

Abstract
Aim:
The aim of the current study was to compare the effect of WaveOne and Reciproc files in reciprocation versus reverse full rotation movements on cervical dentin thickness by virtue of cone beam computed tomography (CBCT) analysis in curved mesial canals of mandibular first molars.
Methods:
Mesiobuccal canals of 60 mandibular molars were randomly divided into 4 groups (n = 15): Group 1; WaveOne/Reciprocation, Group 2; WaveOne/Full-Rotation, Group 3; Reciproc/Reciprocation, and Group 4; Reciproc/Full-Rotation. Pre- and post-instrumented CBCT scans were prepared for assessment of cervical dentin thickness changes (2 mm, 4 mm below the highest point of the root furcation) in both groups. Data statistically analyzed using two-way ANOVA test.
Results:
There was no statistically significant difference between four experimental groups in terms of remaining dentin thickness at 2 and 4 mm levels below the highest point of the furcation (P > 0.05). No separation of instruments occurred in any group.
Conclusion:
WaveOne and Reciproc files with two different motions have similar effects on cervical of root canals in terms of dentin thickness changes.
Keywords: Cervical dentin, full-rotation, Reciproc, WaveOne
Background
Furcal side of the root canal wall in mandibular molars (danger zone [DZ]) has the least thickness among the root canal walls and therefore is highly vulnerable to iatrogenic accidents such as root fracture and strip perforation caused by the aggressive removal of dentin.[1] When curvatures are present, endodontic preparation becomes more difficult, and all available preparation techniques have the tendency to deviate the prepared canal away from the original shape.[2] Therefore, using suitable instruments with the least danger for high-risk areas such as DZ is necessary to preserve the original canal shape especially in curved root canals.
To preserve root canal curvatures, “balanced forced technique” was proposed by Roane et al. in 1985.[3] Reciprocal action is specifically designed to work in a similar manner but in a reverse balanced force motion. Reciprocal movement is a limited rotational movement in clockwise (CW) and counter clockwise (CCW) direction with the aim of reducing torsional stress and therefore fracture of the files.[4] A large rotating angle in the CCW motion causes the instrument advances in the canal and engages dentin to cut it (because of the direction of the spiraling flutes), whereas a smaller rotation angle in the CW motion allows immediate file disengagement and its safely moving along the canal path.[5] The term reciprocating motion includes several possible back and forth angles of movement, each of which may impact the performance and resistance to failure of nickel-titanium instruments. The actual movements and angles for the newest commercially available single-file instruments (Reciproc and WaveOne) are not clearly disclosed by manufacturers, and there is no evidence that the reciprocating motion suggested by manufacturers is the best choice in terms of preserving DZ. Another point to be considered is a different rheological feature of these two newly marketed single files. The result of one study showed that WaveOne file had more fatigue resistance than Twisted file and Protaper Universal files; this could justify its application in full rotational movements.[6] Another reason for applying reverse full rotation movement for WaveOne and the Reciproc files in this study was the expense of specific reciprocating motors suggested by manufacturers for WaveOne and Reciproc files; we assumed that if reverse full rotation motion has acceptable effects on DZ, instead of expensive specific reciprocating motors we could apply these single-files with any conventional or smart motors that are usually adjustable for reverse full rotation motion.
Furthermore, previous literature indicated that root canal preparation with both rotary and reciprocating instruments resulted in dentinal defects. At the apical level of the canals, using WaveOne and Reciproc with reciprocating motion produced significantly more incomplete dentinal cracks than full-sequence rotary systems.[7] Therefore, we intend to propose the idea of applying WaveOne and Reciproc in reverse full rotation motion and investigating its effects on root canals.
To the best of our knowledge, there exist few data in literature regarding using WaveOne and Reciproc single files in reverse full rotation motion and investigating its effect on cervical dentin thickness.[8] Therefore, the current study was designed to compare the effect of the type of instrument (WaveOne versus Reciproc) and motion (reciprocating versus full rotation) on remaining dentin thickness of canal walls after preparation with WaveOne and Reciproc single files using cone beam computed tomography (CBCT) imaging system.
