

Abstract
Background
Few studies have investigated physical activity (PA) and sedentary behavior (SB) in relation to fasting (FG) and 2-h postprandial plasma glucose (2hPG) levels and gestational diabetes mellitus (GDM); we investigated these associations among Asian pregnant women.
Methods
As part of the Growing Up in Singapore Towards healthy Outcomes cohort study, PA and SB (sitting and television times) were assessed by interviewer-administered questionnaire. During 75 g oral glucose tolerance tests at 26–28 weeks’ gestation we measured FG, 2hPG levels and GDM (FG ≥ 7.0 mmol/L and/or 2hPG ≥ 7.8 mmol/L). Associations were analysed by multiple linear and logistic regression.
Results
Among the 1083 women studied, 18.6% had GDM. SB was not associated with FG, 2hPG and GDM. Higher categories of PA were associated with lower 2hPG and a lower likelihood of GDM (p-trend < 0.05), but not with FG levels. Compared to insufficiently active women, highly active women had lower 2hPG levels [β (95% CI): -0.32 (−0.59, −0.05), p = 0.020) and were less likely to have GDM [OR: 0.56 (0.32–0.98), p = 0.040]. Stratified analysis revealed no associations among under/normal-weight women, but significant associations among overweight/obese women; in those with BMI ≥23 kg/m2, sufficiently active and highly active women were less likely to have GDM [OR: 0.52, (0.29–0.93), p = 0.028, and OR: 0.34, (0.15–0.77), p = 0.010, respectively].
Conclusion
Higher PA was associated with lower 2hPG levels and a lower prevalence of GDM, particularly in overweight/obese women. Further studies are warranted to confirm these findings, and to examine the effectiveness of PA promotion strategies for the prevention of gestational hyperglycemia.
Keywords: Physical activity, Sedentary behavior, Gestational diabetes mellitus, Maternal glucose levels, Pregnancy
Background
Gestational diabetes mellitus (GDM) is defined by the onset or first detection of any degree of glucose intolerance during pregnancy [1]. It has been reported that almost 17.8% of all pregnancies are affected by GDM [2]; this rate ranges from 1 to 25.5% depending on the population studied and the diagnostic tests performed [2, 3]. GDM is associated with a higher risk of complications for both mother and offspring, including caesarean section, preeclampsia, perinatal morbidity, including macrosomia, neonatal hypoglycemia and jaundice [4], and developing type 2 diabetes later in life for mothers and offspring [5]. This emphasises the importance of research on modifiable factors to prevent GDM.
Physical activity (PA) is one of the modifiable lifestyle factors known to have direct and indirect impacts on insulin sensitivity and glucose homeostasis [6–8]. At least 150 min of moderate intensity PA per week is recommended for healthy pregnant women [9, 10], in line with the World Health Organization (WHO) recommendation for health benefit in general adult populations [11, 12]. Evidence suggests that regular PA during pregnancy may be inversely associated with the risk of GDM [6, 13–20]. The literature also highlights the role of pre-pregnancy body mass index (BMI) as a strong predictor of GDM [21, 22]. However, to our knowledge few studies have examined the association between PA and GDM according to pre-pregnancy BMI and their results were inconsistent [23–25].
Engaging in prolonged sedentary behavior (SB) may have an effect on metabolic health regardless of PA [26]. SB is defined as any waking behavior in a sitting or reclining posture with less than or equal to 1.5 metabolic equivalent tasks (METs) of energy expenditure [27]. A recent meta-analysis reported that prolonged sedentary time is independently associated with deleterious health outcomes, including type 2 diabetes [28]. However, the influence of sedentary behavior (SB) during pregnancy on GDM is poorly understood and the results of existing studies are inconsistent [24, 29, 30].
The majority of previous studies on PA and SB have been conducted in Western populations [17, 23–25, 29, 30], and only a few studies have been conducted among Asian women [31, 32]. However, Asian populations appear to be at a higher risk of developing GDM [21, 33–35], highlighting the public health relevance of examining the association of PA and SB with GDM in Asian women. Moreover, previous studies have investigated the association of PA and SB with gestational glycaemia mainly based on an established glycemic level cut-off points for GDM diagnosis [36]. However, the international multicenter Hyperglycemia and Adverse Pregnancy Outcomes (HAPO) study reported that maternal fasting and stimulated glucose levels even below previous GDM cut-off points were linearly associated with increased adverse pregnancy and neonatal outcomes [37]. This suggests the need to additionally investigate continuous maternal glucose levels regardless of GDM cut-off points.
Based on the above evidence and gaps in the existing literature, we examined the associations of PA and SB during pregnancy with maternal glycemic levels and GDM among Asian women. Additionally, we investigated the magnitude of these associations according to pre-pregnancy BMI subgroups.
Methods
Study design and population
The Growing Up in Singapore Towards healthy Outcomes (GUSTO) mother-offspring cohort study recruited pregnant women attending their first-trimester antenatal dating ultrasound scan clinics at two major public maternity units in Singapore, KK Women’s and Children’s Hospital (KKH) and National University Hospital (NUH) from June 2009 to September 2010. Pregnant women aged 18 years and above, major ethnic groups (Chinese, Malay and Indian), Singapore citizen or permanent residents who had the intention of delivering in KKH/NUH and staying in Singapore for at least next 5 years, and who had agreed to donate their birth tissues were invited to participate in the study. Women who had type I diabetes mellitus, or who were receiving chemotherapy or psychotropic drugs were excluded. The GUSTO study was designed to investigate the early determinants of child health and development. More details on the study are available elsewhere [38, 39]. The study protocol was approved by the ethics committees of the hospitals involved: SingHealth Centralized Institutional Review Board and the National Healthcare Group Domain Specific Review Board in Singapore. All participants gave written informed consent.
Data collection
As part of interviewer-administered questionnaires at recruitment, women were asked about their age, ethnicity, educational level, pre-pregnancy weight, family history of diabetes, and maternal history of GDM in previous pregnancies. When seen at 26–28 weeks gestation, women were asked questions about cigarette smoking during pregnancy and whether they were exposed to cigarette smoking at home or in their workplace during pregnancy; answers were combined to determine active/passive cigarette smoking during pregnancy.
Participants’ dietary energy intake was ascertained based on a 24-h dietary recall; this was administered by trained interviewers at a face-to-face interview at 26–28 weeks of gestation. Various portion sizes of standardized household measuring utensils and food pictures were used to assist women in quantifying their food and beverage intake. Nutrient analysis software (Dietplan, version 7, Forestfield Software) with a food composition database of locally available foods was used to calculate total daily energy intake. Additionally, for food items not found in the database, nutrient information was obtained from food labels or the USDA national nutrient database [19].
Parity data was collected from hospital medical records. Height (to the nearest 0.1 cm) and weight (to 0.01 kg) were measured by trained research staff using a stadiometer (SECA model 213, Hamburg, Germany) and a weighing scale (SECA model 803), respectively. Self-reported pre-pregnancy weight, and height measured at the 26–28 weeks gestational visit were used to calculate pre-pregnancy BMI (kg/m2). BMI was categorized as underweight, normal weight, overweight and obese (<18.5, 18.5–23, 23–27.5 and ≥27.5, respectively) according to Asian cut-offs [40–42]. Gestational weight gain until 26–28 weeks was calculated by subtracting self-reported pre-pregnancy weight from the weight measured at 26–28 weeks’ gestation [43].
Assessment of maternal blood glucose concentrations
Participants underwent a 75-g oral glucose tolerance testing (OGTT) at 26–28 weeks’ gestation; overnight fasting (8–10 h) and 2-h postprandial blood specimens were collected. Colorimetry [Advia 2400 Chemistry system (Siemens Medical Solutions Diagnostics) and Beckman LX20 Pro analyzer (Beckman Coulter)] were used to measure both fasting glucose (FG) and 2-h postprandial glucose (2hPG) concentrations. Glucose concentrations were used to classify GDM according to the 1999 WHO standard criteria: ≥7.0 mmol/L for FG and/or ≥7.8 mmol/L for 2hPG [36, 44].
