

Abstract
Administrative data from trauma referral centers are useful sources while studying epidemiologic aspects of injuries. We aimed to provide a hospital-based view of injuries in Shiraz considering victims’ age and gender, using administrative data from trauma research center.
A cross-sectional registry-based study of adult trauma patients (age ≥15 years) sustaining injury through traffic accidents, violence, and unintentional incidents was conducted. Information was retrieved from 3 hospital administrative databases. Data on demographics, injury mechanisms, injured body regions, and injury descriptions; outcomes of hospitalization; and development of nosocomial infections were recorded. Injury Severity Score (ISS) was calculated by crosswalking from ICD-10 (International Classification of Diseases) injury diagnosis codes to AIS-98 (Abbreviated Injury Scale) severity codes. Patients were compared based on age groups and gender differences.
A total of 47,295 trauma patients with a median age of 30 (interquartile range: 24–44 years) were studied, of whom 73.1% were male and the remaining 26.9% were female (M/F = 2.7:1.0). The most common injury mechanisms in the male group were car and motorcycle accidents whereas females were mostly victims of falls and pedestrian accidents (P < .01). As age increased, a shift from transportation-related to unintentionally caused injuries occurred. Overall, young men had their most severe injuries on head, whereas elderly women suffered more severe extremity injuries. Injury severity was similar between men and women; however, elderly had a significantly higher ISS. Although incidence of nosocomial infections was independent of victims’ age and gender, elderly men had a significantly higher mortality rate.
Based on administrative data from our trauma center, male gender and age >65 years are associated with increased risk of injury incidence, prolonged hospitalizations, and in-hospital death following trauma. Development of a regional trauma surveillance system may provide further opportunities for studying injuries and evaluating preventive actions.
Keywords: age, epidemiology, gender, injury, Iran, pattern, trauma
1. Introduction
Injuries are the leading cause of morbidity and mortality in developing countries, where more than 90% of world's injury-related deaths occur with preventive efforts often nonexistent, and healthcare systems being least prepared to meet this challenge.[1,2] Iran as a middle-income developing country with a population of 79 million, faces a high incidence of injury-related mortality and morbidly.[3] Overall, injuries accounted for 4 million (26%) of the total 14.4 million disability-adjusted life years in 2003,[4] and if proper preventive strategies are not undertaken, this number is estimated to reach 4.6 million by the year 2025.[5]
Fars is the fourth most populous province in Iran located in the south west of the country with more than 4 million residents. With road-traffic-accident mortality rate of 42 per 100,000 of population in 2011, Fars was fourth of the top 5 deadliest provinces in Iran regarding injuries.[6] The majority of studies in Fars have focused on fatal road-traffic accidents using data from forensic medicine organizations,[6–8] though nonfatal injuries induce considerable burden, which deserve epidemiologic research attention. In addition, it is known that the quality, reliability, and coverage of data vary between surveillance systems[9,10] and therefore, hospital administrative databases may be considered as potential sources of valuable information while studying epidemiologic aspects of injuries. Over the recent years, Shahid Rajaee Trauma Center (Emtiaz) is becoming the major referral center for adult trauma in Fars, highlighting an opportunity for studying the epidemiologic pattern of traumatic injuries in this region. Findings of such studies may provide invaluable information to the health authorities in making major decisions. During the recent 2 years (2014–15), we attempted to determine the injury patterns, severity, and outcomes among various groups of trauma patients referring to Shahid Rajaee Trauma Center with specific focus on age groups and gender differences.
2. Patients and method
This study was carried out at Shiraz Trauma Research Center affiliated to Shiraz University of Medical Sciences as a cross-sectional registry-based analysis of adult trauma patients referring to Emtiaz Hospital (a trauma referral center) during the years 2014 and 2015. The hospital is located in Shiraz, the capital of Fars province, a southern referral province of Iran. The hospital is a tertiary healthcare center for trauma (level I trauma center) which receives trauma patients from all over the province (both urban and rural areas). We aimed to study major injury patterns, severity, and outcome considering the victims’ gender and age. The main source of information was the administrative records of Emtiaz hospital which is a governmental trauma referral center in Shiraz city. Shiraz is the capital of Fars province located in southwest of Iran with a generally hot semiarid climate and a population of 1.7 million Muslim residents (65% of its adult population younger than 45 years, sex ratio 1.02:1.00).
2.1. Study population
As this center is the largest referral center for trauma in Fars province and the emergency medical service's policy in Shiraz is to transfer the majority of trauma patients to this center, we estimate that the patients who visited our center are a powerful sample of the entire injured population of Shiraz. The sampling method was enumeration (census) of all hospitalized patients in emergency departments or other hospital wards during the study period. Inclusion criteria were all trauma patients older than 15 years injured in traffic-related incidents (car, motorcycle, and pedestrian accidents), falls, violence-related incidents, and accidents caused by firearm, and those who were struck by or against objects (47,979 cases). Patients with the following characteristics were excluded: admission for surgical procedures other than emergency trauma intervention, complications of previous trauma surgeries (infection) along with those injured through burns, foreign body aspirations, and sports injuries (684 cases). A total number of 47,295 observations from January 2014 to December 2015 met the inclusion/exclusion criteria which underwent statistical analysis after data validation. The data is entered into a computer-based database and is double-checked and validated by an emergency medicine specialist and a general surgery resident.
