

Abstract
Background and study aims
Recent literature suggests that chemo(radio)therapy might reduce the patency of plastic stents in patients with malignant biliary obstruction. Whether this might also be valid for other types of stents is unknown. The aim of this study was to determine the influence of chemo(radio)therapy on the patency of fully-covered self-expandable metal stents (FCSEMSs) and plastic stents.
Patients and methods
We retrospectively reviewed the electronic medical records of patients with distal malignant biliary obstruction who underwent biliary stent placement between April 2001 and July 2015. Primary outcome was duration of stent patency. Secondary outcome was stent patency at 3 and 6 months. We used Kaplan–Meier survival analyses to compare stent patency rates between patients who received chemo(radio)therapy and patients who did not.
Results
A total of 291 biliary stents (151 metal and 140 plastic) were identified. The median cumulative stent patency of FCSEMSs did not differ between patients receiving chemo(radio)therapy (n = 51) and those (n = 100) who did not ( P = 0.70, log-rank test). The estimated cumulative stent patency of plastic stents was also comparable in 99 patients without and 41 patients with chemo(radio)therapy ( P = 0.73, log-rank test). At 3 and 6 months, FCSEMS patency rates were 87 % and 83 % in patients without chemo(radio)therapy and 96 % and 83 % in patients with therapy, respectively. Plastic patency rates were 69 % and 55 % in patients without and 85 % and 39 % in patients with therapy, respectively. After 1 year, 78 % of the FCSEMSs were still patent in patients without chemo(radio)therapy and 69 % of the FCSEMSs were still patent in patients with therapy.
Conclusion
Our data indicate that chemo(radio)therapy does not reduce the patency of biliary fully-covered metal and plastic stents.
Introduction
In Europe and the United States, pancreatic cancer is, respectively, the 6th and 4th leading cause of cancer-related deaths 1 2 . Only 15 – 20 % of patients are candidates for surgery, because in the majority, the cancer has already spread to other parts of the body or there is locally advanced disease at the time of diagnosis 3 . Even after complete surgical resection, long-term survival is rare as a result of local recurrence or distant metastases 4 .
Therefore, chemo(radio)therapy is increasingly used in the hope of improving long-term survival. Unfortunately, the use of adjuvant chemo(radio)therapy has shown no considerable improvements in overall survival 5 . Neoadjuvant therapy seems to offer the possibility of downstaging borderline resectable tumors into resectable tumors 6 . And secondly, it implies enhanced survival in the case of resectable tumors by increasing the R0 resection rate 7 .
Approximately 70 % of patients with periampullary tumors develop jaundice during the course of their disease due to malignant biliary obstruction 8 . Chemotherapy requires a normal liver function to avoid toxicity and therefore, adequate biliary drainage 9 . Endoscopic biliary retrograde cholangiopancreaticography (ERCP) with biliary stent placement is the preferred method over percutaneous stent placement and surgical bypass 10 11 . Accumulating evidence shows that self-expandable metal stents (SEMSs) are superior to plastic stents in terms of stent patency 12 .
In theory, chemo(radio)therapy might reduce stent patency, as immunosuppression can result in bacterial colonization of the stent 13 14 15 16 . Plastic stents in particular might be susceptible to early stent dysfunction during chemo(radio)therapy, as biofilm and sludge formation are the main causes of plastic stent dysfunction, while fully-covered self-expandable metal stents (FCSEMSs) are prone to migration 17 18 19 . Several clinical studies have supported this hypothesis by showing that the use of chemo(radio)therapy reduces the patency of plastic stents, while SEMSs seem to maintain patency during the time required for patients to complete neoadjuvant therapy 13 14 15 20 21 22 23 24 . However, other studies could not establish an effect of chemo(radio)therapy on either plastic or metal stent patency 16 25 26 . Because of these heterogeneous results, we sought to clarify the influence of chemo(radio)therapy on biliary stents in this retrospective study. Therefore, we investigated the stent patency rates of FCEMSs and plastic stents in patients with distal malignant biliary obstruction who received chemo(radio)therapy and patients who did not receive chemo(radio)therapy. We hypothesized that the patency of both stent types is not reduced by chemo(radio)therapy.
Patients and methods
Study design and patients
We performed a retrospective analysis of a prospective endoscopic database (Endobase: Olympus Medical Systems Europe, Hamburg, Germany) in the Academic Medical Center (AMC), a tertiary referral center in the Netherlands. The Medical Ethics Review Committee of the Academic Medical Center in Amsterdam confirmed that the Dutch Medical Research Involving Human Subjects Act did not apply to the current study and that an official approval was not required.