Assessment of physical activity and sedentary behavior
PA questions were part of a structured questionnaire administered by trained interviewers at 26–28 weeks’ gestation; the questionnaire included questions on physical activities during the past 6 months of pregnancy. The detailed measurement of PA and SB in the cohort has been reported elsewhere [45]. Briefly, total physical activities were categorized as light-moderate (leaves the person tired but not exhausted, e.g. walking, gardening and golf), moderate (leaves the person exhausted but not breathless, e.g. brisk walking, easy swimming and dancing) and vigorous intensity (makes the heart beat rapidly and leaves the person breathless, e.g. jogging, vigorous swimming, cycling and aerobics). The participants reported the frequency and duration of the three different intensity levels of all physical activities. Frequency was categorized in the questionnaire as never, once every 2–3 months, once a month, once a fortnight, 1–2 times per week, 3–6 times per week, once a day, and more than once a day. Based on these categories an average frequency per week was converted into 0, 0.1, 0.25, 0.5, 1.5, 4.5, 7, and 10.5 times per week, respectively. Women reported an average duration of each period of activity, and the answers were standardized to the nearest 0.5 h. Total hours spent in each intensity level of PA per week was derived by multiplying frequency per week and duration per episode.
An absolute metabolic equivalent task (MET) value was assigned for light-moderate, moderate and vigorous intensity activities (3.3, 4.0 and 8.0, respectively), adapted from the protocol for the International Physical Activity Questionnaire (IPAQ) short form, with 1.0 MET corresponding to resting energy expenditure [46]. Energy expended on each level of PA intensity in MET-hours per week was calculated by multiplying total hours spent on specific intensity per week with its corresponding MET value. Energy expended per week in all three PA intensity levels were summed to estimate total energy expenditure (TEE) on PA per week (light-moderate + moderate + vigorous MET-hours/week), which was then converted into MET-minutes per week. TEE on PA was categorized into insufficiently active (<600 MET-minutes/week), sufficiently active (600 to <3000 MET-minutes/week), and highly active (≥3000 MET-minutes/week). This approach is based on the WHO PA recommendation of a minimum of 600 MET-minutes per week for health benefits in adults [11, 12], and on the IPAQ definition of at least 3000 MET-minutes per week for highly active adults [46]. For example, women who engaged in 30 min of moderate intensity PA at least for 5 days per week were classified as sufficiently active, and women who additionally engaged in 120 min of light-moderate intensity PA daily were classified as highly active.
Sedentary behavior was determined by asking participants to report total sitting time per day during the past 6 months of pregnancy during an interview at 26–28 weeks of gestation; the answers were standardized to the nearest 0.5 h. A separate question determined time spent watching television per day; answers were categorized as none, less than an hour, 1–2 h, 2–3 h, 3–4 h, 4–5 h, and more than 5 h. Based on these categories, an average television viewing duration was converted into 0, 0.5, 1.5, 2.5, 3.5, 4.5 and 5.5 h per day, respectively. In the absence of cut-offs for SB, daily total sitting time during pregnancy was categorized into tertiles to define low, medium and high total sitting time (<7, 7–10, ≥10 h/day, respectively). Higher television viewing time per day during pregnancy was determined based on an upper tertile, which was ≥3 h per day in this sample. This category corresponds with the existing literature, in which 20 or more hours of television viewing time per week during pre-pregnancy has been associated with GDM [47].
Statistical analysis
Frequencies and percentages were calculated for categorical variables, and means and standard deviations for continuous variables. Differences between women with and without GDM were compared using an independent t-test for continuous variables and chi-square tests for categorical variables. Multivariable linear regression was used to investigate the associations of PA, total sitting time and television time with FG and 2hPG concentrations. Multivariable logistic regression was used to assess the associations of PA, total sitting time and television time with GDM. Based on the literature, models were adjusted for following confounders: maternal age, ethnicity, education, pre-pregnancy BMI (continuous), parity at recruitment, history of GDM in previous pregnancy, family history of diabetes, dietary energy intake, exposure to active/passive smoking during pregnancy and pregnancy weight gain at 26–28 gestational visit [24, 48–50]. Additionally, PA and total sitting time, and PA and television viewing time were mutually adjusted in separate models, to explore the independent associations of PA, total sitting time, and television viewing time with all outcome measures. The magnitude of these associations according to pre-pregnancy BMI subgroups was tested by stratifying regressions according to BMI subgroups, though the interaction between PA/SB and BMI subgroups on FG/2hPG/GDM was not statistically significant (p > 0.05). BMI subgroups were combined into two groups, under/normal weight and overweight/obese to enhance statistical power. Based on the observed standard deviations, a targeted statistical power of ≥80% and a type I error of 5%, our study is powered to detect differences of 0.05 and 0.14 mmol/L for fasting and 2-h glucose, respectively. For a subgroup of 100 participants, the differences that could be detected were 0.14 and 0.43 mmol/L, respectively. All association tests were two-tailed, and confidence intervals were calculated at the 95% level. All statistical analyses were performed using Statistical Package for the Social Sciences v19 (IBM, Chicago, IL, USA).
Results
There were 1236 women eligible for the study; among them, 1083 (87.6%) participants completed the OGTT and answered PA and SB questions and were thus included in the present analysis (Fig. 1). Excluded women were similar to included subjects in relation to their age, education, parity, BMI, history of GDM, family history of diabetes and dietary energy intake (p > 0.05), but they were more likely to be of Malay or Indian ethnicity (p = 0.033). In our sample 18.6% (n = 201) of the women had been diagnosed with GDM; these women were more likely to be older, of Indian ethnicity, highly educated, to have a higher BMI and a history of GDM and to not report active/passive smoking during pregnancy (p < 0.05) (Table 1).
Fig. 1.
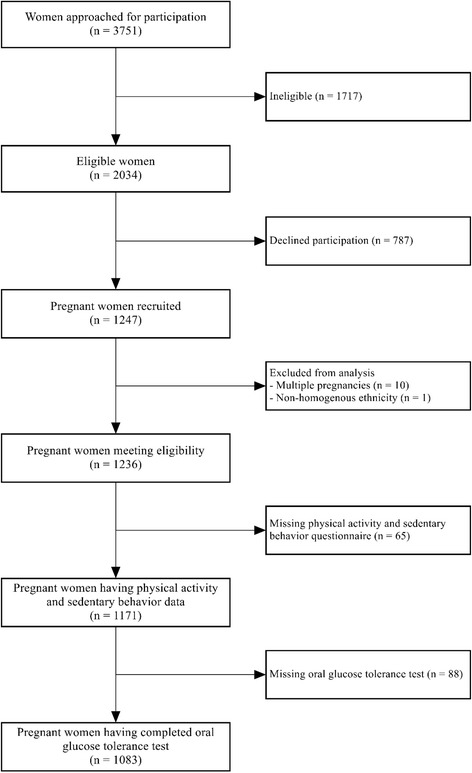
Study flow diagram
Table 1.
