

Abstract
Research identifying racial and ethnic disparities in child protective services (CPS) involvement in the U.S. has focused on the overrepresentation of Black children and the growing Latino child population. Little attention has been paid to children of Asian origin, the most underrepresented group of children in the U.S. CPS system. The objective of this analysis was to examine subgroup patterns of CPS involvement in California for Asian and Pacific Islander (API) children prospectively based on maternal nativity and ethnic origin. We extracted data for API children born in California in 2006 and 2007 (N = 138,858) from population-based birth records and linked those records to CPS records spanning the first 5 years of life (through 2012). We assessed distributional differences in risk indicators for the full birth cohort of API children and calculated a summary risk variable representing the cumulative number of risks present at birth. Generalized linear models were used to estimate API children’s adjusted relative risk of CPS report by subgroup. Overall, 12.2% of children born in California in the 2006–2007 birth cohort were API. The majority of API children had foreign-born mothers (80.9%). Children of U.S.-born Hawaiian, Guamanian, or Samoan mothers had the highest rate, with 20.4% being reported to CPS by their 5th birthday. The lowest rates of child abuse and neglect reporting were observed among children of foreign-born Asian Indian (2.5%), Korean (2.7%), and Chinese (2.8%) mothers, compared to 5.4% of all Asian and Pacific Islander children, and 14.8% of children in general population. Findings underscore the presence of disparities in CPS involvement among API children, which has implications for health and well-being across the life course and for targeted maltreatment prevention strategies.
Keywords: child welfare system, racial and ethnic disparities, foreign-born, Asian and Pacific Islander, California
Research identifying racial and ethnic disparities in child protective services (CPS) involvement in the U.S. has largely focused on the overrepresentation of Black children (Lanier, Maguire-Jack, Walsh, Drake, & Hubel, 2014; Putnam-Hornstein, Needell, King, & Johnson-Motoyama, 2013; Drake, Jolley, Fluke, Lanier, Barth, & Jonson-Reid, 2011) and the growing Latino child population (Johnson-Motoyama, Putnam-Hornstein, Dettlaff, Zhao, Finno-Velasquez, & Needell, 2015; Cardoso, Dettlaff, Finno-Velasquez, Scott, & Faulkner, 2014; Putnam-Hornstein et al., 2013). Growing concern around enhancing sensitivity to ethnicity and culture in the child welfare field has led to increasing efforts to disaggregate data by ethnic groups to identify potentially unique patterns of child maltreatment risk based on factors such as parental birthplace. Despite increased attention given to ethnic and cultural diversity with Latino and Native American groups in child abuse and neglect research and practice, relatively little research has focused on the scope of child abuse in the Asian and Pacific Islander (API) population (Fong & Mokuau, 1994).
API groups comprise 30% of the total immigrant population in the U.S., with a disproportionate concentration residing in California (Grieco et al., 2010; U.S. Census Bureau, 2010). In 2010, API groups surpassed Latino immigrants as the fastest-growing minority population, with the number of foreign- and U.S.-born API residents growing 46% from 2000 to 2010 and 10% from 2010 to 2013 (U.S. Census Bureau, 2012). This growth is expected to continue, with the U.S. Census Bureau predicting the API population to increase 79% by 2050 (Ortman & Guarneri, 2009).
National data aggregated by ethnic group have consistently reported API children to be at lower risk of maltreatment than other groups, but the few studies that examined subgroup differences suggest otherwise. In 2014, the rate of substantiated or indicated maltreatment reports of abuse or neglect among API children in the United States was 1.7 per 1,000, much lower than other races and ethnicities (8.6 per 1,000 for Whites, 8.8 per 1,000 for Hispanics, and 15.3 per 1,000 for African Americans; U.S. Department of Health and Human Services, 2016). In California, in the 2006–2007 birth cohort, by the age of 5 just 5.4% of API children were reported to CPS, compared to 13.7% of White children, 31.6% of African American children, 21.2% of Latino children of U.S. born mothers, 11.8% of Latino children of foreign born mothers, and 36.5% of Native American children (Putnam-Hornstein, Mitchell, & Hammond, 2014). These numbers suggest that API children are less likely to become involved with CPS than children of other racial and ethnic groups, yet researchers have not accounted for factors that might contribute to diversity in the general API population, such as ethnic origin and maternal nativity.
Additionally, no known studies have prospectively followed a group of API children from birth to determine exposure to risk of report to CPS. Although sparse, existing regionally based studies have demonstrated a great deal of variation in patterns of abuse and neglect among Asian subgroups with a history of involvement with CPS. For example, an examination of 1,263 API families reported for suspected child abuse to the Washington State Division of Child and Family Services Case and Management Information System between 1995 and 1997 found that Southeast Asian and Samoan families were overrepresented relative to the overall API community, whereas Japanese, Chinese, Korean, and Filipino families were underrepresented (Pelczarski & Kemp, 2006). A study in San Diego, California, that examined 158 API families reported for child maltreatment determined that Filipinos, Pacific Islanders, and Koreans were less likely to have a report of child abuse and neglect, whereas Vietnamese and Cambodians were more likely to be referred (Ima & Hohm, 1991). Another study examining child maltreatment among Korean, Vietnamese, Chinese, and Cambodian families analyzed 761 case files retrieved from the Asian Pacific Unit of the Los Angeles County Department of Children and Family Services. In that study, Cambodian refugee families were the most frequently reported ethnic group and were overrepresented in CPS reports compared to their share in the Los Angeles population (Chang, Rhee, & Berthold, 2008; Chang, Rhee, & Weaver, 2006; Rhee, Chang, Berthold, & Mar, 2012; Rhee, Chang, Weaver, & Wong, 2008).
Additionally, a recent theory of cumulative risk that has shown the number of exposures to different household risks to influence the potential for child maltreatment (Begle, Dumas, & Hanson, 2010). Despite the fact that APIs fare better across a range of health outcomes compared to other racial groups (e.g., Barnes, Adams, & Powell-Griner, 2008; Ye, Rust, Baltrus, & Daniels, 2009), a closer examination of risk associated with CPS involvement revealed substantial diversity in various health and prenatal risks in different API ethnic groups (e.g., Gomez, Kelsey, Glaser, Lee, & Sidney, 2004; Holland & Palaniappan, 2012; Islam et al., 2010). For instance, although definitions of Pacific Islander are inconsistent across studies, in general, this group tends to present with worse health, mental health, and access to health care than other Asian groups (Aczon-Armstrong, Inounye, & Reyes-Salvail, 2013; Bitton, Zaslavsky, & Ayanian, 2010; Juarez, Samoa, Chung, & Seto, 2010). Furthermore, some important prenatal and perinatal indicators of risk for child maltreatment, such as maternal age, maternal education, birth weight, and insurance type, have been found to vary by API ethnic origin (Rao, Daniels, El-Sayed, Moshesh, & Caughey, 2006; Schempf, Mendola, Hamilton, Hayes, & Makuc, 2010; Wong et al., 2008). Socioeconomic risks most highly correlated with child protection involvement also vary widely in the API population. Asian Indians and Chinese Americans, for example, have on average much higher levels of college education than Southeast Asian groups (Allard, 2011). And compared to other ethnic groups, a substantial proportion of Cambodians, Hmong, Laotians, and Samoans live in poverty (U.S. Census Bureau, 2012). Given such variability in health and socioeconomic risks of different API ethnic groups, it is possible that differences in cumulative exposure to such risks may contribute to differential rates of maltreatment reports among API subgroups.