2.2. Measurements and data collection
After a patient is screened and on admission, information regarding identifications and baseline demographics including age, gender, admission date and time, and injury mechanism is electronically recorded by the admission unit employees 24 hours a day and 7 days a week. After a patient is discharged, hard-copied records are transferred to the medical records unit where trained staff, routinely extracts information regarding external causes of the injury, injury diagnosis, and final outcome of hospitalization. Information is then coded using International Classification of Diseases (ICD)-10 coding system and entered to an electronic database. Demographic characteristics and injury diagnosis data were extracted from these 2 local databases in hospital and merged.
2.3. Injury description, ISS, and injured body regions (AIS and ISS)
The ISS was calculated according to the ICD-10 code according to the previously described method.[11] An algorithm was designed to convert each ICD-10 rubric (injury diagnosis code) to its relevant AIS-98 score (Abbreviated Injury Scale) where possible. The algorithm was developed using the Microsoft Excel program text functions which entails transforming text strings into numbers. In the ICD-10 lexicon, each injury is described by a code ranging from S.00.0 to T79.7 and a code description. We exclude the ICD-10 diagnostic codes related to foreign bodies (T15.0–T19.9), burns and corrosion injuries (T20.0–T32.9), environmental exposures (T33.0–T35.7, T66.0–T75.8), and poisonings (T36.0–T65.9). Complications of medical care and late effects of injury (T80.0–T98.0) were also excluded leaving a total number of 47,295 patients to be included for ISS calculation. Each injury-related ICD-10 code was assigned to an appropriate AIS-98 severity code (number) where possible. Conservatively, we transformed the ICD-10 codes to the lowest AIS-98 severity score. In cases where, the ICD-10 codes could not be transformed to an accurate AIS severity score, that particular injury was not used in calculating the ISS. Specifically, in cases where the ICD-10 describes injuries to multiple, unidentified, or unspecified body regions, a 99 (missing) code was used (eg, S09.7 multiple injuries of head). We also assigned each ICD-10 injury code to 1 of 6 ISS body regions with the same procedure. ISS was calculated as originally defined by Baker et al.[12]
2.4. Length of stay (LOS), hospital acquired infections (HAI), and mortality
The hospitalization period (LOS) or interval between admission and death were calculated based on subtracting discharge/death date from admission date for each individual. Subjects who were pronounced dead on arrival were not included. Patients were considered to have acquired nosocomial infections, if 1 or more positive cultures were obtained from blood, respiratory secretions, urinary system, surgical incision site, or cerebrospinal fluid. Individuals with a positive culture and LOS less than 48 hours were not assumed to have a nosocomial infection. Since information regarding infectious complications was registered in a different database, the injury characteristics’ data was merged with HAI database.
2.5. Statistical analysis
The statistical Package for Social Sciences Software (SPSS Inc., Chicago, IL, version 18) was used to conduct all statistical analyses. Patterns of injury mechanisms and severity, injured body regions, LOS, development of HAI, and death following admission were compared considering patients’ age and gender. Normality was checked using the 1-sample Kolmogorov-Smirnov test for continuous variables. Summary statistics, including frequency (%) and median interquartile range (IQR) were used where appropriate. Patients were not normally distributed regarding age, ISS, and LOS. Age, ISS, and LOS were categorized into groups for analyses. Chi-square test was used to compare categorical variables between groups. The parametric variables with normal distribution were compared using independent t test for 2 groups and 1-way analysis of variance (ANOVA) for more than 2 groups. The parametric variables without normal distribution were compared using Mann-Whitney U test or Kruskal-Wallis test for 2 or more groups, respectively. A 2-sided P value of less than .05 was considered statistically significant.
3. Results
3.1. Descriptive findings
In this cross-sectional study of injured patients, there were 47,295 individuals older than 15 years, during the years 2014 and 2015. Of the studied individuals, 73.1% were male and the remaining 26.9% were female (M/F = 2.7:1.0) with a median age of 30 years (IQR: 23–44 years). The majority of patients were injured in car accidents (39.6%) and falls (18.8%). There were 454 recorded injury-related deaths during the study period resulting in a 1.0% in-hospital mortality rate. There were 8338 patients staying more than 48 hours (17.6%), of whom 507 (6.1%) developed a nosocomial infection in the course of admission. Table 1 represents demographic characteristic of the studied population.
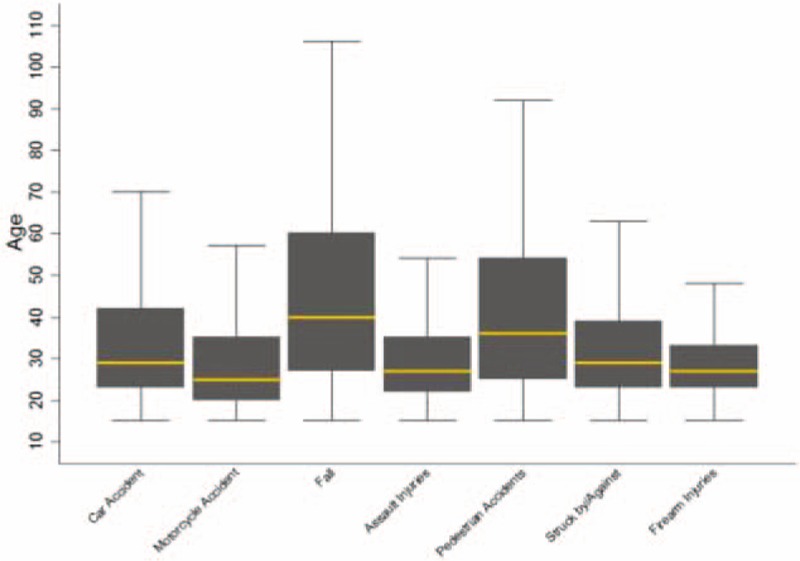
Table 1.
