

Abstract
Background
Highly caffeinated energy drinks (EDs) are popular with adolescents and young adults, but longitudinal consumption patterns are poorly understood especially in relation to other substance use.
Methods
ED and other substance use were assessed annually (modal ages 21–25) among a sample (n=1099) who were originally recruited as first-year college students (modal age 18). Trajectory groups were derived based on probability of past-year use during ages 21–24, and compared for possible differences in substance use outcomes at age 25, holding constant demographics, sensation-seeking, other caffeine consumption, and age 21 substance use.
Results
From age 21 to 25, ED consumption declined in both annual prevalence [62.5%wt to 49.1%wt (wt=weighted)] and frequency of use among consumers (35.2 to 26.3 days/year). Yet individuals exhibiting a Persistent trajectory (51.4%) of consumption outnumbered those with Non-Use (20.6%), Intermediate (17.4%), or Desisting (10.6%) trajectories. Age 25 cocaine use, nonmedical use of prescription stimulants (NPS), and alcohol use disorder (AUD) risk were significantly associated with trajectory group membership, with Persistent and Intermediate groups exhibiting the highest risk for such outcomes, even accounting for prior substance use and other risk factors. Neither marijuana nor tobacco use were associated with group membership.
Conclusions
The typical pattern of ED consumption among this sample was sustained use throughout young adulthood. Such individuals appear to be at high risk for adverse substance use outcomes, and results suggest possible specificity regarding cocaine use and NPS, and AUD risk. More research is needed to understand the mechanisms underlying the connection between ED and substance use.
Keywords: caffeine, energy drinks, substance use, cocaine, nonmedical prescription stimulants, college students, longitudinal studies, young adults
1. Introduction
Energy drinks (EDs) and shots are highly caffeinated products marketed primarily to adolescents and young adults (Heckman et al., 2010; Reissig et al., 2009). Although caffeine is the most commonly used drug in the world (Juliano et al., 2009), the introduction of EDs to the marketplace—and the rapid growth in their popularity—have taken caffeine use in a new direction (Branum et al., 2014; Packaged Facts, 2013). EDs differ from traditional caffeinated beverages by typically containing higher doses and concentrations of added caffeine in the form of sweet, flavored beverages or shots designed to be ingested quickly (Juliano et al., 2009; Reissig et al., 2009; Seifert et al., 2011). Marketed primarily to youth (Heckman et al., 2010), some branding is related to risky behaviors (e.g., Rehab, Full Throttle, AMP Energy) and their consumption has become intertwined with high-risk alcohol use (Arria et al., 2010; Arria et al., 2011a; O’Brien et al., 2013; O’Brien et al., 2008; Reissig et al., 2009).
Approximately one in three U.S. adolescents and young adults consume EDs and energy shots, with estimates as high as 50% for past-month use among college students (Arria et al., 2014; Miller, 2008b; Terry-McElrath et al., 2014; Velazquez et al., 2012; Woolsey et al., 2015). One study reported that 10% of college students consumed EDs at least weekly during the past year (Arria et al., 2011a). While White males are at highest risk for ED consumption among college students (Poulos and Pasch, 2015), other minority groups appear to be at risk among community samples (Arria et al., 2014; Berger et al., 2011).
Because of the high caffeine levels contained in most of these products, at least two major health concerns have been raised. First, acute cardiovascular effects have been discussed (Seifert et al., 2011); in particular, increased blood pressure (Franks et al., 2012; Phan and Shah, 2014; Shah et al., 2016), arrhythmias (Goldfarb et al., 2014), and increased platelet aggregation (Worthley et al., 2010) have been reported clinically. The second concern—and the focus of this paper—is the possible longer-term consequences of consuming highly caffeinated EDs, namely the increased potential for substance use and related problems. Significant cross-sectional associations between ED consumption and substance use (e.g., alcohol, tobacco, marijuana, nonmedical use of prescription drugs) have been reported (Arria et al., 2011a; Miller, 2008a; Skewes et al., 2013; Terry-McElrath et al., 2014; Trapp et al., 2014; Woolsey et al., 2014). Research has focused on the interrelationships between ED consumption and high-risk drinking, as well as the consequences thereof. Almost one-quarter of college students have mixed an ED with alcohol (O’Brien et al., 2008), and cross-sectional evidence links this behavior to increased risk for alcohol-related problems such as alcohol dose escalation and heavy drinking patterns, subjective increases in alcohol desires and expectancies, injuries, and sexual consequences (Arria et al., 2010; Ferré and O’Brien, 2011; Ferreira et al., 2013; Mallett et al., 2014; Marczinski et al., 2013; Miller, 2012; O’Brien et al., 2013; O’Brien et al., 2008). We previously reported that ED consumption is associated with an increased risk for alcohol dependence and more frequent drunk driving, even after adjustment for family history, conduct disorder, other caffeine consumption, and sensation-seeking (Arria et al., 2016b; Arria et al., 2011a).
Other research has observed a relationship between EDs and illicit substance use. From two waves of data from the study that is the focus of the present analysis, college students who consumed EDs were twice as likely to initiate nonmedical prescription stimulant use one year later compared with students who did not consume EDs, controlling for risk factors and other caffeine consumption (Arria et al., 2010). Other studies have also observed cross-sectional associations between ED consumption and other drug use (Kelly and Prichard, 2016; Kumar et al., 2015; Miller, 2008a; Miller and Quigley, 2011; Terry-McElrath et al., 2014; Trapp et al., 2014; Woolsey et al., 2014; Woolsey et al., 2015). At least three potential mechanisms exist to explain the association. First, ED consumers and individuals who use illicit substances might share a propensity for risk-taking. Problem behavior theory [PBT (Donovan and Jessor, 1985; Jessor, 1987)] would predict that ED consumers engage in substance use because they share many of the same characteristics as individuals with heavy substance use involvement [e.g., sensation-seeking, conduct problems (Kristjansson et al., 2013)]. Such commonalities point to a “third factor” hypothesis to explain the association between ED consumption and substance use.
Second, opportunities to be exposed to both EDs and other substances might overlap with each other. The social development model (Catalano and Hawkins, 1996) informs our understanding of the complex interplay of risk factors that might lead to high-risk substance use—and perhaps ED consumption—in that personal vulnerability to developing a substance use disorder (SUD) operates in the context of environmentally-driven opportunities to use a substance. ED consumption might increase an individual’s interest in using illicit drugs (Reissig et al., 2009). If ED consumers are drawn to affiliate with each other, such a peer network might provide increased opportunities for and more accepting attitudes toward substance use.
Third, neurobiological evidence supports the possibility that frequent ED consumption might contribute to an increased risk for SUD due to caffeine’s ability to potentiate the addictive properties of other substances (Ferré, 2016). Laboratory studies have shown that caffeine enhances nicotine’s reinforcing and analgesic effects and potentiates the addictive properties of other stimulant drugs (Jones and Griffiths, 2003; O’Neill et al., 2015; Sigmon and Griffiths, 2011; Tanda and Goldberg, 2000). Furthermore, the rapid-onset stimulant effects of EDs—especially among younger consumers who have not yet developed tolerance to caffeine—might provoke some consumers to seek out similar or even more intense effects via other drugs (Reissig et al., 2009). Some have argued that the high doses of caffeine in EDs might accelerate the development of caffeine dependence, which in turn could predict other SUDs (Meredith et al., 2013). If ED consumption contributes independently to intensification of substance use patterns, after accounting for shared risk factors, then prevention efforts could be targeted at ED consumption as a novel risk factor for substance use.
