

Abstract
Background
High mammographic density is strongly associated with increased breast cancer risk. Some, but not all, risk factors for breast cancer are also associated with higher mammographic density.
Methods
The study cohort (N=24,840) was drawn from the Research Program in Genes, Environment and Health of Kaiser Permanente Northern California and included non-Hispanic white females aged 40–74 years with a full-field digital mammogram (FFDM). Percent density (PD) and dense area (DA) were measured by a radiological technologist using Cumulus. The association of age at menarche and late adolescent BMI with PD and DA were modeled using linear regression adjusted for confounders.
Results
Age at menarche and late adolescent BMI were negatively correlated. Age at menarche was positively associated with PD (p-value for trend<0.0001) and DA (p-value for trend <0.0001) in fully adjusted models. Compared to the reference category of age 12–13 years at menarche, menarche at age >16 years was associated with an increase in PD of 1.47% [95% CI: (0.69, 2.25)] and an increase in DA of 1.59cm2 [95% CI: (0.48, 2.70)]. Late adolescent BMI was inversely associated with PD (p-value <0.0001) and DA (p-value <0.0001) in fully adjusted models.
Conclusions
Age at menarche and late adolescent BMI are both associated with Cumulus measures of mammographic density on processed FFDM images.
Impact
Age at menarche and late adolescent BMI may act through different pathways. The long-term effects of age at menarche on cancer risk may be mediated through factors besides mammographic density.
Keywords: adolescence, breast cancer, childhood growth, epidemiology, mammography
Introduction
Mammographic density, or the extent to which the breast tissue appears dense on a mammogram, is strongly associated with breast cancer risk (1,2). Ductal tissue, where breast cancer arises, and the surrounding structurally supportive stromal collagen appear white, while fatty tissue appears dark. Women with high breast density have four to six times higher risk of breast cancer than women with very low breast density (2,3).
Mammographic density can be assessed using several different metrics. The quantitative area-based Cumulus measurement is a particularly good measure because of its consistently strong associations with breast cancer risk across studies (2,4). Cumulus measures include quantification of the dense area (DA), the area of the breast that appears radiopaque on a mammogram, and percent density (PD), a measure of the dense area as a percentage of the total breast area. Most previous epidemiologic studies using Cumulus have assessed breast density using images from film-screen mammography, whereas full-field digital mammography (FFDM) has largely replaced conventional film mammography in health care settings over the last decade. Recently, we (5) and others (6,7) have shown that mammographic density measured with Cumulus on processed digital mammograms is also significantly associated with breast cancer risk.
Studies of the determinants of mammographic density may increase our ability to identify and understand risk factors that play a role in the early stages of breast cancer development. As a modifiable risk factor, mammographic density appears to change within each woman over time. Mammographic density generally peaks during late adolescence, and declines with increasing age (8). Many lifestyle, demographic, genetic and reproductive factors are thought to influence mammographic density and breast cancer risk. Epidemiologic studies have found that mammographic density is associated with BMI at screening (9–11), reproductive factors such as parity and age at first birth (12–14), and with hormonal therapies (11). Further study of the early-life determinants of mammographic density may provide useful information about potential preventive strategies for breast cancer.
Age of menarche and late adolescent BMI have been reported to have inverse associations with breast cancer risk (15,16), but the relationship of these pubertal factors with mammographic density remains poorly understood. Inconsistent associations between age of menarche and mammographic density have been reported (17–19), which could be because large sample sizes and quantitative density measures are required to these effects with high statistical power. Late adolescent BMI is a related pubertal factor whose relationship to mammographic density has not been evaluated in many studies, however one recent study found an inverse association of late adolescent BMI with adult mammographic density (20). A large cohort of screening-age women is needed to resolve the inconsistent associations that have been reported with age at menarche and further study the association with late adolescent BMI. This study investigates two interrelated pubertal characteristics, age at menarche and late adolescent BMI, in relation to mammographic density quantified using Cumulus on FFDM images for 24,840 screening-age women in a large integrated healthcare system.
Materials and methods
Setting
This study is ancillary to a genome wide association study (GWAS) of mammographic density conducted among approximately 25,000 non-Hispanic white female participants of the Research Program in Genes, Environment and Health (RPGEH). The methods related to this resource have been described previously (5). Briefly, the RPGEH was developed and is administered by the Division of Research, Kaiser Permanente Northern California (KPNC) as a resource for research on the genetic and environmental determinants of common, age-related complex health conditions. The resource links together surveys, biospecimens and derived data, with longitudinal data from electronic health records (EHRs) on a cohort of ~200,000 consenting adult KPNC members. Genome-wide genotyping has been performed on DNA extracted from saliva samples of more than 100,000 RPGEH participants enrolled before 2010 (RC2 AG036607). The mammographic density subcohort includes women in the RPGEH, who completed a health survey and provided a saliva sample for genotyping and who had at least one screening FFDM between the ages of 40 and 74 during 2003–2013. Further inclusion and exclusion criteria based on mammograms are given below and illustrated in Figure 1.
Figure 1.
