Mitchell J, Hennings S, Day NE. Validity and repeatability of the EPIC-Norfolk Physical Activity Questionnaire. Int J Epidemiol. 2002; 31 (1): 168– 74. [DOI] [PubMed] [Google Scholar]
- 39. Wijndaele K, Brage S, Besson H, et al. Television viewing and incident cardiovascular disease: prospective associations and mediation analysis in the EPIC Norfolk Study. PLoS One. 2011; 6 (5): e20058. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40. Wijndaele K, Brage S, Besson H, et al. Television viewing time independently predicts all-cause and cardiovascular mortality: the EPIC Norfolk study. Int J Epidemiol. 2011; 40 (1): 150– 9. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.