

Abstract
Background:
Capsulectomy is performed during hip arthroscopic surgery in young adult patients with hip pain to improve intraoperative visualization. The stability of the hip joint after anterior capsulectomy is relatively unknown.
Purpose:
To evaluate anterior hip stability in capsular sectioned states with a labral injury to test whether the load required for anterior translation would decrease with greater capsular injuries.
Study Design:
Controlled laboratory study.
Methods:
Sixteen hips from 8 of 10 human cadaveric pelvises (mean age, 54.25 years) were prepared/mounted onto a custom-built fixture and tested in 5 states: intact capsule, intact labrum (all intact); sutured capsule, intact labrum (sutured intact); sutured capsule, 1-cm partial labrectomy (sutured labrectomy); partial capsulectomy, 1-cm partial labrectomy (partial capsulectomy); and total capsulectomy, 1-cm partial labrectomy (total capsulectomy). Each hip was tested in a neutral position with a 20-N compressive force. The load at 12 mm of anterior translation was recorded for each state after 2 preconditioning trials.
Results:
A repeated-measures analysis of variance with Bonferroni adjustment showed no difference between the all-intact versus sutured-intact states and demonstrated no significant difference between the sutured-intact and sutured-labrectomy states. There were significant differences between the sutured-labrectomy and partial capsulectomy (P = .01), sutured-labrectomy and total capsulectomy (P < .001), and partial capsulectomy and total capsulectomy (P = .04) states.
Conclusion:
The findings demonstrate that the capsule/labrum plays an important role in anterior hip stability and that the iliofemoral ligament is crucial for preventing anterior translation in labral-injured states. In addition, the ischiofemoral and pubofemoral ligaments provide resistance to anterior translation in iliofemoral- and labral-deficient states. Intraoperative capsulectomy should be avoided in patients with large, irreparable labral tears to prevent postoperative anterior hip instability.
Clinical Relevance:
This study quantifies the roles of the capsulolabral structures in anterior hip stability and demonstrates the importance of maintaining/repairing them during hip arthroscopic surgery.
Keywords: hip biomechanics, hip arthroscopic surgery, capsulectomy, labrectomy, labral injury, iliofemoral ligament, ischiofemoral ligament, pubofemoral ligament, pelvis, cadaveric specimens
With the advent of hip arthroscopic surgery, the treatment of hip pain in the young adult athlete has changed dramatically. Labral tears and bony abnormalities such as femoroacetabular impingement can now be addressed without the need for an invasive open surgical dislocation procedure. Despite the advances in arthroscopic instrumentation, mobility inside the hip joint can be difficult because of its ball-and-socket configuration and extensive muscular and soft tissues surrounding the joint. In addition, arthroscopic visualization can be obstructed by the capsule, especially in patients with femoroacetabular abnormalities. As a result, hip arthroscopic surgeons are now performing extensive capsulotomy or partial capsulectomy during surgery to remove any barriers that increase surgical difficulty.5
Increased instability after hip capsulectomy has been described in the adult reconstructive literature.18,20 However, limited patient/clinical data have been reported regarding hip instability after hip arthroscopic surgery. Duplantier et al5 examined 11 patients with hip instability after hip arthroscopic surgery and reported predominantly anterior hip dislocations, as well as a high association with labral lesions, capsular insufficiency, and a failure to repair the capsulotomy site. Multiple isolated case reports or case series of postoperative instability after hip arthroscopic surgery have been published in the literature to date.2,12,13,15,16 In addition, several biomechanical studies have found increased instability after an anterior capsular injury.1,9,11,14 One study of a human cadaveric model investigated the impact of iliofemoral ligament separation and its effect on external and internal rotation during manual flexion and extension of the hip.11 The authors found that release of the medial and lateral arms of the iliofemoral ligament increased motion in external rotation, with the lateral arm having the greatest increase in flexion and a neutral position. Myers et al14 also evaluated hip joint stability using biplane fluoroscopy after serial capsulolabral sectioning in a human cadaveric model. They found increased external rotation and anterior translation in hips with iliofemoral ligament sectioning and capsulolabral-injured states compared to the intact state when a 5-N·m external and internal rotation torque force was applied to the hip. Abrams et al1 examined the effect of capsulotomy, capsulectomy, and repair of capsulotomy on external rotation. They demonstrated significantly increased external rotation with T-capsulotomy and capsulectomy compared to the intact hip, with no significant difference from the intact hip after repair of T-capsulotomy.1
To our knowledge, no evaluation of isolated anterior hip instability with increasing anterior capsulolabral injuries has been reported in the literature. The purpose of this study was to evaluate the impact of multiple anterior capsulolabral states (of increasing injury) on anterior hip stability. These anterior capsulolabral states included: (1) intact capsule, intact labrum (all intact); (2) sutured capsule, intact labrum (sutured intact); (3) sutured capsule, 1-cm partial labrectomy (sutured labrectomy); (4) partial capsulectomy, 1-cm partial labrectomy (partial capsulectomy); and (5) total capsulectomy, 1-cm partial labrectomy (total capsulectomy). Our hypothesis was that the load required for anterior hip translation would decrease as the injury to both the capsule and labrum increased.
