

Abstract
Objective:
The purpose of this study was to provide a best-synthesis summary of the literature for effective workplace health promotion interventions (WHPI) for work-related mechanical neck pain (MNP) and to determine the congruence between knowledge of WHPI for work-related MNP and coverage of MNP in the chiropractic postgraduate program at Macquarie University.
Methods:
A literature review was undertaken to determine effective WHPI for work-related MNP. We searched Cochrane Library, PubMed, EMBASE, CINAHL, and PEDro (from 1991 to 2016) for systematic reviews and meta-analyses. The PRISMA (2009) 27-item checklist was used to critically appraise included articles. Lectures, tutorials, and assessment tasks within the chiropractic postgraduate program were mapped to the literature review findings and analyzed.
Results:
There was moderate-quality evidence for multidimensional WHPI, including aspects of mental and physical functioning, activity performance and modifications, and environmental modifications, to reduce MNP and disability in workers, particularly in the long term. Education on coverage of MNP and effective WHPI for MNP was inadequately covered although congruent with synthesis of current literature. Education on body functions and structures and personal factors were the most commonly covered components.
Conclusion:
Multidimensional WHPI, focusing on physical, mental, and environmental modifications, appear to reduce self-reported MNP primarily in office workers. There is adequate congruence between the chiropractic postgraduate program at Macquarie University and the published literature on some WHPI. However, there is inadequate coverage on aspects of MNP and effective WHPI for MNP, particularly those focusing on activity and participation and environmental factors.
Key Indexing Terms: Chiropractic, Curriculum, Educational Measurement, Neck Pain, Workplace
INTRODUCTION
Mechanical neck pain (MNP) is broadly defined as pain experienced in the posterior neck or shoulders, caused by abnormal stress and strain on cervical musculoskeletal structures in the absence of serious pathology (e.g., radiculopathy, tumor, fracture, infection, etc.).1–3 The etiology of MNP is multidimensional and poorly understood.4–6 Because of this complexity, the impact of different risk factors in the pathogenesis and exacerbation of MNP is difficult to explain,3 and it is unlikely that a single pathophysiological mechanism is responsible for tissue damage alone.7 MNP is a highly prevalence and burdensome musculoskeletal disorder (MSD), accounting for much of workplace disability and absenteeism.5,8 Global MNP figures are predicted to account for the next largest number of years lived with disability when compared to other MSDs.9
Workplace Interventions
Workplace health promotion interventions (WHPI) are defined as interventions to prevent, minimize, and eliminate workplace health hazards and aim to maintain and promote quality work ability.10,11 The increase in health care costs and awareness of work performance losses are driving the need for effective WHPI.12 However, WHPI are challenging to implement because of the multifactorial nature of work-related disability, and they have evolved considerably over the past 2 decades.13,14 Such complex processes often require complex interventions, and thus there is a need for evidence from examining multicomponent interventions and a standardized framework in which to classify and categorize interventions.5
In 2001, the World Health Organization (WHO) approved the international classification of functioning, disability, and health (ICF).15 The ICF and the International Classification of Diseases (ICD-10) form the 2 core classification systems of the WHO, where diseases, disorders, and disabilities are included.15 The ICF and ICD-10 provide reliable and comparable data with standardized frameworks and classifications, providing information on determining the overall health of populations and the prevalence and incidence of nonfatal health outcomes and measuring health care needs and the performance and effectiveness of health care systems. The ICF components can be used to provide a framework that groups WHPI into 4 main categories of interventions targeting: (1) mental body functions and mental health education, (2) musculoskeletal body functions and physical education and relaxation breaks, (3) modification of activity performance, and (4) physical modification of activity performance. The framework provides a sound method of arranging WHPI based on the ICF components.15
Curriculum Mapping
Curriculum maps (CM) are instruments used to display how and when content is taught and which measurement outcomes can be used to determine the successful delivery of information.16 CM accurately arrange every aspect of the curriculum in a logical and transparent manner, making them useful tools for academics and students.16 CM have evolved considerably since the 1980s: earlier concepts included time lines and scheduling of content taught within the curriculum and review of material taught and examination of content.17 Today, data are collected electronically and used to create CM.17–19
CM are dynamic and time-consuming processes that require ongoing feedback and evaluation from academics and students. However, CM are extremely useful because they assist academics in ensuring that course content and assessment tasks accurately reflect the curriculum while also allowing students to identify the learning outcomes required for the successful completion of the program. With respect to continuing professional development at Macquarie University (MU), Sydney, Australia, this ensures that all graduating students meet the mandatory professional requirements and capabilities to practice safely and effectively.20–24 While there is extensive literature on CM within medicine,25–28 there appears to be substantially less literature available for chiropractic curricula.16,29,30 As primary health care providers, it is imperative for both medical and chiropractic academics to continue to critically appraise the ability of their programs to adequately prepare graduates with the required clinical skills and knowledge to practice safely and effectively.