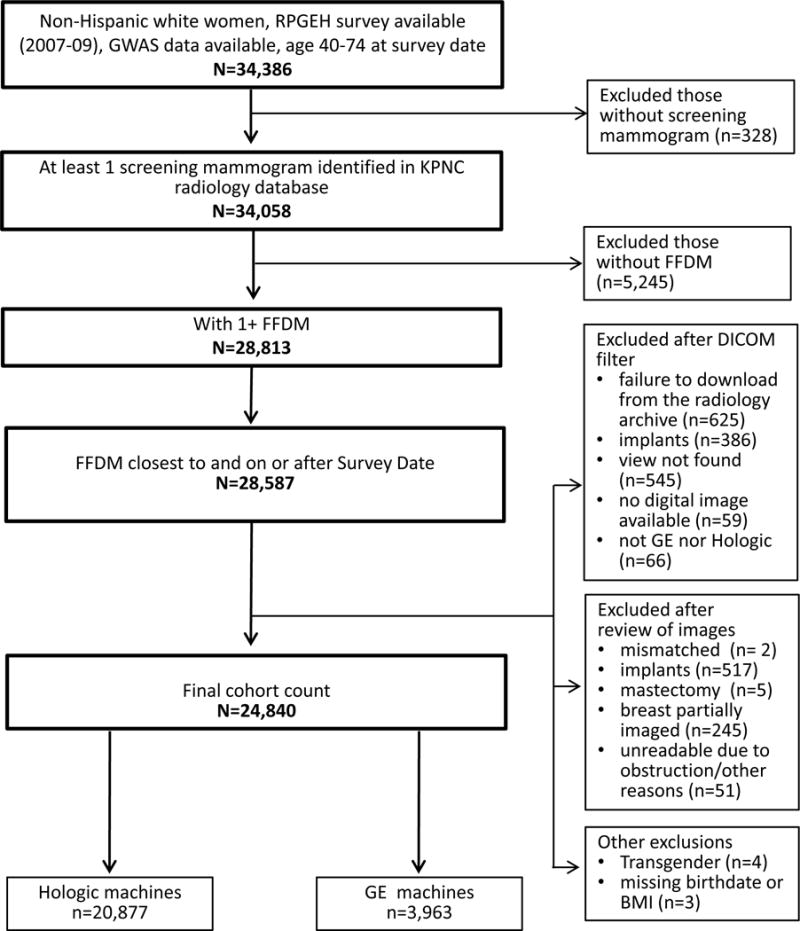
Design of study cohort and inclusion criteria.
Mammograms
The EHR was used to identify screening mammograms on the study population. Processed FFDMs from 37 different mammography facilities, with 1–5 machines per facility, were obtained from the KPNC imaging archive. For the large majority of women who did not have a personal history of breast cancer, we randomly selected the right craniocaudal (CC) view for approximately 10% to blind the reader to case-control status, and used the left CC view otherwise. For women with a history of breast cancer, we obtained the closest pre-diagnostic FFDM after the RPGEH survey when available, or prior to the survey date otherwise, and selected the CC view of the unaffected breast (i.e., we used the left view for cases with cancer in the right breast and the right view for cases with cancer in the left breast). We excluded women who had bilateral breast cancer (n=15), breast implants (n=903), breasts too large to be completely imaged on a single exposure (n=245), unreadable images (n=44) or unavailable images (n=625). FFDM images, in Digital Imaging and Communications in Medicine (DICOM) format, were de-identified and downsampled from a pixel size of 70 microns to a pixel size of 200 microns for transfer to the Stanford Radiology 3D and Quantitative Imaging Laboratory. Prior studies of scanned film mammograms have used larger pixel sizes [8], and downsampling would not be expected to influence computer-assisted density measurements on standard monitors that have lower resolution than the study images.
Density assessments
Processed images acquired from Selenia Digital Mammography System machines manufactured by Hologic, Inc. for approximately 21,000 women were randomly assembled into 23 batches of up to 1,100 images including 10% random replicates for quality control. FFDM images processed using Tissue Equalization software manufactured by General Electric (GE) for approximately 4,000 women were randomly assembled into 6 additional batches of up to 700 images including 10% random replicates for quality control. Density measurements were estimated with the Cumulus interactive threshold method [9]. We previously found that noise reduction of processed Hologic FFDM images to make them appear more film-like can significantly (p < 0.001) improve the reproducibility of readers with little prior experience applying Cumulus to processed FFDM images (5). As readers gained experience over time, high levels of reproducibility (Pearson’s r >0.90) were attained on processed FFDM images with or without noise reduction. Here, we applied a median filter with a radius of three pixels to all processed Hologic FFDM images (21). A single radiological technologist (RYL), trained in Cumulus assessments by MJY and JAL who consistently attained a within-reader reliability >0.9 measured the total area of the breast and area of dense tissue in the pre-assembled batches using Cumulus6 (provided by MJY), which automatically detects the outer edge of the breast for most digital mammograms. The Cumulus software also calculated the percentage of the total breast area occupied by dense tissue (percent density).
Data sources for characteristics of cohort
Age at mammogram was determined based on date of birth and date of mammogram. We used the body mass index (BMI) measured at the patient visit closest to mammogram date when available from the EHR, and computed from self-reported height and weight on the RPGEH survey otherwise. The RPGEH survey provided self-reported information on parity, age at first birth, number of children, age at menarche, weight at age 18, family history of breast cancer and menopause. Late adolescent BMI was defined as BMI at age 18, computed based on self-reported weight at age 18 and adult height available from the EHR. The KPNC pharmacy database, which records all dispensed outpatient and inpatient prescriptions, was used to determine use of menopausal hormones within the five years prior to FFDM.
Statistical Methods
We modeled the outcomes of PD and DA using multivariable linear regression analyses. To reduce skew and heteroscedasticity in model residuals, we transformed PD by taking the square root and we transformed DA by taking the cube root, similar to previous studies (14,22). We evaluated the effects of age at menarche and late adolescent BMI in minimally adjusted models and fully adjusted models. Minimally adjusted models controlled for age, BMI at screening and image batch. For the key covariates age and BMI at screening, we considered alternative models for coding the covariates using linear and polynomial terms as well as log-transformation for BMI. We used the AIC to evaluate model fit and chose the best fitting model for age and BMI. The additional covariates in the fully adjusted model were chosen a priori and included parity, age at first birth, number of children, family history of breast cancer, menopausal status, use of menopausal hormones within five years, and image batch. Missing covariate data from the survey was imputed using a Markov chain Monte Carlo approach, with the initial estimate starting from the posterior mode of the expectation-maximization algorithm solution to the maximum likelihood estimates (21). We tested for a linear trend in associations across category levels of age at menarche using a Wald test. Late adolescent BMI was modeled as a continuous variable, which provided a better than fit than log-transformed BMI based on the AIC to compare model fit. Separate multivariable linear regression models were fit for Hologic and GE mammograms, and random-effects meta-analysis was used to obtain combined estimates. Parameter estimates and standard errors were transformed from square root of percent density back to percent density and from cube root of dense area back to dense area using the Delta method (23). These non-linear transformations induce a slight dependence of the rescaled parameter estimate on the density of the reference category. Our transformation for percent density used the overall mean percent density of 21.0% and our transformation for dense area used the overall mean dense area of 28.0 cm2. A level of 0.05 was used as the cutoff for statistical significance. Regression analyses were implemented in SAS version 9.3 and meta-analyses were implemented in R version 3.2.2.
