

Abstract
OBJECTIVES:
This retrospective study aimed to evaluate the dentoalveolar, skeletal, and soft tissue effects obtained with bone-anchored pendulum appliance in patients with Class II malocclusion.
MATERIALS AND METHODS:
A total of 18 patients (4 male, 14 female) at a mean pretreatment age of 14.0 years (+1.08) were enrolled in this study. All patients were treated with the bone-anchored pendulum appliance for an average duration of 4.8 months. Only the active distalization period was evaluated with predistalization and postdistalization lateral cephalograms. Skeletal, dentoalveolar, and soft tissue variables were obtained. Based on these variables, the treatment effects were evaluated with dependent t-test.
RESULTS:
Correction of Class II molar relationship resulted from distal movement of 3.45 mm and tipping of 11.24° of the first maxillary molars. The premolars were distalized accompanying the molars.
CONCLUSIONS:
The bone-anchored pendulum appliance proved to be an effective method for distalization of maxillary molars in cases that require maximum anchorage, avoiding reciprocal mesial movement of premolars and incisors.
Keywords: Angle Class II, malocclusion, orthodontic anchorage procedures, orthodontic appliance design
Introduction
Depending on the anteroposterior discrepancy severity, there are many resources to treat nonextraction Class II malocclusions. An option is molar distalization; however, this alternative often requires patient compliance to achieve successful results, which may compromise the treatment. To eliminate patient compliance requirements, several intraoral distalizing devices have been developed, such as the jones jig distalizar,[1] repelling magnets distalizers,[2] the pendulum appliance,[3] and its variation.[4]
The pendulum appliance designed by Hilgers has been widely researched and partially satisfies the requirements of an ideal device for maxillary molars distalization.[5,6,7,8,9] The original design was modified incorporating telescopic tubes and removable springs to provide greater patient convenience and produce more controlled distal movements.
The conventional pendulum appliance is anchored on the palate and premolars to produce distal movement of the maxillary molars. However, this type of anchorage also produces unfavorable side effects such as mesial movement of canines and premolars and incisors protrusion. This implies that the space obtained between the first molar and second premolar results in 55–70% distal molar movement and leads to 30–45% of anchorage loss.[5,7,10]
To minimize unfavorable side effects, a modified bone-anchored pendulum appliance with removable springs was developed. Therefore, the objective of this study is to evaluate the dentoalveolar, skeletal, and soft tissue effects resulting from molar distalization with the bone-anchored pendulum appliance.
Materials and Methods
This study was approved by the Ethics in Research Committee of University City of São Paulo, São Paulo, Brazil. (Protocol PP – 13646743) and was conducted in accordance with the Declaration of Helsinki (1964). All participants signed an informed consent.
The sample size was calculated based on an alpha significance level of 0.05 and a beta of 0.2 to achieve 80% power to detect a mean difference of 2 mm in molar relationship change between the pre- and posttreatment stages, with a 2.27 mm of estimated standard deviation.[11] The sample size calculation showed that 12 patients were needed, and to increase the power even more it was decided to increase the sample to 20 patients. Two patients were excluded from the sample due to appliance loss by peri-implantitis.
Therefore, the final sample consisted of 18 patients (14 females, 4 males), with an initial mean age of 14.0 years (SD: 1.08), who were prospectively treated at the Department of Orthodontics at University City of São Paulo, São Paulo, Brazil. The criteria for sample selection were: good oral hygiene, complete permanent dentition with the second molars erupted or partially erupted, permanent molar relationship of at least ½ or edge-to-edge Class II, absence or a minimum crowding in the mandibular arch, horizontal or balanced facial growth pattern in cephalometric analysis, and no previous orthodontic treatment. The group received intraoral molar distalization before fixed appliances treatment. Two serial cephalograms for each patient were obtained at the beginning of the treatment (T0) and at the end of the distalization (T1). All patients and parents were informed about the surgical procedure to install the orthodontic implants and were asked to sign a consent form.
