

Abstract
Ischemic mitral regurgitation (IMR) is a frequent complication of left ventricular (LV) global or regional pathological remodeling due to chronic coronary artery disease. It is not a valve disease but represents the valvular consequences of increased tethering forces and reduced closing forces. IMR is defined as mitral regurgitation caused by chronic changes of LV structure and function due to ischemic heart disease and it worsens the prognosis. In this review, we discuss on etiology, pathophysiology, and mechanisms of IMR, its classification, evaluation, and therapeutic corrective methods of IMR.
Keywords: Coronary artery disease, echocardiography, ischemic mitral regurgitation, mitral regurgitation, mitral valve repair
Introduction
Ischemic mitral regurgitation (IMR) is a frequent complication of left ventricular (LV) global or regional pathological remodeling due to chronic coronary artery disease. IMR is defined as mitral regurgitation (MR) caused by chronic changes of LV structure and function due to ischemic heart disease. It is not a valve disease but represents the valvular consequences of increased tethering forces and reduced closing forces.[1] It is reported in approximately one-fifth of patients following acute myocardial infarction (MI) and one-half of those with congestive heart failure.[2] IMR is a frequent complication of coronary artery disease and it worsens the prognosis.[3,4]
It is important to distinguish between primary MR due to organic disease of one or more components of the mitral valve apparatus and secondary MR which is not a valve disease, but represents LV disease. Secondary MR is defined as functional MR, due to LV remodeling by cardiomyopathy or coronary artery disease. In the latter clinical setting, secondary functional MR is called IMR. There are some limitations in this definition of functional IMR. Recent studies have revealed evidence of structural changes in the mitral leaflets in response to tethering on them by LV pathological remodeling. The leaflet adaptation includes enlargement and increased stiffness.[2]
Definition, Etiology, and Pathophysiology of Ischemic Mitral Regurgitation
IMR can be defined as “MR resulting from prior MI associated with normal mitral valve leaflets and chordae.”[5] This definition (based solely on the history of MI) is inadequate as it fails to take into account the lesions or dysfunction(s) that result in IMR.[5] Furthermore, MR in patients with prior history of infarction does not necessarily imply IMR (degenerative disease and rheumatic disease may coexist with coronary artery disease), hence the need to also define IMR based on lesions and dysfunction.[6]
MR results from an unbalance between increased tethering forces and reduced closing forces.[1,7] MI of the segments underlying the papillary muscles (typically a lateral or inferior infarct) results in remodeling of that region of the ventricle. Due to LV remodeling, the papillary muscles are displaced apically, posterior, and laterally. The papillary muscle contributes nonextensible chordae to both leaflets; its displacement results in a more apical position of the leaflets and their coaptation point, and a characteristic deformity of the anterior leaflet described as “seagull sign.”[8] Annular dilatation, predominantly of the septolateral dimension, is usually present. The incomplete closure of the normal mitral leaflets results in increased tethering forces.[9] Reduced closing forces include reduction in LV contractility, altered systolic annular contraction, reduced synchronicity between the two papillary muscles and global LV dyssynchrony, especially in basal segments. The pathophysiological process then becomes self-perpetuating as resultant MR leads to ventricular dilatation which, in turn, leads to further papillary muscle displacement, annular enlargement, and then further MR.[8,9,10,11]
Carpentier's classification[12] of leaflet dysfunction is based on the motion of the margin of the leaflet in relation to the annular plane. IMR can be best characterized by this classification. The leaflet dysfunction resulting in the most common form of IMR is Type IIIb, with restricted motions of the margin of the leaflet(s) in systole. Therefore, for the majority of patients, IMR is defined by the presence of the following (a) prior history of MI (b) tethering of predominantly the posterior-medial scallop of the posterior leaflet, and (c) Type IIIb Carpentier's dysfunction with restricted leaflet motion in systole.[12] Other forms of IMR are less common. Type I dysfunction without leaflet restriction (normal leaflet motion) and isolated annular dilatation can occur in the setting of isolated basilar MI. Some patients with IMR have Type II dysfunction (excess leaflet motion), resulting from either an acute (ruptured papillary muscle) or chronic (fibrotic and elongated papillary muscle) myocardial ischemic event. Acute ischemia with papillary muscle dysfunction that would reverse with revascularization alone is now recognized to be valid in only a small percentage of patients with IMR.[7]
The IMR has dynamic characteristics.[13,14] The dynamic characteristics of MR can be appreciated during an exercise Doppler echocardiogram.[15] The degree of MR at rest is unrelated to exercise-induced changes in effective regurgitant orifiace area (EROA) or regurgitant volume.[16] The degree of exercise-induced increase or decrease in MR relates to changes in LV remodeling and valvular deformation and also to changes in LV and papillary muscles synchronicity.[1] Another aspect of the dynamic characteristics of IMR is a possible reduction in regurgitant volume related to a reverse LV remodeling obtained by medical treatment.[15]
Classification of Ischemic Mitral Regurgitation
Depending on echocardiography parameters such as leaflet motion, origin, and characteristics of regurgitant jets, IMR is classified into asymmetric and symmetric tethering patterns.[6]
Asymmetric tethering pattern
Asymmetric tethering is commonly associated with inferolateral infarcts, mild-moderate increased tenting areas, inferolateral remodeling, and a MR jet that is posterior directed due to an anterior mitral valve leaflet override [Figures 1–4].
Figure 1.
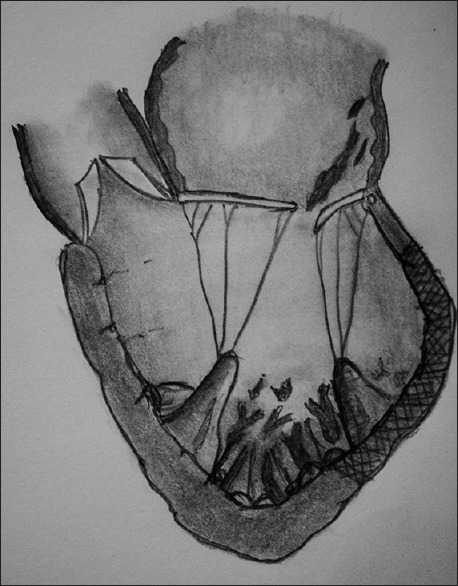
Posterior and apical displacement of posterior-medial papillary muscle typically seen with infero-lateral akinesia or dykinesia at the base of the left ventricular. It causes tethering of posterior mitral leaflet leading to coaptation defect and posterior directed mitral regurgitation jet
Figure 4.