Results
Our study cohort included 24,840 women who had a mean age of 62 years, and a mean BMI of 28. Most women were post-menopausal (81%). Digital mammograms were captured predominantly on Hologic machines (84%), with fewer mammograms acquired from GE machines (16%). Table 1 provides additional descriptive characteristics of the cohort.
Table 1.
Descriptive characteristics of study cohort of 24,840 women.
| N | (%) | |
|---|---|---|
| FFDM machine type | ||
| Hologic | 20,877 | (84.0) |
| GE | 3,963 | (16.0) |
| Age, Mean (IQR) | 61.5 | (56.0–68.0) |
| BMI (kg/m2), Mean (IQR) | 27.6 | (23.2–30.7) |
| Late adolescent BMI (kg/m2), Mean (IQR) | 21.1 | (19.3–22.3) |
| Menopause (based on survey) | ||
| Pre-menopause | 4,835 | (19.5) |
| Post-menopause | 20,005 | (80.5) |
| Menopausal Hormone Therapy in last 5 years | ||
| No (includes pre-menopausal women) | 18,680 | (75.2) |
| Yes | 6,160 | (24.8) |
| Parity | ||
| Nulliparous | 2,318 | (9.3) |
| One child | 3,662 | (14.7) |
| Two children | 9,217 | (37.1) |
| Three children | 4,168 | (16.8) |
| Four or more children | 2,045 | (8.2) |
| Missing | 3,430 | (13.8) |
| Age at first birth | ||
| Have not given birth | 2,318 | (9.3) |
| <20 years | 2,584 | (10.4) |
| 20–24 years | 6,734 | (27.1) |
| 25–29 years | 5,502 | (22.2) |
| 30–34 years | 2,748 | (11.1) |
| 35–40 years | 1,133 | (4.6) |
| >40 years | 252 | (1.0) |
| Missing | 3,569 | (14.4) |
| Age at menarche | ||
| <10 years | 491 | (2.0) |
| 10–11 years | 4,617 | (18.6) |
| 12–13 years | 13,177 | (53.1) |
| 14–15 years | 4,147 | (16.7) |
| >16 years | 920 | (3.7) |
| Never had a menstrual period | 10 | (<0.1) |
| Missing | 1,478 | (5.9) |
| Family history of breast cancer | ||
| No | 22,505 | (90.6) |
| Yes | 2,335 | (9.4) |
| Percent Density (%), Mean (IQR) | 21.0 | (8.1–31.1) |
| Dense Area (cm2), Mean (IQR) | 28.0 | (14.4–37.0) |
Age at menarche and late adolescent BMI were negatively correlated (Pearson correlation=−0.16, p-value<0.001). Bivariate analyses of these two pubertal characteristics indicated a difference in mean late adolescent BMI across categories of age at menarche. Women who were younger than 10 years at menarche had a mean late adolescent BMI that was 1.39 kg/m2 higher (95%CI: 1.13 to 1.65) than women aged 12–13 years at menarche.
In linear regression models of square root transformed percent density, we found that age and BMI at screening were both inversely associated with the outcome. We found that the best fitting covariate model for age and BMI at screening included both linear and squared terms for age, and included polynomial terms up the third order for BMI. This covariate model with age and BMI terms alone explained 42.4% of the variance of PD in Hologic mammograms and 35.0% of the variance in GE mammograms. In comparison, a model with age, age squared and log-transformed BMI explained 40.8% of the variance in Hologic mammograms and 34.0% of the variance in GE mammograms. These covariate models differed mainly in the relationship of BMI to percent density among women with BMI greater than 40 or less than 20 (Figure 2).
Figure 2.
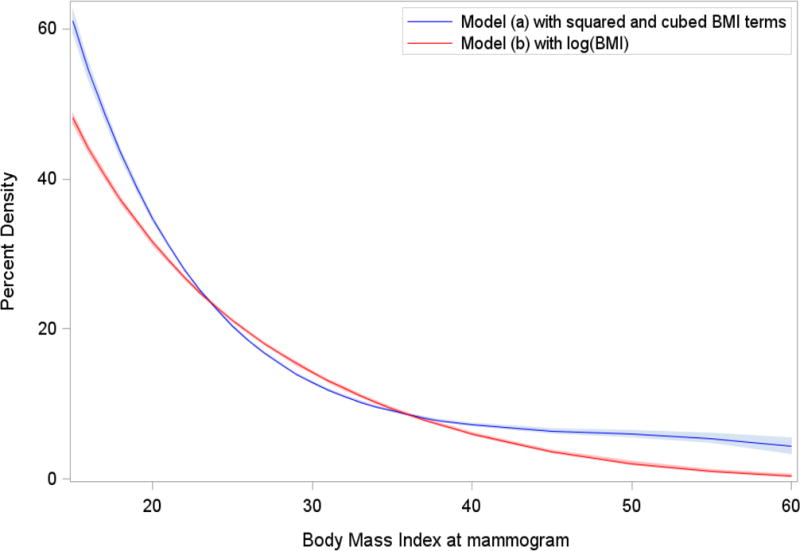
Relationship of BMI to percent density under two alternative models for BMI.