The purpose of this study is fourfold: (1) to describe the prevalence and frequency of ED consumption among a young adult sample throughout a five-year interval (ages 21 to 25); (2) to identify subsets of individuals who consume EDs with distinct trajectories of such use during the first four years of that interval (ages 21 to 24); (3) to describe the pattern of ED consumption within each trajectory group; and (4) to examine the relationship between ED trajectory group membership and subsequent alcohol use disorder (AUD) risk and other substance use at age 25, after accounting for variables that reflect the known shared propensity for risk-taking among individuals who consume EDs and individuals who use other substances. By taking these risk factors into account, we will be able to isolate the unique effect, if any, of trajectories of ED use on substance use, even in the context of the commonalities in their respective risk factors. This approach allows for simultaneous evaluation of two competing hypotheses that are both empirically and theoretically grounded: (1) a “third factor” hypothesis derived from PBT, and (2) a possible contributory relationship operating through neurobiological mechanisms. This component of the model reflects our hypothesis that EDs uniquely contribute to risk for AUD and other substance use.
2. Methods
2.1. Study design
Participants were enrolled in an ongoing longitudinal study that began at college entry in 2004 at one large public university (see (Arria et al., 2008; Vincent et al., 2012). Recruitment occurred in two stages, beginning with a pre-college survey during summer orientation (N=3,401; 89% response rate), followed by a two-hour baseline assessment with a sample of screened students (n=1,253; 87% response rate). To ensure adequate statistical power for analyzing longitudinal drug use patterns, students who used illicit substances or prescription medications nonmedically at least once during high school were purposively oversampled with 100% probability, and all others with 40% probability. At baseline, participation was restricted to first-time college students ages 17 to 19. Data for the present analysis were collected during Years 4 through 8 of the study (76% to 88% follow-up rates annually), and therefore encompass college graduation and the first few post-college years for most of the sample, although continued college attendance and graduation were not requirements for participation. The study was approved by the university’s IRB, and written informed consent was obtained. Further protection was provided by a federal Certificate of Confidentiality. Participants were paid for each assessment.
2.2. Participants
For the present study, the analysis sample was 1,099 individuals (54% women, 72% non-Hispanic White) who completed at least one of the annual assessments in which ED consumption patterns were assessed, that is Years 4 through 8, when modal ages were 21 through 25, respectively. Relative to the analysis sample, excluded individuals were over-representative of men (66% vs. 46%, p<.001) and slightly older at college entry (18.3 vs. 18.2 years, p=.002), but were similar with respect to race/ethnicity, parents’ education, and prior ED consumption assessed during Years 2 and 3.
2.3 Measures
2.3.1. ED consumption
Participants were asked which EDs they had consumed during the past year. Responses were open-ended and did not distinguish between energy shots (which deliver similarly high doses of caffeine in a smaller volume) and other types of EDs. For each product they consumed, participants were asked how many days they had consumed that product during the past year. Responses were later summed to derive an overall frequency of ED consumption. The summed frequencies were also categorized as frequent (≥52 days), occasional (≥12 days and <52 days), and infrequent (≥1 days and <12 days) patterns of use. Dichotomous variables representing past-year use (once or more versus none) were also constructed for each assessment year.
2.3.2. Other caffeine consumption
Participants were asked in Year 4 to estimate the frequency and quantity (in fluid ounces) of caffeinated beverages other than EDs consumed (i.e., coffee, tea, and soft drinks, assessed separately) during a typical week during the past year and later summed to approximate overall weekly caffeine consumption other than EDs.
2.3.3. Alcohol use and AUD risk
Past-year frequency of alcohol use and DSM-IV criteria for AUD risk were assessed in Year 4 and 8 using standard items (Substance Abuse and Mental Health Services Administration, 2003). A dichotomous variable representing the presence or absence of AUD risk was later derived based on standard criteria (American Psychiatric Association, 1994). No clinical assessment of AUD was conducted; therefore, herein we represent this self-reported proxy variable as “AUD risk”.
2.3.4. Other substance use
Dichotomous variables representing use and non-use of the following substances were derived from past-year frequency items assessed at Year 4 and Year 8: tobacco cigarettes, marijuana, cocaine, nonmedical use of prescription stimulants (NPS), and nonmedical use of prescription analgesics (NPA).
2.3.5. Impulsive sensation-seeking, behavioral dysregulation, and conduct problems
The Zuckerman-Kuhlman Personality Questionnaire (Zuckerman, 2002) was self-administered at baseline; the 7-item impulsive sensation-seeking subscale which was used for the present study has previously demonstrated good predictive validity with drug use and other risky behaviors (Zuckerman and Kuhlman, 2000). The Dysregulation Inventory (Mezzich et al., 2001) was also self-administered at baseline, and standard procedures were used to compute the behavioral dysregulation subscale score. Prior research has established its validity as an indicator of risk for illicit substance use and dependence (Mezzich et al., 2001).
An adapted version of the conduct disorder screener was also administered at baseline to capture the occurrence of 18 conduct problems during childhood, corresponding to the DSM-IV criteria for conduct disorder, and standard scoring methods were used to derive a scale score accounting for severity and frequency of each problem (Falls et al., 2011; Johnson et al., 1995; Nurco et al., 1999).
2.3.6. Demographics
Gender was recorded at baseline (i.e., modal age 18). Race/ethnicity was self-reported allowing for multiple responses, and later dichotomized due to the preponderance of Non-Hispanic Whites (72% vs. 28% other race/ethnicity). Parents’ education was self-reported by students at baseline for each parent, and later recoded as the maximum attainment of either parent.
2.4. Analytic strategy
Statistical weights were used to compute annual prevalence estimates that reflect the general population of incoming students at the home university and were adjusted for both attrition and sampling design. Statistical weights for the comparisons by trajectory group were computed to adjust for sampling design. Unweighted data were used for the regression modeling.
Group-based trajectory modeling was used to identify subsets of the sample who shared similar trajectories of ED consumption. A form of multivariate mixture modeling, this method uses PROC TRAJ (Jones et al., 2001) in SAS (SAS Institute Inc., 2008) and has proven helpful in understanding other substance use patterns longitudinally (Caldeira et al., 2012a; Caldeira et al., 2012b; Jackson et al., 2005; Kertesz et al., 2012; Suerken et al., 2016). We tested all one- to seven-group solutions with a second-degree polynomial in a series of three alternative sets of analyses. The first two sets of analyses modeled the variable representing overall past-year frequency of ED consumption, assuming, first, a zero-inflated Poisson (ZIP) distribution and, second, a normal distribution. The third set of analyses modeled the dichotomous variable representing past-year ED consumption (once or more versus none) in a logit model. Model fit was evaluated based on lower Bayesian Information Criterion (BIC) scores and the heuristic value of the resulting set of trajectory groups. Thus, even with a low BIC, models were regarded unfavorably if they yielded trajectory groups that were very small (<5% of sample) or difficult to interpret.
Based on the PROC TRAJ analyses described above, a categorical variable representing trajectory group membership was derived from the best-fitting model. Correlates of group membership were then examined using χ2 tests of independence for categorical variables and analysis of variance for continuous variables. Lastly, the prospective association of group membership with other substance use at modal age 25 (i.e., Year 8) was examined via logistic regression using the dichotomous variables on AUD risk and use of tobacco, marijuana, cocaine, NPS, and NPA, holding constant the effects of demographics, sensation-seeking, caffeine consumption, and prior substance use at modal age 21. Thus, our analysis examined the overall risk for substance use, regardless of whether it represented the initiation of new use or continuation of use that might have commenced prior to the observed ED consumption patterns.
With respect to missing data, trajectories were analyzed for the 1,033 individuals who had at least one observation during modal ages 21 to 24, most of whom had all four observations (87%). For the regression analyses, 170 individuals were excluded due to missing data on either (a) the substance use outcomes assessed at age 25 (n=82), or (b) one or more of the baseline risk factors (n=88), yielding a final analytic sample of n=863.
