

Abstract
Private well stewardship, including on-going testing and treatment, can ensure private well users are able to maintain source-water quality and prevent exposures to potentially harmful constituents in primary drinking water supplies. Unlike municipal water supplies, private well users are largely responsible for their own testing and treatment and well stewardship is often minimal. The importance of factors influencing regular testing, and treatment behaviors, including knowledge, risk perception, convenience and social norms, can vary by geography and population characteristics. The primary goals of this study were to survey a general statewide population of private well users in Wisconsin in order to quantify testing and treatment patterns and gather data on motivations and barriers to well stewardship. The majority of respondents reported using and drinking well water daily but only about one half of respondents reported testing their wells in the last ten years and of these, only 10% reported testing in the last 12 months. Bacteria and nitrates were contaminants most often tested; and, a private laboratory most often conducted testing. The most commonly reported water treatment was a water softener. Living in a particular geographic region and income were the most significant predictors of water testing and treatment. Iron and hardness, which influence water aesthetics but not always safety, were the most commonly reported water quality problems. Health concerns or perceived lack thereof were, respectively, motivators and barriers to testing and treatment. Limited knowledge of testing and treatment options were also identified as barriers. Results confirm previous findings that well stewardship practices are minimal and often context specific. Understanding the target population’s perceptions of risk and knowledge are important elements to consider in identifying vulnerable populations and developing education and policy efforts to improve well stewardship.
Keywords: Private well, well stewardship, testing, treatment, prevention, SHOW
Graphical abstract
1. Introduction
The public health importance of private well stewardship—including periodic testing, appropriate treatment, and maintenance of wells—is often overlooked. Approximately 13 million households (or 15%) in the United States rely on a private well as their primary source of drinking water.1 Unlike public water supplies, no federal laws and minimal state regulations are in place to ensure systematic monitoring for chemical or microbial contaminants in domestic private wells. Rather, well owners have primary responsibility for overall testing, treatment, and maintenance. Public health practitioners acknowledge well stewardship as an important prevention measure to identify problems early and to ensure private well users have access to high quality drinking water. However, additional research is needed to identify factors that influence well stewardship in order to develop strategies that will improve this practice.
Well stewardship is both a local and a national public health challenge.2–4 A USGS report testing private wells in 48 states found that more than one-fifth of all sampled wells had levels greater than health-based standards, and almost 25% of rural wells located in largely agricultural areas exceeded health based standards, with over 34% testing positive for nitrates.2 Private well stewardship is a particularly important issue in states like Wisconsin where at least one quarter of the population is served by a private well as their primary drinking water source5. Wisconsin is fortunate to have a vast resource of deep and plentiful aquifers to supply water for over 800,000 residents throughout many metro-fringe and rural areas of the state. Wisconsin also has a number of potential groundwater quality issues associated with naturally occurring mineral deposits and geological formations in addition to anthropometric threats from agriculture (e.g. nitrate, bacteria) and industry.5,6, 7A recent study by Knobeloch et al. (2013) found that over 47% of samples provided to the Wisconsin State Laboratory of Hygiene for testing had levels of one or more groundwater constituents at or above health based standards.8 Despite occurrence of potentially harmful contaminants found in well water, it is also well established that private well users are often unlikely to regularly test or treat well water according to public health recommendations.7, 9–11 For example, the Wisconsin Department of Natural Resources (DNR) estimates only 10% of the almost one million private well users in the state test their wells according to their agency recommended guidelines with similar findings in Maine and elsewhere.12,8
Proper well stewardship can help private well users maintain drinking water quality and identify source-water quality issues early; however, preventing exposures to potentially harmful constituents requires understanding the specific motivation and barriers to testing and treatment in populations. A recent review by Morris, 2016 categorized drivers of well stewardship into four domains: 1) knowledge and information; 2) risk perception; 3) convenience; and 4) personal and social beliefs.6, 7 The importance and relevance of each domain, as well as specific factors in each domain, are often context specific and can vary across geographies and even within and across communities. A recent expert panel convened by the national Centers for Disease Control and Prevention concluded that additional research to understand testing and treatment behaviors as well as barriers to proper well stewardship is needed in order to identify vulnerable populations and guide targeted outreach and education efforts.3 Given the increasing awareness of the need to understand contextual drivers of well stewardship, several recent studies have examined issues in areas with greater risk of exposure to specific contaminants such as arsenic or general populations in rural Canada.6, 10, 13–19 However, there is a paucity of data available describing determinants of well stewardship among general populations of private well users in the United States.
Given a limited regulatory infrastructure, education campaigns and local well testing programs are the major tools available to promote well stewardship in most communities. For example, state agencies in Wisconsin including the Department of Health, the Wisconsin Department of Natural Resources and the Department of Agriculture provide well owners with contaminant-specific recommendations that suggest regular testing annually for constituents such as nitrates and bacteria and every five to ten years for arsenic and other contaminants. Previous research from across the United States has shown that while messages are well intentioned the public is often confused about how often and when to test.10,18 Some states have begun to develop policies such as mandatory testing at the sale of a property or at the time of new well construction, however, these policies are dependent on population mobility and new construction to initiate or monitor water quality testing.14, 20 Additional research into motivators and barriers to testing in a general population sample of well users could provide important insights into how best to target intervention and policy strategies to promote well stewardship.
This study emerged as part of a community-academic partnership including state and local environmental and health agencies to address current gaps in understanding private well stewardship across Wisconsin. Previous literature in the United States has focused primarily on testing and treatment behaviors among residents in high-risk areas who have potential exposure to groundwater contaminants through private wells. Less is known about the general population. The Survey of the Health of Wisconsin (SHOW) program, an existing health-based examination study that generated a representative sample of Wisconsin adults, was used to recruit participants for a follow-up study of private well users. The primary goals of the project were to: 1) describe the social and demographic characteristics of private well users among a general population based sample of state residents; 2) identify how often private well water was used for everyday living; and 3) to quantify testing and treatment patterns. A final aim of the study was to identify knowledge of, motivations for, and barriers to regular, ongoing well stewardship and to use this information to identify target populations and effective strategies for promoting well stewardship.
2. Methods
2.1 Study Population
Participants were identified based on their indication of being served by a private well as their primary drinking water source during participation in the baseline 2008–2013 Survey of the Health of Wisconsin (SHOW) program (n=726 households). Details and methods of the baseline survey have been previously published.21 In brief, SHOW is a household based examination survey that includes in-home personal interviews, a self-administered questionnaire, audio-computer assisted interviews, and a physical exam. The 2008–2013 cohort included non-institutional adults aged 21–74. Baseline data collection included- but were not limited to -questionnaires on individual health history; socio-demographic and lifestyle factors, health care access and utilization and household characteristics. The physical exam includes objective anthropometric measurements, blood pressure and bio-specimen collection. Beyond initial questions about primary drinking water for each household, no further information on well stewardship was collected at baseline. Of the 726 households recruited at baseline who reported a private well as their primary source of water, 31 households did not give consent to be contacted for future SHOW studies. Some households also divided into multiple households between baseline and follow-up due to moving or divorce (n=24), leaving 719 households as the final target sample for mail-based follow-up. The target population was defined as private well users rather than private well owners because approximately 5% of those using private wells for drinking water were renters and not owners.
