

Abstract
Objectives:
Hepatitis B virus (HBV) and hepatitis C virus (HCV) are the most common causes of liver cirrhosis and hepatocellular carcinoma. Medical, applied medical science, and dental students constitute a high-risk group for HBV and HCV infections during their training or at the beginning of their careers. This study aimed to explore senior health science students’ knowledge of and attitudes toward these infections.
Methods:
Between December 2014 and December 2015, a cross-sectional survey was conducted among senior health science at the College of Medicine, the College of Dentistry, and the Laboratory Section of Applied Medical Sciences in Qassim University, Al-Qassim, Saudi Arabia. A validated questionnaire was randomly distributed to male and female senior students to test students’ knowledge of the general information on hepatitis B and C as well as their attitudes toward hepatitis B and hepatitis C patients and the disease in general.
Results:
A total of 205 respondents were invited, but only 180 participated in this survey. Higher knowledge was positively correlated with a higher belief in providing equitable care to hepatitis B/C patients and general anxiety about handling such patients (P < 0.004). Higher beliefs in equity and anxiety predicted higher knowledge when everything else was held constant.
Conclusion:
We found a positive relationship between knowledge levels and attitudes toward HBV and HCV patients. We therefore encourage health science colleges to offer more lectures on HBV and HCV to improve students’ knowledge and thereby improve their attitudes.
Keywords: Attitudes, belief, hepatitis B, hepatitis C, knowledge, medical students
Background
Viral hepatitis, or inflammation of the liver due to viral etiology, is a term specifically reserved to infection of the liver by a group of viruses with high affinity to the liver.1,2 Worldwide, viral hepatitis is the most common cause of hepatitis.1 The main five viruses, or so-called “hepatotropic” viruses, are hepatitis A, hepatitis B viruses (HBV), hepatitis C viruses (HCV), hepatitis D, and hepatitis E viruses.1,2 Viral hepatitis B and C can be self-limiting, progress into a chronic state or carrier, or even lead to hepatocellular carcinoma (HCC) or liver failure, whereas viral hepatitis A and E have an acute state and are both self-limited.1 HBV and HCV are the most common causes of liver cirrhosis and HCC, and both are leading causes of death, with HBV infection ranking the tenth worldwide.1,3 Both viruses are blood-borne infections and also can be transmitted through other body fluids; hence, they are transmitted sexually as well as vertically.1
Worldwide, of the two billion people infected with HBV, 400 million are HBV carriers and 170 million people live with HCV.4 Approximately 500,000-700,000 die due to HBV infection every year4 and 8,000-13,000 due to HCV.5 The Middle East is classified as an area of intermediate HBV prevalence, that is, 2-5%,6 and an area of high HCV prevalence, that is, >3.5%.5 In Saudi Arabia, although the prevalence has greatly declined, viral hepatitis has been a burden on the country’s health-care system. For example, in 2007, viral hepatitis was one of the most prevalent viral diseases, being just second to chickenpox, with an incidence of almost 9,000 new cases diagnosed in that year: HBV represented 52% of all new cases and HCV 32%, according to the Saudi Ministry of Health.4 The prevalence of HBV in the general population in Saudi Arabia is almost 4.25%; however, it is <1% for HCV though it increases among patients with multiple transfusions, reaching up to 56%.7
Since HBV and HCV are transmitted through blood and body fluids, many health-care personnel (HCP) and health laboratory personnel are susceptible to infection with these viruses following exposure to body fluids or blood of infected patients and its other components.8 The Center for Disease Control estimates that each year, close to 385,000 sharps-related injuries take place among health-care workers.9 According to the Exposure Prevention Information Network data from 2011, nurses were the most frequently injured HCP (45%), followed by physicians (14%), and medical trainees (13%).10 Although HCP are highly vulnerable to HBV infections, the prevalence of HBV among HCP has declined by almost 98%, from 17,000 cases annually to 263, largely due to HBV immunization.8
As a part of HCP training, health science students, including medical students, medical applied sciences students, and dental students constitute a high-risk group for HBV and HCV infection during their training or when they first start work.8,10-13 Unfortunately, in Saudi Arabia, there is a paucity of studies on students’ knowledge, attitudes toward, and practices regarding HBV and HCV infections. Thus, the main objective of this study was to evaluate knowledge levels about HBV and HCV among senior health students at Qassim University. The secondary objective was to explore students’ attitudes toward patients infected with HBV and/or HCV and to analyze the correlation between students’ level of knowledge and their attitudes.