Injury patterns, severity, and outcomes by gender.
3.2. Gender differences
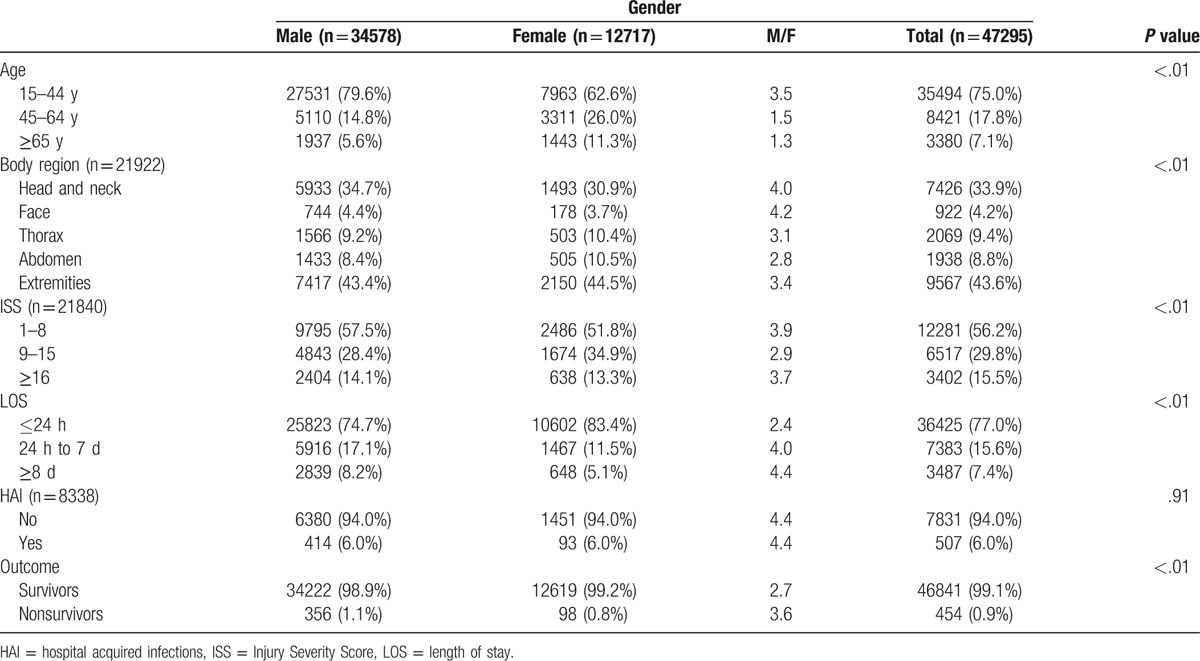
Injured female individuals were significantly older than males (median 35 years [IQR: 25–53] vs 28 years [IQR: 22–40], P < .01). As age increased, the male to female ratio dropped from 3.5 for the 15 to 44 years to 1.3 for patients over 65 years (χ2 (3) = 1782.4, P < .01) (Table 1). There was a statistically significant difference between men and women in terms of injury mechanisms (χ2 (6) = 2781.1, P < .01). The most common injury mechanisms in the male group were car accidents, motorcycle accidents, and falls whereas in the females these were mostly car accidents, falls, and pedestrian accidents (Fig. 1). Comparing to women, a greater proportion of men had their most severe injuries on head and neck (34.7% vs 30.9%) (χ2 (4) = 46, P < .01). A higher proportion of women suffered from severe injuries (χ2 (2) = 75.6, P < .01). Injured male patients stayed significantly longer comparing to females (P < .01). Case-fatality rate was significantly higher among men comparing to women (χ2 (1) = 19.1, P < .01), However, the prevalence of nosocomial infections was similar (χ2 (1) = 0.01, P = .917) (Table 1).
Figure 1.
The mechanism of injury according to the gender in 47,295 trauma patients admitted to our center during 2014 and 2015 (the values are percentage of each category).
