

Abstract
This current study identifies distinct parent prevention communication profiles and examines whether youth with different parental communication profiles have varying substance use trajectories over time. Eleven schools in two rural school districts in the Midwestern United States were selected, and 784 students were surveyed at three time points from the beginning of 7th grade to the end of 8th grade. A series of latent profile analyses were performed to identify discrete profiles/subgroups of substance-specific prevention communication (SSPC). The results revealed a 4-profile model of SSPC: Active-Open, Passive-Open, Active-Silent, and Passive-Silent. A growth curve model revealed different rates of lifetime substance use depending on the youth’s SSPC profile. These findings have implications for parenting interventions and tailoring messages for parents to fit specific SSPC profiles.
Despite a decline in illicit substance use involvement among adolescents in the past several years in the United States (Miech, Johnston, O’Malley, Bachman, & Schulenberg, 2015), the social and health costs of adolescent substance use remains high. In 2011, almost 40% of adolescent emergency department visits were related to the use and abuse of illicit substances (SAMHSA, 2013), and substance use is linked to a variety of cancers, coronary heart disease, and respiratory disease (Baan et al., 2007; Shield, Parry, & Rehm, 2013). Alcohol use, in particular, is a popular activity among youth in the United States (Chen & Jacobson, 2012). According to the 2015 Monitoring the Future Study (MTF) (National Institute on Drug Abuse, 2016), 30% of U.S. youth reported consuming alcohol by 8th grade, and more than 13% of 8th grade students reported having been drunk at least once in their life. Moreover, in an analysis of MTF data, Cavazos-Rehg and colleagues (2016) found that 45% of high school seniors had consumed alcohol during the past month, 26% reported binge drinking (i.e., consuming five or more drinks on at least one occasion in the past 2 weeks), 17% percent reported riding with a driver who drank alcohol, nearly 12% reported driving in the past 2 weeks after drinking alcohol, and 7% reported driving after binge drinking. These findings are consequential because of the potential loss of life, with alcohol use related to 26% of motor vehicle fatalities involving young drivers between 15 and 20 years old (National Center for Statistics and Analysis, 2016).
To better understand substance use and abuse in later adolescence and to help prevent it, it is critical to understand the etiology of substance use in early adolescence. For example, early age of initiation is one of the most important predictors of later misuse (Newton-Howes & Boden, 2015; Spoth, Trudeau, Guyll, Shin, & Redmond, 2009). This is why efforts to prevent substance use are often aimed at early adolescents, such as school-based or family-based interventions (Komro et al., 2008; Williams, Ayers, Baldwin, & Marsiglia, 2016) and media campaigns (Stephenson, Quick, Atkinson, & Tschida, 2005) that encourage parents to talk with their adolescents about substances.
Prevention efforts aimed at getting parents to talk with their young adolescents are often guided by primary socialization theory (PST) (Oetting & Donnermeyer, 1998), which asserts that parents can influence their children’s substance-use perceptions and behaviors through communication (Kam & Yang, 2013). Indeed, there is considerable evidence that suggests parent-adolescent communication can effectively buffer the risks of early use initiation (Miller-Day, 2002) and reduce binge drinking (Turrisi, Wiersma, & Hughes, 2000) by shaping youth’s antisubstance use attitudes, norms, intentions, and behaviors (Kam, Matsunaga, Hecht, & Ndiaye, 2009).
Yet, most interventions and media campaigns promoting parental communication about substances takes a one size fits all approach, treating all parents as a homogenous group and advocating for general prescriptions to “talk with your child” about substances. The current study seeks to address this limitation by moving beyond generic conceptualizations of parental prevention, and instead, examines substance-specific prevention communication (SSPC) as a heterogeneous process that is complex and multifaceted. It also contributes to the current theorizing about parental prevention communication and allows for a more nuanced approach to parent-based prevention efforts.
Parental communication about substances and substance use
Health communication research shows that personalized messages from family members are helpful in eliciting healthy behaviors and behavior changes (Noar, Harrington, & Aldrich, 2009), yet until the turn of the century, there had been little communication research attention paid to parental messages about substance use. Much of the past communication research focused on general communication quality (e.g., “I feel comfortable communicating with my parent about a variety of topics”) or in terms of examining presence or absence of talk about substances (e.g., “Do you talk” or “do you not talk” with your adolescent about substances?). This research found that greater frequency and quality of general parent–child communication are negatively associated with adolescent substance use (Ackard, Neumak-Sztainer, Story, & Perry, 2006).
Around the turn of the 21st century, prevention research both in and outside the field of communication moved beyond general conceptions of communication and began to highlight the importance of SSPC as talk about substances with a goal toward preventing substance use. Miller-Day and Kam (2010) and Kam (2011) refer to SSPC as “targeted parent-child communication,” but both terms refer to direct or indirect, preventive messages that focus on issues related to substances and substance use that may occur on an ongoing basis or at a few situated times during the adolescent’s development and have a significant impact on adolescent substance use (Ennett, Bauman, Foshee, Pembertonm, & Hicks, 2001; Kam, Potocki, & Hecht, 2014; Miller-Day & Kam, 2010; Napper, Hummer, Lac, & LaBrie, 2014; Reimuller, Hussong, & Ennett, 2011). Merging terminology for clarity sake, we believe that SSPC is the more descriptive term to represent this construct. It maintains the focus on targeting substance use specifically and emphasizes the intention of prevention. Although parents may convey permissive messages in their substance-specific communication (Napper, Froidevaux, & LaBrie, 2016; Reimuller et al., 2011), the primary focus of SSPC is on prevention.
Variation in parental prevention messages
In early adolescence, the most dominant approach to SSPC seems to be parent-only communication, with youth discussing substances and substance use with parents rather than with friends (Kam, 2011). Yet, when examining SSPC and parents’ anti-use prevention messages, there seems to be a good deal of variation across parents in both message type and strategic approaches to prevention (Ebersole, Miller-Day, & Raup-Krieger, 2014; Kam & Middleton, 2013; Miller-Day, 2008; Vermeulen-Smit, Verdurmen, & Engels, 2015).
Miller-Day and colleagues have developed a growing body of literature examining SSPC with young adults (Miller-Day, 2008) and adolescents (Miller, Alberts, Hecht, Trost, & Krizek, 2000; Miller-Day & Hecht, 2013). Miller-Day and Dodd (2004) identified four dimensions of prevention messaging including ongoing messages, targeted messages, direct messages, and indirect messages. Some parents believed that direct, targeted messages conveyed only once (often referred to as “one shot” talks) are all that are needed to promote their child’s healthy behaviors and prevent substance use, and other parents in this study integrated messages into the fabric of everyday life on an ongoing basis and across time (Miller-Day & Dodd, 2004).
This body of research provides ample evidence that not only does “one size not fit all” parents (Miller-Day, 2002), but that individual parents may use multiple types of conversational strategies (Miller-Day & Kam, 2010) and gravitate toward certain strategic prevention messages (Miller-Day, 2008). For example, families characterized by low levels of family expressiveness tend to use indirect messages or “hints,” while those characterized by high levels of family expressiveness tend to articulate no-tolerance rules, provide information, or reward their offspring for non-use (Miller-Day, 2008).
In addition, SSPC may include warnings about the dangerous consequences of substance use, commenting when impaired characters are on television, providing suggestions for avoiding offers of substances, discussing others who were in trouble because of substances, providing written information from the internet or other source, or generally lecturing about substance or substance use (Kam, 2011; Miller-Day & Kam, 2010). General prescriptions to “talk with your child about drugs” do not take into account the variation in how parents might naturally communicate with their children about sensitive, and perhaps even taboo topics. These prescriptions presume all parents communicate with their children similarly and are likewise expressive. Yet, as we know from family communication theory, parents differ in how they communicate with their children and in some family environments with low levels of expressiveness, open discussions about substances and substance use may not be comfortable.
Family environments and SSPC
According to Koerner and Fitzpatrick’s general theory of family communication schemata (2002), families are characterized by uniquely shared world views that shape how family members interact, perceive their social environments, and communicate with one another inside the family. What is a comfortable way of communicating in one family may not be comfortable for another. Hence, these varying schemata would likely shape family communication about substances. Within the field of family communication, investigations of family communication patterns (FCP) have dominated the literature, providing explanations for differing communication styles across family types. Fitzpatrick and Ritchie (1994) initiated a new generation of FCP research when they merged work on husband-wife and parent-child schemata to identify family communication environments that vary by both openness and control themes and are captured in three factors: expressiveness, structural traditionalism, and avoidance.
As pointed out by Baxter, Bylund, Imes, and Scheive (2005), expressiveness is conceptually similar to the conversation orientation dimension of FCP. Moreover, structural traditionalism and avoidance are similar to the conformity orientation of FCP, but in different ways. Both structural traditionalism and avoidance suppress independence of opinion, but structural traditionalism emphasizes conformity to the legitimate authority structure of a family, whereas avoidance emphasizes suppression of unpleasant topics. Conformity in families high in structural traditionalism is grounded in legitimation of authority structures, whereas conformity in families high in avoidance is motivated by a desire to avoid unpleasant talk (Baxter et al., 2005).