Methods
Ten fresh-frozen human cadaveric pelvises (20 hips) with postmortem radiographic evidence of no degenerative joint disease, femoroacetabular impingement, or bony abnormalities (reviewed by the senior author [J.K.S.]) were harvested. The mean (±SD) donor age was 54.25 ± 11 years, with a range of 29 to 64 years. There were 5 female and 5 male donors. Two pelvises were not used, as there were problems with potting of one or both hips. For testing and analysis, 8 pelvises (16 hips) were used. To mark the neutral hip position, a screw was inserted into the greater trochanter positioned parallel to the epicondylar axis of the distal femur at the time of harvest. Pelvises were stored in a –20°F freezer until specimen preparation and potting.
To prepare the femur for potting, the bone was cut 6 cm distal to the lesser trochanter. The femoral canal was irrigated to remove all bone marrow tissue, and the remaining medullary canal was dried. A 6-inch metal screw (three-eighths–inch or one-half–inch diameter) was cemented into the canal using polymethyl methacrylate (PMMA). The screw diameter was selected on the basis of the diameter of the femoral canal to achieve the best fit and fill. An 8-cm polyvinyl chloride sleeve was placed around the femur and secured to the bone with 3 screws. This construct was cemented in place with PMMA to provide additional stability for the femoral construct.
The pelvis had 6-inch (three-eighths–inch diameter) metal screws drilled into the sacrum and ilium, which allowed a custom metal plate to be affixed to the back of the pelvis. For additional stability, 2 one-quarter–inch metal threaded rods were screwed into the iliac wings and attached to the metal plate.
During preparation, the pelvises were dissected of soft tissue to allow for potting and mounting plate fixation. Muscle and soft tissues surrounding the capsule were left intact during this phase to prevent desiccation. Immediately before testing, the pelvises were dissected of the remaining tissue, leaving the iliofemoral, pubofemoral, and ischiofemoral ligaments intact.
The construct was then mounted on a custom-designed testing apparatus (Figure 1). The pelvis was oriented in a neutral position with the pubic symphysis and anterior superior iliac spine (ASIS) perpendicular to the ground. The femur was placed in neutral adduction/abduction and assisted by using the angle between the shaft of the femur and a horizontal line in the ASIS/pubic symphysis plane. The angle between the shaft of the femur and a vertical line in the ASIS/pubic symphysis plane was used to place the femur in neutral flexion/extension. The screw placed in the greater trochanter at the time of harvest and a horizontal line in the ASIS/pubic symphysis plane were used to set neutral external/internal rotation. Once neutral positions for the pelvis and femur were achieved, the capsule was vented to remove the suction effect of the hip joint.9 A compressive load of 20 N was applied to the pelvis by placing counterweights on the back of the testing apparatus.
Figure 1.