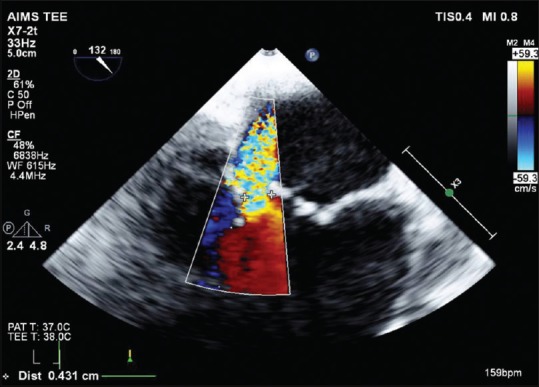
Mitral regurgitation jet is posterior directed and wall hugging
Figure 2.
The mitral regurgitation jet is seen in the posterior-medial commissure. Typically P2 and P3 segments are tethered causing the appearance of pseudo prolapsed of A2/A3 segments of anterior mitral leaflet
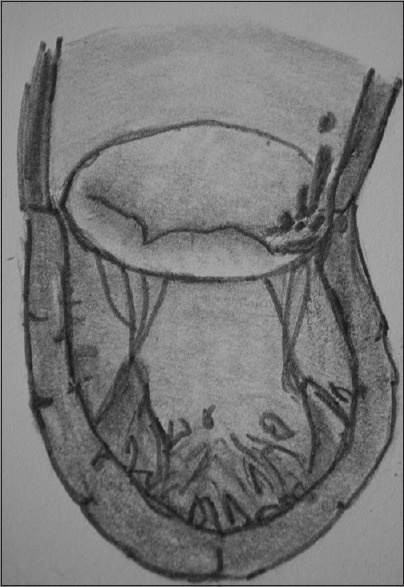
Figure 3.
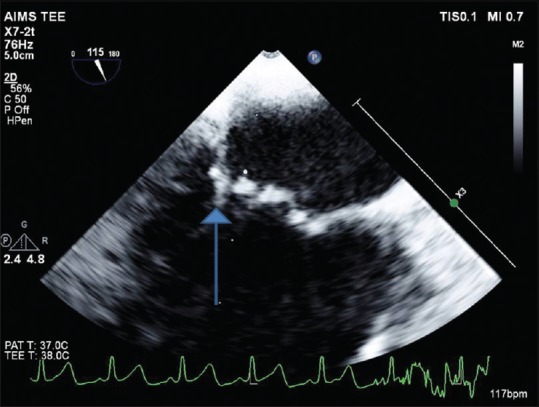
Transesophageal echocardiography LAX view showing restricted posterior mitral leaflet with tethering causing pseudo-prolapse of anterior mitral leaflet
Symmetric tethering pattern
Symmetric tethering is associated with large anterior or multiple infarcts, greater eccentric spherical remodeling, bi-leaflet apical tethering, ventricularization of leaflet coaptation, larger tenting areas, and a central jet direction [Figure 5]. Annular dilatation increases the potential severity of MR associated with asymmetric or symmetric tethering.[6]
Figure 5.
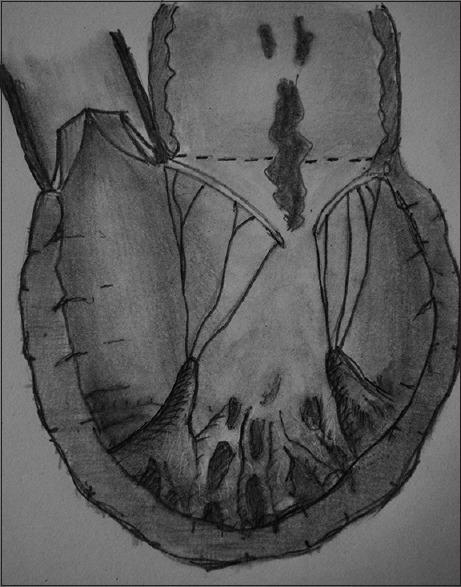
Symmetric mitral regurgitation due to tethering of both leaflets. The left ventricular is spherical due to remodeling. This is typically seen in extensive old anterior wall infarction
Evaluation of Ischemic Mitral Regurgitation
The main risk in patients with functional IMR is to misdiagnose or underestimate MR because whose clinical presentation is ischemic cardiomyopathy with a low intensity systolic murmur. In patients with organic MR, the intensity of cardiac murmur is generally well correlated with the regurgitant volume, but in severe functional IMR, the cardiac murmur is of low intensity, because of low output. Hence, a careful Echocardiography examination is the only means to assess correctly the mechanism and volume of the regurgitation.[17]
Echocardiography
Echocardiography is important in patients with IMR to quantify MR, to elucidate the mechanism of MR and to exclude any abnormality in the mitral valve leaflets. Perioperative transesophageal echocardiography (TEE) provides additional information, especially when TTE gives suboptimal results.
