

Abstract
INTRODUCTION:
Esthetics plays an essential role in orthodontic treatment. The psychological effects of malocclusion are an inspiration to improve one's esthetics and seek treatment.
OBJECTIVES:
This study aimed to assess relationships between self-esteem and malocclusion severity and type in adolescents using a self-esteem measurement scale and the index of treatment need (IOTN) and to investigate the influence of age, sex, and school type in these relationships.
MATERIALS AND METHODS:
Adolescent students aged 12–19 years randomly selected from four private and two governmental schools were enrolled for this study. After completing the self-esteem questionnaire, participants were examined by researchers to evaluate malocclusion severity and type using the IOTN.
RESULTS:
The sample consisted of 886 participants: 558 females (62.9%) and 328 males (37.1%) with a mean age of 16 years. Chi-square analysis showed that 17.1% of males and 31% of females showed low levels of self-esteem, with a statistically significant difference (P < 0.001). Cases with multiple malocclusions showed significantly lower self-esteem (P = 0.018) compared with single-category malocclusion. Anterior teeth spacing, crowding, and overjet malocclusion showed the highest percentages of low self-esteem.
CONCLUSIONS:
The present study supports that malocclusion has negative effects on self-esteem; multiple malocclusions with spacing, crowding, and overjet had the greatest effects.
Keywords: Adolescent, index of treatment need, malocclusion, self-esteem
Introduction
Physical appearance and attractiveness have imperative roles in interpersonal communication and interaction;[1,2] hence, malocclusion may have a negative effect on social relationships, and this in turn will affect the self-image and self-worthiness of people with malocclusion. Self-esteem is an essential part of human psychology; it is how we value and appreciate ourselves, it influences our trust in others, work, relationships, and almost every part of our lives. Individuals with positive or higher self-esteem will have better qualities of life and will be able to handle stressful events in a better manner.[3] On the other hand, low or negative self-esteem is a debilitating condition in which the person feels unworthy, incapable, and incompetent.[4]
The impact of dental appearance varies among the sexes, age groups, socioeconomic groups, and according to the cultural standards of beauty.[5,6,7,8] Females are usually more concerned with their appearance and looks; therefore, malocclusion concerns women more than men. Thus, it seems to have different psychological impacts between the sexes in their perceptions of facial and dental appearance. Sardenberg et al. found that children in low social class families suffered a 60% greater negative impact from malocclusion than those in higher social class families;[9] however, Bellot-Arcís et al. believed that no such association was present.[7]
Adolescence is known as a period of developmental and psychological instability. Research on self-esteem during the adolescent stage provides controversial results. Kuzucu et al. concluded that adolescence is the stage of self-esteem formation;[10] however, in a cross-sectional study, Robins et al. examined age differences in self-esteem in a large sample ranging in age from 9 to 90 years and stated that “self-esteem levels were high in childhood, dropped during adolescence, rose gradually throughout adulthood, and declined sharply in old age.”[4]
Several factors related to malocclusion, such as anterior crowding, midline malalignment, and facial asymmetry, have strong effects on the perception of facial esthetics, which influence the psychological development of children and adolescents, and in turn, influence social acceptance and self-perception. Controversial results were found in several studies evaluating the effects of malocclusion and orthodontic treatment on self-esteem. Some studies found a significant correlation between lower self-esteem and malocclusion and the improvement of self-esteem as a result of orthodontic treatment.[7,11,12,13,14,15] On the other hand, Kiyak reported that orthodontic intervention did not significantly affect self-esteem.[16]
This study is important due to the limited number of studies that explored the effect of malocclusion on self-esteem and the level of self-esteem in relation to the precise types of malocclusion conducted in the western region of Saudi Arabia. Therefore, it is necessary to perform a study to establish these relationships in Saudi Arabian culture.
The aim of the present study was to evaluate the psychological effect of malocclusion on self-esteem by determining the association between the severity and type of malocclusion and self-esteem in adolescence using the index of treatment need (IOTN) and to investigate the influence of demographic data on the psychological status of adolescents with malocclusion.
Materials and Methods
Participants
This cross-sectional, descriptive and analytic study was conducted in Saudi Arabia on a sample of male and female secondary school students aged 12–15 years and high school students aged 15–19 years who were randomly selected from governmental and private schools from different demographic areas of western region.
