

Abstract
One of the most preferred compliance free fixed functional appliances in nongrowing patients is Twin Force Bite corrector (TFBC). The aim of this case report is to evaluate the effectiveness of TFBC in the treatment of an adult Class II case. A 16-year 1-month-old boy having skeletal and dental Class II relationship was selected. Roth 0.018 × 0.025 inch slots brackets were attached; a fixed lingual arch in the mandibular dental arch and a Nance appliance in the maxillary dental arch were used to increase anchorage. The TFBC therapy used for sagittal activation and stimulation of forward mandibular growth lasted for 3 months. The post-TFBC treatment lasted 6 months and the total treatment time was 9 months. Treatment of a young adult Class II malocclusion with TFBC resulted in a Class I molar occlusion, an ideal overjet, overbite, and incisor angulation in a short time and maintained in the 10-year follow-up.
Keywords: Class II treatment, Fixed functional appliance, Twin Force Bite corrector
Introduction
Class II malocclusion is one of the most frequent problems encountered in orthodontics and can be described as a distal relationship of the mandible related to the maxilla with a combination of different dental and skeletal components which can affect facial esthetics and functional status.[1] The most common characteristic of Class II malocclusion is mandibular retrognathia rather than maxillary protrusion.[2]
Class II division 1 malocclusions with a mandibular deficiency have been treated for more than a century with different types of functional appliances. Appliance selection can involve removable or fixed functional appliances according to the existing anteroposterior discrepancy, cooperation, and growth period of the patient.[3] Examples of these appliances are removable functional appliances, headgears, Class II elastics, and activator-headgear combinations. All these methods require good patient cooperation for success.[4] There is great interest in techniques that minimize the need for patient cooperation. Recently, several methods of Class II treatment by fixed functional mandibular anterior positioning appliances that do not rely on patient compliance become popular during last decade.[5]
Fixed functional appliances have the advantages of not requiring patient compliance, 24 h continuous force, and easy application. They can also be used currently with brackets. Their disadvantages are that they are prone to breakage and difficult to clean or remove.[6] Fixed functional appliances may give constant horizontal forces and have an additive headgear effect.[7] They may require additional chairside time and laboratory support and may be more prone to breakages.[6]
These devices can be categorized into two subgroups: Semielastic (e.g., Eureka Spring, Twin Force Bite Corrector, Jasper Jumper) and rigid (e.g., Herbst, MARA) bite jumping devices.[8] Both subgroups demonstrate similar results regarding the dentoskeletal correction.[9] Fixed functional appliances may be further subclassified as fixed rigid (Herbst, fixed twin block, mandibular anterior repositioning appliance), fixed flexible (Jasper jumper), and fixed hybrid (Forsus fatigue device, Twin Force Bite corrector).[10]
Nongrowing patients with Class II mandibular retrusion are mostly treated with fixed functional appliances which do not require the patient's collaboration.[11] One of the most preferred compliance free fixed functional appliances is Twin Force Bite Corrector (TFBC; Ortho Organizers CA, USA).
The aim of this case report is to evaluate the effectiveness of TFBC in the treatment of an adult Class II case and show the long-term follow-up results.
Diagnosis and Etiology
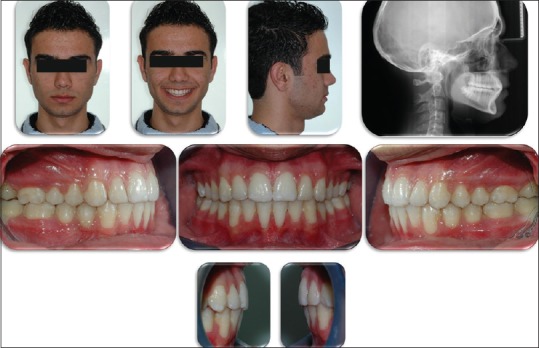
A 16-year 1-month-old boy was referred to X University Dental Clinic for orthodontic treatment with the chief complaint of backward lower jaw and unsatisfactory esthetics. He had no temporomandibular joint disorder or congenital craniofacial deformity. He had a convex profile and normal facial form with no asymmetries [Figure 1].