Another factor to consider when examining CPS involvement among API groups is parent (typically maternal) nativity. In the Latino child population, a small but growing body of work highlights the protective effect of parent immigrant status as it relates to CPS involvement, wherein children of Latino immigrants have overall lower rates of reporting, substantiation, and risks associated with maltreatment, than children of U.S. born Latino parents (Cardoso, Dettlaff, Finno-Velasquez, Scott & Faulkner, 2014; Dettlaff, Earner, & Phillips, 2009; Johnson-Motoyama et al., 2015; Putnam-Hornstein & Needell, 2011; Putnam-Hornstein et al., 2013). It is equally plausible that differences in nativity in the API population—which may be reflective of characteristics of recent immigrants that differentiate them from those who do not migrate and distinctive cultural norms, processes, behaviors, interactions with systems, and environmental contexts around family and community supports—may also result in varying levels of involvement with CPS. Yet because API children have, for the most part, been studied as a panethnic group, the extent to which immigrant status protects API children from abuse and neglect is unknown.
To our knowledge, no studies have examined the effect of ethnic affiliation in conjunction with nativity on risk of CPS involvement among children born to API mothers. We take advantage of the state of California having the largest and most diverse API population in the U.S. (Ponce et al., 2009) by prospectively following API children born in California to their 5th birthday to determine whether the cumulative likelihood that a child is reported for maltreatment differs by API maternal nativity and ethnic origin.
Methods
Dataset
This analysis is based on an Asian and Pacific Islander subset of a population-based dataset constructed by linking California vital birth records to CPS records (Putnam-Hornstein, Mitchell, & Hammond, 2014). CPS records were matched to the complete file of 2006 and 2007 birth records during the first 5 years of life using open source, probabilistic linkage software (Campbell, Deck, & Krupski, 2008; Registry Plus, 2007), with potential record pairs established based on a combination of unique (e.g., maternal Social Security number) and nonunique (e.g., first and last name, date of birth) child and parental personal identifiers common to both files. Once record pairs were generated, match score thresholds were established for determining a record pair to be a match or a nonmatch. All pairs falling between the lower- and upper-bound scores were clerically reviewed before a final match assignment was made. This analytic dataset consisted of all births occurring in 2006 and 2007 for which maternal race and ethnicity was self-reported as Asian in the vital birth record data (N = 138,858). Birth records also indicated mother’s place of birth, which was used to determine maternal nativity. In the analytic sample, individuals were further stratified by ethnic origin, again as self-reported by the mother. Each child’s cumulative CPS involvement was documented until their 6th birthday (through 2012). This study received approval from California’s Health and Human Services’ Committee for the Protection of Human Subjects and [blinded for review].
Variables
Dependent variable
In this analysis, we defined CPS involvement as any report of maltreatment between birth and their 5th birthday. We examined all reports of maltreatment made to the central intake unit, including those that were not evaluated in for investigation, regardless of whether the child was substantiated as a victim of maltreatment. The decision was made to focus on all reports because in the interest of preventing maltreatment in early childhood, a report is a strong indicator of risk to children even when maltreatment is not substantiated. Additionally, in preliminary analyses, overall patterns of report among different API subgroups did not substantially differ from substantiation patterns of these same groups, alleviating concerns of disproportionate reporting of some groups due to biases.
Independent variables
Children were categorized based both on self-reported maternal nativity (U.S.-born, foreign-born) and ethnic origin as recorded in the birth record (Filipino, Chinese, Asian Indian, Vietnamese, Korean, Japanese, Hmong, Cambodian, Laotian, Thai, Hawaiian, Guamanian, Samoan, Pacific Islander). Ethnic affiliation was disaggregated to the smallest denominator allowable to complete analyses, in order to to draw comparisons between ethnic subgroups that fall under the broader ethnic category of “Asian” on California birth records. Paternal nativity was not considered because of high missingness of paternity information and our analytic focus on prenatal indicators and maternal health conditions that reflect risk factors. Just eight children in the overall birth cohort of 1,133,226 could not be identified by maternal nativity or race and ethnicity. Surveys of APIs in California vary substantially in how they define Asian subgroup categorizations, sometimes including Native Hawaiian and other Pacific Island groups, and other times not (Islam et al., 2010). In this analysis, all children whose mothers identified as being of Asian race/ethnicity were included in analyses, but separate categories were created only for the largest ethnic origin subgroups. This included many groups from East Asia (Chinese, Korea, Japanese), Southeast Asia (Filipino, Hmong, Cambodian, Laotian, Vietnamese, Thai), and India. Variables of interest did not differ significantly between children of U.S. territory Hawaiian, Guamanian, and Samoan mothers, and as such we combined these groups into one group for analyses to ensure a sufficient level of aggregation. Those from other Pacific Islands (defined by the Census as including Polynesian, Micronesian, and Melanesian islands)) were considered to be their own ethnic group on child birth records.
Risk covariates
Covariates drawn from birth records were used to explore and control for subgroup variation in risk of CPS involvement, and included maternal characteristics surrounding the birth and measures of socioeconomic status. The following variables were dichotomized to represent the presence of risk (yes or no) of the following: low infant birth weight (< 2500 grams); no or missing prenatal care; maternal education of a high school degree or less; maternal age of less than 20 years; paternity missing; and public health insurance. Rates of missing values for all risk covariates were very low, ranging from 0.01% (maternal age) to 1.75% (maternal education). Among women giving birth without health insurance in California, children are retroactively enrolled in the state’s public health insurance program and therefore fall in the public birth payment group. Paternity was coded based on whether or not a father was named on the birth record. Paternity established at birth serves as a proxy for marriage and/or household status (two parents vs. one parent) and financial and social resources available to the mother during early childhood. In California, paternity is established through marriage or when a father signs a voluntary declaration of paternity in the hospital. These risk co-variates were used to create a cumulative risk variable indicating the total number of risks present at childbirth (0, 1, 2, or 3+).
Analysis
We used chi-square tests to assess distributional differences in risk indicators for the full 2006–2007 birth cohort of API children, with stratifications by maternal nativity and ethnic origin. We calculated a variable representing the cumulative number of risks present at birth by summing the presence of the five risk covariates. Figure 1 documents distributional differences in cumulative number of risks stratified by maternal nativity and ethnic origin. We used generalized linear models to estimate the adjusted relative risk of report in models stratified by nativity and origin. CPS report by maternal nativity and ethnic origin are presented as percentages. Rate ratios (RR) with corresponding 95% confidence intervals (CI) for each U.S.-born and foreign-born ethnic group are depicted in Figure 2.
Figure 1.
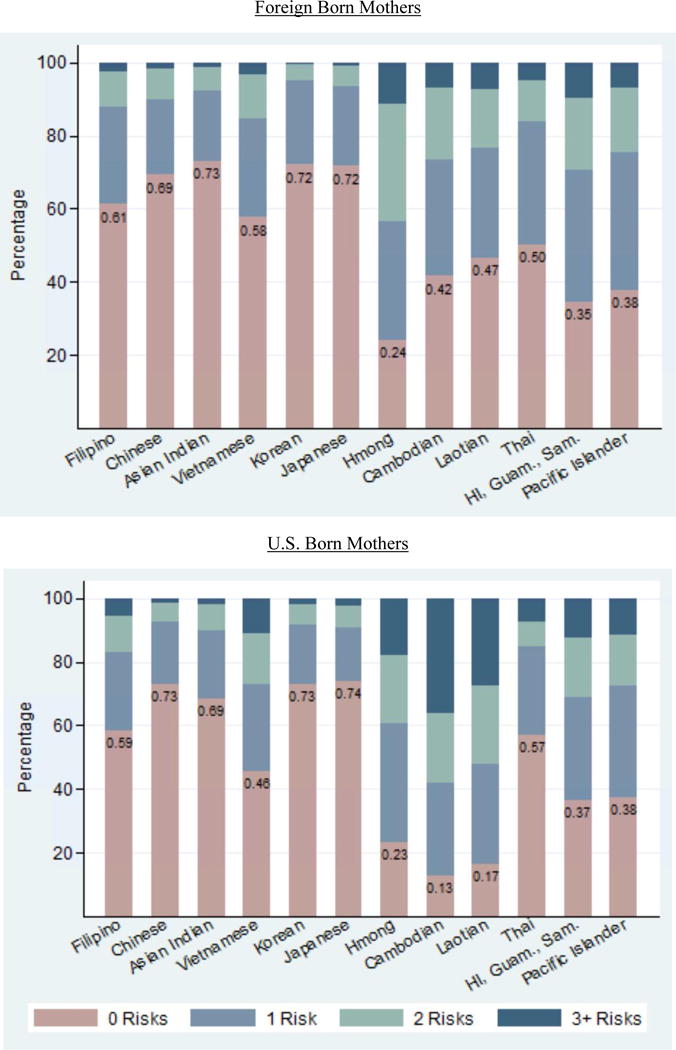
Cumulative number of risks by maternal nativity and ethnic origin (%)
Figure 2.