We identified patients who had undergone biliary drainage with a FCSEMS or plastic stent for malignant biliary obstruction. We included patients who were treated with chemo(radio)therapy between April 2001 and July 2015. Patients who had undergone plastic stent placement and who did not receive chemo(radio)therapy were included between July 2010 and July 2015. Reports of the endoscopic procedures were reviewed to identify patients with distal common bile duct obstruction caused by pancreatic cancer or distal cholangiocarcinoma. All patients were included regardless of tumor resectability. Furthermore, we included patients who received neoadjuvant therapy as well as palliative therapy. The oncologic therapy regimes were chosen by an oncologist and the majority of patients participated in clinical trials. Patients with malignant obstruction at the level of the hilum caused by a proximal cholangiocarcinoma or gallbladder malignancy, were excluded from the study because hilar obstructions cannot be drained with FCSEMSs. Ampullary carcinomas were excluded because chemo(radio)therapy is not recommended for this type of tumor. Moreover, patients were excluded if they received an uncovered SEMS. Finally, we excluded patients who had undergone percutaneous biliary drainage simultaneously.
Data collection
In order to collect data, we reviewed stent placement procedures and electronic medical records for all selected patients. We collected data on patient demographics (gender, age) and tumor characteristics which included type of tumor, resectability and presence of histological or cytological confirmation of the diagnosis. All endoscopic procedures were performed or supervised by an experienced therapeutic endoscopist. Stent type, length and diameter were at the discretion of the endoscopist. Furthermore, we collected data on the type and timing of chemo(radio)therapy, duration of stent patency, stent patency at 3 and 6 months after placement, and the reason for stent exchange. In order to collect all data, we contacted referral centers if a patient received local care after stent insertion. Likewise, we contacted general practitioners to determine the day of death when electronic medical records lacked this information in our institution.
Study outcomes
The primary outcome was the duration of stent patency. Stent patency was defined as the time between stent placement and stent exchange due to dysfunction. Stent dysfunction was suspected when patients presented with increased cholestasis or cholangitis necessitating stent exchange by ERCP as judged by the clinician. Secondary outcome was plastic stent and FCSEMS patency at 3 and 6 months and FCSEMS patency at 1 year.
Follow-up
Patients were followed until they underwent elective stent exchange, experienced stent dysfunction, died, or underwent surgical pancreatoduodenectomy or palliative hepaticojejunostomy. If none of these end points had occurred, the follow-up ended 1 year after stent insertion.
Statistical analysis
Each stent placement was recorded as an independent event, considering that each patient may have received multiple stents during the course of their treatment. Descriptive statistics were used to describe the population. Continuous variables with a normal distribution were summarized using means and standard deviations (SD), whereas medians and interquartile ranges (IQR) or ranges were used for skewed distributions. Categorical variables were summarized using numbers and percentages. Comparisons between the groups with and without chemo(radio)therapy were performed with the independent samples t test for continuous variables with a normal distribution. The Chi-squared test was used for categorical variables and Fisher’s exact test in cases where cell count was less than five. A probability ( P ) value of 0.05 or smaller was considered to imply statistical significance and all reported P values are two-sided. Cumulative stent patency rates were estimated using Kaplan – Meier analysis and life table analyses. Censored cases included patients who underwent elective stent exchange, patients who underwent stent removal during surgery, and patients who had died before stent dysfunction had occurred within 1 year of follow-up. In addition, patients were censored in cases when stent dysfunction did not occur within 1 year after stent insertion. The log-rank test was used to compare the cumulative stent patency of FCSEMSs and plastic stents with and without chemo(radio)therapy. All analyses were performed using SPSS software version 22 (SPSS, Inc, Chicago, Illinois, United States).
Results
Baseline characteristics
In total, 266 patients were included in this study, and a total of 291 biliary stents were placed between April 2001 and July 2015. Of these, 151 were FCSEMSs and 140 were plastic stents (10 French). Baseline characteristic are summarized in Table 1 . The mean age of the overall cohort was 65.6 ± 10.3 years, and 185 (63.6 %) stents were placed in male patients. The majority of patients (82.8 %) suffered from pancreatic cancer, and a tissue diagnosis was present in 88.3 % of all patients. About one-third (35.1 %) of the stents were placed in patients with resectable tumors and 92 of 291 stents (31.6 %) were placed in patients receiving chemo(radio)therapy. The majority (71.1 %) were treated with gemcitabine-based chemo(radio)therapy (see Supplementary Table 1 for details with regard to type of chemotherapy).