Procedures
In this in vitro experimental study, sixty mesiobuccal canals from mandibular first molars were selected. Immediately after extraction, all soft tissues and calculus were removed mechanically from the teeth, and all the teeth were radiographed to verify the presence of mature apex and absence of any resorption, calcification, or endodontic obturation. A size 15 K-file (Dentsply, Maillefer, Switzerland) was inserted into the embedded teeth with anti-curvature movements before applying the rotary instruments to verify the orientation of the canal axis and the absence of obstructions or ledge. The specimen was excluded from the study in case of any obstructions or ledge.
The teeth were decontaminated by immersion in 5.25% sodium hypochlorite (Golrang, Pakshoo Co., Tehran, Iran) for 30 min. Teeth were then stored in sterile normal saline 0.9% (Samen Co., Tehran, Iran) at room temperature. The storage time of all teeth was <2 months before the experiment initiation.
Digital periapical radiographs (Dr Suni, Apteryx Inc., USA) were taken from each tooth from buccal and proximal aspects (mesial and distal) to determine the radius and degree of curvature of the canals. Canals with completely formed apices and severe angles of curvature (20-45°) were selected. The degree of the curvature was standardized as described by Schneider.[9] The roots were mounted using a polyvinyl siloxane impression material (Speedex; Coltene AG, Alstatten, Switzerland) on a custom-made mounting jig (2 cm × 6 cm × 6 cm) which served as a stable guide to reinsert the samples. Dimensions of the jig corresponded to the exposure field of the New Tom VG 9000 CBCT machine (NewTom VGI, QR Verona, Italy). The coronal portions of the teeth were embedded in polyvinyl siloxane impression material, leaving the roots-oriented upward and the access opening facing down and the highest point of the furcation area was determined as the reference point using a guiding radiopaque pin. To compare dentin thickness changes in the cervical third of the roots, three-dimensional CBCT images were acquired before and after instrumentation. CBCT images were performed from cross-sections located 2 and 4 mm below reference point. The sections were 0.5 mm thick from apical to the canal orifice. The beginning and the end point of the scanning (on the z axis) were recorded to allow repeated scanning of the specimen at the same horizontal levels.
The crowns of the teeth were not removed to resemble the clinical endodontic practice, in which the interference of cervical dentin projections creates tensions on the files during root canal instrumentation. The teeth were randomly allocated into four identical groups of 15 teeth and WaveOne primary (tip size 25 with a taper of 0.08) was used in each group as below: Group 1; WaveOne in reciprocation movement and group 2; WaveOne in continuous reverse rotation, group 3; Reciproc R25 in reciprocation movement and group 4; Reciproc R25 in continuous reverse rotation. Reciproc R25 file and the WaveOne primary reciprocating file were selected for this investigation. This was done in accordance with the recommendations of the manufacturers as these sizes are designated for narrow and curved canals.
The working length was determined by measuring the length of the size 15 K-File at the apical foramen minus 1 mm. Glide path was prepared using 15 K-file in both groups. Each canal was shaped by reciprocating files until reaching full working length, using 5.25% NaOCl as lubricating agent. Teeth were prepared using endodontic engine X-Smart Plus Endo Motor (Dentsply, Maillefer, Switzerland) which was adjusted on WaveOne coupled with 16:1 contra angle. According to the manufacturer's instructions, WaveOne file was used in a reciprocating, slow in-and-out pecking motion in group 1. The flutes of the instrument were cleaned after three pecks. Each file was used to prepare 4 canals and the preparation time was recorded.
In group 2, teeth were instrumented using the WaveOne file in continuous rotation by means of X-Smart Plus Endo Motor.
Reciproc file was applied in preparing canals using X-Smart Plus Endo Motor adjusted on reciprocating motion for group 3 and reverse full rotation for group 4; the speed of rotation was 300 rpm, and the torque limit was 5 N.cm in both groups, and the motor was set on reverse action in group 4. For all groups during and after the use of each file, canals were irrigated with 5 mL of a 5.25% NaOCl solution using a 10 cc 30-gauge needle (Monoject; Sherwood Medical, St. Louis, MO).