2.2 Follow-Up Survey Development and Implementation
The mail survey questionnaire development was supported by a collaboration between academic partners, public health practitioners and environmental managers from the Wisconsin Departments of Health Services (DHS) and Natural Resources (DNR) who had been identified as key stakeholders with interest in private well stewardship. A stakeholder meeting was held to gather baseline information and identify data gaps regarding private well stewardship from public health and environmental protection practitioners and academic partners in water resources. Existing items from previous private well surveys10, 13, 22, 23 were compiled to generate a first draft of the questionnaire to be reviewed and modified by the team. After careful review, stakeholders approved the final questionnaire and study design, and the full study protocol was sent to and approved by the University of Wisconsin Institutional Review Board (study # 2013-0251).
A modified Tailored Design Method was used to recruit participation in the mailed survey.24 The initial survey packet mailing included an invitation letter, a five-dollar bill, the self-administered questionnaire, and a return stamped envelope asking one participant per household to complete the survey. A random self-selection method was used to identify one participant per eligible household to complete the survey. If two household members had originally participated in the baseline survey, households were asked to select one respondent of their choosing to participate. Up to three additional attempts at follow-up were made. Two weeks after the initial mailing, non-respondent households were mailed a follow-up reminder post-card. Five weeks after the initial mailing, another letter, paper survey, and stamped return envelope were mailed and then followed up via email and/or telephone. The final survey instrument is available in supplemental materials (Appendix 1).
2.3 Data Analyses
Personal demographic and health history data from the baseline 2008–2013 SHOW survey were linked to the private well survey responses and used to summarize detailed population characteristics. Existing health conditions were described using the baseline 2008–2013 data. Body mass index (BMI, kg/m2) was calculated using measured height (m) and weight (kg). BMI categories were defined based on World Health Organization cut-points for underweight (<18.5 kg/m2), normal (18.5–24.9 kg/m2), overweight (25.0–29.9 kg/m2), and obese (≥30 kg/m2).25 Smoking status, cancer and diabetes history were all derived from self-reported health history data. Hypertension was defined as a participant having systolic blood pressure equal to or greater than 140 mm Hg and/or diastolic blood pressure equal to or greater than 90 mm Hg, or a self-report of current use of an anti-hypertensive medication.
Urbanicity of each participant’s home, as well as the census block group, county, and health region a participant resides in, were determined using geocoded latitude and longitude for each verified household address. Urban residence was defined as living in an Urbanized Area (50,000 or more people) or Urban Cluster (2,500 to 50,000 people) based on the 2010 US Census definitions.26 All other areas were classified as “rural.” Health regions were defined by the Wisconsin’s Department of Human Services (DHS) and consist of multiple contiguous counties making up public health service regions and consortiums.
In addition to defining private well population characteristics, demographic and geographic data were also used to determine if there were significant differences between respondents who test and treat private wells compared to those who did not. In order to better understand motivations and barriers for testing we also asked detailed questions about testing patterns, types of parameters tested, and what organization conducted the tests. Additional questions asked about risk perceptions and concerns driving testing behaviors and used categorical and open-ended response options. Similarly, we asked about treatment behaviors to determine types of treatment used and reasons for treating or not treating well again using categorical and open-ended response options. Questions were asked to address each of the four previously mentioned categories of motivators and barriers including 1) knowledge and information; 2) risk perceptions; 3) convenience or lack therefore and 4) social perceptions or demographic beliefs.
All analyses were conducted using ESRI ArcGIS version 10.1 and SAS version 9.3. Descriptive statistics, cross tabulations, and logistic regression were used to identify proportions of population and assess the associations between (a) self-reported behaviors (well water testing and treatment), and (b) demographic characteristics, motivators and barriers. Testing was defined first based on response of yes or no to the question “Have you tested your well in the last ten years?” “Yes” responses were followed by a question to understand temporality of testing in response to the question, in the last 12-month (<1 year), 1–5 years or 6–10 years. Well water treatment was defined based on participant self-report of using a carbon filter or other treatment device designed to reduce the concentration of microorganisms and/or chemical contaminants or water softener. Potential confounding variables were selected based on demographic predictors of testing and treatment by demographic subcategory at p<. 05 and included age, income, gender and geographic region.
3. Results
Private Well User Testing Patterns, Constituents Found, Problems Identified and Actions Taken
Private well users identified at baseline were more likely to be older, have slightly less education, have household income between $50,000 and $100,000 and live in rural areas (see Supplemental Table 1) compared to the overall state population. Respondents to the follow-up survey were more likely to be over 60 years of age and have a higher education, higher family income, and higher BMI than non-respondents (data not shown). The majority of respondents (95%) reported drinking their well water at home with 75% reporting they always drink well water. Nearly all also reported using their private well water for cooking, dish washing, showering and bathing (Figure 1).
Figure 1.
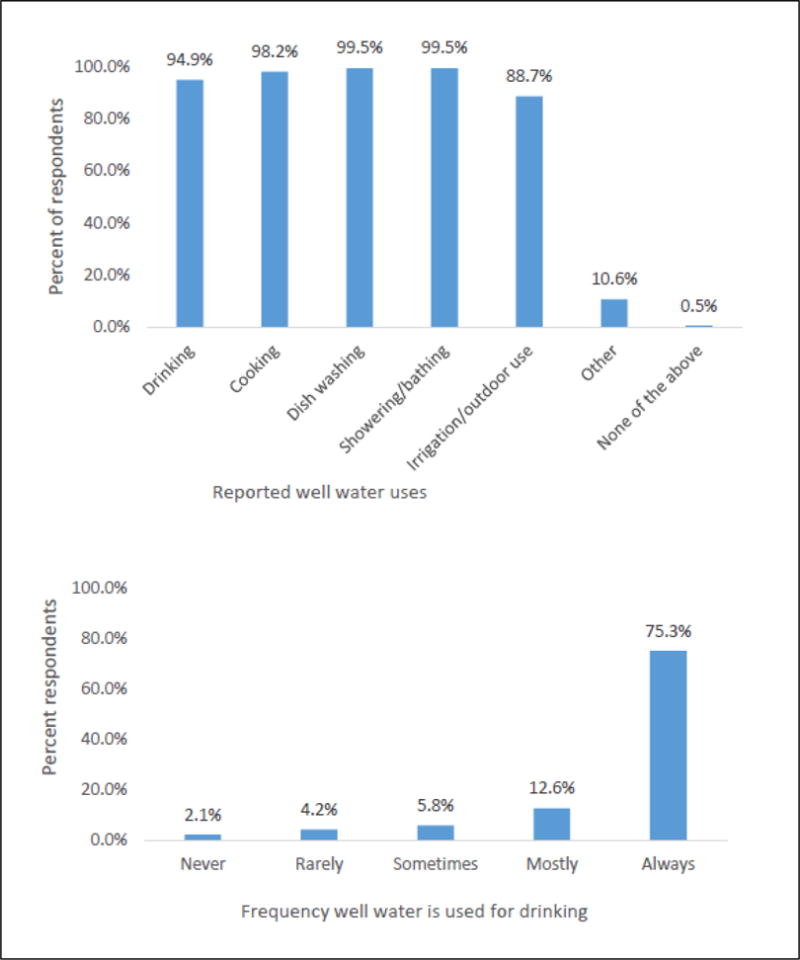
Primary Uses of Drinking Water by Proportion of 434 households (top). Proportion of participants reporting frequency of never, rarely, sometimes, mostly and always drinking water, 429 households (bottom).
