

Abstract
Aim:
The aim of this study is to compare tunica vaginalis (TV), dorsal dartos, and ventral dartos flap as a second layer vascular cover during Snodgrass repair.
Materials and Methods:
Data of 83 patients who underwent primary hypospadias repair with Snodgrass technique (age range: 1.6–12 years) were retrospectively collected and compared. They were divided into three groups. Group A (26 patients) included cases using TV flap, Group B (36 patients) included those where dorsal dartos from prepuce was used as second cover, and Group C (21 patients) included those with ventral dartos as cover.
Results:
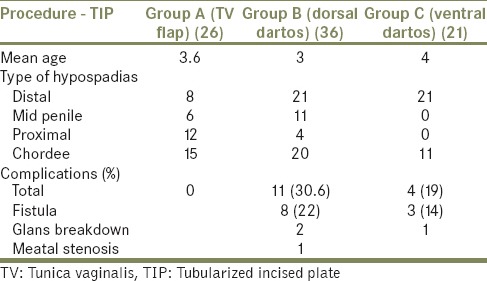
In Group A, no complications recorded. Mild scrotal edema was present in 5 patients which was conservatively managed. In Group B, there were 8 fistulas, 2 glans breakdown, and 1 meatal stenosis. In Group C, there were 3 fistulas and 1 glans breakdown.
Conclusion:
TV flap is better than dorsal dartos and ventral dartos as vascular cover for primary hypospadias repair with Snodgrass technique.
Keywords: Dorsal dartos flap, Snodgrass surgery, tunica vaginalis flap, ventral dartos flap
INTRODUCTION
There are over 200 different types of hypospadias repairs. Tubularized incised plate (TIP) urethroplasty or Snodgrass technique can be used for all types of hypospadias repairs from distal to proximal where urethral plate can be preserved.[1] The reported incidence of complications for hypospadias surgery by Snodgrass technique ranges from 0% to 53%,[2,3] varying with the severity of the hypospadias blaming it on surgical technique, suture material, surgeons’ experience, age of patient and type of coverage, etc., The high complication rates of hypospadias repair remain a significant problem despite the development of improved surgical techniques, suture materials, and postoperative care.
Many studies have shown good results with Snodgrass technique, but the most common complication reported is urethrocutaneous fistula which forms >60% of all complications.[4] A second vascular cover on the tube such as spongiosum, dartos, or tunica vaginalis (TV) is known to minimize or avoid this complication[2,5,6,7,8,9,10,11,13,14,15] but which flap provides a better cover is still a matter of debate since decades because results have been conflicting with different results in the hands of different surgeons. The aim of our study is to present our experience with TIP urethroplasty using tunica, dorsal, and ventral dartos as second cover and see which had a better outcome.
MATERIALS AND METHODS
Data of 83 patients who underwent Snodgrass repair (age range: 1.6–12 years) in the previous 4 years (July 2010–June 2014) in our institute were retrospectively collected and compared after obtaining approval from hospital review board. Only patients undergoing primary repair were included in the study. They were divided into three groups. Group A included cases using TV flap, Group B included those where dorsal dartos was used as vascular cover, and Group C included those with ventral dartos as cover. Follow-up data were collected from operative register, morbidity register, follow-up OPD register, and telephonic contact with the patient. Follow-up period ranged from 6 months to 3 years. Patients with no follow-up (23 cases), redo hypospadias repairs, patients in whom human chorionic gonadotropin or testosterone was given, and those in whom repair other than Snodgrass was used were excluded from the study. All three groups were similar in their demography and age distribution.
Operative technique
In all three groups, the general technique was the same as described by Snodgrass[1] and was done by a single surgeon. Magnification (2.5 × Loupes), fine instruments, and bipolar electrocautery were used. An inverted U-shaped incision was made encircling the meatus to the corona, preserving the urethral plate, and then extended circumferentially around the corona. A Gitte's test was done to evaluate the chordee after penile degloving. Glans wings are raised. A transverse incision made over the urethral plate, and it was tubularized over an appropriate sized catheter using 6-0 vicryl suture using subcuticular sutures. The technique of putting a soft-tissue cover over this neourethra differed among the groups. At the end, Beyers flap was cut, brought ventrally, and sutured to give an appearance of a midline raphe.