Table 1. Baseline characteristics of patients included in this study.
| Total | FCSEMS | FCSEMS + C(R)T | P value | Plastic stent | Plastic stent + C(R)T | P value | |
| Total no. of stents, n (%) | 291 (100) | 100 (66.2) | 51 (33.8) | n/a | 99 (70.7) | 41 (29.3) | n/a |
| Age, mean ± SD, years | 65.6 ± 10.3 | 67.3 ± 10.8 | 65.1 ± 9.1 | 0.22 | 66.9 ± 9.2 | 58.8 ± 10.2 | < 0.05 |
| Male, n (%) | 185 (63.6) | 54 (54) | 35 (68.6) | 0.08 | 66 (66.7) | 30 (73.2) | 0.45 |
| Type of tumor, n. (%) | 0.14 | < 0.05 | |||||
|
241 (82.8) | 81 (81) | 46 (90.2) | 74 (74.7) | 40 (97.4) | ||
|
50 (17.2) | 19 (19) | 5 (9.8) | 25 (25.3) | 1 (2.4) | ||
| Resectability, n (%) | < 0.05 | < 0.05 | |||||
|
186 (63.9) | 52 (52) | 45 (88.2) | 53 (53.5) | 36 (87.8) | ||
|
102 (35.1) | 45 (45) | 6 (11.8) | 46 (46.5) | 5 (12.2) | ||
|
3 (1) | 3 (3) | n/a | n/a | n/a | ||
| Systemic therapy, n (%) | n/a | n/a | |||||
|
199 (68.4) | 100 (100) | n/a | 99 (100) | n/a | ||
|
58 (19.9) | n/a | 37 (72.5) | n/a | 21 (51.2) | ||
|
34 (11.7) | n/a | 14 (27.5) | n/a | 20 (48.8) | ||
| Timing of C(R)T, n (%) | n/a | n/a | |||||
|
20 (21.7) | n/a | 10 (19.6) | n/a | 10 (24.4) | ||
|
72 (78.3) | n/a | 41 (80.4) | n/a | 31 (75.6) |
FCSEMS, fully-covered self-expandable metal stent; C(R)T, chemo(radio)therapy.
Supplementary Table 1. Overview of chemotherapy regimes.
|
FCSEMS + C(R)T
n (%) |
Plastic stent + C(R)T
n (%) |
|
| Gemcitabine | 8 (15.7) | 10 (24.4) |
| Gemcitabine + cisplatin | 3 (5.9) | n/a |
| Gemcitabine + capecitabine | n/a | 1 (2.4) |
| Gemcitabine + erlotinib | n/a | 1 (2.4) |
| Gemcitabine + erlotinib + metformin/placebo | 9 (17.6) | 1 (2.4) |
| Gemcitabine + erlotinib + bevacizumab/placebo | n/a | 1 (2.4) |
| Gemcitabine + nadroparin | 3 (5.9) | 2 (4.9) |
| Gemcitabine + etalocib/placebo | n/a | 2 (4.9) |
| Gemcitabine + RT | 9 (17.6) | 7 (17.1) |
| Gemcitabine + nelfinavir + RT | 1 (2) | 5 (12.2) |
| Gemcitabine + panitumumab + RT | 1 (2) | n/a |
| Folfirinox | 11 (21.6) | 1 (2.4) |
| Capecitabine + everolimus | n/a | 1 (2.4) |
| Capecitabine + celecoxib + nadroparin | 1 (2) | n/a |
| 5FU | n/a | 1 (2.4) |
| 5FU + RT | n/a | 1 (2.4) |
| 5FU + leucovorin + RT | n/a | 1 (2.4) |
| 5FU + leucovorin + celecoxib + RT | 3 (5.9) | 6 (14.6) |
| Unknown | 2 (3.9) | n/a |
| Total | 51 (100) | 41 (100) |
RT, radiotherapy; 5FU, fluorouracil; FCSEMS, fully-covered self-expandable metal stent; C(R)T, chemo(radio)therapy.
Apart from tumor resectability, there were no differences in baseline characteristics between the two groups with FCSEMSs. In the case of plastic stents, patients with chemo(radio)therapy were younger, suffered more frequently from pancreatic cancer, and the tumors were more often unresectable ( Table 1 ).