A review by Gorrell et al29 examined commonly presenting complaints to chiropractors and MSD for which there is published evidence that chiropractic treatment is effective and mapped the assessment tasks of the chiropractic postgraduate program at MU. The review adopted concepts from (1) the 2011 Health and Workforce Australia Simulated Learning Environment Chiropractic Curriculum Report, compiled by the School of Chiropractic and Health Sciences at Murdoch University in Australia,31 and (2) prescriptive and descriptive models of CM proposed by Prideaux.19 The review concluded that there was congruence between the chiropractic postgraduate program at MU and the 2 domains against which it was mapped: MSD commonly treated by chiropractors and MSD for which there is evidence that chiropractic treatment is effective.29 The methodological strategy used in the review has been effectively rationalized and provides sound justification for use in this review.
The purpose of this review was to (1) review the literature for effective WHPI for work-related MNP and (2) map the syllabus of the chiropractic postgraduate program at MU to these effective WHPI and the aspects of MNP.
METHODS
Literature Search
To investigate CM, 2 authors independently searched the Education Resources Information Center (ERIC) and A+ Education databases using the MU Library Web portal on June 4, 2016. Reference lists from identified articles were also hand searched for articles not returned in the initial search. See Appendix A for search strategy. To investigate WHPI for work-related MNP, 2 authors independently searched the Cochrane Library, PubMed, EMBASE, CINAHL, and PEDro using the MU Library Web portal on June 4, 2016, for peer-reviewed articles investigating effective WHPI for work-related MNP. See Appendices B to E for search strategies. Reference lists from identified articles were also hand searched for articles not returned in the initial search.
Study Selection and Eligibility Criteria
Inclusion criteria for the review investigating CM included full-text articles, English-language systematic reviews, and meta-analyses published from January 1, 2006, to June 4, 2016. Inclusion criteria for the review investigating effective WHPI for MNP included full-text articles, articles that focused on at least 1 or more of the 4 ICF main categories of intervention and were conducted in the workplace, English-language systematic reviews, and meta-analyses in which articles included participants with neck pain not due to a specific pathology (e.g., cervical radiculopathy, tumors, infections, fracture, etc.) and published from January 1, 2006, to June 4, 2016. Exclusion criteria for both reviews were abstract only, non–English language, and articles that were not systematic reviews or meta-analyses. There were no exclusion criteria for the hand search.
Initially, all abstracts and titles were independently reviewed and sorted based on the predefined inclusion criteria. The full text of the studies that match these criteria was then independently reviewed and once again sorted based on the predefined inclusion criteria. Both reviewers held a meeting to confirm the articles to be included in the review. Consensus was used to solve disagreements; if disagreements persisted, a third review author was consulted. Disagreements may have arisen when, for example, discussing whether the WHPI adopted in a paper could be appropriately categorized into the ICF framework. The search protocol is summarized in Figure 1.
Figure 1.
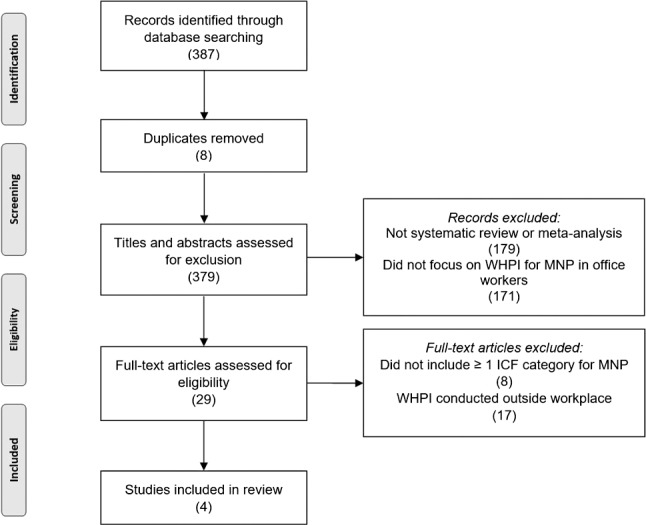
Flowchart of selection process.
Following this review, unit guides from each of the 16 2015–2016 chiropractic postgraduate program units were accessed through the MU website: http://unitguides.mq.edu.au (last accessed July 28, 2016). These unit outlines were both printed as a hard copy and saved to Google Drive (Google Inc., Santa Clara, CA). Portable document format files of the lecture slides and tutorial handbooks were accessed through individual consultation with chiropractic postgraduate program unit conveners. Qualitative mapping of the chiropractic postgraduate program lectures, tutorials, and assessment tasks were then completed via vertical and horizontal integration against the results from the included systematic reviews and meta-analyses. Inclusion criteria for the unit outlines included the final draft of all units studied within the 2015–2016 chiropractic postgraduate program. Criteria for exclusion were units not studied within the 2015–2016 chiropractic postgraduate program.