We believe it is likely that variations observed in SSPC might be related to differing family communication environments. Existing research on SSPC does seem to suggest that perhaps families high in expressiveness might use more frequent and more direct strategies to prevent their children from using illicit substances. Moreover, parents and youth who tend not to avoid difficult topics will likely directly address the topic of substances and substance use applying multiple strategies, but perhaps only when children respect parental authority; that is, perceive parents’ messages to be influential.
Different family environments with varying levels of expressiveness, topic avoidance, and respect for parental authority may employ different prevention strategies. But, the research to-date is insufficient to determine this. Understanding SSPC approaches in different family environments could provide a potential classification system for parental prevention communication. Research has provided no clear parent prevention communication classification system for SSPC within the context of family communication environments. A classification system can enable researchers to carry out comparative studies of important features, connections, and functions of parental prevention communication. A classification system of parental prevention communication should be useful to prevention scholars seeking to understand and compare the variety and effectiveness of parental prevention communication approaches.
In summary, research to-date has moved from examining the effects of general family communication style to a more refined examination of substance-specific preventive communication. Yet, general family communication is still important because this appears to establish an environment conducive (or not) to sharing messages about substances. Although more research attention has been focused on SSPC in recent years, empirical examination of this parenting practice is underdeveloped. This study moves one step further to advance the fields of prevention and family communication by exploring if distinct parent prevention communication profiles can be identified using SPCC and family communication environments as profile indicators. Thus, we pose the following research question:
RQ1: Do adolescents report distinct parent prevention communication profiles characterized by their substance-specific prevention communication and family communication environment?
In addition to examining variations across prevention profiles, the majority of SSPC research in communication has been cross sectional with limited evidence that SSPC impacts actual adolescent substance use over time. In their qualitative study, Miller-Day and Dodd (2004) argued that direct and ongoing SSPC across time would more effectively prevent adolescent substance use than indirect, infrequent SSPC. No empirical evidence, however, have supported this claim. Undeniably, a plethora of other research suggests that SSPC will inhibit adolescent substance use across time and across a variety of substances (Kam, Castro, & Wang, 2014; Kam et al., 2014; Kumpfer, Alvarado, & Whiteside, 2003; Napper et al., 2016; Reimuller et al., 2011). However, it is unclear if considering factors of family communication environment along with SSPC might demonstrate different trajectories of adolescent substance use over time. This present study seeks to fill this gap by conducting a longitudinal investigation, tracking youth from 7th grade to the end of 8th grade, to answer the following question:
RQ2: Do parental prevention communication profiles have different adolescent substance use trajectories over time?
Method
Data collection procedures
Data for this study came from surveys administered by the Survey Research Center at Pennsylvania State University to youth at the beginning of 7th grade in Fall 2009 (wave 1) and subsequently at the end of 7th grade in the Spring of 2010 (wave 2) and the end of 8th grade in spring 2011 (wave 3) as part of a randomized controlled trial investigating the effects of the 7th grade keepin’ it REAL substance use prevention curriculum (see Colby et al., 2013). Students in 39 schools from rural school districts in two Midwestern states took part in the project. Only randomly assigned control schools (n = 11) were used in this analysis to prevent confounding program effects, leaving a total sample size of 784 participants. Among the students, 47% were female, and 92% non-Latino White with an average age of 12.3 years at wave 1 (SD = 0.51). The control-school sample used in this study is representative of the larger study sample on all demographic variables and sample demographics mirror schools in these geographic areas (Graham et al., 2014).
Lists of 7th grade students were obtained from participating schools and passive informed consent forms were mailed to parents of all students at the beginning of 7th grade, the end of 7th grade, the end of 8th grade, and the end of 9th grade. Parents had the opportunity to withdraw their child from the study at any of these points in time. In addition, child assent forms were read aloud and provided in writing prior to completing surveys. All procedures were approved by the university institutional review board.
The 55-minute survey included a variety of assessments including adolescent’s perceptions of family communication environments, SSPC, and lifetime use of alcohol and tobacco (chewing and smoking). This study restricted substance use to the two primary substances used by youth in early adolescence: alcohol and tobacco. At the time of the study, prevalence rates for these two illicit substances exceeded all other substances used by youth at this stage of development (Johnston, 2010). Overall, there were 146 items administered in a 3-form, planned missing design (Graham, Hofer, & MacKinnon, 1996), where students completed one of three versions of the survey each consisting of 109 items. One block of items measuring core variables (e.g., substance use) appeared on all the surveys and three additional blocks items (AB, AC, BC) were given at random to different subsets of students.
Measures
Family communication environment
Seventeen items measuring youth perceptions of their family communication style were modified from the Family Communication Environment Inventory instrument (Fitzpatrick & Ritchie, 1994) measuring: openness/expressiveness (6 items); structural traditionalism/authority structure (6 items), and avoidance of unpleasant topics (5 items). Items were measured on a five-point frequency scale (1 = never, 5 = all the time) with the exception of three of the avoidance items (items 15, 16, 17), which were measured on a four-point scale ranging from “not at all true” to “extremely true.” FCE was administered at wave 1 (See more details regarding response scales in Table 1–3).
Table 1.
Means and standard deviations (SD) of the four parent prevention communication profiles with family communication environment (FCE)-openness/expressiveness.
| Item | Openness/Expressiveness | Overall Sample
|
Passive-Silent (n = 275) 36% |
Active-Silent (n = 117) 15% |
Passive-Open (n = 249) 31% |
Active-Open (n = 143) 18% |
|||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Mean | SD | Mean | SD | Mean | SD | Mean | SD | Mean | SD | ||
| 1 | My parents ask my opinion when the family is talking about something | 2.90 | 1.25 | 2.15a | 0.07 | 2.54b | 0.11 | 3.34c | 0.11 | 3.94d | 0.11 |
| 2 | I tell my parents what I am thinking about | 2.71 | 1.33 | 1.72a | 0.06 | 2.26b | 0.12 | 3.26c | 0.12 | 4.09d | 0.10 |
| 3 | I can tell my parents almost anything | 3.28 | 1.46 | 2.24a | 0.09 | 2.87b | 0.14 | 4.03c | 0.11 | 4.41d | 0.10 |
| 4 | My parents encourage me to express my feelings | 3.41 | 1.46 | 2.24a | 0.11 | 3.08b | 0.17 | 4.17c | 0.09 | 4.70d | 0.07 |
| 5 | In my family, we talk about our feelings and emotions. | 2.27 | 1.28 | 1.40a | 0.05 | 1.75b | 0.09 | 2.72c | 0.12 | 3.64d | 0.13 |
| 6 | My parents like to hear my opinions, even when they don’t agree with me. | 3.13 | 1.45 | 2.06a | 0.09 | 2.52b | 0.16 | 3.85c | 0.11 | 4.51d | 0.07 |
Note. Family Communication Environment (openness/expressiveness) was measured on a 5-point scale (1 = never, 5 = all the time). Mean with the different subscripted alphabet letter in each raw indicated that means of item among profiles were statistically distinguishable at the .05 alpha level, based on ANOVA with Tukey ad-hoc method in SPSS. Order of Alphabet indicated statistically lager mean in each item. When LPA was performed in Mplus, it assigned each individual into a specific profile based on the most likely class membership. ANOVA with an ad-hoc method was conducted based on this information to compare item’s mean difference among profiles. Although a Wald test was superior to a simple ANOVA test to explore an item’s mean difference among profiles, we did not conduct it to minimize type I error (36 Wald tests = 6 tests to compare one item among profiles × 6 items) statistically increased Type I errors.
Table 3.
Means and standard deviations (SD) of the four parent prevention communication profiles with family communication environment (FCE)-avoidance of unpleasant topics.
| Item | Avoidance of Unpleasant Topics | Overall Sample
|
Passive-Silent (n = 275) 36% |
Active-Silent (n = 117) 15% |
Passive-Open (n = 249) 31% |
Active-Open (n = 143) 18% |
|||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Mean | SD | Mean | SD | Mean | SD | Mean | SD | Mean | SD | ||
| 13 | My parents say things like “There are some things that just shouldn’t be talked about” | 2.42 | 1.35 | 2.03a | 0.08 | 2.78b | 0.17 | 2.27a | 0.09 | 3.11b | 0.14 |
| 14 | My parents often say things like “You should give in one arguments rather than risks making people mad” | 2.04 | 1.28 | 1.62a | 0.07 | 2.41c | 0.17 | 1.99b | 0.09 | 2.66c | 0.16 |
| 15 | Some issues will disappear if two people can just avoid arguing about them | 2.39 | 0.96 | 2.09a | 0.06 | 2.49b | 0.11 | 2.55b | 0.06 | 2.64b | 0.09 |
| 16 | It is better to hide one’s true feelings in order to avoid hurting a family member | 2.17 | 1.03 | 2.16a | 0.06 | 2.28a | 0.12 | 2.16a | 0.07 | 2.14a | 0.11 |
| 17 | In a family, it is better to avoid conflicts than to engage in them | 2.76 | 1.09 | 2.47a | 0.07 | 2.97b | 0.11 | 2.93b | 0.08 | 2.91b | 0.11 |
Note. Family Communication Environment (avoidance of unpleasant topics) was measured on either a 5-point scale (1 = never, 5 = all the time) for item 13 and 14 or a 4-point scale (1 = not true at all, 4 = extremely true) for item 15–17. Mean with the different subscripted alphabet letter in each raw indicated that means of item among profiles were statistically distinguishable at the .05 alpha level, based on ANOVA with Tukey ad-hoc method in SPSS. Order of Alphabet indicated statistically larger mean in each item. When LPA was performed in Mplus, it assigned each individual into a specific profile based on the most likely class membership. ANOVA with an ad-hoc method was conducted based on this information to compare item’s mean difference among profiles. Although a Wald test was superior to a simple ANOVA test to explore an item’s mean difference among profiles, we did not conduct it to minimize type I error (30 Wald tests = 6 tests to compare one item among profiles × 5 items) statistically increased Type I errors.