Methods
Setting
This cross-sectional study was conducted between January 2014 and January 2015 at Qassim University. Qassim University is a public university in Saudi Arabia that was established in 2004. Its main campus, where this study was conducted, is located in Almulyda, Al Qassim, Saudi Arabia. The main campus has many colleges, including the College of Medicine, the College of Dentistry, and the College of Applied Medical Sciences. The College of Applied Medical Sciences encompasses subspecialties, including a medical laboratory.
Sample
A simple convenience random sample of senior students was selected from three colleges at Al-Qassim University, Saudi Arabia: College of Medicine, College of Dentistry, and College of Applied Sciences. A total of 180 students out of 205 responded to the survey.
An anonymous, self-administered, validated questionnaire was used.12 For piloting purposes, a few students from the College of Medicine were initially asked to take part in the study, and ten students verbally consented to participate. They received a full explanation of the study and its importance and were informed that no incentives were offered for their participation. The pilot study evaluated the tool’s design, length of time taken to fill in the questionnaire, and clarity and relevance of the questions. Students were asked about their overall impression of the survey tool after completing the questionnaire. The tool was modified based on the students’ suggestions.
The final version of the questionnaire was distributed to students of all three colleges. Male and female final-year students of each batch of every college were included in the study. The purpose and importance of the study were explained to all potential participants. Consent was obtained from every participant before enrollment in this study.
Questionnaire
Respondents were asked at the beginning of the questionnaire to identify their gender and college of study. A test, which included 25 selected questions from medical evidence and the literature, was administered to score students’ knowledge of the general information on hepatitis B and C (infectivity, modes of transmission, diagnosis, prognosis, care, prevention, and long-term complications). In effect, the researcher scored each student’s answers in a true/false manner. Thus, the minimum expected knowledge score was zero and the maximum was 25 (denoting zero to 100% possible percentage correct answers). Moreover, the researcher asked respondents to answer with “undecided,” “disagree,” or “agree” on 17 questions that explored attitudes (behaviors and beliefs) toward hepatitis B and hepatitis C patients and the disease itself. The 17 items asked students about specific behaviors, such as whether they like to care for infected individuals, whether they felt disgusted to care for infected people, whether they believe they treat hepatitis B and C patients with humanely, justly, and with equity, whether they believe patients should be isolated and delayed from receiving care until other patients are attended to in full, whether precautions and special medical equipment and diagnostics are necessary when caring for hepatitis patients, and whether such equipment should be obligatory when handling hepatitis B or C patients. Students were also asked to answer questions that assessed their attitudes regarding preventive/self-protective measures, such as wearing gloves and personal protection equipment, and whether they tend to spend less time interacting with hepatitis B and C patients.
Institutional review board approval was obtained from the University for this study.
Statistical analysis
Means and standard deviations were utilized to describe continuous variables, such as knowledge and attitude scores, and medians were utilized when appropriate for specific tests. Percentages were used to describe categorical variables. Alpha significance level was preset to 0.05 throughout the analysis.
Principal component analysis (PCA) with non-orthogonal (Promax) rotation of the Z-scores (standardized scores) of the 17 attitude survey questions was conducted on data gathered from 178 participants. An examination of the Kaiser-Meyer-Olkin (KMO) measure of sampling adequacy suggested that the sample was factorable (KMO = 0.858) and none of the included items had initial variance explained by the factors solutions, which was <0.2. In fact, the majority had initial loadings above 0.4, and the correlation matrix between raw attitude variables yielded many Pearson’s correlations (r) above 0.3, with significance ≤0.05. This denoted an overall suitability and consistency of the included items. The intent of doing PCA was to identify constructs, if they existed, within the 17-item questionnaire and to find out how items would coalesce when they were analyzed to compute composite scores from those items; no factor scores were utilized in the analysis. The same factor structure was also double-checked using the categorical PCA, with tetrachoric correlations between items. However, Cronbach’s alpha test of internal consistency was found to be adequately high (alpha = 0.82) between the 17 items.