Characteristics of pregnant women according to GDM in the GUSTO cohort study (n = 1083)
| GDM absent n = 882 (81.4%) |
GDM present n = 201 (18.6%) |
p-value | |
|---|---|---|---|
| Mean age in years (SD) | 30.3 (5.1) | 32.5 (4.7) | <0.001 |
| Ethnicity (n, %) | 0.001 | ||
| Chinese | 494 (56.0) | 126 (62.7) | |
| Malay | 245 (27.8) | 31 (15.4) | |
| Indian | 143 (16.2) | 44 (21.9) | |
| Education (n, %) | 0.008 | ||
| No-formal/Primary/Secondary | 279 (31.6) | 46 (22.9) | |
| GCE ‘A’ levels/polytechnic/Diploma/Technical education | 312 (35.4) | 72 (35.8) | |
| University | 278 (31.5) | 83 (41.3) | |
| Missing data | 13 (1.5) | 0 (0.0) | |
| BMI in kg/m2 (n, %) | <0.001 | ||
| < 18.5 | 105 (11.9) | 16 (7.9) | |
| 18.5–23 | 431 (48.9) | 81 (40.3) | |
| 23.0–27.5 | 179 (20.3) | 54 (26.9) | |
| ≥ 27.5 | 97 (11.0) | 43 (21.4) | |
| Missing data | 70 (7.9) | 7 (3.5) | |
| Parity at recruitment (n, %) | 0.128 | ||
| 0 | 407 (46.1) | 85 (42.3) | |
| ≥ 1 | 463 (52.5) | 116 (57.7) | |
| Missing data | 12 (1.4) | 0 (0.0) | |
| History of GDM (n, %) | |||
| No | 834 (94.6) | 181 (90.0) | <0.001 |
| Yes | 18 (2.0) | 18 (9.0) | |
| Missing data | 30 (3.4) | 2 (1.0) | |
| Family history of diabetes (n, %) | |||
| No | 603 (68.4) | 133 (66.2) | 0.072 |
| Yes | 253 (28.7) | 67 (33.3) | |
| Missing data | 26 (2.9) | 1 (0.5) | |
| Dietary energy intake in kcal (Mean, SD) | 1881.3 (604.5) | 1815.2 (520.7) | 0.118 |
| Missing data (n,%) | 6 (0.7) | 2 (1.0) | |
| Active/ passive smoking during pregnancy (n, %) | 0.001 | ||
| No | 503 (57.0) | 138 (68.6) | |
| Yes | 350 (39.7) | 52 (25.9) | |
| Missing data | 29 (3.3) | 11 (5.5) | |
| Pregnancy weight gain at week 26–28 (Mean, SD) | 8.7 (4.5) | 8.0 (4.4) | 0.061 |
| Missing (n,%) | 79 (9.0) | 7 (3.5) | |
| Physical activity during pregnancy (n, %) | 0.125 | ||
| Insufficiently active | 289 (32.8) | 78 (38.8) | |
| Sufficiently active | 415 (47.1) | 95 (47.3) | |
| Highly active | 167 (18.9) | 25 (12.4) | |
| Missing data | 11 (1.2) | 3 (1.5) | |
| Total sitting time during pregnancy (n, %) | 0.193 | ||
| Low (<7 h/day) | 252 (28.6) | 43 (21.4) | |
| Medium (7–10 h/day) | 239 (27.1) | 62 (30.8) | |
| High (≥10 h/day) | 389 (44.1) | 95 (47.3) | |
| Missing data | 2 (0.2) | 1 (0.5) | |
| Total television viewing time (n, %) | 0.066 | ||
| Low (<3 h/day) | 593 (67.2) | 142 (70.6) | |
| High (≥3 h/day) | 289 (32.8) | 58 (28.9) | |
| Missing data | 0 (0.0) | 1 (0.5) |
GDM gestational diabetes mellitus, SD, standard deviation, GCE ‘A’ levels General Certificate of Education-Advance levels, BMI body mass index
p-values were determined by Chi-square or independent t-test
Associations of PA and SB during pregnancy with maternal blood glucose levels
PA and television time during pregnancy were not significantly associated with FG levels in the overall sample and in BMI subgroups (Table 2). Total sitting time was inversely associated with FG levels in the unadjusted model (overall p = 0.029; p for trend =0.035), however, after adjustment this was attenuated with no linear trend (overall p = 0.074; p for trend = 0.183). Associations with 2hPG are shown in Table 3. Higher PA during pregnancy was associated with lower 2hPG (p for trend = 0.016). Compared with insufficiently active women, highly active women had lower 2hPG levels [β (95% CI): -0.32 (−0.59, −0.05), p = 0.020]. However, a sufficient level of PA was not significantly associated with 2hPG levels [β: −0.16 (−0.37, 0.04), p = 0.116]. Stratified analysis revealed associations only among overweight/obese women, but not among underweight/normal weight women (β: −0.51 (−1.00, −0.01), p = 0.044, and −0.17 (−0.49, 0.15), p = 0.291, respectively).
Table 2.
Associations of physical activity and sedentary behavior with fasting glucose levels (mmol/l) during pregnancy in the GUSTO study
| Variables | Overall sample | Underweight/Normal weight | Overweight/obese | P for interaction | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| n | Unadjusted | Adjusteda | Adjustedb | Adjustedb | ||||||||
| β (95% CI) | P-value | β (95% CI) | P-value | n | β (95% CI) | P-value | n | β (95% CI) | P-value | |||
| Physical activity | 0.759 | 0.806 | 0.525 | 0.863 | 0.933 | |||||||
| Insufficiently active | 325 | Reference | Reference | 202 | Reference | 123 | Reference | |||||
| Sufficiently active | 436 | 0.01 (−0.06, 0.08) | 0.822 | 0.01 (−0.06, 0.08) | 0.754 | 284 | 0.03 (−0.03, 0.10) | 0.321 | 152 | −0.001 (−0.15, 0.15) | 0.988 | |
| Highly active | 160 | 0.04 (−0.06, 0.13) | 0.463 | 0.03 (−0.06, 0.12) | 0.512 | 99 | 0.04 (−0.05, 0.13) | 0.350 | 61 | 0.05 (−0.15, 0.25) | 0.631 | |
| p for trend | 0.492 | 0.520 | 0.286 | 0.681 | ||||||||
| Total sitting time | 0.029 | 0.074 | 0.106 | 0.202 | 0.457 | |||||||
| Low (<7 h/day) | 251 | Reference | Reference | 153 | Reference | 98 | Reference | |||||
| Medium (7–10 h/day) | 265 | 0.02 (−0.06, 0.11) | 0.627 | 0.04 (−0.04, 0.13) | 0.304 | 160 | 0.06 (−0.01, 0.14) | 0.111 | 105 | 0.002 (−0.17, 0.18) | 0.980 | |
| High (≥10 h/day) | 417 | −0.07 (−0.15, 0.003) | 0.060 | −0.04 (−0.12, 0.04) | 0.285 | 277 | −0.01 (−0.08, 0.06) | 0.843 | 140 | −0.13 (−0.30, 0.04) | 0.144 | |
| p for trend | 0.035 | 0.183 | 0.598 | 0.119 | ||||||||
| Television time | 0.446 | 0.367 | 0.134 | 0.791 | 0.399 | |||||||
| Low (<3 h/day) | 640 | Reference | Reference | 411 | Reference | 229 | Reference | |||||
| High (≥3 h/day) | 294 | 0.03 (−0.04, 0.09) | 0.03 (−0.04, 0.10) | 180 | 0.05 (−0.02, 0.11) | 114 | −0.02 (−0.17, 0.13) | |||||
β beta-coefficient, CI confidence interval, BMI body mass index
AaAdjusted for maternal age, ethnicity, education, pre-pregnancy BMI, parity at recruitment, history of GDM in previous pregnancy, family history of diabetes, dietary energy intake, active/passive smoking during pregnancy and pregnancy weight gain at 26–28 gestational visit
BbAdjusted for maternal age, ethnicity, education, parity at recruitment, history of GDM in previous pregnancy, family history of diabetes, dietary energy intake, active/passive smoking during pregnancy and pregnancy weight gain at 26–28 gestational visit
p-values were determined by multivariable linear regression
Table 3.