Appliance construction and activation
Initially, bands with triple buccal and palatal tubes were adapted on the maxillary first molars. After predrilling of 6 mm depth made with 2 mm diameter drill, bilateral titanium screws of 2.4 mm diameter and 14 mm length were inserted into the palate, 6 to 9 mm posteriorly to the incisive foramen and 3 to 6 mm distant from the paramedian suture. The screw heads had an exposure of 8 mm in the oral cavity, which was enclosed by the Nance button.
Sequentially, the Nance buttons were constructed on duplicate dental casts, with spaces matching the implants inserted into the palate. The Nance buttons contained two stainless steel telescopic tubes (Morelli Ortodontia, Sorocaba, São Paulo, Brazil) of 12 mm in length and 0.9 mm imbedded internal diameter [Figure 1].
Figure 1.
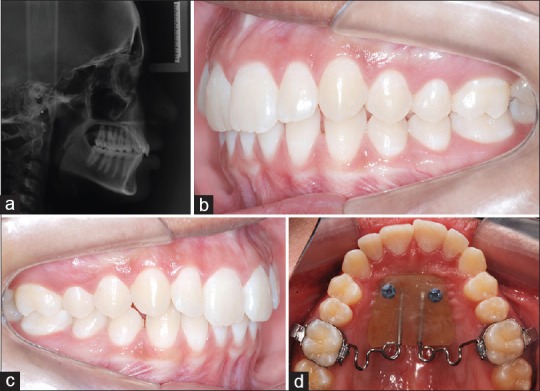
Pretreatment lateral cephalometric radiograph (a) and photographs (b-d) of a patient with the bone-anchored pendulum appliance
Two 0.032-inch titanium molybdenum distalizing removable springs were constructed to fit into the telescopic tubes. These springs were preactivated by a slight bend in the helicoid (250 gf), keeping them parallel to the suture,[3] with an antibending inclination of 15° to minimize palatal molar movement,[7] and had a simple vertical loop bend that could be activated to avoid posterior crossbite [Figure 1].[8] Patients were monitored monthly, but only the first activation was maintained during the active treatment period. The first molars were distally moved until overcorrection of 2 mm in molar relationship was achieved [Figures 2 and 3]. At every appointment, the soft tissues around the Nance button were checked for compression of the palatal mucosa and local inflammation. After molar distalization (4–6 months), the pendulum and screws were removed and a conventional Nance button was installed as anchorage to resume treatment. When necessary, anchorage reinforcement was achieved with cervical headgear with the outer bows tilted 15–20° upward from the occlusal plane, exerting 400–500 g of force with an average wear of 10–12 hours per day or with Class II elastics.
Figure 2.
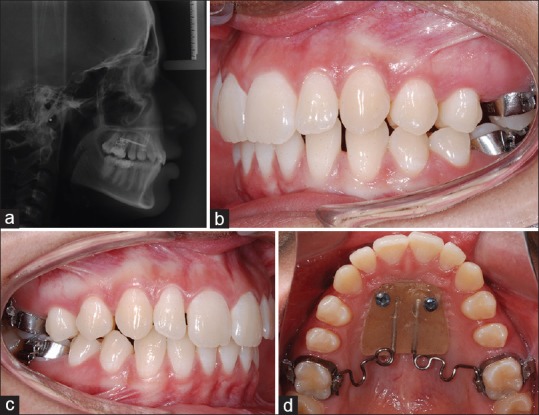
Post-distalization lateral cephalometric radiograph (a) and photographs (b-d) of a patient with the bone-anchored pendulum appliance
Figure 3.