There were no statistically significant differences in testing patterns by demographics with the exception of health region. Approximately one half of well users (53%) reported having tested their well water in the last 10 years. Crude rates of testing in the last ten years verses not testing trended higher for females, non-smokers, those with a median family income of $50,000–$99,000, and those with more children in the home. Among those who tested, about one-fifth reported testing their well water within the past 12 months (19%); a lower testing rate compared to testing 1 to 5 years ago (42%) and between 6 to 10 years ago (37%). Families with children and individuals living in the northern health region tended to report testing in the last 1–5 years rather than 6–10 years. There were no differences in testing rates between those with or without self-report cancer, diabetes, or measured hypertension (data not shown). Models estimating the odds of testing also revealed no statistically significant demographic factors predicted increased odds of testing except for jurisdictional health region in both unadjusted and adjusted models (see supplemental Tables 2 and 3) Private well owners in the Southern Health Region were the most likely to test their wells in the last ten years (66.2%) and had a 2.4 increased odds of testing their well water compared to those in the Southeast (see supplemental Tables 2 and 3).
Figure 3 illustrates reported reasons for and against testing well water, with over a third reporting concerns about water safety as the most prevalent reason for testing. About a fifth reported a real estate transaction; followed by the presence of children, babies, or pregnant women in the home; a well test program offered in the area or community was also important for testing. A small number of respondents (<2%) selected “other-specify,” and identified several other motivations for testing including installation of a new water pump, piping, or tank, occurrence of a natural or man-made disaster, and need to acquire water softener specification. Two respondents indicated concern about contamination from a nearby factory or dairy farm motivated testing.
Figure 3. Main Reasons for or Against Testing Well Water Among Private Well Users in a Statewide Sample of Private Well Users*.
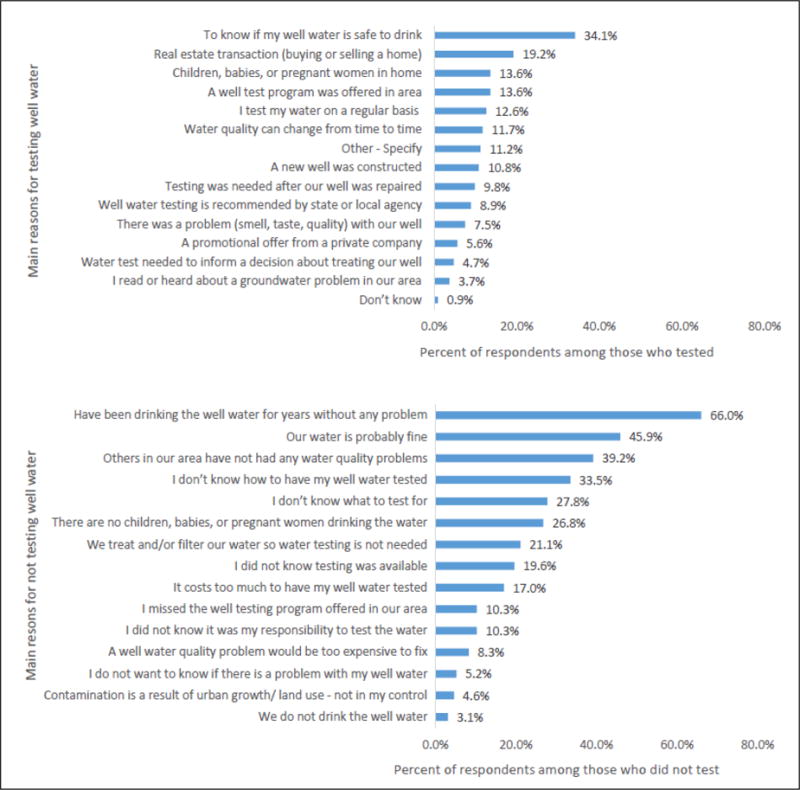
*The main reasons household respondents test their water among the 222 household respondents who reported testing (top) and the main reasons household respondents did not test their water among the 194 respondents who reported not testing (bottom).
Similar to motivations, the top three reasons for not testing well water were related to a lack of perceived problems, with 66% reporting they have been drinking the well water for years without any problem, 46% that their water is probably fine, and 34% that they had not heard of any water quality problems in the area. Over a quarter of participants indicated they didn’t know how to test well water or did not know what to test for. Approximately one-fifth indicated they were treating and/or filtering water so water testing is not needed (21.1%) or they did not have children or pregnant women in the home (Figure 3). Not knowing water testing was available, costs, lack of a local water-testing program, and lack of awareness that testing was the responsibility of private well users were also cited by more than ten percent of respondents. Approximately 8.3% indicated a well water problem would be too expensive to fix so avoided testing.
We also asked participants if they remember what agency may have tested their wells and found a private laboratory or company was most often cited (37%). Local county or city laboratories were reported as providing testing for 15.5% of respondents. State agencies including the Wisconsin State Laboratory of Hygiene, University of Wisconsin Extension and Wisconsin, and the Department of Natural Resources were also cited among ten percent or fewer respondents. Approximately one-third of respondents were unable to identify who tested their well (Table 2).
Table 2.
Primary Organizations Identified as Conducting Private Well Testing and Treatment Types among a Representative Samples of Private Well-Users
| n | % | |
|---|---|---|
| Organization that conducted last test (n=222): | ||
| Private laboratory or company | 78 | 36.6 |
| Wisconsin State Laboratory of Hygiene | 22 | 10.3 |
| Wisconsin Department of Natural Resources | 10 | 4.7 |
| County or City Laboratory (health department) | 33 | 15.5 |
| University of Wisconsin-Extension program | 17 | 8.0 |
| Don’t know | 62 | 29.1 |
|
| ||
| Treatment or filter type used: | ||
| Water Softener | 193 | 42.0 |
| Refrigeration system | 86 | 18.7 |
| Carbon filter | 62 | 13.5 |
| Pitcher-type water filter | 37 | 8.0 |
| Absorbent media (Iron-oxide filter) | 31 | 6.7 |
| Reverse osmosis | 30 | 6.5 |
| Drink only bottled water | 22 | 4.8 |
| Don’t know | 15 | 3.2 |
| Other (specify): (all other responses) | 12 | 2.6 |
| Distillation | 6 | 1.3 |
Figure 4 summarizes water quality parameters tested for, problems identified and actions taken among all respondents who reported testing in the last ten years. Of the 460 respondents 222 (48%) reported testing and provided information on specific water quality parameters they had tested for. Bacteria and nitrates were most commonly reported followed by iron, hardness, lead and pesticides. Testing for other parameters such as pH and/or alkalinity, and conductivity were identified among less than 15% of those providing specific parameter information. Arsenic, manganese, cadmium, cobalt, aluminum, sulfur, chloride, nickel, zinc, calcium, chromium, strontium were reported among even fewer (<2%). Of the 222 who indicated testing for a specific parameter, only 60 (or 13% of all 460 respondents) reported that a water quality problem was identified through testing. Presence of iron and water hardness were most common problems cited despite the greater overall testing rates reported for nitrates and bacteria. A similar proportion reported they “didn’t know” if testing detected a problem. Nitrates were the fourth most common problem identified followed by “other, specify” and bacteria.