Substance-specific prevention communication
Substance-specific prevention communication was measured at wave 1 with eight items adapted from Miller-Day and Kam’s (2010) Targeted Parent-Child Communication about Substances scale, which measures SSPC. Items asked youth to share how frequently their parents engaged in various conversational strategies such as lecturing, warning of dangers, commenting on media portrayals of drinking and smoking, and soliciting youths’ opinions about alcohol or tobacco use (1 = never, 2 = occasionally, 3 = quite often, 4 = all the time) (See Table 4).
Table 4.
Means and standard deviations (SD) of the four parent prevention communication profiles with substance-specific prevention communication (SSPC)
| Item | Substance-Specific Prevention Communication | Overall Sample
|
Passive-Silent (n = 275) 36% |
Active-Silent (n = 117) 15% |
Passive-Open (n = 249) 31% |
Active-Open (n = 143) 18% |
|||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Mean | SD | Mean | SD | Mean | SD | Mean | SD | Mean | SD | ||
| 18 | Lecture you or give you a speech about drinking alcohol, chewing/smoking tobacco or other drug use? | 2.23 | 0.95 | 1.67a | 0.05 | 2.77b | 0.11 | 2.03c | 0.07 | 3.23d | 0.08 |
| 19 | Warn you about the dangers of drinking alcohol, chewing/smoking tobacco, or other drug use? | 2.63 | 0.99 | 1.92a | 0.06 | 3.39b | 0.08 | 2.46c | 0.07 | 3.72d | 0.05 |
| 20 | Talk to you about how to handle offers of alcoholic drinks, chew, cigarettes, or other drugs? | 2.47 | 1.03 | 1.72a | 0.06 | 3.29b | 0.12 | 2.26c | 0.07 | 3.63d | 0.06 |
| 21 | Make comments about how drinking alcohol is bad if a character on TV is drinking or drunk? | 2.10 | 1.06 | 1.43a | 0.04 | 3.10b | 0.17 | 1.71c | 0.06 | 3.25b | 0.10 |
| 22 | Make comments about how chewing or smoking is bad if a character on TV is chewing/smoking tobacco? | 2.06 | 1.03 | 1.40a | 0.04 | 2.96b | 0.16 | 1.73c | 0.07 | 3.19d | 0.11 |
| 23 | Tell you stories of people who drink alcohol or have been drunk? | 2.12 | 0.99 | 1.70a | 0.05 | 2.53b | 0.12 | 1.95c | 0.06 | 2.89d | 0.11 |
| 24 | Show you information on the web, TV, or in the news about the dangers of drinking alcohol, smoking/chewing, or other drug use? | 1.83 | 1.01 | 1.28a | 0.04 | 2.28b | 0.15 | 1.64c | 0.05 | 2.90d | 0.12 |
| 25 | Ask about your thoughts and opinion about drinking alcohol, smoking/chewing or other drug use? | 2.04 | 1.01 | 1.33a | 0.04 | 2.50b | 0.12 | 1.95c | 0.07 | 3.23d | 0.08 |
Note. Substance-Specific Prevention Communication was measured on a 4-point scale (1 = no, never to 4 = Yes, all the time). Mean with the different subscripted alphabet letter in each raw indicated that mean of items among profiles were statistically distinguishable at the .05 alpha level, based on ANOVA with Tukey ad-hoc method in SPSS. Order of Alphabet indicated statistically lager mean in each item. When LPA was performed in Mplus, it assigned each individual into a specific profile based on the most likely class membership. ANOVA with an ad-hoc method was conducted based on this information to compare item’s mean difference among profiles. Although a Wald test was superior to a simple ANOVA test to explore an item’s mean difference among profiles, we did not conduct it to minimize type I error (48 Wald tests = 6 tests to compare one item among profiles × 8 items) statistically increased Type I errors.
Adolescent substance use
Substance use measures assessed lifetime use of alcohol, smoking tobacco, and chewing tobacco. Each variable was treated separately and was measured at waves 1, 2, and 3. A sample item regarding lifetime substance use was, “How many drinks of alcohol have you had in your entire life?” Consistent with prior substance use research (e.g., Hansen & Graham, 1991), a 10-point scale was employed for alcohol use (M = 2.04, SD = 1.50 at wave 1, M = 2.46 SD = 1.80 at wave 2, M = 3.13 SD = 2.37 at wave 3) and cigarette smoking (M = 1.34, SD = 1.28 at wave 1, M = 1.55 SD = 1.63 at wave 2, M = 1.99 SD = 2.30 at wave 3). The item for chewing tobacco was rated on an eight-point scale ranging from never to more than 50 times (M = 1.24, SD = 0.96 at wave 1, M = 1.37, SD = 1.22, at wave 2, M = 1.57, SD = 1.70 at wave 3).
Missing data
School-based, longitudinal survey studies related to substance use typically encounter missing data issues. For example, substance users are less likely to respond to substance use items over time, potentially biasing the data. In our sample, 541 students (70%) responded to the lifetime alcohol use item at all three waves, and 181 students (23%) responded only at waves 1 and 2. Similarly, 559 students (71%) responded to the lifetime cigarette item at all three waves, and 174 students (22%) at waves 1 and 2. Last, 565 students (72%) answered the chewing tobacco item across all three waves with 174 students (22%) answering at waves 1 and 2. The remaining students were categorized in different patterns of missingness (e.g., student appears at wave 1 and dropped out at wave 2 but appear at wave 3).
Because there were a noticeable number of people who appeared at wave 1 and 2 but disappeared at wave 3 across three lifetime substance use categories, we were concerned about missing data. To examine the impact of missingness on growth factors (e.g., intercept and slope), we created six new variables (3 substances × 2 missingness patterns). The two missingness patterns were (1) nonmissing substance use across all waves (coded as 0) and nonmissing substance use at wave 1 and 2 but missing at wave3 (coded as 1) and (2) nonmissing substance use across all waves (coded as 0) and any type of missing pattern (coded as 1).
These new variables were included as covariates to investigate whether missingness patterns influenced growth factors on substance use. Separately, we employed the second type of missing pattern variable (nonmissing alcohol use versus missing at any time) as a covariate in the same model. Across all substance use, none of the types of missingness significantly influenced growth factors, thus full information maximum likelihood estimation (FIML) was employed to account for missing data, assuming data are missing at random (MAR) (Graham, Cumsille, & Elek-Fisk, 2003). FIML generates unbiased estimates with MAR (Enders & Bandalos, 2001) and robust estimates even though the MAR assumption is not completely met (Newman, 2003).
Data analysis plan
To address our research questions and identify any latent parent prevention communication profiles, a Latent Profile Analysis (LPA) was conducted using each item instead of making composite scores because the larger number of indicators in the LPA help with model stability. To answer the second research question regarding whether profiles would have different substance use trajectories, a Latent Growth Curve Model (LGCM, See Preacher, Wichman, MacCallum, & Briggs, 2008 in details) was employed. All analyses were conducted with maximum likelihood with robust standard errors using Mplus 6.0 (Muthén & Muthén, 2007) for nonnormally distributed substance use variables. To avoid convergence of local maximum likelihood value, 200 sets of random starting values for 10 iterations each and then 20 best performing starting values were employed to convergence. The final model was less likely to converge to local maximum likelihood because of repetition of likelihood values.
Parent prevention communication profiles
To identify underlying parent prevention communication profiles (i.e., subgroups) with family communication environments and SPCC variables as indicators, a latent profile analysis (LPA) was computed. A series of model fit comparisons were conducted to determine the optimal number of profiles (Vermunt & Magidson, 2002). All 17 FCE items as well as all eight SSPC items were included in the latent profile analysis. The analysis started from a single profile model to a five-profile model, which was not well identified. To identify the optimal number of profiles, we employed three criteria: (1) the Bayesian information criterion (BIC: Schwartz, 1978), (2) the bootstrap likelihood ratio test (BLRT: McLachlan & Peel, 2000), and (3) theoretical interpretation (Nylund, Asparouhov, & Muthen, 2007; Tofighi & Enders, 2007; Yang, 2006).