Occlusal photograph after removal of the bone-anchored pendulum appliance
Cephalometric analysis
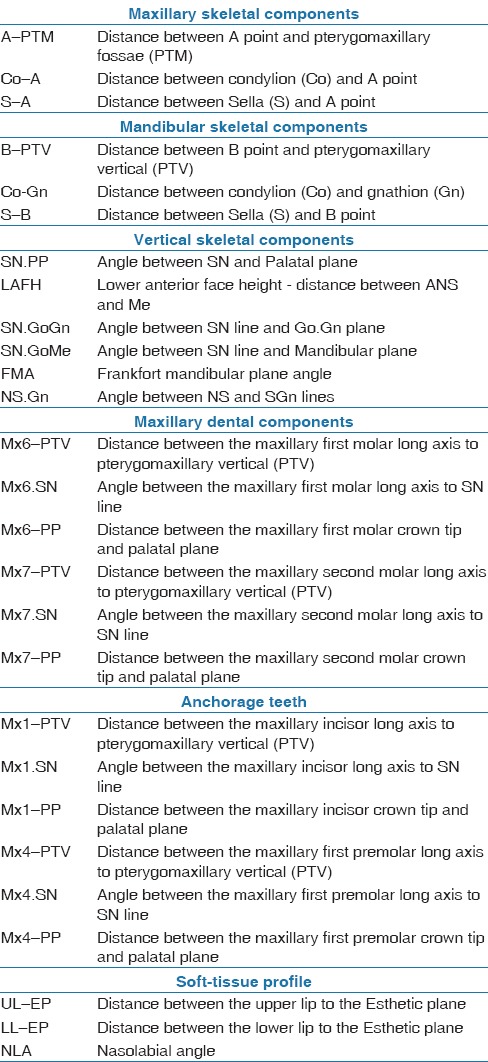
Lateral cephalograms obtained at T0 and T1 were digitized and had the landmarks identified by a single operator in the software Dolphin Imaging 11.5 (Dolphin Imaging and Management Solutions, Chatsworth, California, EUA). The software automatically corrected 10% radiographic magnification of the headfilms and performed the measurements of the variables described in Table 1.
Table 1.
Definition of cephalometric variables evaluated
Error study
Nine radiographs, representing 50% of the sample, were randomly selected, had the landmarks identified again, and were remeasured by the same examiner. The random errors were calculated using the Dahlberg's formula (Se2= Σd2/2n). Se2 was the error variance and d was the difference between two determinations of the same variable. The systematic errors were evaluated with dependent t-test at P < 0.05.
Statistical analyses
Normal distribution of variables was evaluated by Kolmogorov–Smirnov tests, which demonstrated that all variables had a normal distribution.
Descriptive statistics were performed for all cephalometric variables at T0 and T1. Intragroup comparison of the treatment changes was performed with dependent t-test. Results were considered significant at P < 0.05. All statistical analyses were performed using SPSS® Statistics for Mac, version 21.0 (IBM Corporation – Armonk, NY).
Results
The random errors ranged from 0.25 (overbite) to 5.39 (Mx7. Sn), and most variables had errors below 1 degree or millimeter. No systematic errors were detected.
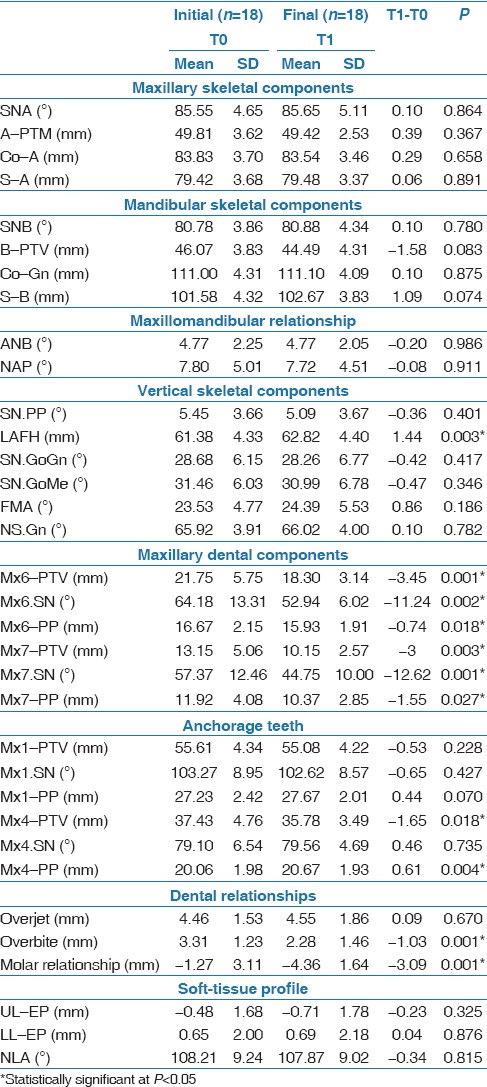
There was significant increase in lower anterior face height of 1.44 mm, significant distalization of 3.45 mm and 3 mm, distal tipping of 11.24° and 12.62°, and intrusion of 0.74 mm and 1.55 mm of the first and second maxillary molars, respectively. The first premolars had significant distalization of 1.45 mm and extrusion of 0.61 mm. Overbite significantly decreased in 1.03 mm and molar relationship was significantly improved in 3.09 mm [Table 2].
