

Abstract
Purpose
Postcardiac arrest syndrome (PCAS) shares many features with sepsis including plasma cytokine elevation with dysregulation of cytokine production, and the presence of endotoxin in plasma. PCAS is closely related to ischemia-reperfusion injury. During ischemia-reperfusion injury, neutrophil, which is the first line of innate immunity, plays a major role. In this study, we investigated the inflammatory response of human neutrophils in an in vitro model which we simulated with hypoxia-normoxia and hypoxia-hyperoxia environments.
Methods
After separation of neutrophils from the whole blood, they were divided into 3 experimental groups: normoxia-normoxia, hypoxia-normoxia, and hypoxia-hyperoxia groups. The production of H2O2, the expression of Toll-like receptor 4 (TLR4) receptor, and the extent of apoptosis of the neutrophils were checked.
Results
The in vitro hypoxia-normoxia and -hyperoxia models, which simulated the PCAS, showed initiation of the neutrophils' inflammatory reaction by hypoxia insult. Lipopolysaccharide amplifies such inflammation; therefore, prevention of secondary infection may be critical in postresuscitation patients. Temporary hyperoxia following hypoxic insult showed no difference in inflammatory reaction compared with hypoxia-normoxia. Rather, temporary hyperoxia may suppress or minimize inflammation by attenuation of TLR4 receptor.
Conclusion
It is well known that continuous hyperoxygenation after successful cardiac arrest harms patients, but temporary hyperoxygenation with 100% O2 in a clinical situation may be helpful.
Keywords: Neutrophil, Reperfusion injury, Hypoxia, Hyperoxia
INTRODUCTION
Since the introduction of modern cardiopulmonary resuscitation and emergency cardiovascular care 60 years ago, there have been progressive improvements in the management of cardiac arrest. Nevertheless, after successful resuscitation, patients admitted to an intensive care unit have a high risk of multiple life-threatening disorders together known as “postresuscitation disease” or “postcardiac arrest syndrome (PCAS),” which can lead to multiple organ dysfunction syndrome (MODS) including neurologic failure and a poor prognosis [1]. PCAS is well known to share many features with severe sepsis. Similarities between PCAS and sepsis can be described as ischemia-reperfusion injury with features including plasma cytokine elevation with dysregulated cytokine production, the presence of endotoxin in plasma, coagulation abnormalities, and adrenal dysfunction [2]. Tissue damage directly related to revascularization known as reperfusion-induced injury may be even more harmful than severe tissue and organ damage by prolonged ischemia [3].
The neutrophil is the first line of cellular response during acute inflammation. Neutrophil contribute to early innate response by rapid migration to the inflammatory site, and their activation initiates microbial mechanisms such as the release of proteolytic enzymes and antimicrobial peptides, and rapid production of reactive oxygen species (ROS) in oxidative burst [4]. Released free oxygen radicals are known as one of the major mechanisms of self-destruction of tissue. An American Heart Association guideline recommends avoiding an excessive and prolonged hyperoxic state after successful resuscitation because excessive oxygen produces excessive oxygen species and overactivates inflammatory reaction, which, in turn, causes self-destruction of tissues. Lesions of gut mucosa after ischemia and reperfusion injury cause functional impairment with increased permeability of the mucosal barrier, diarrhea, and endotoxin or bacterial translocation. Increased plasma endotoxin levels seen in the first few days after successful resuscitation may be explained by translocation of endotoxins through gut-wall ischemia sites and reperfusion damage [5]. Endotoxins and bacteria in circulation may contribute to the aggravation of tissue damage and eventually to multiple organ damage by aggravation of the neutrophil's inflammatory response [2]. Triantafilou et al. [6] noted that when the innate immune system recognizes bacterial lipopolysaccharide (LPS), the inevitable proinflammatory response will lead to fatal sepsis syndrome.
