

Abstract
This study sought to examine the relationships among emotion regulation difficulties, childhood maltreatment, and risky sexual behavior in a sample of 320 heterosexual men recruited from urban STD clinics. Overall childhood maltreatment and several specific types of child abuse were significantly associated with emotion dysregulation, number of sexual partners, and STI diagnosis. There was evidence of an additive effect of multiple forms of maltreatment on difficulties with emotion regulation and sexual risk-taking. Impulse control difficulties and access to emotion regulation strategies, two components of emotion dysregulation, were related to measures of risky sexual behavior. Furthermore, limited access to emotion regulation strategies mediated the relationship between frequency of childhood sexual abuse and a greater number of lifetime sexual partners. This study has important implications for developing effective interventions to reduce the spread of STI’s and HIV by expanding affect regulation and distress tolerance strategies among men who have experienced childhood maltreatment.
Keywords: Emotional abuse, maltreatment, neglect, physical abuse, sexual abuse, children, adult survivor, black or African American
Risky sexual behavior in adulthood is a critical issue because of its potential short and long-term negative consequences, which can include the contraction of sexually transmitted infections (STIs) and HIV. The prevalence of risky sexual behavior among adults is difficult to measure and depends upon how one defines “risky.” Examples of behaviors that have been operationalized as risky because they increase the likelihood of contracting a STI or HIV include unprotected sex and sex with multiple partners, choosing risky partners, involvement in prostitution or sex trade, the use of drugs or alcohol with sex, sex with intravenous drug using partners, young age at first consensual intercourse and at first pregnancy, and sex with a partner without knowing their sexual history (Greenberg et al., 1999; Medrano et al., 1999; Rodgers et al., 2004; Senn et al., 2008). High rates of sexual risk-taking are evidenced by the large number of individuals diagnosed with a STI. In the United States, epidemiological studies estimate 19 million people are infected with a STI for the first time each year (Center for Disease Control and Prevention [CDC], 2007). The CDC (2008) estimated that 0.5% of adults living in U.S. households are infected with HIV and men ages 18–49 are the group most likely to be infected, with HIV rates of approximately 0.7% among this specific population. Among heterosexual men visiting STD clinics, HIV prevalence rates are as high as 5.9% depending on region (CDC, 1997). Studies examining the risk factors associated with the contraction of STIs and HIV are critical to the development of timely and effective interventions for this widespread problem.
Childhood Maltreatment and Risky Sexual Behavior
Risky sexual behavior has been linked to a variety of childhood maltreatment experiences, including childhood sexual, physical, and emotional abuse and physical and emotional neglect. Childhood sexual abuse (CSA), in particular, is one of the most well-established correlates of risky sexual behavior in adulthood (e.g. Banyard, 2003). For example, Senn, Carey, Vanable, Coury-Doniger, and Urban (2006) found that men and women recruited from a STI clinic who had a history of CSA reported greater numbers of lifetime and recent sexual partners, a greater number of episodes of unprotected sex in the previous three months, an increased likelihood of having exchanged sex for money or drugs, and an increased likelihood of having been diagnosed with an STI as compared to individuals without a history of sexual abuse.
Although explored to a lesser extent, physical and emotional abuse and neglect have been associated with increases in sexual risk-taking among men and women (Klein, Elifson, & Sterk, 2007; Newcomb, Locke, & Goodyear, 2003; Wilson & Widom, 2008). In a study of women from a population that was defined as “at risk” for HIV based on current drug abuse, poverty, low education, lack of medical care or insurance, unemployment, and criminal history, Klein et al. (2007) found that participants with a history of childhood neglect had more negative attitudes toward condom use and increased numbers of risky sexual behaviors.
Rodgers et al. (2004) offered evidence that there is an additive effect of multiple types of maltreatment on risky sexual behavior. Specifically, women who had experienced multiple forms of childhood maltreatment were more likely than women who had experienced only one form of maltreatment to have a history of risky sexual behavior, including greater numbers of lifetime sexual partners, younger age at first consensual intercourse, and younger age at first pregnancy. In a large-scale epidemiological study, Anda et al. (2006) found a dose-response effect of adverse childhood experiences on sexual behavior. Individuals reporting more than four adverse childhood experiences were 6.6 times more likely to be at risk for early intercourse and two times more likely to have more than 30 lifetime sexual partners. These findings are consistent with broader research indicating that there is a cumulative effect of adverse childhood experiences on a wide variety of health outcomes (Dube et al., 2009).
As stated above, a limitation of the previous research on childhood maltreatment and risky sexual behavior is that it has been primarily focused on CSA and has failed to adequately examine physical and emotional abuse and neglect as factors that can increase risky sexual behavior (Klein, Elifson, & Sterk, 2007). A broader conceptualization of childhood maltreatment provides the opportunity to compare forms of maltreatment and their influence on risky sexual behavior. Additionally, although the research on the relationship between childhood maltreatment and risky sexual behavior and other negative outcomes is substantial, the majority of studies have been done with women (Banyard, Williams, & Siegel, 2004). Finkelhor, Hotaling, Lewis, and Smith (1990) estimated that 16% of men have a history of CSA. The Administration for Children and Families (2006) stated that 48% of children referred to a child protective service agency for physical or sexual abuse were male. The existing literature’s focus on the relationship among child abuse and risky sex predominately among women is insufficient given prevalence rates showing that childhood maltreatment is a pervasive issue for both sexes.
Childhood Maltreatment and Emotion Regulation
A well-established relationship in the literature is the connection between childhood maltreatment and difficulties in emotion regulation. Emotion regulation has been defined as:
The (a) awareness and understanding of emotions, (b) acceptance of emotions, (c) ability to control impulsive behaviors and behave in accordance with desired goals when experiencing negative emotions, and (d) ability to use situationally appropriate emotion regulation strategies flexibly to modulate emotional responses as desired in order to meet individual goals and situational demands. (Gratz and Roemer, 2003, p. 42–43)
Problems with emotion regulation can be measured by examining an individual’s nonacceptance of emotional responses, difficulties engaging in goal-directed behaviors, impulse control difficulties, lack of emotional awareness, limited access to emotion regulation strategies, and lack of emotional clarity (Gratz & Romer, 2003). This multidimensional conceptualization of emotion regulation should be differentiated from approaches that view emotion regulation as limited to repressing or avoiding emotions. Additionally, emotion regulation is distinguished from self-regulation, which is a broader construct involving the regulation of attention and behavior in conjunction with emotions (Raffaelli & Crockett, 2003).
Research indicates that self-regulation processes, including emotion regulation, develop in early childhood from the combined influence of the child’s characteristics and the environment (Raffaelli & Crockett, 2003). Cook et al. (2005) reported that emotion regulation difficulties such as the reduced ability to identify and distinguish affective states can already be seen at age 30 months in children who have experienced maltreatment. The influential role of all types of childhood maltreatment on emotion management skills has been confirmed by both developmental and adult literature (Cloitre et al., 2005). Shields and Cicchetti (1998) proposed a developmental pathology framework that described this unique influence that childhood maltreatment has on emotion regulation difficulties: Achieving “affective homeostatis” is considered one of the early stage-salient developmental tasks, and this task can be interrupted by maltreatment during the time when a child is acquiring this ability. Disrupted acquisition of affective homeostasis at the early stages of development produces difficulties in emotion regulation that show up as emotional deficits such as emotional intensity, attenuated empathy, contextually inappropriate affective experiences and expressions, lability, and angry reactivity (Shields & Cicchetti, 1998).