Figure 4.
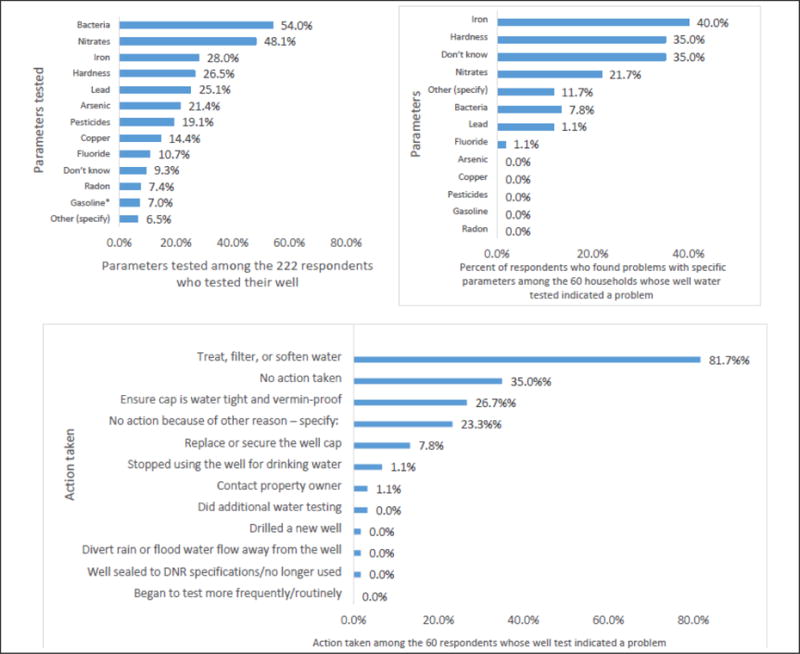
Proportion of Participants Who Tested for Specific Parameters and Actions Taken post Testing Among: a) Total population testing (n=222) (top right); b)Those Whose Testing Indicated a Problem (n=60) (top right) and; c) Actions Taken Among Those Whose Testing Indicated a Problem (n=60) (bottom).
Treating, filtering, or softening water were the most common actions reported as a result of testing. Approximately one-third of those whose test revealed a problem took no further action. A smaller number did report taking steps to protect their well-head and other maintenance including securing the well cap, making it vermin proof or replacing it. Problems reported did not vary based on time since last testing (data not shown).
Demographic and Geographic Patterns of Private Well Treatment, Treatment Type, Motivations and Barriers
Similar to testing, treatment varied by geographic region. Those in the Southeast and Southern health regions were 2.9 (95% CI: 1.4–5.9) and 2.3 (95% CI: 1.4–4.6) times more likely to treat or filter their well water when compared to those in the Western Health region for which overall rates of treatment were lowest. In contrast to testing, income was a statistically significant predictor of treatment. The adjusted odds of treating and/or filtering well water was 2.5 (95% CI: 1.2–5.4) times greater among those with a family income greater than $99,999 compared with those having less than a $25,000 family income. (See Supplemental tables 2 and 3).
Figure 5 summarizes reasons for treating private wells. While bacteria and nitrates had the highest testing rates, the main reason cited for treating water was due to hardness or iron in the water (73.2%), which is consistent with problems identified in Figure 4. About one-third of respondents used treatment because they believed it is healthier and safer (36.4%) and another one-third because treated water tastes and/or smells better (32.7%). Nearly half of all “other-specify” responders indicated treating with a filter system that came with the refrigerator and/or their home (n = 20; 7.4%).
Figure 5. Main Reasons for or Against Treating Well Water Among Private Well Users in a Statewide Representative Sample*.
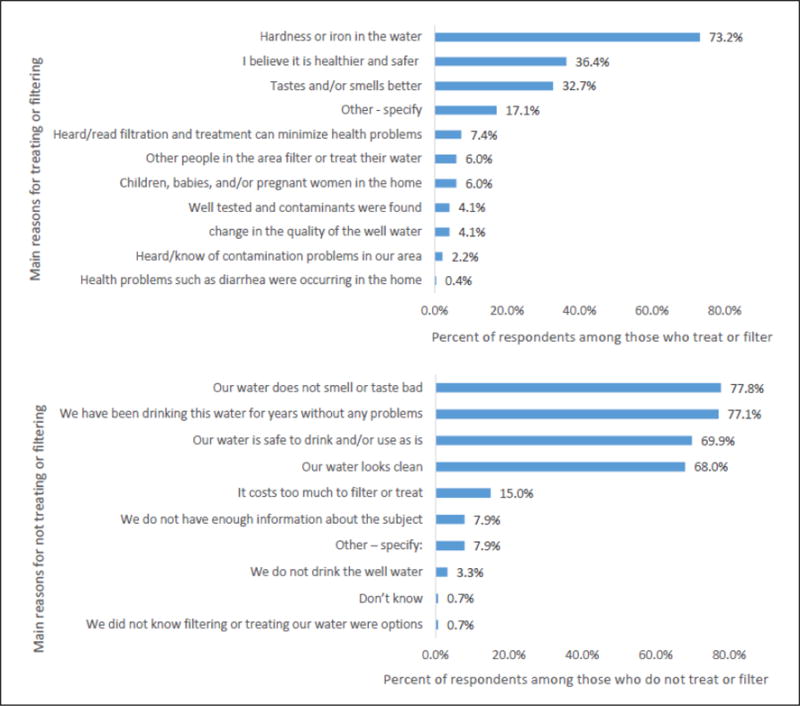
*The main reasons household respondents treat or filter their water among the 265 household respondents who reported treating or filtering (top) and the main reasons household respondents do not treat or filter their water among the 159 household respondents who reported not treating or filtering (bottom).
Aesthetics and perceived safety were among the primary reasons cited for treating well water. As summarized in Figure 5, two-thirds of respondents did not treat because they felt the water did not smell or taste bad (78%), they had been drinking the water “for years without any problems” (77%) or they felt their water was safe to drink and/or use as is (and/or it looks clean (68.0%). In contrast to demographic predictors of treatment, only 15% self-reported cost as a determining factor preventing treating and/or filtering well water.
Table 2 describes the different types of water treatment devices reported. Water softener (42%) was most commonly reported followed by refrigeration system (18.7%), carbon filter (13.5%) or pitcher type water filter (8.0%). Other options including absorbent iron-oxide filter, reverse osmosis system or use of bottled water were reported as treatment types by fewer than ten percent of respondents.