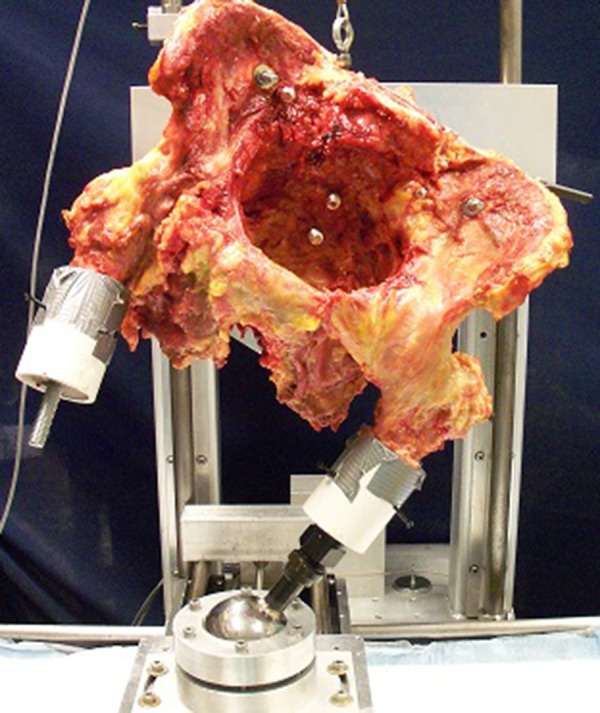
Cadaveric specimen mounted to the custom-built testing apparatus. The acetabulum was oriented parallel to the floor to allow an even compressive force across the joint similar to native muscular forces across the upright hip.
The custom testing apparatus recorded anterior-posterior displacement of the femur, superior-inferior displacement of the acetabulum, compressive force on the joint, and dislocation force at the joint. Measurements were taken using calibrated linear variable differential transformers: one 25 mm and one 50 mm. The loads were measured with a 200-N and 300-N load cell. All data were sampled at 100 Hz and recorded with LabVIEW (National Instruments) onto a desktop computer.
Ten trials were run for preconditioning of the specimen as well as for pilot testing before any data were collected. For pilot testing, the femur was anteriorly translated at a rate of 1 mm/s for a total translation of 13 mm. This amount of translation did not result in any plastic deformation to the specimen, soft tissue laxity, or decrease in load with repeated cycles. Each hip was tested using 5 conditions in sequential order: (1) intact capsule, intact labrum (all intact); (2) sutured capsule, intact labrum (sutured intact); (3) sutured capsule, 1-cm partial labrectomy (sutured labrectomy); (4) partial capsulectomy, 1-cm partial labrectomy (partial capsulectomy); and (5) total capsulectomy, 1-cm partial labrectomy (total capsulectomy). The all-intact state described the native hip state without any capsulolabral injury. The sutured capsule was created by performing longitudinal capsulotomy in the upper two-thirds of the iliofemoral ligament in line with the femoral neck, simulating interportal capsulotomy. This capsulotomy was performed 7 mm from the labrum to ensure adequate tissue for repair. The capsulotomy site was then repaired using braided, nonabsorbable No. 2.0 suture in an interrupted manner (Figure 2). The 1-cm partial labrectomy procedure was performed using a No. 15 scalpel blade at the 2:30-o’clock position on the labrum. Partial capsulectomy was performed by resecting the entire iliofemoral ligament from the acetabular rim to the intertrochanteric line, leaving the ischiofemoral and pubofemoral ligaments intact (Figure 3). The remaining capsular ligaments were then resected for the total capsulectomy state.
Figure 2.
