

Abstract
BACKGROUND:
Caregiver burden threatens the psychological, emotional, functional and even physical health of caregivers. The aims of this study were to determine caregiver burden and family distress and the relationship between them, also to explore predictors of caregiver burden in a sample of Iranian family caregivers of cancer patients.
MATERIALS AND METHODS:
This is a cross-sectional study with correlational design. A total of 104 family caregivers of cancer patients were asked to respond to the Caregiver Burden Inventory (CBI) and the Family Distress Index (FDI) together with a sociodemographic questionnaire. For evaluating the relationship between CBI and FDI scores, the Pearson's product-moment correlation was used. In addition, multiple linear regression analysis was applied to explore the predictive factors of caregiver burden.
RESULTS:
A high burden was experienced by almost half of the caregivers (48.1%). The FDI mean score was 9.76 ± 5.40 ranged from 0 to 24. A strong positive correlation was found between the caregiver burden and family distress (r = 0.76). Multiple linear regression results showed the predictive role of FDI score (β = 0.71, P = 0.001), patient's gender (β = −0.25, P = 0.001), and early cancer diagnosis (β =0.13, P = 0.027) in caregiver burden. They could explain 65% of variance in the level of burden in family caregivers.
CONCLUSION:
Family nurses should consider the caregivers burden and vulnerability of families with cancer patient, especially if the patient is a male or has a new diagnosis. They should also design special programs for the whole family as a system that family can adapt to the new situation.
Keywords: Cancer patient, caregiver burden, family distress, family nurse
Introduction
Cancer as a chronic disease is associated with considerable, continuing, and fluctuating problems and special needs of patients.[1,2] Medical advances in treatment and current attitudes toward outpatient cancer treatment enable care to be performed in the patient's home setting, and family members are engaged to undertake the important roles as caregivers.[3,4] Family caregivers need preparation to face the demands of their new roles and responsibilities, including physical care as well as psychological, spiritual, and social support.[5] Family caregivers are expected to provide complex and multidimensional care in the home with little preparation or support. When the demands of the caregiving roles exceed the caregivers limited resources, they feel overwhelmed and report high stress, leading to more caregiver burden.[6]
Caregiver burden is defined as a strain or load of distressful consequences associated with caring for a chronically ill family member.[7] Caregiver burden threatens the psychological, emotional, functional, and even physical health of caregivers.[3] When a family member receives a cancer diagnosis, the entire family system is faced with the new situation and for reaching a revised balance to decrease caregiver burden the family needs adaptation.[8]
Family adaptability describes families’ ability to modify family dynamics such as roles and responsibilities as needed and to show flexibility.[9] Family maladaptation can cause family distress,[10] in the other hand, if the flexibility of a family and its adaptive function is impaired, the family is unable to respond to a wide variety of needs such as caregiver burden.[8]
According to our investigations, the relationship between caregiver burden and family distress in Iranian cancer patients’ families remains unclear. However, the aims of this study were (1) to determine caregiver burden and family distress and the relationship between them, and (2) to explore predictors (Family Distress Index [FDI] and sociodemographic factors) of caregiver burden in a sample of Iranian family caregivers of cancer patients.
Materials and Methods
Design, sample, and data collection
This is a cross-sectional study with correlational design, which was carried out in family caregivers of cancer patient referred to the outpatient chemotherapy wards of five university hospitals in Tehran (January–April 2016). This study has been approved by the Ethics Committee of Shahid Beheshti University of Medical Sciences. All the caregivers were informed about the purposes of this study and their right to consent or refuse to participate in the study. They also signed informed consent forms. The purposive sampling was used in this study. Purposive sampling involves the conscious selection by the researcher of certain subjects or elements to include in the study.[11] Hence, according to inclusion criteria, 120 caregivers of all patients referred to outpatient chemotherapy ward nonrandomly, were recruited for this study. Of these, 16 caregivers did not complete the questionnaires entirely (answered <80% of the questions), so they were excluded from the study. Thus, a total of 104 family caregivers of cancer patients were included in this study.
The inclusion criteria for recruiting of the family caregivers were as follows: Providing unpaid care by a family member of a cancer patient in the family, a family caregiver as the main caregiver was confirmed by the patient, the patient received adjuvant chemotherapy following an operation at the outpatient chemotherapy ward. For having more unify samples, the patients with recurrent cancer diagnosis were eliminated from the study.