Ethical approval for this study was obtained from the Research Ethics Committee at King Abdulaziz University. All students were given a hard copy of the questionnaire; after completion of the questionnaire, participants were examined in the school premises under natural light by the authors. The IOTN was used to record the severity of malocclusion; orthodontically treated students were only given the questionnaire and were not examined according to the IOTN; craniofacial anomaly was excluded from this study.
Questionnaire
The questionnaire consisted of two main parts: demographic data and 14 questions tailored from both State Self-Esteem Scale[4] and Collective Self-Esteem Scale,[17] assessed using a Likert scale of 3, with the following responses: 1 = not at all, 2 = somewhat, and 3 = extremely. The reliability of the questionnaire was tested using Cronbach's alpha analysis on forty questionnaires. The questionnaire score was summed for each participant; participants who scored 70% or greater were considered to have moderate-to-high self-esteem, while participants who scored <70% were considered to have low self-esteem.
Malocclusion assessment
Malocclusion assessment was performed using the dental health component (DHC) of the IOTN. The DHC contains different malocclusion traits ranked according to the severity into five grades: 1–2 indicate no or little treatment need, 3 indicates a moderate or borderline treatment need, and 4–5 indicate a severe-to-extreme treatment need.[18]
After the questionnaire was completed, the authors examined each participant according to the DHC of the IOTN and also recorded the main type of malocclusion. The parameters of malocclusion were taken from the IOTN and consisted of degree of overjet and anterior overbite, presence or absence of anterior crossbite, posterior crossbite, anterior openbite, posterior open bite, and severity of crowding and spacing.
The researchers were calibrated prior to examining the participants to minimize inter-examiner error, each author examined forty cases twice; the follow-up examinations were conducted after a 2-week interval. The intra-examiner kappa value for the DHC was 0.85, which indicates good intra-examiner reproducibility. Regarding inter-examiner reproducibility, the same forty cases were checked twice by both authors, and 80% of the cases were rated identically.
Statistical analyses
Statistical analyses were performed using the Statistical Package for the Social Sciences version 20 (SPSS Inc., Chicago, IL, USA). Descriptive analyses of the data were performed. Cronbach's alpha and Pearson's correlation coefficient were used to test the reliability and validity of the questionnaire, and Chi-square test was used to examine distribution differences in self-esteem according to the demographic data, orthodontic treatment, IOTN, and type of malocclusion.
Results
Descriptive data
A total of 975 adolescents were invited to take part in the main study; 89 students were excluded from the study because of incomplete questionnaire. The participants included in the study were 886 students: 558 female participants (62.9%) and 328 male participants (37.1%). Ages ranged from 12 to 19 years with a mean age of 16 years. Four hundred and sixty-seven participants attended private schools and 419 attended public schools (52.7% and 47.3%, respectively). Seven hundred and sixty-one study participants had no orthodontic treatment (85.9%), whereas 125 students had orthodontic treatment (14.1%).
Reliability of the questionnaire
The reliability of the questionnaire was tested using Cronbach's alpha analysis on forty questionnaires. It showed a coefficient of 0.712 for the self-esteem scale.
Validity of the questionnaire
Pearson's correlation test was used to determine the construct validity of the questionnaire, showing r values ranging between 0.4 and 0.5, indicating moderate validity. However, the correlation values of all variables were highly significant (<0.001) due to the large sample size.
Relationship between self-esteem and demographic data
Table 1 shows correlations in self-esteem levels according to the demographic data. There was a highly statistically significant difference in self-esteem between the sexes; 31% of female participants showed low levels of self-esteem versus 17.1% of male participants (P < 0.001).
Table 1.
Correlations between self-esteem level and the demographic data (sex, age group, school type, and level of education)

Older participants, i.e. ≥18 years old showed the greatest moderate-to-high levels of self-esteem versus the group aged 14–15 years that showed the least moderate-to-high levels of self-esteem (76.4% and 71%, respectively) with no statistically significant difference. Private and public school students showed no statistical difference in self-esteem (27.6% and 23.9%, respectively). Secondary school students showed greater levels of low self-esteem than high school students (28.2% and 24.4%, respectively) with no statistical difference.
Relationship between self-esteem, malocclusion treatment needs, and type of malocclusion
Table 2 illustrates that 31.6% of the cases with an extreme need for treatment showed low self-esteem levels when compared with cases with a mild need for treatment (24.7%) with no statistically significant difference.