For BIC, a smaller value indicates a better fit. Also, the BLRT is a bootstrapping method with samples to generate the empirical distribution of the log likelihood difference test statistic. BLRT offers a p-value in terms of a model comparison between k-1 and k profiles. That is, when p-value is less than .05, it indicates that k-profiles model is statistically better than k-1-profiles model (Nylund et al., 2007). Consistent with previous LPA studies (e.g., Connella & Frye, 2006; Matsunaga, Hecht, Elek, & Ndiaye, 2010), theoretical and practical implications were considered as an important factor to determine the number of profiles.
Substance use trajectories
Once the model with the best fit was identified, we computed a LGMM with fixed equal spacing to investigate whether adolescent lifetime substance use trajectories (e.g., intercept and slope) were differentiated by each profile. Because youth who have a higher level of substance use at wave 1 were more likely to use substance compared with counterparts, we allowed estimating correlations between intercept and slope in the LGMM. To attain this goal, we conducted two separate analyses. First, unconditional LGCM was conducted by specifying models for each lifetime substance use within each profile. In other words, unconditional LGCM showed whether intercepts and slopes within each profile were significantly different from zero. Second, we examined whether slopes and intercepts within each profile were statistically different from each other.
For comparison of profiles’ substance-use trajectories, we calculated a chi-square difference test following McLachlan and Peel (2000); that is, the difference (d) between the log-likelihood values from the two comparison model was doubled (2d) as the chi-square difference and the degree of freedom for the chi-square difference test was obtained based on the difference in the number of parameters between two comparison models (McLachlan & Peel, 2000). In order to avoid unnecessary comparison tests, the largest mean difference was tested first, followed by next greatest mean difference. Whenever a test was not significant, subsequent tests were not performed. In addition, a Bonferroni correction was employed for chi-square difference test to account for increased probability of type I error from computing multiple comparisons (Cabin & Mitchell, 2000; Rice, 1989).
Results identifying parent prevention communication profiles
Comparisons across multiple LPA models revealed that a four-profile model was the most suitable (BIC = 57238.91, BLRT = 642.98, p < .001). When the two (BIC = 58578.61, BLRT = 3357.16, p < .001), three (BIC = 57708.61, BLRT = 1043.27, p < .001), and four-profile solutions were added, the BIC and BLRT dropped substantively and the five-profile solution was not well identified. As a result, we stopped adding new profiles.
All profiles extracted in the four profiles showed clearly distinct patterns, clearly diverging most distinctly in terms of the FCE expressiveness dimension (i.e., items 1–6) and all of the SSPC items (e.g., 18–25). However, this occurred with only the expressiveness dimension of family communication environments. Structural traditionalism (items 7–12) and avoidance (items 13–17) provided less clear distinctions (See Table 2 & 3). That is, there was no clear profile including very high scores of either structural traditionalism or avoidance dimensions.
Table 2.
Means and standard deviations (SD) of the four parent prevention communication profiles with family communication environment (FCE)-structural traditionalism/authority structure.
| Item | Structural Traditionalism/Authority Structure | Overall Sample
|
Passive-Silent (n = 275) 36% |
Active-Silent (n = 117) 15% |
Passive-Open (n = 249) 31% |
Active-Open (n = 143) 18% |
|||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Mean | SD | Mean | SD | Mean | SD | Mean | SD | Mean | SD | ||
| 7 | When anything really important is involved, my parents expect me to obey without question | 3.77 | 1.27 | 3.19a | 0.10 | 3.77b | 0.14 | 4.13c | 0.08 | 4.31c | 0.08 |
| 8 | In my home, my parents usually have the last word | 3.55 | 1.33 | 3.03a | 0.10 | 3.79bc | 0.13 | 3.71c | 0.08 | 4.10c | 0.11 |
| 9 | My parents feel that it is important to be the boss | 3.68 | 1.36 | 3.28a | 0.10 | 3.97b | 0.14 | 3.76b | 0.10 | 4.11b | 0.12 |
| 10 | My parents say things like “You’ll know better when you grow up” | 2.92 | 1.44 | 2.36a | 0.09 | 3.55c | 0.17 | 2.81b | 0.10 | 3.67c | 0.15 |
| 11 | My parents say things like “My ideas are right and you should not question them” | 2.10 | 1.33 | 1.91a | 0.09 | 2.42b | 0.17 | 1.89a | 0.10 | 2.56b | 0.15 |
| 12 | My parent say things like “A child should not argue with adults” | 2.74 | 1.49 | 2.32a | 0.10 | 3.41b | 0.17 | 2.53a | 0.11 | 3.35b | 0.16 |
Note. Family Communication Environment (structural traditionalism) was measured on a 5-point scale (1 = never, 5 = all the time). Mean with the different subscripted alphabet letter in each raw indicated that means of item among profiles were statistically distinguishable at the .05 alpha level, based on ANOVA with Tukey ad-hoc method in SPSS. Order of Alphabet indicated statistically lager mean in each item. Active-Silent profile’s mean of item 8 statistically differed from one in Passive Silent, but it was not statistically distinguishable from ones in Passive-Open and Active-Open. When LPA was performed in Mplus, it assigned each individual into a specific profile based on the most likely class membership. ANOVA with an ad-hoc method was conducted based on this information to compare items’ mean difference among profiles. Although a Wald test was superior to a simple ANOVA test to explore an item’s mean difference among profiles, we did not conduct it to minimize type I error (36 Wald tests = 6 tests to compare one item among profiles × 6 items) statistically increased Type I errors.
Thus, the four distinct profiles that emerged were identified as follows: Class 1(lowest frequency of SSPC, lowest expressiveness, lowest structural traditionalism, lowest avoidance) was labeled Passive-Silent (36%); Class 2 (high SSPC, low expressiveness, medium-to-relatively-high structural traditionalism, relatively high avoidance) was labeled Active-Silent (15%); Class 3 (low SSPC, high expressiveness, medium-to-relatively-high structural traditionalism, medium-to-relatively-low avoidance) was labeled Passive-Open (31%); Class 4: (highest SSPC, highest expressiveness, high structural traditionalism, relatively high avoidance) was labeled Active-Open (18%). Profiles are shown in Tables 1–4.
Substance use trajectories within profiles
LGCMs were computed to examine how each profile’s substance use trajectories would differ. Models were similar for all three types of substances and show, in general, a trend toward increased alcohol, smoking tobacco, and chewing tobacco use over time. However, different rates of lifetime substance use were observed depending on the youth’s parent prevention communication profile. The results revealed that mean intercepts and slopes (see Table 5) within each prevention communication profile were significant and positive across all substances, indicating differences in the initial levels of alcohol, cigarette, and chewing tobacco use (intercept) as well as the growth rate of alcohol, cigarette, and chewing tobacco (slope) across the different parent profiles.
Table 5.
Result from growth curve model for each parent prevention communication profile.
| Lifetime alcohol
|
Lifetime cigarette
|
Lifetime chewing tobacco
|
|||||||
|---|---|---|---|---|---|---|---|---|---|
| Est | SE | z-value | Est | SE | z-value | Est | SE | z-value | |
| G1: Passive-Silent | |||||||||
| Intercept | 2.42a | 0.11 | 21.63* | 1.53a | 0.10 | 15.83* | 1.41a | 0.08 | 18.28* |
| Slope | 0.58a | 0.07 | 8.57* | 0.53a | 0.08 | 6.764* | 0.26a | 0.05 | 4.78* |
| G2: Active-Silent | |||||||||
| Intercept | 1.78b | 0.13 | 13.82* | 1.35ab | 0.13 | 10.45* | 1.30a | 0.11 | 12.29* |
| Slope | 0.71a | 0.14 | 5.22* | 0.33ab | 0.11 | 3.07* | 0.18a | 0.09 | 1.96 |
| G3: Passive-Open | |||||||||
| Intercept | 1.76b | 0.07 | 24.58* | 1.23b | 0.06 | 20.58* | 1.24a | 0.06 | 20.21* |
| Slope | 0.51ab | 0.06 | 7.98* | 0.18b | 0.05 | 3.59* | 0.15a | 0.04 | 3.45* |
| G4: Active-Open | |||||||||
| Intercept | 1.72b | 0.12 | 14.87* | 1.15b | 0.08 | 14.29* | 1.21a | 0.08 | 15.45* |
| Slope | 0.33b | 0.07 | 4.83* | 0.23b | 0.06 | 4.08* | 0.16a | 0.05 | 3.18* |
Note. Est: estimation. Parameter estimates with the same subscripted alphabet letter in each column are statistically indistinguishable at the .05 alpha level (classic-Bonferroni correction).
p < .05.