Measurements
Caregiver Burden Inventory
The Caregiver Burden Inventory (CBI) is a self-reporting instrument, widely used in the studies of the caregiver burden of chronically ill patients, including cancer. This questionnaire consists of 24 items Likert-format scale for which the responses are scored on a five-point (0–4).[12] This instrument measures five dimensions of burden. These dimensions include developmental (describe the caregivers’ feeling of being left behind, incapable to enjoy the same expectations and opportunities with respect to their peers), time dependence (the burden on caregiver due to restriction on the caregivers’ time), physical (feelings of chronic fatigue and physical health problems), social (which describe caregivers’ sense of perceived conflict of roles), and emotional burden (caregivers’ negative feelings toward their patient, which can be induced by the patient's bizarre and unpredictable behavior).[13] All subscales consist of five questions and range from 0 (lowest) to 20 (highest), but the physical subscale consist of four items and ranges from 0 to 16. As Novak and Guest[12] have suggested the physical burden score is better to weight by a factor of 1.25 to make its score range equivalent to the other subscales. The total score ranges from 0 to 96, a score more than 36 shows a risk of “severe burden” and scores near or slightly above 24 indicate a necessity to seek some form of respite care.[13] The internal consistency coefficient of this instrument ranged from 0.92 to 0.94.[14] The Persian version of the CBI has been validated in Iranian society previously with Cronbach's alpha coefficient 0.90.[15] In the present study, Cronbach's alpha coefficient was 0.88.
Family Distress Index
The FDI was used to measure family maladaptation.[9] It is an index with 8-item to obtain family self-report observations about the occurrence of family hardships and challenges that demonstrate family disharmony and family intolerance. The severity of the distress is recorded by the main family caregiver. Thus, scores on the FDI reflect the degree to which families display certain behaviors or patterns of functioning that show the family's continuous condition of disharmony and imbalance. The English version of FDI had good internal consistency with an alpha of 0.87.[10] Permission for Persian translation of the FDI was obtained from Professor Hamilton McCubbin, the developer of the questionnaire. The process of translation and adaptation of the instrument was done by a special guideline.[16] Cronbach's alpha for the Persian version of this instrument in this study was 0.77.
Sociodemographic information and clinical data: A questionnaire that consisted of two parts was used for gathering caregiver and his patient's sociodemographic and clinical data. The first part of the questionnaire asked about the characteristics of family caregivers, including age, gender, educational level, marital status, employment status, sufficient monthly income, having a chronic disease, and relationship with the patient. The second part asked about patients characteristics, including age, gender, cancer type, and time duration since the cancer diagnosis.
Statistical analysis
Data analysis was carried out by SPSS version 18.0 (IBM, Armonk, NY, United States of America). The outcome variables had a normal distribution pattern when they were examined by the Kolmogorov–Smirnov tests. Hence, in this study, parametric statistics was used to analyze the data. The Pearson's product-moment correlation and multiple linear regression analyses were used for evaluating the relationship between the scores of caregiver burden and FDI.
In the initial univariate regression analyses, all sociodemographic and clinical variables with P < 0.05, one by one was entered into a series of backward multiple linear regression analysis (caregivers’ educational level, the caregiver's relationship with the patient and the sufficient family monthly income as well as cancer type, and time since diagnosis). Finally, independent variables (FDI score, in addition to selected sociodemographic variables) were entered into the final backward multiple linear regression analysis to examine their ability to predict family caregiver burden.
Results
Demographic and clinical characteristics
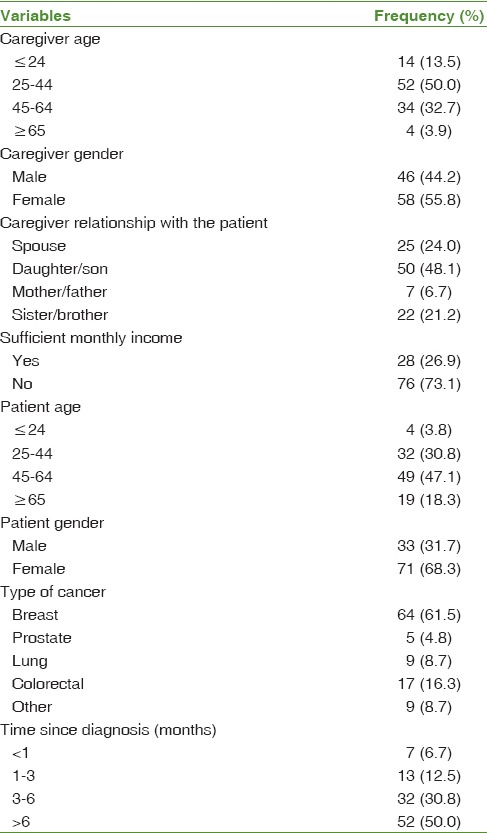
Demographic and clinical characteristics of caregivers and their patient are summarized in Table 1, respectively. The study results showed that 55.8% of the caregivers were women with a range of 18–79 years of age (mean ± standard deviation: 40.29 ± 13.47).