Quantification of mitral regurgitation
Several methods are available for the quantification of IMR in patients scheduled for coronary artery bypass grafting (CABG). MR can be quantified by vena contracta. Vena contracta is the width of the regurgitant jet as it escapes the regurgitant orifice. It reflects the regurgitant orifice area. The vena contracta in IMR is not circular but is elongated along the mitral coaptation line. Therefore in functional MR, a mean vena contracta width obtained from 4 chamber and 2 chamber views may be more accurate. Vena contracta >7 mm is consistent with severe MR.[18] Doppler volumetric method can also be used for the quantification of MR. In this method, the regurgitant volume is measured as the difference between the mitral and aortic stroke volumes. Flow convergence method is one of the most recommended quantitative methods. The proximal iso-velocity surface area (PISA) is measured at mid-systole using the first aliasing velocity. Effective regurgitant orifice area can be calculated using the formula EROA = 2 πr2 Va/Vp where r is the radius of hemispheric PISA zone, Va is the aliasing velocity and Vp is the peak MR velocity. Regurgitant volume can be calculated as the product of EROA and MR VTI.[19] EROA ≥0.2 cm2, regurgitant volume ≥30 ml, regurgitant fraction ≥50% are quantified as severe IMR.[20]
Mitral valve deformation
The normal mitral valve is saddle-shaped. With annular dilatation and LV remodeling associated with ischemic cardiomyopathy, the mitral valve flattens out and loses its saddle. The balance between the closing and tethering forces ensures the proper functioning of mitral valve resulting in adequate coaptation.[21] Ischemic cardiomyopathy results in posterior and apical displacement of papillary muscles, thereby increasing the tethering force. This leads to an apical shift of the coaptation point resulting in increased tenting height, tenting area, and anterior and posterior leaflet angles.[22] Tenting height is the maximal mid systolic distance from mitral leaflet tips to the mitral annular plane. Tenting area is the area bounded by the mitral annular plane and the anterior and posterior mitral leaflets at mid-systole. Thus, the important measurements required for the assessment of mitral valve deformation include leaflet length, diameter of the mitral annulus, coaptation length or tenting height, tenting area, nonplanarity angle, and anterior leaflet and posterior leaflet angles [Figure 6].
Figure 6.
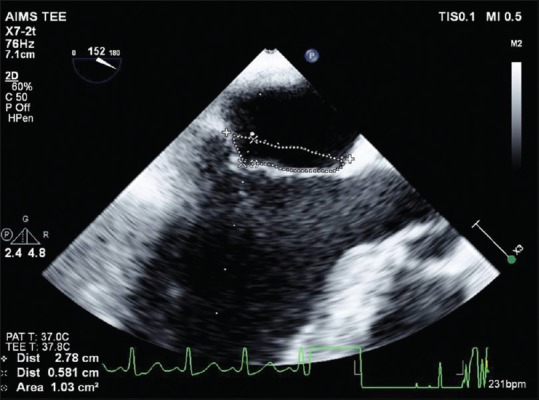
Calculation of tenting area and height
Tenting height <0.5 cm, tenting area of 0 cm2, anterior and posterior leaflet angles <35° are considered normal. Tenting height ≥1 cm, tenting area >2.5–3 cm2, complex jets and posterolateral angle >45° are associated with poor outcome after mitral valve repair (MV repair).[18]
Local and global left ventricular remodeling
The decrease in ventricular function and mechanical coordination disrupts the balance between closing and tethering forces. Decreased ventricular function results in a decreased closing force and papillary muscle displacement leads to increased tethering force.
LV end diastolic and end systolic dimensions, volumes, ejection fraction and dP/dT of the MR jet give an idea about the ventricular function. The sphericity index is an outcome marker which increases with LV dilatation and LV remodeling. The sphericity index is the ratio between the LV end diastolic volume and the volume of an imaginary sphere with its diameter extending from the midpoint of the annular plane to the apex. End-diastolic diameter >65 mm, end-systolic diameter >51 mm and systolic sphericity index >0.7 portend an unfavorable outcome for MV repair in secondary MR.[18,23]
A regional infarct disrupts the normal orientation of papillary muscles and creates asymmetry in the mitral valve apparatus anatomy and function. The papillary muscles are displaced posterior and laterally. This increases the distance between the posterior papillary muscle (PPM) head and intervalvular fibrosa and also the interpapillary distance.[23] Interpapillary distance >20 mm, posterior papillary fibrosa distance >40 mm and lateral wall motion abnormality are associated with poor outcome after MV Repair surgery.[18]
Left atrial remodeling
The volume overload of IMR results in left atrial (LA) dilatation. The LA volume can be measured at end systole and can be indexed to body surface area.
Invasive Investigations
LV angiography frequently associated with coronary angiography is considered as a reference method for the assessment of the volume of MR. However, it has some limitations due to the influence of loading conditions. Quantitative Doppler echocardiography provides more objective data regarding the prognostic role of the regurgitation than ventricular angiography.[17]
Therapeutic Methods in Ischemic Mitral Regurgitation
Medical treatment
Medical therapy in patients with IMR is generally aiming at preventing, delaying, or reverting LV remodeling and heart failure, as well as to prevent myocardial ischemia. There are no specific recommendations specifically targeted to patients with IMR, beyond usual medical treatment of heart failure including angiotensin-converting enzyme inhibitors (ACEIs), β-blockers, spironolactone, nitrates, and diuretics. The combination of β-blockers and ACEIs inhibits progressive LV remodeling, and is associated with a significant reduction in MR severity in patients with chronic heart failure.[24]
Cardiac re-synchronization therapy