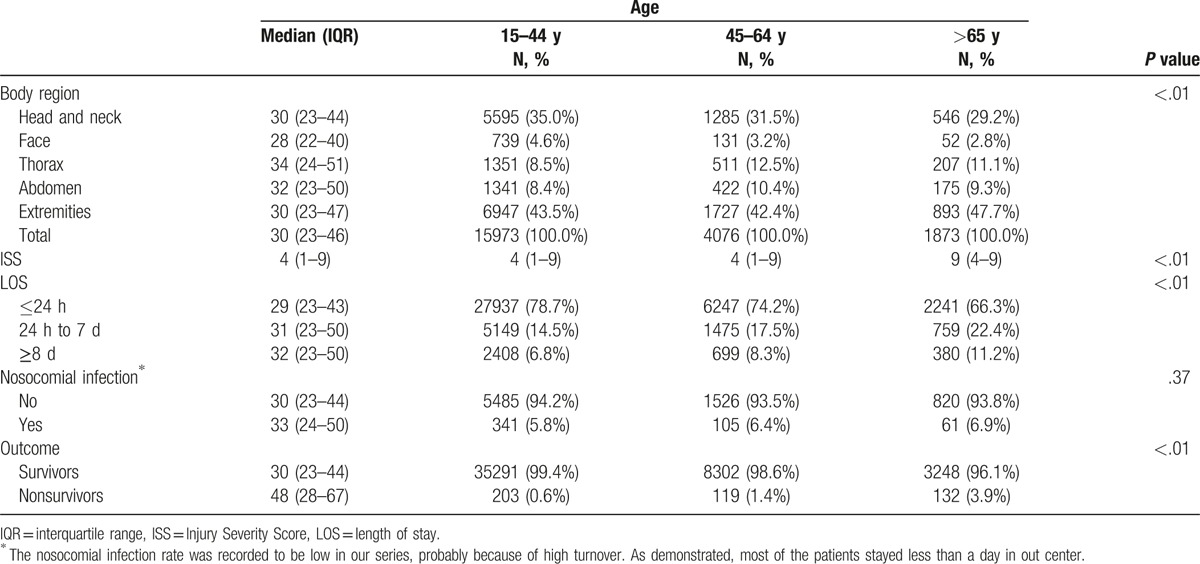
3.3. Age differences
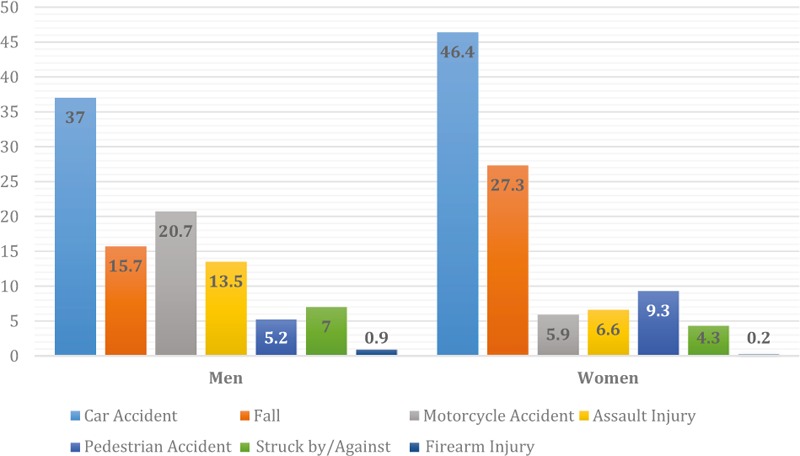
The injury patterns were significantly different among young, middle-aged, and elderly (χ2 (12) = 4350, P < .01) (Figs. 2 and 3). The young age group was mostly injured in car and motorcycle accidents. The middle-aged patients suffered mostly from car accidents and falls. Those >65 years old were mostly injured through falls and car accidents (Table 2). A higher proportion of the elderly (47.7%) had their most severe injuries on extremities compared with the middle-aged (42.2%) and young (43.5%) (χ2 (8) = 137, P < .01). Those older than 65 years had a significantly higher ISS and LOS comparing to young individuals. Similarly, nosocomial infection rate (χ2 (2) = 24, P < .01) and mortality rate (χ2 (2) = 383, P < .01) were significantly higher in the elder group.
Figure 2.
Injury mechanism in young, middle-aged, and elderly trauma patients in Shahid Rajaee (Emtiaz) Hospital Shiraz during 2014 and 2015 (the values are percentage of each category).
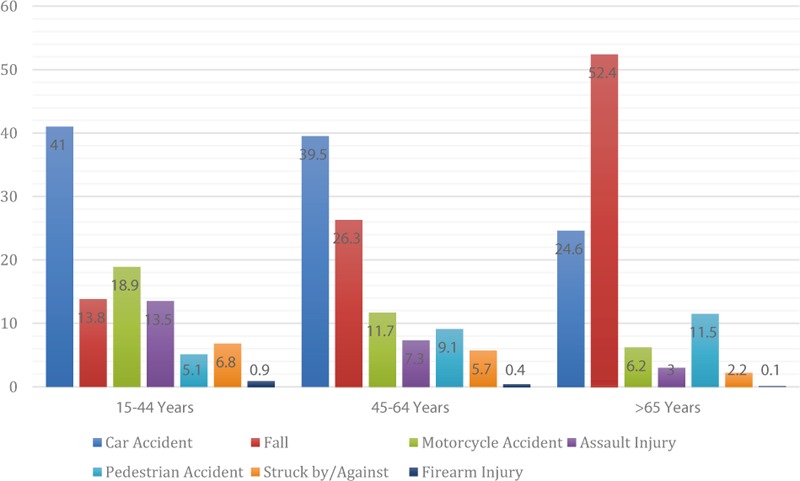
Figure 3.
Age box-plot for various injured patients in Shahid Rajaee (Emtiaz) Hospital Shiraz (2014–15).
Table 2.
Injury patterns, severity, and outcomes in different age groups.
4. Discussion
In this epidemiologic evaluation of injuries, a huge number of trauma patients were evaluated and analyzed. Considering the most recent census in Shiraz (2011), the male to female ratio was 0.98 indicating a similar distribution of Shiraz population across gender categories. The 2.7 observed M/F ratio among injured individuals in Shiraz signifies a higher risk of being injured among males. Most of the existing published data on injuries, originate from university affiliated trauma referral centers (Namazi, Chamran, and Shahid Rajaee hospitals).[6,13–15] Overall the reported M/F ratio among injured patients in Shiraz varies from 1.8 to 4.1, which originates from methodological variations in defining the injured population across different studies.