Table 1.
Demographic-clinical characteristics of the family caregivers and patients (n=104)
Caregiver burden in family caregivers of cancer patients
The mean score of burden in family caregivers of cancer patients was 36.92 ± 19 ranging from minimum 2 to maximum 96. A high burden was experienced by almost half (48.1%) of the caregivers (score ≥36 out of 96; n = 50), and 26% of the caregivers had a score between 24 and 35. The subscales of CBI were as follows: Developmental burden (11.64 ± 5.23), time dependence burden (9.49 ± 5.58), physical burden (7.89 ± 5.75), emotional burden (6.02 ± 5.05), and social burden (3.44 ± 3.82), respectively.
For exploring the predictive variables of caregiver burden, all demographic-clinical variables were entered into the univariate regression analysis, after dummy-coding (0, 1 coding) for categorical variables, except for age. In the present study, four variables, including being a spouse, having a male patient, caregiver unsatisfaction of family monthly income, early cancer diagnosis (under 1 month) had a significant effect on caregiver burden (P < 0.05) after running a series of univariate regression analyses.
The relationship between caregiver burden and Family Distress Index
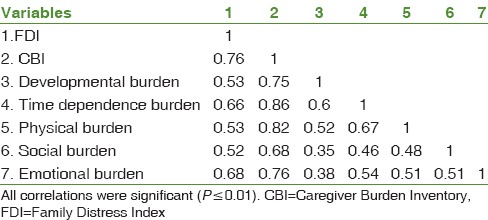
The FDI mean score was 9.76 ± 5 (ranged from 0 to 24). The degree of association between the CBI and FDI scores showed that there was a strong positive correlation between these variables (r = 0.76, P < 0.001). The correlation coefficients of FDI and caregiver burden subscales were shown in Table 2.
Table 2.
Correlation matrix of Caregiver Burden Inventory and Family Distress Index scores in family caregivers of cancer patients (n=104)
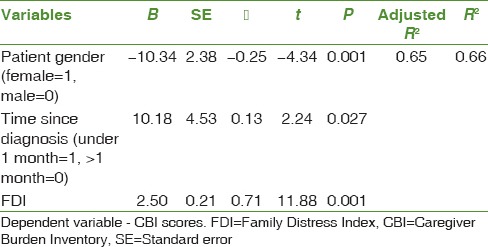
To further explore the contribution of family distress and demographic-clinical characteristics to caregiver burden, the FDI score, patient gender, the type of caregiver relationship with the patients, sufficient monthly family income, time since diagnosis, and cancer type were entered as independent fixed control variables in a backward multiple linear regression analysis [Table 3]. Among these variables, FDI score, patient gender, and time duration since cancer diagnosis were significant predictors of burden in family caregivers of cancer patients. They could explain 65% of variance in caregiver burden. As shown in Table 3, the final model explained 65% of variance in the level of burden in family caregivers. The FDI was the main predictor for caregiver burden (β=0.71, P = 0.001), patient gender (β= −0.25, P = 0.001) and time since cancer diagnosis (β=0.13, P = 0.027) were the other significant predictors.
Table 3.
The results of multiple linear regression analysis in family caregivers of cancer patients (n=104)
Discussion
This study investigated the levels of caregiver burden and family distress and the relationship between them in a sample of Iranian family caregivers of cancer patients. In addition, it explored how family distress and demographic-clinical variables predicted family caregivers burden.