3. Results
3.1. Overall prevalence and frequency
Annual prevalence of ED consumption ranged from 62.5%wt (wt=statistically weighted to reflect the general population of incoming students at the home university) at modal age 21 to 49.1%wt at modal age 25 (see Table 1). Individuals with infrequent past-year consumption patterns (≥1 days and <12 days) consistently comprised about one-quarter of the sample in any given year (range 25.6%wt to 26.7%wt), whereas frequent (≥52 days) consumers declined from 11.7%wt to 5.9%wt and occasional (≥12 days and <52 days) consumers declined from 25.2%wt to 17.2%wt. Among past-year ED consumers, mean past-year frequency of use declined from 35.2 to 26.3 days by age 25.
Table 1.
Annual prevalence and frequency of energy drink consumption throughout five consecutive years (Nwt=3281).
| Modal age
|
Overall % changea | |||||
|---|---|---|---|---|---|---|
| 21 | 22 | 23 | 24 | 25 | ||
| (n=1097) | (n=1019) | (n=1000) | (n=982) | (n=951) | ||
|
|
||||||
| Unweighted % (n) consumed energy drinks at least once during the past year | 65.5 (719) | 60.2 (613) | 56.5 (565) | 54.7 (537) | 51.7 (492) | −21.1 |
| Weighted %wt consumed energy drinks at least once during the past year | 62.5 | 57.0 | 53.3 | 51.8 | 49.1 | −21.4 |
| Past-year consumption frequency pattern | ||||||
| %wt Did not consume (0 days) | 37.5 | 42.7 | 46.5 | 48.0 | 50.7 | 35.2 |
| %wt Infrequent (≥1 and <12 days) | 25.6 | 26.7 | 26.6 | 26.3 | 26.2 | 2.3 |
| %wt Moderate (≥12 to <52 days) | 25.2 | 21.1 | 19.8 | 17.6 | 17.2 | −31.7 |
| %wt Frequent (≥52 days) | 11.7 | 9.6 | 7.0 | 8.0 | 5.9 | −49.6 |
| Mean (SD) frequency of use among individuals who consumed them | 35.2 (51.0) | 30.0 (43.4) | 26.8 (42.5) | 28.5 (48.7) | 26.3 (47.5) | −25.3 |
Significant differences were observed between modal ages 21 and 25, based on the Χ2 test of independence for unweighted sample prevalence (p<.001) and ANOVA for unweighted frequency among users (p=.002).
3.2. Trajectories of ED consumption
The trajectory models based on frequency of ED consumption were largely uninformative: the ZIP models did not converge, and the best-fitting model assuming a normal distribution yielded a two-group solution. This convergence problem was likely due to floor effects for the ED variable, for which the frequency of occurrence of zero ranged from 34.5% to 48.3% over the assessment time points. A more informative solution was obtained from the logit models on probability of ED consumption, wherein the four-group solution provided the best fit to the data (see Figure 1). After refitting the four-group solution omitting non-significant quadratic and cubic terms from the polynomials, average probability of group membership was high in all four groups (≥.74, see Figure 1).
Figure 1.
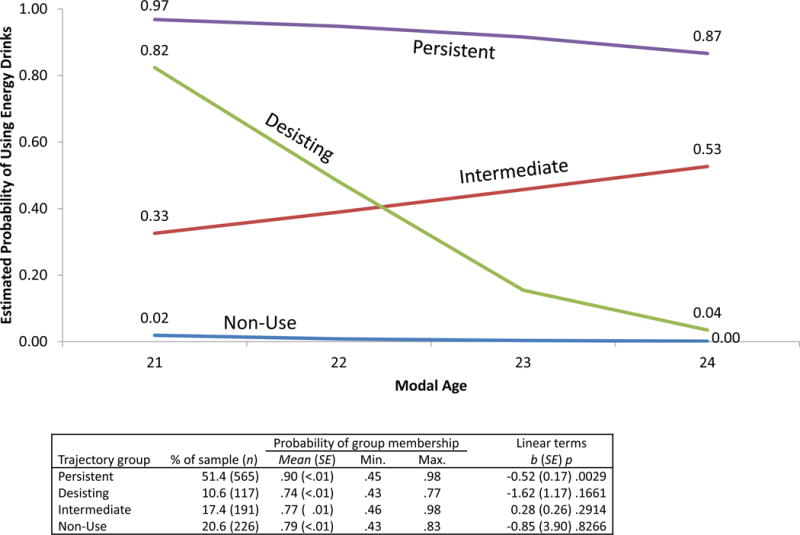
Estimated probability of energy drink consumption during the past year, by modal age and trajectory group membership (n=1099).
Note. Group membership percentages reflect observed proportions in the sample. Corresponding estimated proportions were 49.0%, 12.5%, 21.7%, and 16.8% for Persistent, Desisting, Intermediate, and Non-Use groups, respectively. All quadratic and cubic terms were dropped from the polynomial for each of the four trajectory groups because they were not significant (all ps>.05).
As shown in Figure 1, the resulting four groups can be characterized on the basis of their probability of ED consumption as Desisting (i.e., steadily declining probability), Non-Use (i.e., probability consistently at or near zero), Persistent (i.e., consistently high probability), and Intermediate (i.e., probability ranging between 33% and 53%). A significant overall linear decline in ED consumption probability was observed in the Persistent group [b(SE)= −0.52 (0.17), p=.0029], but the linear terms were non-significant in the other three groups. This was particularly unexpected in the Desisting group, where the decline in probability was steep (from .82 to .04) but still did not attain statistical significance [b(SE)= −1.62(1.17), p=.1661]. For all four trajectory groups, the higher-order terms (quadratic, cubic) were omitted from the final model because they were not significant (all ps>.05).
Half the sample was classified in the Persistent group (51.4%), in which the probability of consuming EDs was consistently high (≥87% during all four years). By contrast, in the Non-Use group, which represented 20.6% of the sample, the probability of past-year ED consumption never exceeded 2%. Individuals classified in the Intermediate trajectory group outnumbered those in the Desisting group (17.4% and 10.6%, respectively).
3.3. Frequency of consumption by trajectory group membership
As shown in Figure 2, individuals with less frequent ED consumption patterns (i.e., 1 to 11 days, and 12 to 51 days) comprised the vast majority of ED consumers in three of the four trajectory groups, whereas the fourth group consistently refrained from any ED consumption (Non-Use, see Figure 2, Panel A). In the Intermediate group (Panel B), the prevalence of infrequent consumption increased more than 3-fold (from 12% at modal age 21 to 44% at age 24) whereas moderate use hovered at or near 10% and frequent use patterns remained scarce (≤4%). In the Desisting group (Panel C), declines were more pronounced for infrequent consumption (64% to 2%) than for moderate (28% to 0%) or frequent (8% to 0%) consumption. The Persistent group (Panel D) was the only group with a substantial proportion of frequent consumers, which declined appreciably over time (24% to 14%), in contrast to a more modest decline in moderate consumption (45% to 36%) and a slight increase in infrequent consumption (31% to 37%).
Figure 2.