Stent patency
The primary outcome per group is summarized in Table 2 . The overall median patency of FCSEMSs without chemotherapy was 36 days [IQR 21 – 90 days]. In total, 44 patients (44 %) underwent surgery after a median preoperative drainage time of 29 days [IQR 22 – 38 days]. Ten stents (10 %) were exchanged prematurely after a median of 16 days [IQR 8 – 91 days]. Premature exchange was performed in the case of stent dysfunction. Reasons for stent dysfunction are included in Table 3 . The overall median patency of FCSEMSs in patients receiving chemo(radio)therapy was 191 days [IQR 119 – 365 days]. Eight stents (15.7 %) were removed at surgery after 123 days [IQR 107 – 157] and 10 stents (19.6 %) were exchanged prematurely after a median of 126 days [IQR 96 – 291 days]. A total of 12 FCSEMSs were still patent after maximum follow-up of 1 year in the group of patients who were treated with chemo(radio)therapy.
Table 2. Stent patency data.
| Stents placed, n (%) | Median patency, days, [IQR] or (range) 1 | |
| FCSEMS | ||
| Total no. of stents | 100 (100) | 36 [21 – 90] |
| Elective exchange | 1 (1) | 73 |
| Premature exchange | 10 (10) | 16 [8 – 91] |
| Others | ||
|
44 (44) | 29 [22 – 38] |
|
38 (38) | 80 [20 – 177] |
|
7 (7) | 365 |
| FCSEMS + C(R)T | ||
| Total no. of stents | 51 (100) | 191 [119 – 365] |
| Elective exchange | n/a | n/a |
| Premature exchange | 10 (19.6) | 126 [96 – 291] |
| Others | ||
|
8 (15.7) | 123 [107 – 157] |
|
21 (41.2) | 191 [112 – 249] |
|
12 (23.5) | 365 |
| Plastic stent | ||
| Total no. of stents | 99 (100) | 38 [23 – 58] |
| Elective exchange | 2 (2) | 48 (41 – 54) |
| Premature exchange | 24 (24.2) | 38 [19 – 88] |
| Others | ||
|
55 (55.6) | 34 [22 – 46] |
|
17 (17.2) | 112 [51 – 195] |
|
1 (1) | 365 |
| Plastic stent + C(R)T | ||
| Total no. of stents | 41 (100) | 133 [96 – 214] |
| Elective exchange | 2 (4.9) | 201 (126 – 276) |
| Premature exchange | 27 (65.9) | 127 [91 – 157] |
| Others | ||
|
3 (7.3) | 94 [41 – 133] |
|
8 (19.5) | 183 [135 – 263] |
|
1 (2.4) | 365 |
FCSEMS, fully-covered self-expandable metal stent; C(R)T, chemo(radio)therapy; IQR, interquartile range.
Range: is used in the case of insufficient data for constructing IQR.
One year after stent insertion.
Table 3. Reasons for stent dysfunction.
|
FCSEMS
(n = 10) |
FCSEMS + C(R)T
(n = 10) |
Plastic stent
(n = 24) |
Plastic stent + C(R)T
(n = 27) |
|
| Sludge formation | 4 | 2 | 11 | 12 |
| Stent migration | 4 | 6 | 5 | 3 |
| Tumor overgrowth | 1 | 2 | 0 | 0 |
| Other 1 | 1 | 0 | 2 | 0 |
| Unknown | 0 | 0 | 6 | 12 |
FCSEMS, fully-covered self-expandable metal stent; C(R)T, chemo(radio)therapy
Other: combination of sludge formation and stent migration, cholecystitis, choledocholithiasis.
The overall median patency of plastic stents was 38 days [IQR 23 – 58 days] in patients who did not receive chemo(radio)therapy. Twenty-four stents (24.2 %) were exchanged prematurely after a median of 38 days [IQR 19 – 88 days]. Finally, in the group of plastic stents with chemo(radio)therapy, the overall median patency was 133 days [IQR 96 – 214 days]. In this group, 27 stents (65.9 %) were exchanged prematurely after a median of 127 days [IQR 91 – 157 days].
Cumulative stent patency
The Kaplan – Meier curves for estimated cumulative stent patency are shown in Fig. 1 . Ninety percent of the FCSEMSs without chemo(radio)therapy and 80.4 % of the FCSEMSs with chemo(radio)therapy were censored. A more detailed overview of the censored cases is presented in Fig. 2 . The estimated cumulative stent patency of FCSEMSs did not differ between patients receiving chemo(radio)therapy and those who did not ( P = 0.70, log-rank test). Both medians were not reached. The rate of censored cases in the group of plastic stents without chemo(radio)therapy was 75.8 %, and 34.1 % in the group with chemo(radio)therapy ( Fig. 2 ). The estimated cumulative stent patency of plastic stents was comparable in patients with (median: 144 days [95 %CI:125 – 163]) and without (median: 182 days [95 %CI: 103 – 261]) chemo(radio)therapy ( P = 0.73, log-rank test).