Table 2.
Correlations between self-esteem level, the index of treatment need, and type of malocclusion
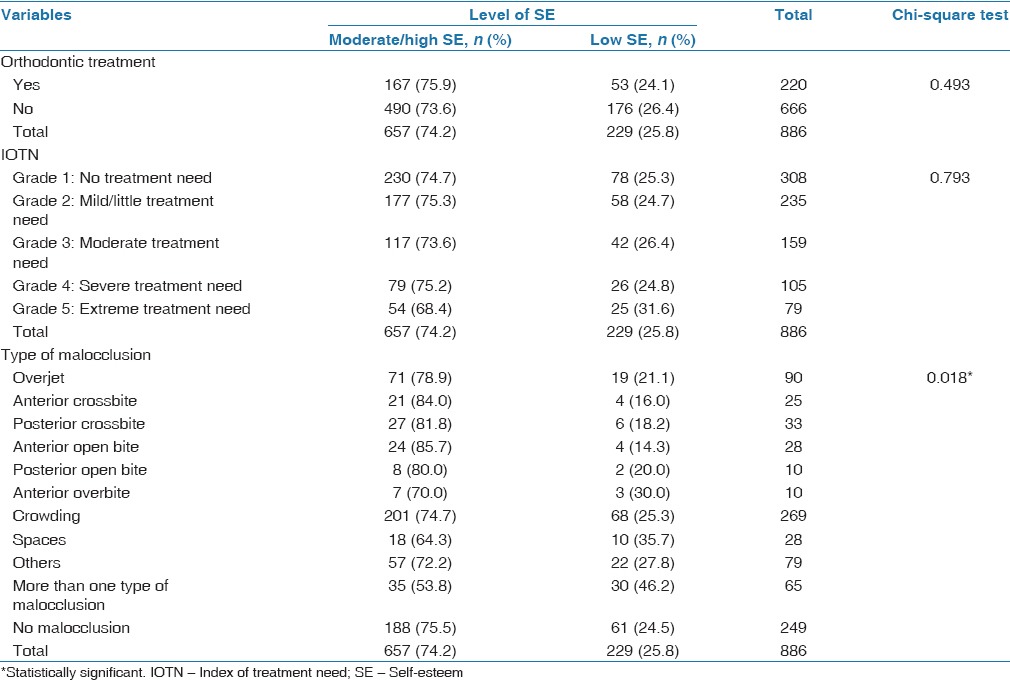
When levels of self-esteem were compared among different types of malocclusion, 46.2% of cases with multiple malocclusions showed significantly lower self-esteem (P = 0.018) when compared with single-category malocclusion. Spacing of the anterior teeth, crowding, and overjet malocclusions showed the highest percentages of low self-esteem levels (35.7%, 25.3%, and 21.1%, respectively) in Chi-square tests. Orthodontically treated students showed a slight increase in self-esteem levels when compared with nonorthodontically treated students (75.9% and 73.6%, respectively) with no significant difference.
Discussion
The reliability of the questionnaire in the present study was 0.712 for the self-esteem scale; Bowling's recommendation for an acceptable alpha is between 0.7 and 0.9, indicating acceptable reliability of the questionnaire.[19]
In this study, we used the DHC of the IOTN; the validity of this index has been reported in the literature.[20] Hassan, who used the IOTN among participants seeking orthodontic treatment, concluded that the IOTN is a valid screening tool.[21] Bellot-Arcís et al. stated that “several authors agree that the IOTN-DHC measures the severity of malocclusion;”[7] Trivedi et al. also showed similar results.[22]
This study confirms the relationship between malocclusion and self-esteem, supporting the belief that the enhancement of dental esthetics will improve one's self-esteem, which is a major motivating factor for orthodontic treatment. These results are in agreement with those of other studies.[9,12,22,23,24,25,26,27,28]
Several studies have been reported on self-esteem and malocclusion in different societies and ethnic backgrounds in Caucasian,[26] Asian,[5] Hispanic,[7,9] and Mediterranean populations.[13,20,29] The above-mentioned studies are in agreement with the present study; we can conclude that, in this wide variety of cultural backgrounds and ethnic groups, malocclusion represents one important factor that affects quality of life through self-esteem.