In this study, we investigated the inflammatory response of neutrophils in a postcardiac arrest state with spontaneous circulation in vitro, which we simulated with hypoxia-normoxia and hypoxia-hyperoxia environments. We hypothesized that ischemic injury is similar to hypoxic injury and reperfusion is similar to normoxic or hyperoxic injury. Additionally, reperfusion injury can be divided into 2 types; one is a theoretical reperfusion injury, which is hypoxia followed by normoxia; the other is commonly found in clinical situations where temporary hyperoxia is given after hypoxia. We hypothesized that secondary infection is caused by the presence of LPS. The purposes of this study were (1) to determine whether hypoxia-normoxia or temporary hyperoxic insult may initiate or effect the inflammatory response of neutrophils, (2) to determine whether LPS insult amplifies the inflammation of primed neutrophils with hypoxia-normoxia or -hyperoxia, (3) to determine whether temporary hyperoxia after hypoxic insult has any effect on the inflammatory response of neutrophils.
METHODS
Study design
The study included 3 groups
Normoxia group: No insult was given to this group. Neutrophils were cultured and incubated at 37℃ in room oxygen tension for 18 hours. The normoxia group was a control group.
Hypoxia/normoxia group: Initial hypoxia insult for 2 hours was given, followed by incubated at 37℃ in room oxygen tension for 16 hours.
Hypoxia-hyperoxia group: Initial hypoxia insult for 2 hours was given, followed by hyperoxic insult and 2 hours of culture at 37℃, then incubation in room oxygen tension for 14 hours.
The production of hydrogen peroxide (H2O2) and the expression of Toll-like receptor 4 (TLR4) were measured after 4 hours of neutrophil culture. Apoptosis was measured after 18 hours including first and second insults and culture for 14 hours in room oxygen tension (Fig. 1). The equivalent setting of the study was repeated with LPS insult (Fig. 2). This study protocol and written informed consent form was reviewed and approved by Korea University Guro Hospital (Institutional review board No. 11018).
Fig. 1. Culture of neutrophils without lipopolysaccharide under normoxia-normoxia, hypoxia-normoxia, and hypoxia-hyperoxia. Normoxia group: No insult was given to this group. Polymorphonuclear neutrophils (PMN) was cultured and incubated at 37℃ in a 5% CO2 incubator in room air. Normoxia group was control group. Hypoxia-normoxia group: An initial hypoxia insult was administered for 2 hours; then normoxic insult and 2 hours of culture at 37℃ in 5% CO2 incubator followed by incubation in room air for 14 hours. Hypoxia-hyperoxia group: An initial hypoxia insult for 2 hours was given, then hyperoxic insult and 2 hours of culture at 37℃, followed by incubation in room air for 14 hours. Hydrogen peroxide (H2O2) and Toll-like receptor 4 (TLR4) were measured after 4 hours of PMN culture. Apoptosis was measured after 18 hours, including period of first and second insults and culture for 14 hours in room air.

Fig. 2. Culture of neutrophils with lipopolysaccharide (LPS) under normoxia-normoxia, hypoxia-normoxia, and hypoxia-hyperoxia. Normoxia group: polymorphonuclear neutrophils (PMN) was cultured and incubated with LPS in room air. Normoxia group was control group. Hypoxia-normoxia group: An initial hypoxia insult for 2 hours was given, then normoxic insult and 2 hours of culture at 37℃ followed by incubation in room air for 14 hours with LPS insult. Hypoxia-hyperoxia group: Initial hypoxia insult for 2 hours was given; then hyperoxic insult and 2 hours of culture at 37℃, followed by incubation in room air for 14 hours with LPS insult. hydrogen peroxide (H2O2) and Toll-like receptor 4 (TLR4) receptors were measured after 6 hours of PMN culture. Apoptosis was measured after 18 hours, including period of first and second insults and culture for 14 hours in room air.

Study setting
Different oxygen environment setting
Normoxic environment: The neutrophil dish was placed at 37℃ in room oxygen tension.
Hypoxic environment: The neutrophil dish was placed in the modular incubator chamber (Billups-Rothenburg Inc., Del Mar, CA, USA). The connector tube from a gas tank containing 1% oxygen was connected to a flow meter then connected to an inlet port with the outlet port left open. The desired mixture of gas was flushed through the chamber for 40 minutes, then both inlets were closed and the outlet port was tightened using the attached plastic clamp.