Fig. 1.
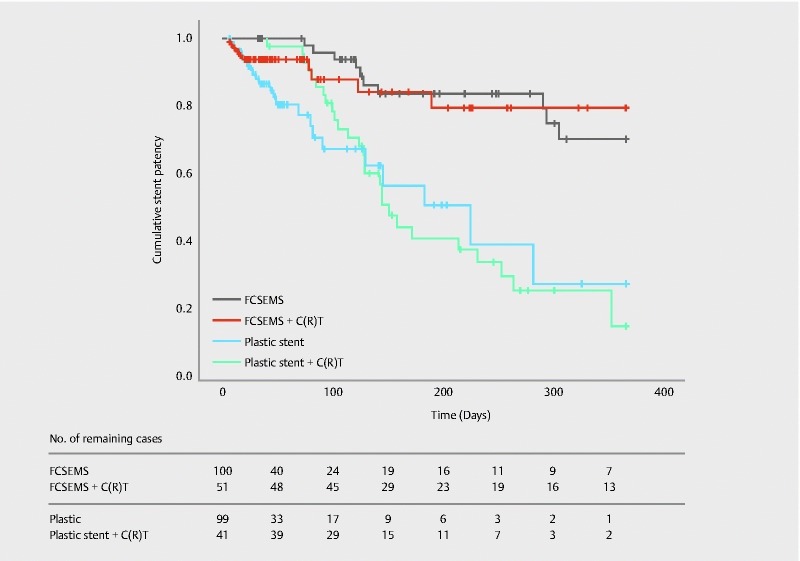
Kaplan-Meier curves showing cumulative stent patency. FCSEMS: fully-covered self-expandable metal stent; C(R)T: chemo(radio)therapy.
Fig. 2.
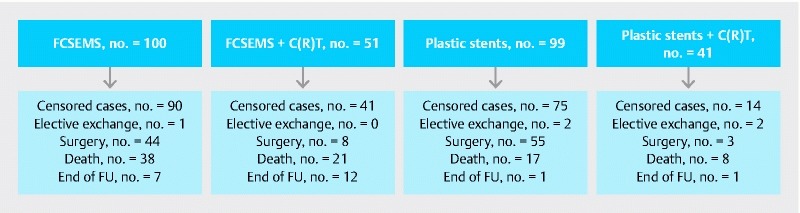
Overview of censored cases. FCSEMS: fully-covered self-expandable metal stent; C(R)T: chemo(radio)therapy; FU: follow-up.
Cumulative stent patency at 3 and 6 months
Life table analysis showed FCSEMS patency rates of 87 % at 3 months, 83 % at 6 months and 78 % at 1 year in patients who did not receive chemo(radio)therapy. In patients who were treated with chemo(radio)therapy, the patency rates of FCSEMSs were 96 % at 3 months, 83 % at 6 months, and 69 % at 1 year. Plastic patency rates were 69 % and 55 % at, respectively 3 and 6 months in patients without chemo(radio)therapy, and 85 % and 39 % in patients with chemo(radio)therapy.
Discussion
This retrospective study determined the potential influence of chemo(radio)therapy on the patency of biliary stents in patients with malignant biliary obstruction. We hypothesized that the patency of FCSEMSs and plastic stents is not reduced by chemo(radio)therapy. Our data confirmed this hypothesis by revealing no difference in cumulative stent patency rates for FCSEMSs, as well as plastic stents.
After 3 months, 96 % of the FCSEMSs were still patent in patients with chemo(radio)therapy, and 87 % of the FCSEMSs in patients without therapy ( Fig. 1 ). After 6 months, stent patency rates were 83 % in both groups. These stent patency rates are clinically relevant since most neoadjuvant therapy regimes last approximately 3 – 6 months. In an earlier retrospective analysis of 80 patients who underwent palliative chemo(radio)therapy, life table analysis showed similar FCSEMS patency rates of 97 % at 3 months and 85 % at 6 months 27 . Our study further expanded the literature, because we also provided data showing that patency rates of FCSEMSs in patients who did not receive chemo(radio)therapy during the same time frame, did not differ. Furthermore, two earlier Japanese studies support our data, because they found no effect of chemotherapy on metal stent patency 25 26 .
