

Abstract
Hearing loss (HL) is a common sensory impairment in humans, with significant economic and social impacts. With nearly 20% of the world’s population, China has focused on economic development and health awareness to improve the care for its hearing-impaired population. Recently the Chinese government has initiated national programs such as the China Disabled Persons Federation (CDPF) to fund prevention, treatment, and rehabilitation of hearing impairment. Newborn hearing screening and auditory rehabilitation programs in China have expanded exponentially with government support. While facing many challenges and overcoming obstacles, cochlear implantation (CI) programs in China have also experienced considerable growth. This review discusses the implementation of CI programs for hearing loss in China and presents current HL data including epidemiology, newborn hearing screening, and determination of genetic etiologies. Sharing the experience in Chinese auditory rehabilitation and CI programs will shine a light on the developmental pathway of healthcare infrastructure to meet emerging needs of the hearing-impaired population in other developing countries.
Keywords: Cochlear implants, hearing loss, newborn hearing screening, genetic test, China
1. Introduction
Hearing loss is a significant global health issue due to its growing prevalence and negative impact on quality of life. Appropriate management of hearing disorders is essential to alleviating medical and social burdens on patients, their family, and society. With China accounting for approximately 20% of the world’s population, the socioeconomic impact of hearing loss is further magnified in this population. Cochlear implants are sophisticated medical devices used to provide auditory stimulation in patients with a bilateral severe to profound sensorineural hearing loss (SNHL). As the most effective treatment for patients with bilateral severe to profound SNHL (Eshraghi et al., 2012a), the clinical indications for CI have expanded to include patients with some residual hearing and those with single-sided deafness. As such, CI provide a great opportunity to appreciably reduce the impact of hearing loss both on the patient and society. Positive changes to the socioeconomic environment in response to China’s auditory rehabilitation programs provide a potential model for other developing countries. Recent economic development and increasing health consciousness have driven the Chinese government to direct efforts towards the prevention, treatment, and rehabilitation of hearing impairment. As a result, underprivileged hearing impaired children in China now have access to CI programs and appropriate clinical management.
2. Current situation of hearing loss in China
2.1 Overview
According to World Health Organization (WHO), four out of five patients suffering from hearing loss come from developing countries (World Health Organization, 2014). The growing population with hearing impairment is a serious social and economic problem in China (Table 1&2) (China Disabled Persons’ Federation, 2006). Data from the Second National Sample Survey on Disability by the Chinese government in 2006 reported that more than 27.8 million people present with hearing loss in China (CDPF, 2006). Among these individuals more than half of a million are under the age of eighteen, 6.77 million are adults (i.e. 18–60 years old) and 20.45 million are >60 years of age. In addition, between 20,000 and 30,000 infants in China are born with deafness each year. Since the CDPF report in 2006, the Chinese government has worked to expand and standardize their hearing rehabilitation services. By 2014, the CDPF reported that 32,000 deaf children and 39,000 parents of deaf children participated in auditory rehabilitation programs. Now hearing loss programs in China are supported by 5,772 trained professionals, 31 provincial-level institutions specializing in hearing rehabilitation, and 1,025 smaller hearing service providers. The government provided hearing aids to 19,600 children and 38,352 adults in efforts to lessen the social and economic burden of a deaf individual (CDPF, 2014). The CDPF report in 2014 is also the first to describe in detail the nation-wide infrastructure that provides hearing services and specific aims to expand the current hearing rehabilitation programs in China.
Table 1.
Age distribution of hearing impaired individuals in China. Data Source (China Disabled Persons’ Federation 2006)
| Age Group (years) | Population (million) | Percentage (%) |
|---|---|---|
| 0–6 | 0.14 | 0.50 |
| 7–14 | 0.29 | 1.04 |
| 15–17 | 0.15 | 0.55 |
| 18–59 | 6.77 | 24.33 |
| 60 + | 20.45 | 73.58 |
| Total | 27.80 | 100 |
Table 2.
Severity of hearing disability in different age groups. Data Source (China Disabled Persons’ Federation 2006)
| Age Group (years) | Profound (%) |
Severe (%) |
Moderate (%) |
Mild (%) |
|---|---|---|---|---|
| 0–3 | 66.95 | 16.95 | 14.41 | 1.69 |
| 4–6 | 56.25 | 11.11 | 19.44 | 13.19 |
| 7–14 | 44.78 | 12.59 | 20.5 | 22.12 |
| 15–59 | 29.57 | 11.65 | 30.16 | 28.62 |
| 60- | 10.11 | 10.75 | 45.54 | 33.59 |
2.2 Newborn hearing screening in China
According to published data, the incidence of infant hearing loss is estimated at 1 to 4 per 1000 new born infants in the world (Northern & Hayes, 1994; Center for Disease Control and Prevention, 2009) and 20,000 to 30,000 deaf neonates every year in China (CDPF, 2006). In 1999, the CDPF endorsed early detection and early intervention for childhood deafness. Together with the Ministry of Health and the Ministry of Education of China, protocols recommending newborn hearing screening to be included as part of the routine medical examination for neonates were developed. By 2007, the Chinese government released “Prevention and Rehabilitation of Hearing Impairment in China Project” which established programs for effective hearing screening, diagnosis of hearing loss, hearing aid fitting, and auditory rehabilitation. At the turn of the 21st century, more than 20 out of 34 provincial governments have initiated and implemented newborn hearing screening projects.