Temporary hyperoxic environment: A neutrophil dish is placed in the modular incubator chamber (Billups-Rothenburgn Inc.). The connector tube from the gas tank containing 80% oxygen was connected to the flow meter, then to the inlet port, and the outlet port was left open. The desired mix of gas was flushed through the chamber for 40 minutes and both inlet and outlet ports were closed tightly using the attached plastic clamp.
Neutrophil preparation
Whole blood from healthy volunteers was collected into a sterile vacutainer with ethylenediaminetetraacetic acid. A sterile processing environment was maintained with a clean bench, and 5 mL of each whole blood sample collected was separated in aliquots into 15-mL test tubes with 5 mL of polymorphprep (Axis-Shield, Oslo, Norway), followed by centrifugation for approximately 35 minutes at 500 G. Among the resulting cell layers after centrifugation, the polymorphonuclear neutrophils (PMN) cell layer, located between the monocyte and red blood cell layers, was collected with a pipette. To remove the red blood cells remaining in the collected PMN cell sample, the sample was incubated with a 0.2% saline solution for 30 seconds, after which a 1.8% saline solution was added to create 0.9% normal osmotic pressure. The samples were centrifuged at 450 G for 10 minutes, followed by 2 washes with phosphate-buffered saline. The isolated PMN cells were incubated in Roswell Park Memorial Institute tissue culture medium 1640 containing 10% fetal bovine serum, 1% penicillin-streptomycin, 10 mM 4-(2-hydroxyethyl)-1-piperazineethanesulfonic acid, and 0.005% 2-mercaptoethanol. We confirmed cell densities of 1 × 106 cells/mL and viabilities above 95% using trypan blue dye.
LPS preparation
One microgram per milliliter (1 µg/mL; final concentration) of LPS (Sigma-Aldrich, St. Louis, MO, USA) was prepared for stimulation.
Measurement of inflammatory reaction
Reactive oxygen species
During severe hypoxia, neutrophils undergo oxidative stress and ROS are produced [7]. In this study we measured H2O2. Production of H2O2 was measured by 5-6-chloromethyl-2,7'-dichlorodihydroflourescein diacetate (CM-H2DCFDA) (Invitrogen, Waltham, MA, USA) assay. The cells were loaded with 2×106 µmol/mL of CM-H2DCFDA and were incubated in the dark for 30 minutes, at 37℃, in a 5% carbon dioxide environment. The relative amount of generated ROS was measured by flow cytometry determining the mean fluorescence intensity.
Apoptosis
Neutrophils have a short life span (8–20 hours); neutrophils undergo spontaneous apoptosis in the absence of cytokines or proinflammatory agents, before their removal by macrophages [8]. This phagocytic activity prevents neutrophils from releasing cytotoxic contents into the extracellular environment that would occur by cell necrosis. Prolonging the life span of neutrophil is critical in their efficacy against pathogens. Apoptosis is an intrinsic cellular process that can be regulated by external stimuli [9]. The cells were labeled with annexin V fluorescein isothiocyanate and propidium iodide (ApoScan Annexin V FITC Apoptosis Detection Kit; Genzyme, Cambridge, MA, USA), and the presence of apoptotic cells was assessed using flow cytometric analysis.
Toll-like receptor
TLRs are pattern recognition receptors that are important in the innate immune response and are believed to play an important role in the central nervous system response to the injury-induced endogenous ligands termed damage-associated molecular patterns as well as towards pathogens [10]. TLRs are also known for the initiation of inflammation after ischemiareperfusion injury. Expression of cell surface TLR4 receptor was determined by flow cytometry analysis. The cells were stained with 5 µL (2 µg) of PE conjugated anti-TLR4 monoclonal antibody (clone HTA125, eBioscience, San Diego, CA, USA) in the dark for 1 hour on ice. After staining, the cells were analyzed by flow cytometry using Cytomics FC 500 (Beckman Coulter, Brea, CA, USA) and CXP software (Beckman Coulter).
Statistical analysis
All statistical analyses were performed with IBM SPSS Statistics ver. 20.0 (IBM Co., Armonk, NY, USA). The statistical analysis consisted of a comparison by t-test. Significance was accepted at P < 0.05. All experiments were performed 18 times.