The model comparison of intercepts (see Tables 5 & 6) showed that the intercept of the Passive-Silent profile in the lifetime alcohol model was higher than any other profile (see Figure 1). However, no significant intercept differences for lifetime alcohol use were detected among other profiles. Similarly, the intercept in the Passive-Silent profile in the two tobacco models was highest among all profiles (see Figure 2), but chewing tobacco scores were not distinguishable among profiles (see Figure 3).
Table 6.
Results from log-likelihood difference tests for free to vary model versus constrained models.
| Model | logL | df | ΔlogL | (ΔlogL)*2 | Δdf |
|---|---|---|---|---|---|
| Model: Lifetime alcohol trajectories | |||||
| Overall free to vary model | −4785.21 | 23 | — | — | |
| Intercept comparisons‡ | |||||
| C1: Passive-Silent vs. Active-Open | −4794.48 | 22 | 9.27 | 18.53*** | 1 |
| C2: Passive-Silent vs. Passive-Open | −4797.39 | 22 | 12.18 | 24.35*** | 1 |
| C3: Passive-Silent vs. Active-Silent | −4792.18 | 22 | 6.96 | 13.93*** | 1 |
| C4: Active-Silent vs. Active-Open | −4785.26 | 22 | 0.05 | 0.09 | 1 |
| Slope comparisons‡ | |||||
| C1: Active-Silent vs. Active-Open | −4788.59 | 22 | 3.38 | 6.76** | 1 |
| C2: Passive-Silent vs. Active-Open | −4788.50 | 22 | 3.29 | 6.58** | 1 |
| C3: Active-Silent vs. Passive-Open | −4786.18 | 22 | 0.97 | 1.93 | 1 |
| Model: Lifetime smoking trajectories | |||||
| Overall free to vary model | −4629.02 | 21 | — | — | |
| Intercept comparisons‡ | |||||
| C1: Passive-Silent vs. Active-Open | −4633.40 | 20 | 4.39 | 8.78** | 1 |
| C2: Passive-Silent vs. Passive-Open | −4632.51 | 20 | 3.50 | 6.99** | 1 |
| C3: Active-Silent vs. Passive-Open | −4629.85 | 20 | 0.84 | 1.68 | 1 |
| Slope comparisons‡ | |||||
| C1: Passive-Silent vs. Passive-Open | −4636.08 | 20 | 7.06 | 14.12** | 1 |
| C2: Passive-Silent vs. Active-Open | −4633.86 | 20 | 4.84 | 9.68** | 1 |
| C3: Passive-Silent vs. Active-Silent | −4630.17 | 20 | 1.16 | 2.31 | 1 |
| Model: Lifetime chewing tobacco trajectories | |||||
| Overall free to vary model | −4204.90 | 23 | — | — | |
| Intercept comparisons | |||||
| C1: Passive-Silent vs. Active-Open | −4206.40 | 22 | 1.50 | 3.01 | 1 |
| Slope comparisons | |||||
| C1: Passive-Silent vs. Passive-Open | −4206.24 | 22 | 1.35 | 2.69 | 1 |
Note.
Alpha level was adjusted based on Bonferroni correction where 0.05 alpha-level is divided by the number of tests.
p < .001,
p < .01.
To avoid unnecessarily comparison tests, the largest mean difference was tested first, followed by next greatest mean difference. Whenever a test was not significant, subsequent tests were not performed.
Figure 1.
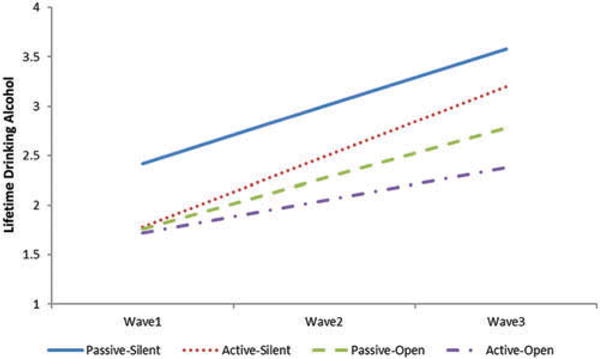
Trajectories for lifetime alcohol use from the beginning of 7th grade until the end of 8th grade.
Figure 2.
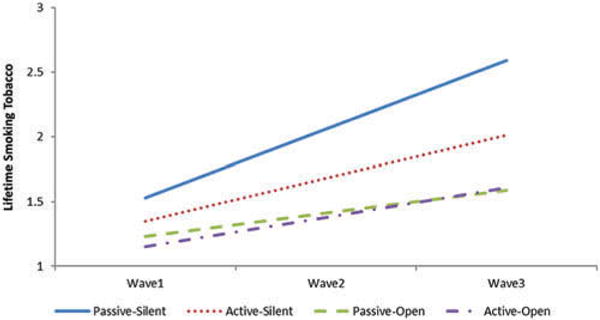
Trajectories for lifetime tobacco use from the beginning of 7th grade until the end of 8th grade.
Figure 3.
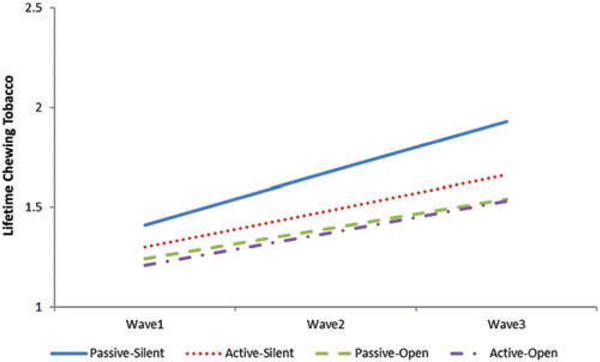
Trajectories for lifetime chewing tobacco use from the beginning of 7th grade until the end of 8th grade.
Next, slopes were compared to examine the rate of growth of use. For alcohol use, the slopes of the Active-Silent and Passive-Silent profiles were statistically higher than the one of Active-Open profile. That is, the average rate of lifetime alcohol use in Active-Silent and Passive-Silent families grew significantly faster compared with the Active-Open profile. No other slope differences were significant. In the smoking tobacco model, the slope of the Silent Passive profile was statistically higher than the slopes of Active-Open and Passive-Open profiles, but there were no significant differences in the chewing tobacco model. Thus, evidence suggests that for alcohol and cigarettes, but not for chewing tobacco, that the Passive-Silent profile, which accounts for 36% of the sample, presented the highest risk.
Discussion
The current study revealed four distinct parent prevention communication profiles and the implications of each for adolescents’ use of illicit substances. Study results extended past research examining parental prevention communication by combining SSPC and FCE into an empirically based classification, identifying four parent prevention communication profiles. Additionally, this study compared the effectiveness of these profiles on adolescent use of three illicit substances from the beginning of 7th grade to the end of 8th grade, finding significant differences between parents who encouraged expressiveness and actively participated in SSPC and parents who did not encourage expressiveness and avoided SSPC. As predicted by our guiding theory, parental prevention communication appears to influence adolescent’s substance-use behaviors. We discuss each of these findings in greater detail later.
Profiles
Affirming pluralism in the ways parents approach their role as prevention agents, these findings identified four new profiles for parental prevention communication. Empirically derived profiles diverged primarily on the degree to which they actively use substance-specific prevention communication as well as the general expressiveness in family communication. Profiles differed most cleanly along two dimensions: active/passive (use of substance-specific prevention communication) and silent/open (expressiveness) resulting in four profiles reflective of the four quadrants: Active-Silent (high SSPC, low general expressiveness, medium-to-relatively-high structural traditionalism, relatively high avoidance), Active-Open (highest SSPC, highest general expressiveness, high structural traditionalism, relatively high avoidance), Passive-Silent (lowest SSPC, lowest general expressiveness, lowest structural traditionalism, lowest avoidance), and Passive-Open (low SSPC, high general expressiveness, medium-to-relatively— high structural traditionalism, medium-to-relatively-low avoidance).
The active-open parent directly addressed substance use, applying a variety of messages and encouraged open expression of ideas and concerns in parent-adolescent communication. The passive-open parent generally promoted openness in family communication but did not directly employ prevention messages. The active-silent parent actively employed prevention messages but did not encourage discussion and the open expression of ideas between parent and adolescent. Finally, the passive-silent parent neither promoted expressiveness and discussion nor actively communicated prevention messages.
The two most common profiles in this sample were passive, with adolescents reporting few parent prevention messages. Despite the current health promotion messages asking parents to be the “antidrug” and “talk with your child about substances,” 67% of the youth report a parental profile that suggests no to very little active communication about substances or substance use. This is concerning, especially when prevention efforts in early adolescence are integral to delaying initiation of substance use and is a predictor of less substance abuse in later adolescence (Newton-Howes & Boden, 2015). Health promotion efforts may be needed for parents who do not naturally engage their adolescents in conversation, who avoid difficult topics, and/or who just trust their child to “use their own judgment” when opportunities arise for decision-making about substance use.