Analysis
To achieve an overview of the coverage of MNP and effective WHPI for MNP within the chiropractic postgraduate program, a summary map (Fig. 2) conceptualized by Gorrell et al29 was used. All aspects of MNP and WHPI, including but not limited to anatomy, physiology, pathophysiology, clinical manifestations, demographic characteristics, management strategies, diagnosis, and etiology, were considered as coverage of MNP and WHPI in the chiropractic postgraduate program. The ICF components were used to conceptualize a framework in which aspects of MNP and effective WHPI for MNP were grouped into 4 main categories.15 If a category was sufficiently covered in a unit, this was marked with an “X,” and if the category was not sufficiently covered, the box was left blank. Significant depth of coverage of a category within a unit was considered to have occurred if it was equivalent to a 1-hour lecture or tutorial or to an assessment task. If a unit within the chiropractic postgraduate program achieved an average of 3 X's, it was deemed to adequately address aspects of MNP or effective WHPI for MNP. If at least 8 or more of the 16 chiropractic postgraduate program units achieved 3 or more X's, it was deemed that overall the chiropractic postgraduate program adequately addressed aspects of MNP or effective WHPI for MNP.
Figure 2.

Process mapping for the 2-year master of chiropractic curriculum as conceptualized in the review by Gorrell et al.29
Following this, the unit outlines were hand searched for mapping the weighting of content vs skills acquisition for each of the assessment tasks (Fig. 3). Theory acquisition represents theory taught, whereas skills acquisition includes behaviors such as history taking, clinical decision making, or manual therapy skills. Specifically, assessment tasks were mapped, as it was assumed that important ICF categories within each unit would have appropriate representation. Further analysis of skills acquisition is beyond the scope of this article. Following this, each final examination was hand searched, and the corresponding spread of marks allocated to each of the 4 categories was subsequently mapped against individual units. The data obtained in this way were entered into a Microsoft Excel (Microsoft Corp, Redmond, WA) spreadsheet. Descriptive analysis was completed using tables and histograms enabling accurate and clearly defined mapping of the assessment tasks delivered within each of the chiropractic postgraduate program units to the ICF categories.
Figure 3.

Percentage of skills versus theory acquisition examined in assessment tasks. Numbers along the X-axis refer to the chiropractic postgraduate program units (873 and 874 = Neuromusculoskeletal Diagnosis 1 and 2; 891 and 892 = Clinical Chiropractic 1 and 2; 916 and 917 = Diagnostic Imaging 1 and 2; 918 and 919 = Physical/Functional Assessment and Clinical Management; 931 and 932 = Diagnosis and Management 1 and 2; 903 and 904 = Clinical Chiropractic 3 and 4; 921 and 922 = Topics in Chiropractic 1 and 2; 896 and 897 = Clinic Internship 1 and 2).
RESULTS
A comprehensive search of the literature for systematic reviews and meta-analyses on effective WHPI for MNP in office workers revealed 2 systematic reviews and 2 meta-analyses. The Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) 2009 27-item checklist32 was used to critically appraise the 4 included papers (Table 1).33–36
Table 1.
Critical Appraisal of the Included 4 Articles Examining Effective WHPI for MNP Using the PRISMA 2009 27-Item Checklist, With Number of Articles Synthesized and Summary of Effective WHPI in Each Article
|
Included articles |
PRISMA Score |
No. Articles |
Effective WHPI |
| Aas et al33 | 26/27 | 10 RCT | LQE: neither supports nor refutes benefits of any specific WHPI for MNP. |
| MQE: multidimensional WHPI (mental and physical health education, relaxation and breaks, activity and physical environment modifications) compared to no interventions reduces sickness absence in intermediate term. | |||
| Coury et al34 | 15/27 | 18 RCT | MQE: resistance exercises (dumbbells, isokinetic equipment, elastic bands, and exercises against gravity) are effective in controlling MNP. |
| MQE: light workplace training has no effect on reducing MNP. | |||
| SQE: long-term training (>10 weeks) is effective in reducing MNP. | |||
| Hoe et al35 | 26/27 | 13 RCT | MQE: use of arm support with alternative mouse may reduce the incidence of MNP. |
| MQE: incidence of MNP is not reduced when comparing alternative and conventional mouse with and without arm support. | |||
| VLQE-LQE: other ergonomic WHPI do not prevent work-related MNP (although limited by study paucity and heterogeneity). | |||
| Varatharajan et al36 | 22/27 | 5 RCT | MQE: adding computer-prompted exercise and work breaks to a combined WHPI approach (ergonomic adjustment and general education) improves self-reported MNP. |
| MQE: combined WHPI approach (postural exercises and a graded activity intervention) has same outcomes as fitness and strengthening exercises for MNP. |
Note: HQE (high-quality evidence); LQE (low-quality evidence); MNP (mechanical neck pain); MQE (moderate-quality evidence); PRISMA (preferred reporting items for systematic reviews and meta-analyses); RCT (randomized controlled trials); SQE (strong-quality evidence); VLQE (very-low-quality evidence); WHPI (workplace health promotion intervention).