To the best of our knowledge, only one small prospective randomized study has been conducted with regard to FCSEMS patency in patients with a malignant obstruction, receiving neoadjuvant therapy. In that study, 54 patients were randomized to receive a FCSEMS, uncovered SEMS (USEMS) or plastic stent. The outcome variables of interest were the time to stent occlusion, attempted surgical resection or death after the initiation of neoadjuvant therapy. The mean time to stent occlusion was significantly longer in FCSEMSs compared with USEMSs and plastic stents (220 days vs 74 days and 76 days, P < 0.01) 24 . However, the use of mean times to stent occlusion represents a statistical limitation. Stent occlusion was only observed in 21 patients because others underwent surgery (n = 18) or had died (n = 15) before stent occlusion had occurred. Calculating the mean time to stent occlusion with only the measurements of patients who experienced stent occlusion could have underestimated or overestimated the time to stent occlusion. On the other hand, Kaplan – Meier survival analysis enables all of the information available to be used by taking account of the patients who underwent surgery or died when estimating the cumulative stent patency time. Furthermore, that study lacked controls who did not receive chemo(radio)therapy.
Additionally, our data did not show a difference in cumulative patency of plastic stents between patients who did and who did not receive chemo(radio)therapy. However, the premature stent exchange rates, 24.2 % in patients without chemo(radio)therapy vs. 65.9 % in patients with chemo(radio)therapy, respectively, seem to be inconsistent with the previously drawn conclusion ( Table 2 ). But the discrepancy between the low premature exchange rate in patients without therapy and the high rate in patients with therapy can be explained by the fact that more than half of the stents in the group without chemo(radio)therapy were removed during surgery within 1 month. Hence, these stents never had the chance to become occluded.
At least two earlier studies refuted the claim that chemo(radio)therapy might reduce the patency of plastic stents 16 28 . Our results confirm the findings of an earlier small trial by Lofts et al. 16 . They performed a retrospective study in 80 patients with a malignant biliary obstruction caused by heterogeneous primary tumors of whom 39 received a plastic biliary stent. The median stent patency in that study did not differ between patients with and without chemotherapy (105 vs. 119 days, respectively). On the other hand, a recently published trial suggested that chemo(radio)therapy reduces the patency of plastic biliary stents 13 . That retrospective trial included 173 patients with borderline resectable pancreatic cancer who underwent neoadjuvant chemo(radio)therapy. A total of 233 plastic stents were placed, and 35.6 % of the plastic stents were exchanged prematurely after a median of 49 days. The authors suggested shortening the interval for elective exchange, as only 34.3 % of the plastic stents remained patent at the recommended exchange interval of 3 months. Unfortunately, that study lacked a control group of patients who did not receive chemo(radio)therapy during the same time frame. Another retrospective study (n = 49) concluded similarly to Ge et al. that plastic stents do not maintain patency during the time required for completing neoadjuvant therapy. However, stent patency rates at 3 and 6 months were not provided in that study 20 .
The median stent patency rates shown in Table 2 require some clarification. We considered the median stent patency less appropriate to compare stent patency rates between groups with and without chemo(radio)therapy than estimations of the cumulative stent patency ( Fig. 1 ). However, the median stent patency rates are shown because they provide extra insights, even though the outcomes are biased due to an unequal patient distribution. The short overall median stent patency durations in patients without therapy (36 days with FCSEMSs and 38 days with plastic stents) most likely reflect the shorter preoperative drainage times in these patient groups as patients without chemo(radio)therapy underwent immediate surgery, whereas patients with chemo(radio)therapy underwent surgery after completion of neoadjuvant therapy. Also the surprisingly short patency of prematurely exchanged stents in patients without chemo(radio)therapy needs explanation: 16 days with FCSEMSs and 38 days with plastic stents. Of all placed stents (n = 291), 14 were prematurely exchanged within 3 weeks after placement, mainly due to persistent cholestasis caused by early stent migration or persistent biliary sludge. Even if they would have been scheduled for chemotherapy, the patients who received these stents were likely to end up in the non-chemo(radio)therapy groups, since inadequate biliary drainage prohibited these patients from starting chemotherapy.
The abovementioned results should be interpreted taking into account several limitations. First, the retrospective nature of data collection is subject to bias, and its nonrandomized nature caused inequalities in patient characteristics. The second limitation of this study concerns the statistical analysis. We had to take the presence of many censored cases into account and the retrospective data collection contributed to a different distribution of censored cases across the groups. A final possible limitation is that we might have missed events of stent dysfunction or elective stent exchange if a patient received local care after stent insertion. Consequently, this could have caused overestimation of stent patency.