At present one million newborns (annual birth rate of 16 million) have received hearing screenings annually at secondary and tertiary medical institutions (general hospitals, specialty hospitals, and maternal and child health hospitals) in China. Otoacoustic Emissions (OAE) are generally used for this preliminary hearing screening, followed by an Auditory Brainstem Response (ABR) test for rescreening. Despite the significant advancements in detection and prevention of hearing loss, only 2 to 5% of all newborn infants and 20% of NICU patients undergo screening for hearing loss in China (Han et al., 2012). The published incidence of infants with hearing loss is lower in China compared to some other countries (Kliegman et al., 2011; Nelson et al., 2008). The true prevalence of newborn hearing impairment in China may be underestimated due to the present low level of newborn hearing screening. In an effort to continue to improve early detection and intervention for newborn hearing loss, the Chinese government continues to promote newborn hearing screening and to widen the screening coverage area (CDPF 2014).
2.3 Genetic hearing loss in China
Genetic mutations related to hearing loss in the Chinese population have been studied for many years. The largest study collected DNA samples from 3564 deaf Chinese patients and showed that 21% are due to GJB2 mutations, 3.8% to mitochondrial A1555G mutations, and 0.6% involve C1494T mutations (Dai et al., 2007). In the nonsyndromic deaf Chinese population, the overall detection rate of a known gene mutation is from 13.6% to 48.7%. The detection of GJB2 mutation in this population ranges from 21% to 37% (Zhang et al., 2016). The most common mutation observed in the GJB2 gene in China is 235delC variation (Zheng et al., 2000; Wang et al., 2001). In a study that screened 37,573 healthy newborns in Beijing, 2.6% of these newborns carried one of four types of a GJB2 mutation, and more than half of those GJB2 mutations were the 235delC variation (Han et al., 2016). The A1555G mutation in mitochondrial 12S rRNA is the most common cause of genetic deafness that results from exposure to ototoxic drugs in China. This maternally transmitted mutation results in structural changes of mitochondrial rRNA with increased affinity for aminoglycosides (Yuan et al., 2008). Genetic analysis of patients with large vestibular aqueducts in China showed that at least one SLC26A4 (pendrin) gene mutation is found in 95% ~ 97% of these patients confirming that the large vestibular aqueduct syndrome is a genetic disease with specific mutations in China (Dai et al., 2006). In contrast, a multi-institutional study of large vestibular aqueduct patients in the Unites States and England showed that only 27% of these patients had a SLC26A4 gene mutation (Madden et al., 2007). The knowledge of genetic hearing loss continues to expand as hearing evaluation and genetic screening becomes more common practice in China. The investigation and analysis of common genetic mutations serves as an integral part to building a comprehensive algorithm for evaluation of hearing loss tailored to the ethnicity of the population being studied.
3. Cochlear implants in China
3.1 Overview
In 2014, nearly 400,000 people globally had received cochlear implants, including 200,000 pediatric patients and 60,000 bilateral users (Zeng et al., 2015). However, the number of CI patients pales in comparison to the much larger population of deaf patients with no access to CI. Cost is one of the main hurtles that limit access to CI, especially in developing countries.
There are three Food and Drug Administration (FDA) approved devices in the United States: Cochlear Ltd. in Australia, Med-El in Austria, and Advanced Bionics by SONOVA Group in Switzerland. These three manufacturers control most of the CI market in the world. Despite variations in components, design and sound-processing strategies, hearing outcome is generally comparable among the three major implant manufacturers (Zeng, 2004). Oticon Medical (William Demant Group in Denmark) also manufactures cochlear implants which are available in Europe and North Africa (Eshraghi et al., 2012b).
3.2 Development of cochlear implant technology in China
For more than 30 years several independent research groups in China have been developing domestic CI products. Until recently domestic Chinese CI devices have seen little market penetration and have not been widely used in clinical application until the recent launch of Nurotron (i.e. a 26-electrode cochlear implant) in 2011. This new multi-channel implant achieved satisfactory results in clinical trials at five respected tertiary care hospitals in China (Zeng et al., 2015b). The Nurotron cochlear implant system received China Food and Drug Administration (CFDA) approval in 2011 and European Union (CE) certification in 2012 (Li et al., 2014).