Cardiac resynchronization therapy (CRT) has a beneficial effect on functional MR, through reverse LV remodeling, improved LV systolic function, increased closing force, and improved coordinated timing of mechanical activation of PM. The benefit of CRT is limited in patients with IMR, especially in those with important LV dilation and leaflet tethering, or in the presence of a scar at the LV pacing lead tip, which may impede resynchronization, particularly in the posterolateral LV segments.[24]
Thrombolysis and percutaneous coronary intervention
Thrombolysis reduces the incidence of MR following MI through a reduction in local remodeling. Percutaneous coronary interventions (PCIs) also reduce the incidence and severity of MR following MI. Isolated PCI without correcting MR is not an adequate option for the treatment of patients with IMR.[25]
Surgical intervention for ischemic mitral regurgitation
Surgical management of IMR has primarily comprised revascularization with or without the addition of MVR with a variety of techniques including suture, band or ring annuloplasty, or mitral valve replacement.[26,27]
Surgical revascularization alone
Surgical revascularization alone with CABG is sufficient in patients with mild MR. The decision to address the mitral valve in case of moderate IMR is still controversial. Revascularization may lead to reverse remodeling of the left ventricle which in turn may result in a reduction in regurgitation; however, the success of isolated revascularization depends on the extent of viable myocardium. A study by Aklog et al.[8] investigated the role of CABG alone in the correction of moderate IMR. Moreover, this study concluded that CABG alone may not be the optimal therapy for most patients and suggest that concomitant mitral annuloplasty may improve results. The first prospective randomized controlled trial comparing isolated CABG versus CABG plus MV Repair in patients with moderate MR was published in 2009. This single center Italian study randomized 102 patients; 48 patients underwent CABG plus restrictive mitral valve annuloplasty (MVA), while 54 underwent CABG alone. In this study, only 15.5% of patients in the CABG plus MVA group demonstrated New York Heart Association (NYHA) Class II or greater heart failure symptoms versus 43.7% in the isolated CABG group (P = 0.002) at the time of the last follow-up. In addition, CABG-only patients had higher rates of postoperative MR, with lesser improvements in LV dimensions.[27] A Randomized Ischemic Mitral Evaluation (RIME) trial was designed by Chan et al.,[28] to determine whether the addition of MV Repair to CABG in moderate IMR may improve functional capacity and LV reverse remodeling compared with CABG alone. The results of this study show that adding MVA to CABG in patients with moderate IMR may improve functional capacity, LV reverse remodeling, MR severity, and B-type natriuretic peptide (BNP) levels when compared with CABG alone. The largest prospective randomized trial to date is the Surgical Treatment of Moderate Ischemic Mitral Regurgitation Trial, conducted by the Cardiothoracic Surgical Trials Network (CTSN). This trial randomized 301 patients at 26 sites to CABG plus MVA using an undersized complete ring (n = 150) or isolated CABG (n = 151). The primary endpoint was left ventricular end-systolic volume index (LVESVI) at 12 months and secondary endpoints included a major adverse cardiac or cerebral-vascular events (MACCE) composite, as well as mortality, functional status, and quality of life.[29,30] Unlike the RIME trial, there was no significant difference in LVESVI between the groups. Similar to other studies, isolated CABG patients had more residual MR (31.0% vs. 11.2%, P < 0.001), but this was not associated with any difference in MACCE or survival at 12 months. Furthermore in contrast to previous studies, there was no difference in 30-day mortality, functional status, or quality of life at 1 year between the two groups. The CTSN study did demonstrate a significantly higher rate of neurologic events (i.e., stroke, transient ischemic attack, and metabolic encephalopathy) as well as supraventricular arrhythmias in the CABG plus MVA group as compared to the CABG alone group. There may be a subset of patients whose survival, functional status or symptoms may improve with MVA, but this subset of patients has yet to be definitively identified and may comprise patients with predominantly heart failure symptoms with elevated BNP levels.[31]
Surgical revascularization with a mitral valve procedure
The majority of patients with moderate-to-severe IMR require surgical revascularization with a concomitant mitral valve procedure. The optimal strategy for surgical management of IMR remains controversial. Those favoring MV Repair promote its beneficial effects on survival, preserved ventricular function, and the avoidance of long-term anticoagulation, whereas those favoring Mitral valve Replacement (MVR) argue that it ensures long-term freedom from recurrent mitral insufficiency. In addition, proponents of MVR argue that improved surgical techniques to preserve the subvalvular apparatus reduce the previously observed survival benefits of MV Repair, and that the use of bio-prosthetic valves avoids the use of long-term anticoagulation.[32]
Mitral Valve Annuloplasty and Coronary Artery Bypass Grafting
Patients with IMR frequently present severe multi vessel coronary artery disease and thus often undergo CABG. Most frequently used technique, when IMR is severe, is restrictive MVA.[33,34] In various retrospective studies done in patients with moderate to severe MR, using propensity score-matched cohorts of patients showed that CABG combined with MVA is superior to CABG alone with respect to the reduction of MR and symptomatic status improvement in the early postoperative phase, but not on the long-term (10 years).[33,34,35] The ischemic mitral valve is repaired during CABG with the use of an annuloplasty ring, which achieves mitral valve competency by restoring the size of the mitral annulus and increasing mitral leaflet coaptation.[36]
