

Abstract
Young children in foster care often experience adversity, such as maltreatment and lack of stability in early caregiving relationships. As a result, these children are at risk for a range of problems, including deficits in executive functioning. The Attachment and Biobehavioral Catch-up for Toddlers (ABC-T) intervention was designed to help foster parents behave in ways that promote the development of young children’s emerging self-regulatory capabilities. Participants included 173 parent–toddler dyads in three groups: foster families that were randomly assigned to receive either the ABC-T intervention (n = 63) or a control intervention (n = 58), as well as low-risk parent–toddler dyads from intact families (n = 52). At a follow-up conducted when children were approximately 48 months old, children’s executive functioning abilities were assessed with the attention problems scale of the Child Behavior Checklist (Achenbach & Rescorla, 2000) and a graded version of the Dimensional Change Card Sort developed for preschoolers (Beck, Schaefer, Pang, & Carlson, 2011). Results showed that foster children whose parents received the ABC-T intervention and low-risk children never placed in foster care had fewer parent-reported attention problems and demonstrated greater cognitive flexibility during the Dimensional Change Card Sort than foster children whose parents received the control intervention. These results indicate that an attachment-based intervention implemented among toddlers in foster care is effective in enhancing children’s executive functioning capabilities.
Children in foster care are at risk for negative developmental outcomes as the result of experiences of abuse, neglect, and unstable attachment relationships (Jackson, Gabrielli, Fleming, Tunno, & Makanui, 2014). In addition to the initial removal from their birth parents, children in foster care often experience repeated disruptions in their attachment relationships as they transition between multiple caregivers and placements (Dozier & Lindhiem, 2006; Sanchirico & Jablonka, 2000). As a result, foster children often struggle with effectively regulating their cognitions (Bernedo, Salas, Fuentes, & García-Martín, 2014; Tarren-Sweeney, 2008), emotions (Pears, Kim, Buchanan, & Fisher, 2015), behaviors (Clausen, Landsverk, Ganger, Chadwick, & Litrownik, 1998; Keller et al., 2001), and physiology (Bernard, Butzin-Dozier, Rittenhouse, & Dozier, 2010; Bruce, Fisher, Pears, & Levine, 2009).
In the United States, about 20% of children in foster care are between the ages of 1 and 3 years old (US Department of Health and Human Services, 2015). Children in this age group face several critical developmental tasks: establishing attachment relationships with caregivers (Sroufe, 2005), using attachment relationships to coregulate difficult emotions (Cassidy, 1994), and developing strategies to become increasingly independent in regulating their emotions (Cole et al., 2011). The task of developing independent self-regulatory strategies is particularly difficult for toddlers who have experienced early adversity (Bernard et al., 2010; Bruce et al., 2009), which can make parenting toddlers in foster care quite challenging. In particular, these children often struggle with dysregulation and may have difficulty clearly signaling their need for support (Dozier & Bick, 2007).
Although interventions supporting the development of children in the child welfare system have been developed (Dozier, Higley, Albus, & Nutter, 2002; Fisher, Gunnar, Dozier, Bruce, & Pears, 2006), these interventions do not address the unique developmental needs of toddlers. To fill this gap in services, the Attachment and Biobehavioral Catch-up for Toddlers (ABC-T) was adapted from the Attachment and Biobehavioral Catch-up for Infants (ABC-I) intervention, which has been found to be efficacious in supporting the development of infants who have experienced early adversity (Dozier, Meade, & Bernard, 2014). Similar to the ABC-I intervention, ABC-T was designed to help foster parents behave in sensitive and nurturing ways to promote the development of secure attachment relationships and to support children’s physiological and behavioral regulation. In addition to these original goals of ABC-I, the ABC-T intervention encourages parents to use the attachment relationship to help toddlers calm down effectively when they are frustrated or overwrought. Unlike interventions that aim to enhance children’s behavioral regulation using strategies with strong self-regulatory demands (e.g., time out), ABC-T focuses on helping the parent stay physically and psychologically available to the child, thus serving as an effective coregulator. These positive experiences of coregulation are seen as critical from an attachment perspective because they provide the young child with experiences of an available parent when he or she is struggling with potentially overwhelming emotions. The parent’s support can help the child modulate emotion, providing a model and positive experiences of regulating negative emotions. Over time and with continued support, the child can begin to take over some of the regulatory demands, as the positive parent–child interactions provide a foundation for increasingly independent regulation. Given the emphasis on enhancing children’s regulatory capabilities in the ABC-T intervention, we expected the intervention to promote foster children’s executive functioning, an important predictor of later success in handling challenges in academic and peer contexts (Allan, Hume, Allan, Farrington, & Lonigan, 2014).
Caregiving Influences on the Development of Executive Functioning
Executive functioning refers to an interrelated set of top-down neurocognitive processes involved in the conscious, goal-directed control of attention, thought, behavior, and emotion; included among these executive functions are cognitive flexibility, inhibitory and attentional control, and working memory (Miyake, 2000; Zelazo & Frye, 1998). Though executive functioning skills begin to emerge in infancy, a dramatic improvement in these capabilities occurs during the toddler and preschool periods, and these foundational skills provide the basis for future, more advanced cognitive, behavioral, and emotional regulation abilities (Blair, 2016; Carlson, Mandell, & Williams, 2004; Diamond, 2013; Hughes & Ensor, 2007, 2011). Executive functioning deficits in early childhood have been shown to predict various problematic developmental outcomes, including poor academic achievement (Allan et al., 2014), behavioral problems (Hughes & Ensor, 2006), and attention-deficit/hyperactivity disorder (Semrud-Clikeman, Walkowiak, Wilkinson, & Butcher, 2010).
Early experiences within parent–child attachment relationships are believed to play a critical role in promoting the development of children’s self-regulatory capabilities. During infancy, children depend on their parents as coregulatory partners to help with emotional, attentional, and behavioral modulation (Hofer, 2004; Kopp, 1982; Raver, 1996). Parents who interact with their children in sensitive ways, interpreting their children’s signals and responding promptly and appropriately, help children regulate effectively (Kopp, 2002; Laible, Thompson, & Froimson, 2015). Sensitive caregiving helps promote children’s budding self-control abilities by actively supporting children’s engagement with contextual challenges, avoiding excessive stimulation of children, and soothing children effectively when they are distressed. During toddlerhood, sensitive caregiving involves remaining physically and psychologically available to children during experiences of anger or frustration, thereby helping regulate negative emotions. As children become more independent through developmental advances in gross motor, cognitive, and language abilities, they take increasingly active roles in their own self-regulation (Diener & Mangelsdorf, 1999; Harrist & Waugh, 2002). It is thought that children who experience highly sensitive parenting internalize the effective regulation strategies they learn through coregulation, leading to the development of strong self-regulatory capabilities over time.
Sensitive parenting has been observed to predict improved performance on executive functioning tasks later in development (Bernier, Beauchamp, Carlson, & Lalonde, 2015; Bernier, Carlson, & Whipple, 2010; Conway & Stifter, 2012; Moilanen, Shaw, Dishion, Gardner, & Wilson, 2010), and to buffer children from the harmful effects of early adverse experiences (Asok, Bernard, Roth, Rosen, & Dozier, 2013; Belsky & Fearon, 2002; Laucht, Esser, & Schmidt, 2001; Serbin, Hubert, Hastings, Stack, & Schwartzman, 2014). The impact of parenting on executive functioning may have implications for other child outcomes as well, as executive functioning has been found to mediate the link between early insensitive parenting and children’s later externalizing problems and social difficulties (Bindman, Pomerantz, & Roisman, 2015; Conway et al., 2014; Low & Webster, 2015; Sulik et al., 2015).