The first meta-analysis, by Aas et al 2011,33 included 10 randomized controlled trials (RCTs) with a population of 2745 workers. The objective was to determine the effectiveness of WHPI in adult workers with neck pain. Two studies were rated as having low risk of bias, and 8 trials examined office workers specifically. The authors concluded that there was low-quality evidence across all included trials showing no significant differences between WHPI and no interventions for pain prevalence or pain severity. Furthermore, none of the significant results for pain, in favor of WHPI, were sustained across different follow-up times. A major limitation in this meta-analysis was the high level of heterogeneity across the included trials: significant heterogeneity in target groups, intervention, follow-ups, and outcome measures, which restricted pooling of data across the included studies.33 The results were inconclusive regarding the efficacy of any specific intervention; however, there is moderate evidence that multidimensional WHPI are effective in reducing absenteeism. However, the major strength of the meta-analysis was its comprehensive search strategy, use of ICF terminology to classify the intervention components, and inclusion of a variety of WHPI and outcome measures.33
The second meta-analysis, by Hoe et al 2012,35 included 13 RCTs with a population of 2397 workers. The objective was to assess the effects of WHPI for the prevention of work-related upper-limb and neck complaints in adults. One trial was rated as having low risk of bias, and 11 trials examined office workers specifically. Moderate-quality evidence suggests that the use of arm support with alternative mouse may reduce the incidence of neck and shoulder complaints but not for the right-upper-limb complaints.35 Furthermore, moderate-quality evidence suggests that the incidence of neck and shoulder and right-upper-limb complaints is not reduced when comparing alternative and conventional mouse with and without arm support. The limitations of this analysis were significant heterogeneity and lack of available trials that demonstrated high-quality evidence for WHPI for upper-limb and neck and shoulder complaints and lack of a standardized framework for classifying interventions and use of terminology. However, the strength of the meta-analysis was its comprehensive search strategy and inclusion of a variety of WHPI and outcome measures.35
The first systematic review, by Coury et al 2009,34 included 18 RCTs. The number of the study population was not reported on. The objective was to assess and provide evidence of the effectiveness of workplace exercise in controlling musculoskeletal pain. Six trials were rated as high quality, and 9 trials examined office workers specifically. Strong-quality evidence was found to support the effectiveness of physical exercise in controlling neck pain among workers who performed sedentary tasks in offices or administrative environments. Limitations of this review include lack of a standardized framework for classifying interventions and use of terminology, including trials that evaluated only physical-based interventions and therefore did not consider the multifactorial nature of work-related musculoskeletal complaints, and the inclusion of 13 low-quality trials.
The second systematic review, by Varatharajan et al 2014,36 included 16 RCTs with a population of 958 workers. The objective was to critically appraise and synthesize literature on the effectiveness of WHPI in workers with neck pain, whiplash-associated disorders, or upper-extremity disorders. Many of the included trials (69%) had poor internal validity with inadequate randomization, concealment or blinding methods, or differences between treatment arms at baseline, or they used outcome measures with poor validity or reliability. Evidence from a cluster of trials suggested that adding computer-prompted exercise and work breaks or work breaks alone to a combined WHPI approach improves recovery and reduces progression of work-related neck and upper-extremity pain. Limitations of this review include the lack of qualitative studies that explored work-related neck and upper-limb complaints, and thus the review could not comment on the values and experience of patients who have used WHPI. However, the review had many strengths, including a rigorous search of the literature, clear inclusion and exclusion criteria, standardization of the critical appraisal, and the use of evidence-based synthesis methods to minimize bias with using low-quality trials.
As shown in Table 2, overall there is inadequate coverage of aspects of MNP and effective WHPI for MNP in relation to the WHO's ICF components throughout the 2-year MU chiropractic postgraduate program. Seven of the 16 chiropractic postgraduate program units were deemed to adequately address aspects of MNP, and only 1 unit was deemed to adequately address effective WHPI for MNP. The units CHIR921 and CHIR922 (Topics in Chiropractic 1 and 2) do not directly cover aspects of MNP; rather, they cover aspects of research methodology, and over the course of the 2 semesters, students are expected to design and execute a primary or secondary research project to create new knowledge in a clinically relevant area. Similarly, the units CHIR896 and CHIR897 (Clinical Internship 1 and 2) make up students' yearlong chiropractic internship at MU. As such, it is expected that students will be exposed to cases or reports on aspects of MNP and therefore gain a clinical understanding of MNP and practical application of effective WHPI for MNP. However, this cannot be ascertained due to the unique nature of each student's clinical internship experience. For instance, chiropractic interns are assigned to 1 of 3 student clinics that manage varying demographics, depending on their location. The units CHIR931 and CHIR932 (Diagnosis and Management 1 and 2) comprise case studies, evidence-based practice, nutrition, pharmacology, and mental health, which may not directly cover MNP; however, they are critical for students to develop clinical reasoning skills by exposing them to the widest possible range of clinical scenarios that may be encountered in chiropractic practice.