There have been more than 2,900 Nurotron cochlear implant recipients in China, Mexico, Venezuela, and India. Li and colleagues (Li et al, 2014) found no statistically significant difference in speech perception scores in recipients of Nurotron implanted patients compared to speech perception scores in recipients of Cochlear Nucleus implants (see Figure 1). In addition, Yu, et al. studied long-term outcomes in 60 prelingual children (Yu et al., 2015). These children achieved average scores of consonants, vowels, monosyllabic words and disyllabic words which were 94.52±7.98%, 86.04±13.66%, 95.83±12.42%, 94.05±15.67%, respectively (Figure 2). These results achieved with Nurotron cochlear implants were comparable to results achieved with cochlear implants from the other implant manufacturers.
Figure 1.
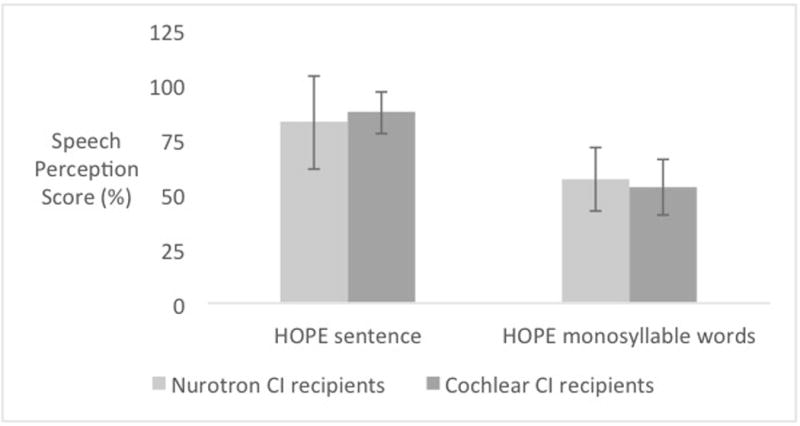
The speech perception score of Nurotron Venus CI adult users and Cochlear CI 24 adult users. No statistically significant (P>0.05) difference could be found between two groups. The Mandarin speech test material, HOPE, was developed by the Auditory Implantation Center of the Department of Otolaryngology & Head and Neck Surgery of PLA General Hospital. Each list of HOPE monosyllable words contains 25 monosyllable words and each list of HOPE sentence tests contains 10 sentences and 50 key words.
Figure 2.
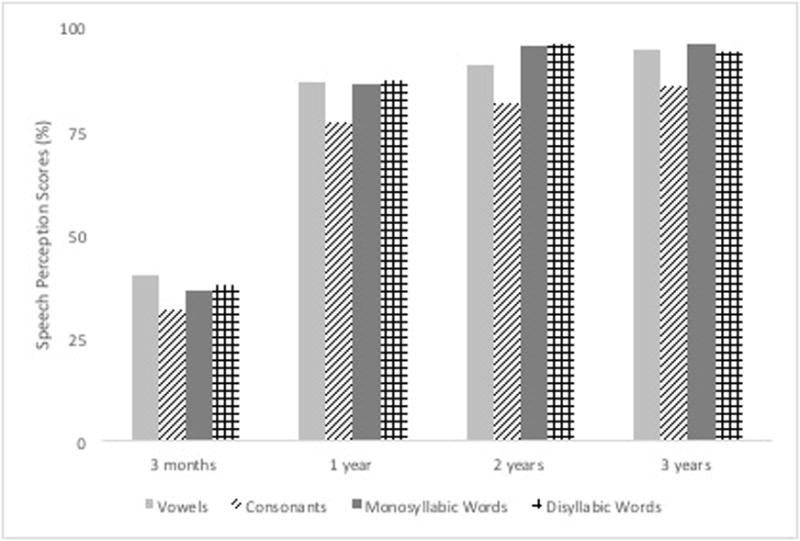
The trends of hearing results at follow up among Nurotron Venus CI pediatric users.
Since its introduction in 2011, utilization of the Nurotron cochlear implant in Chinese tertiary care centers has rapidly increased. Currently, Nurotron devices account for 10% of almost two thousand cochlear implant recipients in the Chinese PLA General Hospital (Chen et al., 2016). High cost has been the main prohibitive factor limiting access to cochlear implants in China. The list prices for any non-domestic cochlear implant devices (e.g. Cochlear, MED EL, or Advanced Bionics) in China ranges from $25,000–46,000 US dollars. The cost of a domestic Nurotron device is approximately one third to half the cost of the non-domestic devices. Senior otologists and scientists from multiple leading institutions in China are involved in the development and evaluation of the Nurotron cochlear implant (Zeng et al., 2015b), resulting in an increased level of enthusiasm and heightened awareness in the general public for this domestic product. This experience has demonstrated the need for availability of lower-cost devices and involvement of local physicians and scientific leaders in promoting cochlear implant utilization in developing countries.