Approximately 37% of respondents reported testing their well in the last ten years and that they are currently treating or filtering their well water. Seventeen percent tested in the last ten years but indicated they did not treat or filter. Approximately 26% reported treating and filtering well water but did not report testing water in the last ten years (data not shown). No consistent patterns between testing and treatment behaviors were identified when comparing those who tested with those who treated.
4. Discussion
The State of Wisconsin has a large rural population that primarily relies on private wells as their primary drinking water source and for whom detailed information on well stewardship is largely unknown. Well stewardship is an important protective public health measure because it ensures ongoing assessment of water quality. Regular testing and treatment can lead to early identification of potential drinking water quality problems, help guide selection of appropriate treatment options if warranted and monitor success of mitigation. This is the premise by which the federal safe drinking water act (SDWA) established regulations requiring systematic monitoring of municipal water supplies. Similar regulations on state and federal level have not been employed for private well owners. Over 13 million households are served by private wells in the United States; however, well stewardship is often minimal. Respondents were selected from the Survey of the Health of Wisconsin, a well-characterized population based study that collects extensive survey and exam based data on health and wellness of the states population on an ongoing basis.21 The parent survey provided information on the demographics of populations served by private wells but less detail on well stewardship providing a unique opportunity for a more detailed follow-up study.
Overall results confirm previous research demonstrating that the majority of private well users rely on their well water for every day drinking, bathing and cooking, yet, many do not regularly test. The reported rate of testing in the last ten years (53%) was considerably lower than might have been expected (80%) based on previous studies of target populations living in areas at risk for arsenic and nitrates in Wisconsin.27 Overall testing rates were also lower compared to recent studies which found average lifetime testing rates were above 70% in New Jersey and as high as 89% in Maine.10, 14, 15, 28 Five year testing rates (41%) were also comparable to testing rates from studies of target populations in communities at high risk of arsenic exposure in Wisconsin (41%)27 and Maine (37%) as well as general Wisconsin population estimates from the Wisconsin Department of Health Services (38%).29 Rates of testing for common groundwater constituents of concern in the Wisconsin including arsenic and uranium were particularly low and reported by less than 2% of users. Lower overall rates of testing in our sample may be because we asked about testing in the last ten years rather than ever as was done in these previous studies or it could be due to differences in sample selection. Previous studies in Maine and New Jersey have focused on domestic well stewardship and voluntary testing largely among populations living in areas with high risk of exposure to arsenic or nitrates.4, 10 In contrast, as previously mentioned, SHOW participants were randomly selected to provide both a demographically and geographically representative sample of state residents and not selected based on potential for increased exposure to particular ground water contaminants or concerns.
Motivators and barriers to private well testing could be largely categorized into four domains previously described by Morris, 2016 including: knowledge, risk perception, convenience and social norms. Within these domains we found concerns about health were among the top reasons for testing.6 Knowledge needed for a real estate transaction was the second highest reason reported and suggests that policies of lending institutions and social norms, which have housing inspected prior to sale, may prompt water testing in Wisconsin, despite formal policy requirements. Testing programs like those in Oregon and New Jersey can serve as potential important opportunities for both education and surveillance of well water quality and promotion of stewardship.14, 20 A recent analysis of statewide programs requiring private well testing at the time of real-estate transactions have found testing rates to increase after policy implementation.14 A desire for knowledge about water quality and safety when there were children or pregnant women in the home also relates to risk perceptions and was ranked as the third reason for testing. Convenience was additionally important as having a well testing program in the area was also among the top five reasons for testing.
Barriers to testing appear to fall largely in the domains of social norms, knowledge and convenience as well as risk perception. Studies of private well users in Canadian populations have found complacency, inconvenience, privacy concerns and limited household resources as primary barriers to testing.18, 19 Similarly, we found factors relating to social norms and risk perceptions were most often cited as reasons for not testing. Optimistic bias to believe that oneself is at less risk than others is pervasive.30 People tend to downgrade information that indicates a problem, such as recalling a lower test result than indicated in a lab test.7 Finally, sensory information, such the perception that water looks and tastes good, has a dominate influence on perceived risk and behavior.7 These tendencies, in tandem with social norms, indicate why people thought their water was probably fine and were experiencing no problems with their water. Never hearing of water quality issues among others in the community was another main reason for not testing, supporting findings from prior studies which found nearby wells with a problem increases perceived risk and intentions to test.31, 32
Previous research suggests a common barrier to testing is a lack of understanding of what regular testing and treatment entails. We found that the majority of private well users that do test do not test according to recommended public health guidelines. The Wisconsin Department of Natural Resources (DNR) suggests testing annually for bacteria and nitrates if living in a high agricultural area or if there are children live in the home, and every five to ten years for other naturally occurring constituents such as arsenic and uranium.33 However, only a small proportion (about 10% of the total population) indicated testing in the last year and approximately one-third reported testing in the last 1–5 years. Findings are consistent with studies in Maine where the majority of respondents (80%) did not test within provincial recommended guidelines of every 12 months10 and only 20% of respondents in New Jersey or Maine have ever tested for arsenic in the past.14, 15 It is postulated this lack of regular testing is in part because testing guidelines can be confusing and users are often unaware of which guidelines to follow. A lack of knowledge about how and what to test for were the fourth and fifth cited reasons cited for not testing well water, suggesting potential modifications to existing education and outreach efforts in addition to changing risk perceptions and social norms could all reduce important barriers to testing.7
We also found motivations and barriers to private well stewardship are context specific. Wisconsin has indeed had a long history of high quality groundwater for which many in the state are proud. The long history has led to an overall perception and social norm that groundwater in the state is good and therefore, testing and treatment are not important. At the same time, the state is largely agricultural and changing demands in water table use raise questions about the future of water quality and need for ongoing well stewardship. Previous studies tracking private well water quality across the United States including studies in Oregon, Washington, and by the USGS have found geography to be an important predictor of well water quality.2, 20
Geographic differences in tangible features of water and nuisance constituents also appear to be important contextual drivers of well stewardship in this study population. In multivariate models that adjusted for confounding, the only statistically significant predictor of testing was health regions. Health regions are clusters of neighboring counties combined into jurisdictional areas that also mirror in some respect the unique geological formations that influence hydrology and naturally occurring ground water constituents across Wisconsin. For example, large portions of the south and south west of the state are known as the non-glacial driftless areas from the ice age and contain large mineral deposits of iron ore, calcium and magnesium. Iron and hardness were the second most commonly reported reasons for testing. Iron and hardness are considered nuisance constituents because they do not necessarily pose health risks but do impact aesthetics and can alter taste, impact water use (e.g, washing clothes) and can be somewhat bothersome to private well users.6,34 Thus, the high treatment rates for iron and hardness in our population are also likely motivated by these geological differences in ground water constituents that change tangible features of drinking water, are easy to detect and readily apparent to users and influence both perceived risk and behavior.7
Data were also suggestive that existing well stewardship programs do, in fact, make a difference in testing and treatment patterns in the state. Higher testing rates for bacteria and nitrates are likely due to the extensive network of both local and state public health and academic partners supporting private well testing awareness throughout the state. Wisconsin has a long standing program run by many local health agencies and academic programs in rural areas to educate, fund and sponsor local testing programs for nitrates and bacteria. Local health departments largely target households with pregnant women and children for nitrate testing due to concerns of methemoglobinemia. Over 15% of the study sample indicated testing for nitrates or bacteria and findings that children and pregnant women were important reasons to test in this sample further suggest these messages and programs are effective in reaching at least some state residents and driving behaviors.