The results of this study showed that almost half of the Iranian family caregivers were at risk of severe burden.[13] Moreover, a group of Iranian family caregivers (26%) showed a need for a short period of rest or relief from caring for the patient. The heaviest burden in the caregivers was developmental burden with a mean of 11.64 ± 5.23. This implies that Iranian family caregivers felt they were divergent with their peers or had feelings of missing life. However, several studies in other provinces of Iran showed higher mean scores for caregiver burden using the same scale on cancer patients’ caregivers. In a study by Salmani et al. was reported a mean of 81.43 ± 21.2, but in another study by Abbasi et al., the mean of burden was 55.30 ± 16.65.[17,18] In both of these studies, the mean time since cancer diagnosis was more than 16 months while in our study, around half of the patients had received the cancer diagnosis 6-month ago. Patients with cancer during the 1st year after the diagnosis may experience few limitations in daily activities.[19] Thus, during the 1st year after cancer diagnosis, there is less demand for caregivers to support their patients to fulfill physical needs, and consequently, these caregivers experience low level of burden.[20]
The level of family distress showed family maladaptation in this study. As expected, the results of our study revealed that there is a strong positive correlation between the levels of caregiver burden and family distress. The final regression model showed that family distress, patient's gender, and time since diagnosis were the predictive variables for burden in Iranian family caregivers with cancer patients. They could explain 65% of variance in the level of burden among family caregivers. Family distress was the strongest predictor of burden in Iranian family caregivers. To the best of our knowledge, very few studies were done to explore this relationship among cancer patients’ families. Since a significant amount of research has been conducted with female cancer survivors,[21] and the main caregiver of the cancer patient, mostly their spouse, not their families as a system. Hence, it seems that these studies neglected other family members that probably have a supportive role for the main caregiver. It can be assumed that the role changes in the family are a consequence of disease. If a family member suffers from a kind of cancer disease, the entire family system is confronted with the new situation and needs to find a balance, which in turn needs readaptation.[8] The way, in which family members adapt to the caregiving role is one of the main factors that influences their perceived burden.[22] The flexibility of a family in obtaining adaptive function is determined by the way the members of the family succeed in changing roles and rules by following external changes. If this flexible function is impaired, the family system is unable to respond to a wide variety of support needs that lead to adaptation. Inflexibility, on the other hand, inhibits the adaptive potential of the main caregiver as a member of the system.[8]
A striking result in this study was related to the patient gender. The caring of a male patient was brought more burden on the caregivers. This finding is consistent with a report regarding to dementia patients that showed higher burden on family caregivers with man patients.[23] The findings with cancer patients indicate contradictory results. In a study, the family caregivers of women patients reported a decreased risk of anxiety,[24] and the caregivers of male patients reported less favorable outcomes.[25] It can be discussed that when the patient is a man, the situation of the family is more vulnerable, because of the traditional role of the man in the family, as a breadwinner and financial support of the family. It seems that the perceived burden of the family caregivers can be influenced by increasing of the stressors, such as financial problems and the lack of sufficient social support in the family.[26] However, there are studies which did not show any significant difference, according to the patient gender.[27] It should be noted that the patient is an important source of both social and financial support of his family.[8] In the Iranian culture, a man has more active roles in the society, in comparison with a woman.[28]
Our findings showed that the family caregivers significantly reported higher burden in <1 month after the cancer diagnosis. A series of studies suggest that caregiver burden can be increased by the length of time as being a caregiver.[17,29] It can be said that a cancer diagnosis is often unpredictable for both the patient and his family caregiver. When the patient confronts physiological, psychological, and economic issues, his family caregiver experiences increased responsibilities and a variety of problems.[30] Thus, this situation can be distressful and needs adaptation. On the other hand, the progression of the illness and the process of treatments require readaptation and flexibility about the roles and responsibilities within the family.[8] It seems that receiving both cancer diagnosis and the process of treatment can be stressful for family members and may be a reason for greater caregiver burden.
It is suggested that family nurses consider the vulnerability of these families and caregiver burden, especially when they have a male patient or a patient with a new diagnosis. They should also design special programs in the whole family as a system that the family can adapt to the new situation.
Conclusion
Almost half of the Iranian family caregivers of cancer patients were at risk of severe burden, and they experienced a high level of burden. There was a strong positive correlation between the levels of caregiver burden and family distress. Moreover, the family distress, patient gender, and time since diagnosis were the predictors of burden in the family caregivers; the family distress was the strongest ones. Thus, the family nurses who are working with cancer patients and their families should assess whole the family as a vulnerable family and arrange special interventional plans when the patient is male or have a new diagnosis.