Effect of profiles on adolescent substance use
The findings support and extend the claim that parental prevention communication is consequential and the lack of that prevention communication may be even more important. Adolescent substance use trajectories studies demonstrate that substance use tends to increase linearly up to middle 20 s (Chen & Jacobson, 2012); thus, we anticipated a linear increase in reported use. The results reveal this increase, but it also revealed that parental prevention communication within expressive family environments significantly affected the rate of this increase in adolescent substance use behaviors. This finding advances our understanding of adolescent substance use trajectories within the context of parental prevention efforts.
These findings suggest that the primary significant differences exist between Passive-Silent and Active-Open profiles. That is, significant differences between family environments that do not encourage expressiveness or specific discussion with children about substance use and substance use issues (and hoping for the best) and family environments that encourage children to participate, along with parents, in discussions about substances and substance use. This notion of bidirectional conversation is key to understanding effective prevention communication. The most commonly reported types of parent communication reported in adolescence are permissive messages to use one’s own discretion when making choices regarding alcohol; additionally, lecturing, and setting rules are common strategies (Miller-Day, 2008).
These appear to be at odds with the bidirectional open expression of ideas revealed as most useful in this study. Even in early adolescence, a child’s opinions, attitudes, questions, and concerns should be of value in any SSPC. During this period of development, a child is actively developing the abilities to think, learn, reason, and remember. They are starting to understand that what they do now can have long-term effects, and to see that information can be interpreted in myriad ways (Boyd & Bee, 2012).
It is important to look at specific substances when interpreting the results of this study. As expected from previous research, those unexpressive parents who do not discuss substances or substance use with their children (the Passive-Silent Profile) had significantly higher alcohol use compared with the other three profiles. Moreover, silent profiles (Passive-Silent, Active-Silent) had significantly higher rates of increase in alcohol use compared to the Active-Open profile. In terms of combustible tobacco use (smoking), the Passive-Silent profile had significantly greater cigarette use and a greater rate of increase than did open profiles (Passive-Open, Active-Open) and there were no significant differences in terms of chewing tobacco.
Overall, for alcohol use, if parents are generally expressive but do not specifically address the topic of substances and substance use (Passive-Open), then their child might not use alcohol at 7th grade but they may be more likely to use alcohol and tobacco earlier than youth with parents who are both generally expressive and specifically address the topic of preventing alcohol use (Active-Open). It is very important to prevent adolescent alcohol use altogether, but also important to delay experimentation and use of alcohol as much as possible (Hawkins et al., 1997). In sum, family environments that are generally expressive, with parents who directly address the topic of substances and substance use (Active-Open) are the most effective combination overall, with the least effective being family environments that are not expressive and parents who avoid directly addressing the topic of substances or substance use.
Given the research to-date, it is surprising that the effects of the Active-Silent profile varied depending on type of substance. We had expected consistent impact of these prevention approaches across all substances. Additional research efforts may be needed to address differences across substance. The Passive-Silent profile demonstrated the most overall alcohol and tobacco use, as well as the fastest rates of increase. This is not surprising given this profile reflects a passive approach to prevention communication within the context of a generally nonexpressive family communication style. Moreover, these findings are consistent with a meta-analysis that observed better psychosocial outcomes were associated with high levels of expressiveness (Schrodt, Witt, & Messersmith, 2008). Although not statistically different at the end of 8th grade, if the trajectories continued throughout high school, it is likely the Open versus Silent profiles would continue to diverge, likely reaching statistical significance.
Validating the findings of previous research (Kam, 2011; Miller-Day, 2008), expressive parents who communicate with—rather than at–their children and address substance use specifically reported the lowest substance use across time, emphasizing the role of parents in antidrug use socialization. Those parents who actively participated in prevention communication (active profiles) often used a variety of prevention messages, but since the Active-Open profile seemed to have the most sustained effects over time with most substances, perhaps examining thresholds in the messages between Active-Open and Active-Silent might be useful.
When comparing mean differences between the Active-Open and Active-Silent profiles, it appears that the bidirectional nature of expressive communication family environments may be consequential when making these messages “stick.” Significantly Active-Open profile parents more frequently asked about their children’s thoughts and opinions about drinking alcohol, smoking/chewing or other substance use than did parents in the Active-Silent profile or any of the other profiles. The sustained effects of the Active-Open profile over other profiles on adolescence alcohol use behavior seems to support the added effects of SSPC given the fact that alcohol use can play a role as “gateway” of other drugs (Kirby & Barry, 2012).
Finally, the existence of four different parent prevention profiles indicates that, indeed, one size does not fit all in terms of family-based prevention efforts. Given this variation, it seems prudent to consider what alternative prevention communication strategies might be effective for families fitting different prevention profiles, especially those families who are Passive-Silent (36% in the current study) and who might not feel comfortable addressing sensitive topics such as substance use. Perhaps interventions are needed for these families to facilitate communication on the topic of substance use and prevention.
One promising intervention strategy that could be developed and adapted to different profiles are e-learning or web-based brief interventions (Lustria et al., 2013). Web-based learning modules might be tailored to parents based on the four parent prevention profiles identified in this study allowing developers to tailor messages, provide behavioral models based on the preferred communication style of the parent, and also provide interactive “coaching” for parents. With e-learning, messages can be tailored to the specific user (Lustria et al., 2013). For example, if a parent indicates she is female, all messages on subsequent pages will include female pronouns. First names will be inserted to heighten identification.
For example, “Sandra, you seem to be a [Passive-Silent] parent who trusts your child to do the right thing without you having to influence them much. Click here to see videos, get tips, and find information on how parents like you, who value your child’s freedom of choice, might best communicate with your child about alcohol and alcohol use.” Although the research in the area of web-based family interventions is limited, early research in the area of substance use prevention and brief web-based interventions is promising (Jander, Crutzen, Mercken, & De Vries, 2015). Based on the findings from this current study, we contend that, at a minimum, additional efforts are needed to assist Passive-Silent families in their efforts to comfortably communicate antisubstance use messages to their adolescent children.
Limitations and conclusions
Several limitations of the current study should be noted. Data were collected only from the adolescent’s perspective reflecting their perceptions of parental approaches and specific messages (e.g., specific rules or specific negative consequences for substance use) were not examined. Future research should explore the variety of topics parents’ address within the different profiles and explore if similar topics are communicated differently across profiles. Moreover, studies are needed to assess if some prevention messages are more effective than others—in general and during specific developmental periods. Parental messages may be in reaction to youth substance use, therefore this must be considered in future research as well as collecting parental use from parents if possible.
In addition, all of the youth in this study lived in rural communities and were predominantly White. More cultural variation is needed to test the generalizability of the findings. Similarly, an extended age range, both younger and older youth, would provide a more comprehensive picture of these processes. Single items for substance use might be considered less than optimal, but Dollinger and Malmquist (2009) showed that single item for substance use in self-report is valid and reliable and, in spite of possible social desirability bias resulting from self-report measurements, data from studies assuring confidentiality are considered to be valid (Harrison & Hughes, 1997; Maisto, McKay, & Connors, 1990).
It is possible that there is variability within profiles. For example, some youth in active-open profiles may have higher increased trajectories compared with other youth within the same profile. It would be useful to assess if variables such as gender influence potential differences within a certain parental prevention profile. However, given the complexity of models, several potential confounding variables (e.g., gender) were not included in our analysis. Future studies should consider how other variables can play roles in adolescent substance-use trajectories given the family communication profiles. Finally, to link this line of research with the broader family studies literature a logical next step might be to investigate parent prevention profiles while controlling for parenting style and parent-child relationship quality and exploring associations among these variables.
In sum, these findings demonstrate a diversity of approaches to parental prevention communication—not all families are the same. This study reinforces the work of Miller-Day (2008) and Kam (2011), demonstrating the complexity of parent-child communication about substances and that adolescents rely on parental messages for antisubstance use socialization. It also extends this work by revealing that parents with different prevention communication profiles approach prevention differently. It may be that contradictory findings regarding the efficacy of parent-adolescent communication in preventing substance use might stem from these disparate approaches to parent prevention communication and the inconsistency between those approaches and what prevention programs advocate. Perhaps utilizing an adaptive intervention framework with parent prevention communication profiles used as the calibration variable could stipulate different intervention content for different family types (see Collins, Murphy, & Bierman, 2004). Findings from this study show that when it comes to families, there is no one way of accomplishing prevention goals. Perhaps adapting intervention efforts to account for different parent prevention communication profiles might be useful when developing programs responsive to family diversity in prevention efforts.
Acknowledgments
This article’s contents are solely the responsibility of the authors and do not necessarily represent the official views of the National Institutes of Health. Portions of this article were presented at the 2013 annual meeting of the National Communication Association.
Funding
This publication was supported by Grant Number R01DA021670 from the National Institute on Drug Abuse to The Pennsylvania State University (Michael Hecht, Principal Investigator).
Footnotes
Color versions of one or more of the figures in the article can be found online at www.tandfonline.com/hjfc.
There is no conflict of interest.