Associations of physical activity and sedentary behavior with 2-h-postprandial glucose levels (mmol/l) during pregnancy in the GUSTO study
| Variables | Overall sample | Underweight/Normal weight | Overweight/obese | P for interaction | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| n | Unadjusted | Adjusteda | Adjustedb | Adjustedb | ||||||||
| β (95% CI) | P-value | β (95% CI) | P-value | n | β (95% CI) | P-value | n | β (95% CI) | P-value | |||
| Physical activity | 0.032 | 0.056 | 0.570 | 0.109 | 0.607 | |||||||
| Insufficiently active | 325 | Reference | Reference | 202 | Reference | 123 | Reference | |||||
| Sufficiently active | 436 | −0.13 (−0.35, 0.08) | 0.222 | −0.16 (−0.37, 0.04) | 0.116 | 284 | −0.07 (−0.31, 0.17) | 0.576 | 152 | −0.28 (−0.66, 0.10) | 0.152 | |
| Highly active | 160 | −0.38 (−0.67, −0.10) | 0.009 | −0.32 (−0.59, −0.05) | 0.020 | 99 | −0.17 (−0.49, 0.15) | 0.291 | 61 | −0.51 (−1.00, −0.01) | 0.044 | |
| p for trend | 0.010 | 0.016 | 0.295 | 0.036 | ||||||||
| Total sitting time | 0.091 | 0.172 | 0.082 | 0.885 | 0.547 | |||||||
| Low (<7 h/day) | 251 | Reference | Reference | 153 | Reference | 98 | Reference | |||||
| Medium (7–10 h/day) | 265 | 0.25 (−0.01, 0.52) | 0.056 | 0.23 (−0.02, 0.47) | 0.073 | 160 | 0.31 (0.02, 0.60) | 0.037 | 105 | 0.10 (−0.34, 0.55) | 0.652 | |
| High (≥10 h/day) | 417 | 0.24 (0.001, 0.48) | 0.049 | 0.17 (−0.06, 0.40) | 0.137 | 277 | 0.25 (−0.01, 0.52) | 0.062 | 140 | 0.02 (−0.41, 0.45) | 0.931 | |
| p for trend | 0.069 | 0.189 | 0.099 | 0.971 | ||||||||
| Television time | 0.284 | 0.649 | 0.925 | 0.571 | ||||||||
| Low (<3 h/day) | 640 | Reference | Reference | 411 | Reference | 229 | Reference | 0.363 | ||||
| High (≥3 h/day) | 294 | −0.11 (−0.32, 0.10) | 0.05 (−0.15, 0.25) | 180 | −0.01 (−0.25, 0.23) | 114 | 0.11 (−0.26, 0.47) | |||||
β beta-coefficient, CI confidence interval, BMI body mass index
AaAdjusted for maternal age, ethnicity, education, pre-pregnancy BMI, parity at recruitment, history of GDM in previous pregnancy, family history of diabetes, dietary energy intake, active/passive smoking during pregnancy and pregnancy weight gain at 26–28 gestational visit
bbAdjusted for maternal age, ethnicity, education, parity at recruitment, history of GDM in previous pregnancy, family history of diabetes, dietary energy intake, active/passive smoking during pregnancy and pregnancy weight gain at 26–28 gestational visit
p-values were determined by multivariable linear regression
Compared to women with low sitting time, women with high sitting time had significantly higher 2hPG levels; this association was no longer apparent after adjusting for potential confounders in the overall sample [unadjusted β 95% CI: 0.24 (0.001, 0.48), p = 0.049, adjusted β: 0.17 (−0.06, 0.40), p = 0.137; p for trend = 0.189]. Among under/normal weight women, those categorized as having medium and high sitting time had higher 2hPG as compared to women with low sitting time [adjusted β 95% CI: 0.31, (0.02, 0.60), p = 0.037, and 0.25 (−0.01, 0.52), p = 0.062, respectively]; however, there was no linear association (p for trend = 0.099). Sitting time was not associated with 2hPG among overweight/obese women. Television time during pregnancy was not associated with the 2hPG level.
Associations of PA and SB with GDM
Table 4 shows that PA during pregnancy was inversely associated with the likelihood of having GDM (p for trend = 0.041): compared with insufficiently active women, highly active women were less likely to have GDM [adjusted OR (95% CI): 0.56 (0.32–0.98), p = 0.040]. However, a sufficient level of PA was not associated with GDM in the overall sample (OR: 0.82 (0.56–1.20), p = 303). Among overweight/obese women, sufficiently active and highly active women during pregnancy were less likely to have GDM as compared to insufficiently active women [adjusted OR: 0.52 (0.29–0.93), p = 0.028, and 0.34 (0.15–0.77), p = 0.010, respectively; p for trend = 0.004]. Among under/normal weight women on the other hand, PA during pregnancy was not associated with GDM [OR: 1.18 (0.71–1.98), p = 0.526, and 0.89 (0.42–1.90), p = 0.766, for sufficiently and highly active women, respectively]. Compared to women in the low sitting time group, women in the medium and high sitting groups had increased odds of having GDM, but this was not statistically significant [OR: 1.45 (0.90, 2.34), p = 131 and 1.42 (0.90, 2.22), p = 131, respectively]. There was no evidence for associations of television viewing time with GDM.
Table 4.
Associations of physical activity and sedentary behavior during pregnancy with GDM in the GUSTO study
| Variables | Overall sample | Underweight/Normal weight | Overweight/obese | P for interaction | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Cases n (%) |
Unadjusted | Adjusteda | Adjustedb | Adjustedb | ||||||||
| OR (95% CI) | P-value | OR (95% CI) | P-value | Cases n (%) |
OR (95% CI)a | P-value | Cases n (%) |
OR (95% CI)a | P-value | |||
| Physical activity | 0.107 | 0.118 | 0.673 | 0.015 | 0.098 | |||||||
| Insufficiently active | 71 (21.8) | 1.0 | 1.0 | 30 (14.9) | 1.0 | 41 (33.3) | 1.0 | |||||
| Sufficiently active | 86 (19.7) | 0.88 (0.62, 1.25) | 0.475 | 0.82 (0.56, 1.20) | 0.303 | 50 (17.6) | 1.18 (0.71, 1.98) | 0.526 | 36 (23.7) | 0.52 (0.29, 0.93) | 0.028 | |
| Highly active | 22 (13.8) | 0.57 (0.34, 0.96) | 0.035 | 0.56 (0.32, 0.98) | 0.040 | 12 (12.1) | 0.89 (0.42, 1.90) | 0.766 | 10 (16.4) | 0.34 (0.15, 0.77) | 0.010 | |
| p for trend | 0.045 | 0.041 | 0.975 | 0.004 | ||||||||
| Total sitting time | 0.197 | 0.246 | 0.532 | 0.304 | 0.660 | |||||||
| Low (<7 h/day) | 39 (15.5) | 1.0 | 1.0 | 19 (12.4) | 1.0 | 20 (20.4) | 1.0 | |||||
| Medium (7–10 h/day) | 55 (20.8) | 1.42 (0.91, 2.24) | 0.126 | 1.45 (0.90, 2.34) | 0.131 | 24 (15.0) | 1.29 (0.65, 2.56) | 0.476 | 31 (29.5) | 1.71 (0.86, 3.40) | 0.123 | |
| High (≥10 h/day) | 87 (20.9) | 1.43 (0.95, 2.17) | 0.089 | 1.42 (0.90, 2.22) | 0.131 | 49 (17.7) | 1.42 (0.77, 2.63) | 0.261 | 38 (27.1) | 1.38 (0.71, 2.69) | 0.341 | |
| p for trend | 0.114 | 0.172 | 0.271 | 0.438 | ||||||||
| Television time | 0.287 | 0.885 | 0.248 | 0.304 | 0.052 | |||||||
| Low (<3 h/day) | 130 (20.3) | 1.0 | 1.0 | 73 (17.8) | 1.0 | 57 (24.9) | 1.0 | |||||
| High (≥3 h/day) | 51 (17.3) | 0.82 (0.58, 1.18) | 1.03 (0.70, 1.51) | 19 (10.6) | 0.71 (0.40, 1.26) | 32 (28.1) | 1.33 (0.77, 2.29) | |||||
GDM gestational diabetes mellitus, BMI body mass index, OR odds ratio, CI confidence interval
AaAdjusted for maternal age, ethnicity, education, pre-pregnancy BMI, parity at recruitment, history of GDM in previous pregnancy, family history of diabetes, dietary energy intake, active/passive smoking during pregnancy and pregnancy weight gain at 26–28 gestational visit
BbAdjusted for maternal age, ethnicity, education, parity at recruitment, history of GDM in previous pregnancy, family history of diabetes, dietary energy intake, active/passive smoking during pregnancy and pregnancy weight gain at 26–28 gestational visit
p-values were determined by multivariable logistic regression
The findings were substantively similar in terms of magnitude and statistical significance after PA and total sitting time, and PA and television viewing time were mutually adjusted in separate models to examine independent associations of PA, total sitting time and television time with FG and 2hPG levels and GDM (data not shown).