Financial support and sponsorship
This research was partially funded by the School of Nursing and Midwifery of Shahid Beheshti University of Medical Sciences.
Conflicts of interest
There are no conflicts of interest.
Acknowledgments
The authors are grateful to all participants who participated in this study and completed the questionnaires.
References
- 1.Teunissen SC, Wesker W, Kruitwagen C, de Haes HC, Voest EE, de Graeff A. Symptom prevalence in patients with incurable cancer: A systematic review. J Pain Symptom Manage. 2007;34:94–104. doi: 10.1016/j.jpainsymman.2006.10.015. [DOI] [PubMed] [Google Scholar]
- 2.Walsh D, Rybicki L, Nelson KA, Donnelly S. Symptoms and prognosis in advanced cancer. Support Care Cancer. 2002;10:385–8. doi: 10.1007/s00520-001-0318-z. [DOI] [PubMed] [Google Scholar]
- 3.Rha SY, Park Y, Song SK, Lee CE, Lee J. Caregiving burden and the quality of life of family caregivers of cancer patients: The relationship and correlates. Eur J Oncol Nurs. 2015;19:376–82. doi: 10.1016/j.ejon.2015.01.004. [DOI] [PubMed] [Google Scholar]
- 4.Burge F, Lawson B, Johnston G. Trends in the place of death of cancer patients, 1992-1997. CMAJ. 2003;168:265–70. [PMC free article] [PubMed] [Google Scholar]
- 5.Grant M, Ferrell B. Nursing role implications for family caregiving. Semin Oncol Nurs. 2012;28:279–82. doi: 10.1016/j.soncn.2012.09.011. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Northouse LL, Katapodi MC, Schafenacker AM, Weiss D. The impact of caregiving on the psychological well-being of family caregivers and cancer patients. Semin Oncol Nurs. 2012;28:236–45. doi: 10.1016/j.soncn.2012.09.006. [DOI] [PubMed] [Google Scholar]
- 7.Utne I, Miaskowski C, Paul SM, Rustøen T. Association between hope and burden reported by family caregivers of patients with advanced cancer. Support Care Cancer. 2013;21:2527–35. doi: 10.1007/s00520-013-1824-5. [DOI] [PubMed] [Google Scholar]
- 8.Kotkamp-Mothes N, Slawinsky D, Hindermann S, Strauss B. Coping and psychological well being in families of elderly cancer patients. Crit Rev Oncol Hematol. 2005;55:213–29. doi: 10.1016/j.critrevonc.2005.03.006. [DOI] [PubMed] [Google Scholar]
- 9.Houltberg BJ, Henry CS, Morris AS. Family interactions, exposure to violence, and emotion regulation: Perceptions of children and early adolescents at risk. Fam Relat. 2012;61:283–96. [Google Scholar]
- 10.Corcoran K, Fischer J. Measures for Clinical Practice and Research, Volume 1: Couples, Families, and Children. New York, USA: Oxford University Press; 2013. [Google Scholar]
- 11.Grove SK, Burns N, Gray J. The Practice of Nursing Research: Appraisal, Synthesis, and Generation of Evidence. China: Elsevier Health Sciences; 2012. [Google Scholar]
- 12.Novak M, Guest C. Application of a multidimensional caregiver burden inventory. Gerontologist. 1989;29:798–803. doi: 10.1093/geront/29.6.798. [DOI] [PubMed] [Google Scholar]
- 13.D’Onofrio G, Sancarlo D, Addante F, Ciccone F, Cascavilla L, Paris F, et al. Caregiver burden characterization in patients with Alzheimer's disease or vascular dementia. Int J Geriatr Psychiatry. 2015;30:891–9. doi: 10.1002/gps.4232. [DOI] [PubMed] [Google Scholar]
- 14.McCleery A, Addington J, Addington D. Family assessment in early psychosis. Psychiatry Res. 2007;152:95–102. doi: 10.1016/j.psychres.2006.07.002. [DOI] [PubMed] [Google Scholar]
- 15.Abbasi A, Asayesh H, Rahmani H, Shariati A, Hosseini SA, Rouhi GH. The burden on caregivers from hemodialysis patients and related factors. J Res Dev Nurs Midwifery. 2011;8:26–33. [Google Scholar]
- 16.Jones PS, Lee JW, Phillips LR, Zhang XE, Jaceldo KB. An adaptation of Brislin's translation model for cross-cultural research. Nurs Res. 2001;50:300–4. doi: 10.1097/00006199-200109000-00008. [DOI] [PubMed] [Google Scholar]