Table 2.
Curriculum Mapping to (1) Coverage of MNP and (2) Effective WHPI for MNP According to the Included Papers Within the MU Chiropractic Postgraduate Program Using the World Health Organization's WHO's 4 International Classification of Functioning, Disability, and Health Components as a Conceptual Framework
|
Curriculum mapping to:a |
MChir Year 1 (2015) |
MChir Year 2 (2016) |
||||||||||||||
|
Semester 1 |
Semester 2 |
Semester 1 |
Semester 2 |
|||||||||||||
|
873 |
891 |
916 |
918 |
874 |
892 |
917 |
919 |
896 |
903 |
921 |
931 |
897 |
904 |
922 |
932 |
|
| (1) Coverage of MNP | ||||||||||||||||
| Body functions and structures | X | X | X | X | X | X | X | X | X | |||||||
| Activity and participation | X | X | X | X | X | X | X | |||||||||
| Environmental factors | ||||||||||||||||
| Personal factors | X | X | X | X | X | X | X | X | X | |||||||
| (2) Effective WHPI for MNPb | ||||||||||||||||
| Body functions and structures | X | X | X | |||||||||||||
| Activity and participation | X | |||||||||||||||
| Environmental factors | X | |||||||||||||||
| Personal factors | X | X | X | X | ||||||||||||
Note: MChir (master of chiropractic); MNP (mechanical neck pain); WHPI (workplace health promotion intervention). Class numbers indicate the following: 873/874 = Neuromusculoskeletal Diagnosis 1 and 2; 891/892/903/904 = Clinical Chiropractic 1, 2, 3, and 4; 916/917 = Diagnostic Imaging 1 and 2; 918 = Physical and Functioning Assessment; 919 = Clinical Management; 896/897 = Clinical Internship 1 and 2; 921/922 = Topics in Chiropractic 1 and 2; 931/932 = Diagnosis and Management 1 and 2.
MChir curriculum lectures, tutorials, and assessment tasks mapped to (1) and (2).
The analysis of the content vs skills acquisition data is presented in Figure 3 and shows a slight bias toward theory acquisition in 8 of the 16 chiropractic postgraduate program units. The exceptions were CHIR891/892 (Clinical Chiropractic 1 and 2), CHIR903/904 (Clinical Chiropractic 3 and 4), and CHIR896/897 (Clinic Internship 1 and 2). These units focus heavily on the practical application of skills acquisition and clinical decision making. Conversely, the units CHIR916/917 (Diagnostic Imaging 1 and 2), CHIR931/932 (Diagnosis and Management 1 and 2), and CHIR921/922 (Topics in Chiropractic 1 and 2) focus heavily on the mastery of theory, which is then applied to the relevant clinical scenario.
To further examine the distribution of content within the curriculum, chiropractic postgraduate program units CHIR919 (Clinical Management), CHIR903/904, and CHIR922 were mapped for congruence with the conclusions formed in the 4 included papers33–36 (Fig. 4). Many of the topics in the syllabus of CHIR919 and CHIR903/904 covered body functions and structures, particularly in lectures and assessments. Units CHIR919, CHIR903/904, and CHIR922 include topics concerning effective WHPI for MNP within their syllabi; however, it is inadequately covered, particularly with regard to activity and participation and environmental factors. CHIR919 is a theoretical-based, multidisciplinary unit incorporating aspects of mental health, pediatric and geriatric assessment, exercise science, and rehabilitation and neurodynamics, focusing primarily on the multimodal management of patients in clinical settings. Conversely, CHIR903/904 are primarily practical-based units that focus on skills acquisition and clinical decision making. As such, WHPI for MNP form a minor aspect in the scope of these multidisciplinary units. CHIR922 is a research unit that focuses primarily on research methodology and workplace health and safety (OHS). Activity and participation and environmental factors are covered, such as OHS solutions and chiropractic and OHS, but only in lectures and the final exanimation. CHIR922 tutorials were designed to give students an opportunity to present their research, and the entirety of the assessment was dedicated to the completion of a primary or secondary research paper.
Figure 4.

Mapping of the Macquarie University chiropractic postgraduate program units CHIR919 (A), CHIR903 (B), CHIR904 (C), and CHIR922 (D) coverage (%) to effective workplace health promotion interventions for work-related mechanical neck pain as reported by the included papers 33 to 36 using the World Health Organization's international classification of functioning, disability, and health components as a conceptual framework.
DISCUSSION
The results demonstrate that lectures, tutorials, and assessment tasks within the chiropractic postgraduate program are overall incongruent with coverage of MNP and effective WHPI for MNP as highlighted by the included 4 papers.33–36 Mapping of lectures, tutorials, and assessment tasks ensured that information captured was informative and enabled a comprehensive and detailed analysis of the chiropractic postgraduate program. It is important to note that there is some subjectivity in the data presented in Table 2 regarding whether the examination of MNP and effective WHIP for MNP were covered adequately within a unit to justify its inclusion in the analysis. The WHO's ICF provided a conceptual framework and categorization, which facilitated reducing this subjectivity.