Attitude (behavior and beliefs) items were recorded as follow: (1) Undecided, (2) disagree, and (3) agree. Summation was used to group items that emerged from the PCA as themes, namely, agreement on equitable/just treatment of hepatitis B or C patients, anxiety, rejection of people infected with hepatitis B or C, and complete fearlessness/openness to hepatitis-infected persons. The openness/fearlessness score comprised the following items: The possibility that I will be infected with HBV or HCV at work is low + HIV is easier to catch than hepatitis B and C + HBV and HCV positive patients should stay away from other family members + testing outpatients for HBV and HCV is not necessary. The minimum and maximum possible scores were 1 and 12, respectively. Equity comprised the following items: I will be protected from HBV and HCV at work if I follow infection control guidelines + I deliver the same standard of care to patients with HBV and HCV as I do for other patients + I am willing to treat people with HBV and HCV + I am not averse to having contact with HBV and HCV patients + I often use additional infection control precautions when treating patients with HBV and HCV + all patients should be tested for HBV and HCV before receiving health care + education is effective in improving knowledge on hepatitis B and C + patients with HBV and HCV should be given the last appointment for the day. The minimum and maximum possible scores were 1 and 24, respectively. The anxiety/fear score comprised the following items: I try not to spend much time when I provide health-care services to HBV and HCV patients + I do not like treating people with HBV and HCV + I feel that I do not have the skills needed to effectively and safely treat patients with HBV and HCV + I would prefer to wear two pairs of gloves when treating a bleeding person with HBV and HCV + health professionals who are HBV or HCV positive should not give health-care services to patients. The minimum and maximum scores were 1 and 15, respectively.
A multivariate linear regression model was utilized to explore the nature of the relationship between students’ demographic variables (gender and college of study) and attitude scores estimated from summative analysis. The goal of the multivariate linear regression model was to identify how the variables interact individually or jointly on predicting the knowledge score of the students and to identify whether differences existed between those factors when considered as a whole set of variables, that is, to identify which predictor provides more practicable and theoretical importance than the others.
Results
Of the 180 students who completed the questionnaire, 103 were male (57.2%). Students of the college of medicine were the least represented (20.0%) compared with dentistry and health science students, who represented 46.7% and 33.3% of the sample, respectively.
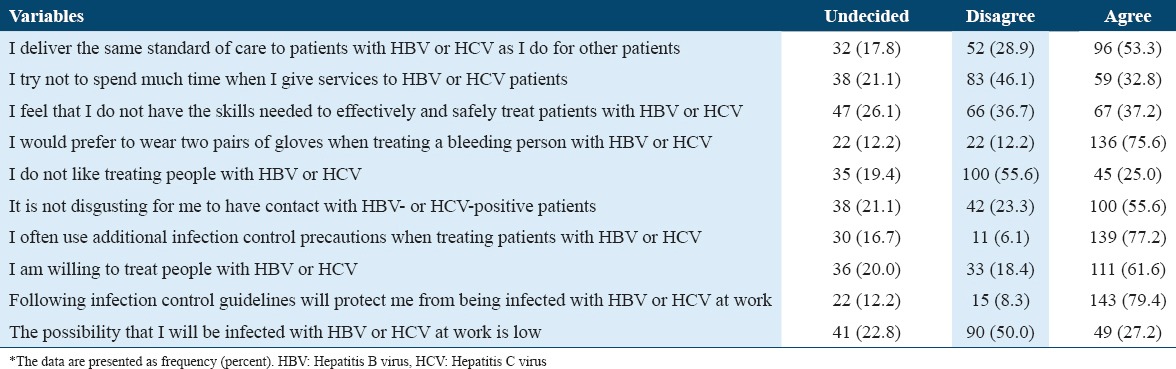
In more than half of cases, students agreed that all patients should be tested for HBV and HCV before receiving health care (Table 1).
Table 1.