Results for the associations of age at menarche and late adolescent BMI with percent density are shown in Table 2 and Supplementary Table 1. To facilitate interpretation, parameter estimates and standard errors on the scale of square root of percent density (Supplementary Table 1) were transformed to estimate the difference in percent density (Table 2). Both age at menarche and late adolescent BMI had statistically significant associations in minimally adjusted models and in fully adjusted models. Older age at menarche was associated with increases in percent density in a minimal model adjusted only for age and BMI at screening and image batch. We tested for a linear trend across categories with respect to square root percent density. The trend across categories was statistically significant (p-value<0.0001), where a one category increase was associated with a change in PD of 0.71. The trend remained statistically significant in the fully adjusted model (p-value<0.0001), although the magnitude of the effect of the trend was attenuated: a one category increase was associated with a change in PD of 0.58. Higher late adolescent BMI was associated with lower percent density at screening age in a minimal model adjusted only for age and BMI at screening and image batch, and the association was only slightly attenuated in fully adjusted models.
Table 2.
Associations of percent density with age at menarche and late adolescent BMI.
| Minimally adjusted models† | Fully adjusted model§ | |||
|---|---|---|---|---|
|
| ||||
| Estimated Difference in PD* | 95% CI | Estimated Difference in PD* | 95% CI | |
| Age at menarche | ||||
| <10 years | −1.24 | (−2.21, −0.28) | −0.96 | (−1.93, 0.00) |
| 10–11 years | −0.48 | (−0.86, −0.11) | −0.37 | (−0.74, 0.00) |
| 12–13 years | 0.00 | Reference | 0.00 | Reference |
| 14–15 years | 0.89 | (0.49, 1.28) | 0.73 | (0.34, 1.12) |
| >16 years | 1.75 | (0.97, 2.54) | 1.47 | (0.69, 2.25) |
| Late adolescent BMI‡ | ||||
| 18.0 (10th percentile) | 0.88 | (0.83, 0.93) | 0.84 | (0.79, 0.90) |
| 19.2 (25th percentile) | 0.49 | (0.43, 0.54) | 0.47 | (0.41, 0.52) |
| 20.7 (median) | 0.00 | Reference | 0.00 | Reference |
| 22.3 (75th percentile) | −0.51 | (−0.56, −0.46) | −0.49 | (−0.54, −0.44) |
| 24.6 (90th percentile) | −1.24 | (−1.29, −1.19) | −1.19 | (−1.24, −1.14) |
Models adjusted only for age at screening, BMI at screening and image batch.
Model with simultaneous inclusion of age at menarche and late adolescent BMI, and adjusted for age at screening, BMI at screening, menopause, MHT, parity, number of children, age at first birth, family history of breast cancer, and image batch.
Parameter estimates from the model for square root of percent density were transformed to estimate the difference in percent density.
Late adolescent BMI was included as a continuous covariate with a linear relationship to square-root percent density. We present estimated differences in percent density for specific percentiles of late adolescent BMI relative to the median.
In linear regression models of cube root transformed dense area, we found that age and BMI at screening were both inversely associated with our outcome. We found that the best fitting covariate model for age and BMI at screening included linear and squared terms for both age and BMI. This covariate model with age and BMI terms alone explained 11.4% of the variance of DA in Hologic mammograms and 9.9% of the variance in GE mammograms.
Results for the associations of age at menarche and late adolescent BMI with dense area are shown in Supplementary Table 2 and Table 3. To facilitate interpretation, parameter estimates and standard errors on the scale of cube root of DA (Supplementary Table 2) were transformed to estimate the difference in DA (Table 3). Both pubertal factors had statistically significant effects in minimally adjusted models and in fully adjusted models. Later age at menarche was associated with greater dense area in minimally adjusted and fully adjusted models. A test for linear trend across categories on the scale of cube root dense area was statistically significant in the minimally adjusted model (p-value<0.0001) and the fully adjusted model (p-value<0.0001). There was some attenuation of the effect in the fully adjusted model as compared to the minimally adjusted model. Higher late adolescent BMI was associated with lower dense area in the minimally adjusted model (p-value<0.0001) and the fully adjusted model (p-value<0.0001). There was only a slight attenuation in the effect of late adolescent BMI in the fully adjusted model as compared to the minimally adjusted model.
Table 3.
Associations of dense area with age at menarche and late adolescent BMI.
| Minimally adjusted models† | Fully adjusted model§ | |||
|---|---|---|---|---|
|
| ||||
| Estimated Difference in DA*, cm2 | 95% CI | Estimated Difference in DA*, cm2 | 95% CI | |
| Age at menarche | ||||
| <10 years | −0.35 | (−1.40, 0.70) | −0.34 | (−1.74, 1.05) |
| 10–11 years | −0.64 | (−1.04, −0.25) | −0.62 | (−1.15, −0.10) |
| 12–13 years | 0.00 | Reference | 0.00 | Reference |
| 14–15 years | 0.56 | (0.14, 0.98) | 0.42 | (−0.14, 0.98) |
| >16 years | 1.76 | (0.91, 2.61) | 1.59 | (0.48, 2.70) |
| Late adolescent BMI‡ | ||||
| 18.0 (10th percentile) | 0.97 | (0.89, 1.06) | 0.94 | (0.86, 1.03) |
| 19.2 (25th percentile) | 0.54 | (0.45, 0.63) | 0.52 | (0.43, 0.61) |
| 20.7 (median) | 0.00 | Reference | 0.00 | Reference |
| 22.3 (75th percentile) | −0.57 | (−0.65, −0.48) | −0.55 | (−0.64, −0.46) |
| 24.6 (90th percentile) | −1.37 | (−1.45, −1.28) | −1.33 | (−1.41, −1.24) |
Models adjusted only for age at screening, BMI at screening and image batch.
Model with simultaneous inclusion of age at menarche and late adolescent BMI, and adjusted for age at screening, BMI at screening, menopause, MHT, parity, number of children, age at first birth, family history of breast cancer, and image batch.
Parameter estimates from the model for cube root of dense area were transformed to estimate the difference in dense area.
Late adolescent BMI was included as a continuous covariate with a linear relationship to cube-root dense area. We present estimated differences in percent density for specific percentiles of late adolescent BMI relative to the median.