Discussion
In our study, levels of PA were inversely associated with 2hPG levels and the likelihood of having GDM, but not with FG levels. Compared to insufficiently active women, highly active women had lower 2hPG levels and were less likely to develop GDM. These associations were stronger among overweight/obese women; compared to insufficiently active women, sufficiently and highly active women were less likely to have GDM. Total sitting time was not associated with FG and 2hPG level, or with GDM. Some possible differences between the BMI subgroups were noted, but they were not consistent and require further investigation. Television viewing time was also not associated with glucose levels and GDM.
Our study in a multi-ethnic Asian population generally supports results of a previous meta-analysis reporting inverse associations between PA during pregnancy and risk of developing GDM [6]. Demspsy et al., observed similar results, indicating that women who engaged in any recreational PA during pregnancy experienced a 48% reduction in GDM risk compared with inactive women [49]. There are a limited number of observational studies that examined the association of PA and maternal glucose concentration in the absence of GDM [24, 32]. Chasen-Taber et al. reported a 50% lower risk of abnormal glucose tolerance among women with high levels of moderate-intensity activity as compared with women in the lowest quartile during pregnancy [32]. Higher levels of PA were associated with a lower 2hPG level in our study, which indicates the importance of PA on glucose tolerance in pregnant women; as a consequence it may also have an effect in preventing adverse pregnancy outcome. For instance, two United Kingdom (UK) cohort studies have reported that higher maternal glucose levels within the non-diabetes range were consistently related to adverse pregnancy outcome [51].
The stratified analysis further highlights that these associations were mainly observed in overweight/obese women. Pre-pregnancy BMI may be an effect modifier for the association of level of PA with glucose concentration and GDM. However, this effect was evaluated in only four previous studies [24, 25, 49, 52]. In contrast to our results, the majority of previous studies indicated either no difference in the association between PA and GDM according to maternal BMI [49] or that the association was only found among women with a pre-pregnancy BMI of <25 kg/m2 [24]. Deierlein AL et al. reported that women with a pre-pregnancy BMI of <25 kg/m2 who engaged in any recreational moderate and vigorous physical activities during pregnancy had a 48% reduced risk of hyperglycemia compared to women who reported no moderate and vigorous activity [52]. The inconsistency between studies might be related to methodological issues, such as study design, population and assessment methods, but also highlights the need for further investigation of these observations. A potential biological mechanism behind the observed associations may be that skeletal muscle contraction as a result of PA may trigger glucose uptake and promote insulin sensitivity [24, 53]. PA-induced reductions in fat mass and increases in muscle mass may also lead to improved glucose tolerance and increased insulin sensitivity. Adipose tissue may also play a significant role in glucose clearance in physically active individuals, especially in obese individuals where this tissue can be considerable enough to contribute to improved glucose metabolism following physical training [49].
In our study, there was no evidence for an association of sedentary behavior with glucose levels and GDM. Nonetheless, we observed consistent increased odds of having GDM in women sitting for ≥7 h/day, but this was not led to statistical significant, which may be due to a lack of statistical power. A previous study that used television viewing time as one of the measures of sedentary behavior also reported no association with abnormal glucose tolerance and GDM risk [24], while another study found that longer sitting time was associated a with higher risk of developing gestational diabetes [30]. These inconsistencies warrant further research.
GUSTO is the first multi-ethnic birth cohort study in Asia investigating the associations of PA, total sitting time and television time during pregnancy with blood glucose levels and GDM. PA and SB data were collected as part of a structured questionnaire, administered by trained interviewers to mitigate the likelihood of systematic reporting errors. Standardized objective methods were used to quantify maternal blood glucose levels, and to determine GDM. Nevertheless, limitations of our study should be considered when interpreting our findings. Firstly, PA and SB data were limited to subjects’ self-reports with potential recall bias due to their complexity, and the questionnaire has not been validated locally against objective methods. Hence, some women might have misclassified their PA intensity categories. Secondly, assigned MET values and categorization of total MET values are suggested for an adult, and not specifically for pregnant women. However, we believe that the magnitude of imprecision is acceptable as the PA assessment was restricted to the first two trimesters of pregnancy. Thirdly, the prevalence of GDM was determined by 1999 WHO diagnostic criteria because only FG and 2hPG data were available, and more recent definitions could not be applied [36]. However, this study also examined the associations of PA and SB with maternal glucose concentrations, which are not influenced by these cut-off criteria for diagnosis. Fourthly, pre-pregnancy BMI was derived from self-reported weight which might have led to misclassification of some women in BMI categories. However, the literature suggests that pre-pregnancy BMI category by self-reported and measured weight are identical for most women [54] Finally, the generalizability of our results is limited because our cohort was not representative of the general Singaporean population [39].
Conclusions
PA was inversely associated with 2hPG levels and GDM, but not associated with FG levels. Highly active women during pregnancy had significantly lower levels of 2hPG and were less likely to be diagnosed with GDM, especially among those who were overweight/obese. Overweight/obese women with the minimum recommended or higher levels of PA were less likely to have GDM. In contrast, there was little evidence of an association between SB (total sitting time or TV viewing time) and glucose levels in our study. These findings suggest the importance of recommending or maintaining sufficiently high levels of physical activity during pregnancy to reduce the risk of adverse pregnancy outcomes for mothers and their offspring due to hyperglycemia. More prospective longitudinal studies and further trials are warranted, combining subjective and objective assessment of PA and SB with activity specific information, and more precise assessment of GDM, to confirm these findings. This knowledge will help to develop more effective health promotion strategies to prevent hyperglycemia among Asian women.