Figure 1.

Pretreatment extra- and intra-oral photographs and lateral cephalometric radiograph of the patient
Intraoral examination revealed a Class II molar occlusion with a 7 mm overjet and 5 mm overbite. The crowding was 1 mm in the maxillary arch and 3 mm in the mandibular arch [Figure 1]. He was in the MP3u skeletal growth stage and completed 99.1% of his skeletal growth.
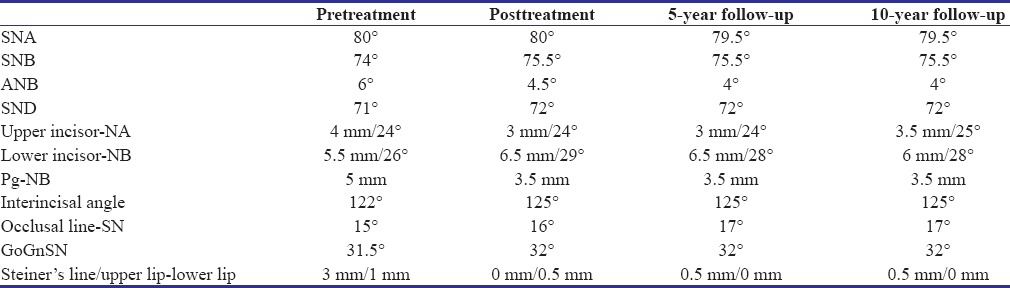
Pretreatment cephalometric analysis is presented in Table 1. Examination of the lateral cephalometric radiograph indicated normal positioned maxilla (SNA: 80°), retrognathic mandible (SNB: 74°), and skeletal Class II malocclusion (ANB: 6°) with normal vertical growth pattern (GoGnSN: 31.5°). The upper incisors were positioned normally (U1-NA: 4 mm/24°) and the lower incisors were proclined (L1-NB: 5.5 mm/26°). Panoramic radiographic evaluation showed permanent dentition with all teeth present except upper third molars. Anteroposterior radiograph revealed no skeletal asymmetry.
Table 1.
Pretreatment, posttreatment, 5-year follow-up, and 10-year follow-up cephalometric analysis
Treatment Objectives
The basic treatment objectives were sagittal activation and stimulation of forward mandibular growth, resolving of lower arch length discrepancy, and obtaining harmonious esthetic soft tissue profile.
Treatment Alternatives
The first treatment alternative was orthognathic surgery with mandibular advancement and genioplasty. However, the patient was not a severe case and he was unwilling to undergo surgery. Nonextraction orthodontic treatment protocol with interarch Class II mechanics could also be a treatment alternative. Therefore, TFBC was chosen for the treatment of the young adult patient because of the advantages of not requiring patient compliance, 24 h continuous force, and easy application.
Treatment Progress
Rothenberg et al. described TFBC (TFBC; Ortho Organizers CA, USA) as a fixed intermaxillary functional appliance with ball and socket joints which permits a wide range of motion, lateral flexibility, and full mandibular movement.[12] It could be classified as a “hybrid” fixed functional appliance that has a plunger system combined with active push coils that deliver a constant force of approximately 210 g.[12]
TFBC consisted of two telescopic systems. The appliance is attached to maxillary and mandibular archwires by ball and socket joints, which allow free lateral mandibular movements. The objective of this appliance is to move the teeth by applying 24 h continuous force with the internal coil springs. At full compression, TFBC postures the patient's mandible forward into an edge-to-edge occlusion. The appliance applies 210 g force and attaches to the archwires with a screw at the mesial of the maxillary molar and distal of the mandibular canines.