We tested for effect modification by menopausal status. There was no evidence of effect modification by menopausal status on the effect of age at menarche on PD (p-value=0.8596) or DA (p-value=0.6725). We did find evidence of a statistically significant effect modification by menopausal status on the effect of late adolescent BMI on PD (p-value= 0.0311) and DA (p-value= 0.0345). The direction of the effect modification was such that a stronger effect was found in premenopausal women for the association with PD but a stronger effect was found in postmenopausal women for the association with DA. The effect modification was modest, and late adolescent BMI remained inversely associated with PD and DA among both premenopausal and postmenopausal women in fully adjusted models. Supplementary Table 3 shows the estimated associations of late adolescent BMI with PD and DA by menopausal status in fully adjusted regression models.
Discussion
In this large study of 24,840 women, we found that age at menarche was positively associated and late adolescent BMI was inversely associated with Cumulus measures of mammographic density on processed FFDM images acquired from Hologic and GE machines.
The association of age at menarche with mammographic density has been inconsistent in previous smaller studies. A number of studies have reported finding no evidence of an association between age at menarche and measures of mammographic density (14,17,24–26). Some studies have reported a positive trend between percent density and age at menarche. Butler et al. (13) reported that percent density increased with increasing age at menarche among pre-and perimenopausal women in unadjusted models, but the trend was not statistically significant in fully adjusted models. Haars et al. (22) reported a positive association between age at menarche and dense area. A positive association between age at menarche and patterns of higher density using Wolfe’s density classification has been reported, which was statistically significant in both adjusted and unadjusted models (19). Our finding of a positive association between age at menarche and percent density is supported by these previous studies that showed some evidence of a positive trend. Moreover, our study provides new stronger evidence because the associations were statistically significant for both percent density and dense area in fully adjusted models.
Although adult BMI at mammography screening is known to have a strong inverse association with PD, very few studies have examined BMI in early life around age 18, puberty or in childhood. The few studies that have examined BMI during these earlier periods have found an inverse association with mammographic density, similar to the association with adult BMI. A study of childhood weight/BMI identified an inverse association between mammographic density measures and BMI measured at ages 7–15 years with the strongest in late adolescence (20). Similarly, Soguel et al. (27) found a negative correlation between BMI at 18 years of age and mammographic density, with correlations of −0.18 and −0.09 for PD and DA, respectively.
Age at menarche and late adolescent BMI are interrelated. Earlier age at menarche is associated with higher BMI in adolescence and higher risk of obesity during young adulthood and midlife (28–30). One concern is that many previously reported associations of age at menarche and mammographic density were reported only in unadjusted models. We found robust positive trends between age at menarche and mammographic density measures that remained statistically significant in fully adjusted models including BMI in youth and adulthood and reproductive factors later in life. Thus, our study provides new evidence that age at menarche is independently positively associated with percent density even after adjusting for BMI at screening and late adolescent BMI.
Overall, effect sizes for both age at menarche and late adolescent BMI were modest. The difference in PD between the youngest and oldest age at menarche categories was estimated to be 2.43% in our fully adjusted model. The difference in PD between the 10th and 90th percentiles of post-adolescent BMI was estimated to be 2.03% in our fully adjusted model. In comparison, postmenopausal hormone use, a well-established risk factor for increased mammographic density, has been associated with difference in PD of approximately 6% (31,32). One reason that previous studies of age at menarche have reported inconsistent effects could be that greater power is required to detect smaller effect sizes.
Although we did find evidence of a statistically significant effect modification by menopausal status on the effect of late adolescent BMI on PD, the effect modification was modest, and late adolescent BMI remained inversely associated with PD and DA among both premenopausal and postmenopausal women in fully adjusted models. Thus, the statistically significant interaction may not represent a true biologic interaction. We also note that these interaction tests were secondary analyses performed after the main statistical analyses and the statistically significant p-values were close to 0.05; thus considerations of multiple testing would indicate that these nominally statistically significant interactions be interpreted more as suggestive effects. In addition, although we adjusted for BMI at the time of the mammogram, it is possible that there is additional confounding by BMI changes across the lifespan.
Relationship to breast cancer risk
Age at menarche is inversely associated with breast cancer risk (33). Since mammographic density has a strong positive relationship to breast cancer risk, one might expect that age at menarche would be inversely associated with mammographic density. In contrast, we found that age at menarche is associated positively with mammographic density. Because these associations are not in the same direction, this suggests that the effect of age at menarche on breast cancer risk is not predominantly mediated through a pathway reflected directly or indirectly by mammographic density. Our findings are supported by a recent mediation analysis, which found that the association of age at menarche with breast cancer risk was not mediated by PD (34). Additional studies are needed to further elucidate the relationship between different pubertal stages and breast density.
BMI in late adolescence is inversely associated with breast cancer risk (35–39). Thus, BMI at screening and BMI in late adolescence are associated with breast cancer risk in different directions. However, the inverse association of late adolescent BMI with both mammographic density and breast cancer risk suggests that the effect of late adolescent BMI on breast cancer risk could be mediated through a pathway acting on mammographic density. Our findings are supported by a large cohort study which found evidence that the inverse association of youth body fatness and breast cancer was mediated by mammographic density (36).
A number of mechanisms have been hypothesized to explain the relationship of mammographic density to breast cancer risk; these potential mechanisms are reviewed in Martin and Boyd 2008 (40) and Pettersson and Tamimi 2014 (41). Studies of the histologic basis of mammographic density show that breast tissue collagen is a major component explaining up to 29% of the variation in percent density (40), and studies have consistently reported that mammographic density is positively associated with the stroma in breast tissue samples (41–43). Age and postmenopausal BMI are positively associated with breast cancer risk (44), inversely associated with mammographic density(45), and inversely related to the percentage of collagen found in breast tissue (46). In contrast, number of live births is inversely associated with breast cancer risk (44), inversely associated with mammographic density(45), and inversely related to the percentage of collagen found in breast tissue (46). Growth factors like IGF-1 and stromal matrix proteins like stromal proteoglycan, expressed in association with breast cancer, have been highlighted as important factors also associated with mammographic density (40,46). Endogenous estrogen is positively associated with breast cancer risk in many studies (47). Mammographic density may reflect cumulative exposure to endogenous estrogens, which may increase breast cancer risk through its mitogenic effects (40). Breast size has been reported to modify the association of dense area with breast cancer, with weaker associations found in larger breasts (48). Thus, the inverse associations of late adolescent BMI with breast density and cancer risk may be mediated by increased non-dense (fatty) area and adipocytes that support normal breast epithelial proliferation throughout puberty and inhibit later carcinogenesis (40).