ABC-I
The ABC-I intervention was designed to increase this sensitive parenting behavior, thereby enhancing infants’ ability to regulate their behavior, emotion, physiology, and cognition. ABC-I focuses on (a) increasing parents’ nurturing care when children are distressed, (b) helping parents follow children’s lead, and (c) decreasing frightening parenting behaviors. Clinicians, who are referred to as “parent coaches,” attempt to change parental behavior in several ways, including discussing research evidence relevant to each target behavior, helping parents practice the behaviors during structured activities with their infants, pointing out times when parents successfully engage in the targeted behaviors, and using video feedback to further reinforce target behaviors. The ABC-I consists of 10 manualized sessions with parents and infants and is implemented in the families’ homes.
The ABC-I has a strong evidence base. Randomized clinical trials with both foster parents and birth parents involved in Child Protective Services have demonstrated that ABC-I is efficacious in improving theoretically and clinically important outcomes, including parents’ sensitive caregiving (Bick & Dozier, 2013), children’s attachment security (Bernard et al., 2012; Dozier et al., 2009), diurnal cortisol levels (Bernard, Dozier, Bick, & Gordon, 2015), and negative emotion expression (Lind, Bernard, Ross, & Dozier, 2014). Most relevant to the current study, the ABC-I intervention also enhances children’s cognitive control abilities. Infants in foster care whose parents received the ABC-I intervention showed greater cognitive flexibility at age 5 than children whose parents received a control intervention (Lewis-Morrarty, Dozier, Bernard, Terracciano, & Moore, 2012).
ABC-T
Given the success of intervening with infants and parents with the ABC-I intervention, ABC-T was developed to enhance parenting behaviors relevant to the developmental changes occurring during toddlerhood. Although promoting secure attachment relationships and physiological regulation through sensitive parenting remains an important intervention target for toddlers, unique developmental challenges emerge at this age (Sroufe, 1979, 1996). In particular, self-regulatory capabilities show rapid development during toddlerhood, as children move from relying on external regulation from their parents to more independent, internal regulation strategies (Eisenberg, Cumberland, & Spinrad, 1998; Kopp, 1982; Silk et al., 2011). During this period, toddlers become increasingly competent in some areas, such as motor skills and mobility, but do not yet have the cognitive abilities to fully understand the consequences of their behavior or to regulate their emotions consistently and effectively (Kopp, 2011; Premo & Kiel, 2014). Thus, toddlers and parents must balance toddlers’ growing need to use independent regulation strategies, even while they are still largely reliant on their parents for help with regulating their emotions and behaviors. Toddlers are often frustrated by this process and become dysregulated, displaying intense negative affect and oppositional, defiant behavior (Shaw, Bell, & Gilliom, 2000). These behaviors can elicit strong emotional reactions from parents that may lead to ineffective coregulatory strategies, such as minimizing/dismissing negative emotion and punitive responses (Fabes, Leonard, Kupanoff, & Martin, 2001). Parents need to override strong emotional reactions to serve as effective coregulators for their children.
The ABC-T intervention was developed to address the emerging regulatory difficulties faced by children who have experienced early adversity, and the challenges faced by parents caring for them. Specifically, ABC-T seeks to enhance children’s regulatory capabilities by (a) increasing parents’ nurturing behaviors in response to children’s distress, (b) increasing parents’ responsiveness to children’s nondistress signals (i.e., “following the lead”), and (c) encouraging parents to serve as coregulators for their children under challenging conditions. Two of the three primary intervention targets (nurturance and following the lead) were shared across the infant and toddler intervention, although they were adapted for older children in ABC-T. These parenting targets were retained because as core components of the ABC-I intervention, they were effective in enhancing physiological regulation (Bernard et al., 2015) as well as cognitive self-regulation (Lewis-Morrarty et al., 2012). These core components of the ABC-I intervention have also been shown to be effective in promoting the secure, organized attachment relationships in which coregulatory strategies could be rooted (Bernard et al., 2012; Dozier et al., 2009).
In addition to these parenting strategies common to the ABC-I intervention, ABC-T focuses on teaching parents strategies for serving as coregulators to their children when children become dysregulated. Opportunities for parental nurturing (a core target in both ABC-I and ABC-T) are distinguished from opportunities for parental coregulating or calming (a target in ABC-T only) based on the specific child emotions that trigger the parental response. Parental nurturance opportunities include times when children are sad, hurt, scared, or worried, whereas parental calming opportunities include times when the child is frustrated, irritated, angry, or otherwise overwhelmed by emotions. The ABC-T helps parents recognize these as coregulation opportunities, understand the importance of remaining psychologically available to their children rather than minimizing their children’s emotions, and implement behaviors that effectively soothe and calm their children. Parent coaches also discuss the importance of avoiding behaviors that can lead to or exacerbate child dysregulation, such as tickling, yelling, lecturing, and unnecessary arguing or butting heads.
Unlike other interventions targeting dysregulated and oppositional behavior in young children, the ABC-T intervention makes the assumption that the parent–child relationship is enhanced if the parent can remain physically and psychologically available to help the child manage his or her behavior and emotions. Thus, ABC-T does not rely on behaviorally based strategies aimed at behavior management, such as time-out or ignoring children’s displays of strong affect (Barkley, 2013; McNeil & Hembree-Kligin, 2010). Instead, ABC-T emphasizes parents’ role as coregulators for children, and the importance of parents’ emotional and physical availability during times when children are overwhelmed by emotion. By teaching strategies to promote effective coregulation and helping parents recognize and override their automatic emotional and behavioral reactions in these situations, ABC-T helps parents and children develop more effective coregulatory processes. These coregulatory processes are, in turn, expected to promote the subsequent development of children’s effective self-regulatory abilities.
Similar to ABC-I, the ABC-T intervention is conducted in families’ homes, and consists of 10 manualized sessions. The goals of the intervention are communicated through discussion of child development research, showing videos clips, pointing out times when parents successfully engage in one of the targeted behaviors, and explaining the importance of following the lead, nurturing, and calming behaviors.
Current Study
This study represents the initial evaluation of the efficacy of the ABC-T intervention for enhancing executive functioning among young children in foster care. Foster children were randomly assigned to receive either ABC-T or a control intervention, Developmental Education for Families (DEF), which focused on directly enhancing children’s motor, cognitive, and language skills. The DEF intervention taught parents how to integrate activities designed to support their children’s development in the targeted areas with play activities (e.g., exercises aimed at gross motor development that are presented to the child as playing with a ball). Both the DEF and the ABC interventions were manualized, 10 sessions, and conducted in families’ homes. Thus, the DEF intervention controlled for nonspecific effects of therapy, receiving parent coaching in the home, and monetary compensation for participation. At postintervention visits, two indices of children’s executive functioning capabilities were assessed: (a) parent-reported problems with attention regulation as measured by the attention problems scale of the Child Behavior Checklist (CBCL), and (b) cognitive flexibility as assessed by the Dimensional Change Card Sort (DCCS) task. Children’s attention regulation and cognitive flexibility are thought to reflect related but also largely distinct aspects of executive functioning (Miyake, 2000; Zelazo & Frye, 1998). These two measures were collected with three groups of children: (a) foster children who were randomly assigned to receive the ABC-T intervention, (b) foster children who were randomly assigned to receive the control intervention (DEF), and (c) children who had never been placed in foster care and were raised by their birth parents in low-risk environments. Based on prior research (Lewis, Dozier, Ackerman, & Sepulveda-Kozakowski, 2007; Pears, Fisher, Bruce, Kim, & Yoerger, 2010), we expected that foster children were at greater risk for deficits in executive functioning compared to the low-risk children. By enhancing parental nurturance, following the lead, and coregulation, ABC-T addressed key processes expected to enhance children’s developing regulatory capabilities. Thus, we expected that foster children whose parents received ABC-T would show improved executive functioning, compared with foster children in the control intervention.