Knowledge regarding appropriateness, efficacy of treatment options are also important elements of well stewardship but are often difficult to assess. Approximately two-thirds of the respondents indicated they treated their wells, however, few treated beyond use of whole house water softeners. Water softeners use ion exchange technology for chemical or ion removal to reduce the amount of calcium and magnesium in the water; they can also be designed to remove iron and manganese.35 Some of these systems can additionally remove heavy metals, some radioactivity, nitrates, arsenic, chromium, selenium, and sulfate but designs vary and there is no way of knowing given current data what systems well-users employed. No water softener is designed to protect against protozoa, bacteria, and viruses, something that is often identified as a potential for concern in many rural areas.2, 8, 20, 36 Only one of five participants reported using carbon filters and approximately one in ten participants reported using bottled water, reverse osmosis or other whole house systems that would effectively reduce exposures to other chemical or biological risks. We were unable to ascertain in this study how often the water treatment systems in place are maintained and future research is needed to increase understanding of how effective water treatments systems are both in adequately treating for identified problems as well as how long term maintenance impacts efficacy overtime.
In the future, studies should also consider focusing efforts to protect the most vulnerable populations that not only face the greatest potential for exposure to groundwater constituents but for whom well stewardship is also minimal. In a separate study the Wisconsin health department summarized testing results of nearly 4,000 rural drinking water supplies for coliform bacteria, nitrate, fluoride, and 13 metals as part of a state-funded program that provides assistance to low-income families and found 47% of these wells had levels of constituents that exceeded one or more water quality standards.8 In the current study we found crude rates of testing were lowest among younger individuals and those with lower education and lower income. Income was also a predictor of treatment in this study, and education an important predictor of treatment in other studies10, 19, 37 providing further evidence that lower SES individuals are likely most vulnerable based on both greater potential for exposure and differences in well stewardship.28 Given the strong association between treatment rates and higher income, the costs of treatment may be a barrier to both testing and treatment. Whole house treatment systems and maintenance of water softeners can be costly for some and likely not priorities for others struggling to meet daily basic needs. Thus, private well stewardship may also be a factor that contributes to health disparities, particularly in rural areas.15
Several strengths of this study are important to note. This study was the result of a community-academic partnership to conduct a comprehensive assessment of well stewardship practices including prevalence of testing and treatment rates by geography and demographics in a well-characterized statewide sample of private well users. The sample was selected irrespective of potential risk of exposure to contaminants or other groundwater quality issues. Thus, findings are more likely to reflect general population-based estimates of well stewardship compared to results from existing studies with similar detailed data collected among participants selected because they live in areas with high risk of ground water quality issues due to geology or other factors. Findings are important for public health practitioners, local health departments and others aiming to understand well-stewardship among these populations. At the same time, some limitations are also important to note. The self-reported nature of this study may lead to inflation of both testing and treatment rates in the study. While response rates of 64% are considered relatively high for this type of study; greater participation by older and more educated individuals results in a sample that does not fully represent private well owners in the state, particularly more vulnerable individuals, a common limitation for survey research.38 The lower rates of problems identified through testing programs may reflect issues of recall bias, mentioned earlier. The cross sectional nature of the study limits inferring that motivations and barriers caused testing and treatment and subsequent behavior.
In conclusion, this study of a geographically diverse population based sample of private well users we confirmed well stewardship is minimal despite regular use of private well water for everyday use. Testing and treatment rates were driven by perceived water quality concerns confirming that contextual factors including knowledge, social norms, and aesthetics are important drivers of well stewardship and that these drivers can vary by geographic location. Thus, national, state and local policy makers and educators should take background differences in knowledge, perceptions and social norms in designing effective outreach strategies. Our findings also suggest that future targeted education and outreach efforts to support proper well-stewardship would be welcome from the general population and likely needed to ensure long term public health protection. This is especially true for the approximately one half of private well users in the state who have not tested at all in the last ten years, yet regularly use water for everyday purposes. Without regular well stewardship, households served by private wells are particularly vulnerable to potential risks of drinking water contamination. Socio-demographics including income and access to information or limited knowledge were among the most significant barriers, therefore, outreach and education may be necessary to improve public health protection. Results suggest without regulatory infrastructure for private well protection, public health prevention efforts should focus on simplifying messages and increasing awareness regarding the important reasons for testing and emphasizing the long term health benefits. With additional resources, efforts should also focus on supporting education and financial incentives to ensure appropriate treatment, long-term maintenance to ensure efficacy of primary prevention efforts.
Supplementary Material
Figure 2.
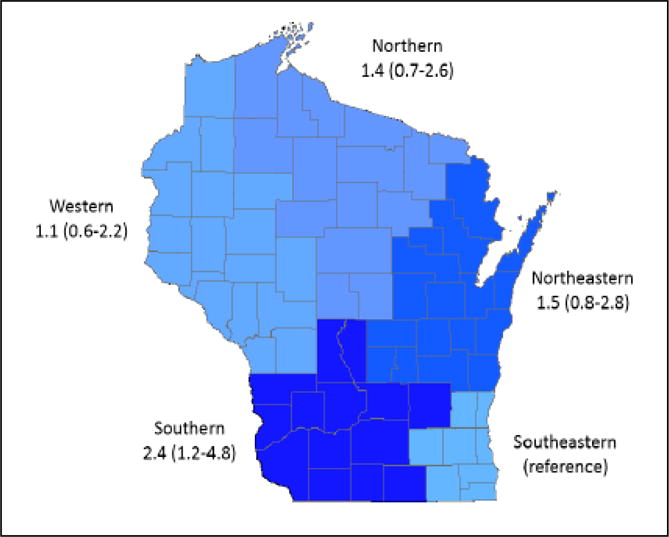
The adjusted odds ratio (AOR) and 95% confidence interval of testing well water comparing each jurisdictional health region to the Southeastern region (reference)
Table 1.