Strengths and Limitations
This study has a number of strengths and limitations. This is the largest cohort study of mammographic density to date and has high statistical power to identify novel epidemiologic risk factors. In addition, all mammographic density measurements were performed by a single radiological technologist using the well-established Cumulus method. Full-field digital mammography is now standard practice in many health care settings, while most research is still based on conventional film mammography. Studies that established Cumulus as the gold standard measurement of mammographic density by showing strong associations with breast cancer risk have used images that were obtained using film mammography and subsequently digitized (1,2,4,11,49). Recently, we reported that mammographic density assessed by Cumulus on FFDM images show similarly strong associations with breast cancer risk, validating the use of Cumulus measures on FFDM images (5).
The cohort is characterized by a wide range of covariate values across age and BMI, and includes both pre-menopausal and post-menopausal women, and is drawn from a population-based sample unselected for breast cancer status or other phenotypes; all of these factors increase the generalizability of results. One limitation is that the cohort includes only non-Hispanic white women because it is ancillary to a GWAS, thus it is not representative of race/ethnicity differences in mammographic density.
In any retrospective study when survey data is collected to assess past information, there is potential for recall bias; however, this is population sample study and density reads were done blinded to survey responses, so any measurement error in the survey data covariates would be nondifferential with respect to density. Another concern arising from the survey data is the missing responses. Since restricting to a complete case analysis would likely induce bias in the parameter estimates, we used an imputation approach which is expected to yield unbiased parameter estimates (21). In addition, we performed a sensitivity analysis by creating a missing category for each variable, and we found that the magnitude and direction of our results were consistent, indicating that our findings were not overly influenced by our imputation procedure.
Conclusions
In this large population-based study, we found that the pubertal factors age at menarche and late adolescent BMI were each associated with quantitative measures of mammographic density. These associations were consistent in minimally adjusted models and fully adjusted models, and across both percent density and dense area. Results support the hypothesis that late adolescent BMI may be associated with breast cancer via a pathway acting on density. However, results do not support a similar hypothesis for age at menarche. Further research is needed to elucidate the biological mechanisms through which early-life factors influence mammographic density and later breast cancer risk, to determine any differences by race and ethnicity, and to enable better early prevention of breast cancer.
Supplementary Material
Acknowledgments
We are grateful to the Kaiser Permanente Northern California members who generously agreed to participate in the Kaiser Permanente Research Program on Genes, Environment and Health. We thank Mark Westley and Marvella Villaseñor at the Division of Research, Marc Sofilos and Shannon Walters in the Stanford Radiology 3D and Quantitative Imaging Laboratory, and Anoma Gunasekara and Gordon Mawdsley at Sunnybrook Health Sciences Center for their technical expertise and assistance.
This study was supported by the National Cancer Institute (R01 CA166827, PI Sieh; K07 CA143047, PI Sieh; and R01 CA168893, PI Habel).
References
- 1.Boyd NF, Guo H, Martin LJ, Sun L, Stone J, Fishell E, et al. Mammographic density and the risk and detection of breast cancer. N Engl J Med. 2007;356:227–36. doi: 10.1056/NEJMoa062790. [DOI] [PubMed] [Google Scholar]
- 2.McCormack VA, dos Santos Silva I. Breast density and parenchymal patterns as markers of breast cancer risk: a meta-analysis. Cancer Epidemiol Biomarkers Prev. 2006;15:1159–69. doi: 10.1158/1055-9965.EPI-06-0034. [DOI] [PubMed] [Google Scholar]
- 3.Boyd NF, Rommens JM, Vogt K, Lee V, Hopper JL, Yaffe MJ, et al. Mammographic breast density as an intermediate phenotype for breast cancer. Lancet Oncol. 2005;6:798–808. doi: 10.1016/S1470-2045(05)70390-9. [DOI] [PubMed] [Google Scholar]
- 4.Byng JW, Yaffe MJ, Jong RA, Shumak RS, Lockwood GA, Tritchler DL, et al. Analysis of mammographic density and breast cancer risk from digitized mammograms. Radiographics. 1998;18:1587–98. doi: 10.1148/radiographics.18.6.9821201. [DOI] [PubMed] [Google Scholar]
- 5.Habel LA, Lipson JA, Achacoso N, Rothstein JH, Yaffe MJ, Liang RY, et al. Case-control study of mammographic density and breast cancer risk using processed digital mammograms. Breast Cancer Res. 2016;18:53. doi: 10.1186/s13058-016-0715-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Fowler EE, Vachon CM, Scott CG, Sellers TA, Heine JJ. Automated Percentage of Breast Density Measurements for Full-field Digital Mammography Applications. Acad Radiol. 2014;21:958–70. doi: 10.1016/j.acra.2014.04.006. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Vachon CM, Fowler EE, Tiffenberg G, Scott CG, Pankratz VS, Sellers TA, et al. Comparison of percent density from raw and processed full-field digital mammography data. Breast Cancer Res. 2013;15:R1. doi: 10.1186/bcr3372. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Boyd N, Martin L, Chavez S, Gunasekara A, Salleh A, Melnichouk O, et al. Breast-tissue composition and other risk factors for breast cancer in young women: a cross-sectional study. Lancet Oncol. 2009;10:569–80. doi: 10.1016/S1470-2045(09)70078-6. [DOI] [PubMed] [Google Scholar]