The specimens were then replaced at the same position on the jig and then were scanned under the same conditions as the initial scans (axial thickness = 0.100, mA = 29.39, kVp = 110, exposure time = 5.4 s, voxel size = 0.1 mm and FOV = 6 cm × 6 cm, Denture Scan mode). The assessment of scans was performed by the software NNT viewer software version 3.00 (Newtom 5G, QR Verona, Italy). The images were aligned, observing the axial vision, through the rotation tool. MPR Screen was utilized for measuring. The “zoom” tool was applied to have a better visualization of the teeth. The vertical and horizontal bars were used as a reference for alignment of the images. The tool “distance”(on coronal section) was employed to determine the measure from the highest point of the furcation area up to 2 and 4 mm apically. Then the horizontal bar was adjusted 2 and 4 mm from furcation area, to have a view of the image in the axial section. Canal wall thickness was measured within the axial plane at two determined locations (slice levels). To evaluate the dentin thickness changes, the shortest distance from the inner canal wall to the corresponding outer wall of the canal (mesial and distal) in uninstrumented and instrumented canals were measured in both safety and DZ of the aforementioned sections [Figure 1]. Mesiolingual uninstrumented canals were used as control group to show the technique is satisfactory. A control group with CBCT before instrumentation and after establishing the gliding path could show the efficacy of CBCT for assessing the amount of reduction of dentin in experimental groups. The diameter of DZ in control group did not change.
Figure 1.
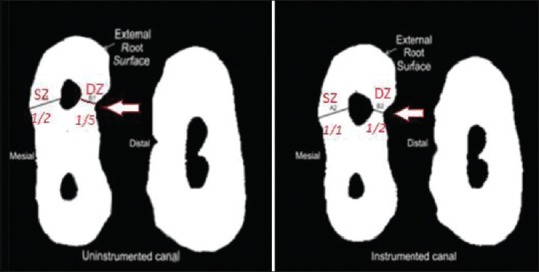
Dentin thickness measured in danger zone and safety zone in cone beam computed tomography images obtained before (left picture) and after (right picture) canal preparation
Two-way ANOVA test was conducted to explore a significant difference in the mean degree of dentin thickness changes between the 2 shaping motions (reciprocating and reverse full rotation), and the t-test for paired samples was used for the comparison between groups (P < 0.05).
Results
The results obtained from comparing the CBCT scans before and after instrumentation with WaveOne and Reciproc files showed that remaining dentin thickness between two experimented files (WaveOne versus Reciproc) and in both instrumentation techniques for each file (reciprocating versus full rotation movement) were not significantly different in two sections (2 and 4 mm apical to the furcation highest point) both in danger and safety zone (P > 0.05) [Figures 2 and 3]. No instrument fracture was reported in this study.
Figure 2.

Interval plot for dentin thickness changes parameter in danger zone in 4 mm (a) and 2 mm. (b) of furcation using different movements; 95% confidence intervals for the mean
Figure 3.

Interval plot for dentin thickness changes parameter in safety zone in 4 mm (a) and 2 mm (b) of furcation using different movements; 95% confidence intervals for the mean
Discussion
In the current study, dentin thickness changes of DZ in mandibular first molar canals was evaluated using WaveOne and Reciproc single files in two different motions (reciprocation versus reverse full rotation), and the result showed that type of instrument and motion in preparing canals have no effect on remaining dentin thickness. In the present study, dentin thickness was measured in 2 and 4 mm below the highest point of the furcation before and after canal preparations because distal wall of mandibular mesial canals (DZ) has the least thickness of dentin.[10] Furcation was chosen for the reference point in this study because this area of the canal is more vulnerable to iatrogenic accidents such as strip perforation.[1] In the current study, remaining dentin thickness after preparation with two different motions did not show any difference in 2 and 4 mm levels. Considering these observations and lack of relevant research in literature concerning application of WaveOne and Reciproc in reverse full rotation motion with the limitations of this study, we reached to the conclusion that in terms of preserving DZ, WaveOne and Reciproc single files can be used with reciprocation smart motors or any commonly used endodontic motors that can be adjusted in reverse full rotation mode. In a study by Kessler et al. in 1983 the distance between canal wall and root surface was measured only once after root canal preparation, so there was no reliable basis for comparing dentin thickness changes before and after preparation[11] whereas in our study, dentin thickness of canal wall was measured before and after preparation to evaluate changes accurately. WaveOne and Reciproc are two specifically designed single files commonly used in reciprocating motion, so this study was conducted to evaluate the effect of motion (reciprocation versus reverse full rotation) on cervical dentin thickness. The reason for adopting full rotation motion was the introduction of newly marketed single file named OneShape by Micro Mega Company which works in full rotation motion. In case of the efficacy of full rotation movement of WaveOne and Reciproc in clockwise or counter clockwise direction (dependant on the cutting direction of each file flutes), these files can be applied with commonly used motors, and there is no need to prepare specific expensive motors for reciprocating movement.