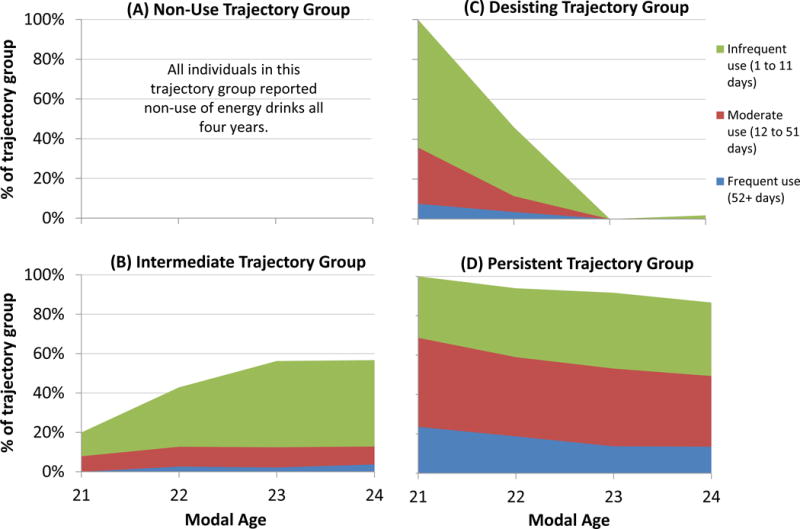
Frequency of energy drink consumption during the past year, by modal age and trajectory group membership (n=1099).
3.4. Correlates of trajectory group membership
ED trajectory group membership was significantly associated with gender and race (ps<.001) such that males and non-Hispanic Whites were overrepresented among the Persistent group (61.0%wt and 70.3%wt, respectively). Males were underrepresented among the Non-Use group (22.2%wt), whereas non-Hispanic Whites were underrepresented among the Intermediate group (58.5%wt; see Table 2). As expected, all three of the psychological risk factors we tested (sensation-seeking, conduct problems, behavioral dysregulation) were positively associated with higher probability of ED consumption, with the Non-Use and Persistent groups having the lowest- and highest-risk scores, respectively (all ps<.001). With respect to alcohol and other substance use at age 21, all of the variables we tested were significantly associated with ED trajectory group membership (all ps<.001). The Non-Use group generally exhibited the lowest level of substance use—with the exception of other caffeine consumption and alcohol use, which were lowest for the Intermediate group—whereas the Persistent group exhibited the highest levels of substance use. The Desisting and Intermediate trajectory groups exhibited intermediate levels of substance involvement, albeit with inconsistent relative rankings and generally modest differences. For example, the proportion who used cocaine during the past year at age 21 ranged from 2.7%wt in the Non-Use group, to 4.9%wt in the Desisting group, to 7.4%wt in the Intermediate group, and 13.1%wt in the Persistent group.
Table 2.
Sample characteristics, by energy drink (ED) trajectory group membership (Nwt=2898)
| Overall sample (Nwt=2898) |
ED trajectory groups
|
||||
|---|---|---|---|---|---|
| Non-Use (nwt=672) |
Desisting (nwt=321) |
Intermediate (nwt=539) |
Persistent (nwt=1366) |
||
|
|
|||||
| %wt Male | 46.9 | 22.2 | 47.9 | 41.3 | 61.0 |
| %wt White, Non-Hispanic | 66.6 | 65.5 | 66.7 | 58.5 | 70.3 |
| %wt College-educated parent(s) | 85.1 | 89.8 | 85.1 | 85.6 | 82.4 |
| Mean (SD) sensation-seeking score | 3.2 (2.1) | 2.7 (2.0) | 2.9 (2.2) | 3.2 (2.0) | 3.6 (2.2) |
| Mean (SD) conduct problems score | 6.2 (4.5) | 4.8 (3.9) | 6.5 (5.1) | 5.6 (4.2) | 7.0 (4.5) |
| Mean (SD) behavioral dysregulation score | 27.6 (11.8) | 25.0 (11.9) | 27.2 (11.3) | 27.5 (11.9) | 28.9 (11.7) |
| %wt ED consumption frequency at age 21 | |||||
| None (0 days) | 38.3 | 100.0 | 0.0 | 81.7 | 0.0 |
| Infrequent (≥1 and <12 days) | 25.5 | 0.0 | 67.7 | 10.5 | 34.1 |
| Moderate (≥12 and <52 days) | 24.7 | 0.0 | 26.2 | 7.8 | 43.2 |
| Frequent (≥52 days) | 11.4 | 0.0 | 6.1 | 0.0 | 22.8 |
| Mean (SD) ED frequency among consumers | 32.7 (49.9) | – | 12.8 (22.9) | 10.6 (10.5) | 39.0 (54.4) |
| Mean (SD) caffeine consumption at age 21 | 100.7 (98.3) | 93.8 (97.8) | 92.3 (85.0) | 86.0 (90.0) | 111.6 (103.4) |
| %wt Alcohol use | |||||
| Age 21 | 95.5 | 92.8 | 94.7 | 92.6 | 98.1 |
| Age 25 | 95.0 | 92.1 | 97.1 | 91.1 | 97.6 |
| %wt Alcohol use disorder (AUD) risk | |||||
| Age 21 | 39.5 | 21.3 | 32.4 | 30.5 | 53.6 |
| Age 25 | 41.6 | 24.4 | 34.0 | 39.6 | 53.2 |
| %wt Tobacco cigarette use | |||||
| Age 21 | 38.8 | 19.4 | 38.5 | 28.4 | 52.5 |
| Age 25 | 26.1 | 10.3 | 24.4 | 25.3 | 35.0 |
| %wt Marijuana use | |||||
| Age 21 | 43.7 | 26.9 | 34.7 | 35.0 | 57.5 |
| Age 25 | 27.8 | 16.2 | 20.8 | 20.4 | 38.8 |
| %wt Nonmedical use of prescription stimulant (NPS) | |||||
| Age 21 | 16.2 | 4.5 | 13.9 | 9.1 | 25.4 |
| Age 25 | 6.3 | 1.1 | 1.1 | 6.5 | 10.2 |
| %wt Cocaine use | |||||
| Age 21 | 8.7 | 2.7 | 4.9 | 7.4 | 13.1 |
| Age 25 | 5.5 | 0.6 | 2.1 | 3.4 | 9.9 |
| %wt Nonmedical use of prescription analgesics (NPA) | |||||
| Age 21 | 8.5 | 1.6 | 8.1 | 6.4 | 12.7 |
| Age 25 | 3.4 | 2.9 | 1.1 | 3.0 | 4.5 |
Note. “Use” reflects prevalent use at least once during the past year. Frequency is the number of days a substance was used during the past year. Age 21 refers to the modal age of the sample in the fourth annual assessment.
Chi-square and ANOVA tests were statistically significant for all characteristics shown (p=.019 for Age 25 NPA; p<.001 for all others).
3.5. Logistic regression predicting Year 8 substance use
As measured at modal age 25, AUD risk, NPS, and cocaine use—but not tobacco, marijuana, or NPA use—were all significantly associated with ED trajectory group membership, after controlling for the effects of demographics, sensation-seeking, other caffeine consumption, and prior substance use at age 21 (see Table 3). Relative to the Non-Use group, individuals in the Persistent group were at significantly higher risk for AUD, NPS, and cocaine use (all ps<.05, see Table 3). Individuals in the Intermediate group were also at increased risk for using NPS [b(SE)=1.32(0.42), p=.002] and cocaine [b(SE)=1.30(0.54), p=.015], relative to the Non-Use group. By contrast, individuals in the Desisting group did not display elevated risk for any of the substance use measures we tested and were significantly less likely than the Non-Use group to report NPA [b(SE)= −1.10(0.50), p=.028]. Examination of pairwise comparisons for NPA (see Figure 3) indicated that the Desisting group also had significantly lower risk than the Intermediate group (p=.02). The findings on AUD risk were less definitive, in that the pairwise comparison between the Persistent and Non-Use groups approached but did not attain statistical significance (p=.074), despite the apparent difference in their respective adjusted means (.52 vs. .38), and despite the significance of the corresponding Chi-square test for the parameter estimate [b(SE)=0.59(0.24), p=.015; see Table 3].