3.3 Pediatric cochlear implants in China
More than 500,000 Chinese children under the age of 18 years old are living with hearing impairment and more than 100,000 children under the age six meet the criteria for CI in China (CDPF, 2006). The multichannel cochlear implant was introduced into China and received approval for treatment of bilateral severe to profound SNHL in adults in 1994, and for treatment of pediatric deafness in 1996 (CDPF, 2011). There are currently more than 30,000 cochlear implant recipients in China, 85% of whom are children (Han & Wang, 2013).
The assistance program for deaf children established by the Chinese government is responsible for a large number of pediatric CI successes. The Chinese central government invested almost 380 million US dollars for diagnosis and treatment of hearing impaired children from 2009 to 2014 (66.4 million USD from 2009 to 2011 and 313.4 million USD from 2011 to 2014). The government provided free cochlear implants to 11,200 deaf children (CDPF, 2014). Pediatric CI has also been included in basic medical insurance provided by select provincial and municipal government in China in the last two years. In addition, supports for underprivileged children in need of cochlear implants continue to pour in from private donations, charity, and local government assistance projects.
3.4 Adult cochlear implants in China
Although the adult hearing-impaired population is much larger than the pediatric population, adults only account for about 15% of all cochlear implant recipients in China. In recent years, CI has gained in popularity with the Chinese public and has provided an improvement in the overall quality and expectancy of life. The number of adult recipients surged in China as the general public and medical community recognized the speech understanding and social benefits provided by CI (Yang et al., 2010b).
Chinese studies () have shown that CI has significantly improved the hearing and speech of adults as measured by the scores of Categories of Auditory Performance (CAP) and Speech Intelligibility Rating (SIR). The CAP measures speech perception performance and reflects auditory receptive abilities in everyday situations. The CAP comprises a hierarchical scale of auditory perceptive ability ranging from 0, “displays no awareness of environmental sounds,” to 7, “can use the telephone with a familiar talker.” The SIR is a rating scale of speech intelligibility by quantifying everyday spontaneous speech. It consists of 5 performance categories ranging from “pre-recognizable words in spoken language” to “connected speech is intelligible to all listeners” (Zhou et al., 2012). In implanted patients, 87.5% communicated freely with strangers at between 3–12 months postoperatively and 25% of the implant recipients could make a phone call with an acquaintance (Li et al., 2010). Yu, et al., showed that hearing loss affects Chinese speech rhythm, resulting in reduced duration of syllables and increased number of breaks in speech. Cochlear implant recipients, however, appear to improve the quality of prosody in Chinese speech (Yu et al., 2003).
Many variables can affect and limit the benefit of cochlear implants in adults. Although heavily debated in studies of English speakers, studies of Chinese implant recipients have shown that the duration of deafness and preoperative speech perception scores are predictive of post-implantation outcomes across the adult population (Yevgeniy et al., 2012; Li et al., 2010). In elderly patients with cochlear implants it has been suggested that age-related degeneration of the spiral ganglion and progressive central auditory dysfunction are barriers to effective implant use (Leung et al., 2005). However, evidence supports that cochlear implants are safe and effective in the elderly patient (Eshraghi et al., 2009). Conversely, studies of adult Chinese cochlear implant recipients suggest that the age at implantation is not predictive of post-implantation outcomes, and equally matched gains in speech understanding have been reported for both elderly and younger groups of implant recipients (Li et al., 2011; Yang et al., 2010a; Leung et al., 2005; Roditi et al., 2009). These conflicting findings demonstrate the controversy that persists surrounding speech perception outcomes in elderly cochlear implant users and the need for further investigation in the Chinese population.
3.5 New trends in China: bilateral cochlear implants and earlier cochlear implantation
Despite improved hearing, unilateral cochlear implant recipients continue to suffer from some of the sequelae of unilateral hearing, including the lack of sound localization and poor word recognition in a noisy environment (Dunn et al., 2008). More and more neurotology specialists in China and around the world have realized that bilateral CI can circumvent these issues and return some binaural advantages. Bilateral CI has been shown to be cost-effective when compared to no intervention, although most of the gains are made by the first implant (Chen et al., 2014). The cost-untility of bilateral CI when compared to unilateral CI varies depending on the analysis performed (Kuthubutheen et al., 2015). Currently, bilateral CI is widely accepted as a safe and effective means of bilateral auditory stimulation in China. Access to CI is limited to unilateral implantation in China forcing patients to pay for cochlear implant devices and medical expenses out of pocket if they decide to pursue a second cochlear implant.
There is increasing evidence to support the benefits of early implantation in children, resulting in re-defining the age limit for pediatric CI. Many studies suggest that implantation at a younger age can maximize the potential for auditory and speech performance (Zwolan et al., 2004; Manrique et al., 2004; Noble et al., 2009; Dettman, et al., 2016). As such, China has experienced a transition to earlier implantation with select tertiary hospitals implanting patients younger than one year of age. At the Chinese PLA General Hospital, 3% (54 cases) of cochlear implants were implanted in patients younger than one year-old in the past five years.