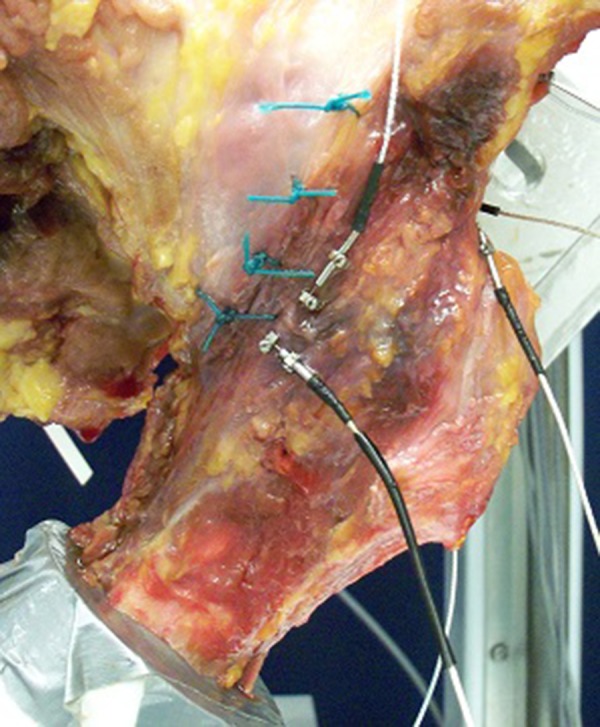
Sutured capsule with interrupted, nonabsorbable braided suture.
Figure 3.
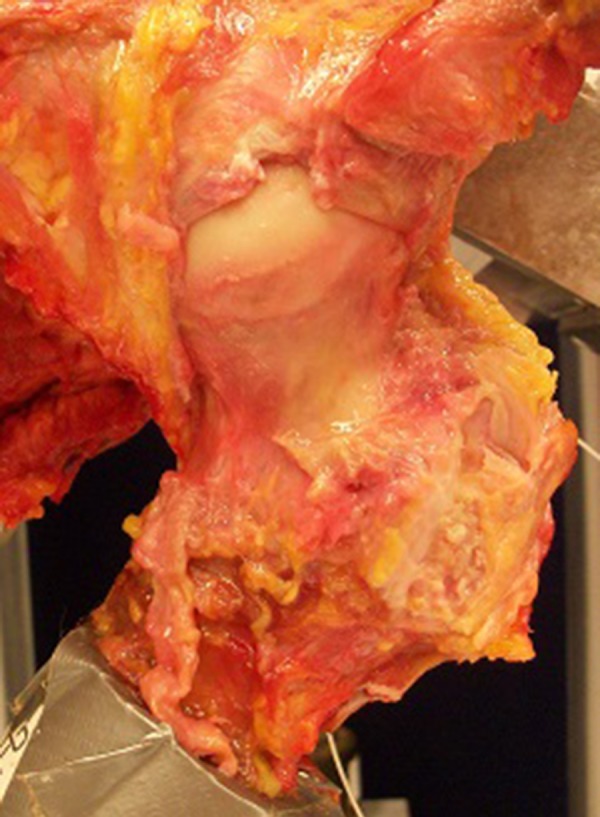
Partial capsulectomy with a resected iliofemoral ligament and 1-cm partial labrectomy.
For each condition, the hip underwent a preconditioning trial. Three data-recorded trials followed the preconditioning trial. Data analysis was performed on the second of the 3 trials. A custom-designed script in MATLAB (MathWorks) was used to identify the load at 12 mm of anterior femoral translation.
Statistical analysis was performed using SAS (SAS Institute). A repeated-measures analysis of variance, as well as paired, 2-tailed t tests, with Bonferroni correction was utilized to compare the 5 conditions. The significance level (alpha) was set at <0.05. A power analysis was performed for an alpha of <0.05 and a power of 0.8 and demonstrated the need for at least 16 hips.
Results
The mean load at 12 mm of anterior femoral translation for the all-intact condition was 160.8 ± 36.2 N. The sutured-intact condition and sutured-labrectomy condition had mean loads of 160.2 ± 39.6 N and 158.3 ± 38.5 N, respectively. A repeated-measures analysis of variance with Bonferroni adjustment was run to compare these 3 states and showed no significant difference among the 3 states (F 2,45 = 0.027, P = .97).