This study may be considered as the first of its kind in reporting ISS of the injured population in Shiraz using a registry-based method of calculating ISS rather than obtaining ISS directly from medical records. Unlike the previous studies in this region, which have mostly focused on fatal traumas, we provided a detailed description of injury patterns, severity, and outcomes considering nonfatal injuries.
From around the country, various studies have reported sex ratios ranging from 1.17 in Mashhad to 4.0 in Tehran.[16–19] As a proper reference work, Rasouli et al studied over 2.9 million patients admitted to university hospital emergency departments around the country and reported a M/F ratio of 2.66,[20] close to our findings. The cultural norms along with national laws of our country as a middle-income Islamic nation, determines that men are far more involved in outdoor activities (occupational or recreational) compared with women. Further, men are more likely to be licensed for driving and even owing vehicles in Iran. In addition, women are not licensed to drive motorcycles at all. Finally, men are more prone to unsafe road practices including speeding, drinking while driving, and not using seatbelts.[21–23]
On the global scale, a wide range of M/F ratios for injured populations have been reported. Values range from 1.15 to 2 in developed countries[24] and 2.6 to 9 in developing nations.[25–27] The sex ratio for injuries in developed countries is considerably lower than that of the developing nations. With precautions, M/F ratio in injured population of each nation may be addressed as an index of women's participation in social activities. In developed world, women represent a considerable proportion of community's active workforce leaving them to be involved in high-risk behaviors of injuries (driving, outdoor occupations) similar to men. Overall, a smaller M/F ratio represents a larger participation of women.
4.1. Age
The distribution of injured patients across age groups is reflected in Table 1. With a median age of 30 years, 75% of the total were located in the 15- to 44-year-old age group, indicating that victims of injuries are mostly the young proportion of the population. The reported mean age of injured patients varies from 26 to 33 across trauma centers in Shiraz[6,13,15] and Iran,[20,21] which is mainly the result of substantial methodological heterogeneity while recruiting various age groups of injured patients. It is proposed that a national consensus-derived structure should be developed and implemented while conducting injury research and reporting results across populations in Iran.
On the statistical perspective, injured men were significantly younger than women on average. This may be described considering the association between age-gender and injury mechanism. As the age increases, a shift from transportation-related to unintentionally caused injuries (falls, being stuck by objects) occurs. At the same time, men are mostly injured in traffic events (car accidents, motor cycle accidents), and women are mostly injured through falls, or pedestrian accidents and the latter are mostly expected in the elderly. Various authors have emphasized such a shift in injury mechanism across age-gender groups.[28,29]
4.2. Injury mechanism
Overall traffic-related events remained the chief mechanism by which this population sustained injuries, followed by unintentionally caused injuries, and violence-related incidents (12.3%). Similar patterns were reported in previous studies of Shiraz trauma patients[13,14] among Iranian population.[20] As opposed to previous reports in Shiraz and Iran, where motorcyclists ranked first among transportation-related injuries,[14,30] we experienced the car accidents to be the most common cause (63.2%), motorcycle accidents the second (26.7%), and pedestrians (10.1%) the third. This change may be interpreted as the result of enforcing motorcycle safety laws (use of safety helmets, age restrictions) in recent years which has led to a decrease in injuries resulting from motorcycle accidents.
Considering the widespread enforcement of the Iranian national law against possession and transportation of firearms, gunshots were the least common cause of injury for both men and women of all ages. A sex ratio of 11.5 and a median age of 29 in this category, signifies the young male as the high-risk group as previously published.[31,32] Assaults caused 11.5% of the total injuries mostly involving young men (M/F = 5.5) which is compatible with a value of 12% reported by Zargar et al in 2001.[31] Such changes seen within our trauma center is caused mainly by social, political, and economic changes of the entire population rather than changes in medical care.
4.3. Injured body region
So far little attention has been paid to comparison of age-gender groups of trauma patients regarding the injured body regions in Iran. The majority of existing literature has reported head and neck and extremities to be the most commonly injured body regions as we did,[33,34] however, when the number of injuries is taken to account and specifically in the case of multiple injuries, the comparison would be difficult considering methodological variations. To overcome this problem, we considered the most severely injured body region based on AIS scores in the case of multiple trauma. Overall men of young age had their most severe injuries on head whereas women of old age suffered more severe extremity injuries. The importance of injured body region and severity of injuries on each body region is more pronounced when mortality is considered. In this case, using Injury Severity Score (ISS) provides better comparisons between men and women of different ages, since the concept of the number of injuries and their severity is simultaneously considered when ISS is calculated.
4.4. Injury Severity Score
Although determining the severity of an injury is not a negligible issue in the rapidly growing and evolving world of modern trauma research, there are only 2 published studies addressing the severity of injuries in trauma victims on a large scale in Iran, both of which were conducted in Tehran and both employed experienced trauma registrars for ISS calculation.[31,33] Herein, we translated ICD-10 injury diagnosis codes to relative AIS-95 severity codes using an algorithm written in Microsoft Excel program for the first time in Iran. Our injured patients had a median ISS of 4 (IQR: 1–9). Consistent with previous domestic studies where the mean ISS ranged from 6 to 7,[14,31,33] such method of ISS calculation based on ICD-10 diagnostic injury codes, could provide satisfying summaries of injury severity across large populations. In addition, algorithm-derived ISS has been shown to function as a reliable estimate of injury severity in administrative databases.[35] Finally, this method could easily increase the administrative data potential while conducting population-based injury research in Shiraz and Iran.