Acknowledgments
We would like to thank GUSTO study group, operational managers, research fellows, study coordinators and data management team. We greatly appreciate the voluntary participation of all participants and cooperation of maternity units in KK Women’s and Children’s Hospital and National University Hospital and their staff. The GUSTO study group includes Allan Sheppard, Amutha Chinnadurai, Anne Eng Neo Goh, Anne Rifkin-Graboi, Anqi Qiu, Arijit Biswas, Bee Wah Lee, Birit F.P. Broekman, Boon Long Quah, Borys Shuter, Chai Kiat Chng, Cheryl Ngo, Choon Looi Bong, Christiani Jeyakumar Henry, Cornelia Yin Ing Chee, Yam Thiam Daniel Goh, Doris Fok, Fabian Yap, George Seow Heong Yeo, Helen Chen, Hugo P S van Bever, Iliana Magiati, Inez Bik Yun Wong, Ivy Yee-Man Lau, Jeevesh Kapur, Jenny L. Richmond, Joanna D. Holbrook, Joshua J. Gooley, Kok Hian Tan, Krishnamoorthy Niduvaje, Leher Singh, Lin Lin Su, Lourdes Mary Daniel, Lynette Pei-Chi Shek, Marielle V. Fortier, Mark Hanson, Mary Foong-Fong Chong, Mary Rauff, Mei Chien Chua, Michael Meaney, Mya Thway Tint, Neerja Karnani, Ngee Lek, Oon Hoe Teoh, P. C. Wong, Pratibha Agarwal, Rob M. van Dam, Salome A. Rebello, Shang Chee Chong, Shu-E Soh, Sok Bee Lim, Chin-Ying Stephen Hsu, Victor Samuel Rajadurai, Walter Stunkel, Wee Meng Han, Wei Wei Pang, Yin Bun Cheung, Yiong Huak Chan and Yung Seng Lee.
Funding
This research is supported by the Singapore National Research Foundation under its Translational and Clinical Research (TCR) Flagship Programme and administered by the Singapore Ministry of Health’s National Medical Research Council (NMRC), Singapore- NMRC/TCR/004-NUS/2008; NMRC/TCR/012-NUHS/2014. Additional funding is provided by the Singapore Institute for Clinical Sciences, Agency for Science Technology and Research (A*STAR), Singapore. KMG is supported by the National Institute for Health Research through the NIHR Southampton Biomedical Research Centre and by the European Union’s Seventh Framework Programme (FP7/2007–2013), projects EarlyNutrition and ODIN under grant agreement numbers 289,346 and 613,977. JKYC received salary support from the Ministry of Health’s National Medical Research Council, Singapore (NMRC/CSA/043/2012).
Availability of data and materials
The datasets generated for this study are stored in the repository belonging to the Growing Up in Singapore Towards healthy Outcomes (GUSTO). The data are not publicly available online, but they can be obtained upon request through the corresponding author.
Abbreviations
- 2hPG
2-h postprandial glucose
- BMI
Body mass index
- CI
Confidence interval
- FG
Fasting glucose
- GDM
Gestational diabetes mellitus
- GUSTO
Growing Up in Singapore Towards healthy Outcomes
- IPAQ
International Physical Activity Questionnaire
- KKH
KK Women’s and Children’s Hospital
- MET
metabolic equivalent tasks
- NUH
National University Hospital
- OGTT
Oral Glucose Tolerance Testing
- OR
Odds ratio
- PA
Physical activity
- SB
Sedentary behavior
- UK
United Kingdom
- WHO
World Health Organization
Authors’ contributions
Conceived and designed the experiments: KK, PDG, KMG, SMS and YSC. Performed the experiments: ISZ and NP. Analyzed the data: NP, JYB, FMR, SL, SLL, SC and JKYC. Wrote the paper: NP, JYB and FMR. All authors read and approved the final manuscript.
Ethics approval and consent to participate
The study protocol was approved by the ethics committees of the hospitals involved: SingHealth Centralized Institutional Review Board and National Healthcare Group Domain Specific Review Board in Singapore. All participants gave written informed consent.
Consent for publication
All participants gave written consent to publish the data collected.
Competing interests
PDG, KMG and YSC report receiving reimbursement for speaking at conferences sponsored by companies selling nutritional products. PDG, KMG and YSC report being part of an academic consortium that has received research funding from Abbott Nutrition, Nestle and Danone. No other disclosures were reported. This does not alter the authors’ adherence to BMC policies on sharing data and materials.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Contributor Information
Natarajan Padmapriya, Email: obgnp@nus.edu.sg.
Jonathan Y. Bernard, Email: Jonathan_Bernard@sics.a-star.edu.sg
Shen Liang, Email: liang_shen@nuhs.edu.sg.
See Ling Loy, Email: Loy.See.Ling@kkh.com.sg.
Shirong Cai, Email: obgcais@nus.edu.sg.
Iris Shen Zhe, Email: iris_shen@nuhs.edu.sg.
Kenneth Kwek, Email: kenneth.Kwek.YC@kkh.com.sg.
Keith M. Godfrey, Email: kmg@mrc.soton.ac.uk
Peter D. Gluckman, Email: pd.gluckman@auckland.ac.nz
Seang Mei Saw, Email: seang_mei_saw@nuhs.edu.sg.
Yap-Seng Chong, Email: yap_seng_chong@nuhs.edu.sg.
Jerry Kok Yen Chan, Email: jerrychan@duke-nus.edu.sg.
Falk Müller-Riemenschneider, Email: falk.mueller-riemenschneider@nuhs.edu.sg.
on behalf of the GUSTO Study Group:
Allan Sheppard, Amutha Chinnadurai, Anne Eng Neo Goh, Anne Rifkin-Graboi, Anqi Qiu, Arijit Biswas, Bee Wah Lee, Birit F. P. Broekman, Boon Long Quah, Borys Shuter, Chai Kiat Chng, Cheryl Ngo, Choon Looi Bong, Christiani Jeyakumar Henry, Cornelia Yin Ing Chee, Yam Thiam Daniel Goh, Doris Fok, Fabian Yap, George Seow Heong Yeo, Helen Chen, Hugo P. S. van Bever, Iliana Magiati, Inez Bik Yun Wong, Ivy Yee-Man Lau, Jeevesh Kapur, Jenny L. Richmond, Joanna D. Holbrook, Joshua J. Gooley, Kok Hian Tan, Krishnamoorthy Niduvaje, Leher Singh, Lin Lin Su, Lourdes Mary Daniel, Lynette Pei-Chi Shek, Marielle V. Fortier, Mark Hanson, Mary Foong-Fong Chong, Mary Rauff, Mei Chien Chua, Michael Meaney, Mya Thway Tint, Neerja Karnani, Ngee Lek, Oon Hoe Teoh, P. C. Wong, Pratibha Agarwal, Rob M. van Dam, Salome A. Rebello, Shang Chee Chong, Shu-E Soh, Sok Bee Lim, Chin-Ying Stephen Hsu, Victor Samuel Rajadurai, Walter Stunkel, Wee Meng Han, Wei Wei Pang, Yin Bun Cheung, Yiong Huak Chan, and Yung Seng Lee
References
- 1.The Expert Committee on the Diagnosis Classification of Diabetes Mellitus Report of the expert committee on the diagnosis and classification of diabetes mellitus. Diabetes Care. 2003;26(Supplement 1):S5–S20. doi: 10.2337/diacare.26.2007.S5. [DOI] [PubMed] [Google Scholar]
- 2.Sacks DA, Hadden DR, Maresh M, Deerochanawong C, Dyer AR, Metzger BE, Lowe LP, Coustan DR, Hod M, Oats JJ, et al. Frequency of gestational diabetes mellitus at collaborating centers based on IADPSG consensus panel-recommended criteria: the hyperglycemia and adverse pregnancy outcome (HAPO) study. Diabetes Care. 2012;35(3):526–528. doi: 10.2337/dc11-1641. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.American Diabetes A. Diagnosis and classification of diabetes mellitus. Diabetes Care. 2014, 37 Suppl 1(1):S81-S90. [DOI] [PubMed]
- 4.Samoa R, Fujimoto W, Wotring A. Gestational diabetes in high-risk populations.(DIABETES ADVOCACY) Clinical Diabetes. 2013;31(2):90. doi: 10.2337/diaclin.31.2.90. [DOI] [Google Scholar]
- 5.Damm P. Future risk of diabetes in mother and child after gestational diabetes mellitus. Int J Gynaecol Obstet. 2009;104(Suppl 1):S25–S26. doi: 10.1016/j.ijgo.2008.11.025. [DOI] [PubMed] [Google Scholar]
- 6.Tobias DK, Zhang C, van Dam RM, Bowers K, FB H. Physical activity before and during pregnancy and risk of gestational diabetes mellitus: a meta-analysis. Diabetes Care. 2011;34(1):223–229. doi: 10.2337/dc10-1368. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Retnakaran R, Qi Y, Sermer M, Connelly PW, Zinman B, Hanley AJ. Pre-gravid physical activity and reduced risk of glucose intolerance in pregnancy: the role of insulin sensitivity. Clin Endocrinol. 2009;70(4):615–622. doi: 10.1111/j.1365-2265.2008.03393.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Gradmark A, Pomeroy J, Renstrom F, Steiginga S, Persson M, Wright A, Bluck L, Domellof M, Kahn SE, Mogren I, et al. Physical activity, sedentary behaviors, and estimated insulin sensitivity and secretion in pregnant and non-pregnant women. BMC Pregnancy Childbirth. 2011;11(1):44. doi: 10.1186/1471-2393-11-44. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.U.S. Department of Health and Human Services. 2008 Physical Activity Guidelines for Americans. In.: https://health.gov/paguidelines/guidelines/summary.aspx; 2008.