The mean load for the partial capsulectomy condition was found to be 122.8 ± 36.1 N, and 99.3 ± 35.9 N was the mean load for the total capsulectomy condition. These loads were found to be incrementally less than the mean load for the sutured-labrectomy condition. Paired, 2-tailed t tests with Bonferroni adjustment were run to compare these 3 different capsular conditions with 1-cm partial labrectomy (Figure 4). There was a significant difference between the sutured-labrectomy condition and partial capsulectomy condition (P = .01) and between the sutured-labrectomy condition and total capsulectomy condition (P < .001). There was also a significant difference when comparing the partial capsulectomy condition and total capsulectomy condition (P = .04).
Figure 4.

Mean force required for 12-mm anterior translation in the 5 tested conditions: intact capsule, intact labrum (all intact); sutured capsule, intact labrum (sutured intact); sutured capsule, 1-cm partial labrectomy (sutured labrectomy); partial capsulectomy, 1-cm partial labrectomy (partial capsulectomy); and total capsulectomy, 1-cm partial labrectomy (total capsulectomy).
Discussion
This study found a significant decline in the force required for anterior translation of the femur with resection of the iliofemoral ligament with 1-cm partial labrectomy compared to the sutured-labrectomy condition. Even after resection of the iliofemoral ligament, we still found that a 122-N force was required to translate the femur anteriorly compared to 99 N in the total capsulectomy state. This sequential resection of the hip capsular ligaments in our study demonstrated a linear decline in the force required for anterior translation (Figure 4). These results indicate that the ischiofemoral and pubofemoral ligaments do provide anterior stability to the hip joint after an injury to the labrum and iliofemoral ligament.
The first purpose of our study was to evaluate the role of the capsuloligamentous structures in providing anterior hip stability in a labral-injured state. No difference was found among the all-intact condition, sutured-intact condition, and sutured-labrectomy condition with regard to anterior translation. On the basis of these results, we concluded that the iliofemoral ligament plays a primary role in anterior hip stability in the labral-injured state. It provides a restraint to anterior translation when the stabilizing effect of the labrum has been lost. These results are corroborated by Myers et al,14 who demonstrated that sectioning of the iliofemoral ligament resulted in significantly greater anterior translation compared to intact and labral-injured states but showed no difference in anterior translation between the intact and labral-injured states (both of which had intact iliofemoral ligaments).
A secondary purpose of our study was to further elucidate the roles of the iliofemoral, ischiofemoral, and pubofemoral ligaments in providing anterior hip stability. In the present study, as well as others, the iliofemoral ligament has been shown to be a primary ligamentous restraint to anterior translation at the hip joint.6,7 On the other hand, the contributions of the ischiofemoral and pubofemoral ligaments to anterior hip stability are less established. Our study demonstrated, however, that the ischiofemoral and pubofemoral ligaments do play a role in anterior stabilization of the hip in an iliofemoral- and labral-deficient state. These biomechanical findings indicate that all 3 capsular ligaments interact to provide hip joint stability, and their roles are not as clearly defined as previously thought.6,7 Although the hip joint is an inherently stable joint because of its osseous structure, the capsular ligaments appear to interact in a complex manner to prevent instability, similar to the glenohumeral ligaments in the shoulder.
Warren et al19 described the circle concept of the shoulder in 1984. This concept postulated that glenohumeral joint stability is provided by static restraints and that opposing structures on each side of the joint provided stability. As a result, translation of the humeral head in one direction would result in tension on the opposite ligamentous structure. Thus, anterior subluxation or dislocation of the humeral head would cause an injury to both the anterior and posterior glenohumeral capsular structures. Although the soft tissue structures play a greater role in shoulder stability compared to the hip, our findings indicate that the hip ligaments interact in a comparable manner. Studies on biomechanical properties of the shoulder and hip have demonstrated many similarities, including near-equivalent midsubstance failure strain, tensile modulus, and maximum stress.3,6,8,10 In our study model, we found that sequential sectioning of the anterior structures did indeed partially destabilize this joint. With resection of the iliofemoral ligament, the remaining ligaments did provide resistance to anterior translation, similar to findings observed for the posterior glenohumeral ligament in anterior shoulder instability.