There is additional neurological and psychophysiological research examining the influence of childhood maltreatment on the development and maintenance of emotion regulation. Systems identified with emotion regulation include the autonomic nervous system, the hypothalamic-pituitary adrenal (HPA) axis, the prefrontal cortex, and electrical activity in the central nervous system (Dawson, 1994; Ford, 2005; Fox, 1994; Stansbury & Gunnar, 1994). Ford (2005) stated that there is evidence of impairment in brain structures and processes involved in emotion regulation in individuals with a history of childhood maltreatment. Research indicates that stressful experiences during the critical period of neurodevelopment in childhood when fear-response and stress-response circuitry is being established in the amygdala, HPA axis, locus coeruleus/noradrenergic and glucocorticoid systems permanently disrupts neuroregulation of emotion (Anda et al., 2006). In a study examining these neurobiological correlates in a large sample, Anda et al. found a cumulative dose-response effect of adverse childhood experiences on two variables related to emotion dysregulation, perceived stress, and difficulty controlling anger. Individuals reporting four or more adverse childhood experiences were 2.2 times more likely to have high perceived stress and four times more likely to have anger control problems. This study provides preliminary evidence for the additive effects of maltreatment on emotion dysregulation.
Risky Sexual Behavior and Emotion Regulation
Although there is a dearth of research on the relationship between risky sexual behavior and emotion regulation, what has been found supports a possible connection. Cooper, Agocha, and Sheldon (2000) have shown that individuals engage in various forms of risky behavior, including but not limited to risky sexual behavior, both to enhance positive affective experiences and to help cope with aversive mood states. Additionally, they found that impulsivity, one aspect of emotion regulation, predicted risky behavior. Conceptualized differently, risky behavior in itself is seen as a mechanism of emotion regulation that serves to help individuals to cope with negative affective states or to enhance positive affective states. While Cooper et al. examined risky behavior in general, Raffaelli and Crockett (2003) found that self-regulation predicted risky sexual behavior specifically. Although broader than emotion regulation, self-regulation is the ability to regulate emotions, attention, and behavior. In a longitudinal study of adolescent females, Raffaelli and Crockett found that lower levels of self-regulation predicted greater risky sexual behaviors as measured by a composite of sexual activity, age at first intercourse, number of partners, and condom use. Other research has indicated that difficulties with emotion regulation can lead to a variety of behavioral control problems such as substance abuse, suicide, and risk-taking (Baumeister, 1997).
Childhood Maltreatment, Emotion Regulation, and Risky Sexual Behavior
Although numerous studies have identified mediators that affect the relationship between childhood trauma and risky sexual behavior (e.g., Raffaelli & Crockett, 2003), to our knowledge, no prior studies have looked specifically at the comprehensive construct of emotion regulation as a mediator in the relationship between childhood maltreatment and risky sexual behavior. However, Batten, Follette, and Aban (2001) found that CSA and experiential avoidance both predicted risky sexual behavior. Experiential avoidance, which can be conceptualized as one component of emotion dysregulation, is defined as “process in which a person is unwilling to experience negatively evaluated private events, such as thoughts, feelings, or memories, and thus makes subsequent attempts to reduce, numb, or alleviate those experiences” (Batten et al., 2001, p. 102). In a study of 257 female undergraduate students, Batten et al. found that the interaction of reported CSA history and high levels of generalized experiential avoidance significantly predicted unprotected sex with a non-primary partner.
The Present Study
Research indicates that there are well-established relationships between childhood maltreatment and both emotion dysregulation and risky sexual behavior. The present study aimed to provide additional evidence for an association between difficulties with emotion regulation and sexual risk-taking as well as to synthesize all of these findings to determine if emotion regulation mediates the relationship between childhood maltreatment and risky sexual behavior. Furthermore, the present study adds to the literature in multiple ways. First, childhood maltreatment was addressed in a broad sense to incorporate the various forms of maltreatment, including sexual, physical, and emotional abuse and physical and emotional neglect. We anticipated that each type of maltreatment would be associated with emotion regulation difficulties and various measures of risky sexual behavior. Second, the present study examined childhood maltreatment, emotion regulation, and risky sexual behavior in a population of heterosexual men, a group that has been understudied in relation to childhood maltreatment. Finally, this study examined emotion regulation as a comprehensive construct with multiple components, including, but not limited to, avoidance and impulsivity, which have previously been associated with childhood maltreatment and risky sexual behavior.
Hypothesis 1
Our first task was to extend prior research conducted with women, and demonstrate that child maltreatment is related to both emotion dysregulation and risky sexual behaviors in a sample of men. Thus, we predicted a significant relationship between overall child maltreatment and scores on measures of emotion regulation difficulties and three measures of risky sexual behaviors: increased number of sexual partners, a smaller proportion of partners with consistent condom use, and a current or past positive diagnosis of a STI (Hypothesis 1a). Also extending prior research, we predicted that each separate type of childhood maltreatment (sexual abuse, physical abuse, emotional abuse, physical neglect, and emotional neglect) would be significantly related to emotion dysregulation and sexual risk behaviors (Hypothesis 1b). Further, we predicted that, cumulatively, experiencing multiple types of childhood maltreatment would be associated with greater emotion dysregulation and sexual risk behaviors than experiencing only one type of maltreatment (Hypothesis 1c).
Hypothesis 2
Our second task was to establish a relationship between emotion dysregulation and sexual risk-taking, which has largely been missing from the literature. We hypothesized that emotion regulation difficulties would be associated with an increase in risky sexual behaviors—specifically, an increased number of sexual partners, a smaller proportion of partners with consistent condom use, and a current or past diagnosis of a STI (Hypothesis 1a). We also wanted to evaluate the relationship between the six separate components of emotion dysregulation and the three types of sexual risk-taking. Based on previous research with constructs of impulsivity and avoidance, we hypothesized that the components of emotion dysregulation most likely to be related to measures of sexual risk-taking would be impulse control difficulties and difficulties engaging in goal-directed behaviors (Hypothesis 2b).
Hypothesis 3
Assuming support for Hypotheses 1 and 2, we planned to test a model in which emotion regulation difficulties mediated the relationship between childhood maltreatment and risky-sexual behaviors. Specifically, we hypothesized that childhood maltreatment would predict decreased condom use, increased number of sexual partners, and a current or past diagnosis of a STI indirectly through difficulties with emotion regulation.
Methods
Participants
The sample consisted of 320 male participants recruited from two urban STI clinics: the Bell Flower Clinic in Indianapolis, Indiana and a City of St. Louis Department of Health STD/HIV Clinic in St. Louis, Missouri. Participation was limited to unmarried, heterosexual men ages 18 to 30 who could speak English. Participants were recruited by researchers who approached men in the waiting room to explain the study and answer questions.