One of the important findings of the present study is that male participants had significantly higher self-esteem than female participants, showing that sex is a factor in self-esteem.[4] Middle school students in Korea were examined clinically for anterior crowding and lip protrusion and evaluated about their self-esteem using Rosenberg's scale; the results showed that sex played an important role in the relationship between self-esteem and malocclusion. Boys showed no significant difference, whereas girls showed a harmful effect on their self-esteem.[5]
In the present study, 68.8% of the orthodontically treated participants were female, and this is in agreement with several other studies.[7,29,30] This might be because the Saudi Arabian society encourages females to pay more attention to their looks and esthetics. Nicodemo et al. also found similar results when they studied the effects of orthognathic surgery on self-esteem and concluded that females showed improved self-esteem levels after surgical correction.[31] The results of other studies did not differentiate between the sexes, suggesting that the psychosocial impact of dental esthetics was similar between the sexes.[9,13,26]
The present study did not show any significant relationship between self-esteem and school types. However, Eremie and Chikweru[32] found that private school students, both males and females, demonstrated high self-esteem, whereas public school students demonstrated low self-esteem. These conflicting results may be due to cultural differences.
Orthodontically treated students showed slightly higher self-esteem than nontreated students, but the difference was not statistically significant. Several studies showed that orthodontic treatment had a short-term positive impact on self-esteem.[16,23,33,34]
Even though there was no significant difference in self-esteem between participants with extreme and mild treatment needs in the present study, we noticed that participants with extreme needs showed a higher percentage of low self-esteem (31.6% and 24.7%, respectively). This is in agreement with the study by Kovalenko et al. from 2012 in which they investigated the psychological status and severity of facial deformity; their results showed that only patients with severe facial deformities showed a higher prevalence of psychological instability presented as introversion, anxiety, emotional instability, and unsociability.[35] In addition, participants with multiple malocclusions showed statistically significantly lower self-esteem than those with single-category malocclusion, which is in agreement with previous studies by Badran,[13] Bellot-Arcís et al.,[7] and Mandall et al.[36] It is logical to say that as malocclusion becomes more complicated, esthetics will be more greatly affected, and several functions such as phonetics, chewing, and lip closure are also affected; these will affect social interaction and self-esteem.
Several studies[9,37] showed that spacing of the anterior teeth had the most negative effect on self-esteem, while other studies showed that crowding had the same influence on self-esteem.[11,24,34,37] Shaw concluded in his study that adolescents notice maxillary anterior crowding more than lip protrusion or overjet.[8] Tessarollo et al.,[24] Sardenberg et al.,[9] and Bellot-Arcís et al.[7] confirmed the negative effect of increased overjet on self-esteem. In the present investigation, spacing, crowding, and increased overjet were common malocclusion traits among the participants, and all showed statistically significant negative effects on self-esteem when compared with other malocclusion traits.
On interpreting the results of the present study, it is important to highlight its limitations. The study had a cross-sectional design, which makes it difficult to determine the timing of the association between orthodontic treatment and self-esteem improvement. Another limitation is the difference in the sample size between orthodontically treated and nonorthodontically treated participants, who represented only 14% of the sample; therefore, these findings (the effect of orthodontic treatment on self-esteem) cannot be generalized and further study is needed. To evaluate the actual effects of orthodontic treatment, it is recommended that a cohort study should be performed both retrospectively and prospectively on patients who are to be treated orthodontically.