Technique of Mitral Valve Annuloplasty
The placement of an undersized, complete remodeling annuloplasty ring to restore the annulus to its native geometry is most crucial step in a successful valve repair. Sizing is done with the goal of reestablishing the coaptation plane between anterior and posterior leaflet. By the mechanism of under sizing the annuloplasty ring, this will bring the annulus and leaflets together and into alignment, achieving the central line of coaptation. Instead of partial (C-ring) annuloplasty ring, a complete ring should used to treat IMR to avoid recurrence as the anterior annulus may dilate as well, even though it does not dilate as much as posterior annulus. In Ischemic functional MR, annular geometries may vary with individual anatomy and ventricular dilation. Hence, a multitude of rings have been designed. In an article which outlines the steps for repair of IMR, the authors emphasize that a complete, undersized ring is of paramount importance to successful repair and will outweigh any minute advantage gained by employing a specially designed ring.[37]
Mitral Valve Repair versus Mitral Valve Replacement
The most effective surgical approach to the treatment of severe IMR remains controversial. Repair or replacement of the mitral valve prevents ongoing volume overload of the ventricle and thus exacerbation of pathologic remodeling, and alleviates LV wall stress, thereby facilitating a more efficient elliptical geometry.[38] MVR might provide a good alternative to MVA for IMR, but there are increased the risk of several complications including prosthesis-patient mismatch, structural valve failure, thromboembolism, and anticoagulant-related bleeding. In high-risk patients, survival seems similar regardless of the type of procedure.[39] In a recent propensity-based analysis, MVR provided better freedom from mild-to-moderate MR than Repair, and similar survival following a mean 2.5-year follow-up, suggesting that MVR remains a viable option for the treatment of IMR.[40] In addition, in patients with severe ventricular-papillary dysfunction, MVR might even provide better and more durable correction of MR. Initial mortalities were similar among patients undergoing prosthetic replacement and valve reconstruction. Poor outcome was primarily related to preexisting comorbidities.[40] In CTSN trial, patients were randomized with chronic, severe IMR, in a 1:1 ratio, to undergo either mitral-valve repair or chordal-sparing replacement. This study came into a conclusion that there was no significant difference in LV reverse remodeling or survival at 12 months between patients who underwent mitral-valve repair and those who underwent mitral-valve replacement. Replacement provided a more durable correction of MR, but there was no significant difference occurred in clinical outcomes.[41] The rate of recurrence of moderate or severe MR over 2 years was higher in the repair group than in the replacement group (58.8% vs. 3.8%, P < 0.001). There were no significant between-group differences in rates of serious adverse events and overall readmissions, but patients in the repair group had more serious adverse events related to heart failure (P = 0.05) and cardiovascular readmissions (P = 0.01).[42]
Other techniques for correction of Ischemic Mitral Regurgitation
Acorn cardiac restraint device (CorCap™)
The Acorn CorCap Cardiac Support Device (CSD; Acorn Cardiovascular, Inc., St. Paul, Minnesota, USA), is a mesh-like implantable device that is surgically positioned around the heart and adjusted to provide circumferential diastolic support. The CSD is intended to reduce wall stress and myocyte overstretching during end diastole and periodic hemodynamic overload conditions. By reducing or limiting the stress and stretching on the myocardium, a key component of the remodeling process might be halted or reversed. The CorCap device appears safe for patients with dilated cardiomyopathy.[43]
Coapsys™ Device
The Coapsys device was developed to treat patients with clinically significant MR and LV dysfunction. The Coapsys device comprises anterior and posterior epicardial pads connected by an expanded polytetrafluoroethylene-coated, braided polyethylene subvalvular chord. The annular head of the posterior pad was positioned at the annular level to draw the posterior leaflet and annulus toward the anterior leaflet. Final device size was selected when MR was minimized or eliminated as assessed using color flow Doppler echocardiography.[44] The Coapsys annuloplasty system is effective in reducing functional IMR and improving NYHA class.[45]
Chordal cutting
Chordal cutting of two critical secondary chordae of anterior leaflet was first described by Messas. Leaflet closure is restricted by tethering to displaced papillary muscles, and is, therefore, incompletely treated by annular reduction. Cutting a minimum number of basal and secondary chordae can improve coaptation and reduce chronic persistent IMR without impairing LVEF. No adverse effects were noted long-term after chordal cutting at the time of infarction.[46] However, there was a conflicting data from Stanford group,[47] cutting second-order chordae resulted in LV systolic dysfunction and neither prevented nor decreased the severity of acute IMR, septal–lateral annular dilation, leaflet tenting area, or leaflet tenting volume.
Subvalvular techniques