3.6 Chinese tone perception with cochlear implant
Mandarin Chinese has four tones, which are distinctive pitch patterns carried by a syllable of a word. Tones are critical and essential features of word meaning in Chinese as changing pitch patterns result in different words. Lexical tone perception in Chinese language is an additional dimension in speech perception that is uniquely challenging for hearing rehabilitation and CI programs in China. Patients with severe SNHL find it difficult to distinguish one tone from another because a tone is complex in both spectral and temporal domains (Xu & Zhou, 2011; Kong et al., 2006). Reduced ability to recognize spectral fine structure such as fundamental frequency (F0) and harmonics significantly impairs tonal recognition in patients with severe sensorineural hearing loss (Wang et al., 2011a). Lexical tones transmitted by CIs are difficult to recognize because CI coding may not provide enough spectral resolution and lack the temporal fine structure information. As such, CI users may rely on secondary cues such as duration and temporal envelope to recognize Chinese tones (Fu et al., 1998; Luo and Fu, 2004). At least eight frequency channels are required for a CI to transmit one tonal pattern, and more than thirty spectral channels are required to effectively convey numerous combinations involving all four tonal patterns with different consonants and vowels (Kuo et al., 2014; Xu & Zhou 2011). A few recent studies have evaluated methods to improve tonal discrimination in CI recipients (Xu et al., 2002) such as aiding the contralateral ear, changing electrode location, and improving sound processing technology. Better tonal recognition was observed with bimodal hearing in CI users with contralateral hearing aid when compared to CI only users (Luo et al., 2014; Chang et al., 2016). Electrode location did not appear to influence tonal discrimination (Lee et al., 2012). Newer sound processing technology such as Advanced Bionics HiResolution 120 has been examined in the context of tone perception (Han et al., 2009). In addition, lexical tone perception is correlated with music pitch perception. Both tone perception and music pitch perception are poor in Chinese CI patients compared to normal-hearing subjects (Wang et al., 2011b; Wang et al., 2012). Research to improve music pitch perception has potential applications in tonal perception. Strategies to improve tonal discrimination, however, remains an area in need of further research.
4. Summary
There is rising demand for hearing-related health services by a population with improved life expectancy in a developing country such as China. The growth of hearing screening and auditory rehabilitation programs in China illustrates the significant impact of government policy in building health care infrastructure. Many aspects of auditory rehabilitation in China, from genetic testing to language specific outcomes, are different from published data in developed countries. This emphasizes a need to tailor hearing research and auditory rehabilitation programs in developing countries to the local population. The growth of domestic CI in China reflects the importance of lower cost and participation of native physician leaders to increase the accessibility of hearing-related health services to a larger proportion of the population in countries worldwide.
Acknowledgments
Source of Funding:
This work was supported by the following:
National Basic Research Program of China (973 Program) (#2012CB967900) to Shi-Ming Yang;
General Financial Grant from the China Postdoctoral Science Foundation (2013M542520), Beijing Nova Program 2016 (Z161100004916130) to Jia-Nan Li;
R01 DC05575, R01 DC01246, and R01 DC012115 from the National Institutes of Health/National Institute on Deafness and Other Communication Disorders to Xuezhong Liu.
Footnotes
Conflict of Interest
Adrien A. Eshraghi is a consultant for Med-EL.
References
- American Academy of Audiology Childhood Hearing Screening Guidelines. 2011 http://www.cdc.gov/ncbddd/hearingloss/documents/AAA_Childhood%20Hearing%20Guidelines_2011.pdf.
- Center for Disease Control and Prevention. CDC’s Hearing Screening and Follow-up Survey. 2009 https://www.cdc.gov/ncbddd/hearingloss/2009-data/2009_ehdi_hsfs_summary_508_ok.pdf.