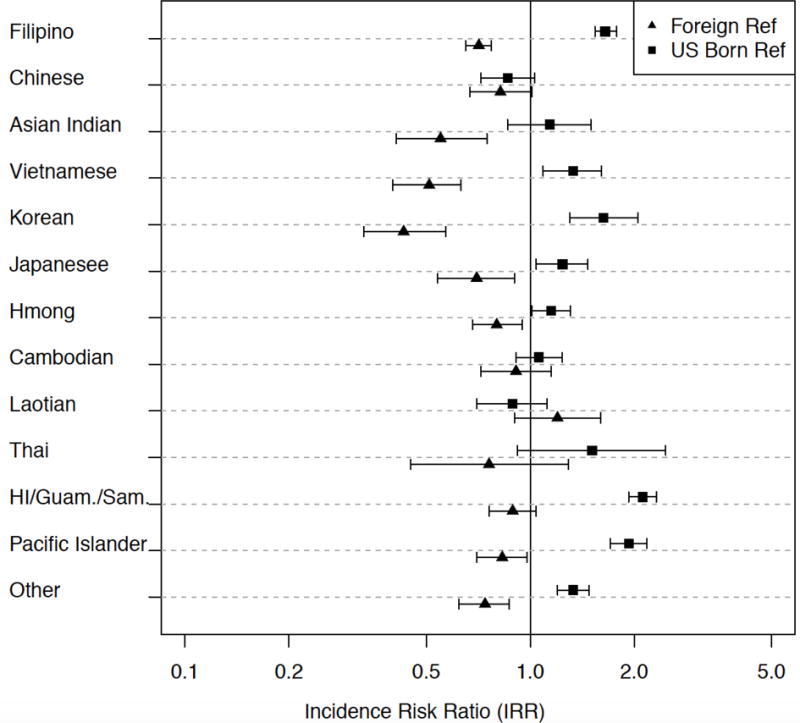
Relative risk of CPS referral for children of U.S. and foreign born mothers by ethnic origin
Notes: Adjusted rates controlled for risks identified in birth record: low birth weight, no prenatal care in 1st trimester, maternal education HS or less, child born to teen mother, no paternity established, public health insurance
Each point (Incidence Risk Ratio) represents relative risk and 95% confidence interval of each group compared to other Asian children of mothers with the same nativity
Results
Birth Record Risks
Overall, 12.2% (N = 138,858) of all children in the 2006–2007 birth cohort were API. Table 1 presents the characteristics of these API children by maternal nativity and ethnic origin. The majority of API children had foreign-born mothers (80.9%). The highest proportion of children was of Filipino descent (22.7%), followed by Chinese (20.0%) and Asian Indian (13.3%). Children of foreign-born mothers were significantly less likely to experience every risk associated with CPS involvement relative to U.S.-born mothers, including low birth weight (7.5% vs. 8.5%, respectively, p < .001); late or absent prenatal care (12.9% vs. 16.5%, p < .001); birth to a mother with no more than a high school degree (22.8% vs. 27.8%, p < .001); birth to a teen mother (1.1% vs. 8.9%, p < .001); no paternity (3.0% vs. 6.0%, p < .001); and public health insurance (23.2% vs. 27.2%, p < .001).
Table 1.
Risks Identified in Birth Record By Maternal Nativity and Ethnic Origin
| Risks
|
|||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Low Birthweight | No Prenatal Care in First Trimester | Maternal Education:HS or less | Child born to Teen Mother | No paternity established | Public health insurance | ||||||||||||||
|
|
|||||||||||||||||||
| χ2 Test | χ2 Test | χ2 Test | χ2 Test | χ2 Test | χ2 Test | ||||||||||||||
| Total N | N | % | P-value | N | % | P-value | N | % | P-value | N | % | P-value | N | % | P-value | N | % | P-value | |
|
| |||||||||||||||||||
| All CA births | 1,133,226 | 77817 | 6.9 | 191269 | 16.9 | 607941 | 55.4 | 107808 | 9.5 | 104878 | 9.3 | 553313 | 49 | ||||||
| All Asian births | 138,856 | ||||||||||||||||||
| U.S. born | 26,425 | 2235 | 8.5 | P<.001 | 4369 | 16.5 | P<.001 | 7232 | 27.8 | P<.001 | 2344 | 8.9 | P<.001 | 1598 | 6.0 | P<.001 | 7150 | 27.2 | P<.001 |
| Foreign born | 112,433 | 8424 | 7.5 | 14555 | 12.9 | 25134 | 22.8 | 1203 | 1.1 | 3409 | 3.0 | 26009 | 23.2 | ||||||
| Filipino | 31,454 | ||||||||||||||||||
| U.S. born | 7,514 | 704 | 9.4 | P=.144 | 1100 | 14.6 | P=.675 | 1691 | 22.8 | P<.001 | 543 | 7.2 | P<.001 | 375 | 5.0 | P=.176 | 1636 | 21.9 | P=.016 |
| Foreign born | 23,940 | 2111 | 8.8 | 3458 | 14.4 | 3866 | 16.4 | 420 | 1.8 | 1104 | 4.6 | 5542 | 23.2 | ||||||
| Chinese | 27,736 | ||||||||||||||||||
| U.S. born | 3,588 | 265 | 7.4 | P=.002 | 218 | 6.1 | P<.001 | 222 | 6.3 | P<.001 | 54 | 1.5 | P<.001 | 75 | 2.1 | P=.338 | 210 | 5.9 | P<.001 |
| Foreign born | 24,148 | 1454 | 6.0 | 2183 | 9.0 | 4307 | 18.2 | 23 | 0.1 | 567 | 2.3 | 4197 | 17.4 | ||||||
| Asian Indian | 18,446 | ||||||||||||||||||
| U.S. born | 1,025 | 131 | 12.8 | P<.001 | 77 | 7.5 | P=.007 | 88 | 8.7 | P<.001 | 25 | 2.4 | P<.001 | 21 | 2.0 | P<.001 | 109 | 10.7 | P=.189 |
| Foreign born | 17,421 | 1603 | 9.2 | 1759 | 10.1 | 2181 | 12.7 | 49 | 0.3 | 115 | 0.7 | 2097 | 12.1 | ||||||
| Vietnamese | 17,717 | ||||||||||||||||||
| U.S. born | 850 | 78 | 9.2 | P=.015 | 202 | 23.8 | P<.001 | 278 | 33.1 | P=.001 | 109 | 12.8 | P<.001 | 98 | 11.5 | P<.001 | 340 | 40.3 | P<.001 |
| Foreign born | 16,867 | 1179 | 7.0 | 2089 | 12.4 | 6402 | 38.7 | 96 | 0.6 | 684 | 4.1 | 4719 | 28.0 | ||||||
| Korean | 11,172 | ||||||||||||||||||
| U.S. born | 977 | 52 | 5.3 | P=.983 | 64 | 6.6 | P=.045 | 89 | 9.2 | P=.529 | 21 | 2.1 | P<.001 | 28 | 2.9 | P<.001 | 119 | 12.2 | P<.001 |
| Foreign born | 10,195 | 541 | 5.3 | 856 | 8.4 | 864 | 8.6 | 17 | 0.2 | 97 | 1.0 | 1830 | 18.0 | ||||||
| Japanese | 5,764 | ||||||||||||||||||
| U.S. born | 2,154 | 170 | 7.9 | P=.734 | 170 | 7.9 | P=.010 | 226 | 10.6 | P=.005 | 32 | 1.5 | P<.001 | 58 | 2.7 | P<.001 | 170 | 7.9 | P<.001 |
| Foreign born | 3,610 | 294 | 8.1 | 358 | 9.9 | 464 | 13.1 | 5 | 0.1 | 39 | 1.1 | 504 | 14.0 | ||||||
| Hmong | 4,352 | ||||||||||||||||||
| U.S. born | 1,560 | 110 | 7.1 | P=.215 | 560 | 35.9 | P=.339 | 925 | 59.9 | P=.003 | 391 | 25.1 | P<.001 | 86 | 5.5 | P<.001 | 1070 | 68.9 | P=.487 |
| Foreign born | 2,792 | 170 | 6.1 | 1043 | 37.4 | 1739 | 64.6 | 306 | 11.0 | 85 | 3.0 | 1885 | 67.8 | ||||||
| Cambodian | 3,648 | ||||||||||||||||||