Kron et al. reported a successful subvalvular repair as an adjunct to standard annuloplasty. In this technique, direct relocation of the PPM using a subvalvular trans-ventricular suture to anchor the PPM to the mitral annulus just posterior to the right fibrous trigone. This may be useful for patients with a minimally dilated left ventricle or regional LV geometric changes causing MR.[48,49]
Papillary muscle approximation
This procedure was reported as an adjunct to surgical coronary revascularization, undersized mitral ring annuloplasty or LV volume reduction. The resultant approximation of the papillary muscles would also reduce LV circumferential diameter. Re-approximation of both the papillary muscles is expected to be an effective in reducing leaflet tethering and hence IMR. It can be accomplished through a limited incision without sacrificing viable myocardium.[50]
Percutaneous mitral valve repair
In the late 1990s, Dr. Frederick G. St. Goar developed the foundation of the current MitraClip system (MitraClip, Abbott, Menlo Park, California, USA) with the aim to less invasively reduce MR through a percutaneous/transcatheter approach which is safe and effective.[51] The device approximates the leaflets in an edge-to-edge percutaneous repair technique that diminishes MR, improves functional status, and improves LV remodeling,[52] which are high-risk for surgical MVR or replacement. Other novel devices are under investigation and will add to armamentarium of catheter-based approaches to MR.[53]
Proposed treatment algorithm is depicted in Figure 7.[54]
Figure 7.
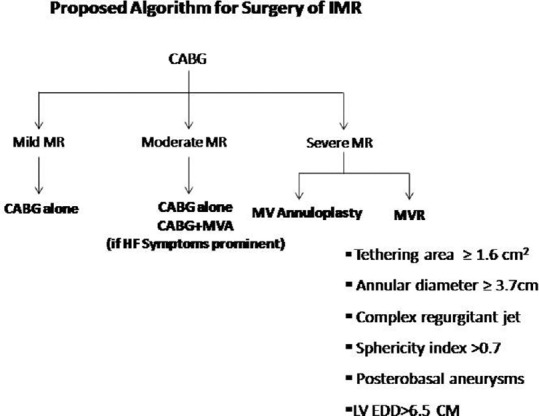
Treatment algorithm for ischemic mitral regurgitation
Conclusion
It is a great challenge to manage IMR. The evaluation of IMR can be accurate by perioperative TEE. Surgical revascularization alone with CABG is sufficient in patients with mild MR, but in the case of severe IMR, CABG along with valve repair can improve functional capacity, LV reverse remodeling, MR severity and BNP levels. The role of concomitant repair in case of moderate IMR is still not clear. The ischemic mitral valve is repaired during CABG with the use of an undersized complete rigid annuloplasty ring. Subvalvular techniques may be added in addition to annuloplasty for the correction of IMR. MVR with Bio-prosthetic valve and total chordal preservation is probably the treatment of choice in severe and complex IMR.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- 1.Piérard LA, Carabello BA. Ischaemic mitral regurgitation: Pathophysiology, outcomes and the conundrum of treatment. Eur Heart J. 2010;31:2996–3005. doi: 10.1093/eurheartj/ehq411. [DOI] [PubMed] [Google Scholar]
- 2.Chaput M, Handschumacher MD, Tournoux F, Hua L, Guerrero JL, Vlahakes GJ, et al. Mitral leaflet adaptation to ventricular remodeling: Occurrence and adequacy in patients with functional mitral regurgitation. Circulation. 2008;118:845–52. doi: 10.1161/CIRCULATIONAHA.107.749440. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Bursi F, Enriquez-Sarano M, Nkomo VT, Jacobsen SJ, Weston SA, Meverden RA, et al. Heart failure and death after myocardial infarction in the community: The emerging role of mitral regurgitation. Circulation. 2005;111:295–301. doi: 10.1161/01.CIR.0000151097.30779.04. [DOI] [PubMed] [Google Scholar]
- 4.Lamas GA, Mitchell GF, Flaker GC, Smith SC, Jr, Gersh BJ, Basta L, et al. Clinical significance of mitral regurgitation after acute myocardial infarction. Survival and ventricular enlargement investigators. Circulation. 1997;96:827–33. doi: 10.1161/01.cir.96.3.827. [DOI] [PubMed] [Google Scholar]
- 5.Serri K, Bouchard D, Demers P, Coutu M, Pellerin M, Carrier M, et al. Is a good perioperative echocardiographic result predictive of durability in ischemic mitral valve repair? J Thorac Cardiovasc Surg. 2006;131:565–73.e2. doi: 10.1016/j.jtcvs.2005.09.037. [DOI] [PubMed] [Google Scholar]
- 6.Anyanwu A, Rahmanian PB, Filsoufi F, Adams DH. The pathophysiology of ischemic mitral regurgitation: Implications for surgical and percutaneous intervention. J Interv Cardiol. 2006;19:S78–86. [Google Scholar]
- 7.Yiu SF, Enriquez-Sarano M, Tribouilloy C, Seward JB, Tajik AJ. Determinants of the degree of functional mitral regurgitation in patients with systolic left ventricular dysfunction: A quantitative clinical study. Circulation. 2000;102:1400–6. doi: 10.1161/01.cir.102.12.1400. [DOI] [PubMed] [Google Scholar]
- 8.Aklog L, Filsoufi F, Flores KQ, Chen RH, Cohn LH, Nathan NS, et al. Does coronary artery bypass grafting alone correct moderate ischemic mitral regurgitation? Circulation. 2001;104(12 Suppl 1):I68–75. doi: 10.1161/hc37t1.094706. [DOI] [PubMed] [Google Scholar]
- 9.Bax JJ, Braun J, Somer ST, Klautz R, Holman ER, Versteegh MI, et al. Restrictive annuloplasty and coronary revascularization in ischemic mitral regurgitation results in reverse left ventricular remodeling. Circulation. 2004;110(11 Suppl 1):II103–8. doi: 10.1161/01.CIR.0000138196.06772.4e. [DOI] [PubMed] [Google Scholar]
- 10.McGee EC, Gillinov AM, Blackstone EH, Rajeswaran J, Cohen G, Najam F, et al. Recurrent mitral regurgitation after annuloplasty for functional ischemic mitral regurgitation. J Thorac Cardiovasc Surg. 2004;128:916–24. doi: 10.1016/j.jtcvs.2004.07.037. [DOI] [PubMed] [Google Scholar]
- 11.Hung J, Papakostas L, Tahta SA, Hardy BG, Bollen BA, Duran CM, et al. Mechanism of recurrent ischemic mitral regurgitation after annuloplasty: Continued LV remodeling as a moving target. Circulation. 2004;110(11 Suppl 1):II85–90. doi: 10.1161/01.CIR.0000138192.65015.45. [DOI] [PubMed] [Google Scholar]
- 12.Carpentier A. Cardiac valve surgery – the “French correction”. J Thorac Cardiovasc Surg. 1983;86:323–37. [PubMed] [Google Scholar]