- 10.Committee Opinion No. 650 summary: physical activity and exercise during pregnancy and the postpartum period. Obstet Gynecol 2015, 126(6):1326-1327. [DOI] [PubMed]
- 11.World Health Organization. Global recommendations on physical activity for health. In.: http://whqlibdoc.who.int/publications/2010/9789241599979_eng.pdf?ua=1; 2010. [PubMed]
- 12.World Health Organization. Global Physical Activity Questionnaire (GPAQ) Analysis Guide. In.: http://www.who.int/chp/steps/resources/GPAQ_Analysis_Guide.pdf.
- 13.Dempsey FC, Butler FL, Williams FA. No need for a pregnant pause: physical activity may reduce the occurrence of gestational diabetes mellitus and preeclampsia. Exerc Sport Sci Rev. 2005;33(3):141–149. doi: 10.1097/00003677-200507000-00007. [DOI] [PubMed] [Google Scholar]
- 14.Dawes J. The role of exercise in the prevention and treatment of gestational diabetes mellitus. Strength Cond J. 2006;28(3):66–68. doi: 10.1519/00126548-200606000-00012. [DOI] [Google Scholar]
- 15.Mottola MF. The role of exercise in the prevention and treatment of gestational diabetes mellitus. Curr Sports Med Rep. 2007;6(6):381–386. [PubMed] [Google Scholar]
- 16.Colberg SR, Castorino K, Jovanovic L. Prescribing physical activity to prevent and manage gestational diabetes. World J Diabetes. 2013;4(6):256–262. doi: 10.4239/wjd.v4.i6.256. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Dempsey JC, Sorensen TK, Williams MA, Lee IM, Miller RS, Dashow EE, Luthy DA. Prospective study of gestational diabetes mellitus risk in relation to maternal recreational physical activity before and during pregnancy. Am J Epidemiol. 2004;159(7):663–670. doi: 10.1093/aje/kwh091. [DOI] [PubMed] [Google Scholar]
- 18.Padayachee C, Coombes JS. Exercise guidelines for gestational diabetes mellitus. World J Diabetes. 2015;6(8):1033–1044. doi: 10.4239/wjd.v6.i8.1033. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Loy SL, Ng MJ, Cheung YB, Godfrey KM, Calder PC, Lek N, Yap F, Muller-Riemenschneider F, Natarajan P, Chong YS, et al. Plasma omega-3 fatty acids in pregnancy are inversely associated with postpartum weight retention in a multiethnic Asian cohort. Am J Clin Nutr. 2017;22(10):151258. doi: 10.3945/ajcn.116.151258. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Chasan-Taber L, Schmidt MD, Pekow P, Sternfeld B, Manson JE, Solomon CG, Braun B, Markenson G. Physical activity and gestational diabetes mellitus among Hispanic women. J Women's Health (2002) 2008;17(6):999–1008. doi: 10.1089/jwh.2007.0560. [DOI] [PubMed] [Google Scholar]
- 21.van der Ploeg HP, van Poppel MN, Chey T, Bauman AE, Brown WJ. The role of pre-pregnancy physical activity and sedentary behaviour in the development of gestational diabetes mellitus. J Sci Med Sport. 2011;14(2):149–152. doi: 10.1016/j.jsams.2010.09.002. [DOI] [PubMed] [Google Scholar]
- 22.Ogonowski J, Miazgowski T, Kuczynska M, Krzyzanowska-Swiniarska B, Celewicz Z. Pregravid body mass index as a predictor of gestational diabetes mellitus. Diabet Med. 2009;26(4):334–338. doi: 10.1111/j.1464-5491.2009.02695.x. [DOI] [PubMed] [Google Scholar]
- 23.Deierlein AL, Siega-Riz AM, Evenson KR. Physical activity during pregnancy and risk of hyperglycemia. J Women's Health (Larchmt) 2012;21(7):769–775. doi: 10.1089/jwh.2011.3361. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Oken E, Ning Y, Rifas-Shiman SL, Radesky JS, Rich-Edwards JW, Gillman MW. Associations of physical activity and inactivity before and during pregnancy with glucose tolerance. Obstet Gynecol. 2006;108(5):1200–1207. doi: 10.1097/01.AOG.0000241088.60745.70. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Dye TD, Knox KL, Artal R, Aubry RH, Wojtowycz MA. Physical activity, obesity, and diabetes in pregnancy. Am J Epidemiol. 1997;146(11):961–965. doi: 10.1093/oxfordjournals.aje.a009223. [DOI] [PubMed] [Google Scholar]
- 26.Owen N, Healy GN, Matthews CE, Dunstan DW. Too much sitting: the population health science of sedentary behavior. Exerc Sport Sci Rev. 2010;38(3):105–113. doi: 10.1097/JES.0b013e3181e373a2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Sedentary Behaviour Research N Letter to the editor: standardized use of the terms “sedentary” and “sedentary behaviours”. Appl Physiol Nutr Metab. 2012;37(3):540–542. doi: 10.1139/h2012-024. [DOI] [PubMed] [Google Scholar]
- 28.Biswas A, PI O, Faulkner GE, Bajaj RR, Silver MA, Mitchell MS, Alter DA. Sedentary time and its association with risk for disease incidence, mortality, and hospitalization in adults: a systematic review and meta-analysis. Ann Intern Med. 2015;162(2):123–132. doi: 10.7326/M14-1651. [DOI] [PubMed] [Google Scholar]
- 29.Gollenberg AL, Pekow P, Bertone-Johnson ER, Freedson PS, Markenson G, Chasan-Taber L. Sedentary behaviors and abnormal glucose tolerance among pregnant Latina women. Med Sci Sports Exerc. 2010;42(6):1079–1085. doi: 10.1249/MSS.0b013e3181c6dec8. [DOI] [PubMed] [Google Scholar]
- 30.Sukumar N, Farmer J, Venkataraman H, Saravanan P. Longer duration of sitting down in pregnancy is associated with gestational diabetes, greater weight gain and depressive symptoms. Endocr Abstr. 2015;38
- 31.Anjana RM, Sudha V, Lakshmipriya N, Anitha C, Unnikrishnan R, Bhavadharini B, Mahalakshmi MM, Maheswari K, Kayal A, Ram U, et al. Physical activity patterns and gestational diabetes outcomes – the wings project. Diabetes Res Clin Pract. 2016;116:253–262. doi: 10.1016/j.diabres.2016.04.041. [DOI] [PubMed] [Google Scholar]
- 32.Chasan-Taber L, Silveira M, Lynch KE, Pekow P, Braun B, Manson JE, Solomon CG, Markenson G. Physical activity before and during pregnancy and risk of abnormal glucose tolerance among Hispanic women. Diabete Metab. 2014;40(1):67–75. doi: 10.1016/j.diabet.2013.09.005. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Jenum AK, Morkrid K, Sletner L, Vangen S, Torper JL, Nakstad B, Voldner N, Rognerud-Jensen OH, Berntsen S, Mosdol A, et al. Impact of ethnicity on gestational diabetes identified with the WHO and the modified International Association of Diabetes and Pregnancy Study Groups criteria: a population-based cohort study. Eur J Endocrinol. 2012;166(2):317–324. doi: 10.1530/EJE-11-0866. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Cheung NW, Wasmer G, Al-Ali J. Risk factors for gestational diabetes among Asian women. Diabetes Care. 2001;24(5):955–956. doi: 10.2337/diacare.24.5.955. [DOI] [PubMed] [Google Scholar]