ORCID
Hye Jeong Choi http://orcid.org/0000-0003-0996-0713)
Michelle Miller-Day http://orcid.org/0000-0003-3248-6095
YoungJu Shin http://orcid.org/0000-0001-6751-8064
Jonathan Pettigrew http://orcid.org/0000-0001-7938-784X
Janice L. Krieger http://orcid.org/0000-0001-9950-9170
References
- Ackard DM, Neumak-Sztainer D, Story M, Perry C. Parent–child connectedness and behavioral and emotional health among adolescents. American Journal of Preventive Medicine. 2006;30:59–66. doi: 10.1016/j.amepre.2005.09.013. [DOI] [PubMed] [Google Scholar]
- Baan R, Straif K, Grosse Y, Secretan B, El Ghissassi F, Bouvard V, Cogliano V. WHO International Agency for Research on Cancer Monograph Working Group. Carcinogenicity of alcoholic beverages. Lancet Oncology. 2007;8:292–293. doi: 10.1016/S1470-2045(07)70099-2. [DOI] [PubMed] [Google Scholar]
- Baxter LA, Bylund CL, Imes RS, Scheive DM. Family communication environments and rule-based social control of adolescents’ healthy lifestyle choices. Journal of Family Communication. 2005;5:209–227. doi: 10.1207/s15327698jfc0503_3. [DOI] [Google Scholar]
- Boyd DR, Bee HL. The developing child. New York, NY: Pearson; 2012. [Google Scholar]
- Cabin RJ, Mitchell RJ. To Bonferroni or not to Bonferroni: When and how are the questions. Bulletin of the Ecological Society of America. 2000;81:246–248. [Google Scholar]
- Cavazos-Rehg PA, Housten AJ, Krauss MJ, Sowles SJ, Spitznagel EL, Chaloupka FJ, Bierut LJ. Selected state policies and associations with alcohol use behaviors and risky driving behaviors among youth: Findings from Monitoring the Future study. Alcoholism: Clinical and Experimental Research. 2016;40:1030–1036. doi: 10.1111/acer.13041. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Chen P, Jacobson KC. Developmental trajectories of substance use from early adolescence to young adulthood: Gender and racial/ethnic differences. Journal of Adolescent Health. 2012;50:154–163. doi: 10.1016/j.jadohealth.2011.05.013. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Colby M, Hecht ML, Miller-Day M, Krieger J, Syvertsen A, Graham J, Pettigrew J. Adapting school-based substance use prevention curriculum through cultural grounding: A review and exemplar of adaptation processes for rural schools. American Journal of Community Psychology. 2013;51:190–205. doi: 10.1007/s10464-012-9524-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Collins LM, Murphy SA, Bierman KL. A conceptual framework for adaptive preventive interventions. Prevention Science. 2004;5(3):185–196. doi: 10.1023/B:PREV.0000037641.26017.00. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Connella AM, Frye AA. Growth mixture modelling in developmental psychology: Overview and demonstration of heterogeneity in developmental trajectories of adolescent antisocial behaviour. Infant and Child Development. 2006;15:609–621. doi: 10.1002/icd.481. [DOI] [Google Scholar]
- Dollinger SJ, Malmquist D. Reliability and validity of single-item self-reports: With special relevance to college students’ alcohol use, religiosity, study, and social life. The Journal of General Psychology. 2009;136:231–242. doi: 10.3200/GENP.136.3.231-242. [DOI] [PubMed] [Google Scholar]
- Ebersole DS, Miller-Day M, Raup-Krieger J. Do actions speak louder than words? Adolescent interpretations of parental substance use. Journal of Family Communication. 2014;14:328–351. doi: 10.1080/15267431.2014.945699. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Enders CK, Bandalos DL. The relative performance of full information maximum likelihood estimation for missing data in structural equation models. Structural Equation Modeling: A Multidisciplinary Journal. 2001;8:430–457. doi: 10.1207/S15328007SEM0803_5. [DOI] [Google Scholar]
- Ennett ST, Bauman KE, Foshee VA, Pembertonm M, Hicks K. Parent–child communication about adolescent tobacco and alcohol use: What do parents say and does it affect youth behavior? Journal of Marriage and the Family. 2001;63:48–62. doi: 10.1111/j.1741-3737.2001.00048.x. [DOI] [Google Scholar]
- Fitzpatrick MA, Ritchie LD. Communication schemata within the family. Human Communication Research. 1994;20:275–301. doi: 10.1111/j.1468-2958.1994.tb00324.x. [DOI] [Google Scholar]
- Graham JW, Cumsille PE, Elek-Fisk E. Methods of handling missing data. In: Schinka JA, Velicer WF, editors. Research methods in psychology. New York, NY: John Wiley & Sons; 2003. pp. 87–114. [Google Scholar]
- Graham JW, Hofer SM, MacKinnon DP. Maximizing the usefulness of data obtained with planned missing value patterns: An application of maximum likelihood procedures. Multivariate Behavioral Research. 1996;31:197–218. doi: 10.1207/s15327906mbr3102_3. [DOI] [PubMed] [Google Scholar]
- Graham JW, Pettigrew J, Miller-Day M, Krieger JL, Zhou J, Hecht ML. Random assignment of schools to groups in the Drug Resistance Strategies Rural Project: Some new methodological twists. Prevention Science. 2014;15:516–525. doi: 10.1007/s11121-013-0403-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hansen WB, Graham JW. Preventing alcohol, marijuana, and cigarette use among adolescents: Peer pressure resistance training versus establishing conservative norms. Preventive Medicine. 1991;20:414–430. doi: 10.1016/0091-7435(91)90039-7. [DOI] [PubMed] [Google Scholar]
- Harrison L, Hughes A. The validity of self-reported drug use: Improving the accuracy of survey estimates. Rockville, MD: National Institute on Drug Abuse; 1997. (NIDA Research Monograph 167). NIH Publication No. 97-4147. [PubMed] [Google Scholar]
- Hawkins JD, Graham JW, Maguin E, Abbott R, Hill KG, Catalano RF. Exploring the effects of age of alcohol use initiation and psychosocial risk factors on subsequent alcohol misuse. Journal of Studies on Alcohol. 1997;58:280–290. doi: 10.15288/jsa.1997.58.280. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Jander A, Crutzen R, Mercken L, De Vries H. Web-based interventions to decrease alcohol use in adolescents: A Delphi study about increasing effectiveness and reducing drop-out. BMC Public Health. 2015;15:340–353. doi: 10.1186/s12889-015-1639-z. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Johnston L. Monitoring the future: National results on adolescent drug use: Overview of key findings. Darby, PA: Diane; 2010. [Google Scholar]
- Kam JA. Identifying changes in youth’s subgroup membership over time based on their targeted communication about substance use with parents and friends. Human Communication Research. 2011;37:324–349. doi: 10.1111/j.1468-2958.2011.01408.x. [DOI] [Google Scholar]
- Kam JA, Castro FG, Wang N. Parent–child communication’s attenuating effects on Mexican early adolescents’ perceived discrimination, depressive symptoms, and substance use. Human Communication Research. 2014;41:204–225. doi: 10.1111/hcre.12043. [DOI] [Google Scholar]
- Kam JA, Matsunaga M, Hecht ML, Ndiaye K. Extending the theory of planned behavior to predict alcohol, tobacco, and marijuana use among youth of Mexican heritage. Prevention Science. 2009;10:41–53. doi: 10.1007/s11121-008-0110-0. [DOI] [PubMed] [Google Scholar]
- Kam JA, Middleton AV. The associations between parents’ references to their own past substance use and youth’s substance-use beliefs and behaviors: A comparison of Latino and European American youth. Human Communication Research. 2013;39:208–229. doi: 10.1111/hcre.12001. [DOI] [Google Scholar]
- Kam JA, Potocki B, Hecht ML. Encouraging Mexican-heritage youth to intervene when friends drink: The role of targeted parent-child communication against alcohol. Communication Research. 2014;14:544–664. doi: 10.1177/0093650212446621. [DOI] [Google Scholar]
- Kam JA, Yang S. Explicating how parent–child communication increases Latino and European American early adolescents’ intentions to intervene in a friend’s substance use. Prevention Science. 2013;15:536–546. doi: 10.1007/s11121-013-0404-8. [DOI] [PubMed] [Google Scholar]
- Kirby T, Barry AE. Alcohol as a gateway drug: A study of US 12th graders. Journal of School Health. 2012;82:371–379. doi: 10.1111/j.1746-1561.2012.00712.x. [DOI] [PubMed] [Google Scholar]
- Koerner AF, Fitzpatrick MA. Toward a theory of family communication. Communication Theory. 2002;12:70–91. doi: 10.1111/j.1468-2885.2002.tb00260.x. [DOI] [Google Scholar]