In Group 1, degloving was done till the root of penis. The TV flap was raised by bringing the testis to the operative field and incising the tunica near the lower pole of testis. After obtaining adequate length, flap was raised if necessary even up to the external ring [Figure 1a], and this was used to cover the entire length of tube and secured in place [Figure 1b].
Figure 1.
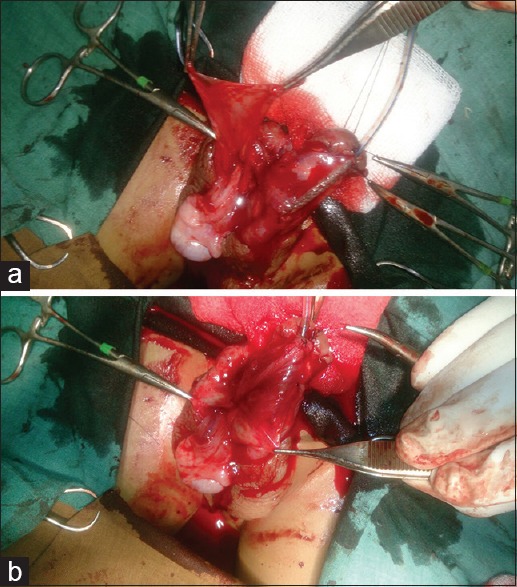
(a) Tunica vaginalis flap raised by incising the tunica near the lower pole of testis and adequate length can be obtaining by dissecting even up to the external ring. (b) The raised tunica vaginalis flap is used to cover the entire length of tube and secured in place
In Group 2, the dartos flap was raised by dissecting between the skin and dartos layer of dorsal prepuce [Figure 2a]. This dartos fascia was de-epithelialized, then brought ventrally from the right or left side, and used to cover the ventral suture line [Figure 2b].
Figure 2.
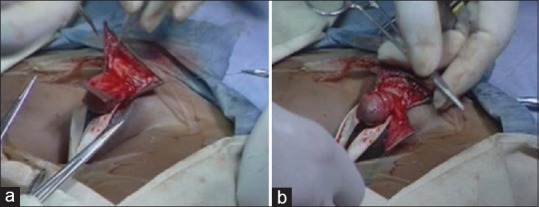
(a) Dartos flap raised by dissecting between the skin and dartos layer of dorsal prepuce. (b) Dartos fascia brought ventrally and then de-epithelialized to cover the ventral suture line
In Group 3, a ventral based dartos flap was used as a cover. After degloving, a longitudinal rectangle was marked on the proximal shaft [Figure 3a] or laterally [Figure 4a], and flap raised from corpus spongiosum and ventral dartos tissue and flipped over neourethra and tacked to the lateral recess of raised glans wings [Figures 3b and 4b].
Figure 3.
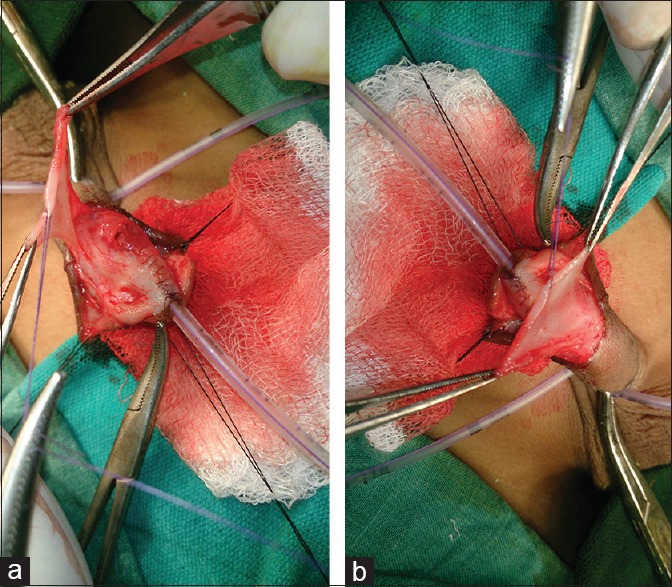
(a and b) Ventral dartos from proximal shaft raised flipped over neourethra and tacked to lateral recess of raised glans wings
Figure 4.