Frequency of students’ responses to questions regarding hepatitis B and C infections and the management of patients with these infections*

Most students reportedly took precautions while caring for hepatitis patients, with close to three-fourths of participants responding that they preferred to wear double gloves; a slightly higher proportion used additional infection control measures when treating hepatitis patients. Approximately four-fifths of the students agreed that following infection guidelines will protect them from hepatitis B and C, and a slightly higher proportion agreed education was effective in improving knowledge on hepatitis B and C. Half of the respondents did not believe they could become infected at work (Table 2).
Table 2.
Frequency of students’ responses to questions regarding their behaviors toward patients with hepatitis B or C infection*
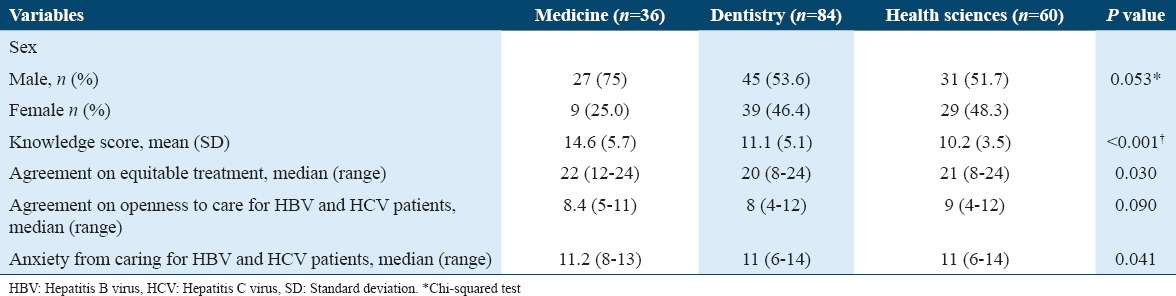
Medical students had the highest knowledge score compared with dental and health science students (P < 0.001). Medical students were also most likely to agree on equitable treatment of all patients, irrespective of their HBV or HCV status (P = 0.03). However, students from all medical colleges expressed anxiety when caring for HBV and HCV patients (P = 0.041). Conversely, respondents from all three colleges did not differ significantly in terms of gender and openness to care for hepatitis B and C patients (Table 3).
Table 3.
Comparison of variables between students of all three colleges
Further analysis demonstrated that higher knowledge scores were moderately correlated with higher beliefs in providing equitable care to hepatitis B and C patients (r = 0.57; P < 0.0041) and anxiety about handling these patients (r = 0.48; P < 0.0041). On the other hand, complete openness/fearlessness were positively, but weakly, correlated with higher knowledge scores (r = 0.24, P < 0.01). Anxiety about caring for hepatitis B or C patients also correlated significantly with both equity and openness/fearlessness (r = 0.27; Table 4).
Table 4.
Correlations between knowledge score and sum of items on specific attitudes toward hepatitis B and C patients

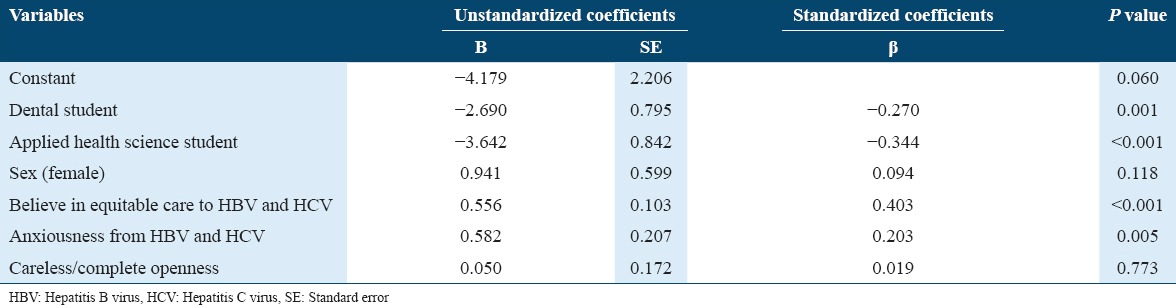
On multivariate analysis, college type was a significant predictor of knowledge (P < 0.001), with students of the colleges of applied medical sciences and dentistry having significantly lower knowledge scores compared with medical students. Similarly, belief in equity for every patient and anxiety when treating hepatitis B and C, patients were significant predictors of knowledge (P < 0.001 in all cases). Conversely, female gender and openness to provide health care to HBV and HCV patients were not significantly correlated with knowledge scores (Table 5).