Proportion of households respondents reporting well water treatment and testing, and testing rates by time period among a population based sample of private well users in Wisconsin, 2014.
| Tested | |||||||
|---|---|---|---|---|---|---|---|
| Total (%) (n=460) |
Treat or Filter (%) (n=265) |
Total Testing in Last 10 years (%) (n=222) |
0–1 year ago (%) (n=40) |
1–5 years ago (%) (n=87) |
6–10 years ago (%) (n=79) |
Don’t know(%) (n=7) |
|
| Total | -------- | 64 | 53 | ||||
|
| |||||||
| Gender | |||||||
| Male | 45 | 43 | 41 | 20 | 42 | 37 | 1 |
| Female | 55 | 57 | 59 | 18 | 40 | 37 | 5 |
| Age group | |||||||
| 21–40 | 16 | 16 | 19 | 13 | 52 | 32 | 3 |
| 41–60 | 53 | 51 | 45 | 21 | 40 | 37 | 2 |
| > 60 | 34 | 33 | 36 | 19 | 37 | 39 | 5 |
| Marital status | |||||||
| Married/with partner | 78 | 81 | 77 | 19 | 40 | 40 | 1 |
| Single (divorced/widowed) | 16 | 17 | 15 | 27 | 33 | 33 | 7 |
| Never Married | 2 | 2 | 3 | 0 | 66 | 17 | 17 |
| Education | |||||||
| H.S./GED or less | 26 | 24 | 28 | 15 | 40 | 37 | 7 |
| some college | 37 | 37 | 32 | 22 | 44 | 31 | 3 |
| Bachelors or higher | 37 | 39 | 39 | 18 | 39 | 42 | 1 |
| Income | |||||||
| < $25,000 | 13 | 12 | 11 | 13 | 54 | 21 | 12 |
| $25,000–$49,999 | 26 | 21 | 24 | 19 | 38 | 38 | 5 |
| $50,000–$99,999 | 39 | 42 | 39 | 16 | 43 | 40 | 1 |
| > $99,999 | 22 | 26 | 21 | 27 | 34 | 36 | 3 |
| BMI | |||||||
| < 25 | 31 | 33 | 33 | 17 | 40 | 39 | 4 |
| >=25 and < 30 | 31 | 33 | 30 | 23 | 40 | 37 | 0 |
| >= 30 | 38 | 42 | 37 | 17 | 42 | 35 | 5 |
| Smoking Status | |||||||
| Current | 14 | 12 | 10 | 17 | 43 | 36 | 4 |
| Former | 36 | 39 | 33 | 17 | 45 | 36 | 2 |
| Never | 50 | 49 | 50 | 20 | 38 | 38 | 4 |
| Urbanicitya | |||||||
| Urban | 14 | 16 | 15 | 19 | 43 | 36 | 2 |
| Rural | 86 | 84 | 85 | 19 | 31 | 44 | 6 |
| Children | |||||||
| 0 | 65 | 61 | 28 | 26 | 39 | 32 | 3 |
| 1 or 2 | 23 | 25 | 11 | 14 | 45 | 41 | 0 |
| 3 or more | 12 | 14 | 6 | 42 | 25 | 25 | 8 |
| Health Region | |||||||
| Southeast | 17 | 20 | 14 | 17 | 30 | 40 | 13 |
| South | 17 | 19 | 20 | 20 | 40 | 40 | 0 |
| West | 18 | 15 | 17 | 20 | 33 | 44 | 3 |
| North | 23 | 21 | 24 | 24 | 49 | 26 | 1 |
| Northeast | 25 | 26 | 25 | 13 | 45 | 40 | 2 |
Urban Area (>=50,000 people), Urban cluster (2,500–50,000). Rural (<2,500/anything else) as defined by Census 2010
Measure of hypertension is defined as a participant having systolic blood pressure equal to or greater than 140 mm Hg and/or diastolic blood pressure equal to or greater than 90 mm Hg and/or self-report of currently taking anti-hypertensive medication
Survey of Health of Wisconsin provides state-wide sample of private well owners
Private well stewardship in Wisconsin is influenced by risk perception and knowledge
Over 95% of users use their water daily but only 10% tested their private well in the last year
Testing rates are highest for nitrates and bacteria; treatment is highest for iron and hardness
Limited knowledge and access to information was a barrier to testing and treatment
Multipronged policy and prevention approaches including reducing costs are likely needed
Acknowledgments
This study would not have been possible without the Survey of the Health of Wisconsin (SHOW). SHOW field staff, coordinators, and analysts collected the data and provided technical assistance throughout the development of this report. Thank you to SHOW for the opportunity to collaborate on this project and to their staff for sharing their time, knowledge, and feedback.
Sources of financial support:
This study was supported by the Groundwater Coordinating Council Wisconsin Department of Natural Resources. Funding for SHOW comes from the Wisconsin Division of Public Health, the Wisconsin Partnership Program (PERC) Award (223 PRJ 25DJ), the National Institutes of Health’s Clinical and Translational Science Award (5UL 1RR025011), and the National Heart Lunch and Blood Institute (1 RC2 HL101468). Investigators are also funded on a core grant to the Center for Demography and Ecology at the University of Wisconsin-Madison (P2C HD047873).
Footnotes
Publisher's Disclaimer: This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final citable form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.
References
- 1.Bureau, U. S. C. American Housing Survey for the United States: 2007. U.S. Government Printing Office; Washington, D.C: 2008. [Google Scholar]
- 2.Desimone LA, National Water-Quality Assessment Program (U.S.) Quality of water from domestic wells in principal aquifers of the United States, 1991–2004. U.S Dept of the Interior, U.S. Geological Survey; Reston, Va: 2009. p. xi, 127. [Google Scholar]
- 3.Fox MA, Nachman KE, Anderson B, Lam J, Resnick B. Meeting the public health challenge of protecting private wells: Proceedings and recommendations from an expert panel workshop. The Science of the total environment. 2016;554–555:113–8. doi: 10.1016/j.scitotenv.2016.02.128. [DOI] [PubMed] [Google Scholar]
- 4.Frederick L, VanDerslice J, Taddie M, Malecki K, Gregg J, Faust N, Johnson WP. Contrasting regional and national mechanisms for predicting elevated arsenic in private wells across the United States using classification and regression trees. Water research. 2016;91:295–304. doi: 10.1016/j.watres.2016.01.023. [DOI] [PubMed] [Google Scholar]
- 5.Resources, W. D. o. N. Wells. http://dnr.wi.gov/topic/wells/ (5/5/2017)
- 6.Morris L, Wilson S, Kelly W. Methods of conducting effective outreach to private well owners - a literature review and model approach. Journal of water and health. 2016;14(2):167–82. doi: 10.2166/wh.2015.081. [DOI] [PubMed] [Google Scholar]
- 7.Severtson DJ, Baumann LC, Brown RL. Applying a health behavior theory to explore the influence of information and experience on arsenic risk representations, policy beliefs, and protective behavior. Risk Anal. 2006;26(2):353–68. doi: 10.1111/j.1539-6924.2006.00737.x. [DOI] [PubMed] [Google Scholar]
- 8.Knobeloch L, Gorski P, Christenson M, Anderson H. Private drinking water quality in rural Wisconsin. Journal of environmental health. 2013;75(7):16–20. [PubMed] [Google Scholar]
- 9.Barros N, Rudo K, Shehee M. Importance of regular testing of private drinking water systems in North Carolina. North Carolina medical journal. 2014;75(6):429–34. doi: 10.18043/ncm.75.6.429. [DOI] [PubMed] [Google Scholar]
- 10.Flanagan SV, Marvinney RG, Zheng Y. Influences on domestic well water testing behavior in a Central Maine area with frequent groundwater arsenic occurrence. The Science of the total environment. 2015;505:1274–81. doi: 10.1016/j.scitotenv.2014.05.017. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Swistock BR, Clemens S, Sharpe WE, Rummel S. Water quality and management of private drinking water wells in Pennsylvania. Journal of environmental health. 2013;75(6):60–6. [PubMed] [Google Scholar]
- 12.Resources, W. D. o. N. Wells. http://dnr.wi.gov/topic/wells.