Although inferential statistics revealed a significant difference between men and women regarding ISS, on a clinical perspective, this difference is of little clinical importance. Similar findings are reported by Roudsari et al in Iran.[21] Finally a meta-analysis found no severity difference between injured men and women.[36] Age stratification revealed a significantly higher ISS in the elderly when compared with middle and young age groups. As discussed earlier, falls and pedestrian accidents are responsible for 60% of the injuries in those older than 65 years. Consistent with previous reports,[14,21] these 2 injury mechanisms cause the most severe injuries in the entire population which leave the elderly with the highest ISS.
4.5. Hospital acquired infections
To the best of our knowledge, our study is the first epidemiologic assessment of HAIs in Shiraz trauma patients using a large hospital administrative database. A 6.1% prevalence of nosocomial infections may be an underestimation since data was not available for all patients, in addition, we defined a HAI as if documented positive cultures were available, the reported value is lower comparing with other centers.[37,38] Incidence of nosocomial infection was independent of victims’ age and gender. A number of other studies have also indicated that acquiring hospital infection may not be independently associated with increased age,[39] however, a systematic review by Lui showed a marked increase in the incidence of sepsis among men.[36] Overall, nosocomial infection is a well-known source of morbidity and mortality in critically ill trauma patients specifically in developing nations.[40] We face an increasing trend of HAI,[41] nonetheless, trauma associated reports are difficult to find in Shiraz. This is because a considerable proportion of trauma patients are admitted to general medical hospitals and medical intensive care units resulting in a tremendous challenge to retrieving, analyzing, and publishing injury-specific information. Among various injury mechanisms, the majority of literature has focused on burn injuries in Shiraz where the incidence of HAI was over 70%.[42,43] We emphasized that patients admitted with other injury mechanisms are also at increased risk of this complication as previously shown that centers should collect and report data separately for trauma and surgical patients in the intensive care unit.[44] Therefore, there is a need for mandatory public reporting of HAI in trauma, identifying high-risk patients in order to implicate proper preventive strategies.
4.6. Limitations and strengths
Study limitations include the standard issue of available clinical data when using a trauma registry. We did not provide data on physiologic parameters of trauma upon admission which are important determinants of outcome. We were not able to account for previous or comorbid conditions or complications after admission that may affect outcomes. In addition, fatalities reported here are not representative of all trauma-related deaths in Shiraz and quality of injury description and severity may be improved. However, ISS was calculated and reported on a large scale based on a newly developed algorithm for the first time in Iran. This study may also provide a primitive framework to construct annual reports of trauma patients to inform the medical community, the public, and decision makers based on a large trauma database in Shiraz.
There are several cultural context of road-traffic accidents in Iranian population, especially in Fars province of Iran with the highest rate of these injuries and highest trauma-associated mortality and morbidity rates.[6,7,45,46] It has been well demonstrated that unsafe behaviors are an important cause of accidents in adolescent age groups in southern Iran. Not using helmets while riding motorcycles, driving when drunk, not obeying the driving rules, uncontrolled high speed, and sleeping when driving are among the most common causes of road-traffic accidents in this region.[47,48] Although the roads condition and absence of safety measures are causes of road-traffic accidents in this region, the newly constructed roads have brought some improvement during the recent years. Currently, there are several regulations on driving behaviors, trying to decrease the road-traffic accidents rate and burden in Iran.
5. Conclusion
In Fars, young men are more likely to suffer from severe head injuries mostly from traffic-related events. Elderly men typically need longer hospitalizations following trauma and sustain an increased chance of in-hospital death. Females are mostly victims of falling down or pedestrian injuries resulting in severe extremity injuries. We propose that trauma centers should actively report with special focus on pre-hospital determinants, injury characteristics, and outcomes/costs of care. Developing a national trauma surveillance system is a primary step since it allows for benchmarking the undertaken actions.
Acknowledgments
We acknowledge Mehrdad Karajizadeh from the Trauma Research Center of Medical Informatics for the help toward drafting of the manuscript. We would also like to acknowledge the editorial assistant of Diba Negar Research Institute for improvement of the language and style of the manuscript.
Footnotes
Abbreviations: AIS = Abbreviated Injury Scale, HAI = hospital acquired infections, ICD = International Classification of Diseases, IQR = interquartile range, ISS = Injury Severity Score, LOS = length of stay.
SB conceived the study. SB and MY contributed in the design of the study. MY and MA performed the statistical analysis, and MY helped in coordination and MA in the collection and interpretation of data. SB, MY, and MA helped to draft the manuscript. All authors read and approved the final manuscript.
This study was supported by Shiraz University of Medical Sciences.
There are no conflicts of interest to be declared regarding the manuscript.