Method
Participants
Participants were 173 parent–toddler dyads in three groups: (a) foster families randomly assigned to receive ABC-T (n = 63), (b) foster families randomly assigned to receive DEF (n = 58), and (c) low-risk comparison families that remained intact (n = 52). The foster care sample consisted of 121 foster children and 99 foster parents (20 foster parents had two children enrolled in the study, two foster parents had three children enrolled in the study, and one foster parent had four children enrolled in the study). To address the non-independence, all analyses were also completed including each parent only once. All results were the same as with the full sample. Families’ participation in any research activities was voluntary. Only one family participated in parent training but declined to participate in research visits.
The low-risk comparison group consisted of 52 children who had never been placed in foster care and were raised by their birth parents. These children were recruited from a university-based childcare center and local preschools. Parents and children in the comparison sample did not receive intervention services.
No significant differences were found between the two intervention groups (ABC-T and DEF) with respect to foster children’s previous placements (see Table 1) or demographic variables (see Table 2). There were some differences in demographic variables between the foster care groups and the low-risk comparison group. There were more African American children, χ2 (4, n = 173) = 22.27, p < .01, and more African American parents, χ2 (4, n = 151) = 19.69, p < .01, in the foster care groups than in the low-risk comparison group. In addition, foster parents were significantly older than parents in the low-risk comparison group, t (148) = −2.93, p < .01. There were no significant differences between the foster families and low-risk comparison group in children’s age, children’s gender, or parents’ gender.
Table 1.
Descriptive statistics for foster children’s caregiving histories
| Variable | DEF Intervention (n = 58) | ABC-T Intervention (n = 63) |
|---|---|---|
| Placement type, number (%) | ||
| Nonrelative | 46 (79.3) | 52 (82.5) |
| Relative | 12 (20.7) | 11 (17.5) |
| Number of placements | ||
| Mean (SD) | 2.2 (0.9) | 2.3 (0.7) |
| Range | 1–6 | 1–4 |
| Age first removed from birth parents (months) | ||
| Mean (SD) | 12.4 (13.5) | 12.5 (13.3) |
| Range | 0–53.0 | 0–47.2 |
| Time with caregiver at postassessment (months) | ||
| Mean (SD) | 28.8 (15.9) | 28.3 (14.2) |
| Range | 4.8–62.6 | 6.4–55.3 |
| Reason for removal (not mutually exclusive), number (%) | ||
| Physical or sexual abuse | 15 (25.9) | 10 (15.9) |
| Neglect | 24 (41.4) | 36 (57.1) |
| Caregiver incarceration | 0 (0.0) | 12 (19.0) |
| Caregiver substance abuse | 21 (36.2) | 28 (44.4) |
| Dependency (i.e., inability to care for child) | 34 (58.6) | 32 (50.8) |
| Caregiver mental health problems | 6 (10.3) | 4 (6.3) |
| Domestic violence | 7 (12.1) | 5 (7.9) |
| Other | 4 (6.9) | 5 (6.3) |
| Missing | 11 (19.0) | 10 (15.9) |
Note: ABC-T, Attachment and Biobehavioral Catch-up for Toddlers; DEF, Developmental Education for Families.
Table 2.
Demographic characteristics for children and parents
| Child Characteristics | DEF Intervention (n = 58) | ABC-T Intervention (n = 63) | Low-Risk Comparison (n = 52) |
|---|---|---|---|
| Gender, number (%) | |||
| Male | 28 (48.3) | 36 (57.1) | 25 (48.1) |
| Female | 30 (51.7) | 27 (42.9) | 27 (51.9) |
| Race/ethnicity, number (%) | |||
| White | 13 (22.4) | 18 (28.6) | 27 (51.9) |
| African American | 34 (58.6) | 34 (54.0) | 11 (21.2) |
| Asian American | 1 (1.7) | 0 (0.0) | 3 (5.8) |
| Hispanic | 3 (5.2) | 5 (7.9) | 6 (11.5) |
| Biracial | 7 (12.1) | 6 (9.5) | 5 (9.6) |
| Age at intervention (months) | |||
| Mean (SD) | 31.8 (8.7) | 29.9 (9.5) | — |
| Range | 14.5–54.7 | 14.0–56.3 | — |
| Age at postintervention (months) | |||
| Mean (SD) | 48.0 (8.8) | 48.6 (9.0) | 45.5 (6.2) |
| Range | 30.6–71.9 | 35.8–74.2 | 35.9–57.0 |
|
| |||
| Parent Characteristics | DEF Intervention (n = 48) | ABC-T Intervention (n = 51) | Low-Risk Comparison (n = 52) |
|
| |||
| Gender, number (%) | |||
| Male | 2 (4.2) | 3 (5.9) | 2 (3.8) |
| Female | 46 (95.8) | 48 (94.1) | 50 (96.2) |
| Race/ethnicity, number (%) | |||
| White | 18 (37.5) | 26 (51.0) | 28 (53.8) |
| African American | 23 (57.9) | 23 (45.1) | 13 (25.0) |
| Asian American | 0 (0.0) | 0 (0.0) | 5 (9.6) |
| Hispanic | 2 (4.2) | 2 (3.9) | 6 (11.5) |
| Biracial | 5 (10.4) | 0 (0.0) | 0 (0.0) |
| Age at intervention (years) | |||
| Mean (SD) | 44.6 (11.3) | 44.8 (9.7) | — |
| Range | 22.0–76.3 | 24.3–67.5 | — |
| Age at postintervention (years) | |||
| Mean (SD) | 45.8 (11.6) | 46.1 (10.0) | 34.4 (4.8) |
| Range | 23.5–76.6 | 24.6–67.9 | 23.4–45.4 |
Note: ABC-T, Attachment and Biobehavioral Catch-up for Toddlers; DEF, Developmental Education for Families.
Procedure
Preintervention and postintervention research assessments
After enrolling in the study, families were randomly assigned to receive either the ABC-T intervention or the control intervention (DEF). Preintervention data were collected during intake visits conducted in the home. The intended schedule for postintervention follow-up assessments included a home visit approximately 1 month after completion of the intervention (1-month postintervention visits were conducted with foster families only because comparison families did not receive intervention services), and yearly postintervention research visits completed at the time of the child’s birthday continuing until age 60 months (i.e., a 36-month visit, a 48-month visit, and a 60-month visit). Data for the present study were collected during the preintervention visit and the first available postintervention visit that included the relevant measures. Approval for the conduct of this research was obtained from the University of Delaware Institutional Review Board.
Interventions
The ABC-T and DEF interventions were similar in structure, frequency, and duration. Both interventions consisted of 10 sessions conducted in the families’ homes and were based on structured manuals.
Experimental intervention: ABC-T
ABC-T was adapted from ABC-I as described above, and focused on three primary targets: (a) increasing parental nurturance in response to child distress, (b) increasing parental following the lead behaviors, and (b) encouraging parents to serve as coregulators for the child when the child became frustrated or upset. These three targets were intended to help children develop their ability to regulate emotion, behavior, physiology, and cognition.