Table 2.
Treatment changes (dependent t-test)
Discussion
The use of only two calibrated operators to treat 18 patients reduces the variability that could have been introduced by several operators. The strict inclusion criteria and treatment protocol resulted in a small sample size, which is greater than most used in similar studies,[11,12,13,14] except one.[4] This research did not present an untreated control group for comparison and evaluation of the growth effect on the results. On the other hand, studies that evaluated pendulum appliance effects usually do not use a control group because the observation period is too short (4.8 months in this study) to observe normal growth changes to play a significant role.[5,6,7,10]
Bone-anchored pendulum appliance
Bilateral titanium screws were inserted into the palate 6–9 mm posteriorly to the incisive foramen and 3–6 mm paramedian to the suture according to a previous study.[15] Another important investigation confirmed that the thickest bone can be found in the anterior part of the palate, at the suture and paramedian areas, 4–8 mm distant from the incisive foramen.[16] Thus, the location chosen for screw insertion is in accordance with the available literature data.
In this study, wider and longer screws than those commonly used on the midpalatal region for BAPA were purposely chosen for different reasons.[4,11,12,13,14] First, because they should be sufficiently exposed in the mouth to be encompassed by the Nance button. Second, because miniscrews do not remain static when undergoing orthodontic forces. Miniscrews (6 mm length × 2 mm diameter) in the midpalatal raphe moved 0.49 mm or less, on average, but some moved more than 1 mm when under 250 gf.[17] Even longer screws (11 mm length × 2 mm diameter) installed in the zygomatic region moved 0.4 mm on average, but up to 1.5 mm movements were detected after application of 400 gf.[18] In these investigations, screw displacement little influenced orthodontic treatment. However, with BAPA, contrary to the literature,[14] miniscrew displacement leads to palatal mucosa compression, which may cause injury and inflammation.[11] Finally, it is important to install the screws before the pendulum. For this, the acrylic buttons were made with windows for the screws. Later, acrylic resin was added to attach the screw head to the button. This procedure avoided pressure against the palatal mucosa during miniscrew installation. Thus, to minimize screw displacement after force application and consequent palatal compression, longer and wider screws were chosen. Figure 3 shows that this precaution had positive results with minimal palatal compression, as seen in all patients.
Skeletal components
Overall, there were no statistically significant changes on the maxillary and mandibular sagittal skeletal components because maxilla and mandible remained stable, corroborating other studies that evaluated the pendulum appliance effects with conventional and skeletal anchorages.[6,7,8,13] On the other hand, LAFH significantly increased during treatment probably because of the clockwise mandibular rotation caused by maxillary molar distalization, which agrees with previous studies.[3,5,8]
Dental components
The significant reduction in the Mx6-PTV variable revealed that the maxillary first and second molars had a significant distalization movement (−3.45 mm), greater than that observed in other studies with conventional or bone anchorage,[6,7,8] but smaller than others.[5,9,10] Such differences may occur due to different needs of molar distalization between samples. This distalization was achieved with distal tipping (−11.24o) of the first maxillary molar, as revealed by the great reduction in the Mx6.SN variable, which was similarly observed in other studies.[3,5,7,8,10] However, most previous studies did not separately present the changes in distal tipping of the first and second molars, except in the study of Fuziy et al.,[8] which reported greater distal second molar tipping. This is expected because the intraoral distalizer appliances forces act on the dental crowns at a distance from the center of resistance of the molars. The maxillary molars also experienced intrusion of the distal and extrusion of the mesial occlusal surface, which is normally due to the distal tipping experienced by these teeth.[5,7,8] The extrusion of the mesial occlusal surface causes an increase in LAFH.