- 13.Yoran C, Yellin EL, Becker RM, Gabbay S, Frater RW, Sonnenblick EH. Dynamic aspects of acute mitral regurgitation: Effects of ventricular volume, pressure and contractility on the effective regurgitant orifice area. Circulation. 1979;60:170–6. doi: 10.1161/01.cir.60.1.170. [DOI] [PubMed] [Google Scholar]
- 14.Schwammenthal E, Chen C, Benning F, Block M, Breithardt G, Levine RA. Dynamics of mitral regurgitant flow and orifice area. Physiologic application of the proximal flow convergence method: Clinical data and experimental testing. Circulation. 1994;90:307–22. doi: 10.1161/01.cir.90.1.307. [DOI] [PubMed] [Google Scholar]
- 15.Rosario LB, Stevenson LW, Solomon SD, Lee RT, Reimold SC. The mechanism of decrease in dynamic mitral regurgitation during heart failure treatment: Importance of reduction in the regurgitant orifice size. J Am Coll Cardiol. 1998;32:1819–24. doi: 10.1016/s0735-1097(98)00461-6. [DOI] [PubMed] [Google Scholar]
- 16.Lebrun F, Lancellotti P, Piérard LA. Quantitation of functional mitral regurgitation during bicycle exercise in patients with heart failure. J Am Coll Cardiol. 2001;38:1685–92. doi: 10.1016/s0735-1097(01)01605-9. [DOI] [PubMed] [Google Scholar]
- 17.Lancellotti P, Moura L, Pierard LA, Agricola E, Popescu BA, Tribouilloy C, et al. European association of echocardiography recommendations for the assessment of valvular regurgitation. Part 2: Mitral and tricuspid regurgitation (native valve disease) Eur J Echocardiogr. 2010;11:307–32. doi: 10.1093/ejechocard/jeq031. [DOI] [PubMed] [Google Scholar]
- 18.Williams ML, Sulzer CF, Glower DD, Milano C, Aronson S. Assessment of the mitral valve in ischemic heart disease. In: Savage RM, Aronson S, Shernan SK, editors. Comprehensive Textbook of Perioperative Transesophageal Echocardiography. 2nd ed. Ch. 28. Philadelphia: Lippincott Williams and Wilkins; 2011. pp. 462–473. [Google Scholar]
- 19.Nishimura RA, Otto CM, Bonow RO, Ruiz CE, Carabello BA, Skubas NJ, et al. 2014 AHA/ACC guideline for the management of patients with valvular heart disease: Executive summary: A report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. Circulation. 2014;129:1–96. [Google Scholar]
- 20.Beeri R, Otsuji Y, Schwammenthal E, Levine RA. Ischemic mitral regurgitation. In: Otto CM, Bonow RO, editors. Valvular Heart Disease: A Companion to Braunwalds Heart Disease. 3rd ed. Ch. 16. Massachusets: Saunders Elsevier; 2009. pp. 260–273. [Google Scholar]
- 21.Shakil O, Jainandunsing JS, Ilic R, Matyal R, Mahmood F. Ischemic mitral regurgitation: An intraoperative echocardiographic perspective. J Cardiothorac Vasc Anesth. 2013;27:573–85. doi: 10.1053/j.jvca.2012.06.003. [DOI] [PubMed] [Google Scholar]
- 22.Agricola E, Oppizzi M, Maisano F, De Bonis M, Schinkel AF, Torracca L, et al. Echocardiographic classification of chronic ischemic mitral regurgitation caused by restricted motion according to tethering pattern. Eur J Echocardiogr. 2004;5:326–34. doi: 10.1016/j.euje.2004.03.001. [DOI] [PubMed] [Google Scholar]
- 23.Unger P, Magne J, Dedobbeleer C, Lancellotti P. Ischemic mitral regurgitation: Not only a bystander. Curr Cardiol Rep. 2012;14:180–9. doi: 10.1007/s11886-011-0241-y. [DOI] [PubMed] [Google Scholar]
- 24.Kang DH, Sun BJ, Kim DH, Yun SC, Song JM, Choo SJ, et al. Percutaneous versus surgical revascularization in patients with ischemic mitral regurgitation. Circulation. 2011;124(11 Suppl):S156–62. doi: 10.1161/CIRCULATIONAHA.110.011254. [DOI] [PubMed] [Google Scholar]
- 25.Anyanwu AC, Adams DH. Ischemic mitral regurgitation: Recent advances. Curr Treat Options Cardiovasc Med. 2008;10:529–37. doi: 10.1007/s11936-008-0045-6. [DOI] [PubMed] [Google Scholar]
- 26.Badiwala MV, Verma S, Rao V. Surgical management of ischemic mitral regurgitation. Circulation. 2009;120:1287–93. doi: 10.1161/CIRCULATIONAHA.108.836627. [DOI] [PubMed] [Google Scholar]
- 27.Fattouch K, Guccione F, Sampognaro R, Panzarella G, Corrado E, Navarra E, et al. POINT: Efficacy of adding mitral valve restrictive annuloplasty to coronary artery bypass grafting in patients with moderate ischemic mitral valve regurgitation: A randomized trial. J Thorac Cardiovasc Surg. 2009;138:278–85. doi: 10.1016/j.jtcvs.2008.11.010. [DOI] [PubMed] [Google Scholar]
- 28.Chan KM, Punjabi PP, Flather M, Wage R, Symmonds K, Roussin I, et al. Coronary artery bypass surgery with or without mitral valve annuloplasty in moderate functional ischemic mitral regurgitation: Final results of the randomized ischemic mitral evaluation (RIME) trial. Circulation. 2012;126:2502–10. doi: 10.1161/CIRCULATIONAHA.112.143818. [DOI] [PubMed] [Google Scholar]
- 29.Smith PK, Puskas JD, Ascheim DD, Voisine P, Gelijns AC, Moskowitz AJ, et al. Surgical treatment of moderate ischemic mitral regurgitation. N Engl J Med. 2014;371:2178–88. doi: 10.1056/NEJMoa1410490. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Gulack BC, Englum BR, Castleberry AW, Daneshmand MA, Smith PK, Perrault LP. Repair or observe moderate ischemic mitral regurgitation during coronary artery bypass grafting? Prospective randomized multicenter data. Ann Cardiothorac Surg. 2015;4:266–72. doi: 10.3978/j.issn.2225-319X.2015.04.02. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.LaPar DJ, Kron IL. Should all ischemic mitral regurgitation be repaired? When should we replace? Curr Opin Cardiol. 2011;26:113–7. doi: 10.1097/HCO.0b013e3283439888. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Mihaljevic T, Lam BK, Rajeswaran J, Takagaki M, Lauer MS, Gillinov AM, et al. Impact of mitral valve annuloplasty combined with revascularization in patients with functional ischemic mitral regurgitation. J Am Coll Cardiol. 2007;49:2191–201. doi: 10.1016/j.jacc.2007.02.043. [DOI] [PubMed] [Google Scholar]