| U.S. born | 969 | 109 | 11.2 | P=.006 | 329 | 34.0 | P<.001 | 694 | 72.7 | P<.001 | 364 | 37.6 | P<.001 | 173 | 17.9 | P<.001 | 748 | 77.5 | P<.001 |
| Foreign born | 2,679 | 222 | 8.3 | 546 | 20.4 | 1412 | 54.2 | 21 | 0.8 | 224 | 8.4 | 1151 | 43.1 | ||||||
| Laotian | 2,079 | ||||||||||||||||||
| U.S. born | 501 | 50 | 10.0 | P=.754 | 175 | 34.9 | P<.001 | 353 | 71.6 | P<.001 | 165 | 32.9 | P<.001 | 76 | 15.2 | P<.001 | 371 | 74.5 | P<.001 |
| Foreign born | 1,578 | 150 | 9.5 | 366 | 23.2 | 753 | 48.9 | 52 | 3.3 | 90 | 5.7 | 618 | 39.3 | ||||||
| Thai | 1,608 | ||||||||||||||||||
| U.S. born | 171 | 9 | 5.3 | P=.478 | 23 | 13.5 | P=.216 | 39 | 23.1 | P=.007 | 13 | 7.6 | P<.001 | 11 | 6.4 | P=.227 | 44 | 25.9 | P=.003 |
| Foreign born | 1,437 | 96 | 6.7 | 247 | 17.2 | 470 | 33.4 | 38 | 2.6 | 63 | 4.4 | 535 | 37.3 | ||||||
| HI/Guam./Sam. | 2,938 | ||||||||||||||||||
| U.S. born | 2,012 | 150 | 7.5 | P=.242 | 582 | 28.9 | P=.003 | 1118 | 56.8 | P=.023 | 215 | 10.7 | P<.001 | 277 | 13.8 | P=.663 | 914 | 45.7 | P=.001 |
| Foreign born | 926 | 58 | 6.3 | 319 | 34.4 | 548 | 61.3 | 48 | 5.2 | 122 | 13.2 | 485 | 52.5 | ||||||
| Pacific Islander | 3,032 | ||||||||||||||||||
| U.S. born | 1,265 | 84 | 6.6 | P=.183 | 357 | 28.2 | P=.059 | 676 | 55.2 | P=.008 | 155 | 12.3 | P<.001 | 131 | 10.4 | P<.001 | 560 | 44.6 | P=.785 |
| Foreign born | 1,767 | 140 | 7.9 | 555 | 31.4 | 851 | 50.3 | 62 | 3.5 | 107 | 6.1 | 794 | 45.1 | ||||||
However, considerable variability in risk among children of foreign-born mothers was evident by ethnic origin. For example, no significant differences in low birth weight existed between children of U.S.-born and foreign-born mothers in several ethnic groups. Some foreign-born mothers (relative to their U.S.-born counterparts), such as Korean (8.4 vs. 6.6, respectively, p = .045) and Japanese (9.90 vs. 7.90, p = .010) mothers, were more likely to have late or absent prenatal care. Children of some foreign-born mothers (e.g., Chinese: 17.4 vs. 5.9, p < .001; Hawaiian, Guamanian, or Samoan: 52.5 vs. 45.7, p = .001) were also more likely to have public (not private) health insurance than those of U.S.-born mothers of the same ethnicities. In short,, little to no prenatal care, high school education or lower, and use of or eligibility for public health insurance (compared to private insurance) were more prevalent among some Southeast Asian (Hmong, Cambodian, Laotian); Pacific Islander; and Hawaiian, Guamanian, or Samoan groups than other Asian ethnic groups, regardless of immigrant status. Teen motherhood was especially high among U.S.-born Hmong (25.1%), Cambodian (37.6%), and Laotian (32.9%) populations.
Figure 1 presents the cumulative number of birth record risks present across each ethnic group, stratified by foreign-born status. The number associated with each bar in Figure 1 represents the proportion of children in each sub-ethnic group category with no risks identified. Among children of foreign-born mothers, significant advantages were observed in number of risks at birth relative to U.S.-born mothers (10.6% vs. 15.3%, respectively, with three or more risks identified, p < .001). Southeast Asian (Hmong, Cambodian, Laotian); Pacific Islander; and Hawaiian, Guamanian, or Samoan groups had a higher number of risks identified at childbirth than other Asian ethnic groups, and this pattern was more pronounced for U.S.-born Hmong (13.8% with three or more risks identified), Cambodian (24.3% with three or more risks identified), and Laotian (18.8% with three or more risks identified) mothers, who had the most risks of all groups. Chinese, Japanese, Korean, and Asian Indian children were most likely to have no risks present at birth compared to all other Asian groups, regardless of maternal nativity.
CPS Reports
The cumulative percentages of children reported to CPS are presented for each group in Table 2. Rates of reporting were lower for foreign-born mothers compared to U.S.-born mothers (4.7% vs 9.5%, respectively). Children of U.S.-born Hawaiians, Guamanians, or Samoans had the highest rate of report, with 20.4% referred to CPS during the first 5 years of life. This was followed by children of U.S.-born Pacific Islanders (18.0%) and U.S.-born Hmong mothers (13.5%). However, higher than average rates of report were also observed for some children of foreign-born mothers, such as Hawaiians, Guamanians, or Samoans (18.6%); Pacific Islanders (13.6%); Hmong (11.2%); and Laotians (10.8%), compared to the average for all children of Asian mothers (5.6%). The lowest rates of report were observed among children of foreign-born Asian Indian (2.5%) Korean (2.7%) and Chinese (2.8%) mothers.
Table 2.