In a study by Dhingra et al. in 2015 with the aim of comparing the effect of two single file systems OneShape and WaveOne on dentin thickness of different canal areas in mesiobuccal canals of mandibular first molars the results demonstrated that dentin removal during preparation in OneShape with full rotation movement was less than WaveOne with reciprocating movement. According to the results of this study, OneShape is preferred to WaveOne in terms of preserving dentin in DZ and preventing accidents such as strip perforation.[12] This difference can be attributed to different file taper of WaveOne and OneShape. This result is in contrast (somehow different result) with our study because we observed no difference in dentin thickness in two different motions.
In a study in 2015 dentin thickness changes of mandibular first molars in cervical of root canals prepared by WaveOne, OneShape, and Reciproc files were compared. In this research dentin removal in OneShape (with full rotation motion) in all areas of canal was more than WaveOne and Reciproc (with reciprocating motion), but there was no statistically difference between WaveOne and Reciproc. The result of this study showed that dentin removal of DZ in full rotation movement is more than reciprocating movement.[13] This result is unlike current study because in our study the type of file movement during canal preparation (reverse full rotation or reciprocation) has no effect on dentin thickness changes. This controversy can be attributed to using different files with different features.
In a study conducted by Paque et al. in 2011 on mesial canals of mandibular first molars, single file preparation technique with ProTaper F2 in reciprocation motion was similar to rotary technique in full sequence motion in terms of dentin removal and the type of file movement has no effect on remaining dentin volume.[14] This result was similar to our study because in our study remaining dentin thickness in two different motions was similar.
In a study by You et al. in 2011 canal volume was assessed after using ProTaper F2 in buccal canals of maxillary molars with 20°–45° curvature in two different movements (full rotation and reciprocation). The comparison of canal volume changes in micro-computed tomography (CT) before and after canal preparation revealed no difference between two groups.[15] This observations can be attributed to applying the same file in two groups that cause the elimination of interfering factors such as different file tapering, cross-section shape, and tip size on the result.
In a study by Kim et al. the effect of two single files (ProTaper F2 and WaveOne Primary) with reciprocating motion on canal volume and surface area of curved root canals was the same in comparing before and after micro-CT scans.[16] Using micro-CT provides more scans with higher resolution than CBCT. We applied CBCT scans to compare canal dentin changes. Although CBCT has a less spatial resolution that could be troublesome while enhancing images,[17] it provided sufficient data in comparing dentin thickness changes before and after canal preparation.
In some studies, simulated canals in resin blocks were applied to evaluate cleaning and shaping effects of files in canal preparation. Simulated resin canals have the advantage of standardization and calibration of canal size, shape, taper, degree and radius of curvature so that the effect of other interfering factors was eliminated. On the other hand, simulated root canals cannot resemble clinical conditions in natural teeth because resin is different from dentin in terms of physical properties and hardness.[18] Another disadvantage of resin canals is softening of resin due to heat generation that attaches to file and cause file flexure and fracture.[19] Therefore, the present study was conducted on human extracted teeth to simulate real clinical conditions. Crown of the extracted teeth was not removed so that the effect of access cavity on canal preparation was not overlooked. Even though there are considerable variables between natural teeth efforts were made to obtain anatomically comparable groups. Therefore, the teeth in all groups were balanced with respect to the apical diameter and the canal length, degree and radius of curvature.
In 2012 Berutti et al. reported that WaveOne Primary file maintains the basic canal shape more effectively than full sequence ProTaper and attributed this observation to reciprocating movement of WaveOne single file.[20] This result is in contrast with our study. One justification for this difference could be related to usage of resin blocks in Berutti study rather than natural teeth in ours.