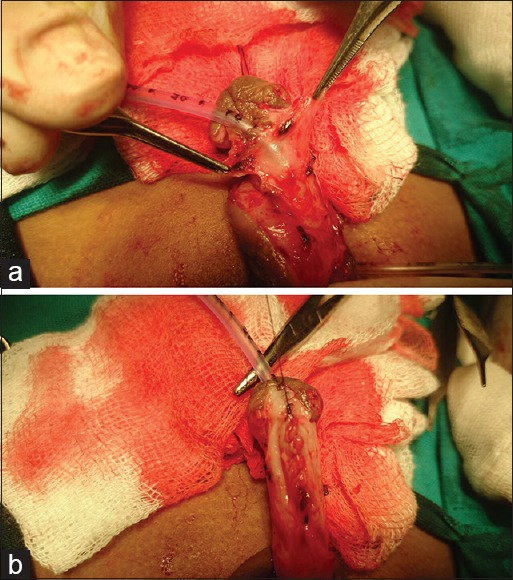
(a and b) Flaps raised on either side of neourethra which includes corpus spongiosum and ventral dartos and approximated in midline
Light compression dressing applied. Intravenous antibiotics were given for 5 days, followed by oral antibiotics till the dressing was removed. Dressing and the catheter were removed on the 10th day. If there was soakage of dressing, it was changed in between, but a clean dressing was left in place for 10 days.
RESULTS
When comparing the type of hypospadias, it was noted that TV flap was most commonly used for proximal repairs, and distal repairs were done more commonly with dorsal or ventral dartos flaps as second cover. Detailed distribution of type of hypospadias, chordee, and type of repair is shown in Table 1. For all patients with chordee, it was corrected with degloving and no additional procedures were required. Ventral dartos was used in 21 patients and all were distal hypospadias repairs. Complications were seen in four patients where three had fistulas and one had glans breakdown. Dorsal dartos was used in 36 patients. Complications were seen in 11 patients. Fistulas were seen in 8 patients; 2 of 21 distal repairs, 4 of 11 mid repairs, and 2 of 4 proximal repairs had fistula.
Table 1.
Distribution of type of hypospadias and complications in each group
All patients with fistula were successfully repaired with fistula closure, except one of proximal hypospadias repair with dorsal dartos as second cover had a recurrent fistula and is awaiting another surgery. Of the three patients with glans breakdown, only one underwent redo surgery. The other two patients’ family did not want another surgery and was happy with a coronal meatus. The patients with meatal stenosis responded to dilatations.
DISCUSSION
The use of a waterproofing second cover for the neourethra is well documented in literature varying from corpus spongiosum, dartos-based flaps (ventral, dorsal, and scrotal dartos flaps) to TV which is known to decrease the incidence of fistula and breakdowns.[2,5,6,7,8,9,10,11,13,14,15] We reviewed studies which used a second vascular cover following TIP repair to see if the success rates were better.
The reported fistula rate with spongioplasty ranges from 0% to 31%.[5] Bhat et al. and Almodhen et al. have shown a very low fistula rate with spongioplasty after Snodgrass repair.[5,6] While several investigators have shown spongioplasty to be as protective as a dartos flap, others have found that spongioplasty is associated with unacceptably high fistula rates when compared with the standard dartos flap and have used both together as waterproof covers. The variable rate of success may be explained at least in part by variations in spongiosal anatomy.[6] Unfortunately, this spongiosal tissue is not always available and well developed and cannot always be mobilized and placed over the neourethral suture line. We did not do only spongioplasty for any of our patients, since while mobilizing the ventral dartos flap, a part of spongiosum is also taken as a cover on the tube; when there was adequate spongiosum and ventral tissue available, we took a ventral dartos flap. When this was not available or not well developed, dorsal dartos from prepuce was preferred. Tunica was used in most of the proximal cases where dissection was done till the root of penis which made accessing the testis and tunica easier. The type of second cover used was decided on table by the operating surgeon on a case to case basis.