CPS Report by Maternal Nativity and Ethnic Origin (%)
| Foreign born mothers
|
U.S. born mothers
|
|
|---|---|---|
| (N=112,433) | (N=26,425) | |
|
|
|
|
| All Asian births | 4.7 | 9.5 |
| Filipino | 6.0 | 9.2 |
| Chinese | 2.8 | 3.2 |
| Asian Indian | 2.5 | 4.7 |
| Vietnamese | 4.6 | 11.6 |
| Korean | 2.7 | 6.9 |
| Japanese | 3.5 | 5.0 |
| Hmong | 11.2 | 13.5 |
| Cambodian | 9.7 | 16.5 |
| Laotian | 10.8 | 13.0 |
| Thai | 8.5 | 8.8 |
| Hawaiian/Guamanian/Samoan | 18.6 | 20.4 |
| Pacific Islander | 13.6 | 18.0 |
Figure 2 illustrates relative risks (RR) adjusted for risk indicators and corresponding 95% confidence intervals (CI) for subgroups stratified by maternal nativity and ethnic origin. Even after adjusting for risk covariates, children of U.S.-born Hawaiian, Guamanian, or Samoan mothers (RR = 2.12; 95% CI = 1.93, 2.32) and Pacific Islander mothers (RR = 1.93; 95% CI = 1.71, 2.18) had approximately twice the risk of being referred to CPS compared to all other children born to Asian mothers. Despite having high overall rates of report, after adjusting for risk factors present at birth, a lower likelihood of being reported was observed for children of foreign-born Pacific Islander (RR = 0.83; 95% CI = 0.70, 0.98) and Hmong (RR = 0.80; 95% CI = 0.68, 0.95) mothers.
Discussion
API populations in the U.S. are underrepresented among those reported to CPS for abuse or neglect and understudied in child maltreatment research. In this population-based analysis, we leveraged linked birth and CPS records to examine risk of CPS report during the first 5 years of life among API children in California by maternal nativity and ethnic origin, information that is not typically captured in CPS records alone. This study represents a significant contribution to the literature given the relative invisibility of and need for disaggregated data on API groups in research (Srinivasan & Guillermo, 2000). Findings highlight variability in the characteristics that define API children in California. First, this analysis documented that despite lower rates of CPS report compared to other children, API children are not at uniformly lower risk. Specifically, children of foreign-born mothers have fewer cumulative risks and lower rates of CPS involvement than those of U.S.-born API mothers. Variability also exists in different API ethnic groups, with Pacific Islander and Southeast Asian groups presenting with distinctly higher risk of report to CPS than other Asian groups.
Both national and California-based studies have shown children of Asian origin to be at substantially lower risk of report for child maltreatment than children of other ethnicities (Chang et al., 2006; Ima & Hohm, 1991; Maker, Shah, & Agha, 2005; Pelczarski & Kemp, 2006; U.S. Department of Health and Human Services, 2016). Nevertheless, to our knowledge, prior to this study no research had examined whether these patterns hold regardless of parent birthplace or Asian ethnic origin. One recent source of data revealed that rates of family violence in API homes were higher when examining specific Asian subgroups as compared to national, aggregate surveys with multiple ethnic groups (Leong, Juang, Qin, & Fitzgerald, 2011). The data from this study support a similar pattern.
Comparable to findings from California-based studies that have shown Latino children with foreign-born mothers to be less likely to have CPS involvement than those with U.S.-born mothers (Johnson-Motoyama et al., 2015; Putnam-Hornstein & Needell, 2011; Putnam-Hornstein et al., 2013), very different patterns of risk and CPS report emerged for children of foreign-born API mothers compared to U.S.-born API mothers. In aggregate, significant advantages were observed for children of foreign-born mothers relative to U.S.-born mothers in number of risks at birth (10.6% vs. 15.3%, respectively, with three or more risks identified, p < .001) and reported maltreatment (4.7% vs. 9.5%, p < .001). This was not entirely unexpected given literature suggesting that Asian immigrant women may have better health (Frisbie, Cho, & Hummer, 2001; Huh, Prause, & Dooley, 2008) and lower rates of mental health disorders (Lau et al., 2013; Takeuchi et al., 2007) compared to native-born Asian women, which may in turn provide them protection from CPS involvement. It is important to note, however, that in those studies, differences in health and mental health between immigrant and nonimmigrant API women were attributed to other experiences such as perceived discrimination, family and cultural conflict (Lau et al., 2013), and specific ethnic group differences (Frisbie et al., 2001).
Thus, perhaps not surprisingly, advantages in CPS involvement were not observed in every API ethnic group. Children of foreign-born Hmong; Cambodian; Laotian; Hawaiian, Guamanian, or Samoan; and Pacific Islander mothers experienced higher rates of CPS reporting than the average API child of a U.S.-born mother (9.5 per 100 reported). These statistics convey that children with mothers born in Southeast Asia and other islands (Hawaii, Guam, Samoa, Pacific Islands) have rates of CPS involvement on par with children of U.S.-born API mothers, offering more refined context to broadly inaccurate perceptions that children of foreign-born mothers are underrepresented in CPS. Furthermore, in this study some groups of children of U.S.-born mothers more closely resembled children of foreign-born mothers in their patterns of CPS involvement. For example, children of U.S.-born Chinese mothers had a lower rate of report (3.2 per 100) than the average child of a foreign-born Asian mother (4.7 per 100). At the very least, these findings paint a picture of API families’ experiences with CPS that are much more nuanced than generally believed. In other words, some but not all groups of children of API foreign-born mothers appear to be at relatively low risk of CPS reporting, whereas some but not all groups of children of U.S.-born API mothers are at relatively high risk of CPS reporting.
These findings are important for several reasons. First, we conceptualized the accumulation of birth risks to represent a proximal measure of socioeconomic status. Foreign-born, thus foreign-born mothers experienced overall fewer risks than U.S.-born mothers, thus benefiting from better socioeconomic status overall. Because foreign-born mothers also had lower risk of CPS involvement, it seems that CPS involvement may largely be explained by the accumulation of social and financial capital. When examining specific subgroups, Southeast Asian and Pacific Islander mothers had higher rates of reports. Similar to findings from other studies (e.g., Huang, Calzada, Cheng, & Brotman, 2012), Southeast Asian groups also appeared to possess the fewest resources. Specifically, adolescent motherhood and use of or eligibility for public health insurance were particularly high among U.S.-born Southeast Asian mothers. Low education was of greatest concern among Southeast Asian and Pacific Islander (Hawaiian, Guamanian, Samoan, and Pacific Islander) mothers, regardless of their birthplace, which is somewhat consistent with existing studies showing low education to be more prevalent among Pacific Islanders (Rao et al., 2006) and Hmong women (Schempf et al., 2010). With more socioeconomic risk, Southeast Asian and Pacific Islander children logically also had higher rates of involvement with CPS than other groups.
One explanation for heightened risk among Southeast Asian groups is tied to their origins and family histories as refugees fleeing from genocide and civil war to the United States, where many signed up for public benefits upon resettlement and struggled with rapid forced acclimation to dominant society and culture (Hsu, Davies, & Hansen, 2004). High rates of mental health disorders among these refugee groups dealing with the effects of trauma are well documented, and this evidence suggests that trauma experienced by parents and caretakers also affects children who were born in the United States (e.g., Chung & Bemak, 2002; Mollica, Poole, Son, Murray, & Tor, 1997; Nicholson, 1997). It is possible that coping mechanisms for dealing with traumatic histories may also translate into additional risk behaviors that relate to CPS involvement. For example, high rates of adolescent motherhood (and CPS involvement) among Southeast Asians could be tied to this group’s disproportionate representation in the juvenile justice system (Krisberg, 2005). In particular, among Southeast Asian adolescents, associating with delinquent peers has been related to risky sexual behaviors (Le & Kato, 2006), introducing high potential for CPS reporting.
As for Pacific Islander groups, low education combined with relative isolation from mainland culture and resources may result in unique risk of CPS involvement. A recent study showed evidence of lower health literacy among Native Hawaiians and Pacific Islanders compared to other ethnicities (Lassetter et al., 2015). It is possible that the mechanisms leading to low health literacy may also result in a lack of knowledge of appropriate parenting behaviors and how to access care for children. However, limited evidence that Pacific Islanders prefer to tackle health issues at home rather than seek medical assistance (McLaughlin & Braun, 1998) also speaks to potential cultural differences in help-seeking behaviors and mistrust of resources and providers, which may place children at greater risk of CPS involvement.