Parent coaches worked to change parenting behaviors through discussion of relevant research, practice of target behaviors during structured activities and throughout sessions, and presentation of videos to illustrate and reinforce target behaviors. A key component of the ABC-T intervention was parent coaches’ provision of “in the moment” feedback about parents’ interactions with their children during the session (Dozier et al., 2014). Parent coaches observed parents’ behavior and made comments about behaviors relevant to intervention targets. For example, if a parent rubbed her child’s back and said “I know you’re mad” when the child became frustrated because he could not go outside, the parent coach might say, “He’s getting angry, and you’re saying, ‘I know you’re mad’; that’s a great example of remaining calm and staying right there with him when he’s upset.” This in vivo feedback was intended to enhance parents’ understanding and consolidation of the target behaviors, as both quantity and quality of comments predicted parent behavior change in ABC-I (Caron, Bernard, & Dozier, 2016). In addition to using the intervention techniques of “in the moment” comments, video feedback, and manualized discussion of research, when appropriate, parent coaches engaged parents in discussion of their own histories of being parented, which were referred to as “voices from the past.” Parents were encouraged to consider how these voices from the past could lead to automatic emotional and behavioral reactions. Parent coaches and parents discussed the importance of “overriding” voices from the past, and instead making intentional decisions about how to respond, based on knowledge of what would best serve the child.
Control intervention: DEF
The DEF intervention was adapted from a home-visiting program developed by Ramey, Yeates, and Short (1984), which was effective in enhancing children’s intellectual functioning when provided intensively and for a long duration (Brooks-Gunn, Klebanov, Liaw, & Spiker, 1993; Ramey et al., 1984). Components that involve parental sensitivity to child cues were excluded in this study in order to distinguish it from ABC-T. Thus, the specific targets of (a) increasing parents’ nurturing behaviors in response to children’s distress, (b) increasing parents’ responsiveness to children’s nondistress signals (i.e., “following the lead”), and (c) encouraging parents to serve as coregulators for their children were unique to ABC-T. Instead, the DEF intervention focused on enhancing children’s motor, cognitive, and language skills directly. Parent coaches discussed methods to help children reach developmental milestones and practiced these skills with the parents and children. Video feedback was also used to review skills and demonstrate children’s gains throughout the intervention. In this way, the DEF intervention served as an active control for nonspecific effects of therapy, receiving parent coaching in the home, and monetary compensation for participation.
Measures
Foster care history
For the foster care group, foster parents provided information regarding the number of placements, placement type (i.e., relative or nonrelative), the child’s age when removed from his or her birth parents, the amount of time the child had been in the current placement, and the reasons for the removal from the birth family. This information was confirmed and supplemented with a review of children’s Division of Family Services records, when available. Any placement with a new caregiver was counted as one placement.
Attention regulation problems
Children’s attention problems were measured with the preschool version of the CBCL (Achenbach & Rescorla, 2000). The CBCL consists of 113 items that describe children’s behavior. Parents rated each behavior on a 3-point scale ranging from 0 (not true) to 2 (very often true) based on the child’s behavior during the prior 2 months. The reliability and validity of the CBCL have been demonstrated in many studies (Bingham, Loukas, Fitzgerald, & Zucker, 2003; Mattison & Spitznagal, 1999). In addition to the postintervention visits, the preschool CBCL was also collected at preintervention as a randomization check. The attention problems scale, which is composed of 5 items that assess difficulty in regulating attention, was used in the current study. These items included having difficulty concentrating or paying attention, having difficulty sitting still, being hyperactive and clumsy, quickly shifting from one activity to another, and wandering away. As recommended in the CBCL manual (Achenbach & Rescorla, 2000), raw scores were used to avoid the issue of a truncated range of variation that is associated with the use of standardized scores. CBCL data were available for 129 children (45 DEF, 45 ABC-T, and 38 low-risk comparison children) at the preintervention assessment and 165 children (53 DEF, 61 ABC-T, and 49 low-risk comparison children) at follow-up assessment. Data were missing due to parents not completing or returning the questionnaires.
Cognitive flexibility
Children’s cognitive flexibility was measured with a graded version of the DCCS task that was developed for preschoolers (Beck, Schaefer, Pang, & Carlson, 2011; Carlson, 2005). The DCCS is a widely used and well-validated measure of executive functioning (Beck et al., 2011). Children’s performance on the DCCS is associated with their performance on other measures of executive functioning, including inhibition and working memory (Zelazo, Carlson, & Kesek, 2008; Zelazo et al., 2003). The DCCS requires children to use rules flexibly to sort cards. Children must attend to a relevant dimension and sort cards based on that dimension (i.e., color). The rule is then switched, and children are required to inhibit their attention to the original dimension that is no longer relevant and attend to the dimension that was ignored in the previous phase (i.e., shape). Thus, task switching on the DCCS requires the formulation and use of a higher order rule for selecting which rules to use (i.e., color or shape) on any particular trial (Zelazo, 2006).
This study used a graded version of the DCCS that consisted of six levels that shared a common core but increased in difficulty (Beck et al., 2011). Children were presented with two boxes with affixed target cards and were asked to sort cards into the boxes based on certain rules. Children began at a specific level based on their age and moved on from one level to the next if they sorted at least five out of the six cards correctly in the preswitch and postswitch phases. Scores consisted of the total number of cards correctly sorted, and could range from 0 to 72.
In the first level, categorization/reverse categorization, children were presented with cards with two categories of dimensions (i.e., big kitty and little kitty) and two boxes, one with a target card with a big kitty affixed to it and the other with a target card with a little kitty. In the preswitch phase of this level, children were asked to categorize the cards by placing them in the corresponding boxes (“Put the big kitties in the big kitty box and the little kitties in the little kitty box”). In the postswitch phase (reverse categorization), children were told to play a “silly” game and reverse the sorting rule that was used in categorization (“Put the big kitties in the little kitty box and the little kitties in the big kitty box”).
In the separated level, one target card was red with a black silhouette of a truck and the other was blue with a black silhouette of a star. The sorting cards were blue cards with a truck silhouette and red cards with a star silhouette. Children were first asked to sort six cards based on one dimension (shape; preswitch) and then switch and sort six cards according to the other dimension (color; postswitch). The integrated level followed the same procedure, but there was a higher degree of perceptual conflict in the stimuli images on the cards. Instead of the dimensions being visually separate, the integrated stimuli images contained both dimensions (shape and color). The target cards had a red truck and a blue star on white backgrounds. The sorting cards were blue trucks and red stars. Children were asked to sort six cards based on shape (preswitch) and then switch and sort six cards according to color (postswitch).
The fourth level, mixed, used the same target and sorting cards as the integrated level. In the mixed level, children were required to sort 12 cards using alternating rules. They were instructed to sort by shape if the experimenter told them to play the “shape game,” and to sort by color if the experimenter told them to play the “color game.” In the fifth level, advanced, some of the sorting cards had a black border around the card and some did not. Children were instructed to play the “color game” (sorting by color) if the card had a black border around it, and play the “shape game” (sorting by shape) if the card did not have a black border. The final level, reverse advanced, used the same procedure except that children were told to play the “shape game” if the card had a black border around it and play the “color game” if the card did not have a black border.
The DCCS was administered at postintervention visits when children were, on average, 47.6 months old (SD= 8.8). Test administrators were unaware of intervention status. Valid postintervention DCCS assessments were available for 147 children (43 DEF, 48 ABC-T, and 52 low-risk comparison children). It was not possible to administer the DCCS at the preintervention visits because children were too young to complete the measure at that time.