Table 3.
Results [b(standard error)p] of multiple logistic regression predicting substance use at modal age 25 on the basis of energy drink (ED) trajectory group membership (n=863)
| AUD Risk | Tobacco | Marijuana | NPS | NPA | Cocaine | |
|---|---|---|---|---|---|---|
| ED trajectory group | ||||||
| Persistent | 0.59 (0.24) .015 | 0.38 (0.28) .167 | 0.21 (0.25) .406 | 1.09 (0.40) .006 | −0.29 (0.31) .345 | 2.00 (0.50) <.001 |
| Desisting | −0.01 (0.32) .977 | −0.07 (0.36) .839 | −0.09 (0.34) .782 | −0.54 (0.63) .392 | −1.10 (0.50) .028 | 0.56 (0.64) .380 |
| Intermediate | 0.377 (0.27) .162 | 0.27 (0.31) .378 | −0.12 (0.29) .692 | 1.32 (0.42) .002 | 0.13 (0.33) .688 | 1.30 (0.54) .015 |
| Non-Use | Ref. | Ref. | Ref. | Ref. | Ref. | Ref. |
| Gender = Male | 0.35 (0.17) .041 | 0.74 (0.18) <.001 | 0.36 (0.18) .041 | 0.06 (0.20) .746 | 0.77 (0.22) <.001 | 0.66 (0.20) .001 |
| Race/Ethnicity = Non-Hispanic White | 0.02 (0.19) .935 | 0.29 (0.20) .153 | −0.10 (0.20) .631 | 0.36 (0.23) .125 | −0.43 (0.22) .047 | −0.06 (0.23) .786 |
| Parents’ education | ||||||
| Graduate degree | 0.12 (0.25) .632 | −0.50 (0.27) .063 | 0.62 (0.29) .030 | −0.20 (0.28) .466 | −0.36 (0.27) .190 | 0.80 (0.34) .019 |
| Four-year college degree | 0.03 (0.27) .906 | −0.59 (0.29) .041 | 0.50 (0.30) .100 | −0.69 (0.31) .026 | −0.69 (0.31) .027 | 0.82 (0.36) .022 |
| Some college, high school, or less | Ref. | Ref. | Ref. | Ref. | Ref. | Ref. |
| Sensation-seeking | 0.06 (0.04) .134 | 0.07 (0.04) .084 | 0.07 (0.04) .101 | 0.13 (0.05) .006 | 0.17 (0.05) .001 | 0.15 (0.05) .001 |
| Other caffeine consumption/10 | <0.01 (<0.01) .555 | <0.01 (<0.01) .897 | <−0.01 (<0.01) .917 | <0.01 (<0.01) .930 | −0.01 (0.01) .249 | −0.02 (0.01) .066 |
| Prior substance use | 1.12 (0.17) <.001 | 2.38 (0.20) <.001 | 2.14 (0.20) <.001 | 2.36 (0.20) <.001 | 1.78 (0.21) <.001 | 2.62 (0.19) <.001 |
Note. Ref=reference group. Other caffeine consumption (ounces/week) was rescaled by a factor of 10 to enhance interpretability. For each dependent variable, prior substance use is the corresponding substance use measure from modal age 21 (i.e., Year 4). Overall Wald Χ2 (df) p for the ED trajectory group variable was statistically significant for AUD risk (p<.05), NPS (p<.001), and cocaine (p<.001), but not for tobacco, marijuana, or NPA (all ps≥.05). See Figure 3 for results of additional pairwise comparisons between the four ED trajectory groups. AUD=Alcohol use disorder; NPS=Nonmedical use of prescription stimulants; NPA=Nonmedical use of prescription analgesics.
Figure 3.
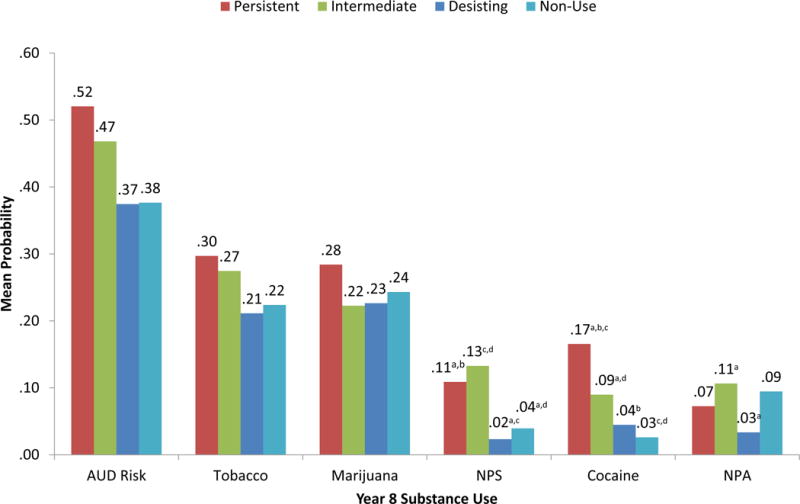
Estimated marginal means for probability of substance use at modal age 25, by energy drink trajectory group membership (n=863).
Note. Results adjusted for the effects of gender, race, parents’ education, sensation-seeking, other caffeine consumption, and the corresponding substance use measure at modal age 21. Matching pairs of superscripted letters denote statistically significant differences in probability of a given substance use outcome (p<.05). A significant difference in NPA is reported between the Desisting and Intermediate groups, but the overall Chi-square for the trajectory group variable did not attain statistical significance in that model (p=.051). AUD=Alcohol use disorder; NPS=Nonmedical use of prescription stimulants; NPA=Nonmedical use of prescription analgesics.
With respect to the background risk factors (gender, race/ethnicity, parents’ education, sensation-seeking, other caffeine consumption, prior substance use), each variable was significantly associated with at least one of the six substance use outcomes we tested (see Table 3), and generally in the expected direction—with the sole exception that other caffeine consumption was not significantly associated with any of the outcomes we tested in the context of the other explanatory variables. Although not a focus of this paper, some noteworthy inconsistencies in the direction of association were observed for parental educational attainment, such that higher attainment was negatively associated with tobacco use, NPS, and NPA, but positively associated with marijuana and cocaine use.
4. Discussion
This study described longitudinal patterns in ED consumption among a young adult sample originally recruited as college students. Overall, higher-frequency use patterns (i.e., ≥52 days/year, and 12 to 51 days/year) declined with age, whereas infrequent use patterns maintained a stable prevalence at approximately 26%wt. Half the sample (51.4%) comprised a Persistent group in which the probability of ED consumption remained at or above 87% throughout the four-year interval studied.
Trajectory group membership was significantly associated with cocaine use, NPS, and AUD risk, but not with marijuana or tobacco use at age 25, with the Persistent and Intermediate trajectory groups having the highest risk, even accounting for prior substance use and other risk factors. These findings suggest that ED consumption might be a novel catalyst for AUD and certain types of subsequent substance use—namely, NPS and cocaine use. Given the significant health and safety concerns associated with substance use during young adulthood (Arria et al., 2016a; Arria et al., 2011b; Caldeira et al., 2012a; Hingson et al., 2005; Kertesz et al., 2007), the current findings are in need of replication to understand if EDs could be a potential target for prevention of subsequent substance use.