Notwithstanding such speculations, after adjusting for risks at birth, higher risk of CPS involvement for most Southeast Asian groups disappeared (and in the case of children of foreign-born Hmong mothers, adjusted risk became lower than average). In contrast, after adjusting for birth risks, children of U.S.-born Islanders (Hawaiian, Guamanian, Samoan, and Pacific Islander) were still approximately twice as likely to have CPS involvement than other Asian children. These findings suggest that other unmeasured factors may better explain disparities in rates of involvement among children of Islanders. Whether those factors relate to a lack of access to supports and services, health literacy issues, or perhaps cultural differences or incongruences in childrearing, is beyond the scope of this study but an area that is open for discovery.
Additionally, in adjusted models, children of U.S.-born Filipino, Vietnamese, and Korean mothers were also at higher risk of reports, whereas children of foreign-born Filipino, Vietnamese, and Korean mothers were at lower risk. This finding supports the notion that some aspect of the immigration and acculturation process may increase risk of CPS involvement with more time and generations in the United States (Cardoso et al., 2014; Dettlaff et al., 2009). To what extent the increase reflects actual risk of being maltreated, as opposed to increased exposure to and surveillance by child-serving agencies and providers, remains unknown.
One factor that may further elucidate disparate patterns of CPS involvement among different API groups is understanding the type of maltreatment reported. Existing studies have indicated that physical abuse is higher among API children than the national average and that API children are more likely to die due to physical abuse compared to White children (Dakil, Cox, Lin, & Flores, 2011). Other regional studies have supported these statistics, having determined that API children are more likely to be reported for physical abuse compared to other groups (Chang et al., 2006; Ima & Hohm, 1991; Maker et al., 2005; Pelczarski & Kemp, 2006). These smaller county-based studies have also shown that maltreatment characteristics may differ by API ethnicity (Chang et al., 2006; Rhee & Chang, 2006). For example, in Los Angeles County physical abuse was the most prevalent type of abuse among Chinese, Vietnamese, and Korean children, whereas neglect was the most prevalent for Cambodians (Chang et al., 2008; Chang et al., 2006; Rhee et al., 2008). To clarify whether a cultural linkage to corporal punishment may exist, a practical next step for deepening this line of inquiry may be to stratify CPS experiences of API subgroups by type of maltreatment.
Limitations
Although this study represents one of the largest and most detailed population-based analyses of API involvement with CPS in the U.S. to date, any examination of experiences of different ethnic and cultural groups using administrative data is not without its limitations. First, these findings may not be generalizable to API groups outside of California. We cannot assume that APIs throughout the U.S. have the same experiences related to their support networks, assimilation processes, and overall integration into the communities where they reside. Despite this limitation, however, California provides an ideal location for study given its largest concentration of diverse Asian ethnic groups and having been a primary settlement location for many API communities over the last several decades.
In this study, we used mothers’ self-report of their primary ethnicity or region of origin for our subgroup categorizations. In a study that compared mono-ethnic and multiethnic mothers with the same primary ethnicity, key indicators of interest did not differ significantly between the two groups (Schempf et al., 2010). Therefore, we felt confident in relying on reports of primary ethnicity for our subgroup categorizations and excluded mothers who reported more than one race or ethnicity as their primary ethnicity (identified as multiethnic). There is surely value in studying individuals who do not limit themselves to one ethnicity, but using an indicator of primary ethnicity appeared to be the strongest valid option for our purposes.
Additionally, the structure of these data is such that a mother’s ethnicity may not always align with her country of birth. For example, it is possible that a mother was born in China but identifies as ethnically Japanese. In such a case, this mother would be included in the Japanese category. This is also likely the reason that a sizable foreign-born Hawaiian, Guamanian, or Samoan group exists in this analysis, meaning that many mothers in this group may identify as native Hawaiian, Guamanian, or Samoan but could have been born in a different country. Because an immeasurable number of subgroups could be created using ethnic identity and birthplace combinations, for this study we elected to simplify by creating groups based on maternal self-reported ethnic identity and foreign-born status.
As discussed above, there are limitations to studying the reporting of maltreatment as a single outcome, without accounting for patterns of specific maltreatment types, such as sexual abuse, physical abuse, neglect, and emotional abuse. Within the API population, for example, some older research has suggested that sexual abuse may be underreported by API groups due to norms of non-disclosure (Yap, 1986; Ima & Hohm, 1991). It is possible that norms around the reporting of certain types of maltreatment are specific to some API groups and not others, suggesting that the relatively low rates of maltreatment among API groups are more nuanced than observed in this study.
As with most studies that utilize administrative data sources, this study does not provide reasons for differential risk among different API subgroups. As mentioned above in the discussion, the concentration of risks observed within specific sub-ethnic groups may be related to cultural barriers and access to needed services at an individual level. However, risk may also be associated with unobserved characteristics of the communities in which individuals settle and reside. Future analyses might take in to account the extent to which the geographical distribution of where certain subgroups are concentrated may influence risk.
Finally, a more refined measure of socioeconomic status that included income would have been desirable in our examination of risk. Enrollment in Medi-Cal and other public insurance programs is far from universal among those who meet income thresholds. However, in a previous study of a 2002 cohort of children born in CA, it was found that, among those coded as non Medi-Cal, almost all were covered by private insurance or an HMO (Putnam-Hornstein & Needell, 2011). Further, California allows for retroactive enrollment of Medi-Cal eligible, nonparticipating mothers into the program to cover costs of labor and delivery, reducing concerns of selective enrollment. Our conceptualization of socio-economic status as an accumulation of birth risks, including Medi-Cal coverage, although imperfect, likely serves as a better proxy for socio-economic struggles and poverty.
Conclusion
This study addressed a significant gap in the literature on child maltreatment; attention to the diverse experiences of API children with CPS in the U.S. is long overdue. Findings are valuable because they represent the largest known population-based study of API ethnic groups involved with CPS since the 1990s (Chang et al., 2006; Ima & Hohm, 1991; Maker et al., 2005; Pelczarski & Kemp, 2006). In this study, groups were disaggregated by both maternal ethnic origin and nativity, offering a deeper understanding of risk and CPS involvement in this population. At the very least, findings provide justification for continuing to disaggregate race data in child abuse and neglect research, and for not treating API families with CPS involvement as a homogenous group in practice. Specifically, patterns of risk and CPS involvement are very different for Islander groups compared to other Asian groups. The fact that Native Hawaiian and Pacific Islander children have substantially higher risk of child welfare involvement than the average child in California signifies that their particular cultural and environmental contexts should be considered when designing and selecting intervention strategies and attempting to alleviate associated risks surrounding CPS involvement for these groups. Additional study of other groups, such as Asian Indian and Korean families, for example, may also be warranted to enhance understanding of the factors that protect some Asian groups from experiencing CPS referrals with their young children.
Clearly, the presence of disparities in risk and in CPS involvement among certain API groups has implications for the health and well-being of API youth and adults across the life course. Specifically, it may be helpful to develop trauma-focused maltreatment prevention strategies and target health literacy for specific groups in California, including Islander and Southeast Asian groups impacted by war and genocide in their countries of origin. In order to better understand why these disparities exist and work to prevent further involvement with the foster care system, CPS agencies should be encouraged make more intentional efforts to match API families with caseworkers of the same ethnic and language background, to help with brokering cultural and linguistic challenges in navigating systems that families may be interfacing. Finally, findings offer evidence for including work with API families in cultural competence training of the CPS workforce in California. Further research is necessary to unravel the complex processes underlying observed risk for CPS involvement as well as the mechanisms for reducing risk for specific API subgroups.
Acknowledgments
The authors wish to thank Barbara Needell and Daniel Webster and other colleagues from the California Child Welfare Indicators Project for their editorial and insightful contributions. We also acknowledge support from collaborators at the Children’s Data Network and California Department of Social Services. Funding for this project was provided by First 5 LA and by award number T32AA007240 from the National Institute on Alcohol Abuse and Alcoholism. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
Contributor Information
Megan Finno-Velasquez, New Mexico State University, Lindsey Palmer and John Prindle, University of Southern California.