RESULTS
Oxygen tension of each culture medium
PH and partial pressure of carbon dioxide (pCO2) were similar in all of the groups. The partial pressure of oxygen (pO2) was lowest in the hypoxia group (39.7 mmHg), and highest in the hypoxia-hyperoxia group (261.3 mmHg) (Table 1).
Table 1. pH, pO2, and pCO2 of culture medium according to the oxygen supplied.

Values are presented as median (range).
pCO2, partial pressure of carbon dioxide; pO2, partial pressure of oxygen.
Viabilities of neutrophils
The viability of neutrophils was checked by trypan blue staining. The viability of neutrophils after the hypoxia insult was 85.8%, and viability of neutrophils in the control group was 99.4%.
Effect of hypoxia-normoxia and hypoxia-hyperoxia on the inflammatory response of neutrophils
In the hypoxia-normoxia group, H2O2 and TLR4 production were increased and apoptosis was delayed compared to the control group (P = 0.106, P < 0.001, P = 0.019, respectively). Compared to the control group, the hypoxia-hyperoxia group had greater H2O2 production, but without statistical significance (P = 0.323), while apoptosis was significantly delayed (P < 0.001). TLR4 receptor in the hypoxia-hyperoxia group was not higher compared to the control group (P = 0.623) (Fig. 3).
Fig. 3. Effects of hypoxia-normoxia and hypoxia-hyperoxia conditions on inflammatory response of neutrophils. Each value has been calculated as ratio (%) relative to control group. In hypoxia-normoxia group, hydrogen peroxide (H2O2) and Toll-like receptor 4 (TLR4) production were higher and apoptosis was delayed compared to control group. In hypoxia-hyperoxia group, production of H2O2 was increased and apoptosis was delayed compared to control group; however, TLR4 receptor production was restored to control group. Mean ± standard deviation (n = 18). *P < 0.05, paired t-test.

Effect of LPS insult on the inflammatory response of neutrophil after hypoxia-normoxia or hypoxia-hyperoxia culture
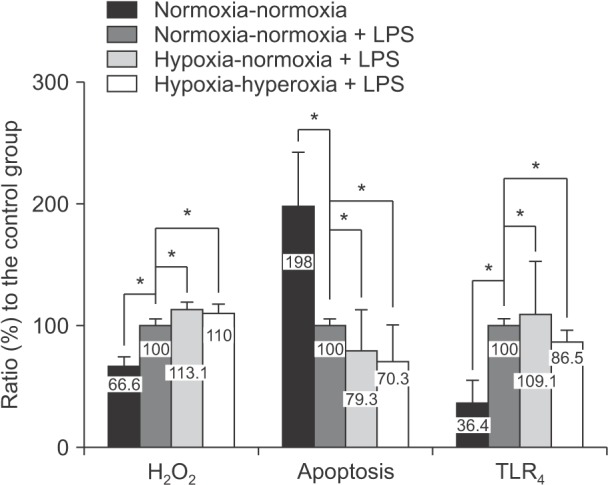
LPS insult significantly increased H2O2 production in both the hypoxia-normoxia group and hypoxia-hyperoxia group compared to the control group with LPS stimulation (P < 0.001, P = 0.018, respectively). Apoptosis was significantly delayed in both the hypoxia-normoxia group and hypoxia-hyperoxia compared to the control group following LPS stimulation (P = 0.004, P = 0.002, respectively). In the hypoxia-normoxia group, TLR4 receptor expression was increased (P = 0.035); however, production was significantly decreased in the hypoxia-hyperoxia group (P < 0.001) (Fig. 4).
Fig. 4. Effects of lipopolysaccharide (LPS) insult in neutrophils precultured in normoxia-normoxia, hypoxia-normoxia, and hypoxia-hyperoxia conditions. Each value has been calculated as ratio (%) relative to control group. Compared to control group, hydrogen peroxide (H2O2) production was increased in all groups, apoptosis was delayed in all groups, and Toll-like receptor 4 (TLR4) receptor production was increased in all groups. Mean ± standard deviation (n = 18). *P < 0.05, paired t-test.