- Chang YP, Chang RY, Lin CY, Luo X. Mandarin tone and vowel recognition in cochlear implant users: Effects of talker variability and bimodal hearing. Ear Hear. 2016;37:271–281. doi: 10.1097/AUD.0000000000000265. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Chen JM, Amoodi H, Mittmann N. Cost-utility analysis of bilateral cochlear implantation in adults: a health economic assessment from the perspective of a publicly funded program. Laryngoscope. 2014;124:1452–8. doi: 10.1002/lary.24537. 2014. [DOI] [PubMed] [Google Scholar]
- China Disabled Persons’ Federation. The second China national sampling survey of people with disabilities in 2006. 2006 [EB/OL]. http://www.cdpf.org.cn/
- China Disabled Persons’ Federation. Implementation plan of the hearing rehabilitation program for children with disabled children in poor. 2011 http://www.cdpf.org.cn/
- China Disabled Persons’ Federation. Statistical Communique on the Development of the Work on Persons with Disabilities in 2014. 2014 http://www.cdpf.org.cn/
- Chinese Medical Association of Otorhinolaryngology Head and Neck Surgery. Guidelines for early hearing detection and intervention in infants and young children. Chinese Journal of Otorhinolaryngology Head and Neck Surgery. 2009;44:883–887. [PubMed] [Google Scholar]
- Dai P. Prevention and interdiction of hereditary deafness. National Medical Journal of China. 2007;87:1–3. [PubMed] [Google Scholar]
- Dai P, Han DY, Feng B, et al. Gene testing for the enlarged vestibular aqueduct syndrome and mutation analysis of the SLC26A4 gene. Chinese Journal of Otorhinolaryngology Head and Neck Surgery. 2006;13:303–307. [Google Scholar]
- Dettman SJ, Dowell RC, Choo D, et al. Long-term Communication Outcomes for Children Receiving Cochlear Implants Younger Than 12 Months: A Multicenter Study. Otol Neurotol. 2016;37:e82–95. doi: 10.1097/MAO.0000000000000915. [DOI] [PubMed] [Google Scholar]
- Dunn CC, Tyler RS, Oakley S, Gantz BJ, Noble W. Comparison of speech recognition and localization performance in bilateral and unilateral cochlear implant users matched on duration of deafness and age at implantation. Ear Hear. 2008;29:352–9. doi: 10.1097/AUD.0b013e318167b870. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Eshraghi AA, Nazarian R, Telischi FF, et al. The cochlear implant: historical aspects and future prospects. Anat Rec (Hoboken) 2012a;295:1967–80. doi: 10.1002/ar.22580. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Eshraghi AA, Gupta C, Ozdamar O, et al. Biomedical engineering principles of modern cochlear implants and recent surgical innovations. Anat Rec (Hoboken) 2012b;295:1957–66. doi: 10.1002/ar.22584. [DOI] [PubMed] [Google Scholar]
- Eshraghi AA, Rodriguez M, Balkany TJ, et al. Cochlear implant surgery in patients more than seventy-nine years old. Laryngoscope. 2009;119:1180–3. doi: 10.1002/lary.20182. [DOI] [PubMed] [Google Scholar]
- Fu Q-J, Zeng FG, Shannon RV, Soli SD. Importance of tonal envelope cues in Chinese speech recognition. J Acoust Soc Am. 1998;104:505–510. doi: 10.1121/1.423251. [DOI] [PubMed] [Google Scholar]
- Han D, Liu B, Zhou N, et al. Lexical tone perception with HiResolution and HiResolution 120 sound processing strategies in pediatric Mandarin-speaking cochlear implant users. Ear Hear. 2009;30:169–177. doi: 10.1097/AUD.0b013e31819342cf. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Han B, Li JQ, Lan L, et al. A retrospective analysis of the neonatal hearing screening in China mainland. Journal of Audiology and Speech Pathology. 2012;20:6–11. [Google Scholar]
- Han DY, Wang CC. The Current Status and Focus of Cochlear Implantation. Chinese Scientific Journal of Hearing and Speech Rehabilitation. 2013;5:330–334. [Google Scholar]
- Helfand M, Thompson DC, Davis R, et al. Systematic Evidence Review No. 5. Agency for Healthcare Research and Quality Publication No. 02-S001. Rockville, MD: Agency for Healthcare Research and Quality; 2001. Newborn Hearing Screening. Available on the AHRQ Web site at: www.ahrq.gov/clinic/serfiles.htm. [PubMed] [Google Scholar]
- Kliegman RM, Stanton BF, Schor NF. Nelson textbook of pediatrics. 19th. Atlanta (GA): Elsevier/Saunders; 2011. pp. 2188–2193. [Google Scholar]
- Kong YY, Zeng FG. Temporal and spectral cues in Mandarin tone recognition. J Acoust Soc Am. 2006;120:2830–2840. doi: 10.1121/1.2346009. [DOI] [PubMed] [Google Scholar]
- Kuthubutheen J, Mittmann N, Amoodi H, Qian W, Chen JM. The effect of different utility measures on the cost-effectiveness of bilateral cochlear implantation. Laryngoscope. 2015;125:442–7. doi: 10.1002/lary.24902. [DOI] [PubMed] [Google Scholar]
- Kuo YC, Lee CY, Chen MC, et al. The impact of spectral resolution on the mismatch response to Mandarin Chinese tones: an ERP study of cochlear implant simulations. Clin Neurophysiol. 2014;125:1568–75. doi: 10.1016/j.clinph.2013.11.035. [DOI] [PubMed] [Google Scholar]