A major limitation in this review is the exclusion of mapping the bachelor of chiropractic science curriculum (BCSC). The BCSC is the undergraduate degree that provides the prerequisite academic background enabling entry into the chiropractic postgraduate program and focuses on training students on a wide range of diagnostic skills in the context of anatomical, physiological, and biomedical sciences. It is likely that concepts of MNP and effective WHPI are covered in the BCSC; therefore, the findings of this review may not entirely reflect the acquisition of skills and theoretical knowledge of chiropractic postgraduate program graduates in relation to concepts in MNP and effective WHPI for MNP. The justification for omitting the BCSC from this review was simply due to constraints on time and resources.
The MU chiropractic postgraduate program focuses on preparing students with the full diagnostic and clinical management knowledge and skills required to graduate and work as chiropractors. A significant number of hours are dedicated to clinical internship and management. MNP and effective WHPI for MNP form a small aspect within what is taught in the MU chiropractic postgraduate program, and while these are pertinent socioeconomic issues, they are among many within the scope of chiropractic.
The exclusion of mapping the final theory examinations was another limitation in this review. Many of the chiropractic postgraduate program final theory examinations aim to examine the understanding of concepts using specific examples (e.g., low back pain) rather than simple recall and comprehension. However, inclusion of the final theory examinations for CM was not feasible due to time constraints. The final practical examinations include, for instance, chiropractic skills, neurological examination, rehabilitation tracks, and radiographic critique and positioning. These assessment tasks are simultaneously examining both mastery of skills and theoretical acquisition. The chiropractic postgraduate program is not merely a content-based degree, and students' exposure to particularly skills acquisition may vary dramatically. An obvious example of this is found within the CHIR896/897 (Clinical Internship 1 and 2) units, where students learn to implement theory and skills taught to actual clinical situations. It is expected that students will be exposed to a variety of clinical presentations that may include work-related MNP; however, the limitation to this assumption is the diverse experience and demographic spectrum to which interns are exposed.
Another limitation of this review was its limited generalizability since it mapped the curriculum from only a single institution. The findings of this review may not translate to other institutions or have total relevance to the wider readership. However, MNP or WHPI could be replaced by any health problem or intervention in other reviews, and therefore the methodology of this review may provide a reasonable framework for other institutions and individuals to critically appraise and map their own curriculum.
The included systematic reviews and meta-analyses provided comprehensive insight and the highest level of evidence into effective WHPI for work-related MNP.33–36 The literature supports the use of long-term multidimensional WHPI, which include graded fitness and strength training (resistance and postural exercises of the neck and shoulder), ergonomic adjustments (of workstation and regular breaks), and mental and physical health education as effective at reducing work-related MNP in office workers. However, the variations in target groups, interventions, follow-ups, and outcome measurements led to significant heterogeneity in the meta-analyses and systematic reviews. Therefore, there is no consensus on the most effective WHPI for work-related MNP in the current literature.
There is still a need for high-quality studies with well-designed multidimensional interventions that are tailored toward neck pain in office workers and are conducted at the workplace. We recommend that researchers use the ICF terminology in future intervention-based studies to ensure that all relevant dimensions of health and functioning are addressed. In addition, for quantifying MNP and disability, we also recommend the use of a combination of research-validated self-reporting instruments that provide a sound balance and distribution of items across the ICF components.
CONCLUSION
Multidimensional WHPI focusing on mental and physical functioning (e.g., health education, relaxation, work breaks, and stress management), activity performance and modifications (e.g., fitness, strengthening or resistance neck and shoulder exercises, and postural adjustments), and environmental modifications (e.g., ergonomic adjustments) appear to reduce MNP severity and disability primarily in office workers, particularly in the long term. There is adequate congruence between the chiropractic postgraduate program at MU and the published literature on some WHPI (body functions and structures). However, there is inadequate coverage on aspects of MNP and effective WHPI for MNP, particularly those focusing on activity and participation and environmental factors. Furthermore, there was a slight bias toward time allocated to theoretical acquisition.
ACKNOWLEDGMENTS
We would like to sincerely thank all the MU chiropractic postgraduate program staff members for their assistance with providing pertinent information on syllabi for this review.
FUNDING AND CONFLICTS OF INTEREST
No sources of funding, monetarily or otherwise, were expended in this review. Peter Tuchin is a member of the Macquarie University Department of Chiropractic, and Martin Frutiger was a research candidate within this department at the time of the study.