Because these clinics provide free or inexpensive STI/HIV testing and counseling, they primarily serve low-income patients. A large percentage (45.9%) of participants reported an income of less than $15,000 per year, and only 18.7% of participants indicated an income greater than $30,000 per year. Consistent with the demographics of the patients served at the clinics, the sample was predominately African American (80%). The remaining participants were White (16%), American Indian/Alaska Native (2%), Asian (0.6%), and Other (0.9%). Two participants (0.5%) did not indicate their race. Nine participants (3%) indicated a Hispanic/Latino ethnicity.
Measures
Demographic measure
Demographic information was obtained using a 15-item questionnaire that included questions about sex, age, education, religion, socioeconomic status, race and ethnicity, and relationship status.
Risky sexual behavior
The Sexual History Questionnaire (SHQ) was developed for this research project and assessed risky sexual behavior. For this study, the two relevant questions on the SHQ were “In your lifetime, with how many people have you had sex (vaginal, oral or anal)?” and “Of the number you gave in the previous question, with how many of these partners did you consistently (every time you had sex) use a condom?” Participants were also asked if they had ever been told by a doctor or nurse that they had any of eight different STIs. Three indicators of risky sexual behavior were examined in this study: (a) the lifetime total number of male and female partners, (b) the lifetime proportion of male and female sexual partners with whom they had engaged in protected sex, and (c) lifetime or current diagnosis of a STI.
Childhood maltreatment
Experiences of childhood maltreatment were assessed with the Child Trauma Questionnaire (CTQ; Bernstein et al., 1994). The CTQ includes 28 items assessing sexual, physical, and emotional abuse and physical and emotional neglect. Items include statements such as “When I was growing up, I didn’t have enough to eat,” “When I was growing up, I felt that I was loved,” “When I was growing up, people in my family hit me so hard that it left me with bruises or marks,” and “When I was growing up, someone tried to touch me in a sexual way, or tried to make me touch them.” Statements are rated on a 5-point scale ranging from 1 (never true) to 5 (very often true). The CTQ provides an overall measure of exposure to child abuse and neglect. It also includes five subscales measuring physical and emotional abuse, physical and emotional neglect, and sexual abuse. High scores on the CTQ are reflective of greater childhood maltreatment. Previously, the CTQ has demonstrated excellent internal consistency (α = .95) and test-retest reliability (α = .88). Convergent validity has been established with an interview measure of childhood traumatic events for physical abuse and sexual abuse (Bernstein et al., 1994).
Difficulties with emotion regulation
The Difficulties with Emotion Regulation Scale (DERS; Gratz & Roemer, 2003) evaluates emotion regulation difficulties in six areas, including nonacceptance of emotional responses, difficulties engaging in goal-directed behaviors, impulse-control difficulties, lack of emotional awareness, limited access to emotion regulation strategies, and lack of emotional clarity. Items include statements such as, “I am clear about my feelings” (reverse scored), “When I’m upset, I become out of control,” “When I’m upset, I can still get things done” (reverse scored), and “When I’m upset, it takes me a long time to feel better.” Statements are rated on a 5-point scale ranging from 1 (almost never) to 5 (almost always). Higher scores on the DERS indicate greater difficulties with emotion regulation. The DERS has demonstrated excellent internal consistency for the total score, α = .93, and within each subscale, ranging from α = .80 to α = .89.
Procedures
Participants completed an informed consent and a series of questionnaires in paper-and-pencil format. Participants spent approximately 45 minutes completing the packet of questionnaires while in the waiting rooms of the clinics. The questionnaire responses remained anonymous unless the participant elected to provide contact information in order to allow researchers to contact him for future studies on a related topic. Payment of $15 was given to participants when they completed the packet of questionnaires.
Results
Preliminary Analyses
Data were collected from 450 participants; 125 participants were eliminated because they failed to complete all of the relevant measures for this study (participants were retained if they had completed at least 85% of each questionnaire) or showed a pattern of inconsistent responding as indicated by claiming to use a condom with more partners than they listed as their lifetime total number of partners. In addition, five participants were excluded as outliers for reporting 200 or more lifetime sexual partners, leaving a total of 320 men in the final sample.
Missing values for items on the CTQ and DERS were replaced with the series mean for the item. The childhood maltreatment total was calculated as a sum of the ratings for each item, and the childhood maltreatment subscale values were a sum of the ratings for each item identified on the subscale. Similarly, the difficulties with emotion regulation total value and individual subscale values were the sum of ratings on all the items for the measure or items identified for the subscale. The total number of partners was calculated by adding the number of male and female partners reported for each participant’s lifetime. The proportion of protected vaginal, anal, and oral sex acts with lifetime partners was calculated by dividing the lifetime total number of partners (male and female) with whom a condom was consistently used by the lifetime total number of partners. Finally, current or past diagnosis of a STI was calculated as a dichotomous variable with 0 indicating no current or past STI and 1 indicating any current or past STI diagnosis.
The Kolmogorov-Smirnov Z test was used to examine the normality of each variable associated with childhood maltreatment, emotion dysregulation, and risky sexual behavior. Due to violations of the assumption of normality and to reduce the impact of extreme scores, natural log transformations were conducted on all variables except the dichotomous measure of STI diagnosis. K–S tests following the transformations indicated that each of the variables except lifetime partner total still contained non-normal distributions; however, the normality of the distributions was improved by the transformations. For the descriptive statistics listed below, we report the non-transformed values. All other analyses used the transformed variables.
Descriptive Statistics
The sample was a high-risk group, with 62% reporting a current or past STI diagnosis. Only one participant reported a past diagnosis of HIV. The lifetime total number of partners ranged from 1 to 150 (M = 24.5, SD = 24.8). Participants ranged from never using a condom with a partner in their lifetime (6.8%) to using a condom with every partner (9.2%). The mean proportion of partners with consistent condom use was 0.62, indicating that, on average, men had consistently used a condom with approximately 62% of their partners.
All but three participants reported some history of negative childhood experiences as evidenced by at least one endorsement of a maltreatement experience occurring at least “rarely.” The total numbers of participants endorsing experiences of maltreatment were divided into emotional abuse (n = 264; 83%), emotional neglect (n = 285; 89%), physical abuse (N = 277; 87%), physical neglect (n = 269; 84%), and sexual abuse (n = 172; 54%). Among our sample, internal consistency was high for the total maltreatment score, α = .91. Finally, based on an independent samples t-test, our participants’ mean DERS (M = 88.1, SD = 20.3) was significantly higher than the mean endorsed by male college students in the original validation study (M = 80.66, SD = 18.79; p < .001; Gratz & Roemer, 2003).
Tests of Hypotheses
Hypothesis 1
To test our first hypothesis, we first conducted bivariate correlations between the total CTQ, DERS, and sexual risk-taking scores (Hypothesis 1a). As shown in Table 1, total childhood maltreatment was significantly correlated with the total measure of emotion dysregulation and with all the subcomponents of emotion dysregultion. Total childhood maltreatment was also significantly correlated with number of lifetime sexual partners and with past or current STI diagnosis but not with proportion of partners with condom use consistency.
Table 1.