Results extend prior cross-sectional studies that have linked ED consumption with alcohol dependence and nonmedical prescription drug use (Arria et al., 2010; Arria et al., 2011a; Miller, 2008a; Woolsey et al., 2014). Importantly, the present findings extend such associations by confirming their presence even in young adulthood, when substance use patterns are more established and fully manifested. Furthermore, the results expand on previous studies by demonstrating that the relationship between EDs and subsequent substance use cannot be entirely accounted for by a general propensity for risk-taking. Finally, because other caffeine consumption was included in the model, it is intriguing that the relationship with substance use outcomes appears to be specific to ED consumption and not to other forms of caffeine. ED consumption might have a unique contributory role for the development and escalation of NPS and cocaine use among young adults. Interestingly, animal studies have supported the notion that caffeine can enhance the reinforcing effects and motivational value of cocaine, especially when co-ingested (O’Neill et al., 2015; Prieto et al., 2016). Earlier research showed an association between caffeine administration and dose-dependent increases in self-administration of stimulants (Schenk et al., 1996). The effect of caffeine on dopamine receptors has been suggested as a mechanism underlying its potentiation of other psychostimulants (Cauli and Morelli, 2005; Ferré, 2016).
Several limitations must be noted. We cannot rule out the possibility of bias related to self-reported recall or social desirability. The loss of 170 participants in the regression analyses, due to missing data, might have resulted in a subsample that was not entirely representative of the larger sample of 1,033 on which the trajectory analyses were conducted. Generalizability is limited due to recruitment from one university with a predominantly non-Hispanic White population. Additionally, this study characterized ED consumption during early adulthood. Therefore, future studies are needed to understand the relationship between ED consumption earlier in life and subsequent drug use, especially given the significant neurodevelopmental changes that occur during adolescence that have an impact on the propensity for addiction. We are unable to clearly distinguish between incident and persistent substance users. However, the significant differences between the trajectory groups in substance use at age 21 suggest that many of the individuals using substances at age 25 had likely been persistent users for several years, and another report on this sample has documented that incident drug use was quite low after age 21 (Arria et al., in press). Finally, the demonstration of a prospective relationship supports but does not prove the existence of a causal relationship between ED consumption and substance use. Efforts to replicate these findings in large longitudinal cohort studies of adolescents are warranted.
Despite the limitations described above, the present findings extend our prior knowledge of EDs in several ways. First, our analyses focus on modeling trajectories of ED consumption during a four-year period. In contrast to static measures of use/non-use, this approach documented the prevalence of different groups of individuals, namely those whose consumption is fleeting from those who go on to sustain their consumption over time. Future studies are needed to investigate other types of health outcomes that might be associated with these different patterns of ED consumption.
Second, we used longitudinal data to test hypotheses that heavier, sustained patterns of ED consumption contribute to the intensification of alcohol-related problems and initiation or continuation of use of other types of stimulant drugs. Importantly, we did not restrict our focus to consumers who co-ingest EDs with alcohol, and therefore increased our flexibility to identify high-risk patterns of ED consumption. Future research is needed to examine the ways in which mixing EDs with alcohol might pose different risks for subsequent use of psychoactive substances than consuming EDs alone.
An intensified research agenda related to EDs is needed to develop better assessment methods, learn more about the long-term consequences of ED consumption, and to begin to fill serious knowledge gaps around this highly prevalent behavior among adolescents and young adults. In particular, future longitudinal studies of younger adolescents should include measures of ED and other caffeine consumption as they have not yet passed through the period of peak risk for initiating illicit drug use, but are likely to have begun to consume EDs (Arria et al., 2014). The lack of empirical information about the long-term relationship between ED consumption and health consequences is a barrier to the development of effective policies governing the regulation and labeling of EDs. Unlike soft drinks, EDs are not subject to any regulation regarding maximum caffeine content, nor labeling requirements for caffeine content (Code of Federal Regulations, 2012). Given previously documented health and safety concerns about EDs, as well as the possibility that ED consumption potentiates other substance use, further research is necessary to inform the prevention and policy efforts to promote young adult health.
Acknowledgments
Funding for this study was provided by the National Institute on Drug Abuse (R01DA14845 and R03DA037936, Dr. Arria, PI). The National Institute on Drug Abuse had no further role in the study design; in the collection, management, analysis, and interpretation of the data; in the writing of the manuscript; or in the decision to submit the paper for publication.
References
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders: DSM-IV. American Psychiatric Press; Washington, DC: 1994. [Google Scholar]
- Arria AM, Caldeira KM, O’Grady KE, Vincent KB, Fitzelle DB, Johnson EP, Wish ED. Drug exposure opportunities and use patterns among college students: Results of a longitudinal prospective cohort study. Subst Abus. 2008;29:19–38. doi: 10.1080/08897070802418451. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Arria AM, Caldeira KM, Kasperski SJ, O’Grady KE, Vincent KB, Griffiths RR, Wish ED. Increased alcohol consumption, nonmedical prescription drug use, and illicit drug use are associated with energy drink consumption among college students. J Addict Med. 2010;4:74–80. doi: 10.1097/ADM.0b013e3181aa8dd4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Arria AM, Caldeira KM, Kasperski SJ, Vincent KB, Griffiths RR, O’Grady KE. Energy drink consumption and increased risk for alcohol dependence. Alcohol Clin Exp Res. 2011a;35:365–375. doi: 10.1111/j.1530-0277.2010.01352.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Arria AM, Caldeira KM, Vincent KB, Garnier-Dykstra LM, O’Grady KE. Substance-related traffic-risk behaviors among college students. Drug Alcohol Depend. 2011b;118:306–312. doi: 10.1016/j.drugalcdep.2011.04.012. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Arria AM, Bugbee BA, Caldeira KM, Vincent KB. Evidence and knowledge gaps for the association between energy drink use and high-risk behaviors among adolescents and young adults. Nutr Rev. 2014;72:87–97. doi: 10.1111/nure.12129. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Arria AM, Caldeira KM, Bugbee BA, Vincent KB, O’Grady KE. Marijuana use trajectories during college predict health outcomes nine years post-matriculation. Drug Alcohol Depend. 2016a;159:158–165. doi: 10.1016/j.drugalcdep.2015.12.009. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Arria AM, Caldeira KM, Bugbee BA, Vincent KB, O’Grady KE. Energy drink use patterns among young adults: Associations with drunk driving. Alcohol Clin Exp Res. 2016b;40:2456–2466. doi: 10.1111/acer.13229. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Arria AM, Caldeira KM, Allen HK, Bugbee BA, Vincent KB, O’Grady KE. Prevalence and incidence of drug use among college students: an 8-year longitudinal analysis. Am J Drug Alcohol Abuse. doi: 10.1080/00952990.2017.1310219. in press. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Berger LK, Fendrich M, Chen HY, Arria AM, Cisler RA. Sociodemographic correlates of energy drink consumption with and without alcohol: Results of a community survey. Addict Behav. 2011;36:516–519. doi: 10.1016/j.addbeh.2010.12.027. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Branum AM, Rossen LM, Schoendorf KC. Trends in caffeine intake among US children and adolescents. Pediatrics. 2014;133:386–393. doi: 10.1542/peds.2013-2877. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Caldeira KM, O’Grady KE, Garnier-Dykstra LM, Vincent KB, Pickworth WB, Arria AM. Cigarette smoking among college students: Longitudinal trajectories and health outcomes. Nicotine Tob Res. 2012a;14:777–785. doi: 10.1093/ntr/nts131. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Caldeira KM, O’Grady KE, Vincent KB, Arria AM. Marijuana use trajectories during the post-college transition: Health outcomes in young adulthood. Drug Alcohol Depend. 2012b;125:267–275. doi: 10.1016/j.drugalcdep.2012.02.022. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Catalano R, Hawkins JD. The social development model: A theory of antisocial behavior. In: Hawkins JD, editor. Delinquency and Crime: Current Theories. Cambridge University Press; New York, NY: 1996. pp. 149–197. [Google Scholar]
- Cauli O, Morelli M. Caffeine and the dopaminergic system. Behav Pharmacol. 2005;16:63–77. doi: 10.1097/00008877-200503000-00001. [DOI] [PubMed] [Google Scholar]
- Code of Federal Regulations. United States Department of Health and Human Services Food and Drug Administration 2012 21CFR182.1180. [Google Scholar]
- Donovan JE, Jessor R. Structure of problem behavior in adolescence and young adulthood. J Consult Clin Psychol. 1985;53:890–904. doi: 10.1037/0022-006X.53.6.890. [DOI] [PubMed] [Google Scholar]
- Falls BJ, Wish ED, Garnier LM, Caldeira KM, O’Grady KE, Vincent KB, Arria AM. The association between early conduct problems and early marijuana use in college students. J Child Adolesc Subst Abuse. 2011;20:221–236. doi: 10.1080/1067828X.2011.581900. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ferré S, O’Brien MC. Alcohol and caffeine: The perfect storm. J Caffeine Res. 2011;1:153–162. doi: 10.1089/caf.2011.0017. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ferré S. Mechanisms of the psychostimulant effects of caffeine: Implications for substance use disorders. Psychopharmacology (Berl) 2016;233:1963–1979. doi: 10.1007/s00213-016-4212-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ferreira SE, Abrahao KP, Souza-Formigoni MLO. Expression of behavioral sensitization to ethanol is increased by energy drink administration. Pharmacol Biochem Behav. 2013;110:245–248. doi: 10.1016/j.pbb.2013.07.014. [DOI] [PubMed] [Google Scholar]
- Franks AM, Schmidt JM, McCain KR, Fraer M. Comparison of the effects of energy drink versus caffeine supplementation on indices of 24-hour ambulatory blood pressure. Ann Pharmacother. 2012;46:192–199. doi: 10.1345/aph.1Q555. [DOI] [PubMed] [Google Scholar]
- Goldfarb M, Tellier C, Thanassoulis G. Review of published cases of adverse cardiovascular events after ingestion of energy drinks. Am J Cardiol. 2014;113:168–172. doi: 10.1016/j.amjcard.2013.08.058. [DOI] [PubMed] [Google Scholar]
- Heckman MA, Sherry K, Gonzalez de Mejia E. Energy drinks: An assessment of their market size, consumer demographics, ingredient profile, functionality, and regulations in the United States. Compr Rev Food Sci Food Saf. 2010;9:303–317. doi: 10.1111/j.1541-4337.2010.00111.x. [DOI] [PubMed] [Google Scholar]
- Hingson R, Heeren T, Winter M, Wechsler H. Magnitude of alcohol-related mortality and morbidity among U.S. college students ages 18–24 Changes from 1998 to 2001. Annu Rev Public Health. 2005;26:259–279. doi: 10.1146/annurev.publhealth.26.021304.144652. [DOI] [PubMed] [Google Scholar]
- Jackson KM, Sher KJ, Schulenberg J. Conjoint developmental trajectories of young adult alcohol and tobacco use. J Abnorm Psychol. 2005;114:612–626. doi: 10.1037/0021-843X.114.4.612. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Jessor R. Problem-behavior theory, psychosocial development, and adolescent problem drinking. Br J Addict. 1987;82:331–342. doi: 10.1111/j.1360-0443.1987.tb01490.x. [DOI] [PubMed] [Google Scholar]
- Johnson EO, Arria AM, Borges G, Ialongo N, Anthony JC. The growth of conduct problem behaviors from middle childhood to early adolescence: Sex differences and the suspected influence of early alcohol use. J Stud Alcohol. 1995;56:661–671. doi: 10.15288/jsa.1995.56.661. [DOI] [PubMed] [Google Scholar]
- Jones BL, Nagin DS, Roeder K. A SAS procedure based on mixture models for estimating development trajectories. Sociol Methods Res. 2001;29:374–393. doi: 10.1177/0049124101029003005. [DOI] [Google Scholar]
- Jones HE, Griffiths RR. Oral caffeine maintenance potentiates the reinforcing and stimulant subjective effects of intravenous nicotine in cigarette smokers. Psychopharmacology (Berl) 2003;165:280–290. doi: 10.1007/s00213-002-1262-4. [DOI] [PubMed] [Google Scholar]
- Juliano LM, Ferre S, Griffiths RR. The pharmacology of caffeine. In: Ries RK, Fiellin DA, Miller SC, Saitz R, editors. Principles of Addiction Medicine. Lippincott Williams & Wilkins; Philadelphia, PA: 2009. pp. 159–178. [Google Scholar]
- Kelly CK, Prichard JR. Demographics, health, and risk behaviors of young adults who drink energy drinks and coffee beverages. J Caffeine Res. 2016;6:73–81. doi: 10.1089/jcr.2015.0027. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kertesz SG, Pletcher MJ, Safford M, Halanych J, Kirk K, Schumacher J, Sidney S, Kiefe CI. Illicit drug use in young and subsequent decline in general health: The Coronary Artery Risk Development in Young Adults (CARDIA) Study. Drug Alcohol Depend. 2007;88:224–233. doi: 10.1016/j.drugalcdep.2006.10.017. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kertesz SG, Khodneva Y, Richman J, Tucker JA, Safford MM, Jones B, Schumacher J, Pletcher MJ. Trajectories of drug use and mortality outcomes among adults followed over 18 years. J Gen Intern Med. 2012;27:808–816. doi: 10.1007/s11606-011-1975-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kristjansson AL, Sigfusdottir ID, Frost SS, James JE. Adolescent caffeine consumption and self-reported violence and conduct disorder. J Youth Adolesc. 2013;42:1053–1062. doi: 10.1007/s10964-013-9917-5. [DOI] [PubMed] [Google Scholar]
- Kumar G, Park S, Onufrak S. Perceptions about energy drinks are associated with energy drink intake among U.S. youth. Am J Health Promot. 2015;29:238–244. doi: 10.4278/ajhp.130820-QUAN-435. [DOI] [PubMed] [Google Scholar]
- Mallett KA, Marzell M, Scaglione N, Hultgren B, Turrisi R. Are all alcohol and energy drink users the same? Examining individual variation in relation to alcohol mixed with energy drink use, risky drinking, and consequences. Psychol Addict Behav. 2014;28:97–104. doi: 10.1037/a0032203. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Marczinski CA, Fillmore MT, Henges AL, Ramsey MA, Young CR. Mixing an energy drink with an alcoholic beverage increases motivation for more alcohol in college students. Alcohol Clin Exp Res. 2013;37:276–283. doi: 10.1111/j.1530-0277.2012.01868.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Meredith SE, Juliano LM, Hughes JR, Griffiths RR. Caffeine use disorder: A comprehensive review and research agenda. J Caffeine Res. 2013;3:114–130. doi: 10.1089/jcr.2013.0016. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mezzich AC, Tarter RE, Giancola PR, Kirisci L. The dysregulation inventory: A new scale to assess the risk for substance use disorder. J Child Adolesc Subst Abuse. 2001;10:35–43. doi: 10.1300/J029v10n04_04. [DOI] [Google Scholar]