Upper and lower first molar teeth were banded. Roth 0.018 × 0.025 inch slots brackets were attached to the teeth. After alignment of upper and lower dental arches, 0.017 × 0.025 inch rectangular stainless steel archwires were applied. For the mandibular incisors, a lingual crown, buccal root torque was bended to prevent labial tipping. To minimize upper incisor retroclination, palatal root torque was applied to the upper incisors. A fixed lingual arch in the mandibular dental arch and a Nance appliance in the maxillary dental arch were used to increase anchorage [Figure 2]. At each monthly visit, the appliance was removed from the mandibular attachments on both sides, and a centric relation registration was taken.
Figure 2.

Extra- and intra-oral photographs and lateral cephalometric radiograph of the patient with Twin Force Bite Corrector appliance
The TFBC therapy lasted for 3 months. To maintain Class I dental relationship and skeletal correction, Class II elastics were used following TFBC removal. Appliances were debonded when ideal buccal occlusion, overjet, and overbite were obtained [Figure 3]. The post-TFBC treatment lasted 6 months and the total treatment time was 9 months.
Figure 3.
Posttreatment extra- and intra-oral photographs and lateral cephalometric radiograph of the patient
Retention phase using maxillary Hawley plate and mandibular lingual retainer [Figure 4] was lasted after 5 years. Extra- and intra-oral photographs and lateral cephalometric radiograph of the patient after 5-year follow-up are shown in Figure 5. The patient had no upper third molar teeth germ, and the lower third molar teeth germs were extracted.
Figure 4.

Patient with upper Hawley retention plate and lower lingual retainer
Figure 5.

Extra- and intra-oral photographs and lateral cephalometric radiograph of the patient after 5-year follow-up
After 10-year follow-up, the Class I molar occlusion, incisor angulation, overjet, and overbite were maintained [Figure 6].
Figure 6.

Extra- and intra-oral photographs and lateral cephalometric radiograph of the patient after 10-year follow-up
Results
Treatment of a young adult Class II malocclusion with TFBC resulted in a Class I molar occlusion, an ideal overjet, overbite, and incisor angulation in a short time [Figure 3]. According to Bjork's structural total and local superimpositions, mandible moved forward, upper incisors retruded, lower incisors protruded, and lower molars moved mesially [Figures 7 and 8]. As the case was a young adult, no changes seen in the superimpositions between posttreatment and postfollow-up periods.
Figure 7.
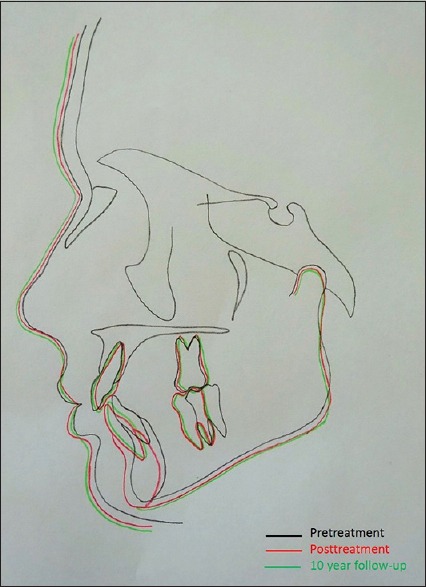
Total superimpositions done according to Bjork's structural superimposition technique
Figure 8.
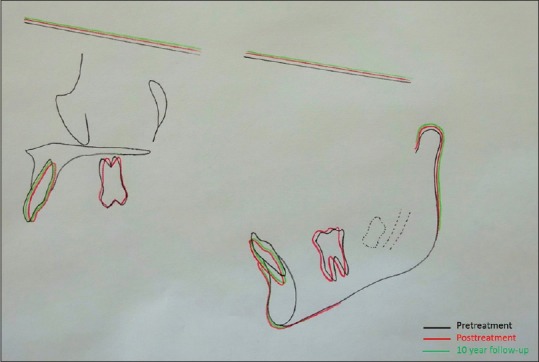
Local superimpositions done according to Bjork's structural superimposition technique
Discussion
Fixed functional appliances apply continuous force on the mandible to stimulate forward mandibular growth. TFBC is a flexible appliance that presents several advantages as it is agreeable to the patient, as it allows free lateral mandibular movements, practicability, and easy installation.[13] It also delivers an intermittent force by the nickel-titanium coil spring in the cylindrical system.