Bivariate Correlations with Types of Childhood Maltreatment
| Scale | Type of Maltreatment
|
|||||
|---|---|---|---|---|---|---|
| Emotional Abuse r |
Physical Abuse r |
Sexual Abuse r |
Physical Neglect r |
Emotional Neglect r |
Total Maltreatment r |
|
| DERS Total | .49** | .40** | .41** | .45** | .36** | .51** |
| Impulse | .42** | .39** | .34** | .33** | .28** | .42** |
| Nonaccept | .43** | .30** | .32** | .33** | .23** | .39** |
| Goals | .32** | .25** | .26** | .21** | .16** | .29** |
| Awareness | .23** | .19** | .27** | .40** | .37** | .36** |
| Strategies | .47** | .38** | .38** | .38** | .29** | .45** |
| Clarity | .31** | .31** | .31** | .38** | .30** | .39** |
| Lifetime Partners | .17** | .16** | .15** | 0.07 | 0.07 | .15** |
| Condom Use Proportion | −0.03 | 0.10 | 0.01 | 0.05 | 0.02 | .03 |
| STI Diagnosis | .16** | 0.10 | .11* | 0.02 | 0.09 | .12* |
Note.
p = .01,
p < .05. DERS = Difficulties with Emotion Regulation Scale, Impulse = Impulse Control Difficulties, Nonaccept = Nonacceptance of Emotional Responses, Goals = Difficulties engaging in Goal-Directed Behavior, Aware = Lack of Emotional Awareness, Strategies = Access to Emotion Regulation Strategies, Clarity = Lack of Emotional Clarity, ERQ = Emotion Regulation Questionnaire, Lifetime Partners = total number of lifetime sexual partners, Condom Use Proportion = proportion of partners with whom a condom was consistently used, STI = Sexually Transmitted Infection.
Additionally, we analyzed the relationships between each type of childhood maltreatment (emotional abuse and neglect, physical abuse and neglect, and sexual abuse) and emotion dysregulation and risky sexual behavior to evaluate whether different types of abuse similarly impacted emotion regulation and risky sexual behavior (Hypothesis 1b). Table 1 shows the results of bivariate correlations, which indicate that increased experiences of all types of childhood maltreatment are significantly related to increased difficulties with emotion regulation. Furthermore, participants reporting more frequent experiences of emotional, physical, and sexual abuse also reported greater numbers of lifetime sexual partners. Participants who reported increased emotional and sexual abuse were more likely to have a current or past STI diagnosis.
Finally, we examined the possibility of the additive effects of multiple types of maltreatment on emotion dyregulation and risky sexual behavior (Hypothesis 1c). We performed a cumulative risk analysis with the childhood maltreatment variables. The cumulative risk index was set equal to 5 if the participant had experienced all types of maltreatment (sexual, physical, and emotional abuse and physical and emotional neglect), 4 if he had experienced four types of maltreatment, etc. Figures 1, 2, and 3 show the cumulative effect of multiple types of maltreatment on difficulties with emotion regulation, lifetime number of partners, and STI diagnosis, respectively. Using linear regression, we found that cumulatively more experiences of childhood maltreatment significantly predicted greater emotion dysregulation, F(1,267) = 78.5, p < .00, R2 = .22. The relationship between number of types of childhood maltreatment and increased number of lifetime sexual partners did not appear to be linear (see Figure 2), so we did not find convincing evidence of a cumulative impact of childhood maltreatment on lifetime number of partners. Results from a logistic regression indicated that the odds of having a current or past STI diagnosis were significantly greater as the number of types childhood maltreatment increased, Wald (1, N = 267) = 6.98, p < .01, OR = 1.30.
Figure 1.
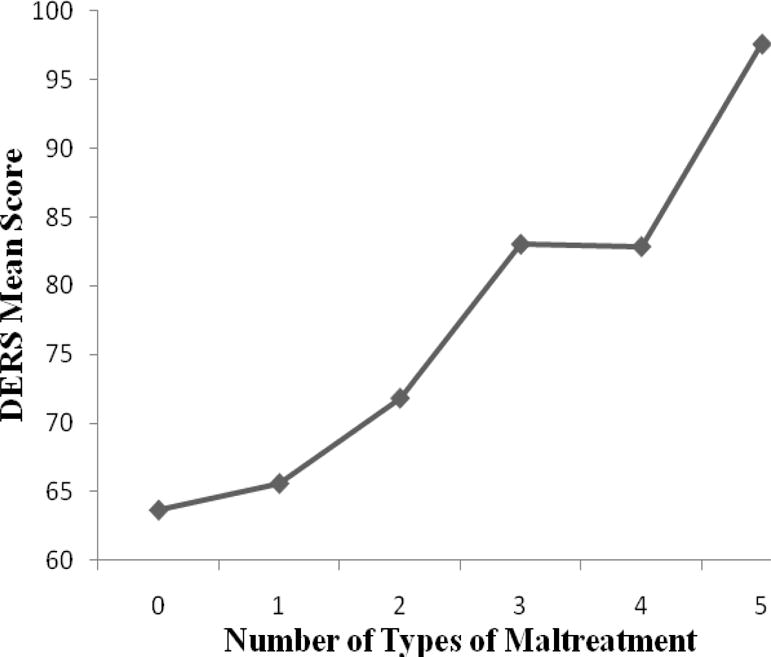
Mean ratings of difficulties with emotion regulation as a function of number of different types of childhood maltreatment.
Figure 2.
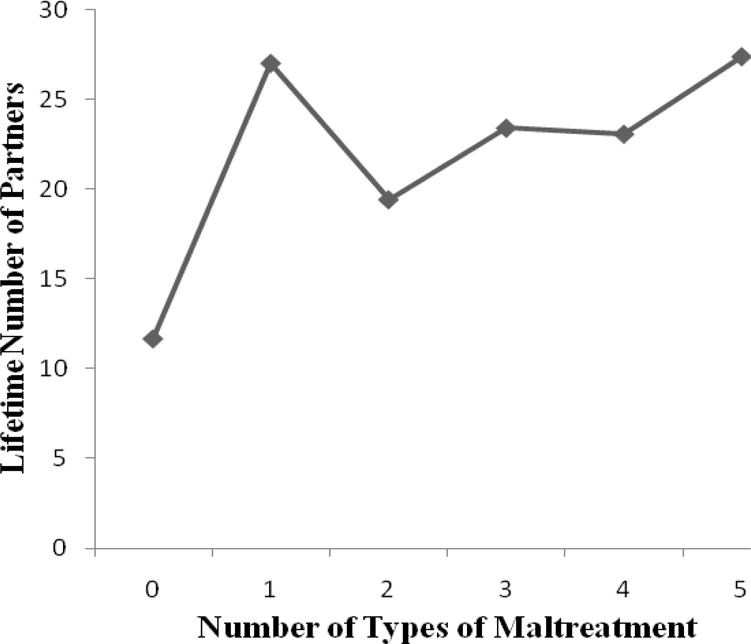
Lifetime number of partners as a function of number of different types of childhood maltreatment.
Figure 3.