Nowadays, single file techniques such as OneShape have been introduced to market that is used with full rotation sequence so that they can be used with any motor capable of being adjusted in full rotation motion. In a study by Saber et al. in 2015, the shaping ability of WaveOne, Reciproc and OneShape single-file systems in 60 mandibular molars with mesiobuccal canals with severely curvature were evaluated. They concluded that all instruments were safe to use. Reciproc and Wave-One instruments respected the original canal curvature better than OneShape files, but the clinical relevance of these differences is likely to be minimal. This can be attributed to the type of motion; WaveOne and Reciproc were used in a reciprocal motion. This working motion has been associated with well-centered preparations and reduced incidence of procedural errors in some studies.[21,22] Furthermore, the differences may be explained by the different design features (tapering, tip size, cross-section shape, etc.) of the instruments used.
The result of some studies has shown that geometric features of canals before instrumentation have more effects on canal changes than techniques of instrumentation.[23] Therefore, more investigation is needed to definitely determine which factor (type of instrument, type of file movement, cross-section shape of the file, canal geometric structure, etc.) is more crucial in canal changes during instrumentation.
Numerous studies have been conducted to investigate cyclic fatigue, torsional strength, debris extrusion of single file techniques but few research was found in literature regarding the impact of single file motion on dentin thickness changes. Hence, more research is recommended to specify the effect of different motions on the efficacy of single files.
Conclusion
With the limitations of this study, it appears that canal preparation with WaveOne and Reciproc files have no statistically significant difference in canal wall dentin thickness changes, no matter if the file is used in reverse full rotation or reciprocation motion.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- 1.Abou-Rass M, Frank AL, Glick DH. The anticurvature filing method to prepare the curved root canal. J Am Dent Assoc. 1980;101:792–4. doi: 10.14219/jada.archive.1980.0427. [DOI] [PubMed] [Google Scholar]
- 2.Javaheri HH, Javaheri GH. A comparison of three Ni-Ti rotary instruments in apical transportation. J Endod. 2007;33:284–6. doi: 10.1016/j.joen.2006.05.004. [DOI] [PubMed] [Google Scholar]
- 3.Roane JB, Sabala CL, Duncanson MG., Jr The “balanced force” concept for instrumentation of curved canals. J Endod. 1985;11:203–11. doi: 10.1016/S0099-2399(85)80061-3. [DOI] [PubMed] [Google Scholar]
- 4.Kim HC, Kwak SW, Cheung GS, Ko DH, Chung SM, Lee W. Cyclic fatigue and torsional resistance of two new nickel-titanium instruments used in reciprocation motion: Reciproc versus WaveOne. J Endod. 2012;38:541–4. doi: 10.1016/j.joen.2011.11.014. [DOI] [PubMed] [Google Scholar]
- 5.Webber J, Machtou P, Pertot W, Kuttler S, Ruddle C, West J. The WaveOne single-file reciprocating system. Roots. 2011;1:28–33. [Google Scholar]
- 6.Castelló-Escrivá R, Alegre-Domingo T, Faus-Matoses V, Román-Richon S, Faus-Llácer VJ. In vitro comparison of cyclic fatigue resistance of ProTaper, WaveOne, and Twisted Files. J Endod. 2012;38:1521–4. doi: 10.1016/j.joen.2012.07.010. [DOI] [PubMed] [Google Scholar]
- 7.Bürklein S, Tsotsis P, Schäfer E. Incidence of dentinal defects after root canal preparation: Reciprocating versus rotary instrumentation. J Endod. 2013;39:501–4. doi: 10.1016/j.joen.2012.11.045. [DOI] [PubMed] [Google Scholar]