- Komro KA, Perry CL, Veblen-Mortenson S, Farbakhsh K, Toomey TL, Stigler MH, Williams CL. Outcomes from a randomized controlled trial of a multi-component alcohol use preventive intervention for urban youth: Project Northland Chicago. Addiction. 2008;103:606–618. doi: 10.1111/j.1360-0443.2007.02110.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kumpfer KL, Alvarado R, Whiteside HO. Family-based interventions for substance use and misuse prevention. Substance Use & Misuse. 2003;38:1759–1787. doi: 10.1081/JA-120024240. [DOI] [PubMed] [Google Scholar]
- Lustria MLA, Noar SM, Cortese J, Van Stee SK, Glueckauf RL, Lee J. A meta-analysis of web-delivered tailored health behavior change interventions. Journal of Health Communication. 2013;18:1039–1069. doi: 10.1080/10810730.2013.768727. [DOI] [PubMed] [Google Scholar]
- Maisto SA, McKay JR, Connors GJ. Self-report issues in substance abuse: State of the art and future directions. Behavioral Assessment. 1990;12:117–134. [Google Scholar]
- Matsunaga M, Hecht ML, Elek E, Ndiaye K. Ethnic identity development and acculturation: A longitudinal analysis of Mexican-heritage youth in the southwest United States. Journal of Cross-Cultural Psychology. 2010;41:410–427. doi: 10.1177/0022022109359689. [DOI] [PMC free article] [PubMed] [Google Scholar]
- McLachlan GJ, Peel D. Finite mixture models. New York, NY: Wiley; 2000. [Google Scholar]
- Miech RA, Johnston LD, O’Malley PM, Bachman JG, Schulenberg JE. Monitoring the Future national survey results on drug use 1975–2014. Darby, PA: Diane; 2015. [Google Scholar]
- Miller M, Alberts JK, Hecht ML, Trost M, Krizek RL. Adolescent relationships and drug use. Mahwah, NJ: Lawrence Erlbaum Associates; 2000. [Google Scholar]
- Miller-Day M. Parent-adolescent communication about alcohol, tobacco, and other drug use. Journal of Adolescent Research. 2002;17:604–616. doi: 10.1177/074355802237466. [DOI] [Google Scholar]
- Miller-Day M. Talking to youth about drugs: What do late adolescents say about parental strategies? Family Relations. 2008;57:1–12. doi: 10.1111/j.1741-3729.2007.00478.x. [DOI] [Google Scholar]
- Miller-Day M, Dodd AH. Toward a descriptive model of parent–offspring communication about alcohol and other drugs. Journal of Social and Personal Relationships. 2004;21:69–91. doi: 10.1177/0265407504039846. [DOI] [Google Scholar]
- Miller-Day M, Hecht ML. Narrative means to preventative ends: A narrative engagement framework for designing prevention interventions. Health Communication. 2013;28:657–670. doi: 10.1080/10410236.2012.762861. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Miller-Day M, Kam JA. More than just openness: Developing and validating a measure of targeted parent–child communication about alcohol. Health Communication. 2010;25:293–302. doi: 10.1080/10410231003698952. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Muthén LK, Muthén BO. Mplus users’ guide. Los Angeles, CA: Muthén & Muthén; 2007. [Google Scholar]
- Napper LE, Froidevaux NM, LaBrie JW. Being blunt about marijuana: Parent communication about marijuana with their emerging adult children. Prevention Science. 2016;17:882–891. doi: 10.1007/s11121-016-0681-0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Napper LE, Hummer JF, Lac A, LaBrie JW. What are other parents saying? Perceived parental communication norms and the relationship between alcohol-specific parental communication and college student drinking. Psychology of Addictive Behaviors. 2014;28(1):31–41. doi: 10.1037/a0034496. [DOI] [PMC free article] [PubMed] [Google Scholar]
- National Center for Statistics and Analysis. Young drivers: 2014 data. Washington, DC: National Highway Traffic Safety Administration; 2016. May, (Traffic Safety Facts. Report No. DOT HS 812 278). [Google Scholar]
- National Institute on Drug Abuse. Monitoring the Future 2015: Teen drug use. 2016 Retrieved from www.drugabuse.gov.
- Newman DA. Longitudinal modeling with randomly and systematically missing data: A simulation of ad hoc, maximum likelihood, and multiple imputation techniques. Organizational Research Methods. 2003;6:328–362. doi: 10.1177/1094428103254673. [DOI] [Google Scholar]
- Newton-Howes G, Boden JM. Relation between age of first drinking and mental health and alcohol and drug disorders in adulthood: Evidence from a 35-year cohort study. Addiction. 2015;111:637–644. doi: 10.1111/add.13230. [DOI] [PubMed] [Google Scholar]
- Noar SM, Harrington NG, Aldrich RS. The role of message tailoring in the development of persuasive health communication messages. Annals of the International Communication Association. 2009;33:73–133. doi: 10.1080/23808985.2009.11679085. [DOI] [Google Scholar]
- Nylund KL, Asparouhov T, Muthen B. Deciding on the number of classes in latent class analysis and growth mixture modeling. A Monte Carlo simulation study. Structural Equation Modeling. 2007;14:535–569. doi: 10.1080/10705510701575396. [DOI] [Google Scholar]
- Oetting ER, Donnermeyer JF. Primary socialization theory: The etiology of drug use and deviance. Substance Use & Misuse. 1998;33:995–1026. doi: 10.3109/10826089809056252. [DOI] [PubMed] [Google Scholar]
- Preacher KJ, Wichman AL, MacCallum RC, Briggs NE. Latent growth curve modeling. Los Angeles, CA: Sage; 2008. [Google Scholar]
- Reimuller A, Hussong A, Ennett ST. The influence of alcohol-specific communication on adolescent alcohol use and alcohol-related consequences. Prevention Science. 2011;12:389–400. doi: 10.1007/s11121-011-0227-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Rice WR. Analyzing tables of statistical tests. Evolution. 1989;43:223–225. doi: 10.2307/2409177. [DOI] [PubMed] [Google Scholar]
- Schrodt P, Witt PL, Messersmith AS. A meta-analytic review of family communication patterns and their associations with information processing, behavioral, and psychosocial outcomes. Communication Monographs. 2008;75:248–269. doi: 10.1080/03637750802256318. [DOI] [Google Scholar]
- Schwartz G. Estimating the dimension of a model. The Annals of Statistics. 1978;6:461–464. doi: 10.1214/aos/1176344136. [DOI] [Google Scholar]
- Shield KD, Parry C, Rehm J. Focus on: Chronic diseases and conditions related to alcohol use. Alcohol Research: Current Reviews. 2013;35:155–173. doi: 10.35946/arcr.v35.2.06. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Spoth R, Trudeau L, Guyll M, Shin C, Redmond C. Universal intervention effects on substance use among young adults mediated by delayed adolescent substance initiation. Journal of Consulting and Clinical Psychology. 2009;77:620–632. doi: 10.1037/a0016029. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Stephenson MT, Quick BL, Atkinson J, Tschida DA. Authoritative parenting and drug-prevention practices: Implications for antidrug ads for parents. Health Communication. 2005;17:301–321. doi: 10.1207/s15327027hc1703_6. [DOI] [PubMed] [Google Scholar]
- Substance Abuse and Mental Health Services Administration, Center for Behavioral Health Statistics and Quality. Drug abuse warning network: Detailed tables: National estimates, drug-related emergency department visits for. Rockville, MD: Substance Abuse and Mental Health Services Administration; 2013. pp. 2006–2011. [Google Scholar]
- Tofighi D, Enders CK. Identifying the correct number of classes in a growth mixture model. In: Hancock GR, editor. Mixture models in latent variable research. Greenwich, CT: Information Age; 2007. pp. 317–341. [Google Scholar]
- Turrisi R, Wiersma KA, Hughes KK. Binge-drinking-related consequences in college students: Role of drinking beliefs and mother–teen communications. Psychology of Addictive Behaviors. 2000;14:342–355. doi: 10.1037/0893-164X.14.4.342. [DOI] [PubMed] [Google Scholar]
- Vermeulen-Smit E, Verdurmen JEE, Engels RCME. The effectiveness of family interventions in preventing adolescent illicit drug use: A systematic review and meta-analysis of randomized controlled trials. Clinical Child and Family Psychology Review. 2015;18:218–239. doi: 10.1007/s10567-015-0185-7. [DOI] [PubMed] [Google Scholar]
- Vermunt JK, Magidson J. Latent class cluster analysis. In: Hagenaars JA, McCutcheon AL, editors. Applied latent class analysis. New York, NY: Cambridge University Press; 2002. pp. 89–106. [Google Scholar]
- Williams LR, Ayers S, Baldwin A, Marsiglia FF. Delaying youth substance-use initiation: A cluster randomized controlled trial of complementary youth and parenting interventions. Journal of the Society for Social Work and Research. 2016;7:177–200. doi: 10.1086/685298. [DOI] [Google Scholar]
- Yang C. Evaluating latent class analysis models in qualitative phenotype identification. Computational Statistics & Data Analysis. 2006;50:1090–1104. doi: 10.1016/j.csda.2004.11.004. [DOI] [Google Scholar]