Table 5.
Multivariate linear regression model predicting knowledge score on hepatitis B and C
Discussion
Viral hepatitis is the most common cause of hepatitis worldwide.1 Both HBV and HCV are leading causes of death, with HBV infection ranking tenth globally.1,3 Medical trainees are at high risk of being exposed to health-care-related injuries.10 The risk of transmission after percutaneous exposure is estimated to be approximately 6-30% for HBV, and almost 1.8% for HCV.14
Assessment of general population knowledge is a beneficial measure to evaluate the extent or limit to which a particular individual, or even the whole community, is to embrace a disease risk-free behavior for a certain disease.15 As such, evaluating students’ knowledge is of a quite significant importance, since being exposed to these infections during their field training, students may serve as particulate nidi of infection jeopardizing patients’ lives.12,16 The infection could transmit to approximately 1-50 patients by merely one infected HCW.14 Hence, knowing the level of students’ perception of them being at risk of contracting these infections, helps us protecting the students and the patients.12,16
In this study, most of the senior health sciences students were obviously aware of the probable occupational risk due to HBV and HCV. This result is in line with a similar study conducted by Al-Hazmi in Al-jouf, Saudi Arabia, among medical students.3 On the contrary, a survey by Mansour-Ghanaei et al.12 as well as another one by Singh and Jain17 reported that the knowledge of medical sciences students and medical students, respectively, to be quite weak and need to be strengthened. Moreover, Mesfin and Kibret18 reported that most medical and health sciences students in showed poor knowledge of viral hepatitis B.
In the current survey, level of knowledge was significantly affected by several factors; the student’s major was the most significant in predicting the level of knowledge. Medical students scored the highest among all the other majors’ students followed by dental and applied medical sciences students. This result may be attributed to the length of time medical students spend in contact with patients with hepatitis B and C during their clinical phase, and to the number of lectures they have been provided with by the college concerning viral hepatitis. This could by noticed and supported by the results Mansour-Ghanei et al.12 reported about medical sciences students’ knowledge about HBV and HCV infections, in which he has noticed that nursing students were the most knowledgeable and has suggested their exposure to patients to be the reason.
It is of a paramount significance that health sciences students be invited and encouraged to take all precautions needed to halt and curb work-related HBV infection transmission including the use of protective personal equipments and getting vaccinated.19,20 In the current work, most students agreed on double-gloving before treating a bleeding patient having Hepatitis B or C. Al-Hazmi3 A reported a similar finding, in which 79.3 of the students agreed on wearing gloves as a protective measure. The result is also in line with a report conducted by Mansour-Ghanaei et al. who found that 77.6% of health science students agreed on double-gloving when treating a patient with hepatitis B or C.12 Not wearing medical gloves during invasive procedures is believed to be a culprit in the epidemiology of HBV transmission among HCWs,16 and using it looks to be effective at bringing down the odds of risk of blood-borne infections for HCWs.21,22 Conversely, a study by Mesfin and Kibret showed that 89.4% of the students had poor practice in concerns to prevention.18
In this report, 68.2% of the students agreed that all patients should be tested for HBV and HCV before receiving health care. Similarly, Mansour-Ghanaei et al.12 showed that 83.3% of health science students thought patients should be screened for viral hepatitis. Regarding students’ opinions on whether patients with HBV and HCV should be given the last appointment at the end of the day, 36.3% of the students agreed on that. A similar finding was reported by Mansour-Ghanaei et al., who found that 34.7% of the respondents were uncomfortable when they came in contact with HBV and HCV patients.12
The current study illustrates the existence of a strong positive relationship between knowledge and attitudes; the higher the knowledge the better the attitude. It was also found that students, who believed in equitable care to all patients, were more likely to be more knowledgeable than the rest. This is clearly exemplified by medical students having better attitudes compared to other groups, taking into account that medical students scored highest in knowledge. Al-Hazmi3 study findings suggested an existence of a correlation of knowledge and attitudes. However, Mansour-Ghanei reported similar findings as ours. This finding is also consistent with Shahbaz et al. Study.23
On the other hand, many students who scored higher knowledge tended also to be anxious. This suggests the existence of different factors other than knowledge controlling students believes including social factors.