References
- [1].Murray CJ, Vos T, Lozano R, et al. Disability-adjusted life years (DALYs) for 291 diseases and injuries in 21 regions, 1990–2010: a systematic analysis for the Global Burden of Disease Study 2010. Lancet 2012;380:2197–223. [DOI] [PubMed] [Google Scholar]
- [2].Gosselin RA, Spiegel DA, Coughlin R, et al. Injuries: the neglected burden in developing countries. Bull World Health Organ 2009;87:246–a. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [3].Ardalan A, Sepehrvand N, Pourmalek F, et al. Deadly rural road traffic injury: a rising public health concern in I.R. Iran. Int J Prev Med 2014;5:241–4. [PMC free article] [PubMed] [Google Scholar]
- [4].Naghavi M, Abolhassani F, Pourmalek F, et al. The burden of disease and injury in Iran 2003. Popul Health Metri 2009;7:9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [5].Khajehkazemi R, Sadeghirad B, Karamouzian M, et al. The projection of burden of disease in Islamic Republic of Iran to 2025. PloS One 2013;8:e76881. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [6].Heydari S, Hoseinzadeh A, Ghaffarpasand F, et al. Epidemiological characteristics of fatal traffic accidents in Fars province, Iran: a community-based survey. Public Health 2013;127:704–9. [DOI] [PubMed] [Google Scholar]
- [7].Heydari ST, Maharlouei N, Foroutan A, et al. Fatal motorcycle accidents in Fars Province, Iran: a community-based survey. Chin J Traumatol [Zhonghua Chuang Shang Za Zhi]/Chin Med Assoc 2012;15:222–7. [PubMed] [Google Scholar]
- [8].Peymani P, Heydari ST, Hoseinzadeh A, et al. Epidemiological characteristics of fatal pedestrian accidents in Fars Province of Iran: a community-based survey. Chin J Traumatol [Zhonghua Chuang Shang Za Zhi]/Chin Med Assoc 2012;15:279–83. [PubMed] [Google Scholar]
- [9].Gillam C, Meuleners L, Versluis L, et al. Electronic injury surveillance in Perth emergency departments: validity of the data. Emerg Med Australas 2007;19:309–14. [DOI] [PubMed] [Google Scholar]
- [10].McKenzie K, Enraght-Moony EL, Walker SM, et al. Accuracy of external cause-of-injury coding in hospital records. Inj Prev 2009;15:60–4. [DOI] [PubMed] [Google Scholar]
- [11].Yadollahi M, Anvar M, Ghaem H, et al. Logistic regression modeling for evaluation of factors affecting trauma outcome in a level I trauma center in Shiraz. Iran Red Crescent Med J 2017;19: e33559. doi: 10.5812/ircmj.33559. [Google Scholar]
- [12].Baker SP, O’Neill B, Haddon W, Jr, et al. The injury severity score: a method for describing patients with multiple injuries and evaluating emergency care. J Trauma 1974;14:187–96. [PubMed] [Google Scholar]
- [13].Soroush AR, Ghahri-Saremi S, Rambod M, et al. Pattern of injury in Shiraz. Chin J Traumatol [Zhonghua Chuang Shang Za Zhi]/Chin Med Assoc 2008;11:8–12. [DOI] [PubMed] [Google Scholar]
- [14].Abbasi HR, Mousavi SM, Akerdi AT, et al. Pattern of traumatic injuries and Injury Severity Score in a major trauma center in Shiraz, Southern Iran. Bull Emerg Trauma 2013;1:81–5. [PMC free article] [PubMed] [Google Scholar]
- [15].Yadollahi M, Paydar S, Sabetianfard Jahromi G, et al. Types and causalities in dead patients due to traumatic injuries. Arch Trauma Res 2015;4:e26028. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [16].Modaghegh MH, Saremi E, Mohamadian M, et al. Characteristics of trauma in North East Iran and the prevention strategies. Arch Iran Med 2013;16:576–9. [PubMed] [Google Scholar]
- [17].Zargar M, Modaghegh MH, Rezaishiraz H. Urban injuries in Tehran: demography of trauma patients and evaluation of trauma care. Injury 2001;32:613–7. [DOI] [PubMed] [Google Scholar]
- [18].Adib-Hajbaghery M, Maghaminejad F. Epidemiology of patients with multiple trauma and the quality of their prehospital respiration management in Kashan, Iran: six months assessment. Arch Trauma Res 2014;3:e17150. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [19].Ansari-Moghaddam A, Martiniuk AL, Mohammadi M, et al. The pattern of injury and poisoning in South East Iran. BMC Int Health Hum Rights 2012;12:17. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [20].Rasouli MR, Saadat S, Haddadi M, et al. Epidemiology of injuries and poisonings in emergency departments in Iran. Public Health 2011;125:727–33. [DOI] [PubMed] [Google Scholar]
- [21].Roudsari BS, Sharzei K, Zargar M. Sex and age distribution in transport-related injuries in Tehran. Accid Anal Prev 2004;36:391–8. [DOI] [PubMed] [Google Scholar]
- [22].Moini M, Rezaishiraz H, Zafarghandi MR. Characteristics and outcome of injured patients treated in urban trauma centers in Iran. J Trauma 2000;48:503–7. [DOI] [PubMed] [Google Scholar]
- [23].Mohammadzadeh M, Paravar M, Mirzadeh AS, et al. Seat belt usage in injured car occupants: injury pattern, severity and outcome after two main car accident mechanism in Kashan, Iran, 2012. Arch Trauma Res 2015;4:e22203. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [24].Blomberg H, Svennblad B, Michaelsson K, et al. Prehospital trauma life support training of ambulance caregivers and the outcomes of traffic-injury victims in Sweden. J Am Coll Surg 2013;217:1010–9.e1-2. [DOI] [PubMed] [Google Scholar]