Results
Preliminary analyses
Children’s attention regulation problems were not associated significantly with their age at the time of the assessment (preintervention: r = .10, p = .27; postintervention: r = .13, p = .10) or gender (coded as male = 1, female = 0); preintervention: t (127) = −1.03, p = .31, d = −0.18, postintervention: t (163) =−1.00, p=.32, d=−0.16. Thus, these variables were not included as covariates in analyses of attention regulation. Children’s DCCS scores were associated with children’s age at the time of the DCCS (r = .51, p < .01), and females had significantly higher DCCS scores than males, t (145) = 2.49, p < .05, d = 0.41. Therefore, child gender and age were included as covariates in analyses involving DCCS.
Controlling for child age and gender, there was a modest but statistically significant negative correlation between the postintervention measures of attention problems and cognitive flexibility (rpartial = −.26, p < .01). This indicates that these measures capture related but largely distinct aspects of executive functioning.
Children’s attention problems at preintervention were examined to evaluate whether foster children randomly assigned to the two intervention conditions differed from one another prior to the intervention. As shown in Figure 1, there were no significant differences in parent-reported attention problems between children in the ABC-T (M = 3.07, SD = 2.31), DEF (M = 2.98, SD = 2.33), or low-risk comparison (M = 2.89, SD = 2.04) groups at the time of the preintervention visits, F (1, 126) = 0.08, p = .94, η2 < 0.01.
Figure 1.
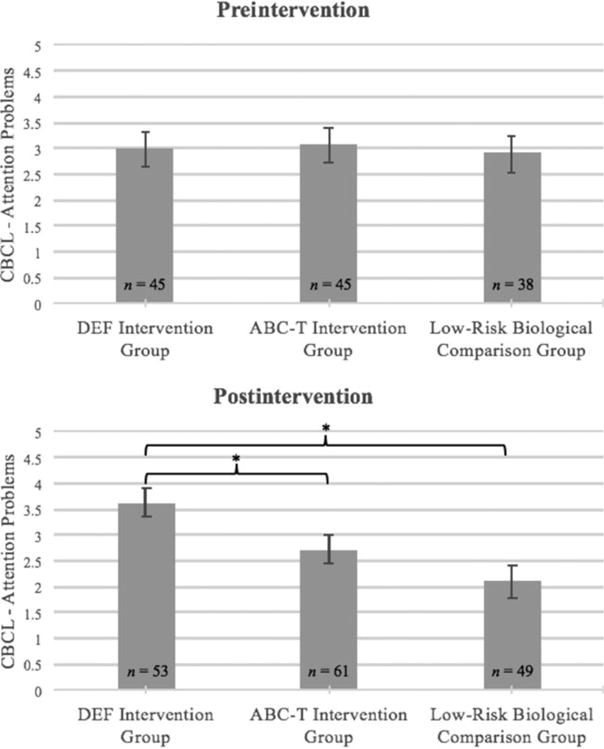
Parents’ reports of children’s attention problem at the pre- and postintervention assessments. ABC-T, Attachment and Biobehavioral Catch-up for Toddlers; DEF, Developmental Education for Families; CBCL, Child Behavior Checklist. *p < .05.
Main analysis
Group differences in attention problems
Analyses of variance were performed, with group (ABC-T, DEF, and low-risk comparison) as the independent variable, and parent-reported attention problems at the time of the postintervention assessment as the dependent variable. As illustrated in Figure 1, there was a main effect for group, F (1, 162) = 7.00, p < .01, η2 = 0.08. Follow-up tests indicated that children in the ABC-T group (M = 2.73, SD = 2.11), F (1, 114) = 5.26, p =.02, d = 0.42, and in the low-risk comparison group (M = 2.10, SD = 2.02), F (1, 101) = 13.85, p < .01, d = 0.75, had significantly lower attention problems scores than children in the DEF group (M = 3.63, SD = 2.13). There were no significant differences in attention problems between the ABC-T and low-risk comparison groups at postintervention, F (1, 109) = 2.49, p = .12, d = 0.32.
Group differences in cognitive flexibility
Analyses of covariance were performed, with group as the independent variable, DCCS score as the dependent variable, and child gender and age as covariates. As shown in Figure 2, there was a main effect for group, F (1, 142) = 6.15, p < .01, η2 = 0.06. Children whose parents received the ABC-T intervention performed significantly better on the DCCS (M = 23.67, SD = 13.06) than the children whose parents received the DEF intervention (M = 18.54, SD = 12.88), F (1, 91) = 4.14, p = .04, d = 0.40, but not significantly differently from the low-risk comparison group (M = 28.26, SD = 13.00), F (1, 98) = 2.92, p = .09, d = 0.36. Children whose parents received the DEF intervention performed more poorly than children in the low-risk comparison group, F (1, 93) = 12.12, p < .01, d = 0.76.
Figure 2.
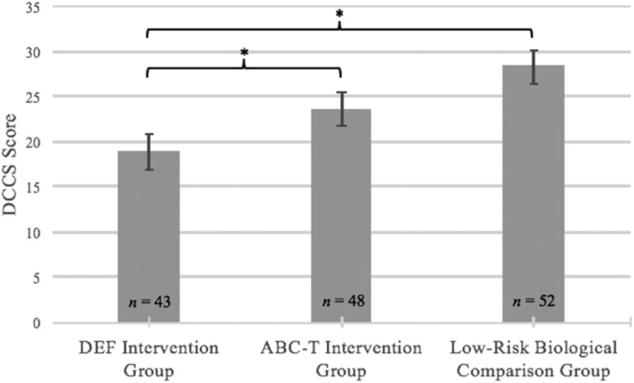
Children’s cognitive flexibility as measured by performance on the Dimensional Change Card Sort Task (DCCS). ABC-T, Attachment and Biobehavioral Catch-up for Toddlers; DEF, Developmental Education for Families. *p < .05.
Discussion
These findings indicate that ABC-T enhances executive functioning skills among toddlers in foster care. Foster children whose parents received the ABC-T intervention demonstrated fewer attention problems and greater cognitive flexibility than children whose foster parents received a control intervention of identical intensity, duration, and in-home method of delivery. Moreover, foster children in the ABC-T group did not differ significantly from the low-risk comparison group with respect to attention problems or cognitive flexibility at the postintervention assessment. These results extend prior findings regarding the effectiveness of the ABC-I intervention (e.g., Lewis-Morrarty et al., 2012) by demonstrating that an attachment-based intervention designed for toddlers enhanced foster children’s executive functioning capabilities. In addition to increasing parents’ nurturing behaviors and responsiveness to children’s signals, the ABC-T intervention also addresses the developmental issues encountered during toddlerhood. Specifically, the ABC-T intervention helps parents remain psychologically and physically available when children are emotionally overwhelmed, thereby helping them serve as effective coregulators. This was central to the intervention because toddlers are beginning to transition from complete reliance on their parents for external regulation to developing their own independent regulatory capabilities (Kopp, 2011). The findings from this study suggest targeting these parenting behaviors helps children to develop enhanced control of their cognitive processes.
The efficacy of the ABC-T intervention for improving foster children’s executive functioning capabilities was rigorously evaluated in this study using a randomized clinical trial. Because the intervention was conducted when the children were toddlers, it was not possible to collect a valid assessment of children’s cognitive flexibility prior to random assignment to the interventions. Nonetheless, parent-reported attention problems did not differentiate children in the two randomized groups at preintervention. In addition, children in the two intervention conditions did not differ from one another with respect to a number of demographic characteristics or the foster children’s caregiving histories. Thus, randomization appears to have been successful, providing confidence that the observed postintervention differences reflect the positive effects of the ABC-T intervention.