Our study, to the best of our knowledge, is the first to evaluate the knowledge and believes of health seniors students in their last, in Qassim, Saudi Arabia. It also concerns a common infectious disease in the region and a more common nightmare for most HCWs. Nevertheless, we still admit that many weak spots exist in the current study. Of which, response rate, especially among female medical students is relatively poor, which makes it difficult to detect several factors of a statistical significance. Coverage of the other two medical colleges as well as coverage of the other health sciences colleges is certainly needed. Evaluating the level of vaccination against HBV as well as the HBs-Ab status is of a quite significant importance. Moreover, although some students reported positive attitudes, believes, and behaviors, we still do not know whether this is actually practiced in real life or not. Further studies are needed to cover the aforementioned points, to have a complete picture of status of viral hepatitis among health sciences students.
Conclusion
To conclude our work, the general knowledge of viral hepatitis B and C was acceptable, and a positive relationship exists between students’ knowledge and attitudes toward HBV and HCV patients; students with higher knowledge scores have better attitudes toward HBV and HCV patients. Thus, health authorities and health-care policy makers in the region should co-operate with health sciences colleges administrators to set an evidence-based academic and clinical education and training on how to prevent viral hepatitis transmission among these students, and from infected ones to the patients, as well as training them on what to do whenever they are exposed to any risk factor including infected body fluids. This would possibly improve students’ knowledge on these infections, thereby improving attitude toward patients with viral hepatitis B and C and would possibly implement the adoption of risk-free behaviors among these students. Efforts should also be made to establish rules mandating HBV vaccinations and regular seromakers checking.
References
- 1.What is Hepatitis? World Health Organization. [[Last accessed on 2016 Oct 10]]. Available from: http://www.who.int/features/qa/76/en .
- 2.Kumar V, Abbas AK, Fusto N, Mitchell RN. Robbins Basics of Pathology. 8th ed. Philadelphia, PA: Saunders, Elsevier; 2007. Liver, gallbladder, and biliary tract; p. 640. [Google Scholar]
- 3.Al-Hazmi A. Knowledge, attitudes, and practice of medical students regarding occupational risks of hepatitis B virus in college of medicine, Aljouf University. Ann Med Health Sci Res. 2015;5:13–9. doi: 10.4103/2141-9248.149765. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Abdo AA, Sanai FM, Al-Faleh FZ. Epidemiology of viral hepatitis in Saudi Arabia: Are we off the hook? Saudi J Gastroenterol. 2012;18:349–57. doi: 10.4103/1319-3767.103425. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Chopra S, Biscegl A, Bloom A. Epidemiology and Transmission of Hepatitis C Virus Infection. [[Last accessed 2016 Oct 10]]. Available from: http://www.uptodate.com/contents/epidemiology-and-transmission-of-hepatitis-c-virus-infection?source=see_link .
- 6.Teo E, Lok AS, Kaplan SL, Esteban R, Mitty J. Epidemiology, Transmission and Prevention of Hepatitis B Virus Infection. 2015. Dec, [[Last accessed on 2016 Oct 10]]. Available from: http://www.uptodate.com/contents/epidemiology-transmission-and-prevention-of-hepatitis-b-virus-infection .
- 7.Comment Viral Hepatitis in the Middle East-The Lancet. Available from: http://www.thelancet.com/pb/assets/raw/Lancet/global-health/middle-east/Oct14_MiddleEastEd.pdf?elsca1=220713 .
- 8.Weber DJ, Rutala WA, Eron J, Bartlett JG, Mitty J. Prevention of Hepatitis B Virus and Hepatitis C Virus Infection Among Healthcare Providers. [[Last accessed on 2016 Oct 10]]. Available from: http://www.uptodate.com/contents/prevention-of-hepatitis-b-virus-and-hepatitis-c-virus-infection-among-healthcare-providers?source=see_link .
- 9.Center for Disease Control and Prevention. Stop Sticks Campaign. [[Last accessed 2016 Oct 10]]. Available from: http://www.cdc.gov/niosh/stopsticks/sharpsinjuries.html .