- Miller KE. Energy drinks, race, and problem behaviors among college students. J Adolesc Health. 2008a;43:490–497. doi: 10.1016/j.jadohealth.2008.03.003. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Miller KE. Wired: Energy drinks, jock identity, masculine norms, and risk taking. J Am Coll Health. 2008b;56:481–490. doi: 10.3200/JACH.56.5.481-490. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Miller KE, Quigley BM. Energy drink use and substance use among musicians. J Caffeine Res. 2011;1:67–73. doi: 10.1089/jcr.2011.0003. [DOI] [Google Scholar]
- Miller KE. Alcohol mixed with energy drink use and sexual risk-taking: Casual, intoxicated, and unprotected sex. J Caffeine Res. 2012;2:62–69. doi: 10.1089/caf.2012.0015. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Nurco DN, Blatchley RJ, Hanlon TE, O’Grady KE. Early deviance and related risk factors in the children of narcotic addicts. Am J Drug Alcohol Abuse. 1999;25:25–45. doi: 10.1081/ADA-100101844. [DOI] [PubMed] [Google Scholar]
- O’Brien MC, McCoy TP, Rhodes SD, Wagoner A, Wolfson M. Caffeinated cocktails: Energy drink consumption, high-risk drinking, and alcohol-related consequences among college students. Acad Emerg Med. 2008;15:453–460. doi: 10.1111/j.1553-2712.2008.00085.x. [DOI] [PubMed] [Google Scholar]
- O’Brien MC, McCoy TP, Egan KL, Goldin S, Rhodes SD, Wolfson M. Caffeinated alcohol, sensation seeking, and injury risk. J Caffeine Res. 2013;3:59–66. doi: 10.1089/jcr.2013.0004. [DOI] [PMC free article] [PubMed] [Google Scholar]
- O’Neill CE, Levis SC, Schreiner DC, Amat J, Maier SF, Bachtell RK. Effects of adolescent caffeine consumption on cocaine sensitivity. Neuropsychopharmacology. 2015;40:813–821. doi: 10.1038/npp.2014.278. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Packaged Facts. Energy drinks and shots: US market trends. Rockville, MD: p. 2013. [Google Scholar]
- Phan JK, Shah SA. Effect of caffeinated versus noncaffeinated energy drinks on central blood pressures. Pharmacotherapy. 2014;34:555–560. doi: 10.1002/phar.1419. [DOI] [PubMed] [Google Scholar]
- Poulos NS, Pasch KE. Socio-demographic differences in energy drink consumption and reasons for consumption among US college students. Health Educ J. 2015 doi: 10.1177/0017896915578299. [DOI] [Google Scholar]
- Prieto JP, Scorza C, Serra GP, Perra V, Galvalisi M, Abin-Carriquiry JA, Piras G, Valentini V. Caffeine, a common active adulterant of cocaine, enhances the reinforcing effect of cocaine and its motivational value. Psychopharmacology (Berl) 2016;233:2879–2889. doi: 10.1007/s00213-016-4320-z. [DOI] [PubMed] [Google Scholar]
- Reissig CJ, Strain EC, Griffiths RR. Caffeinated energy drinks-A growing problem. Drug Alcohol Depend. 2009;99:1–10. doi: 10.1016/j.drugalcdep.2008.08.001. [DOI] [PMC free article] [PubMed] [Google Scholar]
- SAS Institute Inc. SAS 9.2.SAS Institute Inc. Cary, NC: 2008. [Google Scholar]
- Schenk S, Worley CM, McNamara C, Valadez A. Acute and repeated exposure to caffeine: Effects on reinstatement of extinguished cocaine-taking behavior in rats. Psychopharmacology (Berl) 1996;126:17–23. doi: 10.1007/bf02246406. [DOI] [PubMed] [Google Scholar]
- Seifert SM, Schaechter JL, Hershorin ER, Lipshultz SE. Health effects of energy drinks on children, adolescents, and young adults. Pediatrics. 2011;127:511–528. doi: 10.1542/peds.2009-3592. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Shah SA, Chu BW, Lacey CS, Riddock IC, Lee M, Dargush AE. Impact of acute energy drink consumption on blood pressure parameters: A meta-analysis. Ann Pharmacother. 2016;50:808–815. doi: 10.1177/1060028016656433. [DOI] [PubMed] [Google Scholar]
- Sigmon SC, Griffiths RR. Caffeine choice prospectively predicts positive subjective effects of caffeine and d-amphetamine. Drug Alcohol Depend. 2011;118:341–348. doi: 10.1016/j.drugalcdep.2011.04.018. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Skewes MC, Decou CR, Gonzalez VM. Energy drink use, problem drinking and drinking motives in a diverse sample of Alaskan college students. Int J Circumpolar Health. 2013;72:1–6. doi: 10.3402/ijch.v72i0.21204. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Substance Abuse and Mental Health Services Administration. 2002 National Survey on Drug Use and Health Questionnaire. Rockville, MD: Office of Applied Studies; 2003. [Google Scholar]
- Suerken CK, Reboussin BA, Egan KL, Sutfin EL, Wagoner KG, Spangler J, Wolfson M. Marijuana use trajectories and academic outcomes among college students. Drug Alcohol Depend. 2016;162:137–145. doi: 10.1016/j.drugalcdep.2016.02.041. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Tanda G, Goldberg SR. Alteration of the behavioral effects of nicotine by chronic caffeine exposure. Pharmacol Biochem Behav. 2000;66(00):47–64. 00234–3. doi: 10.1016/S0091-3057. [DOI] [PubMed] [Google Scholar]
- Terry-McElrath YM, O’Malley PM, Johnston LD. Energy drinks, soft drinks, and substance use among United States secondary school students. J Addict Med. 2014;8:6–13. doi: 10.1097/01.ADM.0000435322.07020.53. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Trapp GSA, Allen KL, O’Sullivan T, Robinson M, Jacoby P, Oddy WH. Energy drink consumption among young Australian adults: Associations with alcohol and illicit drug use. Drug Alcohol Depend. 2014;134:30–37. doi: 10.1016/j.drugalcdep.2013.09.006. [DOI] [PubMed] [Google Scholar]
- Velazquez CE, Poulos NS, Latimer LA, Pasch KE. Associations between energy drink consumption and alcohol use behaviors among college students. Drug Alcohol Depend. 2012;123:167–172. doi: 10.1016/j.drugalcdep.2011.11.006. [DOI] [PubMed] [Google Scholar]
- Vincent KB, Kasperski SJ, Caldeira KM, Garnier-Dykstra LM, Pinchevsky GM, O’Grady KE, Arria AM. Maintaining superior follow-up rates in a longitudinal study: Experiences from the College Life Study. Int J Mult Res Approach. 2012;6:56–72. doi: 10.5172/mra.2012.6.1.56. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Woolsey CL, Barnes LB, Jacobson BH, Kensinger WS, Barry AE, Beck NC, Resnik AG, Evans MW. Frequency of energy drink use predicts illicit prescription stimulant use. Subst Abus. 2014;35:96–103. doi: 10.1080/08897077.2013.810561. [DOI] [PubMed] [Google Scholar]
- Woolsey CL, Williams RD, Jr, Jacobson BH, Housman JM, McDonald JD, Swartz JH, Evans MW, Jr, Sather TE, Barry AE, Davidson RT. Increased energy drink use as a predictor of illicit prescription stimulant use. Subst Abus. 2015;36:413–419. doi: 10.1080/08897077.2014.969470. [DOI] [PubMed] [Google Scholar]
- Worthley MI, Prabhu A, De Sciscio P, Schultz C, Sanders P, Willoughby SR. Detrimental effects of energy drink consumption on platelet and endothelial function. Am J Med. 2010;123:184–187. doi: 10.1016/j.amjmed.2009.09.013. [DOI] [PubMed] [Google Scholar]
- Zuckerman M, Kuhlman DM. Personality and risk taking: Common biosocial factors. J Pers. 2000;68:999–1029. doi: 10.1111/1467-6494.00124. [DOI] [PubMed] [Google Scholar]
- Zuckerman M. Zuckerman-Kuhlman Personality Questionnaire (ZKPQ): An alternative five-factorial model. In: de Raad B, Perugini M, editors. Big Five Assessment. Hogrefe & Huber; Seattle, WA: 2002. pp. 377–396. [Google Scholar]