Conclusions
It was found that malocclusion has a negative effect on self-esteem
Sex and multiple malocclusions were found to be significant factors affecting self-esteem
Spacing, crowding, and overjet had the greatest effects on self-esteem. Thus, the assumption that these conditions could affect speech, profile, and oral hygiene might be correct; however, more investigation is needed
Orthodontists should keep in mind that spacing, crowding, and overjet affect the level of self-esteem more than other characteristics of malocclusion, thus cases with these conditions require immediate attention.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- 1.McKenna G, Lillywhite GR, Maini N. Patient preferences for dental clinical attire: A cross-sectional survey in a dental hospital. Br Dent J. 2007;203:681–5. doi: 10.1038/bdj.2007.1109. [DOI] [PubMed] [Google Scholar]
- 2.Brosky ME, Keefer OA, Hodges JS, Pesun IJ, Cook G. Patient perceptions of professionalism in dentistry. J Dent Educ. 2003;67:909–15. [PubMed] [Google Scholar]
- 3.Theunissen SC, Rieffe C, Netten AP, Briaire JJ, Soede W, Kouwenberg M, et al. Self-esteem in hearing-impaired children: The influence of communication, education, and audiological characteristics. PLoS One. 2014;9:e94521. doi: 10.1371/journal.pone.0094521. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Robins RW, Trzesniewski KH, Tracy JL, Gosling SD, Potter J. Global self-esteem across the life span. Psychol Aging. 2002;17:423–34. [PubMed] [Google Scholar]
- 5.Jung MH. Evaluation of the effects of malocclusion and orthodontic treatment on self-esteem in an adolescent population. Am J Orthod Dentofacial Orthop. 2010;138:160–6. doi: 10.1016/j.ajodo.2008.08.040. [DOI] [PubMed] [Google Scholar]
- 6.Scapini A, Feldens CA, Ardenghi TM, Kramer PF. Malocclusion impacts adolescents’ oral health-related quality of life. Angle Orthod. 2013;83:512–8. doi: 10.2319/062012-509.1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Bellot-Arcís C, Montiel-Company JM, Almerich-Silla JM. Psychosocial impact of malocclusion in Spanish adolescents. Korean J Orthod. 2013;43:193–200. doi: 10.4041/kjod.2013.43.4.193. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Shaw BA, Liang J, Krause N. Age and race differences in the trajectories of self-esteem. Psychol Aging. 2010;25:84–94. doi: 10.1037/a0018242. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Sardenberg F, Martins MT, Bendo CB, Pordeus IA, Paiva SM, Auad SM, et al. Malocclusion and oral health-related quality of life in Brazilian school children. Angle Orthod. 2013;83:83–9. doi: 10.2319/010912-20.1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Kuzucu Y, Bontempo DE, Hofer SM, Stallings MC, Piccinin AM. Developmental change and time-specific variation in global and specific aspects of self-concept in adolescence and association with depressive symptoms. J Early Adolesc. 2014;34:638–66. doi: 10.1177/0272431613507498. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Jung MH. An evaluation of self-esteem and quality of life in orthodontic patients: Effects of crowding and protrusion. Angle Orthod. 2015;85:812–9. doi: 10.2319/091814.1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Vaida L, Pirte A, Corega C, Slavescu D, Mutiu G. Correlations between the changes in patients’ dental-facial morphology at the end of the orthodontic treatment and the psychological variables. Rom J Morphol Embryol. 2009;50:625–9. [PubMed] [Google Scholar]
- 13.Badran SA. The effect of malocclusion and self-perceived aesthetics on the self-esteem of a sample of Jordanian adolescents. Eur J Orthod. 2010;32:638–44. doi: 10.1093/ejo/cjq014. [DOI] [PubMed] [Google Scholar]
- 14.Perillo L, Esposito M, Caprioglio A, Attanasio S, Santini AC, Carotenuto M. Orthodontic treatment need for adolescents in the Campania region: The malocclusion impact on self-concept. Patient Prefer Adherence. 2014;8:353–9. doi: 10.2147/PPA.S58971. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Phillips C, Beal KN. Self-concept and the perception of facial appearance in children and adolescents seeking orthodontic treatment. Angle Orthod. 2009;79:12–6. doi: 10.2319/071307-328.1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Kiyak HA. Does orthodontic treatment affect patients’ quality of life? J Dent Educ. 2008;72:886–94. [PubMed] [Google Scholar]
- 17.Luhtanen R, Crocker J. A collective self-esteem scale: Self-evaluation of one's social identity. Pers Soc Psychol Bull. 1992;18:302–18. [Google Scholar]