- 8.Shantiaee Y, Dianat O, Paymanpour P, Nahvi G, Ketabi MA, Kolahi Ahari G. Alterations of the danger zone after preparation of curved root canals using WaveOne with reverse rotation or reciprocation movements. Iran Endod J. 2015;10:156–61. doi: 10.7508/iej.2015.03.002. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Sordillo PP, Helson L, Hajdu SI, Magill GB, Kosloff C, Golbey RB, et al. Malignant schwannoma – Clinical characteristics, survival, and response to therapy. Cancer. 1981;47:2503–9. doi: 10.1002/1097-0142(19810515)47:10<2503::aid-cncr2820471033>3.0.co;2-3. [DOI] [PubMed] [Google Scholar]
- 10.Zuckerman O, Katz A, Pilo R, Tamse A, Fuss Z. Residual dentin thickness in mesial roots of mandibular molars prepared with Lightspeed rotary instruments and Gates-Glidden reamers. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2003;96:351–5. doi: 10.1016/s1079-2104(02)91710-5. [DOI] [PubMed] [Google Scholar]
- 11.Kessler JR, Peters DD, Lorton L. Comparison of the relative risk of molar root perforations using various endodontic instrumentation techniques. J Endod. 1983;9:439–47. doi: 10.1016/S0099-2399(83)80260-X. [DOI] [PubMed] [Google Scholar]
- 12.Dhingra A, Parimoo D. Evaluation of remaining dentine thickness using wave one and one shape file system with cone beam computed tomography. Int J Contemp Dent Med Rev. 2014:1–3. [Google Scholar]
- 13.Dhingra A, Ruhal N, Miglani A. Evaluation of single file systems reciproc, oneshape, and WaveOne using cone beam computed tomography – An in vitro study. J Clin Diagn Res. 2015;9:ZC30–4. doi: 10.7860/JCDR/2015/12112.5803. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Paqué F, Zehnder M, De-Deus G. Microtomography-based comparison of reciprocating single-file F2 ProTaper technique versus rotary full sequence. J Endod. 2011;37:1394–7. doi: 10.1016/j.joen.2011.06.031. [DOI] [PubMed] [Google Scholar]
- 15.You SY, Kim HC, Bae KS, Baek SH, Kum KY, Lee W. Shaping ability of reciprocating motion in curved root canals: A comparative study with micro-computed tomography. J Endod. 2011;37:1296–300. doi: 10.1016/j.joen.2011.05.021. [DOI] [PubMed] [Google Scholar]
- 16.Kim HC, Hwang YJ, Jung DW, You SY, Kim HC, Lee W. Micro-computed tomography and scanning electron microscopy comparisons of two nickel-titanium rotary root canal instruments used with reciprocating motion. Scanning. 2013;35:112–8. doi: 10.1002/sca.21039. [DOI] [PubMed] [Google Scholar]
- 17.Özer SY. Comparison of root canal transportation induced by three rotary systems with noncutting tips using computed tomography. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2011;111:244–50. doi: 10.1016/j.tripleo.2010.08.017. [DOI] [PubMed] [Google Scholar]
- 18.Bryant ST, Thompson SA, Al-Omari MA, Dummer PM. Shaping ability of profile rotary nickel-titanium instruments with ISO sized tips in simulated root canals: Part 1. Int Endod J. 1998;31:275–81. doi: 10.1046/j.1365-2591.1998.00153.x. [DOI] [PubMed] [Google Scholar]
- 19.Gelfand M, Sunderman EJ, Goldman M. Reliability of radiographical interpretations. J Endod. 1983;9:71–5. doi: 10.1016/S0099-2399(83)80079-X. [DOI] [PubMed] [Google Scholar]
- 20.Berutti E, Chiandussi G, Paolino DS, Scotti N, Cantatore G, Castellucci A, et al. Canal shaping with WaveOne primary reciprocating files and ProTaper system: A comparative study. J Endod. 2012;38:505–9. doi: 10.1016/j.joen.2011.12.040. [DOI] [PubMed] [Google Scholar]
- 21.Varela-Patiño P, Ibañez-Párraga A, Rivas-Mundiña B, Cantatore G, Otero XL, Martin-Biedma B. Alternating versus continuous rotation: A comparative study of the effect on instrument life. J Endod. 2010;36:157–9. doi: 10.1016/j.joen.2009.09.023. [DOI] [PubMed] [Google Scholar]
- 22.Franco V, Fabiani C, Taschieri S, Malentacca A, Bortolin M, Del Fabbro M. Investigation on the shaping ability of nickel-titanium files when used with a reciprocating motion. J Endod. 2011;37:1398–401. doi: 10.1016/j.joen.2011.06.030. [DOI] [PubMed] [Google Scholar]
- 23.Peters OA, Laib A, Göhring TN, Barbakow F. Changes in root canal geometry after preparation assessed by high-resolution computed tomography. J Endod. 2001;27:1–6. doi: 10.1097/00004770-200101000-00001. [DOI] [PubMed] [Google Scholar]