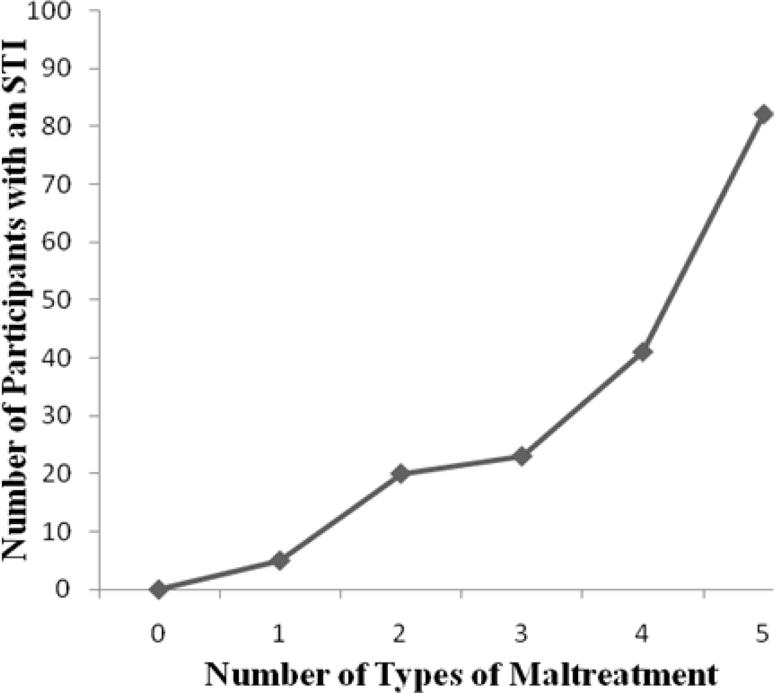
Number of participants endorsing a current or past STI diagnosis as a function of number of different types of childhood maltreatment.
Hypothesis 2
To test our second hypotheses regarding the relationship between emotion dysregulation and sexual risk-taking, we examined overall total emotion dysregulation as well as the six subcomponents. Bivariate correlations were calculated among the following variables: total emotion dysregulation, subscales of emotion dysregulation, lifetime total number of partners, proportion partners with whom a condom was consistently used, and history of STI. Results indicated that total emotion dysregulation was only marginally significantly related to lifetime number of partners, r = .11, p = .06, and unrelated to the proportion of partners with whom a condom was consistently used, r = .04, p = .45 and to STI diagnosis, r = .05, p = .38, providing minimal support for Hypothesis 2a.
Of the six emotion dysregulation subscales, lifetime number of partners was significantly correlated with impulse control difficulties, r = .12, p = .03 (providing partial support for Hypothesis 2b) and limited access to emotion regulation difficulties, r = .16, p < .001. In contrast to our prediction, the subscale measuring difficulties engaging in goal-directed behaviors was not significantly related to any of our measures of risk-taking. The remaining bivariate correlations for our variables of interest were also non-significant and are presented in Table 2.
Table 2.
Bivariate Correlations between Variables of Interest
| DERS Scale | Risky Sexual Behavior Index
|
||
|---|---|---|---|
| Lifetime Partners | Condom Use Proportion | STI Diagnosis | |
| Total | .11 | .04 | .05 |
| Impulse | .12* | .09 | .10 |
| Nonaccept | .08 | .02 | .02 |
| Goals | .05 | .01 | .01 |
| Awareness | .02 | .05 | −.06 |
| Strategies | .16** | .03 | .11 |
| Clarity | .08 | −.01 | .05 |
Note.
p < .01,
p < .05. DERS = Difficulties with Emotion Regulation Scale, Impulse = Impulse Control Difficulties, Nonaccept = Nonacceptance of Emotional Responses, Goals = Difficulties engaging in Goal-Directed Behavior, Aware = Lack of Emotional Awareness, Strategies = Access to Emotion Regulation Strategies, Clarity = Lack of Emotional Clarity, Lifetime Partners = total number of lifetime sexual partners, Condom Use Proportion = proportion of partners with whom a condom was consistently used, STI = Sexually Transmitted Infection.
Hypothesis 3
Once we had established a relationship between certain components of emotion dysregulation and measures of sexual risk taking, we proceeded with mediation analyses using only the subscales of difficulties with emotion regulation, which significantly predicted sexual risk taking based on bivariate correlations. To test our hypotheses, a series of regression analyses were conducted according to Baron and Kenny’s (1986) suggested analysis for mediation followed by the Sobel test, which determines the extent to which the mediator accounts for the influence of the independent variable on the dependent variable. We tested two separate models (a) to determine if limited access to emotion regulation strategies mediated the relationship between childhood maltreatment and lifetime number of partners, and (b) to determine if impulse control difficulties mediated the relationship between childhood maltreatment and lifetime number of partners.
First, a higher lifetime number of partners was predicted by increased experiences of total childhood maltreatment, F(1,318) = 7.12, p < .01. Second, increased frequency of childhood maltreatment significantly predicted more limited access to emotion regulation strategies, F(1, 318) = 82.58, p < .001. Third, more limited access to emotion regulation strategies significantly predicted an increased lifetime number of partners, F(1,318) = 8.35, p = .004. Last, although childhood maltreatment was no longer a significant predictor of number of partners (β = .10, p = .13) when controlling for limited access to emotion regulation strategies, the mediator also did not significantly predict increased lifetime numbers of partners, β = .12, p = .06, although there was a trend in that direction. Finally, using a Sobel test calculation, we examined the difference between the mediation path and the direct path from childhood maltreatment to lifetime number of partners. Results indicated that limited access to emotion regulation strategies failed to significantly mediate the path between childhood maltreatment and lifetime number of partners, Sobel = 1.84, p < .07, although, again, there was a trend toward significance. Our mediation hypothesis was not strongly supported for overall maltreatment.
For impulse control difficulties, the first step relating childhood maltreatment and lifetime number of partners is established in the previous mediation analyses. Second, childhood maltreatment significantly predicted greater impulse control difficulties, F(1,318) = 72.25, p < .001. Third, increased impulse control difficulties significantly predicted a greater number of lifetime partners, F(1,318) = 5.26, p = .02. However, impulsive control difficulties was no longer a significant predictor of number of partners, β = .08, p = .19 when entered into the regression with childhood maltreatment, suggesting that mediation did not occur.
Exploratory Follow-up Analyses
Previous research has specifically focused on the impact of CSA on sexual behavior in adulthood. As CSA was a significant predictor of number of lifetime partners (see Table 1), we tested more specific mediation models to determine if the previously examined components of emotion dysregulation (access to emotion regulation strategies and impulse control difficulties) accounted for part of the impact of sexual abuse on having more sexual partners.
In the first step, CSA significantly predicted lifetime number of partners, F(1,318) = 7.5, p < .01. Second, more frequent CSA was significantly related to more limited access to emotion regulation strategies, F(1,318) = 52.99, p < .001. Third, lifetime number of partners was regressed on the access to emotion regulation strategies subscale and results indicated that more limited access to emotion regulation strategies significantly predicted an increased lifetime number of partners, F(1,318) = 8.35, p = .004. Last, CSA was no longer a significant predictor of lifetime number of partners (β = .11, p = .07) when controlling for access to emotion regulation strategies, which remained a significant predictor (β = .12, p < .05). The overall model was significant, F(2,317) = 5.81, p < .01, and accounted for 2.9% of the variance in lifetime number of partners. Finally, using a Sobel test calculation, we examined the difference between the mediation path and the direct path from childhood maltreatment to lifetime number of partners. Results indicated that limited access to emotion regulation strategies significantly mediated the path between CSA and lifetime number of partners, Sobel = 1.94, p = .05.