Conclusion
Our retrospective data indicate that chemo(radio)therapy does not reduce the patency of biliary stents. Furthermore, our data do not support the suggestion to shorten the regular intervals for stent exchange in patients with malignant biliary obstruction receiving chemo(radio)therapy.
Footnotes
Competing interests None
References
- 1.Ferlay J, Steliarova-Foucher E, Lortet-Tieulent J et al. Cancer incidence and mortality patterns in Europe: Estimates for 40 countries in 2012. Eur J Cancer. 2013;49:1374–1403. doi: 10.1016/j.ejca.2012.12.027. [DOI] [PubMed] [Google Scholar]
- 2.Siegel R L, Miller K D, Jemal A. Cancer statistics, 2015. CA Cancer J Clin. 2015;65:5–29. doi: 10.3322/caac.21254. [DOI] [PubMed] [Google Scholar]
- 3.SEER Cancer Statistics Factsheets: Pancreas Cancer Bethesda, Maryland: National Cancer Institute; 2015. Available from:http://seer.cancer.gov/statfacts/html/pancreas.htmlAccessed: 25 October 2015
- 4.Sperti C, Pasquali C, Piccoli A et al. Recurrence after resection for ductal adenocarcinoma of the pancreas. World J Surg. 1997;21:195–200. doi: 10.1007/s002689900215. [DOI] [PubMed] [Google Scholar]
- 5.Oettle H, Post S, Neuhaus P et al. Adjuvant chemotherapy with gemcitabine vs observation in patients undergoing curative-intent resection of pancreatic cancer. JAMA. 2007;297:267–277. doi: 10.1001/jama.297.3.267. [DOI] [PubMed] [Google Scholar]
- 6.Gillen S, Schuster T, Meyer Zum Büschenfelde C et al. Preoperative/neoadjuvant therapy in pancreatic cancer: a systematic review and meta-analysis of response and resection percentages. PLoS Med. 2010;7:e1000267. doi: 10.1371/journal.pmed.1000267. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Artinyan A, Anaya D A, McKenzie S et al. Neoadjuvant therapy is associated with improved survival in resectable pancreatic adenocarcinoma. Cancer. 2011;117:2044–2049. doi: 10.1002/cncr.25763. [DOI] [PubMed] [Google Scholar]
- 8.Lillemoe K D, Pitt H A. Palliation. Surgical and otherwise. Cancer. 1996;78:605–614. doi: 10.1002/(SICI)1097-0142(19960801)78:3<605::AID-CNCR41>3.0.CO;2-#. [DOI] [PubMed] [Google Scholar]
- 9.Eklund J W, Trifilio S, Mulcahy M F.Chemotherapy dosing in the setting of liver dysfunction Oncology (Williston Park) 2005191057–1063.; discussion 1063-1064, 1069 [PubMed] [Google Scholar]
- 10.Speer A G, Cotton P B, Russel R C et al. Randomised trial of endoscopic versus percutaneous stent insertion in malignant obstructive jaundice. Lancet. 1987;2:57–62. doi: 10.1016/s0140-6736(87)92733-4. [DOI] [PubMed] [Google Scholar]
- 11.Smith A C, Dowsett J F, Russell R C et al. Randomised trial of endoscopic stenting versus surgical bypass in malignant low bileduct obstruction. Lancet. 1994;344:1655–1660. doi: 10.1016/s0140-6736(94)90455-3. [DOI] [PubMed] [Google Scholar]
- 12.Almadi M A, Barkun A, Martel M. Plastic vs. self-expandable metal stents for palliation in malignant biliary obstruction: a series of meta-analyses. Am J Gastroenterol. 2017;112:260–273. doi: 10.1038/ajg.2016.512. [DOI] [PubMed] [Google Scholar]
- 13.Ge P S, Hamerski C M, Watson R R et al. Plastic biliary stent patency in patients with locally advanced pancreatic adenocarcinoma receiving downstaging chemotherapy. Gastrointest Endosc. 2015;81:360–366. doi: 10.1016/j.gie.2014.08.020. [DOI] [PubMed] [Google Scholar]
- 14.Adams M A, Anderson M A, Myles J D et al. Self-expanding metal stents (SEMS) provide superior outcomes compared to plastic stents for pancreatic cancer patients undergoing neoadjuvant therapy. J Gastrointest Oncol. 2012;3:309–313. doi: 10.3978/j.issn.2078-6891.2011.050. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Aadam A A, Evans D B, Khan A et al. Efficacy and safety of self-expandable metal stents for biliary decompression in patients receiving neoadjuvant therapy for pancreatic cancer: a prospective study. Gastrointest Endosc. 2012;76:67–75. doi: 10.1016/j.gie.2012.02.041. [DOI] [PubMed] [Google Scholar]
