

Abstract
Dissecting cellulitis of the scalp (DC) is a chronic inflammatory condition of the scalp that ultimately leads to scarring alopecia. A healthy 19-year-old male presented with a solitary, soft, alopecic nodule that had appeared 1 year before. A color Doppler ultrasound examination showed a hypodermal anechoic fluid collection in the left parietotemporal region of the scalp, connected to the base of widened hair follicles, and presented inner echoes suggestive of debris, as well as several fragments of hair tracts. A diagnosis of DC was made and an epidermal or trichilemmal cyst was ruled out. This case shows the importance of color Doppler ultrasound for supporting the diagnosis at an early stage or with an unusual presentation of DC.
Key words: Alopecia, early diagnosis, ultrasonography
INTRODUCTION
Dissecting cellulitis of the scalp (DC), also known as perifolliculitis capitis abscedens et suffodiens, is a chronic inflammatory condition, characterized by relapsing folliculitis and painful, fluctuant abscesses in the scalp that ultimately leads to scarring alopecia. Due to its association with acne conglobata, hidradenitis suppurativa, and pilonidal cyst (follicular occlusion tetrad), it is believed to be the result of an abnormal follicular keratinization and occlusion process that leads to follicular destruction and a neutrophilic and granulomatous inflammatory response.[1]
CLINICAL CASE
We present a healthy 19-year-old male with one alopecic patch that had appeared 1 year ago. The patient referred occasional swelling, pain, and purulent discharge. On the physical examination, a soft alopecic and minimally raised nodule was found, without discharge or a distinguishable central ostium [Figure 1].
Figure 1.

Soft alopecic, minimally raised nodule, without discharge or a distinguishable central ostium
A color Doppler ultrasound examination was requested to support the diagnosis. This showed a 1.5 cm × 0.6 cm × 1.4 cm hypodermal anechoic fluid collection in the left parietotemporal region of the scalp. The fluid collection was connected to the base of widened hair follicles and presented inner echoes suggestive of debris as well as several hyperechoic linear structures compatible with fragments of hair tracts [Figure 2]. Increased vascularity with low velocity arterial and venous vessels was detected in the periphery of the fluid collection [Figure 3]. The latter findings were suggestive of DC and ruled out an epidermal or trichilemmal cyst.
Figure 2.

Perifolliculitis capitis abscedens et suffodiens fluid collection (gray scale; transverse view; left parietotemporal region). Dermal and hypodermal hypoechoic fluid collection connected to the base of widened hair follicles (arrowheads pointing up). Notice the hair tract fragment within the collection
Figure 3.
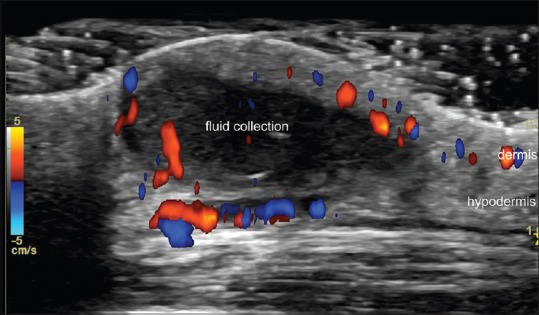
Perifolliculitis capitis abscedens et suffodiens fluid collection vascularity (color Doppler ultrasound; transverse view; left parietotemporal region). The image demonstrates increased vascularity in the periphery of the fluid collection suggestive of inflammation and activity of the disease
DISCUSSION
DC is classified as a neutrophilic scarring alopecia and it has been reported that working with oily substances might trigger DC in individuals who may be otherwise predisposed to this condition.[2] Our patient worked in a fast-food restaurant.
Clinically, DC is characterized by multiple interconnecting abscesses, especially in vertex and occipital area,[2] which is different from the present case, with a single lesion.
The ultrasound appearance of the fluid collection in our case is similar to previous sonographic descriptions of fluid collections in DC;[3,4] however, in literature, the reports show severe cases with patchy alopecia, large fluid collections and fistulous tracts.[3,4] To the best our knowledge, the report of a single fluid collection with this morphology has not been described. Interestingly, the morphology of this fluid collection is similar to one already described for fluid collections that are sonographically seen hidradenitis suppurativa.[5]
Nonruptured epidermal and trichilemmal cysts present a different ultrasound morphology, commonly characterized by well-defined, oval-shaped, structures that contain anechoic fluid and/or hypoechoic material (keratin).[6]
Evidence has shown that isotretinoin should be considered the first-line treatment, in doses ranging from 0.5 to 1 mg/kg/day for 3 months to 1 year.[7] This treatment may provide remission of up to 2.5 years.[8] For advanced-stage disease, complete scalp excision plus split-thickness skin grafting has been attempted, with variable results. Laser depilation and TNF-alpha blockers may be used in recalcitrant disease.[4]
This case highlights an unusual presentation of DC and the usage of color Doppler ultrasound for supporting an early diagnosis of this disease.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- 1.Mundi JP, Marmon S, Fischer M, Kamino H, Patel R, Shapiro J. Dissecting cellulitis of the scalp. Dermatol Online J. 2012;18:8. [PubMed] [Google Scholar]
- 2.Segurado-Miravalles G, Camacho-Martínez FM, Arias-Santiago S, Serrano-Falcón C, Serrano-Ortega S, Rodrigues-Barata R, et al. Epidemiology, clinical presentation and therapeutic approach in a multicentre series of dissecting cellulitis of the scalp. J Eur Acad Dermatol Venereol. 2017;31:e199–e200. doi: 10.1111/jdv.13948. [DOI] [PubMed] [Google Scholar]
- 3.Wortsman X, Wortsman J, Matsuoka L, Saavedra T, Mardones F, Saavedra D, et al. Sonography in pathologies of scalp and hair. Br J Radiol. 2012;85:647–55. doi: 10.1259/bjr/22636640. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Wortsman X, Roustan G, Martorell A. Color Doppler ultrasound of the scalp and hair. Actas Dermosifiliogr. 2015;106(Suppl 1):67–75. doi: 10.1016/S0001-7310(16)30009-6. [DOI] [PubMed] [Google Scholar]
- 5.Wortsman X. Imaging of hidradenitis suppurativa. Dermatol Clin. 2016;34:59–68. doi: 10.1016/j.det.2015.08.003. [DOI] [PubMed] [Google Scholar]
- 6.Wortsman X. Ultrasound in dermatology: Why, how, and when? Semin Ultrasound CT MR. 2013;34:177–95. doi: 10.1053/j.sult.2012.10.001. [DOI] [PubMed] [Google Scholar]
- 7.Scheinfeld N. Dissecting cellulitis (Perifolliculitis Capitis Abscedens et Suffodiens): A comprehensive review focusing on new treatments and findings of the last decade with commentary comparing the therapies and causes of dissecting cellulitis to hidradenitis suppurativa. Dermatol Online J. 2014;20:22692. [PubMed] [Google Scholar]
- 8.Scerri L, Williams HC, Allen BR. Dissecting cellulitis of the scalp: Response to isotretinoin. Br J Dermatol. 1996;134:1105–8. [PubMed] [Google Scholar]