- 10.Exposure Prevention Information Network. Monograph on the Internet. Sharp-Object Injury and Blood and Body Fluid Exposure Reports by Year (1997-2011) [[Last accessed on 2016 Oct 22]]. Available from: http://www.medicalcenter.virginia.edu/epinet/epinetdatareports.html .
- 11.Odusanya OO, Meurice FP, Hoet B. Nigerian medical students are at risk for hepatitis B infection. Trans R Soc Trop Med Hyg. 2007;101:465–8. doi: 10.1016/j.trstmh.2006.08.001. [DOI] [PubMed] [Google Scholar]
- 12.Mansour-Ghanaei R, Joukar F, Souti F, Atrkar-Roushan Z. Knowledge and attitude of medical science students toward hepatitis B and C infections. Int J Clin Exp Med. 2013;6:197–205. [PMC free article] [PubMed] [Google Scholar]
- 13.Al-Hazmi AH. Knowledge, attitudes and practice of dentists concerning the occupational risks of hepatitis B virus in Al Jouf Province, Saudi Arabia. Niger J Clin Pract. 2015;18:276–81. doi: 10.4103/1119-3077.151067. [DOI] [PubMed] [Google Scholar]
- 14.Beltrami EM, Williams IT, Shapiro CN, Chamberland ME. Risk and management of blood-borne infections in health care workers. 2000;13:385–407. doi: 10.1128/cmr.13.3.385-407.2000. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC88939 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.El-Nasser GA, El-Baset EA. Assessment of students knowledge and attitude toward hepatitis B and C in Sohag University/Egypt. Kufa J Nurs Sci. 2013;3:1–14. [Google Scholar]
- 16.Razi A, Ur Rahman R, Naz S, Ghafoor F, Khan MA. Knowledge attitude and practices of university students regarding hepatitis B and C. ARPN J Agric Biol Sci. 2010;5:38–43. [Google Scholar]
- 17.Singh A, Jain S. Prevention of Hepatitis B-Knowledge and Practices among Medical Students. 2012. Feb, Available from: http://www.medind.nic.in/ice/t12/i2/icet12i2p52.pdf .
- 18.Mesfin YM, Kibret KT. Assessment of Knowledge and Practice towards Hepatitis B among Medical and Health Science Students in Haramaya University, Ethiopia. Available from: http://www.journals.plos.org/plosone/article?id=10.1371/journal.pone.0079642 . [DOI] [PMC free article] [PubMed]
- 19.Reis JM, Lamounier Filho A, Rampinelli CA, Soares EC, Prado Rda S, Pedroso ER. Training-related accidents during teacher-student-assistance activities of medical students. Rev Soc Bras Med Trop. 2004;37:405–8. doi: 10.1590/s0037-86822004000500007. [DOI] [PubMed] [Google Scholar]
- 20.Swarnalatha N. Do nursing students know about hepatitis B? A study from nursing college in Tamil Nadu. [[Last cited on 2016 Dec 12]];Int J Health Rehabil Sci. 2014 3:69–74. DOI:10.5455/IJHRS.000000055. Available from: http://www.scopemed.org/?mno=165735 . [Google Scholar]
- 21.Pido B, Kagimu M. Prevalence of hepatitis B virus (HBV) infection among Makerere University medical students. Afr Health Sci. 2005;5:93–8. [PMC free article] [PubMed] [Google Scholar]
- 22.Ciorlia LA, Zanetta DM. Hepatitis B in healthcare workers: Prevalence, vaccination and relation to occupational factors. Braz J Infect Dis. 2005;9:384–9. doi: 10.1590/s1413-86702005000500005. [DOI] [PubMed] [Google Scholar]
- 23.Shahbaz T, Raza SM, Manzoor Z, Jamshid A. Hepatitis B and C: Knowledge, Attitude and Perception of Medical Students at Lahore Medical & Dental College, Lahore. Available from: http://www.pjmhsonline.com/2014/july_sep/pdf/789%20%20%20Hepatitis%20B%20and%20C%20Knowledge,%20attitude%20and%20Perception%20of%20medical%20students%20at%20Lahore%20Medical%20&%20Dental%20College,%20Lahore.pdf .