Smith performed tubularized incised plate urethroplasty for repair in 64 patients and used the ventral based dartos pedicle flap for covering the neourethra in 56 of the repairs (85.5%) without complication.[7] Furness reported that of the 111 patients with reconstruction using the ventral based vascularized dartos pedicle to cover the tubularized incised plate, urethroplasty was successful in 109 (98.2%) with only 2 patients developing fistula formation.[8] He commented that the technique simply uses vascular dartos tissue that is already present in situ, with great care taken so that abundant subcuticular tissue is left proximal to the hypospadiac meatus when ventral incision and dissection is performed. Soygur et al. adopted the ventral based dartos flap and found the flap much easier to construct with little time added to surgery and no harvesting related complications.[9] They also obtained satisfactory results with a fistula rate of 8.3%. Yutaro Hayashi et al. reported an incidence of 9% fistula rate with ventral based dartos flap.[10]
Belman used the de-epithelialized preputial skin flap as a vascular cover for hypospadias repairs.[12] This was later adopted to TIP procedure by many surgeons and Snodgrass himself.[2,13,14] Necrosis of the Beyers skin flap and penile rotation are the complications with this technique. Skin necrosis can be prevented by limiting the aggressive dissection between the skin and preputial dartos. Penile rotation can be limited by making a button hole to bring the dartos ventrally without causing vascular compromise. We did not make any button hole and brought the preputial dartos from the right or left side without tension, and none of our cases had any significant penile torsion or skin necrosis.
Dartos-based flaps have the advantage that they are available locally and do not require another incision or extension of the incision like for TV flaps. However, various studies have reported a lesser degree of complications with TV flap. Snodgrass himself reported that fistula reduced from 33% to 10% by two-layered subepithelial closure in mid and proximal repairs instead of a single layer closure. He used dartos barrier covering in all 65 patients.[2] Snodgrass later used tunica as barrier layer instead of dartos and found that the fistula rate reduced to almost 0%.[15] Chatterjee et al., while describing a comparison of dartos (20 cases) and tunica vaginalis flap (TVF) (29 cases) in primary repair of hypospadias, reported zero fistula rate with TVF as opposed to 15% in dartos group.[16] It is well documented that TV gives very good results when used in redo surgeries.[17]
Various studies have documented that TV is a better cover, decreasing the incidence of fistula rates when compared to dorsal dartos flaps.[16,18,19] Structural alterations in patients with hypospadias are held responsible for these dartos flap complications. The prepuce is defective in most hypospadiac patients and is usually in the form of a partial prepuce that does not fully cover the glans penis. Cağrı Savaş et al. studied microvessel density of prepuce in children with hypospadias and found it to be significantly less.[20] Soyer et al. found that there is a decreased vascular endothelial growth factor in prepuce of hypospadiac patients which could be the cause of impaired wound healing and recurrent complications after preputial reconstruction.[21] Pichler et al. did a quantitative measurement of androgen receptors (AR) in prepuce of hypospadias and found AR mRNA (P = 0.013), and AR protein (P = 0.014) was significantly elevated.[22] All these indicate that dorsal dartos flaps and prepuce used for reconstruction may not be the ideal tissue due to structural alterations at vascular, neural, and immunological level.
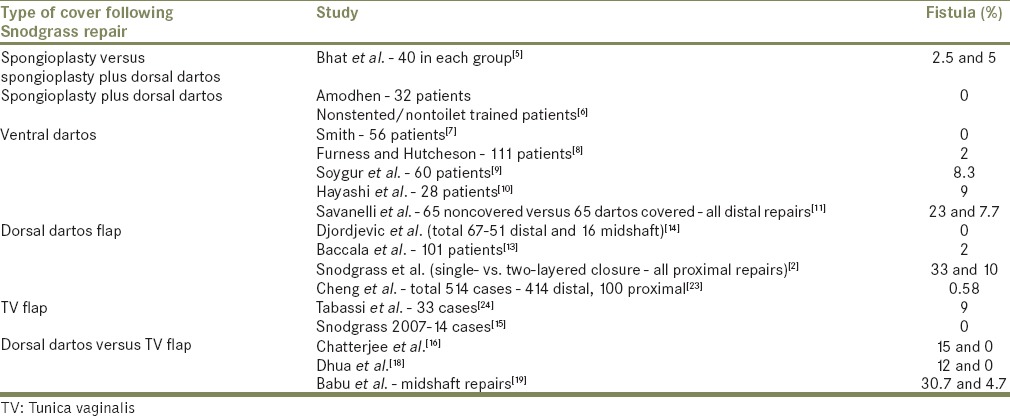
In our study, the fistula rate remained high for dorsal dartos (22%) and ventral dartos flaps (14%) compared to TV group (0%). Our study and many other studies[16,18,19] indicate that tunica is a better cover than dartos for primary repair with Snodgrass technique. However, there are studies documenting very low fistula rates with spongioplasty, ventral dartos, dorsal dartos flap, and double covering [Table 2]. We cannot compare these studies since some included mostly proximal repairs and some mostly distal repairs. Some were stentless, some were double-layered subepithelial urethroplasties, and some used a double covering. This conflict calls for a prospective randomized study with molecular biology included to help choose an ideal cover.