No appliance damage was observed in this case, as was observed in others.[5] Furthermore, the patient did not have any clinically observable adverse effects on the temporomandibular joint.
In a study, Rothenberg et al.[12] found decrease in overjet, ANB, and NAPg after TFBC treatment. Rothenberg et al. pointed that the time to achieve Class I molar relationship is 3 months and they also found an increase in the proclination of the mandibular incisors.[12] Similarly, TFBC therapy lasted for 3 months in the current case, and mandibular incisors protruded.
Some studies evaluated changes after fixed functional appliances (e.g.,. Herbst) treatment in adults.[14] A significant improvement of the facial profile after the use of Herbst appliance has been reported previously.[14]
Dalci et al. compared the treatment outcomes of a fixed functional appliance (TFBC) and a conventional removable functional appliance (activator) in the treatment of skeletal Class II malocclusions.[11] They found that both appliances were successful in treating the Class II relationship with varying degrees of skeletal and dental change. The duration of treatment was significantly shorter in the TFBC group.
Flores et al. examined the effects of functional appliances on soft tissue profile and found an improvement of the facial convexity.[15] They mentioned that the changes produced by fixed functional appliances seem to restrict the forward movement of the upper lip. The soft tissue changes are similar between nongrowing young adult and growing adolescent samples.[15] In the presented case, cephalometric measurements and superimpositions demonstrated improvements in both the skeletal and soft tissue parameters [Table 1 and Figures 7, 8].
One of the keys to success in Class II treatment is treatment timing. The most favorable time to treat patients with fixed functional appliances is during the peak of the pubertal growth spurt.[4] The patient presented in this article was in the MP3u skeletal growth stage and completed 99.1% of his skeletal growth at the beginning of treatment. Although he is in postpubertal growth period, the treatment time with TFBC was 3 months and total treatment time was 9 months.
Application of negative torque to the lower incisors and a lingual arch eliminated the unfavorable lower incisor protrusion. Even with these anchorage mechanics, mandibular incisors were proclined 1 mm in the presented case [Table 1]. Increase in the mandibular incisor inclination is a similar common finding of fixed functional appliances as shown by the other studies.[16] To eliminate this side effect of the TFBC, it could be effective to use mandibular rectangular archwires of greater size and addition of negative torque in the lower incisor region can be considered.[3]
Follow-up studies of Class II patients have shown a tendency to return to the original malocclusion after treatment. Madore and Ingervall found increases in overjet and overbite and relapse of the molar relationships.[17] The presented case was followed up for 10 years. Stable treatment results were obtained with the TFBC in this young adult patient [Figure 6]. The stable results in the long-term follow-up periods in our case report may be related with finishing the treatment with stable interdigitation in permanent dentition and the patient's postpeak growth.