Christina C. Tam, University of California, Berkeley, Emily Putnam-Hornstein, University of Southern California
References
- Aczon-Armstrong M, Inouye J, Reyes-Salvail F. Depression and chronic illness: Asian/Pacific Islander adults in Hawaii. Issues in Mental Health Nursing. 2013;34:169–179. doi: 10.3109/01612840.2012.738356. [DOI] [PubMed] [Google Scholar]
- Allard MD. Asians in the U.S. labor force: Profile of a diverse population. Monthly Labor Review. 2011;134(11):3–22. [Google Scholar]
- Barnes PM, Adams PF, Powell-Griner E. Health characteristics of the Asian adult population: United States, 2004–2006. Atlanta, GA: U.S. Department of Health and Human Services, Centers for Disease Control and Prevention, National Center for Health Statistics; 2008. [Google Scholar]
- Begle AM, Dumas JE, Hanson RF. Predicting child abuse potential: An empirical investigation of two theoretical frameworks. Journal of Clinical Child & Adolescent Psychology. 2010;39:208–219. doi: 10.1080/15374410903532650. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bitton A, Zaslavsky AM, Ayanian JZ. Health risks, chronic diseases, and access to care among US Pacific Islanders. Journal of General Internal Medicine. 2010;25:435–440. doi: 10.1007/s11606-009-1241-0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Campbell KM, Deck D, Krupski A. Record linkage software in the public domain: A comparison of Link Plus, the Link King, and a ‘basic’ deterministic algorithm. Health Informatics Journal. 2008;141:5–15. doi: 10.1177/1460458208088855. [DOI] [PubMed] [Google Scholar]
- Cardoso JB, Dettlaff AJ, Finno-Velasquez M, Scott J, Faulkner M. Nativity and immigration status among Latino families involved in the child welfare system: Characteristics, risk, and maltreatment. Children and Youth Services Review. 2014;44:189–200. doi: 10.1016/j.childyouth.2014.06.008. [DOI] [Google Scholar]
- Chang J, Rhee S, Berthold SM. Child abuse and neglect in Cambodian refugee families: Characteristics and implications for practice. Child Welfare. 2008;87:141–160. [PubMed] [Google Scholar]
- Chang J, Rhee S, Weaver D. Characteristics of child abuse in immigrant Korean families and correlates of placement decisions. Child Abuse & Neglect. 2006;30:881–891. doi: 10.1016/j.chiabu.2006.03.002. [DOI] [PubMed] [Google Scholar]
- Chen E, Matthews KA, Boyce WT. Socioeconomic differences in children’s health: how and why do these relationships change with age? Psychological bulletin. 2002;128(2):295. doi: 10.1037/0033-2909.128.2.295. [DOI] [PubMed] [Google Scholar]
- Chung RCY, Bemak F. Revisiting the California Southeast Asian mental health needs assessment data: An examination of refugee ethnic and gender differences. Journal of Counseling & Development. 2002;80:111–119. doi: 10.1002/j.1556-6678.2002.tb00173.x. [DOI] [Google Scholar]
- Dakil SR, Cox M, Lin H, Flores G. Racial and ethnic disparities in physical abuse reporting and child protective services interventions in the United States. Journal of the National Medical Association. 2011;103:926–931. doi: 10.1016/S0027-9684(15)30449-1. [DOI] [PubMed] [Google Scholar]
- Dettlaff AJ, Earner I, Phillips SD. Latino children of immigrants in the child welfare system: Prevalence, characteristics, and risk. Children and Youth Services Review. 2009;31:775–783. doi: 10.1016/j.childyouth.2009.02.004. [DOI] [Google Scholar]
- Drake B, Jolley JM, Lanier P, Fluke J, Barth RP, Jonson-Reid M. Racial bias in child protection? A comparison of competing explanations using national data. Pediatrics. 2011;127(3):471–478. doi: 10.1542/peds.2010-1710. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Fong R, Mokuau N. Not simply “Asian Americans”: Periodical literature review on Asians and Pacific Islanders. Social Work. 1994;39:298–305. doi: 10.1093/sw/39.3.298. [DOI] [Google Scholar]
- Frisbie WP, Cho Y, Hummer RA. Immigration and the health of Asian and Pacific Islander adults in the United States. American Journal of Epidemiology. 2001;153:372–380. doi: 10.1093/aje/153.4.372. [DOI] [PubMed] [Google Scholar]
- Gomez SL, Kelsey JL, Glaser SL, Lee MM, Sidney S. Immigration and acculturation in relation to health and health-related risk factors among specific Asian subgroups in a health maintenance organization. American Journal of Public Health. 2004;94:1977–1984. doi: 10.2105/AJPH.94.11.1977. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Grieco EM, Acosta YD, de la Cruz GP, Gambino C, Gryn T, Larsen LJ, Walters NP. The foreign-born population in the United States: 2010. 2010 Retrieved from https://www.census.gov/prod/2012pubs/acs-19.pdf.
- Hoeffel EM, Rastogi S, Kim MO, Shahid H. The Asian population: 2010. 2012 Retrieved from https://www.census.gov/prod/cen2010/briefs/c2010br-11.pdf.
- Holland AT, Palaniappan LP. Problems with the collection and interpretation of Asian-American health data: Omission, aggregation, and extrapolation. Annals of Epidemiology. 2012;22:397–405. doi: 10.1016/j.annepidem.2012.04.001. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Huang KY, Calzada E, Cheng S, Brotman LM. Physical and mental health disparities among young children of Asian immigrants. Journal of Pediatrics. 2012;160:331–336.e1. doi: 10.1016/j.jpeds.2011.08.005. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hsu E, Davies CA, Hansen DJ. Understanding mental health needs of Southeast Asian refugees: Historical, cultural, and contextual challenges. Clinical psychology review. 2004;24(2):193–213. doi: 10.1016/j.cpr.2003.10.003. [DOI] [PubMed] [Google Scholar]
- Huh J, Prause JA, Dooley CD. The impact of nativity on chronic diseases, self-rated health and comorbidity status of Asian and Hispanic immigrants. Journal of Immigrant and Minority Health. 2008;10:103–118. doi: 10.1007/s10903-007-9065-7. [DOI] [PubMed] [Google Scholar]
- Ima K, Hohm CF. Child maltreatment among Asian and Pacific Islander refugees and immigrants: The San Diego case. Journal of Interpersonal Violence. 1991;6:267–285. doi: 10.1177/088626091006003001. [DOI] [Google Scholar]
- Islam NS, Khan S, Kwon S, Jang D, Ro M, Trinh-Shevrin C. Methodological issues in the collection, analysis, and reporting of granular data in Asian American populations: Historical challenges and potential solutions. Journal of Health Care for the Poor and Underserved. 2010;21:1354–1381. doi: 10.1353/hpu.2010.0939. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Jaurez DT, Samoa RA, Chung RS, Seto TB. Disparities in health, obesity and access to care among an insured population of Asian and Pacific Islander Americans in Hawai‘i. Hawai‘i Medical Journal. 2010;69:42–46. [PMC free article] [PubMed] [Google Scholar]
- Johnson-Motoyama M, Putnam-Hornstein E, Dettlaff AJ, Zhao K, Finno-Velasquez M, Needell B. Disparities in reported and substantiated infant maltreatment by maternal Hispanic origin and nativity: A birth cohort study. Maternal and Child Health Journal. 2015;19:958–968. doi: 10.1007/s10995-014-1594-9. [DOI] [PubMed] [Google Scholar]