These findings also advance our basic understanding of the significance of early attachment experiences in children’s development of executive functioning capabilities. Prior research in this area largely has relied on correlational research designs (e.g., Bernier et al., 2010; Bindman et al., 2015; Sulik et al., 2015), which do not allow for strong causal interpretations. The current study extends this body of research and helps strengthen causal claims by providing evidence that experimental manipulation of parents’ nurturing, responsive, and coregulating caregiving behavior leads to improvements in children’s cognitive self-regulation abilities.
The findings in this study are strengthened by multimethod assessment of children’s executive functioning abilities through the DCCS task and the CBCL. Results were consistent across the two measures, even though they represent different methodologies and target different executive functioning abilities. These data suggest that ABC-T is effective at enhancing multiple aspects of executive functioning. Future research is needed to evaluate the degree to which ABC-T helps promote other aspects of executive functioning, such as inhibitory control or working memory. In addition, additional research is needed to investigate whether the effects of ABC-T are specific to children’s executive functioning abilities or whether ABC-T helps children to develop more adaptive self-regulation across a range of domains (i.e., cognitive, behavioral, emotional, and physiological).
In conclusion, the current study provides novel evidence that an attachment-based intervention designed for toddlers with histories of adversity resulted in improvements in children’s executive functioning capabilities. Because the current study implemented the ABC-T intervention only with foster parents and children, future studies should evaluate the robustness of ABC-T’s effects on children’s executive functioning across different populations of children who have experienced early adversity. However, we have found that the infancy intervention is effective across populations of vulnerable infants and their parents (e.g., Bernard et al., 2012; Lewis-Morrarty et al., 2012), and we anticipate the toddler intervention to show similar effects. In addition, nearly all of the primary caregivers of the foster children in this study were females. The efficacy of the ABC-T intervention with paternal caregivers remains an open question. We expect that characteristics related to risk status (e.g., drug use, homelessness) will be more likely to moderate the effectiveness of the intervention than the parents’ gender (e.g., Bick, Dozier, & Moore, 2012). It will also be critical to conduct effectiveness trials of ABC-T in which the intervention is administered by community clinicians (e.g., Caron, Weston-Lee, Haggerty, & Dozier, 2016). Finally, it will be important to test whether the observed improvements in executive functioning during toddlerhood are linked to other future outcomes, such as enhancements in academic achievement or reductions in behavior problems.
Acknowledgments
The project described was supported by National Institutes of Mental Health Grants R01MH052135 and R01MH074374 (to M.D.). The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institute of Mental Health. We thank the children and families who participated in the research and gratefully acknowledge the support of child protection agencies in Delaware.
References
- Achenbach TM, Rescorla LA. Manual for the ASEBA preschool forms and profiles. Burlington, VT: University of Vermont, Department of Psychiatry; 2000. [Google Scholar]
- Allan NP, Hume LE, Allan DM, Farrington AL, Lonigan CJ. Relations between inhibitory control and the development of academic skills in preschool and kindergarten: A meta-analysis. Developmental Psychology. 2014;50:2368–23679. doi: 10.1037/a0037493. [DOI] [PubMed] [Google Scholar]
- Asok A, Bernard K, Roth TL, Rosen JB, Dozier M. Parental responsiveness moderates the association between early-life stress and reduced telomere length. Development and Psychopathology. 2013;25:577–585. doi: 10.1017/S0954579413000011. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Barkley RA. Defiant children: A clinician’s manual for assessment and parent training. 3rd. New York: Guilford Press; 2013. [Google Scholar]
- Beck DM, Schaefer C, Pang K, Carlson SM. Executive function in preschool children: Test–retest reliability. Journal of Cognition and Development. 2011;12:169–193. doi: 10.1080/15248372.2011.563485. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Belsky J, Fearon RMP. Early attachment security, subsequent maternal sensitivity, and later child development: Does continuity in development depend upon continuity of caregiving? Attachment & Human Development. 2002;4:361–387. doi: 10.1080/1461673021016726. [DOI] [PubMed] [Google Scholar]
- Bernard K, Butzin-Dozier Z, Rittenhouse J, Dozier M. Cortisol production patterns in young children living with birth parents vs children placed in foster care following involvement of Child Protective Services. Archives of Pediatrics and Adolescent Medicine. 2010;164:438–443. doi: 10.1001/archpediatrics.2010.54. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bernard K, Dozier M, Bick J, Gordon MK. Intervening to enhance cortisol regulation among children at risk for neglect: Results of a randomized clinical trial. Development and Psychopathology. 2015;27:829–841. doi: 10.1017/S095457941400073X. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bernard K, Dozier M, Bick J, Lewis-Morrarty E, Lindhiem O, Carlson EA. Enhancing attachment organization among maltreated children: Results of a randomized clinical trial. Child Development. 2012;83:623–636. doi: 10.1111/j.1467-8624.2011.01712.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bernedo IM, Salas MD, Fuentes MJ, García-Martín MÁ. Foster children’s behavior problems and impulsivity in the family and school context. Children and Youth Services Review. 2014;42:43–49. doi: 10.1016/j.childyouth.2014.03.022. [DOI] [Google Scholar]
- Bernier A, Beauchamp MH, Carlson SM, Lalonde G. A secure base from which to regulate: Attachment security in toddlerhood as a predictor of executive functioning at school entry. Developmental Psychology. 2015;51:1177–1189. doi: 10.1037/dev0000032. [DOI] [PubMed] [Google Scholar]
- Bernier A, Carlson SM, Whipple N. From external regulation to self-regulation: Early parenting precursors of young children’s executive functioning. Child Development. 2010;81:326–339. doi: 10.1111/j.1467-8624.2009.01397.x. [DOI] [PubMed] [Google Scholar]
- Bick J, Dozier M. The effectiveness of an attachment-based intervention in promoting foster mothers’ sensitivity toward foster infants. Infant Mental Health Journal. 2013;34:95–103. doi: 10.1002/imhj.21373. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bick J, Dozier M, Moore S. Predictors of treatment use among foster mothers in an attachment-based intervention program. Attachment & Human Development. 2012;14:439–452. doi: 10.1080/14616734.2012.706391. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bindman SW, Pomerantz EM, Roisman GI. Do children’s executive functions account for associations between early autonomy-supportive parenting and achievement through high school? Journal of Educational Psychology. 2015;107:756–770. doi: 10.1037/edu0000017. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bingham CR, Loukas A, Fitzgerald HE, Zucker RA. Parental ratings of son’s behavior problems in high-risk families: Convergent validity, internal structure, and interparent agreement. Journal of Personality Assessment. 2003;80:237–251. doi: 10.1207/S15327752JPA8003_03. [DOI] [PubMed] [Google Scholar]