- 13.Flanagan SV, Marvinney RG, Johnston RA, Yang Q, Zheng Y. Dissemination of well water arsenic results to homeowners in Central Maine: influences on mitigation behavior and continued risks for exposure. The Science of the total environment. 2015;505:1282–90. doi: 10.1016/j.scitotenv.2014.03.079. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Flanagan SV, Spayd SE, Procopio NA, Chillrud SN, Braman S, Zheng Y. Arsenic in private well water part 1 of 3: Impact of the New Jersey Private Well Testing Act on household testing and mitigation behavior. The Science of the total environment. 2016;562:999–1009. doi: 10.1016/j.scitotenv.2016.03.196. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Flanagan SV, Spayd SE, Procopio NA, Marvinney RG, Smith AE, Chillrud SN, Braman S, Zheng Y. Arsenic in private well water part 3 of 3: Socioeconomic vulnerability to exposure in Maine and New Jersey. The Science of the total environment. 2016;562:1019–30. doi: 10.1016/j.scitotenv.2016.03.217. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Imgrund K, Kreutzwiser R, de Loe R. Influences on the water testing behaviors of private well owners. Journal of water and health. 2011;9(2):241–52. doi: 10.2166/wh.2011.139. [DOI] [PubMed] [Google Scholar]
- 17.Jones AQ, Dewey CE, Dore K, Majowicz SE, McEwen SA, David WT, Eric M, Carr DJ, Henson SJ. Public perceptions of drinking water: a postal survey of residents with private water supplies. BMC public health. 2006;6:94. doi: 10.1186/1471-2458-6-94. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Kreutzwiser R, de Loe R, Imgrund K, Conboy MJ, Simpson H, Plummer R. Understanding stewardship behaviour: factors facilitating and constraining private water well stewardship. Journal of environmental management. 2011;92(4):1104–14. doi: 10.1016/j.jenvman.2010.11.017. [DOI] [PubMed] [Google Scholar]
- 19.Roche SM, Jones-Bitton A, Majowicz SE, Pintar KD, Allison D. Investigating public perceptions and knowledge translation priorities to improve water safety for residents with private water supplies: a cross-sectional study in Newfoundland and Labrador. BMC public health. 2013;13:1225. doi: 10.1186/1471-2458-13-1225. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Hoppe BO, Harding AK, Staab J, Counter M. Private well testing in Oregon from real estate transactions: an innovative approach toward a state-based surveillance system. Public Health Rep. 2011;126(1):107–15. doi: 10.1177/003335491112600115. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Nieto FJ, Peppard PE, Engelman CD, McElroy JA, Galvao LW, Friedman EM, Bersch AJ, Malecki KC. The Survey of the Health of Wisconsin (SHOW), a novel infrastructure for population health research: rationale and methods. BMC public health. 2010;10:785. doi: 10.1186/1471-2458-10-785. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Liukken B, Severtson DJ, Kilne Robach R. Social Dimensions of Private Well-Testing: Why People Don’t Test Their Wells. 2009 [Google Scholar]
- 23.Healthier Wisconsin Partnership Project. Arsenic in Wisconsin’s residential drinking water Planning for action 2006–2007: Report. 2008 [Google Scholar]
- 24.Dillman DA, Smyth JD, Christian LM. Internet, phone, mail, and mixed-mode surveys: the tailored design method. Fourth. Wiley; Hoboken: 2014. p. xvii, 509. [Google Scholar]
- 25.Consultation, W. Obesity: Preventing and managing the global epidemic - Introduction. Who Tech Rep Ser. 2000;894:1–253. [PubMed] [Google Scholar]
- 26.Bureau, U. S. C. Census Urban and Rural Classification and Urban Area Criteria. 2010 https://www.census.gov/geo/reference/ua/urban-rural-2010.html (January 7, 2017)
- 27.Project, H. W. P. Arsenic in Wisconsin’s residential drinking water planning for action 2006–2007. 2008 [Google Scholar]
- 28.Flanagan SV, Spayd SE, Procopio NA, Chillrud SN, Ross J, Braman S, Zheng Y. Arsenic in private well water part 2 of 3: Who benefits the most from traditional testing promotion? The Science of the total environment. 2016;562:1010–8. doi: 10.1016/j.scitotenv.2016.03.199. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Knobeloch L. 2008–2009 Survey of Private Well Owners in Wisconsin. Wisconsin: Department of Health Services; 2011. [Google Scholar]
- 30.Weinstein ND. Unrealistic optimism about susceptibility to health problems: Conclusions from a community-wide sample. Journal of Behavioral Medicine. 1987;10(5):481–500. doi: 10.1007/BF00846146. [DOI] [PubMed] [Google Scholar]
- 31.Severtson DJ. The influence of environmental hazard maps on risk beliefs, emotion, and health-related behavioral intentions. Research in Nursing & Health. 2013;36(4):330–348. doi: 10.1002/nur.21544. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Severtson DJ, Vatovec C. The theory-based influence of map features on risk beliefs: Self-reports of what is seen and understood for maps depicting an environmental health hazard. Journal of Health Communication: International Perspectives. 2012;17(7):836–856. doi: 10.1080/10810730.2011.650933. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Services, W. D. o. H. a. H. Tests for Drinking Water for Private Wells. Wisconsin: 2011. [Google Scholar]
- 34.Knobeloch LM, Zierold KM, Anderson HA. Association of arsenic-contaminated drinking-water with prevalence of skin cancer in Wisconsin’s Fox River Valley. J Health Popul Nutr. 2006;24(2):206–13. [PubMed] [Google Scholar]
- 35.Prevention, C. f. D. C. a. A Guide to Drinking Water Treatment Technologies for Household Use. 2008 [Google Scholar]
- 36.Hexemer AM, Pintar K, Bird TM, Zentner SE, Garcia HP, Pollari F. An investigation of bacteriological and chemical water quality and the barriers to private well water sampling in a Southwestern Ontario Community. Journal of water and health. 2008;6(4):521–5. doi: 10.2166/wh.2008.070. [DOI] [PubMed] [Google Scholar]
- 37.Lothrop N, Wilkinson ST, Verhougstraete M, Sugeng A, Loh MM, Klimecki W, Beamer PI. Home Water Treatment Habits and Effectiveness in a Rural Arizona Community. Water. 2015;7(3):1217–1231. doi: 10.3390/w7031217. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Galea S, Tracy M. Participation rates in epidemiologic studies. Ann Epidemiol. 2007;17(9):643–53. doi: 10.1016/j.annepidem.2007.03.013. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.