- Krisberg B. Juvenile justice: Redeeming our children. Thousand Oaks, CA: Sage; 2005. [Google Scholar]
- Lanier P, Maguire-Jack K, Walsh T, Drake B, Hubel G. Race and ethnic differences in early childhood maltreatment in the United States. Journal of Developmental & Behavioral Pediatrics. 2014;35(7):419–426. doi: 10.1097/DBP.0000000000000083. [DOI] [PubMed] [Google Scholar]
- Lassetter JH, Clark L, Morgan SE, Brown LB, VanServellen G, Duncan K, Hopkins ES. Health literacy and obesity among native Hawaiian and Pacific Islanders in the United States. Public Health Nursing. 2015;32:15–23. doi: 10.1111/phn.12155. [DOI] [PubMed] [Google Scholar]
- Lau AS, Tsai W, Shih J, Liu LL, Hwang WC, Takeuchi DT. The immigrant paradox among Asian American women: Are disparities in the burden of depression and anxiety paradoxical or explicable? Journal of Consulting and Clinical Psychology. 2013;81:901–911. doi: 10.1037/a0032105. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Le TN, Kato T. The role of peer, parent, and culture in risky sexual behavior for Cambodian and Lao/Mien adolescents. Journal of Adolescent Health. 2006;38:288–296. doi: 10.1016/j.jadohealth.2004.12.005. [DOI] [PubMed] [Google Scholar]
- Leong FTL, Juang L, Qin DB, Fitzgerald HE, editors. Asian American and Pacific Islander children and mental health. Santa Barbara, CA: Praeger; 2011. (Vol. 1 and Vol. 2) [Google Scholar]
- Maker AH, Shah PV, Agha Z. Child physical abuse: Prevalence, characteristics, predictors, and beliefs about parent-child violence in South Asian, Middle Eastern, East Asian, and Latina women in the United States. Journal of Interpersonal Violence. 2005;20:1406–1428. doi: 10.1177/0886260505278713. [DOI] [PubMed] [Google Scholar]
- McLaughlin LA, Braun KL. Asian and Pacific Islander cultural values: Considerations for health care decision making. Health & Social Work. 1998;23:116–126. doi: 10.1093/hsw/23.2.116. [DOI] [PubMed] [Google Scholar]
- Mollica RF, Poole C, Son L, Murray CC, Tor S. Effects of war trauma on Cambodian refugee adolescents’ functional health and mental health status. Journal of the American Academy of Child & Adolescent Psychiatry. 1997;36:1098–1106. doi: 10.1097/00004583-199708000-00017. [DOI] [PubMed] [Google Scholar]
- Nicholson BL. The influence of pre-emigration and postemigration stressors on mental health: A study of Southeast Asian refugees. Social Work Research. 1997;21:19–31. doi: 10.1093/swr/21.1.19. [DOI] [Google Scholar]
- Ortman JM, Guarneri CE. United States population projections: 2000 to 2050. Washington, DC: U.S. Census Bureau; 2009. [Google Scholar]
- Pelczarski Y, Kemp SP. Patterns of child maltreatment referrals among Asian and Pacific Islander families. Child Welfare. 2006;85:5–31. [PubMed] [Google Scholar]
- Putnam-Hornstein E, Mitchell MN, Hammond I. Cumulative risk of child protective service involvement before age 5: A population-based examination. 2014 Retrieved from http://www.datanetwork.org/research/1002.
- Putnam-Hornstein E, Needell B, King B, Johnson-Motoyama M. Racial and ethnic disparities: A population-based examination of risk factors for involvement with child protective services. Child Abuse & Neglect. 2013;37(1):33–46. doi: 10.1016/j.chiabu.2012.08.005. [DOI] [PubMed] [Google Scholar]
- Putnam-Hornstein E, Needell B. Predictors of child protective service contact between birth and age five: An examination of California’s 2002 birth cohort. Children and Youth Services Review. 2011;33:1337–1344. doi: 10.1016/j.childyouth.2011.04.006. [DOI] [Google Scholar]
- Putnam-Hornstein E, Needell B, King B, Johnson-Motoyama M. Racial and ethnic disparities: A population-based examination of risk factors for involvement with child protective services. Child Abuse & Neglect. 2013;37:33–46. doi: 10.1016/j.chiabu.2012.08.005. [DOI] [PubMed] [Google Scholar]
- Rao AK, Daniels K, El-Sayed YY, Moshesh MK, Caughey AB. Perinatal outcomes among Asian American and Pacific Islander women. American Journal of Obstetrics and Gynecology. 2006;195:834–838. doi: 10.1016/j.ajog.2006.06.079. [DOI] [PubMed] [Google Scholar]
- Registry Plus. Link Plus user’s guide (Version 2.0) Atlanta, GA: Centers for Disease Control and Prevention; 2007. [Google Scholar]
- Rhee S, Chang J. Child abuse: Characteristics and patterns among Cambodian, Chinese, Korean, and Vietnamese American families. 2006 Retrieved from https://web.csulb.edu/projects/ccwrl/Rhee_module.pdf.
- Rhee S, Chang J, Berthold SM, Mar G. Child maltreatment among immigrant Vietnamese families: Characteristics and implications for practice. Child and Adolescent Social Work Journal. 2012;29:85–101. doi: 10.1007/s10560-011-0253-x. [DOI] [Google Scholar]
- Rhee S, Chang J, Weaver D, Wong D. Child maltreatment among immigrant Chinese families: Characteristics and patterns of placement. Child Maltreatment. 2008;13:269–279. doi: 10.1177/1077559507313461. [DOI] [PubMed] [Google Scholar]
- Schempf AH, Mendola P, Hamilton BE, Hayes DK, Makuc DM. Perinatal outcomes for Asian, Native Hawaiian, and other Pacific Islander mothers of single and multiple race/ethnicity: California and Hawaii, 2003–2005. American Journal of Public Health. 2010;100:877–887. doi: 10.2105/AJPH.2009.177345. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Shaw TV, Putnam-Hornstein E, Magruder J, Needell B. Measuring racial disparity in child welfare. Child welfare. 2008;87(2):23. [PubMed] [Google Scholar]
- Srinivasan S, Guillermo T. Toward improved health: Disaggregating Asian American and Native Hawaiian/Pacific Islander data. American Journal of Public Health. 2000;90:1731–1734. doi: 10.2105/AJPH.90.11.1731. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Takeuchi DT, Zane N, Hong S, Chae DH, Gong F, Gee GC, Alegría M. Immigration-related factors and mental disorders among Asian Americans. American Journal of Public Health. 2007;97:84–90. doi: 10.2105/AJPH.2006.088401. [DOI] [PMC free article] [PubMed] [Google Scholar]
- U.S. Census Bureau. Annual Estimates of the resident population by sex, race alone or in combination, and Hispanic origin for the United States, States, and Counties: April 1, 2010 to July 1, 2014 population estimates. 2012 Retrieved May 24, 2016, from https://www.whitehouse.gov/administration/eop/aapi/data/facts-and-figures.
- U.S. Department of Health and Human Services. Child maltreatment 2014. 2016 Retrieved from https://www.acf.hhs.gov/cb/resource/child-maltreatment-2014.
- Wong LF, Caughey AB, Nakagawa S, Kaimal AJ, Tran SH, Cheng YW. Perinatal outcomes among different Asian-American subgroups. American Journal of Obstetrics and Gynecology. 2008;199:382.e1–382.e6. doi: 10.1016/j.ajog.2008.06.073. [DOI] [PubMed] [Google Scholar]
- Yap JG. Philippine ethnoculture and human sexuality. Journal of Social Work & Human Sexuality. 1986;4(3):121–134. [Google Scholar]
- Ye J, Rust G, Baltrus P, Daniels E. Cardiovascular risk factors among Asian Americans: Results from a national health survey. Annals of Epidemiology. 2009;19:718–723. doi: 10.1016/j.annepidem.2009.03.022. [DOI] [PMC free article] [PubMed] [Google Scholar]