The maxillary incisors remained in the initial position without significant changes, similar to other studies.[4,11] This shows that bone-anchorage is an excellent option to avoid reciprocal unwanted movements in the incisors, described in other studies using conventional dental anchorage devices.[5,6,8,9,19]
There was significant distal movement of the first premolars [Table 2]. These were spontaneously obtained, without force application, as a result of the transseptal periodontal fibers action.[13] This conflicts with the side effects of mesial movement of the premolars, when conventional Pendulum is used[5,6,8,9] demonstrating that the use of skeletal anchorage with the Pendulum appliance can control this collateral effect.[13,14] Despite the spontaneous distalization and distal tipping, the premolars had also some extrusion, reported in other studies.[7,8] Probably premolar extrusion is consequent to the extrusion of the mesial surface of the first molars through the transseptal fibers action.
There was no significant overjet changes, the overbite significantly decreased, and molar relationship was significantly improved. These results contrast with other studies with conventional pendulum appliances that observed overjet increase.[5,6,8,9,10] This shows that anchorage reinforcement with a Nance button is not enough to resist the reciprocal mesial force during molar distalization, leading to anchorage loss.[13,14,20]
Decrease in overbite was consequent to mesial occlusal surface extrusion of the maxillary molars, as previously discussed, and that may usually occur during distalization. Molar relationship evidently improved with distalization of the molars and is the primary effect to be expected with this type of treatment.[3,5,6,8,10] This has already been shown by the studies with intraoral distalizers.[1,3,4]
Soft tissue profile
There were no significant changes in upper and lower lips, which implies that the position of the maxillary incisors was not affected by the treatment, agreeing with one study and differing with another, in which the NLA decreased due to anchorage loss.[4,5]
Conclusions
The results of this study showed that the bone-anchored pendulum appliance was effective as anchorage, producing:
Distal movement of maxillary molars;
Spontaneous distal movement of the maxillary first premolars;
No undesirable side effects in the maxillary incisors and lips;
Establishment of a Class I molar relationship.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- 1.Jones RD, White JM. Rapid Class II molar correction with an open-coil jig. J Clin Orthod. 1992;26:661–4. [PubMed] [Google Scholar]
- 2.Gianelly AA, Vaitas AS, Thomas WM, Berger DG. Distalization of molars with repelling magnets. J Clin Orthod. 1988;22:40–4. [PubMed] [Google Scholar]
- 3.Hilgers JJ. The pendulum appliance for Class II non-compliance therapy. J Clin Orthod. 1992;26:706–14. [PubMed] [Google Scholar]
- 4.Polat-Ozsoy O, Kircelli BH, Arman-Ozcirpici A, Pektas ZO, Uckan S. Pendulum appliances with 2 anchorage designs: Conventional anchorage vs bone anchorage. Am J Orthod Dentofacial Orthop. 2008;133:339.e9–17. doi: 10.1016/j.ajodo.2007.10.002. [DOI] [PubMed] [Google Scholar]
- 5.Bussick TJ, McNamara JA., Jr Dentoalveolar and skeletal changes associated with the pendulum appliance. Am J Orthod Dentofacial Orthop. 2000;117:333–43. doi: 10.1016/s0889-5406(00)70238-1. [DOI] [PubMed] [Google Scholar]
- 6.Byloff FK, Darendeliler MA. Distal molar movement using the pendulum appliance. Part 1: Clinical and radiological evaluation. Angle Orthod. 1997;67:249–60. doi: 10.1043/0003-3219(1997)067<0249:DMMUTP>2.3.CO;2. [DOI] [PubMed] [Google Scholar]