- Blair CB. The development of executive functions and self-regulation: A bidirectional psychobiological model. In: Vohs KD, Baumeister RF, editors. Handbook of self-regulation: Research, theory, and applications. 3rd. New York: Guilford Press; 2016. pp. 417–439. [Google Scholar]
- Brooks-Gunn J, Klebanov PK, Liaw FR, Spiker D. Enhancing the development of low-birthweight, premature infants: Changes in cognition and behavior over the first three years. Child Development. 1993;64:736–753. doi: 10.1111/j.1467-8624.1993.tb02940.x. [DOI] [PubMed] [Google Scholar]
- Bruce J, Fisher PA, Pears KC, Levine S. Morning cortisol levels in preschool-aged foster children: Differential effects of maltreatment type. Developmental Psychobiology. 2009;51:14–23. doi: 10.1002/dev.20333. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Carlson SM. Developmentally sensitive measures of executive function in preschool children. Developmental Neuropsychology. 2005;28:595–616. doi: 10.1207/s15326942dn2802_3. [DOI] [PubMed] [Google Scholar]
- Carlson SM, Mandell DJ, Williams L. Executive function and theory of mind: Stability and prediction from ages 2 to 3. Developmental Psychology. 2004;40:1105–1122. doi: 10.1037/0012-1649.40.6.1105. [DOI] [PubMed] [Google Scholar]
- Caron EB, Bernard K, Dozier M. In vivo feedback predicts parent behavior change in the Attachment and Biobehavioral Catch-up intervention. Journal of Clinical Child & Adolescent Psychology. 2016 doi: 10.1080/15374416.2016.1141359. Advance online publication. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Caron EB, Weston-Lee P, Haggerty D, Dozier M. Community implementation outcomes of Attachment and Biobehavioral Catchup. Child Abuse & Neglect. 2016;53:128–137. doi: 10.1016/j.chiabu.2015.11.010. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cassidy J. Emotion regulation: Influences of attachment relationships. Monographs of the Society for Research in Child Development. 1994;59(2–3):228–249. doi: 10.1111/j.1540-5834.1994.tb01287.x. Serial No. 240. [DOI] [PubMed] [Google Scholar]
- Clausen JM, Landsverk J, Ganger W, Chadwick D, Litrownik A. Mental health problems of children in foster care. Journal of Child and Family Studies. 1998;7:283–296. doi: 10.1023/A:1022989411119. [DOI] [Google Scholar]
- Cole PM, Tan PZ, Hall SE, Zhang Y, Crnic KA, Blair CB, Li R. Developmental changes in anger expression and attention focus: Learning to wait. Developmental Psychology. 2011;47:1078–1089. doi: 10.1037/a0023813. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Conway A, McDonough SC, Mackenzie M, Miller A, Dayton C, Rosenblum K, Sameroff A. Maternal sensitivity and latency to positive emotion following challenge: Pathways through effortful control. Infant Mental Health Journal. 2014;35:274–284. doi: 10.1002/imhj.21445. [DOI] [PubMed] [Google Scholar]
- Conway A, Stifter CA. Longitudinal antecedents of executive function in preschoolers. Child Development. 2012;83:1022–1036. doi: 10.1111/j.1467-8624.2012.01756.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Diamond A. Executive functions. Annual Review of Psychology. 2013;64:135–168. doi: 10.1146/annurev-psych-113011-143750. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Diener ML, Mangelsdorf SC. Behavioral strategies for emotion regulation in toddlers: Associations with maternal involvement and emotional expressions. Infant Behavior and Development. 1999;22:569–583. doi: 10.1016/S0163-6383(00)00012-6. [DOI] [Google Scholar]
- Dozier M, Bick J. Changing caregivers: Coping with early adversity. Pediatric Annals. 2007;36:205–208. doi: 10.3928/0090-4481-20070401-09. [DOI] [PubMed] [Google Scholar]
- Dozier M, Higley E, Albus KE, Nutter A. Intervening with foster infants’ caregivers: Targeting three critical needs. Infant Mental Health Journal. 2002;23:541–554. doi: 10.1002/imhj.10032. [DOI] [Google Scholar]
- Dozier M, Lindhiem O. This is my child: Differences among foster parents in commitment to their young children. Child Maltreatment. 2006;11:338–345. doi: 10.1177/1077559506291263. [DOI] [PubMed] [Google Scholar]
- Dozier M, Lindhiem O, Lewis E, Bick J, Bernard K, Peloso E. Effects of a foster parent training program on young children’s attachment behaviors: Preliminary evidence from a randomized clinical trial. Child and Adolescent Social Work Journal. 2009;26:321–332. doi: 10.1007/s10560-009-0165-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Dozier M, Meade E, Bernard K. Attachment and Biobehavioral Catch-up: An intervention for parents at risk of maltreating their infants and toddlers. In: Timmer S, Urquiza A, editors. Advances in child abuse prevention knowledge. Vol. 3. New York: Springer; 2014. pp. 43–59. [Google Scholar]
- Eisenberg N, Cumberland AJ, Spinrad TL. Parental socialization of emotion. Psychological Inquiry. 1998;9:241–273. doi: 10.1207/s15327965pli0904_1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Fabes RA, Leonard SA, Kupanoff K, Martin CL. Parental coping with children’s negative emotions: Relations with children’s emotional and social responding. Child Development. 2001;72:907–920. doi: 10.1111/1467-8624.00323. [DOI] [PubMed] [Google Scholar]
- Fisher PA, Gunnar MR, Dozier M, Bruce J, Pears KC. Effects of therapeutic interventions for foster children on behavioral problems, caregiver attachment, and stress regulatory neural systems. Annals of the New York Academy of Sciences. 2006;1094:215–225. doi: 10.1196/annals.1376.023. [DOI] [PubMed] [Google Scholar]
- Harrist AW, Waugh RM. Dyadic synchrony: Its structure and function in children’s development. Developmental Review. 2002;22:555–592. doi: 10.1016/S0273-2297(02)00500-2. [DOI] [Google Scholar]
- Hofer MA. Developmental psychobiology of early attachment. In: Casey BJ, editor. Developmental psychobiology. Arlington, VA: American Psychiatric Publishing; 2004. pp. 1–28. [Google Scholar]
- Hughes C, Ensor R. Behavioural problems in 2-year-olds: Links with individual differences in theory of mind, executive function and harsh parenting. Journal of Child Psychology and Psychiatry. 2006;47:488–497. doi: 10.1111/j.1469-7610.2005.01519.x. [DOI] [PubMed] [Google Scholar]
- Hughes C, Ensor R. Executive function and theory of mind: Predictive relations from ages 2 to 4. Developmental Psychology. 2007;43:1447–1459. doi: 10.1037/0012-1649.43.6.1447. [DOI] [PubMed] [Google Scholar]
- Hughes C, Ensor R. Individual differences in growth in executive function across the transition to school predict externalizing and internalizing behaviors and self-perceived academic success at 6 years of age. Journal of Experimental Child Psychology. 2011;108:663–676. doi: 10.1016/j.jecp.2010.06.005. [DOI] [PubMed] [Google Scholar]
- Jackson Y, Gabrielli J, Fleming K, Tunno AM, Makanui PK. Untangling the relative contribution of maltreatment severity and frequency to type of behavioral outcome in foster youth. Child Abuse & Neglect. 2014;38:1147–1159. doi: 10.1016/j.chiabu.2014.01.008. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Keller TE, Wetherbee K, Le Prohn NS, Payne V, Sim K, Lamont ER. Competencies and problem behaviors of children in family foster care: Variations by kinship placement status and race. Children and Youth Services Review. 2001;23:915–940. doi: 10.1016/S0190-7409(01)00175-X. [DOI] [Google Scholar]
- Kopp CB. Antecedents of self-regulation: A developmental perspective. Developmental Psychology. 1982;18:199–214. doi: 10.1037/0012-1649.18.2.199. [DOI] [Google Scholar]