APPENDIX A. ERIC AND INFORMIT A+ EDUCATION SEARCH STRATEGY
chiro* AND
educat* OR
curric* OR
map* OR
design OR
undergrad* OR
postgrad* OR
medical OR
learning outcomes OR
grad* capabilit*
APPENDIX B. COCHRANE LIBRARY SEARCH STRATEGY
neck pain
nonspecific neck*
#1 or #2
work*
work* intervention*
health promotion*
#4 or #5 or #6
#3 and #7
systematic review*
meta-analys*
#9 or #10
#8 and #11
APPENDIX C. PUBMED SEARCH STRATEGY
(((((neck pain) AND work*) AND intervention)) AND systematic review) AND meta-analys*
APPENDIX D. EMBASE SEARCH STRATEGY
exp neck pain/
exp treatment outcome/
exp health education/ or exp health promotion/ or exp health program/ or exp health care/ or exp prevention/
exp work disability/ or exp work/ or exp work environment/ or exp return to work/
exp occupational health/ or exp occupational disease/ or exp occupational health service/ or exp occupational hazard/
2 and 3 and 4 and 5
1 and 6
systematic review.mp. or exp “systematic review"/
meta analysis/
8 or 9
7 and 10
APPENDIX E. CINAHL SEARCH STRATEGY
Neck pain or cervical pain or neck ache AND
Work* AND
Work* intervention* AND
Systematic review or meta-analysis
APPENDIX F. PEDro SEARCH STRATEGY
neck pain*, work*, systematic review, meta-analysis*
REFERENCES
- 1. Merskey H, Bogduk N, . International Association for the Study of Pain Subcommittee on Taxonomy. Classification of chronic pain. Descriptions of chronic pain syndromes and definitions of pain terms. Pain Suppl. 1986; 3: S1– S226. [PubMed] [Google Scholar]
- 2. Misailidou V, Malliou P, Beneka A, et al. Assessment of patients with neck pain: a review of definitions, selection criteria, and measurement tools. J Chiropr Med. 2010; 9: 49– 59. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3. Guzman J, Hurwitz EL, Carroll LJ, et al. A new conceptual model of neck pain: linking onset, course, and care: the bone and joint decade 2000–2010 task force on neck pain and its associated disorders. Spine (Phila Pa 1976). 2008; 33: S14– S23. [DOI] [PubMed] [Google Scholar]
- 4. Bongers PM, Kremer AM, ter Laak J. . Are psychosocial factors, risk factors for symptoms and signs of the shoulder, elbow, or hand/wrist? A review of the epidemiological literature. Am J Ind Med. 2002; 41: 315– 342. [DOI] [PubMed] [Google Scholar]
- 5. Côté P, van der Velde G, Cassidy JD, et al. The burden and determinants of neck pain in workers: results of the bone and joint decade 2000–2010 task force on neck pain and its associated disorders. Spine (Phila Pa 1976). 2008; 33: S60– S74. [DOI] [PubMed] [Google Scholar]
- 6. Punnett L, Wegman DH. . Work-related musculoskeletal disorders: the epidemiologic evidence and the debate. J Electromyogr Kinesiol. 2004; 14: 13– 23. [DOI] [PubMed] [Google Scholar]
- 7. Visser B, van Dieen JH. . Pathophysiology of upper extremity muscle disorders. J Electromyogr Kinesiol. 2006; 16: 1– 16. [DOI] [PubMed] [Google Scholar]
- 8. Hoy D, March L, Woolf A, et al. The global burden of neck pain: estimates from the global burden of disease 2010 study. Ann Rheum Dis. 2014; 3: 1309– 1315. [DOI] [PubMed] [Google Scholar]
- 9. Murray CJ, Vos T, Lozano R, et al. Disability-adjusted life years (DALYs) for 291 diseases and injuries in 21 regions, 1990–2010: a systematic analysis for the global burden of disease study 2010. Lancet. 2012; 380: 2197– 2223. [DOI] [PubMed] [Google Scholar]
- 10. Cancelliere C, Cassidy JD, Ammendolia C, et al. Are workplace health promotion programs effective at improving presenteeism in workers? A systematic review and best evidence synthesis of the literature. BMC Public Health. 2011; 11: 395. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11. Malik SH, Blake H, Suggs LS. . A systematic review of workplace health promotion interventions for increasing physical activity. Br J Health Psychol. 2014; 19: 149– 180. [DOI] [PubMed] [Google Scholar]
- 12. Chapman LS. . Meta-evaluation of worksite health promotion economic return studies: 2005 update. Am J Health Promot. 2005; 19: 1– 11. [DOI] [PubMed] [Google Scholar]
- 13. Pelletier KR. . A review and analysis of the clinical and cost-effectiveness studies of comprehensive health promotion and disease management programs at the worksite: update VI 2000–2004. J Occup Environ Med. 2005; 47: 1051– 1058. [DOI] [PubMed] [Google Scholar]
- 14. Pelletier KR. . A review and analysis of the clinical and cost-effectiveness studies of comprehensive health promotion and disease management programs at the worksite: update VII 2004–2008. J Occup Environ Med. 2009; 51: 822– 837. [DOI] [PubMed] [Google Scholar]
- 15. World Health Organization. The international classification of functioning, disability and health (ICF). Geneva, Switzerland; 2001. http://apps.who.int/classifications/icfbrowser. Updated May 1, 2016. Cited May 22, 2016.