For the mediation using impulse control difficulties, the first step relating CSA and lifetime number of partners is established in the previous mediation analyses. Second, CSA significantly predicted greater impulse control difficulties, F(1,318) = 40.40, p < .001. Third, increased impulse control difficulties significantly predicted a greater number of lifetime partners, F(1,318) = 4.62, p = .03. However, impulsive control difficulties was no longer a significant predictor of number of partners, β = .08, p = .19 when entered into the regression with CSA, indicating that mediation did not occur.
Discussion
The Mediating Effects of Emotion Regulation
Similar to prior studies of women (e.g. Batten, Follette, & Aban, 2000) and consistent with our hypotheses, experiences of childhood maltreatment are associated with adult problems with emotion dysregulation and sexual risk taking in a high-risk population of men. While overall difficulties with emotion regulation were not associated with greater risky sexual behavior, certain components of emotion dysregulation, including limited access to emotion regulation strategies and impulse control difficulties, predicted greater lifetime numbers of sexual partners. Furthermore, the findings from this study provide preliminary evidence that aspects of difficulties with emotion regulation may mediate the relationship between CSA and sexual risk-taking. Specifically, higher frequency of CSA predicted more limited access to emotion regulation strategies, which in turn predicted more sexual partners.
It has been suggested that individuals who have experienced childhood maltreatment, including CSA, develop a more sensitive fight or flight response system and fail to cognitively mediate their behaviors during potentially risky situations, leaving them vulnerable to poor decision making and risky behaviors, including sexual risk-taking (Lescano, Brown, Puster, & Miller, 2004). Cognitive mediation involves using adaptive emotion regulation strategies such as challenging dysregulated thoughts, affect management, distress tolerance, and minimizing avoidance or dissociative strategies. Perhaps this increased reactivity to the fight or flight system and impairment in cognitive mediation abilities reduces the use of emotion regulation strategies that could be employed to prevent sexual risk-taking. Further research examining the protective role of cognitive mediation and the function of risky sexual behavior in men who have experienced CSA would assist in clarifying this relationship.
It is also possible that men with histories of CSA may use sex with new or multiple partners as a way to manage unwanted negative emotions because they lack alternative strategies for coping with negative affect. Auerbach et al. (2007) found that individuals who lacked emotional repair strategies, which they conceptualized as an aspect of emotion regulation, were more likely to engage in risky behavior to cope with negative affective states including depression and anxiety. If this is the case, implementing sexual risk-taking prevention interventions that focus on psychoeducation about emotion regulation strategies may be useful with men who have experienced CSA. For example, Lescano et al. (2004) encouraged the application of Dialectical Behavior Therapy’s emotion regulation strategy training to HIV prevention protocols to increase limit-setting in sexual situations for adolescents.
Results of this study also suggest that impulse control difficulties are associated with increased numbers of sexual partners. With the exception of limited access to emotion regulation strategies (discussed above), other aspects of emotion regulation were unrelated to measures of sexual risk-taking, indicating that interventions aimed at increasing impulse control may be particularly beneficial in preventing risky sexual behavior. However, our results failed to provide evidence of impulsivity acting as a mediator between childhood maltreatment and risky sexual behavior, suggesting that sexual risk-taking behavior was better explained by the presence of maltreatment than by impulsivity. For men abused in childhood, the causes of their sexual risk-taking may be too multifaceted and complex to be explained merely by a measure of impulsivity. Thus interventions aimed at reducing impulsivity may be beneficial in reducing risky sexual behavior among a sample of nonabused men, but reducing impulsivity may not be sufficient to address risky behavior in men with a history of childhood maltreatment.
The fact that overall emotion dysregulation and the majority of its components were unrelated to sexual risk-taking was surprising and inconsistent with our hypotheses. The lack of significant findings in these relationships prevented further analysis of emotion dysregulation as a mediator between childhood maltreatment and risky sexual behavior. It is possible that difficulties with emotion regulation are simply not associated with sexual risk-taking. However, based on our study and previous research it is more likely that only certain aspects of emotion dysregulation impact the occurrence of risky sexual behavior. Emotion dysregulation is a broad construct encompassing multiple components, each of which likely has different behavioral correlates. This may explain our lack of significant results when we examined the relationship between sexual risk behavior and emotion dysregulation as a whole.
The Impact of Types of Maltreatment
This study went beyond previous research that has focused on CSA as associated with risky sexual behavior to examine the impact of various types of childhood maltreatment on sexual risk-taking in adulthood. As expected, the strong associations between the various types of childhood maltreatment and emotion dysregulation and sexual risk-taking provide evidence that experiences other than CSA increase these kinds of difficulties in adulthood. In fact, emotional abuse was at least as strong a predictor of emotion dysregulation, number of sexual partners, and STI history as sexual abuse.
Our analyses also suggested there may be an additive effect of maltreatment experiences on difficulties with emotion regulation and STI diagnosis in adulthood. Previous research also has found evidence for the additive effect of childhood maltreatment on problematic behavior later in life. For example, a study of urban youth found that adolescents who had experienced sexual abuse, physical abuse, and neglect reported significantly more sexual partners than adolescents who had experienced a single form of childhood maltreatment (Arata et al., 2007). Although we did not find evidence of an additive effect of maltreatment on number of sexual partners, our results confirm that additional research examining the cumulative effects of various types of childhood maltreatment on adult risk behaviors, especially in men, is needed.
Limitations
This study had a number of limitation including, most notably, the measurement of risky sexual behavior. Despite transformation of the variables, there remained problems with kurtosis and skewness for our measure of condom use. This problem is consistent with non-normal distributions in the extant literature on sexual risk-taking (Weinhardt, Forsyth, Carey, Jaworski, & Durant, 1998). Furthermore, a number of participants were eliminated from the study because they responded inconsistently to risk-taking items; it is unclear whether this was a result of carelessness, confusion about the questions, or intentional misrepresentation. Our use of items that ask about lifetime sexual experiences introduces the possibility that participants may have had difficulty remembering and reporting sexual partners accurately. This may have been a particular problem with our measure of condom use and account for the fact that our condom use variable was not associated with our predicted correlates. Because we measured the proportion of partners with whom the participant had consistently used condoms, participants were required to remember and accurately report both their lifetime number of partners and the number of partners with whom they had consistently used condoms. Furthermore, on a conceptual level there is variability in what should be considered “risky;” a high number of partners may not place men at risk for STIs if condoms were used consistently with all partners. Schroder et al. (2003a) also warned that social context biases responses on measures of sexual health, so it is possible that the men in this study were uncomfortable with the public nature of the STI clinic and underreported their sexual experiences. Researchers have made a number of recommendations for increasing the usefulness of sexual risk-taking measures including using multiple continuous measures assessing condom use that is specific to partner, specific to sex act, and specific to shorter recall periods; using count rather than relative frequency methods; using psychometrically validated measures; and conducting in-person interviews in which a working trust can be established (Noar et al., 2006; Schroder et al., 2003a, 2003b; Weinhardt et al., 1998).