- Lee FP, Hsu HT, Lin YS, Hung SC. Effects of the electrode location on tonal discrimination and speech perception of Mandarin-speaking patients with a cochlear implant. Laryngoscope. 2012;122:1366–78. doi: 10.1002/lary.23313. [DOI] [PubMed] [Google Scholar]
- Leung J, Wang NY, Yeagle JD. Predictive models for cochlear implantation in elderly candidates. Arch Otolaryngol Head Neck Surg. 2005;131:1049–1054. doi: 10.1001/archotol.131.12.1049. [DOI] [PubMed] [Google Scholar]
- Li JN, Han DY, Hong MD, et al. Cochlear implants in post-lingual deafness patients with long-term total hearing loss. Chinese Journal of Otology. 2010;8:376–381. [Google Scholar]
- Li JN, Ji F, Chen W, et al. Analysis of the performance of post-lingually deafened patients with Nurotron® Venus™ cochlear implants. Acta Otolaryngol. 2014;134:609–614. doi: 10.3109/00016489.2014.894250. [DOI] [PubMed] [Google Scholar]
- Li JN, Ji F, Yang SM. Current status of the study on the central auditory processing disorders in presbycusis. Chinese Journal of Otorhinolaryngology Head and Neck Surgery. 2011;46:523–525. [PubMed] [Google Scholar]
- Li JN, Xi X, Hong MD, et al. Study of aural rehabilitation in post- lingual deafened patients with multi-channel cochlear implant. Journal of Clinical Otorhinolaryngology Head and Neck Surgery. 2010;24:580–582. [PubMed] [Google Scholar]
- Liu W, Rask-Andersen H, Li P, et al. Electric acoustic stimulation implant from round window. Chinese ENT News and Reviews. 2011;28:85–87. [Google Scholar]
- Luo X, Fu QJ. Enhancing Chinese tone recognition by manipulating amplitude envelope: Implications for cochlear implants. J Acoust Soc Am. 2004;116:3659–3667. doi: 10.1121/1.1783352. [DOI] [PubMed] [Google Scholar]
- Luo X, Chang YP, Lin CY, Chang RY. Contribution of bimodal hearing to lexical tone normalization in Mandarin-speaking cochlear implant users. Hear Res. 2014;312:1–8. doi: 10.1016/j.heares.2014.02.005. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Madden C, Halsted M, Meinzen-Derr J, et al. The influence of mutations in the SLC26A4 gene on the temporal bone in a population with enlarged vestibular aqueduct. Arch Otolaryngol Head Neck Surg. 2007;133:162–8. doi: 10.1001/archotol.133.2.162. [DOI] [PubMed] [Google Scholar]
- Manrique M, Cervera-Paz FJ, Huarte A. Advantages of cochlear implantation in prelingual deaf children before 2 years of age when compared with later implantation. Laryngoscope. 2004;114:1462–1469. doi: 10.1097/00005537-200408000-00027. [DOI] [PubMed] [Google Scholar]
- Nelson HD, Bougatsos C, Nygren P. Universal Newborns hearing screening: Systematic Review to Update the 2001 U.S. Preventive Services Task Force Recommendation. Pediatrics. 2008;122:266–276. doi: 10.1542/peds.2007-1422. [DOI] [PubMed] [Google Scholar]
- Noble W, Tyler RS, Dunn CC, Bhullar N. Younger- and older-age adults with unilateral and bilateral cochlear implants: speech and spatial hearing self-ratings and performance. Otol Neurotol. 2009;30:921–9. doi: 10.1097/MAO.0b013e3181b76b3b. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Northern JL, Hayes D. Universal screening for infant hearing impairments: necessary, beneficial and justifiable. Audial Today. 1994;6:10–3. [Google Scholar]
- Prosser JD, Cohen AP, Greinwald JH. Diagnostic Evaluation of Children with Sensorineural Hearing Loss. Otolaryngol Clin North Am. 2015;48:975–82. doi: 10.1016/j.otc.2015.07.004. [DOI] [PubMed] [Google Scholar]
- Roditi RE, Poissant SF, Bero EM. A predictive model of cochlear implant performancein postlingually deafened adults. Otol Neurotol. 2009;30:449–454. doi: 10.1097/MAO.0b013e31819d3480. [DOI] [PubMed] [Google Scholar]
- Semenov YR, Martinez-Monedero R, Niparko JK. Cochlear Implants: Clinical and Societal Outcomes. Otolaryngol Clin N Am. 2012;45:959–981. doi: 10.1016/j.otc.2012.06.003. [DOI] [PubMed] [Google Scholar]
- Wang P, Wang YS, Du B, et al. High frequency mutation of the 233de1C in connexin 26 gene in Chinese deafness populations. Chinese Journal of Otorhinolaryngology Head and Neck Surgery. 2001;8:24–26. [Google Scholar]
- Wang S, Mannell R, Newall P, Han D. Contribution of spectral cues to mandarin lexical tone recognition in normal-hearing and hearing-impaired Mandarin Chinese speakers. Ear Hear. 2011a;32:97–103. doi: 10.1097/AUD.0b013e3181ec5c28. [DOI] [PubMed] [Google Scholar]
- Wang W, Zhou N, Xu L. Musical pitch and lexical tone perception with cochlear implants. Int J Audiol. 2011b;50:270–278. doi: 10.3109/14992027.2010.542490. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wang S, Liu B, Dong R, et al. Music and lexical tone perception in Chinese adult cochlear implant users. Laryngoscope. 2012;122:1353–60. doi: 10.1002/lary.23271. [DOI] [PubMed] [Google Scholar]
- World Health Organization. Factsheet. Deafness and hearing los. 2015 http://www.who.int/mediacentre/factsheets/fs300/en/ [Internet]. Geneva: (Updated March 2015). Last accessed 12/16/2015.