Recent biomechanical studies have examined the role of capsulolabral structures in anterior hip instability.4,17 Crawford et al4 demonstrated decreased hip stability with forces of distraction, rotation, and femoral head displacement with a 15-mm labral tear. Smith et al17 observed no significant difference in the stability ratio (peak dislocation force/compressive load) with a circumferential labral tear ≤3 cm. They did demonstrate a significant decrease in the stability ratio with 2-cm partial labrectomy. Although these studies were well planned and well executed, they only evaluated the labrum and did not assess the role of the capsule in hip stability. Abrams et al1 demonstrated significantly increased external rotation with T-capsulotomy and capsulectomy compared to the intact hip, with no significant difference from the intact hip after repair of T-capsulotomy. Although Abrams et al1 demonstrated the effect of capsulotomy and capsulectomy, they did not evaluate the role of labral injuries in anterior hip stability. In addition, they primarily assessed external rotation rather than anterior translation. Finally, Myers et al14 demonstrated that sectioning of the iliofemoral ligament resulted in significantly greater anterior translation compared to intact and labral-injured states when testing specimens in external and internal rotation. Myers et al14 showed no difference in anterior translation when comparing the intact and labral-injured states. This was a very well-executed study that assessed the effect of iliofemoral and labral injuries on anterior hip stability. However, Myers et al14 only evaluated the role of the iliofemoral ligament and did not assess the other capsuloligamentous structures.
Limitations
The patient population most likely to undergo excessive capsulectomy constitutes those with femoroacetabular impingement. Our cadaveric specimens were selected with normal hip morphology and joint surfaces. It is not known if the capsular composition changes with bony abnormalities. Although this study did evaluate the impact of capsulectomy in a postoperative setting, it evaluated the specimens at time zero in the recovery process. It did not address hip stability in the later recovery stages. Capsulectomy performed during surgery can vary in size and is difficult to reproduce in a cadaveric model. Although useful for comparison in the laboratory setting, a total capsulectomy state is unlikely and may not be clinically relevant in the hip arthroscopic setting. In addition, we sectioned the ischiofemoral and pubofemoral ligaments at the same time. As a result, the role of these ligaments in maintaining anterior hip stability cannot be evaluated individually. However, comparison between the total capsulectomy and partial capsulectomy states does clearly demonstrate that the ischiofemoral and pubofemoral ligaments (in conjunction) play a significant role in maintaining anterior hip stability. Furthermore, only 16 cadaveric hips were included in our study. Although this is a limited sample size, our study was adequately powered. Future studies should evaluate the size and location of the capsulectomy site and how this resection affects anterior hip stability.
Conclusion
The study findings demonstrate that both the capsule and labrum play important roles in providing anterior hip stability and that the iliofemoral ligament is crucial for preventing anterior translation in labral-injured states. In addition, the ischiofemoral and pubofemoral ligaments provide resistance to anterior translation in iliofemoral- and labral-deficient states. Intraoperative capsulectomy should be avoided in patients with large, irreparable labral tears to prevent postoperative anterior hip instability.
Footnotes
The authors declared that they have no conflicts of interest in the authorship and publication of this contribution.
Ethical approval was not sought for the present study.