- [25].Donaldson RI, Hung YW, Shanovich P, et al. Injury burden during an insurgency: the untold trauma of infrastructure breakdown in Baghdad, Iraq. J Trauma 2010;69:1379–85. [DOI] [PubMed] [Google Scholar]
- [26].Tyson AF, Varela C, Cairns BA, et al. Hospital mortality following trauma: an analysis of a hospital-based injury surveillance registry in sub-Saharan Africa. Journal of surgical education 2014;72:e66–72. [DOI] [PubMed] [Google Scholar]
- [27].Rastogi D, Meena S, Sharma V, et al. Causality of injury and outcome in patients admitted in a major trauma center in North India. Int J Crit Ill Inj Sci 2014;4:298–302. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [28].Schoeneberg C, Probst T, Schilling M, et al. Mortality in severely injured elderly patients: a retrospective analysis of a German level 1 trauma center (2002–2011). Scand J Trauma Resusc Emerg Med 2014;22:45. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [29].Lawson CM, Alexander AM, Daley BJ, et al. Evolution of a Level I Trauma System: changes in injury mechanism and its impact in the delivery of care. Int J Burns Trauma 2011;1:56. [PMC free article] [PubMed] [Google Scholar]
- [30].Bhalla K, Naghavi M, Shahraz S, et al. Building national estimates of the burden of road traffic injuries in developing countries from all available data sources: Iran. Inj Prev 2009;15:150–6. [DOI] [PubMed] [Google Scholar]
- [31].Zargar M, Modaghegh M-HS, Rezaishiraz H. Urban injuries in Tehran: demography of trauma patients and evaluation of trauma care. Injury 2001;32:613–7. [DOI] [PubMed] [Google Scholar]
- [32].Amiri A, Sanaei-Zadeh H, Zavarei HT, et al. Firearm fatalities. A preliminary study report from Iran. J Clin Forensic Med 2003;10:159–63. [DOI] [PubMed] [Google Scholar]
- [33].Eftekhar B, Zarei MR, Ghodsi M, et al. Comparing logistic models based on modified GCS motor component with other prognostic tools in prediction of mortality: results of study in 7226 trauma patients. Injury 2005;36:900–4. [DOI] [PubMed] [Google Scholar]
- [34].Moini M, Rezaishiraz H, Zafarghandi MR. Characteristics and outcome of injured patients treated in urban trauma centers in Iran. J Trauma Acute Care Surg 2000;48:503–7. [DOI] [PubMed] [Google Scholar]
- [35].Haas B, Xiong W, Brennan-Barnes M, et al. Overcoming barriers to population-based injury research: development and validation of an ICD-10-to-AIS algorithm. Can J Surg 2012;55:21. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [36].Liu T, Xie J, Yang F, et al. The influence of sex on outcomes in trauma patients: a meta-analysis. Am J Surg 2015;210:911–21. [DOI] [PubMed] [Google Scholar]
- [37].Niven DJ, Fick GH, Kirkpatrick AW, et al. Cost and outcomes of nosocomial bloodstream infections complicating major traumatic injury. J Hosp Infect 2010;76:296–9. [DOI] [PubMed] [Google Scholar]
- [38].Askarian M, Yadollahi M, Assadian O. Point prevalence and risk factors of hospital acquired infections in a cluster of university-affiliated hospitals in Shiraz, Iran. J Infect Public Health 2012;5:169–76. [DOI] [PubMed] [Google Scholar]
- [39].Appelgren P, Hellstrom I, Weitzberg E, et al. Risk factors for nosocomial intensive care infection: a long-term prospective analysis. Acta Anaesthesiol Scand 2001;45:710–9. [DOI] [PubMed] [Google Scholar]
- [40].Allegranzi B, Bagheri Nejad S, Combescure C, et al. Burden of endemic health-care-associated infection in developing countries: systematic review and meta-analysis. Lancet 2011;377:228–41. [DOI] [PubMed] [Google Scholar]
- [41].Asl HM, ed. The National Nosocomial Infections Surveillance in Iran. A 4 years report. In: BMC Proceedings. BioMed Central Ltd; 2011. [Google Scholar]
- [42].Askarian M, Hosseini RS, Kheirandish P, et al. Incidence and outcome of nosocomial infections in female burn patients in Shiraz, Iran. Am J Infect Control 2004;32:23–6. [DOI] [PubMed] [Google Scholar]
- [43].Askarian M, Hosseini RS, Kheirandish P, et al. Incidence of urinary tract and bloodstream infections in Ghotbeddin Burn Center, Shiraz 2000–2001. Burns 2003;29:455–9. [DOI] [PubMed] [Google Scholar]
- [44].Wallace WC, Cinat M, Gornick WB, et al. Nosocomial infections in the surgical intensive care unit: a difference between trauma and surgical patients. Am Surg 1999;65:987–90. [PubMed] [Google Scholar]
- [45].Heydari ST, Hoseinzadeh A, Sarikhani Y, et al. Time analysis of fatal traffic accidents in Fars Province of Iran. Chin J Traumatol 2013;16:84–8. [PubMed] [Google Scholar]
- [46].Abbasi H, Bolandparvaz S, Yadollahi M, et al. Time distribution of injury-related in-hospital mortality in a trauma referral center in South of Iran (2010–2015). Medicine 2017;96:e6871. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [47].Tabrizi R, Akbari M, Lankarani KB, et al. Relationship between religion and school students’ road behavior in southern Iran. Chin J Traumatol 2017;pii: S1008-1275(16)30237-1. doi: 10.1016/j.cjtee.2016.12.001. [Epub ahead of print]. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [48].Yadollahi M, Ghiassee A, Anvar M, et al. Analysis of Shahid Rajaee hospital administrative data on injuries resulting from car accidents in Shiraz, Iran: 2011–2014 data. Chin J Traumatol 2017;20:27–33. [DOI] [PMC free article] [PubMed] [Google Scholar]