Comparison of the inflammatory response of neutrophils with or without LPS insult between hypoxia-normoxia and hypoxia-hyperoxia conditions
There were no differences in the production of H2O2 between the hypoxia-normoxia and hypoxia-hyperoxia groups with or without LPS (P = 0.324, P = 0.490, respectively). Delay of apoptosis was prominent in the hypoxia-normoxia group without LPS insult compared to the hypoxic-hyperoxic group (P = 0.02). TLR4 receptor expression was lower in the hypoxia-hyperoxia group with or without LPS insult than in the hypoxia-normoxia group (P = 0.006, P < 0.001, respectively) (Fig. 5).
Fig. 5. Comparison of neutrophils' inflammatory response with or without lipopolysaccharide (LPS) insult between hypoxia-normoxia and hypoxia-hyperoxia groups. (A, B) There were no differences in production of hydrogen peroxide (H2O2) between hypoxia-normoxia and hypoxia-hyperoxia groups with or without LPS insult. (A, B) Delay of apoptosis was prominent in hypoxia-normoxia group without LPS insult compared to hypoxia-hyperoxia group with LPS insult. (A, B) Toll-like receptor 4 (TLR4) receptor production was decreased in hypoxia-hyperoxia group with or without LPS insult compared to hypoxia-normoxia group with or without LPS insult. Mean ± standard deviation (n = 18). *P < 0.05, paired t-test.

DISCUSSION
In this study, we examined the inflammatory response of neutrophils cultured in normoxia, hypoxia-normoxia, and hypoxia-hyperoxia conditions in vitro. The hypoxia-normoxia and hypoxia-hyperoxia models that simulated the PCAS, demonstrated the initiation of the inflammatory response in neutrophils by hypoxic insult. We proposed that LPS functioned as a source of secondary infection in PCAS and that it amplified the inflammatory infection of neutrophils primed by hypoxia. Temporary hyperoxia, which physicians commonly use in clinical situations, did not show a difference in the inflammatory reaction of neutrophils compared to the hypoxia-normoxia group. Rather, it seemed to downregulate the inflammatory responses by attenuating TLR4 receptor production.
Hypoxia-normoxia or hypoxia-hyperoxia models simulated with different oxygen tensions have been used in other studies [11]. In this study, analysis of the culture medium showed little difference in pH and pCO2 among groups; however, the distinction in the pO2 level was clear with the lowest level (39.7 mmHg) in hypoxia and the highest in hypoxia-hyperoxia (261.3 mmHg). We were able to produce normoxic, hypoxic, and hyperoxic environments successfully according to standard definitions. In this study, although it was not statistically significant, under hypoxia-normoxia and hypoxia-hyperoxia conditions, compared to the control group, production of H2O2 was elevated. It was previously determined that the release of free oxygen radicals such as H2O2 with cytokines and complement-activation products leads to marked activation of neutrophils during reperfusion injury [2]. ROS produced by hypoxia facilitates a rapid microvascular inflammatory response that is characterized by enhanced leukocyte-endothelial adherence and migration, which increases vascular permeability and eventually, self-destruction of tissue [12].
We showed that hypoxia-normoxia or hypoxia-hyperoxia culture delayed apoptosis of neutrophils compared to the control group. Haslett et al. [13] and Mecklenburgh et al. [14] showed that incubation of isolated human peripheral blood neutrophils under hypoxic conditions caused a profound inhibition of neutrophil apoptosis. Other studies have shown a delay in apoptosis of neutrophils during hypoxia and as a result, persistent inflammation has been noticed [8,15]. As a result of the prolongation of the neutrophil's life span, the inflammatory response can persist and develop into systemic inflammation syndrome.