- 18.Profit WR, Fields HW, David MS. Contemporary Orthodontics. Mosby. 5th edition. Elsevier; 2013. [Google Scholar]
- 19.Bowling A. Mc Graw Hill. 3rd edition. McGraw Hill: 2009. Research Methods in Health Investigating Health and Health Services. [Google Scholar]
- 20.Dawoodbhoy I, Delgado-Angulo EK, Bernabé E. Impact of malocclusion on the quality of life of Saudi children. Angle Orthod. 2013;83:1043–8. doi: 10.2319/012713-83.1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Hassan AH. Orthodontic treatment needs in the Western region of Saudi Arabia: A research report. Head Face Med. 2006;2:2. doi: 10.1186/1746-160X-2-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Trivedi K, Shyagali TR, Doshi J, Rajpara Y. Reliability of aesthetic component of IOTN in the assessment of subjective orthodontic treatment need. J Adv Dent Res. 2011;II:59–65. [Google Scholar]
- 23.Gazit-Rappaport T, Haisraeli-Shalish M, Gazit E. Psychosocial reward of orthodontic treatment in adult patients. Eur J Orthod. 2010;32:441–6. doi: 10.1093/ejo/cjp144. [DOI] [PubMed] [Google Scholar]
- 24.Tessarollo FR, Feldens CA, Closs LQ. The impact of malocclusion on adolescents’ dissatisfaction with dental appearance and oral functions. Angle Orthod. 2012;82:403–9. doi: 10.2319/031911-195.1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Zhou Y, Wang Y, Wang X, Volière G, Hu R. The impact of orthodontic treatment on the quality of life a systematic review. BMC Oral Health. 2014;14:66. doi: 10.1186/1472-6831-14-66. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Klages U, Claus N, Wehrbein H, Zentner A. Development of a questionnaire for assessment of the psychosocial impact of dental aesthetics in young adults. Eur J Orthod. 2006;28:103–11. doi: 10.1093/ejo/cji083. [DOI] [PubMed] [Google Scholar]
- 27.Azuma S, Kohzuki M, Saeki S, Tajima M, Igarashi K, Sugawara J. Beneficial effects of orthodontic treatment on quality of life in patients with malocclusion. Tohoku J Exp Med. 2008;214:39–50. doi: 10.1620/tjem.214.39. [DOI] [PubMed] [Google Scholar]
- 28.Peres SH, Goya S, Cortellazzi KL, Ambrosano GM, Meneghim Mde C, Pereira AC. Self-perception and malocclusion and their relation to oral appearance and function. Cien Saude Colet. 2011;16:4059–66. doi: 10.1590/s1413-81232011001100011. [DOI] [PubMed] [Google Scholar]
- 29.Abu Alhaija ES, Al-Nimri KS, Al-Khateeb SN. Self-perception of malocclusion among North Jordanian school children. Eur J Orthod. 2005;27:292–5. doi: 10.1093/ejo/cjh094. [DOI] [PubMed] [Google Scholar]
- 30.de Oliveira CM, Sheiham A. Orthodontic treatment and its impact on oral health-related quality of life in Brazilian adolescents. J Orthod. 2004;31:20–7. doi: 10.1179/146531204225011364. [DOI] [PubMed] [Google Scholar]
- 31.Nicodemo D, Pereira MD, Ferreira LM. Self-esteem and depression in patients presenting angle class III malocclusion submitted for orthognathic surgery. Med Oral Patol Oral Cir Bucal. 2008;13:E48–51. [PubMed] [Google Scholar]
- 32.Eremie MD, Chikweru AE. Self esteem among private and public secondary schools students in Rivers State: Implications for counseling. Arabian J Bus Manag Rev. 2015;5:1–4. [Google Scholar]
- 33.Claudino D, Traebert J. Malocclusion, dental aesthetic self-perception and quality of life in a 18 to 21 year-old population: A cross section study. BMC Oral Health. 2013;13:3. doi: 10.1186/1472-6831-13-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Jung MH, Heo W, Baek S. Effects of malocclusion on the self-esteem of female university students. Korean J Orthod. 2008;38:388–96. [Google Scholar]
- 35.Kovalenko A, Slabkovskaya A, Drobysheva N, Persin L, Drobyshev A, Maddalone M. The association between the psychological status and the severity of facial deformity in orthognathic patients. Angle Orthod. 2012;82:396–402. doi: 10.2319/060211-363.1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Mandall NA, McCord JF, Blinkhorn AS, Worthington HV, O’Brein KD. Perceived aesthetic impact of malocclusion and oral self-perceptions in 14-15- year-old Asian and Caucasian children in greater Manchester. Eur J Orthod. 1999;21:175–83. doi: 10.1093/ejo/22.2.175. [DOI] [PubMed] [Google Scholar]
- 37.Bernabé E, Sheiham A, Tsakos G, Messias de Oliveira C. The impact of orthodontic treatment on the quality of life in adolescents: A case-control study. Eur J Orthod. 2008;30:515–20. doi: 10.1093/ejo/cjn026. [DOI] [PubMed] [Google Scholar]