- 35.Chu SY, Abe K, Hall LR, Kim SY, Njoroge T, Qin C. Gestational diabetes mellitus: all Asians are not alike. Prev Med. 2009;49(2–3):265–268. doi: 10.1016/j.ypmed.2009.07.001. [DOI] [PubMed] [Google Scholar]
- 36.World Health Organization. Diagnostic Criteria and Classification of Hyperglycaemia First Detected in Pregnancy. In.: http://apps.who.int/iris/bitstream/10665/85975/1/WHO_NMH_MND_13.2_eng.pdf; 2013. [PubMed]
- 37.Group HSCR. Metzger BE, Lowe LP, Dyer AR, Trimble ER, Chaovarindr U, Coustan DR, Hadden DR, McCance DR, Hod M, et al. Hyperglycemia and adverse pregnancy outcomes. N Engl J Med. 2008;358(19):1991–2002. doi: 10.1056/NEJMoa0707943. [DOI] [PubMed] [Google Scholar]
- 38.Soh SE, Chong YS, Kwek K, Saw SM, Meaney MJ, Gluckman PD, Holbrook JD, Godfrey KM, Group GS Insights from the growing up in Singapore towards healthy outcomes (GUSTO) cohort study. Ann Nutr Metab. 2014;64(3–4):218–225. doi: 10.1159/000365023. [DOI] [PubMed] [Google Scholar]
- 39.Soh SE, Tint MT, Gluckman PD, Godfrey KM, Rifkin-Graboi A, Chan YH, Stunkel W, Holbrook JD, Kwek K, Chong YS, et al. Cohort profile: growing up in Singapore towards healthy outcomes (GUSTO) birth cohort study. Int J Epidemiol. 2014;43(5):1401–1409. doi: 10.1093/ije/dyt125. [DOI] [PubMed] [Google Scholar]
- 40.World Health Organization. BMI classification. In.: WHO:Global Database on Body Mass Index, http://www.euro.who.int/en/health-topics/disease-prevention/nutrition/a-healthy-lifestyle/body-mass-index-bmi.
- 41.WHO Expert Consultation Appropriate body-mass index in Asian populations and its implications for policy and intervention strategies. Lancet. 2004;363(9403):157–163. doi: 10.1016/S0140-6736(03)15268-3. [DOI] [PubMed] [Google Scholar]
- 42.Identification, assessment, and management of overweight and obesity: summary of updated NICE guidance. In: BMJ. vol. 349:g6608: http://www.bmj.com/content/349/bmj.g6608/rr/805398; 2014. [DOI] [PubMed]
- 43.Chen LW, Lim AL, Colega M, Tint MT, Aris IM, Tan CS, Chong YS, Gluckman PD, Godfrey KM, Kwek K, et al. Maternal folate status, but not that of vitamins B-12 or B-6, is associated with gestational age and preterm birth risk in a multiethnic Asian population. J Nutr. 2015;145(1):113–120. doi: 10.3945/jn.114.196352. [DOI] [PubMed] [Google Scholar]
- 44.Chong Y-S, Cai S, Lin H, Soh SE, Lee Y-S, Leow MK-S, Chan Y-H, Chen L, Holbrook JD, Tan K-H, et al. Ethnic differences translate to inadequacy of high-risk screening for gestational diabetes mellitus in an Asian population: a cohort study. BMC Pregnancy Childbirth. 2014;14(1):1–7. doi: 10.1186/1471-2393-14-345. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45.Padmapriya N, Shen L, Soh SE, Shen Z, Kwek K, Godfrey KM, Gluckman PD, Chong YS, Saw SM, Muller-Riemenschneider F. Physical activity and sedentary behavior patterns before and during pregnancy in a multi-ethnic sample of Asian women in Singapore. Matern Child Health J. 2015;19(11):2523–2535. doi: 10.1007/s10995-015-1773-3. [DOI] [PubMed] [Google Scholar]
- 46.IPAQ Research Committee . Guidelines for data processing and analysis of the international physical activity questionnaire (IPAQ) 2005. [Google Scholar]
- 47.Zhang C, Solomon CG, Manson JE, FB H. A prospective study of pregravid physical activity and sedentary behaviors in relation to the risk for gestational diabetes mellitus. Arch Intern Med. 2006;166(5):543–548. doi: 10.1001/archinte.166.5.543. [DOI] [PubMed] [Google Scholar]
- 48.Redden SL, LaMonte MJ, Freudenheim JL, Rudra CB. The association between gestational diabetes mellitus and recreational physical activity. Matern Child Health J. 2011;15(4):514–519. doi: 10.1007/s10995-010-0586-7. [DOI] [PubMed] [Google Scholar]
- 49.Dempsey JC, Butler CL, Sorensen TK, Lee IM, Thompson ML, Miller RS, Frederick IO, Williams MA. A case-control study of maternal recreational physical activity and risk of gestational diabetes mellitus. Diabetes Res Clin Pract. 2004;66(2):203–215. doi: 10.1016/j.diabres.2004.03.010. [DOI] [PubMed] [Google Scholar]
- 50.Dunstan DW, Salmon J, Owen N, Armstrong T, Zimmet PZ, Welborn TA, Cameron AJ, Dwyer T, Jolley D, Shaw JE, et al. Physical activity and television viewing in relation to risk of undiagnosed abnormal glucose metabolism in adults. Diabetes Care. 2004;27(11):2603–2609. doi: 10.2337/diacare.27.11.2603. [DOI] [PubMed] [Google Scholar]
- 51.Ong KK, Diderholm B, Salzano G, Wingate D, Hughes IA, MacDougall J, Acerini CL, Dunger DB. Pregnancy insulin, glucose, and BMI contribute to birth outcomes in nondiabetic mothers. Diabetes Care. 2008;31(11):2193–2197. doi: 10.2337/dc08-1111. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 52.Deierlein AL, Siega-Riz AM, Evenson KR. Physical activity during pregnancy and risk of hyperglycemia. J Women's Health. 2012;21(7):769–775. doi: 10.1089/jwh.2011.3361. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 53.Michelle F. Mottola S-MR: Exercise Guidelines for Women with Gestational Diabetes In.: InTech, Available from: http://www.intechopen.com/books/gestational-diabetes/exercise-guidelines-for-women-with-gestationaldiabetes; 2011.
- 54.Bannon AL, Waring ME, Leung K, Masiero JV, Stone JM, Scannell EC, Moore Simas TA. Comparison of self-reported and measured pre-pregnancy weight: implications for gestational weight gain counseling. Matern Child Health J. 2017;2(10):017–2266. doi: 10.1007/s10995-017-2266-3. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
The datasets generated for this study are stored in the repository belonging to the Growing Up in Singapore Towards healthy Outcomes (GUSTO). The data are not publicly available online, but they can be obtained upon request through the corresponding author.