- 33.Jones RH. Adding mitral valve annuloplasty to surgical revascularization does not benefit patients with functional ischemic mitral regurgitation. J Am Coll Cardiol. 2007;49:2202–3. doi: 10.1016/j.jacc.2007.03.018. [DOI] [PubMed] [Google Scholar]
- 34.Diodato MD, Moon MR, Pasque MK, Barner HB, Moazami N, Lawton JS, et al. Repair of ischemic mitral regurgitation does not increase mortality or improve long-term survival in patients undergoing coronary artery revascularization: A propensity analysis. Ann Thorac Surg. 2004;78:794–9. doi: 10.1016/j.athoracsur.2004.03.022. [DOI] [PubMed] [Google Scholar]
- 35.Braun J, van de Veire NR, Klautz RJ, Versteegh MI, Holman ER, Westenberg JJ, et al. Restrictive mitral annuloplasty cures ischemic mitral regurgitation and heart failure. Ann Thorac Surg. 2008;85:430–6. doi: 10.1016/j.athoracsur.2007.08.040. [DOI] [PubMed] [Google Scholar]
- 36.Mohebali J, Chen FY. Mitral valve repair for ischemic mitral regurgitation. Ann Cardiothorac Surg. 2015;4:284–90. doi: 10.3978/j.issn.2225-319X.2015.05.05. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Nicolini F, Maestri F, Agostinelli A, Molardi A, Benassi F, Gallingani A, Gherli T, et al. Surgical treatment for functional mitral regurgitation secondary to dilated cardiomyopathy: Current options and future trends. World J Cardiovasc Dis. 2013;3:100–7. [Google Scholar]
- 38.Gillinov AM, Wierup PN, Blackstone EH, Bishay ES, Cosgrove DM, White J, et al. Is repair preferable to replacement for ischemic mitral regurgitation? J Thorac Cardiovasc Surg. 2001;122:1125–41. doi: 10.1067/mtc.2001.116557. [DOI] [PubMed] [Google Scholar]
- 39.Chan V, Ruel M, Mesana TG. Mitral valve replacement is a viable alternative to mitral valve repair for ischemic mitral regurgitation: A case-matched study. Ann Thorac Surg. 2011;92:1358–65. doi: 10.1016/j.athoracsur.2011.05.056. [DOI] [PubMed] [Google Scholar]
- 40.Grossi EA, Goldberg JD, LaPietra A, Ye X, Zakow P, Sussman M, et al. Ischemic mitral valve reconstruction and replacement: Comparison of long-term survival and complications. J Thorac Cardiovasc Surg. 2001;122:1107–24. doi: 10.1067/mtc.2001.116945. [DOI] [PubMed] [Google Scholar]
- 41.Acker MA, Parides MK, Perrault LP, Moskowitz AJ, Gelijns AC, Voisine P, et al. Mitral-valve repair versus replacement for severe ischemic mitral regurgitation. N Engl J Med. 2014;370:23–32. doi: 10.1056/NEJMoa1312808. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Goldstein D, Moskowitz AJ, Gelijns AC, Ailawadi G, Parides MK, Perrault LP, et al. Two-year outcomes of surgical treatment of severe ischemic mitral regurgitation. N Engl J Med. 2016;374:344–53. doi: 10.1056/NEJMoa1512913. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.Oz MC, Konertz WF, Kleber FX, Mohr FW, Gummert JF, Ostermeyer J, et al. Global surgical experience with the acorn cardiac support device. J Thorac Cardiovasc Surg. 2003;126:983–91. doi: 10.1016/s0022-5223(03)00049-7. [DOI] [PubMed] [Google Scholar]
- 44.Fukamachi K, Inoue M, Popovic ZB, Doi K, Schenk S, Nemeh H, et al. Off-pump mitral valve repair using the coapsys device: A pilot study in a pacing-induced mitral regurgitation model. Ann Thorac Surg. 2004;77:688–92. doi: 10.1016/S0003-4975(03)01309-2. [DOI] [PubMed] [Google Scholar]
- 45.Mishra YK, Mittal S, Jaguri P, Trehan N. Coapsys mitral annuloplasty for chronic functional ischemic mitral regurgitation: 1-year results. Ann Thorac Surg. 2006;81:42–6. doi: 10.1016/j.athoracsur.2005.06.023. [DOI] [PubMed] [Google Scholar]
- 46.Messas E, Pouzet B, Touchot B, Guerrero JL, Vlahakes GJ, Desnos M, et al. Efficacy of chordal cutting to relieve chronic persistent ischemic mitral regurgitation. Circulation. 2003;108(Suppl 1):II111–5. doi: 10.1161/01.cir.0000087658.47544.7f. [DOI] [PubMed] [Google Scholar]
- 47.Rodriguez F, Langer F, Harrington KB, Tibayan FA, Zasio MK, Liang D, et al. Cutting second-order chords does not prevent acute ischemic mitral regurgitation. Circulation. 2004;110(11 Suppl 1):II91–7. doi: 10.1161/01.CIR.0000138396.24335.6a. [DOI] [PubMed] [Google Scholar]
- 48.Kron IL, Green GR, Cope JT. Surgical relocation of the posterior papillary muscle in chronic ischemic mitral regurgitation. Ann Thorac Surg. 2002;74:600–1. doi: 10.1016/s0003-4975(02)03749-9. [DOI] [PubMed] [Google Scholar]
- 49.Langer F, Rodriguez F, Ortiz S, Cheng A, Nguyen TC, Zasio MK, et al. Subvalvular repair: The key to repairing ischemic mitral regurgitation? Circulation. 2005;112(9 Suppl):I383–9. doi: 10.1161/CIRCULATIONAHA.104.523464. [DOI] [PubMed] [Google Scholar]
- 50.Nair RU, Williams SG, Nwafor KU, Hall AS, Tan LB. Left ventricular volume reduction without ventriculectomy. Ann Thorac Surg. 2001;71:2046–9. doi: 10.1016/s0003-4975(01)02460-2. [DOI] [PubMed] [Google Scholar]
- 51.Dal-Bianco JP, Inglessis I, Melnitchouk S, Daher M, Palacios IF. Percutaneous mitral valve edge-to-edge repair for degenerative mitral regurgitation. Curr Treat Options Cardiovasc Med. 2015;17:389. doi: 10.1007/s11936-015-0389-7. [DOI] [PubMed] [Google Scholar]
- 52.Young A, Feldman T. Percutaneous mitral valve repair. Curr Cardiol Rep. 2014;16:443. doi: 10.1007/s11886-013-0443-6. [DOI] [PubMed] [Google Scholar]
- 53.Sorajja P, Nishimura RA, Thompson J, Zehr K. A novel method of percutaneous mitral valve repair for ischemic mitral regurgitation. JACC Cardiovasc Interv. 2008;1:663–72. doi: 10.1016/j.jcin.2008.07.008. [DOI] [PubMed] [Google Scholar]
- 54.American Association for Thoracic Surgery Ischemic Mitral Regurgitation Consensus Guidelines Writing Committee. Kron IL, LaPar DJ, Acker MA, Adams DH, Ailawadi G, et al. 2016 update to the American Association for Thoracic Surgery Consensus Guidelines: Ischemic mitral valve regurgitation. J Thorac Cardiovasc Surg. 2017;153:1076–9. doi: 10.1016/j.jtcvs.2016.11.068. [DOI] [PubMed] [Google Scholar]