- 7.Byloff FK, Darendeliler MA, Clar E, Darendeliler A. Distal molar movement using the pendulum appliance. Part 2: The effects of maxillary molar root uprighting bends. Angle Orthod. 1997;67:261–70. doi: 10.1043/0003-3219(1997)067<0261:DMMUTP>2.3.CO;2. [DOI] [PubMed] [Google Scholar]
- 8.Fuziy A, Rodrigues de Almeida R, Janson G, Angelieri F, Pinzan A. Sagittal, vertical, and transverse changes consequent to maxillary molar distalization with the pendulum appliance. Am J Orthod Dentofacial Orthop. 2006;130:502–10. doi: 10.1016/j.ajodo.2004.12.031. [DOI] [PubMed] [Google Scholar]
- 9.Toroglu MS, Uzel I, Çam OU, Hancioglu ZB. Cephalometric evaluation of the effects of pendulum appliance on various vertical growth patterns and of the changes during short-term stabilization. Clin Orthod Res. 2001;4:15–27. doi: 10.1034/j.1600-0544.2001.040103.x. [DOI] [PubMed] [Google Scholar]
- 10.Chaques-Asensi J, Kalra V. Effects of the pendulum appliance on the dentofacial complex. J Clin Orthod. 2001;35:254–7. [PubMed] [Google Scholar]
- 11.Escobar SA, Tellez PA, Moncada CA, Villegas CA, Latorre CM, Oberti G. Distalization of maxillary molars with the bone-supported pendulum: A clinical study. Am J Orthod Dentofacial Orthop. 2007;131:545–49. doi: 10.1016/j.ajodo.2006.08.012. [DOI] [PubMed] [Google Scholar]
- 12.Kaya B, Sar C, Arman-Ozcirpici A, Polat-Ozsoy O. Palatal implant versus zygoma plate anchorage for distalization of maxillary posterior teeth. Eur J Orthod. 2013;35:507–14. doi: 10.1093/ejo/cjs059. [DOI] [PubMed] [Google Scholar]
- 13.Sar C, Kaya B, Ozsoy O, Ozcirpici AA. Comparison of two implant-supported molar distalization systems. Angle Orthod. 2013;83:460–7. doi: 10.2319/080512-630.1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Kircelli BH, Pektas ZO, Kircelli C. Maxillary molar distalization with a bone-anchored pendulum appliance. Angle Orthod. 2006;76:650–9. doi: 10.1043/0003-3219(2006)076[0650:MMDWAB]2.0.CO;2. [DOI] [PubMed] [Google Scholar]
- 15.Bernhart T, Vollgruber A, Gahleitner A, Dortbudak O, Haas R. Alternative to the median region of the palate for placement of an orthodontic implant. Clin Oral Implants Res. 2000;11:595–601. doi: 10.1034/j.1600-0501.2000.011006595.x. [DOI] [PubMed] [Google Scholar]
- 16.Gracco A, Lombardo L, Cozzani M, Siciliani G. Quantitative cone-beam computed tomography evaluation of palatal bone thickness for orthodontic miniscrew placement. Am J Orthod Dentofacial Orthop. 2008;134:361–9. doi: 10.1016/j.ajodo.2007.01.027. [DOI] [PubMed] [Google Scholar]
- 17.Alves M, Jr, Baratieri C, Nojima LI. Assessment of mini-implant displacement using cone beam computed tomography. Clin Oral Implants Res. 2011;22:1151–6. doi: 10.1111/j.1600-0501.2010.02092.x. [DOI] [PubMed] [Google Scholar]
- 18.Liou EJ, Pai BC, Lin JC. Do miniscrews remain stationary under orthodontic forces? Am J Orthod Dentofacial Orthop. 2004;126:42–7. doi: 10.1016/j.ajodo.2003.06.018. [DOI] [PubMed] [Google Scholar]
- 19.Al Thomali Y, Basha S, Mohamed RN. Pendulum and modified pendulum appliances for maxillary molar distalization in Class II malocclusion - a systematic review. Acta Odontol Scand. 2017 doi: 10.1080/00016357.2017.1324636. [Epub ahead of print] [DOI] [PubMed] [Google Scholar]
- 20.Marure PS, Patil RU, Reddy S, Prakash A, Kshetrimayum N, Shukla R. The effectiveness of pendulum, K-loop, and distal jet distalization techniques in growing children and its effects on anchor unit: A comparative study. J Indian Soc Pedod Prev Dent. 2016;34:331–40. doi: 10.4103/0970-4388.191411. [DOI] [PubMed] [Google Scholar]