- Kopp CB. Commentary: The codevelopments of attention and emotion regulation. Infancy. 2002;3:199–208. doi: 10.1207/S15327078IN0302_5. [DOI] [PubMed] [Google Scholar]
- Kopp CB. Development in the early years: Socialization, motor development, and consciousness. Annual Review of Psychology. 2011;62:165–187. doi: 10.1146/annurev.psych.121208.131625. [DOI] [PubMed] [Google Scholar]
- Laible DJ, Thompson RA, Froimson J. Early socialization: The influence of close relationships. In: Grusec JE, Hastings PD, editors. Handbook of socialization: Theory and research. 2nd. New York: Guilford Press; 2015. pp. 35–59. [Google Scholar]
- Laucht M, Esser G, Schmidt MH. Differential development of infants at risk for psychopathology: The moderating role of early maternal responsivity. Developmental Medicine & Child Neurology. 2001;43:292–300. doi: 10.1111/j.1469-8749.2001.tb00208.x. [DOI] [PubMed] [Google Scholar]
- Lewis EE, Dozier M, Ackerman JP, Sepulveda-Kozakowski S. The effect of placement instability on adopted children’s inhibitory control abilities and oppositional behavior. Developmental Psychology. 2007;43:1415–1427. doi: 10.1037/0012-1649.43.6.1415. [DOI] [PubMed] [Google Scholar]
- Lewis-Morrarty E, Dozier M, Bernard K, Terracciano SM, Moore SV. Cognitive flexibility and theory of mind outcomes among foster children: Preschool follow-up results of a randomized clinical trial. Journal of Adolescent Health. 2012;51:S17–S22. doi: 10.1016/j.jadohealth.2012.05.005. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lind T, Bernard K, Ross E, Dozier M. Intervention effects on negative affect of CPS-referred children: Results of a randomized clinical trial. Child Abuse & Neglect. 2014;38:1459–1467. doi: 10.1016/j.chiabu.2014.04.004. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Low JA, Webster L. Attention and executive functions as mediators of attachment and behavior problems. Social Development. 2015 doi: 10.1111/sode.12166. Advance online publication. [DOI] [Google Scholar]
- Mattison RE, Spitznagal EL. Long-term stability of Child Behavior Checklist profile types in a child psychiatric clinic population. Journal of the American Academy of Child & Adolescent Psychiatry. 1999;38:700–707. doi: 10.1097/00004583-199906000-00017. [DOI] [PubMed] [Google Scholar]
- McNeil CB, Hembree-Kligin TL. Parent-child interaction therapy. 2nd. New York: Springer; 2010. [Google Scholar]
- Miyake A. The unity and diversity of executive functions and their contributions to complex “frontal lobe” tasks: A latent variable analysis. Cognitive Psychology. 2000;41:49–100. doi: 10.1006/cogp.1999.0734. [DOI] [PubMed] [Google Scholar]
- Moilanen KL, Shaw DS, Dishion TJ, Gardner F, Wilson M. Predictors of longitudinal growth in inhibitory control in early childhood. Social Development. 2010;19:326–347. doi: 10.1111/j.1467-9507.2009.00536.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Pears KC, Fisher PA, Bruce J, Kim HK, Yoerger K. Early elementary school adjustment of maltreated children in foster care: The roles of inhibitory control and caregiver involvement. Child Development. 2010;81:1550–1564. doi: 10.1111/j.1467-8624.2010.01491.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Pears KC, Kim HK, Buchanan R, Fisher PA. Adverse consequences of school mobility for children in foster care: A prospective longitudinal study. Child Development. 2015;86:1210–1226. doi: 10.1111/cdev.12374. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Premo JE, Kiel EJ. The effect of toddler emotion regulation on maternal emotion socialization: Moderation by toddler gender. Emotion. 2014;14:782–793. doi: 10.1037/a0036684. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ramey CT, Yeates KO, Short EJ. The plasticity of intellectual development: Insights from preventative intervention. Child Development. 1984;55:1913–1925. doi: 10.2307/1129938. [DOI] [PubMed] [Google Scholar]
- Raver CC. Relations between social contingency in mother-child interaction and 2-year-olds’ social competence. Developmental Psychology. 1996;32:850–859. doi: 10.1037/0012-1649.32.5.850. [DOI] [Google Scholar]
- Sanchirico A, Jablonka K. Keeping foster children connected to their biological parents: The impact of foster parent training and support. Child and Adolescent Social Work Journal. 2000;17:185–203. doi: 10.1023/A:1007583813448. [DOI] [Google Scholar]
- Semrud-Clikeman M, Walkowiak J, Wilkinson A, Butcher B. Executive functioning in children with Asperger syndrome, ADHD-combined type, ADHD-predominately inattentive type, and controls. Journal of Autism and Developmental Disorders. 2010;40:1017–1027. doi: 10.1007/s10803-010-0951-9. [DOI] [PubMed] [Google Scholar]
- Serbin LA, Hubert M, Hastings PD, Stack DM, Schwartzman AE. The influence of parenting on early childhood health and health care utilization. Journal of Pediatric Psychology. 2014;39:1161–1174. doi: 10.1093/jpepsy/jsu050. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Shaw DS, Bell RQ, Gilliom M. A truly early starter model of antisocial behavior revisited. Clinical Child and Family Psychology Review. 2000;3:155–172. doi: 10.1023/A:1009599208790. [DOI] [PubMed] [Google Scholar]
- Silk JS, Shaw DS, Prout JT, O’Rourke F, Lane TJ, Kovacs M. Socialization of emotion and offspring internalizing symptoms in mothers with childhood-onset depression. Journal of Applied Developmental Psychology. 2011;32:127–136. doi: 10.1016/j.appdev.2011.02.001. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Sroufe LA. The coherence of individual development: Early care, attachment, and subsequent developmental issues. American Psychologist. 1979;34:834–841. doi: 10.1037/0003-066X.34.10.834. [DOI] [Google Scholar]
- Sroufe LA. Emotional development. New York: Cambridge University Press; 1996. [Google Scholar]
- Sroufe LA. Attachment and development: A prospective, longitudinal study from birth to adulthood. Attachment & Human Development. 2005;7:349–367. doi: 10.1080/14616730500365928. [DOI] [PubMed] [Google Scholar]
- Sulik MJ, Blair CB, Mills-Koonce R, Berry DJ, Greenberg LA. Attachment and development: A prospective, longitudinal study from birth to adulthood. Attachment & Human Development. 2005;7:349–367. doi: 10.1080/14616730500365928. [DOI] [PubMed] [Google Scholar]
- Tarren-Sweeney M. Retrospective and concurrent predictors of the mental health of children in care. Children and Youth Services Review. 2008;30:1–25. doi: 10.1016/j.childyouth.2007.05.014. [DOI] [Google Scholar]
- US Department of Health and Human Services. Child welfare outcomes 2010–2013: Report to Congress. 2015 Retrieved from http://www.acf.hhs.gov/sites/default/files/cb/cwo10_13.pdf.
- Zelazo PD. The Dimensional Change Card Sort (DCCS): A method of assessing executive function in children. Nature Protocols. 2006;1:297–301. doi: 10.1038/nprot.2006.46. [DOI] [PubMed] [Google Scholar]
- Zelazo PD, Carlson SM, Kesek A. Development of executive function in childhood. In: Nelson CA, Luciana M, editors. Handbook of developmental cognitive neuroscience. Cambridge, MA: MIT Press; 2008. [Google Scholar]
- Zelazo PD, Frye D. Cognitive complexity and control: II. The development of executive function in childhood. Current Directions in Psychological Science. 1998;7:121–126. [Google Scholar]
- Zelazo PD, Müller U, Frye D, Marcovitch S, Argitis G, Boseovski JJ, Sutherland A. The development of executive function in early childhood. Monographs of the Society for Research in Child Development. 2003;68(3):vii–151. doi: 10.1111/j.0037-976x.2003.00260.x. Serial No. 274. [DOI] [PubMed] [Google Scholar]