- 17.Salmani N, Ashketorab T, Hasanvand S. The burden of caregiver and related factors of oncology patients of Shah Vali Hospital. Advances in Nursing and Midwifery. 2014;24:51–71. [Google Scholar]
- 18.Abbasi A, Shamsizadeh M, Asayesh H, Rahmani H, Hosseini SA, Talebi M. The relationship between caregiver burden with coping strategies in family caregivers of cancer patients. Iran J Nurs Res. 2013;1:62–71. [Google Scholar]
- 19.Given B, Wyatt G, Given C, Sherwood P, Gift A, DeVoss D, et al. Burden and depression among caregivers of patients with cancer at the end of life. Oncol Nurs Forum. 2004;31:1105–17. doi: 10.1188/04.ONF.1105-1117. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Akgul N, Ozdemir L. Caregiver burden among primary caregivers of patients undergoing peripheral blood stem cell transplantation: A cross sectional study. Eur J Oncol Nurs. 2014;18:372–7. doi: 10.1016/j.ejon.2014.03.013. [DOI] [PubMed] [Google Scholar]
- 21.Mitschke DB. Families Facing Prostate Cancer: Exploring Coping in Cross Cultural Families. Vol. 1050. USA: Ann Arbor; 2006. [Google Scholar]
- 22.Yeh PM, Bull M. Use of the resiliency model of family stress, adjustment and adaptation in the analysis of family caregiver reaction among families of older people with congestive heart failure. Int J Older People Nurs. 2012;7:117–26. doi: 10.1111/j.1748-3743.2011.00275.x. [DOI] [PubMed] [Google Scholar]
- 23.Rosdinom R, Zarina MZ, Zanariah MS, Marhani M, Suzaily W. Behavioural and psychological symptoms of dementia, cognitive impairment and caregiver burden in patients with dementia Preventive medicine. 2013;57:S67–S69. doi: 10.1016/j.ypmed.2012.12.025. [DOI] [PubMed] [Google Scholar]
- 24.Park B, Kim SY, Shin JY, Sanson-Fisher RW, Shin DW, Cho J, et al. Prevalence and predictors of anxiety and depression among family caregivers of cancer patients: A nationwide survey of patient-family caregiver dyads in Korea. Support Care Cancer. 2013;21:2799–807. doi: 10.1007/s00520-013-1852-1. [DOI] [PubMed] [Google Scholar]
- 25.Govina O, Kotronoulas G, Mystakidou K, Katsaragakis S, Vlachou E, Patiraki E. Effects of patient and personal demographic, clinical and psychosocial characteristics on the burden of family members caring for patients with advanced cancer in Greece. Eur J Oncol Nurs. 2015;19:81–8. doi: 10.1016/j.ejon.2014.06.009. [DOI] [PubMed] [Google Scholar]
- 26.Martinez-Rodriguez S, Ortiz-Marqués N, Iraurgi I, Carrasco M, Miguel JJ. Adaptation and analysis of psychometric features of the Caregiver Risk Screen: A tool for detecting the risk of burden in family caregivers. Int Psychogeriatr. 2013;25:755–64. doi: 10.1017/S1041610212002426. [DOI] [PubMed] [Google Scholar]
- 27.Yusuf AJ, Adamu A, Nuhu FT. Caregiver burden among poor caregivers of patients with cancer in an urban African setting. Psychooncology. 2011;20:902–5. doi: 10.1002/pon.1814. [DOI] [PubMed] [Google Scholar]
- 28.Hosseini S, Rezaee A, Keykhosravi Z. A comparison of old men and women's social support, life satisfaction, happiness and depression. Journal of women and society. 2012;2:143–161. [Google Scholar]
- 29.Siefert ML, Williams AL, Dowd MF, Chappel-Aiken L, McCorkle R. The caregiving experience in a racially diverse sample of cancer family caregivers. Cancer Nurs. 2008;31:399–407. doi: 10.1097/01.NCC.0000305760.04357.96. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Cui J, Song LJ, Zhou LJ, Meng H, Zhao JJ. Needs of family caregivers of advanced cancer patients: A survey in Shanghai of China. Eur J Cancer Care (Engl) 2014;23:562–9. doi: 10.1111/ecc.12174. [DOI] [PubMed] [Google Scholar]