References
- 1. Abrams GD, Hart MA, Takami K, et al. Biomechanical evaluation of capsulotomy, capsulectomy, and capsular repair on hip rotation. Arthroscopy. 2015;31(8):1511–1517. [DOI] [PubMed] [Google Scholar]
- 2. Benali Y, Katthagen BD. Hip subluxation as a complication of arthroscopic debridement. Arthroscopy. 2009;25(4):405–407. [DOI] [PubMed] [Google Scholar]
- 3. Bigliani LU, Keldar R, Flatow EL, Pollock RG, Mow VC. Glenohumeral stability: biomechanical properties of passive and active stabilizers. Clin Orthop Relat Res. 1996;330:13–30. [PubMed] [Google Scholar]
- 4. Crawford MJ, Dy CJ, Alexander JW, et al. The 2007 Frank Stinchfield Award: the biomechanics of the hip labrum and the stability of the hip. Clin Orthop Relat Res. 2007;465:16–22. [DOI] [PubMed] [Google Scholar]
- 5. Duplantier NL, McCulloch PC, Nho SJ, Mather RC, 3rd, Lewis BD, Harris JD. Hip dislocation or subluxation after hip arthroscopy: a systematic review. Arthroscopy. 2016;32(7):1428–1434. [DOI] [PubMed] [Google Scholar]
- 6. Hewitt J, Guilak F, Glisson R, Vail TP. Regional material properties of the human hip joint capsule ligaments. J Orthop Res. 2001;19:359–364. [DOI] [PubMed] [Google Scholar]
- 7. Hewitt JD, Glisson RR, Guilak F, Vail TP. The mechanical properties of the human hip capsule ligaments. J Arthoplasty. 2002;17(1):82–89. [DOI] [PubMed] [Google Scholar]
- 8. Hewitt JD, Guilak F, Glisson RR, Vail TP. Mechanical properties of the human hip joint capsule ligaments. Trans Orthop Res Soc. 1999;24:744. [DOI] [PubMed] [Google Scholar]
- 9. Ito H, Song Y, Lindsey DP, Safran MR, Giori NJ. The proximal hip joint capsule and the zona orbicularis contribute to hip joint stability in distraction. J Orthop Res. 2009;27:989–995. [DOI] [PubMed] [Google Scholar]
- 10. Itoi E, Grabowski JJ, Morrey BF, An KN. Capsular properties of the shoulder. Tohoku J Exp Med. 1993;171:203–210. [DOI] [PubMed] [Google Scholar]
- 11. Martin HD, Savage A, Braly BA, Palmer IJ, Beall DP, Kelly B. The function of the hip capsular ligaments: a quantitative report. Arthroscopy. 2008;24(2):188–195. [DOI] [PubMed] [Google Scholar]
- 12. Matsuda DK. Acute iatrogenic dislocation following hip impingement arthroscopic surgery. Arthroscopy. 2009;25(4):400–404. [DOI] [PubMed] [Google Scholar]
- 13. Mei-Dan O, McConkey MO, Brick M. Catastrophic failure of the hip arthroscopy due to iatrogenic instability: can partial division of the ligamentum teres and iliofemoral ligament cause subluxation? Arthroscopy. 2012;28(3):440–445. [DOI] [PubMed] [Google Scholar]
- 14. Myers CA, Register BC, Lertwanich P, et al. Role of the acetabular labrum and the iliofemoral ligament in hip stability: an in vitro biplane fluoroscopy study. Am J Sport Med. 2011;39 Suppl:85S–91S. [DOI] [PubMed] [Google Scholar]
- 15. Ranawat AS, McClincy M, Sekiya JK. Anterior dislocation of the hip after arthroscopy in a patient with capsular laxity of the hip: a case report. J Bone Joint Surg Am. 2009;91:192–197. [DOI] [PubMed] [Google Scholar]
- 16. Sansone M, Ahlden M, Jonasson P, Sward L, Eriksson T, Karlsson J. Total dislocation of the hip joint after arthroscopy and ileopsoas tenotomy. Knee Surg Sports Traumatol Arthrosc. 2013;21(2):420–423. [DOI] [PubMed] [Google Scholar]
- 17. Smith MV, Panchal HB, Ruberte Thiele RA, Sekiya JK. Effect of acetabular labrum tears on hip stability and labral strain in a joint compression model. Am J Sports Med. 2011;39 Suppl:103S–110S. [DOI] [PubMed] [Google Scholar]
- 18. Tsai SJ, Wang CT, Jiang CC. The effect of posterior capsule repair upon postoperative hip dislocation following primary total hip arthroplasty. BMC Musculoskelet Disord. 2008;9:1471–1477. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19. Warren RF, Kornblatt IB, Marchand R. Static factors affecting posterior shoulder stability. Orthop Trans. 1984;8:89–93. [Google Scholar]
- 20. White RE, Forness TJ, Allman JK, Junick DW. Effect of posterior capsular repair on early dislocation in primary total hip replacement. Clin Orthop Relat Res. 2001;(393):163–167. [DOI] [PubMed] [Google Scholar]