

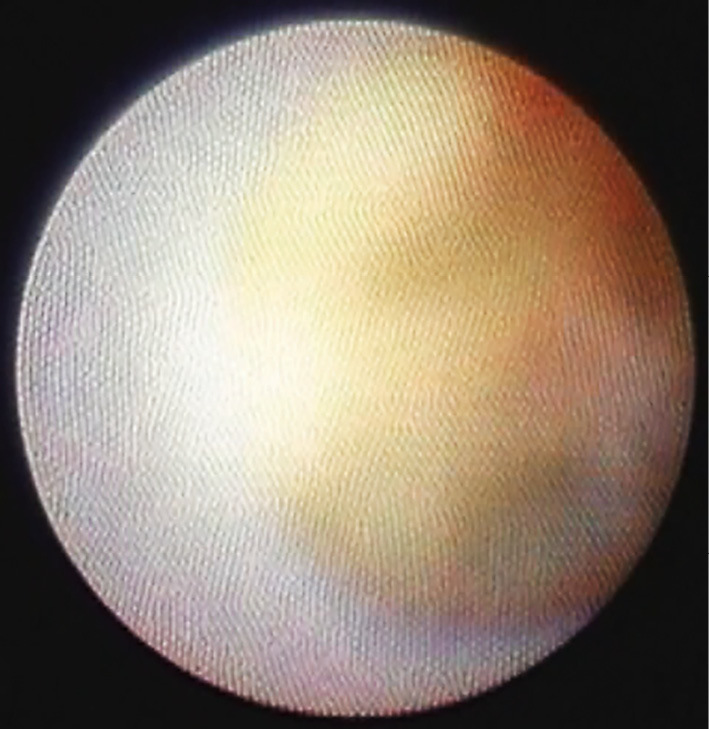
A 78-year-old man with a history of hypertension, dyslipidemia, and diabetes mellitus was referred to our hospital for the evaluation of a systolic murmur. Echocardiography showed severe aortic stenosis with a pressure gradient of 79.7 mmHg; aortic orifice size, 0.46 cm2; and regurgitation, grade III (ejection fraction, 50.5%). Computed tomography revealed marked calcification adhering to the aortic valve and ascending aorta (Picture 1). Coronary angiography revealed no stenosis. Non-obstructive angioscopy using the dual infusion method (1) revealed atheromatous agglutinated sclerosed valvular leaflets and a circular small aortic orifice (Picture 2). The agglutinated cusps did not move, and the size of the aortic orifice did not change between systolic and diastolic phases (Picture 3). The ascending aorta had a rough, bright-yellow surface with red thrombi (Picture 4). This is the first report safely using percutaneous angioscopy to reveal aortic valve stenosis and an atheromatous ascending aorta.
Picture 1.

Picture 2.
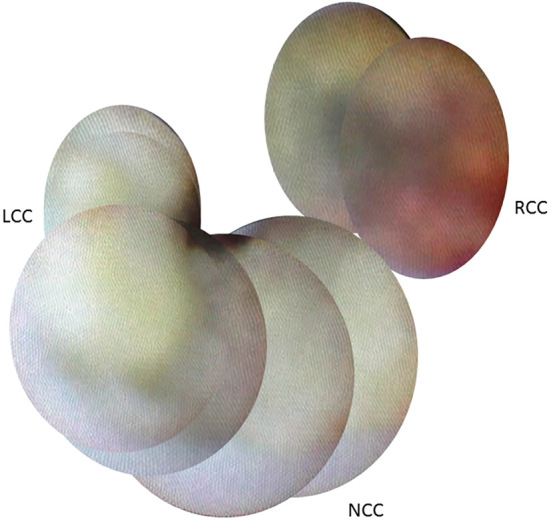
Picture 3.

Picture 4.
Author's disclosure of potential Conflicts of Interest (COI).
Kazuhisa Kodama: Employment, Inter-tec Medicals, Co., Ltd.
Sei Komatsu: Employment, Nemoto Kyorin-do Co., Ltd.
References
- 1.Komatsu S, Ohara T, Takahashi S, et al. . Early detection of vulnerable atherosclerotic plaque for risk reduction of acute aortic rupture and thromboemboli and atheroemboli using non-obstructive angioscopy. Circ J 79: 742-750, 2015. [DOI] [PubMed] [Google Scholar]