In this study, TLR4 receptor production was increased under hypoxia-normoxia conditions compared to the control group. The production of TLR4 receptor in conditions of hypoxia followed by temporary hyperoxia was not higher than that that of the control group. The elevation of TLR4 receptor was closely related to the inflammatory reaction, and hypoxic stress was found to up-regulate TLR4 receptor expression [16,17]. Notably, TLR4 receptor plays a pivotal role in the pathogenesis of cerebral ischemic damage [18], and TLR4-NADPH oxidase 4 (NOX4) signal-mediated ROS production might contribute to the damage [19]. In an animal study, after ischemia-reperfusion injury, the expression of TLR4 receptor was significantly increased in the skin flap tissue with excessive neutrophil infiltration [20]. As we can see from these studies, elevation of TLR4 receptor production is closely related to the aggravation of inflammation by the role of receptors for secondary infection such as LPS. Our study also showed that the inflammatory response of neutrophils exaggerated the response to a secondary infection such as that caused by LPS insult after hypoxia-normoxia or hypoxia-hyperoxia insult. After loss of the gut barrier function by ischemia-reperfusion injury, intestinal permeability is altered whereby bacterial translocation and increased portal endotoxemia lead to systemic endotoxemia and systemic infection. These events will eventually cause a septic state and MODS [21]. There is a close relationship between systemic inflammation and the two-hit model. The priming and subsequent insult to neutrophils has been closely investigated and used to explain the two-hit model [22]. If an initial insult primes the inflammatory response, tissue is injured and reaches a state similar to systemic inflammatory syndrome. At this critical point, if the proper response does not take place, tissue becomes vulnerable to a second hit and is led to MODS [23]. Such a response can be explained by the fact that the first insult with hypoxia-normoxia or hypoxia-hyperoxia makes the tissue vulnerable to the second insult, such as that of LPS, with similar results shown in other studies [24].
In clinical situations, hypoxic insult occurs during cardiac arrest and 100% O2 is supplied during resuscitation. After successful resuscitation, the patient is temporarily ventilated with hyperoxia. In this study, temporary hyperoxia did not worsen the inflammatory response of neutrophils; it actually attenuated TLR4 receptor production and did not delay the apoptosis of the neutrophils. This phenomenon may be explained by (1) endotoxin intolerance or (2) attenuation of inflammation by reoxygenation. Hyporesponsiveness of circulating leukocytes in patients with systemic inflammatory response syndrome has been studied and neutrophil and monocytes as well as lymphocytes seem to be affected [25]. This may protect against overwhelming dysregulation of the proinflammatory process with risk of immune paralysis or endogenous immunosuppression [26]. Reoxygenation may attenuate the adhesion of neutrophils to microvascular endothelial cells, which is a critical step in ischemia-reperfusion injury [27]. Continuous hyperoxygenation may sustain inflammation; however, temporary hyperoxia does not worsen inflammation as part of reoxygenation.
There are a few limitations of this study. First, we simulated in vitro hypoxia-normoxia and hypoxia-hyperoxia conditions to create similar conditions of PCAS. There are complications such as accumulation of carbon dioxide or acidification of blood that is accompanied by ischemic injury in clinical situations, but in this study only manipulation of oxygen tension was performed. Therefore, we only observed hypoxia and overlooked other complications. Second, the viability of the neutrophils was lower than in the control group: 85.8% in hypoxia group and 99.4% in the control group. Therefore, the attenuation of TLR4 receptor production may be affected by decreased viability. Finally, in clinical situations, after successful resuscitation, if indicated, the patient is subjected to therapeutic hypothermia. In our study, we cultured neutrophils in a 37℃ environment, thus the inflammatory response of neutrophils under therapeutic hypothermia could not be tested. In future research, other complications such as the accumulation of Pco2, acidosis, and inflammatory reaction should be evaluated under hypothermic conditions.
The ischemia-reperfusion model in vitro, which simulated the postcardiac arrest state with hypoxia-normoxia and hypoxia-hyperoxia models, showed that hypoxia-normoxia and hypoxia-hyperoxia initiated the inflammation of neutrophils. LPS amplifies such inflammation; therefore, prevention of secondary infection is critical in postresuscitation patients. However, temporary hyperoxia may suppress or minimize inflammation by attenuation of the expression of TLR4 receptor. It is well known that continuous hyperoxygenation after successful cardiac resuscitation can harm the patient and worsen the prognosis; however, temporary hyperoxygenation with 100% O2 in clinical situations may be appropriate treatment.
In conclusion, we suggest that temporary high oxygen support after hypoxia may contribute to the suppression of inflammation through appropriate apoptosis and attenuation of the expression of TLR4 receptor.
ACKNOWLEDGEMENTS
This study was partially supported by Korea University grant and Basic Science Research Program through the National Research Foundation of Korea (NRF) funded by the Ministry of Education, Science and Technology (R1522002).
Footnotes
CONFLICTS OF INTEREST: No potential conflict of interest relevant to this article was reported.