- 16.Lofts F J, Evans T R, Mansi J L et al. Bile duct stents: is there an increased rate of complications in patients receiving chemotherapy? Eur J Cancer. 1997;33:209–213. doi: 10.1016/s0959-8049(96)00365-6. [DOI] [PubMed] [Google Scholar]
- 17.Dumonceau J M, Tringali A, Blero D et al. Biliary stenting: Indications, choice of stents and results: European Society of Gastrointestinal Endoscopy (ESGE) clinical guideline. Endoscopy. 2012;44:277–298. doi: 10.1055/s-0031-1291633. [DOI] [PubMed] [Google Scholar]
- 18.Boulay B R, Parepally M. Managing malignant biliary obstruction in pancreas cancer: Choosing the appropriate strategy. World J Gastroenterol. 2014;20:9345–9353. doi: 10.3748/wjg.v20.i28.9345. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Walter D, van Boeckel P G, Groenen M J et al. Cost efficacy of metal stents for palliation of extrahepatic bile duct obstruction in a randomized controlled trial. Gastroenterology. 2015;149:130–138. doi: 10.1053/j.gastro.2015.03.012. [DOI] [PubMed] [Google Scholar]
- 20.Boulay B R, Gardner T B, Gordon S R. Occlusion rate and complications of plastic biliary stent placement in patients undergoing neoadjuvant chemoradiotherapy for pancreatic cancer with malignant biliary obstruction. J Clin Gastroenterol. 2010;44:452–455. doi: 10.1097/MCG.0b013e3181d2ef06. [DOI] [PubMed] [Google Scholar]
- 21.Wasan S M, Ross W A, Staerkel G A et al. Use of expandable metallic biliary stents in resectable pancreatic cancer. Am J Gastroenterol. 2005;100:2056–2061. doi: 10.1111/j.1572-0241.2005.42031.x. [DOI] [PubMed] [Google Scholar]
- 22.Siddiqui A A, Mehendiratta V, Loren D et al. Self-expanding metal stents (SEMS) for preoperative biliary decompression in patients with resectable and borderline-resectable pancreatic cancer: outcomes in 241 patients. Dig Dis Sci. 2013;58:1744–1750. doi: 10.1007/s10620-012-2482-z. [DOI] [PubMed] [Google Scholar]
- 23.Kubota K, Sato T, Watanabe S et al. Covered self-expandable metal stent deployment promises safe neoadjuvant chemoradiation therapy in patients with borderline resectable pancreatic head cancer. Dig Endosc. 2014;26:77–86. doi: 10.1111/den.12049. [DOI] [PubMed] [Google Scholar]
- 24.Gardner T B, Spangler C C, Byanova K L et al. Cost-effectiveness and clinical efficacy of biliary stents in patients undergoing neoadjuvant therapy for pancreatic adenocarcinoma in a randomized controlled trial. Gastrointest Endosc. 2016;84:460–466. doi: 10.1016/j.gie.2016.02.047. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Nakai Y, Isayama H, Kawabe T et al. Efficacy and safety of metallic stents in patients with unresectable pancreatic cancer receiving gemcitabine. Pancreas. 2008;37:405–410. doi: 10.1097/MPA.0b013e3181706d93. [DOI] [PubMed] [Google Scholar]
- 26.Kitano M, Yamashita Y, Tanaka K et al. Covered self-expandable metal stents with an anti-migration system improve patency duration without increased complications compared with uncovered stents for distal biliary obstruction caused by pancreatic carcinoma: a randomized multicenter trial. Am J Gastroenterol. 2013;108:1713–1722. doi: 10.1038/ajg.2013.305. [DOI] [PubMed] [Google Scholar]
- 27.Kahaleh M, Brock A, Conaway M R et al. Covered self-expandable metal stents in pancreatic malignancy regardless of resectability: a new concept validated by a decision analysis. Endoscopy. 2007;39:319–324. doi: 10.1055/s-2007-966263. [DOI] [PubMed] [Google Scholar]
- 28.Takasawa O, Fujita N, Kobayashi G et al. Endoscopic biliary drainage for patients with unresectable pancreatic cancer with obstructive jaundice who are to undergo gemcitabine chemotherapy. World J Gastroenterol. 2006;12:7299–7303. doi: 10.3748/wjg.v12.i45.7299. [DOI] [PMC free article] [PubMed] [Google Scholar]