Conclusion
TFBC is easy to place, does not require laboratory work and patient compliance, and exerts 24 h continuous force. In the presented young adult case, overjet reduction and forward mandibular growth were done by using fixed functional appliances. Perfect occlusion and harmonious facial profile were obtained in a short treatment period and maintained in the 10-year follow-up.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form the patient(s) has/have given his/her/their consent for his/her/their images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- 1.Alarashi M, Franchi L, Marinelli A, Defraia E. Morphometric analysis of the transverse dentoskeletal features of class II malocclusion in the mixed dentition. Angle Orthod. 2003;73:21–5. doi: 10.1043/0003-3219(2003)073<0021:MAOTTD>2.0.CO;2. [DOI] [PubMed] [Google Scholar]
- 2.McNamara JA., Jr Components of class II malocclusion in children 8-10 years of age. Angle Orthod. 1981;51:177–202. doi: 10.1043/0003-3219(1981)051<0177:COCIMI>2.0.CO;2. [DOI] [PubMed] [Google Scholar]
- 3.Atik E, Kocadereli I. Treatment of class II division 2 malocclusion using the forsus fatigue resistance device and 5-year follow-up. Case Rep Dent. 2016;2016:3168312. doi: 10.1155/2016/3168312. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Read MJ. The integration of functional and fixed appliance treatment. J Orthod. 2001;28:13–8. doi: 10.1093/ortho/28.1.13. [DOI] [PubMed] [Google Scholar]
- 5.Pancherz H. Treatment of class II malocclusions by jumping the bite with the herbst appliance. A cephalometric investigation. Am J Orthod. 1979;76:423–42. doi: 10.1016/0002-9416(79)90227-6. [DOI] [PubMed] [Google Scholar]
- 6.O'Brien K, Wright J, Conboy F, Sanjie Y, Mandall N, Chadwick S, et al. Effectiveness of treatment for class II malocclusion with the herbst or twin-block appliances: A randomized, controlled trial. Am J Orthod Dentofacial Orthop. 2003;124:128–37. doi: 10.1016/s0889-5406(03)00345-7. [DOI] [PubMed] [Google Scholar]
- 7.Oztoprak MO, Nalbantgil D, Uyanlar A, Arun T. A cephalometric comparative study of class II correction with Sabbagh Universal Spring (SUS (2)) and forsus FRD appliances. Eur J Dent. 2012;6:302–10. [PMC free article] [PubMed] [Google Scholar]
- 8.Küçükkeleş N, Ilhan I, Orgun IA. Treatment efficiency in skeletal class II patients treated with the Jasper Jumper. Angle Orthod. 2007;77:449–56. doi: 10.2319/0003-3219(2007)077[0449:TEISCI]2.0.CO;2. [DOI] [PubMed] [Google Scholar]
- 9.Lai M, McNamara JA., Jr An evaluation of two-phase treatment with the herbst appliance and preadjusted edgewise therapy. Semin Orthod. 1998;4:46–58. doi: 10.1016/s1073-8746(98)80041-8. [DOI] [PubMed] [Google Scholar]
- 10.Dandajena T. Current Therapy in Orthodontics. St. Louis, MO: Mosby Elsevier; 2010. Hybrid functional appliances for management of Class II malocclusions; pp. 103–13. [Google Scholar]
- 11.Dalci O, Altug AT, Memikoglu UT. Treatment effects of a twin-force bite corrector versus an activator in comparison with an untreated class II sample: A preliminary report. Aust Orthod J. 2014;30:45–53. [PubMed] [Google Scholar]
- 12.Rothenberg J, Campbell ES, Nanda R. Class II correction with the twin force bite corrector. J Clin Orthod. 2004;38:232–40. [PubMed] [Google Scholar]
- 13.Guimarães CH, Jr, Henriques JF, Janson G, de Almeida MR, Araki J, Cançado RH, et al. Prospective study of dentoskeletal changes in class II division malocclusion treatment with twin force bite corrector. Angle Orthod. 2013;83:319–26. doi: 10.2319/042312-339.1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Hansen K, Pancherz H. Long-term effects of herbst treatment in relation to normal growth development: A cephalometric study. Eur J Orthod. 1992;14:285–95. doi: 10.1093/ejo/14.4.285. [DOI] [PubMed] [Google Scholar]
- 15.Flores-Mir C, Major MP, Major PW. Soft tissue changes with fixed functional appliances in class II division 1. Angle Orthod. 2006;76:712–20. doi: 10.1043/0003-3219(2006)076[0712:STCWFF]2.0.CO;2. [DOI] [PubMed] [Google Scholar]
- 16.Gunay EA, Arun T, Nalbantgil D. Evaluation of the immediate dentofacial changes in late adolescent patients treated with the forsus(™) FRD. Eur J Dent. 2011;5:423–32. [PMC free article] [PubMed] [Google Scholar]
- 17.Madone G, Ingervall B. Stability of results and function of the masticatory system in patients treated with the herren type of activator. Eur J Orthod. 1984;6:92–106. doi: 10.1093/ejo/6.2.92. [DOI] [PubMed] [Google Scholar]