- Xu L, Tsai Y, Pfingst BE. Features of stimulation affecting tonal speech perception: Implications for cochlear prostheses. J Acoust Soc Am. 2002;112:247–258. doi: 10.1121/1.1487843. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Xu L, Zhou N. Tonal languages and cochlear implants. In: Zeng FG, Popper AN, Fay RR, editors. Auditory Prostheses: New Horizons. New York: Springer Science + Business Media, LLC; 2011. pp. 341–364. [Google Scholar]
- Yang SM, Li JN, Ji F, et al. Preliminary clinical research of cochlear implantation in elderly and pre-elderly patients with profound hearing loss. Chinese Journal of Otorhinolaryngology Head and Neck Surgery. 2010a;45:8–12. [PubMed] [Google Scholar]
- Yang SM, Li JN, Han DY. Promotion of cochlear implant in post-lingual deafness adults in China. Chinese Archives of Otolaryngology-Head and Neck Surgery. 2010b;17:23–27. [Google Scholar]
- Ye Q, Klofer J, Yang SM, et al. Cochlear implantation in patients with residual low frequency hearing. Chinese Journal of Otology. 2009;7:22I–225. [Google Scholar]
- Yevgeniy RS, Martinez-Monedero R, Niparko JK. Cochlear Implants: Clinical and Societal Outcomes. Otolaryngol Clin N Am. 2012;45:959–981. doi: 10.1016/j.otc.2012.06.003. [DOI] [PubMed] [Google Scholar]
- Yu LM, Li JN, Wang LY, et al. Long-term results of Nurotron Cochlear Implant System in pediatric deafness. Chinese Journal of Otorhinolaryngology Head and Neck Surgery. 2015;50:646–650. [PubMed] [Google Scholar]
- Yu P, Agramunt A, Guarella Study of speech prosody of the adults deaf with cochlear implant. Chinese Scientific Journal of Hearing and Speech Rehabilitation. 2003;1:26–29. [Google Scholar]
- Yuan HJ, Jiang SC, Yan WY, et al. Screening for the1555G mutation in mitochondrial DNA in pedigrees with aminoglycoside antibiotic induced deafness. Chinese Journal of Otorhinolaryngology Head and Neck Surgery. 1998;33:67–70. [PubMed] [Google Scholar]
- Zeng FG. Trends in cochlear implants. Trends Amplify. 2004;8:1–34. doi: 10.1177/108471380400800102. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Zeng FG, Yang SM, Gao ZQ. Cochlear Implantation: Asia–Pacific Symposium Is an Emerging Force. The Hearing Journal. 2015a;7:8–9. [Google Scholar]
- Zeng FG, Rebscher SJ, Fu QJ, et al. Development and evaluation of the Nurotron 26-electrode cochlear implant system. Hearing Research. 2015b;322:188–199. doi: 10.1016/j.heares.2014.09.013. [DOI] [PubMed] [Google Scholar]
- Zhang F, Xiao Y, Xu L, et al. Mutation Analysis of the Common Deafness Genes in Patients with Nonsyndromic Hearing Loss in Linyi by SNPscan Assay. Biomed Res Int. 2016;2016 doi: 10.1155/2016/1302914. Article ID 1302914. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Zheng WB, Luo JH, Li Y, et al. Mutations in the GJB2 gene in Chinese patients with prelingual non-syndromic hearing impairment. Chinese Journal of Pediatrics. 2000;38:610–613. [Google Scholar]
- Zhou H, Chen Z, Shi H, et al. Comparisons of auditory performance and speech intelligibility in children with cochlear implants placed using different approaches. Otol Neurotol. 2012;33:26–9. doi: 10.1097/MAO.0b013e31823c938e. [DOI] [PubMed] [Google Scholar]
- Zwolan TA, Ashbaugh CM, Alarfaj A. Pediatric cochlear implant patient performance as a function of age at implantation. Otol Neurotol. 2004;25:112–120. doi: 10.1097/00129492-200403000-00006. [DOI] [PubMed] [Google Scholar]