Another important limitation of this study is that it is cross-sectional, which prevents us from making statements about causation. Although we tested mediation models in this study, it is not possible to conclusively determine the direction of the relationships in our model. Although childhood maltreatment is likely to have occurred prior to the development of emotion regulation difficulties, it could be that emotion dyregulation puts children at higher risk for maltreatment. Additionally, it is possible that sexual risk-taking increases components of emotion dysregulation rather than results from limited access to emotion regulation strategies or impulse control difficulties.
A third limitation is that the men in our sample reported, on average, only occasional problems with emotion dysregulation (although their DERS scores were higher than in a prior sample of college students; Gratz & Roemer, 2003). The ratings of total difficulties with emotion regulation failed to significantly predict any index of sexual risk-taking, which undermined the overall mediation model. It is possible that only severe problems with emotion dysregulation result in sexual risk taking. Future research could examine highly emotionally dysregulated populations to clarify the role of severe emotion regulation problems in sexual risk-taking.
Finally, a large majority of the participants in this study were low-income, African American men, which limits the generalizability of our findings. Still, the predominance of African American men can be viewed as a strength as well, given that this population is at much greater risk than White men for contracting a STI or HIV (CDC, 2006). Thus, understanding the factors associated with sexual risk-taking in this population is particularly valuable.
Conclusions
Despite the limitations, the results of this study encourage further research that examines the complex set of factors that contribute to sexual risk-taking in men and a broader consideration for the impact of multiple types of childhood maltreatment on emotional and sexual functioning in adulthood. To create and implement appropriate prevention strategies to reduce the occurrence of STI and HIV contraction in communities, we must improve our understanding of the risk factors associated with sexual risk-taking. The findings from this study indicate that both experiences of childhood maltreatment and difficulties with some aspects of emotion regulation increase the likelihood that men will engage in risky sexual behavior. Furthermore, we found preliminary evidence for the possibility of a mediational relationship demonstrating that men who have experienced CSA lack access to emotion regulation strategies and, consequently, engage in risky sexual behavior. This evidence suggests that there would be value in developing interventions to expand affect regulation and distress tolerance strategies among men who have experienced CSA because these men are at particular risk for engaging in sexual behaviors that increase their chances of contracting HIV or a STI. Accurately identifying at-risk individuals and providing appropriate interventions can ultimately reduce the spread of STIs and HIV associated with sexual risk-taking.
Acknowledgments
This research was conducted as part of Tiffany Mueller’s master’s thesis under the supervision of Zoe Peterson. This research was supported by a grant (R21HD055831; Zoe Peterson, PI) from the Eunice Kennedy Shriver National Institute of Child Health and Human Development (NICHD) at the National Institutes of Health. This article’s contents are solely the responsibility of the authors and do not necessarily represent the official views of NICHD. The authors are grateful to the co-investigators on the grant (Julia R. Heiman, Erick Janssen, Jeffry Thigpen, J. Dennis Fortenberry, and Janet N. Arno) and to David Goodrich and Scott Herbert for help with data collection. The authors also thank Tara Galovski and Ethan McCallum for their feedback on earlier drafts of this article.
Contributor Information
Tiffany M. Mueller, Department of Psychology, University of Missouri, St. Louis, MO
Zoë D. Peterson, Department of Psychology, University of Missouri, St. Louis, MO.
References
- Administration for Children and Families. Childhood maltreatment 2006. Washington, DC: U.S. Department of Health and Human Services; 2006. [Google Scholar]
- Anda RF, Felitti VJ, Bremner JD, Walker JD, Whitfield C, Perry BD, Giles WH. The enduring effects of abuse and related adverse experiences in childhood: A convergence of evidence from neurobiology and epidemiology. European Archives of Psychiatry and Clinical Neuroscience. 2006;256:174–186. doi: 10.1007/s00406-005-0624-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Arata CM, Langhinrichsen-Rohling J, Bowers D, O’Brien N. Differential correlates of multi-type maltreatment among urban youth. Child Abuse & Neglect. 2007;31:393–415. doi: 10.1016/j.chiabu.2006.09.006. [DOI] [PubMed] [Google Scholar]
- Auerbach RP, Abela JR, Ho MR. Responding to symptoms of depression and anxiety: Emotion regulation, neuroticism, and engagement in risky behaviors. Behavior Research and Therapy. 2007;45:2182–2191. doi: 10.1016/j.brat.2006.11.002. [DOI] [PubMed] [Google Scholar]
- Banyard VL. Explaining links between sexual abuse and psychological distress: Identifying mediating process. Child Abuse & Neglect. 2003;27:869–875. doi: 10.1016/S0145-2134(03)00144-3. [DOI] [PubMed] [Google Scholar]
- Banyard VL, Williams LM, Siegel JA. Childhood sexual abuse: A gender perspective on context and consequences. Child Maltreatment. 2004;9:223–238. doi: 10.1177/107755904266914. [DOI] [PubMed] [Google Scholar]
- Baron RM, Kenny DA. The moderator-mediator variable distinction in social psychological research: Conceptual, strategic, and statistical considerations. Journal of Personality and Social Psychology. 1986;51:1173–1182. doi: 10.1037/0022-3514.51.6.1173. [DOI] [PubMed] [Google Scholar]
- Batten SV, Follette VM, Aban IB. Experiential avoidance and high-risk sexual behavior in survivors of child sexual abuse. Journal of Child Sexual Abuse. 2001;10:101–120. doi: 10.1300/J070v10n02_06. [DOI] [PubMed] [Google Scholar]
- Baumeister RF. Esteem threat, self-regulatory breakdown, and emotional distress as factors in self-defeating behavior. Review of General Psychology. 1997;1:145–174. doi: 10.1037/1089-2680.1.2.145. [DOI] [Google Scholar]
- Bernstein DP, Fink L, Handelsman L, Foote J, Lovejoy M, Wenzel K, et al. Initial reliability and validity of a new retrospective measure of child abuse and neglect. American Journal of Psychiatry. 1994;151:1132–1136. doi: 10.1176/ajp.151.8.1132. Retrieved from http://ajp.psychiatryonline.org. [DOI] [PubMed] [Google Scholar]
- Center for Disease Control and Prevention. National HIV Prevalence Surveys, 1997 Summary. Atlanta, GA: Center for Disease Control and Prevention; 1998. [Google Scholar]
- Center for Disease Control and Prevention. Sexually Transmitted Disease Surveillance, 2006. Atlanta, GA: U.S. Department of Health and Human Services; 2007. [Google Scholar]