Table 2.
Fistula rates for various different coverings used in Snodgrass repair
Limitations
All three groups do not have an equal number of cases, but being a retrospective study to get an equal match is difficult. The TV flap group has more cases of proximal hypospadias, and the other two groups have more of distal hypospadias. Complications are said to be more in proximal hypospadias than distal unlike our observation. We attribute tunica as the reason for the good results in proximal hypospadias cases.
CONCLUSION
TV flap is better than dorsal or ventral dartos as a second vascular cover for primary hypospadias repair by Snodgrass technique. Future prospective randomized studies with molecular biology included would help in further evaluation of the same.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- 1.Snodgrass WT. Tubularized incised plate (TIP) hypospadias repair. Urol Clin North Am. 2002;29:285–90, v. doi: 10.1016/s0094-0143(02)00045-9. [DOI] [PubMed] [Google Scholar]
- 2.Snodgrass W, Yucel S. Tubularized incised plate for mid shaft and proximal hypospadias repair. J Urol. 2007;177:698–702. doi: 10.1016/j.juro.2006.09.104. [DOI] [PubMed] [Google Scholar]
- 3.Abolyosr A. Snodgrass hypospadias repair with onlay overlapping double-layered dorsal dartos flap without urethrocutaneous fistula: Experience of 156 cases. J Pediatr Urol. 2010;6:403–7. doi: 10.1016/j.jpurol.2009.09.012. [DOI] [PubMed] [Google Scholar]
- 4.Snodgrass WT, Lorenzo A. Tubularized incised-plate urethroplasty for proximal hypospadias. BJU Int. 2002;89:90–3. [PubMed] [Google Scholar]
- 5.Bhat A, Singla M, Bhat M, Sabharwal K, Kumar V, Upadhayay R, et al. Comparison of results of TIPU repair for hypospadias with “Spongioplasty Alone” and “Spongioplasty with Dorsal Dartos Flap”. Open J Urol. 2014;4:41–8. [Google Scholar]
- 6.Almodhen F, Alzahrani A, Jednak R, Capolicchio JP, El Sherbiny MT. Nonstented tubularized incised plate urethroplasty with Y-to-I spongioplasty in non-toilet trained children. Can Urol Assoc J. 2008;2:110–4. doi: 10.5489/cuaj.484. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Smith DP. A comprehensive analysis of a tubularized incised plate hypospadias repair. Urology. 2001;57:778–81. doi: 10.1016/s0090-4295(00)01062-1. [DOI] [PubMed] [Google Scholar]
- 8.Furness PD, 3rd, Hutcheson J. Successful hypospadias repair with ventral based vascular dartos pedicle for urethral coverage. J Urol. 2003;169:1825–7. doi: 10.1097/01.ju.0000058429.18975.30. [DOI] [PubMed] [Google Scholar]
- 9.Soygur T, Arikan N, Zumrutbas AE, Gulpinar O. Snodgrass hypospadias repair with ventral based dartos flap in combination with mucosal collars. Eur Urol. 2005;47:879–84. doi: 10.1016/j.eururo.2005.02.022. [DOI] [PubMed] [Google Scholar]
- 10.Hayashi Y, Kojima Y, Nakane A, Kurokawa S, Tozawa K, Kohri K, et al. Ventral based dartos flap for the prevention of the urethrocutaneous fistula urethroplasty. Int J Urol. 2007;14:725–8. doi: 10.1111/j.1442-2042.2007.01811.x. [DOI] [PubMed] [Google Scholar]