- 9.Huo CW, Chew GL, Britt KL, Ingman WV, Henderson MA, Hopper JL, et al. Mammographic density-a review on the current understanding of its association with breast cancer. Breast Cancer Res Treat. 2014;144:479–502. doi: 10.1007/s10549-014-2901-2. [DOI] [PubMed] [Google Scholar]
- 10.Boyd NF, Lockwood GA, Byng JW, Little LE, Yaffe MJ, Tritchler DL. The relationship of anthropometric measures to radiological features of the breast in premenopausal women. Br J Cancer. 1998;78:1233–8. doi: 10.1038/bjc.1998.660. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Tamimi RM, Hankinson SE, Colditz GA, Byrne C. Endogenous sex hormone levels and mammographic density among postmenopausal women. Cancer Epidemiol Biomarkers Prev. 2005;14:2641–7. doi: 10.1158/1055-9965.EPI-05-0558. [DOI] [PubMed] [Google Scholar]
- 12.Brisson J, Sadowsky NL, Twaddle JA, Morrison AS, Cole P, Merletti F. The relation of mammographic features of the breast to breast cancer risk factors. Am J Epidemiol. 1982;115:438–43. doi: 10.1093/oxfordjournals.aje.a113321. [DOI] [PubMed] [Google Scholar]
- 13.Butler LM, Gold EB, Greendale GA, Crandall CJ, Modugno F, Oestreicher N, et al. Menstrual and reproductive factors in relation to mammographic density: the Study of Women’s Health Across the Nation (SWAN) Breast Cancer Res Treat. 2008;112:165–74. doi: 10.1007/s10549-007-9840-0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Nguyen TL, Schmidt DF, Makalic E, Dite GS, Stone J, Apicella C, et al. Explaining variance in the cumulus mammographic measures that predict breast cancer risk: a twins and sisters study. Cancer Epidemiol Biomarkers Prev. 2013;22:2395–403. doi: 10.1158/1055-9965.EPI-13-0481. [DOI] [PubMed] [Google Scholar]
- 15.Menarche, menopause, and breast cancer risk: individual participant meta-analysis, including 118 964 women with breast cancer from 117 epidemiological studies. Lancet Oncol. 2012;13:1141–51. doi: 10.1016/S1470-2045(12)70425-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Ahlgren M, Melbye M, Wohlfahrt J, Sorensen TI. Growth patterns and the risk of breast cancer in women. N Engl J Med. 2004;351:1619–26. doi: 10.1056/NEJMoa040576. [DOI] [PubMed] [Google Scholar]
- 17.Gapstur SM, Lopez P, Colangelo LA, Wolfman J, Van Horn L, Hendrick RE. Associations of breast cancer risk factors with breast density in Hispanic women. Cancer Epidemiol Biomarkers Prev. 2003;12:1074–80. [PubMed] [Google Scholar]
- 18.Maskarinec G, Pagano I, Lurie G, Kolonel LN. A longitudinal investigation of mammographic density: the multiethnic cohort. Cancer Epidemiol Biomarkers Prev. 2006;15:732–9. doi: 10.1158/1055-9965.EPI-05-0798. [DOI] [PubMed] [Google Scholar]
- 19.Bucchi L, Costantini M, Buzzi G, Bravetti P, Cicognani A, Torta M, et al. Wolfe’s mammographic patterns in women with gross cystic disease of the breast. J Clin Epidemiol. 1995;48:969–76. doi: 10.1016/0895-4356(94)00226-g. [DOI] [PubMed] [Google Scholar]
- 20.Hopper JL, Nguyen TL, Stone J, Aujard K, Matheson MC, Abramson MJ, et al. Childhood body mass index and adult mammographic density measures that predict breast cancer risk. Breast Cancer Res Treat. 2016;156:163–70. doi: 10.1007/s10549-016-3719-x. [DOI] [PubMed] [Google Scholar]
- 21.Schafer JL. Analysis of Incomplete Multivariate Data. New York: Chapman & Hall; 1997. [Google Scholar]
- 22.Haars G, van Noord PA, van Gils CH, Grobbee DE, Peeters PH. Measurements of breast density: no ratio for a ratio. Cancer Epidemiol Biomarkers Prev. 2005;14:2634–40. doi: 10.1158/1055-9965.EPI-05-0824. [DOI] [PubMed] [Google Scholar]
- 23.Cox C. Delta Method Encyclopedia of Biostatistics. John Wiley & Sons; 2005. [Google Scholar]
- 24.Hart V, Reeves KW, Sturgeon SR, Reich NG, Sievert LL, Kerlikowske K, et al. The effect of change in body mass index on volumetric measures of mammographic density. Cancer Epidemiol Biomarkers Prev. 2015;24:1724–30. doi: 10.1158/1055-9965.EPI-15-0330. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Heng D, Gao F, Jong R, Fishell E, Yaffe M, Martin L, et al. Risk factors for breast cancer associated with mammographic features in Singaporean chinese women. Cancer Epidemiol Biomarkers Prev. 2004;13:1751–8. [PubMed] [Google Scholar]
- 26.Modugno F, Ngo DL, Allen GO, Kuller LH, Ness RB, Vogel VG, et al. Breast cancer risk factors and mammographic breast density in women over age 70. Breast Cancer Res Treat. 2006;97:157–66. doi: 10.1007/s10549-005-9105-8. [DOI] [PubMed] [Google Scholar]
- 27.Soguel L, Diorio C. Anthropometric factors, adult weight gain, and mammographic features. Cancer Causes Control. 2016;27:333–40. doi: 10.1007/s10552-015-0706-1. [DOI] [PubMed] [Google Scholar]
- 28.Garn SM, LaVelle M, Rosenberg KR, Hawthorne VM. Maturational timing as a factor in female fatness and obesity. Am J Clin Nutr. 1986;43:879–83. doi: 10.1093/ajcn/43.6.879. [DOI] [PubMed] [Google Scholar]
- 29.Biro FM, McMahon RP, Striegel-Moore R, Crawford PB, Obarzanek E, Morrison JA, et al. Impact of timing of pubertal maturation on growth in black and white female adolescents: The National Heart, Lung, and Blood Institute Growth and Health Study. J Pediatr. 2001;138:636–43. doi: 10.1067/mpd.2001.114476. [DOI] [PubMed] [Google Scholar]