References
- 1.Negovsky VA. The second step in resuscitation--the treatment of the ‘post-resuscitation disease’. Resuscitation. 1972;1:1–7. doi: 10.1016/0300-9572(72)90058-5. [DOI] [PubMed] [Google Scholar]
- 2.Adrie C, Adib-Conquy M, Laurent I, Monchi M, Vinsonneau C, Fitting C, et al. Successful cardiopulmonary resuscitation after cardiac arrest as a “sepsis-like” syndrome. Circulation. 2002;106:562–568. doi: 10.1161/01.cir.0000023891.80661.ad. [DOI] [PubMed] [Google Scholar]
- 3.Ar'Rajab A, Dawidson I, Fabia R. Reperfusion injury. New Horiz. 1996;4:224–234. [PubMed] [Google Scholar]
- 4.Strieter RM, Kasahara K, Allen RM, Standiford TJ, Rolfe MW, Becker FS, et al. Cytokine-induced neutrophil-derived interleukin-8. Am J Pathol. 1992;141:397–407. [PMC free article] [PubMed] [Google Scholar]
- 5.Adrie C, Laurent I, Monchi M, Cariou A, Dhainaou JF, Spaulding C. Postresuscitation disease after cardiac arrest: a sepsis-like syndrome. Curr Opin Crit Care. 2004;10:208–212. doi: 10.1097/01.ccx.0000126090.06275.fe. [DOI] [PubMed] [Google Scholar]
- 6.Triantafilou M, Triantafilou K. Lipopolysaccharide recognition: CD14, TLRs and the LPS-activation cluster. Trends Immunol. 2002;23:301–304. doi: 10.1016/s1471-4906(02)02233-0. [DOI] [PubMed] [Google Scholar]
- 7.Prabhakar NR, Kumar GK. Oxidative stress in the systemic and cellular responses to intermittent hypoxia. Biol Chem. 2004;385:217–221. doi: 10.1515/BC.2004.015. [DOI] [PubMed] [Google Scholar]
- 8.Savill J, Dransfield I, Gregory C, Haslett C. A blast from the past: clearance of apoptotic cells regulates immune responses. Nat Rev Immunol. 2002;2:965–975. doi: 10.1038/nri957. [DOI] [PubMed] [Google Scholar]
- 9.Francois S, El Benna J, Dang PM, Pedruzzi E, Gougerot-Pocidalo MA, Elbim C. Inhibition of neutrophil apoptosis by TLR agonists in whole blood: involvement of the phosphoinositide 3-kinase/Akt and NF-kappaB signaling pathways, leading to increased levels of Mcl-1, A1, and phosphorylated Bad. J Immunol. 2005;174:3633–3642. doi: 10.4049/jimmunol.174.6.3633. [DOI] [PubMed] [Google Scholar]
- 10.Akira S. TLR signaling. Curr Top Microbiol Immunol. 2006;311:1–16. doi: 10.1007/3-540-32636-7_1. [DOI] [PubMed] [Google Scholar]
- 11.Eker T, Genc V, Sevim Y, Cumaogullari O, Ozcelik M, Kocaay AF, et al. The effects of ventilation with high density oxygen on the strength of gastrointestinal anastomosis. Ann Surg Treat Res. 2015;89:17–22. doi: 10.4174/astr.2015.89.1.17. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Wood JG, Johnson JS, Mattioli LF, Gonzalez NC. Systemic hypoxia increases leukocyte emigration and vascular permeability in conscious rats. J Appl Physiol (1985) 2000;89:1561–1568. doi: 10.1152/jappl.2000.89.4.1561. [DOI] [PubMed] [Google Scholar]
- 13.Haslett C, Savill JS, Whyte MK, Stern M, Dransfield I, Meagher LC. Granulocyte apoptosis and the control of inflammation. Philos Trans R Soc Lond B Biol Sci. 1994;345:327–333. doi: 10.1098/rstb.1994.0113. [DOI] [PubMed] [Google Scholar]
- 14.Mecklenburgh KI, Walmsley SR, Cowburn AS, Wiesener M, Reed BJ, Upton PD, et al. Involvement of a ferroprotein sensor in hypoxia-mediated inhibition of neutrophil apoptosis. Blood. 2002;100:3008–3016. doi: 10.1182/blood-2002-02-0454. [DOI] [PubMed] [Google Scholar]