- 16. Harden RM. . AMEE guide no. 21: curriculum mapping: a tool for transparent and authentic teaching and learning. Med Teach. 2001; 23: 123– 137. [DOI] [PubMed] [Google Scholar]
- 17. Jacobs H. . Mapping the Big Picture. Alexandria, VA: Association for Supervision and Curriculum Development; 1997. [Google Scholar]
- 18. Hege I, Nowak D, Kolb S, et al. Developing and analysing a curriculum map in occupational and environmental medicine. BMC Med Educ. 2010; 10: 60. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19. Prideaux D. . Curriculum design. BMJ. 2003; 326: 268– 270. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20. Haas M, Leo M, Peterson D, et al. Evaluation of the effects of an evidence-based practice curriculum on knowledge, attitudes, and self-assessed skills and behaviors in chiropractic students. J Manipulative Physiol Ther. 2012; 35: 701– 709. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21. Council on Chiropractic Education Australasia. Armadale: Council on Chiropractic Education Australasia, Inc; 2016. http://www.ccea.com.au. Updated May 20, 2016. Cited May 27, 2016.
- 22. Saranchuk R, Watkins T. . Analysis of the relationship between program design and professional practice in CMCC's undergraduate chiropractic program. J Can Chiropr Assoc. 2000; 44: 230– 244. [Google Scholar]
- 23. Souza T. . Differential Diagnosis and Management for the Chiropractor: Protocols and Algorithms. 3rd ed. Burlington, MA: Jones & Bartlett Publishers; 2005. [Google Scholar]
- 24. Vermet S, McGinnis K, Boodham M, et al. Degree of vertical integration between the undergraduate program and clinical internship with respect to lumbopelvic diagnostic and therapeutic procedures taught at the Canadian memorial chiropractic college. J Chiropr Educ. 2010; 24: 46– 56. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25. Davis MH, Harden RM. . Planning and implementing an undergraduate medical curriculum: the lessons learned. Med Teach. 2003; 25: 596– 608. [DOI] [PubMed] [Google Scholar]
- 26. Maxwell S, Walley T, . BPS Clinical Section Committee. Teaching safe and effective prescribing in UK medical schools: a core curriculum for tomorrow's doctors. Br J Clin Pharmacol. 2003; 55: 496– 503. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27. Redwood-Campbell L, Pakes B, Rouleau K, et al. Developing a curriculum framework for global health in family medicine: emerging principles, competencies, and educational approaches. BMC Med Educ. 2011; 11: 46. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28. Willett TG. . Current status of curriculum mapping in Canada and the UK. Med Educ. 2008; 42: 786– 793. [DOI] [PubMed] [Google Scholar]
- 29. Gorrell L, Beirman RL, Vemulpad SR. . Curriculum mapping within an Australian master of chiropractic program: congruence between published evidence for chiropractic and student assessment tasks. J Chiropr Educ. 2015; 29: 29– 36. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30. Shekelle PG, Coulter I, Hurwitz EL, et al. Congruence between decisions to initiate chiropractic spinal manipulation for low back pain and appropriateness criteria in North America. Ann Intern Med. 1998; 129: 9– 17. [DOI] [PubMed] [Google Scholar]
- 31. Cooley J, Parkin-Smith G, Maire J, Simpson K, Chap P, Nook B. . Simulated Learning Environment Chiropractic Curriculum Report Murdoch University. Perth, Australia: Murdoch University; 2011. [Google Scholar]
- 32. Moher D, Liberati A, Tetzlaff J, et al. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. BMJ. 2009; 6: e1000097. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33. Aas RW, Tuntland H, Holte KA, et al. Workplace interventions for neck pain in workers. Cochrane Database Syst Rev. 2011; 13:CD008160. [DOI] [PMC free article] [PubMed]
- 34. Coury HJC, Moreira RFC, Dias NB. . Evaluation of the effectiveness of workplace exercise in controlling neck, shoulder and low back pain: a systematic review. Braz J Phys Ther. 2009; 13: 461– 479. [Google Scholar]
- 35. Hoe VC, Urquhart DM, Kelsall HL, et al. Ergonomic design and training for preventing work-related musculoskeletal disorders of the upper limb and neck in adults. Cochrane Database Syst Rev. 2012; 15:CD008570. [DOI] [PMC free article] [PubMed]
- 36. Varatharajan S, Côté P, Shearer H, et al. Are work disability prevention interventions effective for the management of neck pain or upper extremity disorders? A systematic review by the Ontario protocol for traffic injury management (OPTIMa) collaboration. J Occup Rehabil. 2014; 24: 692– 708. [DOI] [PubMed] [Google Scholar]