- 30.Laitinen J, Power C, Jarvelin MR. Family social class, maternal body mass index, childhood body mass index, and age at menarche as predictors of adult obesity. Am J Clin Nutr. 2001;74:287–94. doi: 10.1093/ajcn/74.3.287. [DOI] [PubMed] [Google Scholar]
- 31.Stuedal A, Ma H, Bjorndal H, Ursin G. Postmenopausal hormone therapy with estradiol and norethisterone acetate and mammographic density: findings from a cross-sectional study among Norwegian women. Climacteric. 2009;12:248–58. doi: 10.1080/13697130802638458. [DOI] [PubMed] [Google Scholar]
- 32.Bremnes Y, Ursin G, Bjurstam N, Lund E, Gram IT. Different types of postmenopausal hormone therapy and mammographic density in Norwegian women. International journal of cancer. 2007;120:880–4. doi: 10.1002/ijc.22437. [DOI] [PubMed] [Google Scholar]
- 33.Collaborative Group on Hormonal Factors in Breast Cancer. Menarche, menopause, and breast cancer risk: individual participant meta-analysis, including 118 964 women with breast cancer from 117 epidemiological studies. Lancet Oncol. 2012;13:1141–51. doi: 10.1016/S1470-2045(12)70425-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Rice MS, Bertrand KA, VanderWeele TJ, Rosner BA, Liao X, Adami HO, et al. Mammographic density and breast cancer risk: a mediation analysis. Breast Cancer Res. 2016;18:94. doi: 10.1186/s13058-016-0750-0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Harris HR, Tamimi RM, Willett WC, Hankinson SE, Michels KB. Body size across the life course, mammographic density, and risk of breast cancer. Am J Epidemiol. 2011;174:909–18. doi: 10.1093/aje/kwr225. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Andersen ZJ, Baker JL, Bihrmann K, Vejborg I, Sorensen TI, Lynge E. Birth weight, childhood body mass index, and height in relation to mammographic density and breast cancer: a register-based cohort study. Breast Cancer Res. 2014;16:R4. doi: 10.1186/bcr3596. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Bardia A, Vachon CM, Olson JE, Vierkant RA, Wang AH, Hartmann LC, et al. Relative weight at age 12 and risk of postmenopausal breast cancer. Cancer Epidemiol Biomarkers Prev. 2008;17:374–8. doi: 10.1158/1055-9965.EPI-07-0389. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Baer HJ, Tworoger SS, Hankinson SE, Willett WC. Body fatness at young ages and risk of breast cancer throughout life. Am J Epidemiol. 2010;171:1183–94. doi: 10.1093/aje/kwq045. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Berkey CS, Frazier AL, Gardner JD, Colditz GA. Adolescence and breast carcinoma risk. Cancer. 1999;85:2400–9. doi: 10.1002/(sici)1097-0142(19990601)85:11<2400::aid-cncr15>3.0.co;2-o. [DOI] [PubMed] [Google Scholar]
- 40.Martin LJ, Boyd NF. Mammographic density. Potential mechanisms of breast cancer risk associated with mammographic density: hypotheses based on epidemiological evidence. Breast Cancer Res. 2008;10:201. doi: 10.1186/bcr1831. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Pettersson A, Graff RE, Ursin G, Santos Silva ID, McCormack V, Baglietto L, et al. Mammographic density phenotypes and risk of breast cancer: a meta-analysis. J Natl Cancer Inst. 2014;106 doi: 10.1093/jnci/dju078. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Ghosh K, Brandt KR, Reynolds C, Scott CG, Pankratz VS, Riehle DL, et al. Tissue composition of mammographically dense and non-dense breast tissue. Breast Cancer Res Treat. 2012;131:267–75. doi: 10.1007/s10549-011-1727-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.Alowami S, Troup S, Al-Haddad S, Kirkpatrick I, Watson PH. Mammographic density is related to stroma and stromal proteoglycan expression. Breast Cancer Res. 2003;5:R129–35. doi: 10.1186/bcr622. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.Key TJ, Verkasalo PK, Banks E. Epidemiology of breast cancer. Lancet Oncol. 2001;2:133–40. doi: 10.1016/S1470-2045(00)00254-0. [DOI] [PubMed] [Google Scholar]
- 45.Titus-Ernstoff L, Tosteson AN, Kasales C, Weiss J, Goodrich M, Hatch EE, et al. Breast cancer risk factors in relation to breast density (United States) Cancer Causes Control. 2006;17:1281–90. doi: 10.1007/s10552-006-0071-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46.Li T, Sun L, Miller N, Nicklee T, Woo J, Hulse-Smith L, et al. The association of measured breast tissue characteristics with mammographic density and other risk factors for breast cancer. Cancer Epidemiol Biomarkers Prev. 2005;14:343–9. doi: 10.1158/1055-9965.EPI-04-0490. [DOI] [PubMed] [Google Scholar]
- 47.Key TJ, Appleby PN, Reeves GK, Travis RC, Alberg AJ, Barricarte A, et al. Sex hormones and risk of breast cancer in premenopausal women: a collaborative reanalysis of individual participant data from seven prospective studies. Lancet Oncol. 2013;14:1009–19. doi: 10.1016/S1470-2045(13)70301-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 48.Stuedal A, Ma H, Bernstein L, Pike MC, Ursin G. Does breast size modify the association between mammographic density and breast cancer risk? Cancer Epidemiol Biomarkers Prev. 2008;17:621–7. doi: 10.1158/1055-9965.EPI-07-2554. [DOI] [PubMed] [Google Scholar]
- 49.Ursin G, Lillie EO, Lee E, Cockburn M, Schork NJ, Cozen W, et al. The relative importance of genetics and environment on mammographic density. Cancer Epidemiol Biomarkers Prev. 2009;18:102–12. doi: 10.1158/1055-9965.EPI-07-2857. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.