- Center for Disease Control and Prevention. HIV infection in the United States household population aged 18–49 years: Results from 1999–2006. NCHS Data Brief. 2008;4:1–7. [PubMed] [Google Scholar]
- Cloitre M, Miranda R, Stovall-McClough KC, Han H. Beyond PTSD: Emotion regulation and interpersonal problems as predictors of functional impairment in survivors of childhood abuse. Behavior Therapy. 2005;36:119–124. doi: 10.1016/S0005-7894%2805%2980060-7. [DOI] [Google Scholar]
- Cloitre M, Stovall-McClough C, Zorbas P, Charuvastra A. Attachment organization, emotion regulation, and expectations of support in a clinical sample of women with childhood abuse histories. Journal of Traumatic Stress. 2008;21:282–289. doi: 10.1002/jts.20339. [DOI] [PubMed] [Google Scholar]
- Cook A, Spinazzola J, Ford J, Lanktree C, Blaustein M, Cloitre M, van der Kolk B. Complex trauma in children and adolescents. Psychiatric Annals. 2005;35:390–398. Retrieved from http://psychiatricannalsonline.com. [Google Scholar]
- Cooper ML, Agocha VB, Sheldon MS. A motivational perspective on risky behaviors: The role of personality and affect regulatory processes. Journal of Personality. 2000;68:1059–1088. doi: 10.1111/1467-6494.00126. [DOI] [PubMed] [Google Scholar]
- Dawson G. Frontal electroencephalographic correlates of individual differences in emotion expression in infants: A brain systems perspective on emotion. Monographs of the Society for Research in Child Development. 1994;59:2–3. doi: 10.2307/1166142. Serial No. 240. [DOI] [PubMed] [Google Scholar]
- Dube SR, Fairweather D, Pearson WS, Felitti VJ, Anda RF, Croft JB. Cumulative childhood stress and autoimmune diseases in adults. Psychosomatic Medicine. 2009;71:243–250. doi: 10.1097/PSY.0b013e3181907888.. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Finkelhor D, Hotaling G, Lewis IA, Smith C. Sexual abuse in a national survey of adult men and women: Prevalence, characteristics, and risk factors. Child Abuse & Neglect. 1990;14:19–28. doi: 10.1016/0145-2134%2890%2990077-7. [DOI] [PubMed] [Google Scholar]
- Ford JD. Treatment implications of altered affect regulation and information processing following child maltreatment. Psychiatric Annals. 2005;35:410–419. Retrieved from http://psychiatricannalsonline.com. [Google Scholar]
- Fox NA. Dynamic cerebral processes underlying emotion regulation. Monographs of the Society for Research in Child Development. 1994;59:2–3. doi: 10.2307/1166143. Serial No. 240. [DOI] [PubMed] [Google Scholar]
- Gratz KL, Roemer L. Multidemensional assessment of emotion regulation and dysregulation: Development, factor structure, and initial validation of the Difficulties in Emotion Regulation Scale. Journal of Psychopathology and Behavioral Assessment. 2003;26:41–54. doi: 10.1023/B:JOBA.0000007455.08539.94. [DOI] [Google Scholar]
- Greenberg J, Hennessy M, Lifshay J, Kahn-Krieger S, Bartelli D, Downer A, Bliss M. Childhood sexual abuse and its relationship to high-risk behavior in women volunteering for an HIV and STD prevention intervention. AIDS and Behavior. 1999;3:149–156. [Google Scholar]
- Klein H, Elifson KW, Sterk CE. Childhood neglect and adulthood involvement in HIV-related risk behaviors. Child Abuse & Neglect. 2007;31:39–53. doi: 10.1016/j.chiabu.2006.08.005. [DOI] [PubMed] [Google Scholar]
- Lescano CM, Brown LK, Puster KL, Miller PM. Sexual abuse and adolescent HIV risk: A group intervention framework. Journal of HIV/AIDS Prevention in Children & Youth. 2004;6:43–57. doi: 10.1300/J499v06n01_04. [DOI] [Google Scholar]
- MacKinnon DP, Dwyer JH. Estimating mediated effects in prevention studies. Eva1uation Review. 1993;17:144–158. doi: 10.1177/0193841X9301700202. [DOI] [Google Scholar]
- Medrano MA, Desmond DP, Zule WA, Hatch JP. Histories of childhood trauma and the effects of risky HIV behaviors in a sample of women drug users. American Journal of Drug Alcohol Abuse. 1999;25:593–606. doi: 10.1081/ADA-100101881. [DOI] [PubMed] [Google Scholar]
- Newcomb MD, Locke TF, Goodyear RK. Childhood experiences and psychosocial influences on HIV risk among adolescent Latinas in Southern California. Cultural Diversity and Ethnic Minority Psychology. 2003;9:219–235. doi: 10.1037/1099-9809.9.3.219. [DOI] [PubMed] [Google Scholar]
- Noar SM, Cole C, Carlyle K. Condom use measurement in 56 studies of sexual risk behavior: Review and recommendations. Archives of Sexual Behavior. 2006;35:327–245. doi: 10.1007/s10508-006-9028-4. [DOI] [PubMed] [Google Scholar]
- Raffaelli M, Crockett LJ. Sexual risk taking in adolescence: The role of self-regulation and attraction to risk. Developmental Psychology. 2003;39:1036–1046. doi: 10.1037/0012-1649.39.6.1036. [DOI] [PubMed] [Google Scholar]
- Rodgers CS, Lang AJ, Laffaye C, Satz LE, Dresselhaus TR, Stein MB. The impact of individual forms of childhood maltreatment on health behavior. Child Abuse & Neglect. 2004;28:575–586. doi: 10.1016/j.chiabu.2004.01.002. [DOI] [PubMed] [Google Scholar]
- Schroder KEE, Carey MP, Vanable PA. Methodological challenges in research on sexual risk behavior: I. Item content, scaling, and data analytical options. Assessment and Analysis of Sexual Behavior. 2003a;26:76–103. doi: 10.1207/S15324796ABM2602_02. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Schroder KEE, Carey MP, Vanable PA. Methodological challenges in research on sexual risk behavior: II. Accuracy of self-reports. Assessment and Analysis of Sexual Behavior. 2003b;26:104–123. doi: 10.1207/S15324796ABM2602_03. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Senn TE, Carey MP, Vanable PA, Coury-Doniger P, Urban MA. Childhood sexual abuse and sexual risk behavior among men and women attending a sexually transmitted disease clinic. Journal of Consulting and Clinical Psychology. 2006;74:720–731. doi: 10.1037/0022-006X.74.4.720. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Shields A, Cicchetti D. Reactive aggression among maltreated children: The contributions of attention and emotion dysregulation. Journal of Clinical Child Psychology. 1998;27:381–395. doi: 10.1207/s15374424jccp2704_2. [DOI] [PubMed] [Google Scholar]
- Small SA, Luster T. Adolescent sexual activity: An ecological risk-factor approach. Journal of Marriage and the Family. 1994;56:181–192. Retrieved from http://www.jstor.org/stable/352712. [Google Scholar]
- Stansbury K, Gunnar MR. Adrenocortical activity and emotion regulation. Monographs of the Society for Research in Child Development. 1994;59:2–3. Serial No. 240. [PubMed] [Google Scholar]
- Weinhardt LS, Forsyth AD, Carey MP, Jaworski BC, Durant LE. Reliability and validity of self-report measures of HIV-related sexual behavior: Progress since 1990 and recommendations for research and practice. Archives of Sexual Behavior. 1998;27:155–180. doi: 10.1023/A:1018682530519. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wilson HW, Widom CS. An examination of risky sexual behavior and HIV in victims of child abuse and neglect: A 30-year follow-up. Health Psychology. 2008;27:149–158. doi: 10.1037/0278-6133.27.2.149. [DOI] [PubMed] [Google Scholar]