- 11.Savanelli A, Esposito C, Settimi A. A prospective randomized comparative study on the use of ventral subcutaneous flap to prevent fistulas in the snodgrass repair for distal hypospadias. World J Urol. 2007;25:641–5. doi: 10.1007/s00345-007-0215-2. [DOI] [PubMed] [Google Scholar]
- 12.Belman AB. De-epithelialized skin flap coverage in hypospadias repair. J Urol. 1988;140:1273–6. doi: 10.1016/s0022-5347(17)42022-2. [DOI] [PubMed] [Google Scholar]
- 13.Baccala AA, Jr, Ross J, Detore N, Kay R. Modified tubularized incised plate urethroplasty (Snodgrass) procedure for hypospadias repair. Urology. 2005;66:1305–6. doi: 10.1016/j.urology.2005.07.011. [DOI] [PubMed] [Google Scholar]
- 14.Djordjevic ML, Perovic SV, Vukadinovic VM. Dorsal dartos flap for preventing fistula in the snodgrass hypospadias repair. BJU Int. 2005;95:1303–9. doi: 10.1111/j.1464-410X.2005.05500.x. [DOI] [PubMed] [Google Scholar]
- 15.Snodgrass WT. Editorial comment. J Urol. 2007;178:1456. doi: 10.1016/j.juro.2008.03.077. [DOI] [PubMed] [Google Scholar]
- 16.Chatterjee US, Mandal MK, Basu S, Das R, Majhi T. Comparative study of dartos fascia and tunica vaginalis pedicle wrap for the tubularized incised plate in primary hypospadias repair. BJU Int. 2004;94:1102–4. doi: 10.1111/j.1464-410X.2004.05111.x. [DOI] [PubMed] [Google Scholar]
- 17.Routh JC, Wolpert JJ, Reinberg Y. Tunneled tunica vaginalis flap is an effective technique for recurrent urethrocutaneous fistulas following tubularized incised plate urethroplasty. J Urol. 2006;176:1578–80. doi: 10.1016/j.juro.2006.06.032. [DOI] [PubMed] [Google Scholar]
- 18.Dhua AK, Aggarwal SK, Sinha S, Ratan SK. Soft tissue covers in hypospadias surgery: Is tunica vaginalis better than dartos flap? J Indian Assoc Pediatr Surg. 2012;17:16–9. doi: 10.4103/0971-9261.91080. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Babu R, Hariharasudhan S. Tunica vaginalis flap is superior to inner preputial dartos flap as a waterproofing layer for primary TIP repair in midshaft hypospadias. J Pediatr Urol. 2013;9:804–7. doi: 10.1016/j.jpurol.2012.10.022. [DOI] [PubMed] [Google Scholar]
- 20.Cağrı Savaş M, Kapucuoğlu N, Gürsoy K, Başpınar S. The microvessel density of the hypospadiac prepuce in children. J Pediatr Urol. 2011;7:162–5. doi: 10.1016/j.jpurol.2010.04.017. [DOI] [PubMed] [Google Scholar]
- 21.Soyer T, Ayva ES, Atasoy P, Aslan MK, Cakmak AM. Comparison of growth factor levels in patients with normal and hypospadiac prepuce. Turk J Med Sci. 2011;41:81–5. [Google Scholar]
- 22.Pichler R, Djedovic G, Klocker H, Heidegger I, Strasak A, Loidl W, et al. Quantitative measurement of the androgen receptor in prepuces of boys with and without hypospadias. BJU Int. 2013;112:265–70. doi: 10.1111/j.1464-410X.2012.11731.x. [DOI] [PubMed] [Google Scholar]
- 23.Cheng EY, Vemulapalli SN, Kropp BP, Pope JC, 4th, Furness PD, 3rd, Kaplan WE, et al. Snodgrass hypospadias repair with vascularized dartos flap: The perfect repair for virgin cases of hypospadias. J Urol. 2002;168:1723–6. doi: 10.1097/01.ju.0000026940.33540.31. [DOI] [PubMed] [Google Scholar]
- 24.Tabassi KT, Mohammadi S. Tunica vaginalis flap as a second layer for tubularized incised plate urethroplasty. Urol J. 2010;7:254–7. [PubMed] [Google Scholar]