- 15.Walmsley SR, Print C, Farahi N, Peyssonnaux C, Johnson RS, Cramer T, et al. Hypoxia-induced neutrophil survival is mediated by HIF-1alpha-dependent NF-kappaB activity. J Exp Med. 2005;201:105–115. doi: 10.1084/jem.20040624. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Yao L, Kan EM, Lu J, Hao A, Dheen ST, Kaur C, et al. Toll-like receptor 4 mediates microglial activation and production of inflammatory mediators in neonatal rat brain following hypoxia: role of TLR4 in hypoxic microglia. J Neuroinflammation. 2013;10:23. doi: 10.1186/1742-2094-10-23. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Kim DH, Billiar TR. Hypoxia activates toll-like receptor 4 signaling in primary mouse hepatocytes through the receptor clustering within lipid rafts. J Korean Surg Soc. 2011;80:194–203. [Google Scholar]
- 18.Hyakkoku K, Hamanaka J, Tsuruma K, Shimazawa M, Tanaka H, Uematsu S, et al. Toll-like receptor 4 (TLR4), but not TLR3 or TLR9, knock-out mice have neuroprotective effects against focal cerebral ischemia. Neuroscience. 2010;171:258–267. doi: 10.1016/j.neuroscience.2010.08.054. [DOI] [PubMed] [Google Scholar]
- 19.Suzuki Y, Hattori K, Hamanaka J, Murase T, Egashira Y, Mishiro K, et al. Pharmacological inhibition of TLR4-NOX4 signal protects against neuronal death in transient focal ischemia. Sci Rep. 2012;2:896. doi: 10.1038/srep00896. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Jian QC, Wu XW, Song HC, Zheng L. The role of toll like receptor-4 signal pathways activation in ischemia-reperfusion injury of island skin flap. Zhonghua Zheng Xing Wai Ke Za Zhi. 2012;28:444–448. [PubMed] [Google Scholar]
- 21.Deitch EA, Sambol JT. The gut-origin hypothesis of MODS. In: Deitch EA, Vincent JL, Windsor A, editors. Sepsis and multiple organ dysfunction. London: Saunders; 2002. pp. 105–113. [Google Scholar]
- 22.Partrick DA, Moore FA, Moore EE, Barnett CC, Jr, Silliman CC. Neutrophil priming and activation in the pathogenesis of postinjury multiple organ failure. New Horiz. 1996;4:194–210. [PubMed] [Google Scholar]
- 23.Biffll WL, Moore EE, Moore FA. The-two-hit model of MODS. In: Deitch EA, Vincent JL, Windsor A, editors. Sepsis and multiple organ dysfunction. London: Saunders; 2002. pp. 127–132. [Google Scholar]
- 24.Molloy EJ, O'Neill AJ, Doyle BT, Grantham JJ, Taylor CT, Sheridan-Pereira M, et al. Effects of heat shock and hypoxia on neonatal neutrophil lipopolysaccharide responses: altered apoptosis, Toll-like receptor-4 and CD11b expression compared with adults. Biol Neonate. 2006;90:34–39. doi: 10.1159/000091743. [DOI] [PubMed] [Google Scholar]
- 25.Cavaillon JM, Adib-Conquy M, Fitting C, Adrie C, Payen D. Cytokine cascade in sepsis. Scand J Infect Dis. 2003;35:535–544. doi: 10.1080/00365540310015935. [DOI] [PubMed] [Google Scholar]
- 26.Munford RS, Pugin J. Normal responses to injury prevent systemic inflammation and can be immunosuppressive. Am J Respir Crit Care Med. 2001;163:316–321. doi: 10.1164/ajrccm.163.2.2007102. [DOI] [PubMed] [Google Scholar]
- 27.Schmitz K, Jennewein M, Pohlemann T, Seekamp A, Oberringer M. Reoxygenation attenuates the adhesion of neutrophils to microvascular endothelial cells. Angiology. 2011;62:155–162. doi: 10.1177/0003319710375943. [DOI] [PubMed] [Google Scholar]